Imaging of spleen ct and mri
61
Imaging of the Spleen : CT with Supplemental MR Examination Radiographics 1994;14:307-332 Dr.Pankaj Kaira JR-II Radiodiagnosis SRMSIMS Bareilly,India
-
Upload
pankaj-kaira -
Category
Health & Medicine
-
view
260 -
download
0
Transcript of Imaging of spleen ct and mri

Imaging of the Spleen : CT with Supplemental MR Examination
Radiographics 1994;14:307-332
Dr.Pankaj KairaJR-II Radiodiagnosis
SRMSIMS Bareilly,India

Normal Anatomy of Spleen
• Splenic size and configuration are variable.• Typical parameters for normal spleen are 12x7x4
cm, with a weight of 150 gm (100-200gm).• The spleen closely relates anatomically to the
fundus of the stomach, upper pole of left kidney, and tail of the pancreas.
• Splenic trabeculae arises from the internal capsule, subdividing the organ into compartments consisting of a lattice of lympahtic follicles and reticuloendothelial cells (white pulp) and interspread vascular lakes (red pulp).

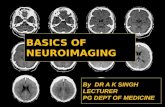
1) Enhanced helical CT scan through the spleen (short straight arrow), obtained after intravenous administration of contrast material, shows the stomach (open arrow), splenic artery (short curved arrow), splenic vein (long straight arrow), and pancreas (long curved arrow). (2) Histologic drawing demonstrates red and white pulpcompartments of the spleen.

CT Examination
• CT attenuation of splenic tissue is homogeneous, typically measuring 40-60 HU on noncontrast material-enhanced scans.
• Splenic attenuation is normally 5-10 HU less than that of liver, a standard of reference used in evaluation of either hepatic or splenicdisease.
• The spleen is optimally evaluated with use of intravenous contrast material.
• The spleen normally demonstrates heterogeneous enhancement, especially during the parenchymal phase of opacification after the administration of contrast.
• It is postulated that the cause for this heterogeneous enhancement relates to the unique histologic features of the vascular system of the spleen, with varying blood flow rates through the cords of red pulp in the spleen.
• One must be cautious and avoid misinterpretation of this early heterogeneity for focal splenic disease.

Dynamic contrastenhanced CT scan obtained after bolus contrast material administration shows normal heterogeneous enhancement of the spleen.

MR Examination
• The spleen is usually evaluated with both T1 and T2-weighted spin-echo (SE) images.
• On T1-weighted images, the normal MR signal intensity of the spleen is less than that of hepatic tissue and slightly greater than that of muscle.
• With T2-weighted images, the spleen demonstrates higher signal intensity, appearing brighter than liver.
• With splenic disease, high-signal-intensity areas on T1-weighted images may represent hemorrhage or high proteinaceous fluid.
• Cystic lesions or vascular masses (eg, hemangioma) have longer T2 relaxation values than those of the spleen and thus appear hyperintense relative to normal splenic tissue .The spleen demonstrates heterogeneous enhancement with dynamic ‘ ‘fast’ ‘ gradient- or spin-echo techniques after administration of Gd contrast.

Bacterial Abscess
• Causes : Immunocompromised patients,Leukemia, aggressive chemotherapy, IV drugs abuse and AIDS.
• (a) metastatic infection (eg, subacute bacterial endocarditis, sepsis) ,
• (b) contiguous infection (eg, infected pancreatitis, perinephric abscess),
• (C) embolic noninfectious events causing ischemia and subsequent superimposed infection,
• (d) trauma, and
• (e) immunodeficiency conditions

• CT is currently the diagnostic method of choice because of its high sensitivity (up to 96%), noninvasiveness, applicability in unstable patients, and value in allowing accurate localization of the lesion in relation to contiguous viscera .
• With CT examination, bacterial abscesses are frequently visualized as a low-attenuation center of fluid or necrotictissue .
• Minimal peripheral contrast enhancement may be present when a capsule has developed.
• The presence of gas in an intrasplenic collection is diagnostic for an abscess.A splenic abscess may contain septae of various thickness from 1 to 10 mm.


Fungal Microabscess
• Constitute up to 26% of splenic abscesses and
occur almost exclusively in individuals with a
compromised host defense mechanism.
• Candida fungus is most frequently encountered, followed by Aspergillus and Cryptococcus fungi.

• CT shows microabscesses to be multiple small lesions of relatively low attenuation
• Typical lesions are smaller than 2 cm in diameter and are usually 5-10 mm in size. Occasionally, a central focus of higher attenuation or a wheel-within-a-wheel pattern may be demonstrated.
• MR imaging may demonstrate multiple small lesions of
intermediate signal intensity on T1-weighted images and high signal intensity on T2-weighted images.
Ring like enhancement may be seen with contrast enhanced CT and Mri imaging.


Tuberculosis
• Infection with Mycobacterium tuberculosis of the spleen usually occurs in a miliary form by hematogenous dissemination.
• CT: May be seen as irregular areas of low attenuation.• Spleenomegaly.• When the lesions increase in size, they may appear as small focal
splenic nodules of low attenuation.• Occasionally, small peripheral wedge-shaped areas of low
attenuation may be present and represent infarcts from septic emboli.
• Abdominal lymphadenopathy of low attenuation may be present• High-attenuation ascites (25-45 HU), nodular peritoneal thickening,
hepatomegaly, and focal hepatic lesions may also occur. Healed calcified granulomas, often incidentally noted on abdominal CT.


Pneumocystitis Carinni infection of Spleen
• The organism appears to spread by both lymphatic and hematogenous routes.
• Intrasplenic P carinii infection is often discovered incidentally in the patient with AIDS who is undergoing CT examination for a fever of unknown origin.
• CT shows an enlarged spleen with focal low-attenuation splenic lesions, which may become progressively calcified either in rimlike or punctatefashion over a few months.
• Associated findings are punctate calcifications in the liver, kidneys, thyroid, and adrenal glands; calcification of lymph nodes; and pleural and peritoneal effusions with subsequent calcifications of the pleural and pentoneal surface.

Disseminated P carinii infection in a 32-year-old man with AIDS. Nonenhanced CT scan demonstrates extensive calcifications

Inflammatory Pseudotumor of Spleen
• Inflammatory pseudotumor is an extremely rare benign lesion of the spleen consisting of a well-circumscribed solitary mass composed of localized areas of inflammatory and reparative fibroblastic changes as well as a granulomatous component .
• The cause of inflammatory pseudotumor is not clear.• Nonenhanced CT demonstrates a rounded mass of low attenuation.
Calcification may be present in the mass.• After a bolus injection of contrast media, contrast enhancement is
observed with a progressive opacification of the lesion. • Central stellate areas of low attenuation may persist within the
mass, histologically corresponding to focal areas of fibrosis• MR imaging may demonstrate a well-defined mass better than CT,
reportedly isointense on T1-weighted images and with either increased or decreased signal intensity on T2-weighted images with respect to the surrounding normal spleen.
• Linear bands of very decreased signal intensity may be seen in the mass representing dense fibrous cords.


Splenic Cysts
• The nonneoplastic splenic cysts can be divided into two categories: primary (true) cysts, which possess a cellular lining, and secondary (false) cysts, which have no cellular lining.
• The primary cysts are either nonparasitic
(epidermoid) or parasitic (echinococcai).
• Parasitic cysts are rare in nonendemic areas.

• True parasitic (echinococcal) cysts rarely involve the spleen. Systemic dissemination and intraperitoneal spread from a ruptured liver cyst constitute the two most important sources of splenic infestation.
• Secondary or false cysts are presumed to result from either unrecognized trauma, previous infarction, or infection of the spleen.
• The contents of the cysts may be serous, hemorrhagic, inflammatory, or degenerative froman infarction.

• CT: Spherical, well-defined cystic lesions with attenuation equal to that of water, a thin or imperceptible wall, and no rim enhancement.
• Cyst wall trabeculation or peripheral septations.
• Cyst wall calcifications.
• Splenic cysts may have areas of increased attenuation resulting from hemorrhage, increased protein content, or infection within the cyst.

• MR : show a well-defined rounded mass with signal intensity equal to that of water with both T1 and T2-weighted sequences.
• However, depending on the protein or hemorrhagic content of the cystic fluid, signal intensity on T1-weighted images may be variable, whereas signal intensity on T2-weighted images remains quite high, characteristic of fluid.

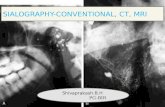
Epidermoid cyst of the spleen (nonparasitic, true cyst) in a 26-year-old man. Enhanced CT scan of the upper abdomen demonstrates a cystic mass occupying nearly the entire spleen. Very minimal peripheral rim calcification is present medially (arrow). The surgical specimen showed an epithelial lining of the cyst.
Calcified splenic cyst. CT scan clearly demonstrates calcification within a cyst of homogeneous

Echinococcal disease. Enhanced CT scan demonstrates multiple homogeneous cystic masses in both the liver and spleen, compatiblewith the diagnosis. Dilated periportal vessels arepresent.

Splenic Fluid collection associated with Pancreatitis
• Intrasplenic fluid collection associated with pancreatitis has been reported to occur in 1%-5% of patients with pancreatitis.
• Intrasplenic fluid collection is assumed to result from direct extension of a pancreatic pseudocyst, digestive effects of pancreatic enzymes on splenic vessels or parenchyma along the splenorenal ligament, or liquefaction of splenic infarcts as a result of thrombosis of the splenic vessels. In addition to intrasplenic fluid collections, CT usually reveals evidence of pancreatitis, including enlargement of the pancreas with ill-defined margins, obliteration of peripancreatic fat planes, or calcifications.

Intrasplenic Pseudocyst.CT scan demonstrates changes of acute andchronic pancreatitis. There are pancreatic calcifications, mild peripancreatic inflammation, and extension ofa pancreatic tail pseudocyst into the spleen.

Splenic Infarction
• Most common cause - embolic, occurring in cardiovascular disease (eg, endocarditis, atrialfibrillation, or left ventricular thrombus).
• Less frequent causes - local thromboses, especially in hematologic diseases (eg, myelofibrosis, sickle cell disease, leukemia, and lymphoma) and vasculitis.Pancreatic disease, splenic artery aneurysm, and splenic torsion, therapeutic result of transcatheter hepatic artery embolization.

• CT:• wedge-shaped, peripheral, hypoattenuating lesions .It is more
common, however, for splenic infarcts to appear round or irregular. • Contrast-enhanced CT markedly improves visualization of a splenic
infarct .Areas of splenic infarction may also appear as heterogeneous, poorly marginated, massive hypoattenuatinglesions that are indistinguishable from other splenic lesions, including abscesses or tumors
• In the hyperacute phase, CT may show areas of mottled increased attenuation, representing areas of a hemorrhagic infarct .
• In the acute and subacute phases, infarcts tend to become focal and progressively better demarcated.
• Chronic phase : They reveal progressive volume loss caused by fibrotic contraction of the infarct, with hypertrophy of the surrounding normal spleen. Occasionally, calcifications may result from an infarct and appear in either a curvilinear or punctate

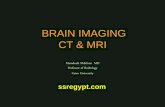
Infarct from Portal hypertension in a 46 years old man with hemochromatosis. T2 weighted MR image reveals a peripheral area of increased signal intensity with a dark rim,compatible with an infarct. Note the cirrhotic liver and markedly decreased signal intensity of the pancreas and the liver, compatible with primary hemochromatosis.
Autoinfarction of the spleen in a 56- year-old woman with sickle cell disease. Nonenhanced CT scan of the upper abdomen reveals a small spleen with calcification.

Sickle cell disease
• End-Stage Spleen (Autosplenectomy).-• The end-stage spleen, often seen in patients with
homozygous sickle cell disease, histologically shows extensive perivascular fibrosis with deposition of hemosidenn and calcium.
• CT - Small and densely calcified spleen .Calcifications may be amorphous, punctate, or rarely curvilinear.
• Splenic size may be as small as 0.5-1.0 cm.• MR imaging typically demonstrates diminished signal
intensity on T1- and T2-weighted images because of hemosiderin deposition (secondary hemochromatosis) and calcification.

Splenic Sequestration
• Acute splenic sequestration is a common complication of sickle cell disease and represents sudden trapping of a large amount of blood in the spleen, resulting in sudden splenic enlargement and a rapid decrease in hematocrit .
• Sequestration occurs almost exclusively during infancy and childhood in patients with homozygous sickle cell disease but may occur at any age in patients with heterozygous sickle cell disease. Hypovolemic shock and death may occur within hours.
• CT scans : The spleen is often enlarged, revealing peripheral hypoattenuating areas that may be interspersed with areas of higher attenuation, representing areas of infarct, pooling of blood, or hemorrhage .
• MR imaging may demonstrate areas of abnormal signal intensity on T1- and T2-weighted images, which may appear hyperintense with a dark rim on T1-weighted images, representing areas of subacutehemorrhage.

Enhanced CT scan shows an enlarged spleen with diffuse low attenuation and increased attenuation near the splenic hilum, representing sequestration of the spleen and hemorrhage.

• Rupture-Splenic rupture is a rare complication of sickle cell disease that occurs in an enlarged spleen often rendered weak by large or repeated infarctions. CT may show fluid or blood outside the spleen and evidence of intrasplenic hemorrhage and peripheral defects in the spleen.
• FunctionalAsplenia.-The spleen may be anatomically present but nonfunctional because of multiple previous infarctions. Nonfunction may also be indicated by absence of tracer uptake on a technetium-99m sulfur colloid scan.CT may show a normalsized or enlarged spleen with calcification.
• Infarction.-Splenic infarction may be encountered in adults with heterozygous sickle cell disease, in which case the spleen is generally enlarged. CT may show focal infarcts as peripheral segmental areas of low attenuation and hemorrhagic infarcts as areas of increased attenuation . Depending on the age of an infarct, the appearance on MR images is variable; it is most commonly seen in the subacute phase and appears as a segmental area of increased signal intensity on both Ti- and T2- weighted images.

• Hemosiderosis. -CT shows increased attenuation in the spleen from iron deposition in the reticuloendothelial system as well as calcium deposition. Ti- and T2-weighted MR images show diffuse diminished signal intensity of the spleen relative to musculature as a result of hemosidenn deposition (secondary hemochromatosis) and calcification.


Diffuse disease causing Spleenomegaly
• Splenomegaly can result from congestion (eg, portal hypertension, splenic vein occlusion, or thrombosis), infiltrative disease (eg, Gaucher disease, histiocytosis),hematologic disorders (eg, polycythemia vera,myelofibrosis), inflammatory disease (eg, infectious mononucleosis, Feltysyndrom, mycobacterial infection),cysts, or tumors (eg, leukemia, lymphoma,metastasis.




Benign Tumours of Spleen
• Hemangioma :• Hemangioma is the most common primary benign
neopiasm of the spleen, reportedly occurring in 0.03%-14% of cases at autopsy.
• These tumors are often found incidentally.• Splenic hemangiomas may be multiple, usually as part of a
generalized angiomatosis (Klippel-Trenaunay-Weber syndrome).
• Although a benign tumor, hemangioma is associated with life-threatening complications , like spontaneous splenicruptune
• Hemangiomatosis may be associated with portal hypertension.

• Hemangiomas of the spleen may appear either solid or cystic on CT scans and may enhance after administration of contrast material in a similar fashion to that of hepatic hemangioma .
• The MR imaging appearance of splenic hemangioma is similar to that of hemangioma ofthe liver: The lesion has low or isointensesignal intensity on Ti-weighted images and higher signal intensity on T2-weighted images with respect to that of the spleen.
• T2-weighted images may show heterogeneous signal intensities representing mixed cystic and solid components of a hemangioma
• Ti-weighted images obtainedafter administration of gadopentetatedimeglumine may allow better differentiation of cystic from solid masses.
• Ti-weighted images may show areas of high signal intensity• representing subacute hemorrhage or proteinaceous fluid.


Hamartoma
• Hamantoma of the spleen is a rare benign tumor without sex predilection, characteristically composed of anomalous mixtures of normal elements ofsplenic tissue .They are usually discovered as incidental findings at autopsy or exploratory laparotomy.
• Hamartomas are usually solid lesions that may contain a cystic or necrotic component.
• They usually appear iso- to hypoattenuating on nonenhanced CT scanshowever, occasionally these tumors are hyperattenuating due to
hemosidenin deposition• MR imaging may demonstrate a welldefined mass of isointensity on
T1-weighted images and high intensity on T2-weighted images• After administration of contrast material, prolonged enhancement
may be appreciated on both CT and MRI.



Lymphoma
• Lymphoma is the most common malignant tumor of the spleen. • Laparotomy with splenectomy reveals splenic involvement
in 23%-34% of patients with Hodgkin lymphomas• Similarly, 30%-40% of patients with non-Hodgkin lymphomas have
splenic involvement when they are initially seen . • CT and MR imaging are less sensitive for detection of splenic
involvement partly because 45%-70% of splenic lesions manifest with either diffuse tumor infiltration in the spleen or tumor foci well under a centimeter in size.
• Splenic lymphoma may be classified as either primary spleniclymphoma or lymphomatous involvement as part of diffuse systemic involvement. Primary or focal splenic lymphoma, without clinical evidence of nodal disease, is uncommon and occurs in 1% of all patients with non-Hodgkin lymphoma.

• CT is the primary tool for diagnosing lymphoma, evaluating the volume and extent of the tumor, and monitoring response to therapy .
• The CT appearances of splenic lymphoma mirror the variety of pathologic appearances.
• These appearances include (a) homogeneous enlargement without a discrete mass, (b) a solitary mass, (c) multifocal lesions, and (d) diffuse infiltration.

• The patterns of a solitary mass and multifocal lesions measuring 1 cm or greater in diameter are often detectable at CT and appear as discrete lesions of lower attenuation than that of surrounding splenic parenchyma
• Primary splenic lymphoma may be bulky ,transgress the splenic capsule, and involve adjacent organs including the diaphragm, stomach, pancreas, and abdominal wall .
• The appearance of infiltration on CT scans is typically one of diffuse low attenuation or diffuse irregularity of sp!enic enhancement .
• It is unusual for lymphoma to enhance, and thus splenic lesions are best defined after a dynamic bolus of iodinated contrast material.
• Necrosis of lymphoma is rare and may appear cystic, so that the differentiation of lymphoma from abscess may become difficult.
• Infarction of the spleen involved by lymphoma is not uncommon and typically appears as a peripheral wedge-shaped area of low CT attenuation .

• Calcifications in splenic lymphoma before or after treatment are rarely detected but, when seen, probably represent dystrophic calcification secondary to necrosis, hemorrhage, and subsequent fibrosis.
• The overall accuracy of CT in depicting splenic lymphoma is approximately 58%-65%.
• Depiction of splenic lymphoma by MR imaging is often not reliable because both the normal spleen and the lymphomatous tissue mayhave similar T1 and T2 relaxation times and proton densities. Therefore, in patients with splenic lymphoma, MR imaging may display similar signal intensities of the tumor and the surrounding normal spleen. When the lesions are cystic, necrotic, or hemorrhagic, they areeasier to detect.



Rare Splenic Tumors
• There are rare primary benign and malignant
splenic tumors, including lymphangioma, malignant fibrous histiocytoma, leiomyosarcoma and fibrosarcoma, all of which may have a nonspecific appearance of either a solid, cystic, or complex splenic mass.


Metastatic Disease
• Splenic involvement by metastases is seen relatively uncommonly but not rarely at autopsy, occurring in up to 7. 1% of patients with malignancy.
• Metastases are believed to be mainly a result of hematogenous spread, most commonly from cancer of the breast (21%), lung (i8%), ovary (8%), stomach (7%), cutaneous melanoma (6%), and prostate gland (6%) .
• On CT scans, splenic metastases are typically areas of slightly decreased attenuation in relation to the normal spleen .
• Lesions may be well defined as either cystic or solid masses. A cystic or necrotic mass may show contrast enhancement at the periphery and within septa ofthe lesion .
• Other lesions may be infiltrative and have lower CT attenuation than that of normal splenic tissue. Calcification of metastases is rare unless the primary tumor is a mucinous adenocarcinoma.
• Splenic metastases from melanoma have been seen in approximately 35% of patients at autopsy, whereas only 1.4%-4.5% of metastases are detected with CT examination .Melanoma commonly causes cystic splenicmetastases.


Peritoneal implants to the surface of Spleen
• Serosal implants to the spleen are seen with peritoneal carcinomatosis, most commonly from primary tumors of the ovary, but also inassociation with gastrointestinal adenocarcinoma and pancreatic cancer .
• CT typically shows scalloping of the surface of the spleen associated with solid or cystic penitoneal implants.
• Either psammomatous or dense calcifications may be present in a case of mucinous adenocarcinoma.
• Scalloping of the spleen in pseudomyxoma penitonei is invariably part of a widespread process that includes scalloping of the liver.
• Peritoneal implants may occasionally intrude into the splenicparenchyma from the serosal surface, which may mimic an intrasplenic mass.
• Use of either CT with intraperitoneal contrast material or MR imaging with air distention of the gastrointestinal tract note improved sensitivity for depiction of penitoneal implants.


Direct invasion of Spleen
• Direct invasion of the spleen is uncommon but may occur from a large gastric or colonic cancer, cancer of the tail of the pancreas, renal cell carcinoma of the left kidney, neuroblastoma, or retroperitoneal sarcoma.
• Peripancreatic or splenic hilar metastases may directly invade the spleen. In most cases, the spleen may be displaced by the adjacent tumor, with direct invasion being less common.
• When extrasplenic tumor extends to the splenicsurface, it may be difficult to separate tumor from spleen.


Conclusion
• Many diseases affecting the spleen have a similar appearance on cross-sectional images.
• Therefore, clinical history is often important in helping narrow the differential diagnosis of suspected splenicdisease.
• If uncertainty of a diagnosis persists, percutaneous biopsy may be useful.
• Because of its cross-sectional imaging capability and short imaging times, CT is currently the imaging method of choice for evaluation ofthe spleen.
• However, in patients who are allergic to iodinated contrast matenial, MR imaging may be valuable as an initial diagnostic tool for evaluation of suspected splenic disease.

Thank You