Imaging in first trimester
93
CHAIRMAN : DR. P.H PATIL CO-CHAIRMAN : DR. V.V HATTIHOLI PRESENTER : DR. JASREEN SIDANA
-
Upload
dr-jasreen-sidana -
Category
Health & Medicine
-
view
1.031 -
download
1
Transcript of Imaging in first trimester

CHAIRMAN : DR. P.H PATILCO-CHAIRMAN : DR. V.V HATTIHOLI
PRESENTER : DR. JASREEN SIDANA

The First Trimester is defined as the first 12 weeks of pregnancy following the last normal menstrual period.
(some authors refer to early pregnancy as 0 - 10 weeks).
It can be divided into a number of phases, each of which has typical clinical issues. These phases are:
1.Conceptus phase : 3 - 5 weeks2.Embryonic phase : 6 - 9 weeks3.Fetal phase : 10 - 12 weeks

It is a part of WHO recommended 3 antenatal visits.
To define the cause of vaginal bleeding.To evaluate pelvic pain.Palpable mass per abdomen.To exclude a non viable pregnancy or an
ectopic pregnancy.To document foetal number in case of
multiple gestation.

According to American College of Radiology(ACR) and American Institute of Ultrasound in medicine (AIUM), Ultrasound during this period is predominantly concerned with the following clinical issues:
1.CONFIRMING INTRAUTERINE PREGNANCY (IUP)
2. DATING OF THE PREGNANCY
3. EARLY PREGNANCY FAILURE
4. NUCHAL LUCENCY
5. ECTOPIC PREGNANCY
6. FIRST TRIMESTER MASSES
Sonographic appearance of the normal IUP includes the visualization of –
1.GESTATIONAL SAC2.YOLK SAC3.EMBRYO AND AMNION4.EMBRYONIC CARDIAC ACTIVITY5.UMBILICAL CORD AND CORD CYST

1.GESTATIONAL SAC
Earliest sonographic finding in pregnancy.
The GS is an echogenic ring (formed by chorio-emryoniccells) surrounding an anechoic centre (as fluid filled).
An ectopic pregnancy will appear the same but it will not be within the endometrial cavity.
The GS is not identifiable until approximately 4 1/2 weeks with a transvaginal scan and 5 weeks with TAS.


Decidual ReactionThe hypertrophic changes of the endometrium which occur as a hormonal response regardless of the site of implantation, intrauterine or ectopic.
Before ovulation, endometrial proliferation occurs in response to the estrogen secretion.
After ovulation, the endometrium becomes thickened, soft and edematous under the influence of the progesterone. The glandular epithelium secretes a glycogen rich fluid. If pregnancy occurs, continued production of progesterone results in more hypertrophic changes in the endometrial cells and glands to provide nourishment to the blastocyst.

Endometrium in the pregnant state is actually called decidua, which has three layers namely :
1.Decidua capsularis2.Decidua vera3.Decidua basalis

INTRADECIDUAL SAC SIGN:
First reliable gray scale evidence of an IUP is visualization of the gestational sac within the thickened decidua ( echogenic focal area at the site of implantation).
An intradecidual gestational sac should be eccentrically located within the endometrium and should abut the endometrial canal.
It is important to ensure that the sac abuts the endometrial canal to distinguish an intra-uterine gestational sac from a decidual cyst.


DOUBLE DECIDUAL SIGN
Described by Nyberg et al, as a method to differentiate between an early IUP and the pseudosac of the ectopic pregnancy.
Visualized by about 5.5 – 6 weeks of GA It is based on visualization of two echogenic rings. The inner ring is formed by the gestational sac as an
echogenic ring formed by the decidua capsularis and chorionic laeve eccetrically.
The outer ring is formed by the echogenic ring of the lining of the uterus ( formed by decidua parietalis).




Normal gestational sac can be differentiated from pseudosac as the normal GS :
Implants immediately beneath the echogenicendometrium stripe
As it enlarges, becomes oval in shapeCan be distorted during TVS examinationGS is filled with chorionic sac fluid that is
normally more echogenic than the amniotic fluid.
2.YOLK SAC Transfer of the nutrients to the developing embryo
in the third and fourth week. Angiogenesis : occurs in the wall of the yolk sac in
the fifth week. Vascular network formed by the angioblasts in the wall of the yolk sac eventually joins the fetal circulation via the paired vitelline arteries and veins through a stalk called vitelline duct.
Hematopoeisis: in fifth week Determination of the amnionicity of a multifetal
pregnancy.
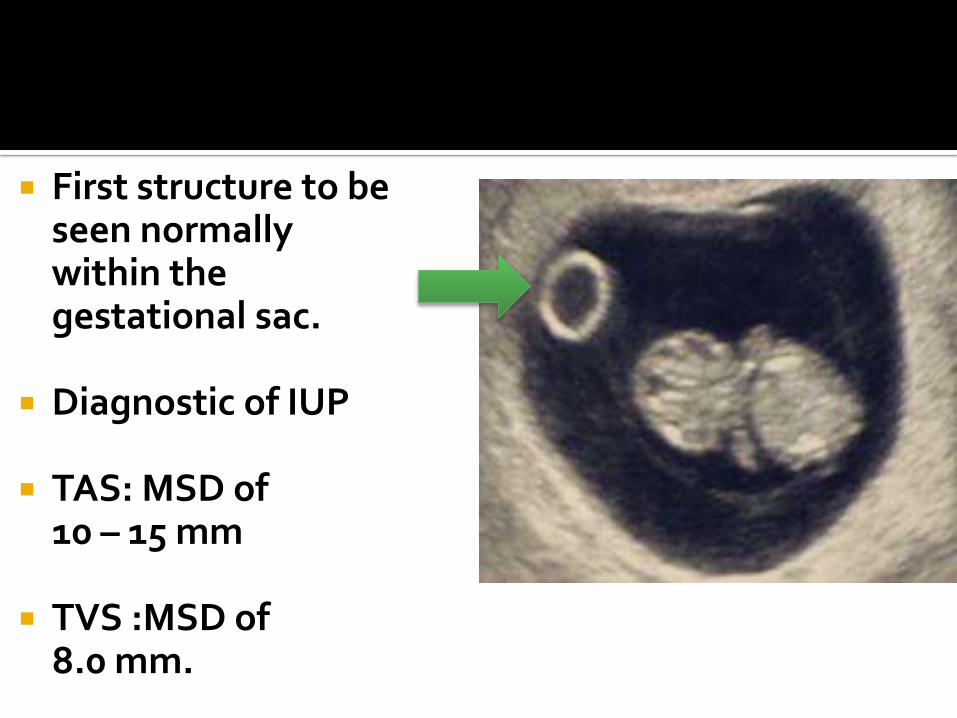
First structure to be seen normally within the gestational sac.
Diagnostic of IUP
TAS: MSD of 10 – 15 mm
TVS :MSD of 8.0 mm.

3. AMNIONDouble bleb sign: it is a
sonographic feature where there is visualisation of a gestational sac containing a yolk sac and amniotic sac giving an appearence of two small bubbles . The embryonic disc is located between the two bubbles.
It can be identified as early as 51/2 weeks when the CRL is 2.0mm.


The 2 sacs are clearly visible.
The outer chorion with the developing placenta and the inner amnion which will "inflate" with the production of fetal urine, to adhere to the chorionobliterating the residual yolk sac.

EMBRYO At 51/2 weeks, when the CR length is 2.o mm,
embryonic disc is situated between the yolk sac and amnion.
As the resolution of the ultrasound equipment improves, visualization of the embryonic structures become possible.
4. EMBRYONIC CARDIAC ACTIVITY
Using a trans-vaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified.
It will be seen alongside the yolk sac.
It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks.
In the early scans at 5-6 weeks just visualizing a heart beating is the important thing.
Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm (approx 4.5 weeks)is an ominous sign .

The very early embryonic heart will be a subtle flicker.
This may be measured using M-Mode(avoid Doppler in the first trimester due to risks of bioeffects).
Initially the heart rate may be slow.
It is advisable to compare the maternal heart rate to confirm that one is not seeing an arteriole.

5.UMBILICAL CORD AND CORD CYST Formed at the end of the sixth week. Contents : all of which are embedded in
Wharton’s jelly.Two umbilical arteriessingle umbilical veinallantoisYolk stalk


Cysts and pseudocysts within the cord occur in first trimester.
Seen usually in 8th week and disappear by 12th
week. Singular, with a mean size of 5.2 mm. Originate from the remnants of allantois or
yolk stalk and have an epithelial lining. If seen in 2nd and 3rd trimester they are
associated with chromosomal abnormalities.

In order of their appearance, the following structures can be measured as indicators of the gestational age:
1.Gestational sac ( MSD)2.CRL ( crown – rump length) 3.Biparietal diameter
1.Gestational sacFrom 5 – 6 weeks gestation, two methods are
used to assign gestational age by USG:1. Mean sac diameter 2. Sonographic identification of the
gestational sac contents

MEAN SAC DIAMETER : the average internal diameter of the gestational sac, is calculated as the mean of the AP, transverse and the longitudinal diameter.
Normally, a yolk sac will be present when MSD : 8 .0 mm.
Embryo will be present when MSD : 16.0 mm.


MSD between 2-14 mm are accurate in predicting the gestational age, before the embryo is seen.

2.CROWN – RUMP LENGTH ( up to 11 weeks)
GA closely correlates with CR length from 6 weeks until the end of the first trimester.
The CRL is the length of the embryo or fetus from the top of its head to the bottom of its torso.
It is measured as the longest dimension of the embryo, excluding the yolk sac and extremities.

Once, the embryo can be visualized ( after 7 weeks), the measurement of choice for estimation of GA becomes crown rump length.
MSD becomes progressively less reliable for predicting GA as the first trimester of pregnancy advances.


3.BIPARIETAL DIAMETER:By the end of the first trimester, measurement
of the BPD becomes more accurate than the CRL, which by that time reflects errors due to biological variabilities.
In addition to BPD, corrected BPD, and HC are the parameters which involve the fetal head.


Rules for measurement of the BPD: 1. Correct plane of section is taken through
the third ventricle and paired thalami. 2. the calvaria should be smooth and
symmetrical bilaterally. 3.the cursors are positioned correctly.

Measured from the outer edge of the cranium nearest the transducer to the inner edge farthest from the transducer.
Corrected BPD =square root of BPD X OFD/ 1.265Significance: it represents the BPD of the
standard shaped head ( one with an OFD / BPD ratio of 1.265) of the same cross sectional area.

Nuchal translucency is referred to as normal subcutaneous fluid filled space between the back of the fetal neck and the overlying skin.
It is a measurement performed during a specific period in the first trimester (11.3-13.6 weeks).
An increased nuchal translucency is thought to relate to dilated lymphatic channels.

1. Only values obtained when CRL values are between 45-84 mm are considered valid.
2. The lucent region is generally not septated.
3. The thickness rather than the appearance (morphology) is considered to be directly related to the incidence of chromosomal and other anomalies.
4. A normal value is usually less than roughly 2.5-3.0 mm in thickness however it is maternal age dependent needs to be matched to exact gestational age and crown rump length (CRL).

The fetus should be transverse (sagittal) in the imaging plane.
The vertebral column should be facing the bottom of the screen.
Fetal head should not be extended or flexed
Fetus should be floating free of the uterine wall (i.e. amniotic fluid should be seen between its back and the uterus)
Only the lucency is measured (again differing from nuchal thickness)
Ideally only the head and upper thorax should be included in the measurement
The level of magnification should be appropriate (fetus should occupy most of the image).
The widest part of the measurement should be taken

The nuchal translucency cannot be adequately assessed if there is :
Unfavourable fetal lieUnfavourable GA: CRL < 45 or > 84 mm.



Interpretation Detection rates for aneupliodic
anomalies with nuchaltranslucency alone approaches 80 -90 % with a false positive rate of ~ 5%.
Correlation With Serum Markers
To increase the clinical accuracy of nuchal
lucency, it can be correlated with serum markers such as
maternal B-HCG alpha feto protein (AFP) pregnancy associated plasma
protein A (PAPP-A) oestriol
Further work up
If abnormal > further work up is carried out which includes
Amniocentesis and / or Chorionic Villussampling
Fetal echocardiography
Natural course - progression As the second trimester approaches, the
region of nuchal translucency might either Regress :
if chromosomally normal, a large proportion of fetuses will have a normal outcome
spontaneous regression does not however mean a normal karyotype
Evolve into a
Nuchal Oedema
Cystic Hygroma

Can be done using sonographic criteria:
1. Embryonic cardiac activity2. Gestational sac features3. Amnion and yolk sac criteria4. Doppler ultrasound assessment
1. Embryonic cardiac activity The presence of cardiac activity indicates that
the embryo is alive. The absence of cardiac activity does not
necessarily indicate embryonic demise, however, because TVS can identify a normal early embryo without cardiac activity.

Embryonic bradycardia:Doubilet and Benson found that a heart rate
less than 80 beats / min in embryos with a CRL less than 5.0 mm was universally associated with subsequent embryonic demise.
Normal : (120 or more beats/ min)Arrhythmias : another indicator of the first trimester loss.
Most common is ventricular bradycardia.


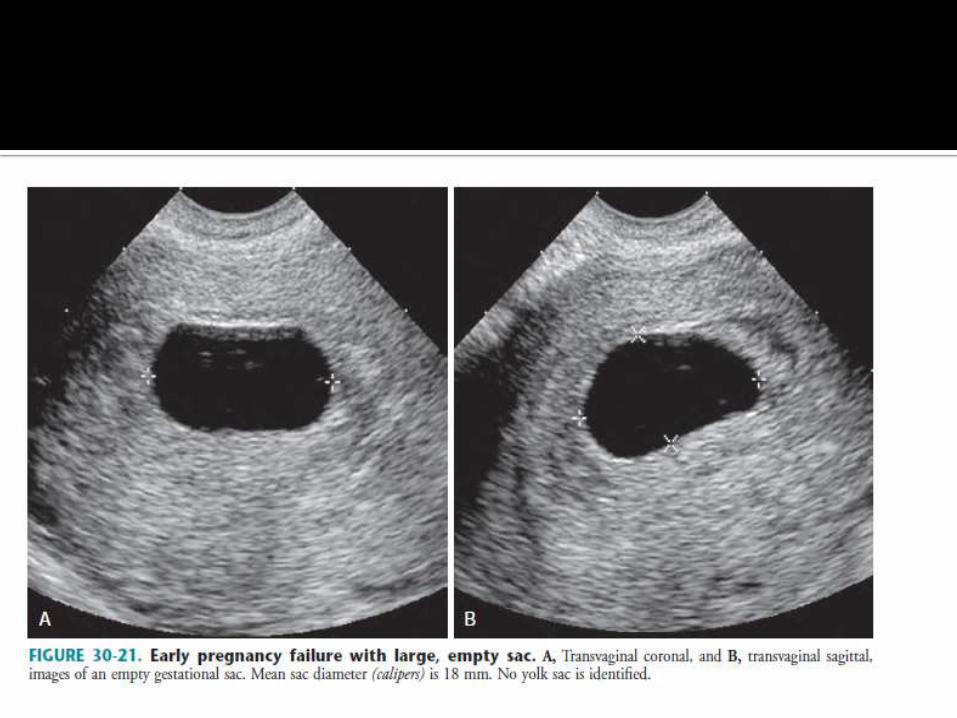
2.Gestational sac features Abnormal size :Nyberg et al refined the definition of an
abnormal gestational sac as MSD of 25.0mm or more without an embryo, or MSD of 20.0 mm or more without a yolk sac.

Bromley et al found that difference between the MSD and CRL should not be less than 5.0 mm.
So if, between to 9 weeks’ GA with MSD less than 5.0mm greater than CRL. ( i.e MSD- CRL = <5.0mm), sometimes termed as early oligohydramnios.

Other features include :• Distorted GS shape• Thin trophoblastic reaction• Weakly echogenic trophoblast• Abnormally low position of the GS within the
endometrial cavity.


4. Amnion and yolk sac criterion Visualization of the amnion in the absence of a
sonographically demonstrable embryo after 7 weeks’ MA is abnormal and diagnostic of the non viable pregnancy.
The amnion is visualized after the embryo. So it should never be visualized in the absence of the embryo.
Other findings that may be useful in the diagnosis of the embryonic demise include a collapsing, irregularly marginated amnion and yolk sac calcification.


Yolk sac size :Internal diameter
of the yolk sac greater than 5.6 mm between 5 and 10 weeks is always associated with the abnormal outcome.


In general if the MSD is 16 mm or greater and no fetal pole / yolk sac can be identified on trans-vaginal scanning then this suggests a non-viable pregnancy (an-embryonic pregnancy).
Repeat scanning with an larger MSD and serial quantitative beta-HCGs is however thought prudent.
In a normal early pregnancy, the diameter of the yolk sac should usually be < 6 mm while its shape should be near spherical.
Natural course As the pregnancy advances, the yolk sac disappears and is
often sonographically not detectable after 14 weeks.

Other abnormalities include :Calcified yolk sac : shadowing echogenic mass.Seen with a dead embryo and may calcify
within 36 hours after demise.

Doppler ultrasound assessment:Assessment of the uterine or spiral arteries for:1.Resistive index2.Pulsatility index
In the normal pregnancy, the indices within these vessels demonstrate a progressive decline from 6 to 12 weeks of POG.the basis for this drop in early pregnancy is
the development of the intervillouscirculation.

1.Resistive indexIf RI < 0.55 - normal pregnancyIf RI >0.55 - corresponds to the high pressure
blood flow, seen in cases with pre eclampsiaand IUGR. Subsequently, leading to miscarriage resulting in early pregnancy failure.

2. Pulsatility indexHigher in the women with recurrent
pregnancy loss andElevated levels of antiphospholipid
antibodies.


A CRL of ≥ 7mm without a heart beat on a transvaginal ultrasound confirms the diagnosis
Additional clues are presence of abnormal hyperechoic material within the uterine cavity and an irregular gestational sac.
If there is an absence of heart beat in a fetus that is less than 7mm, the diagnosis of miscarriage cannot be made with certainty.
This scenario is termed "Pregnancy Of Uncertain Viability (PUV)", and followup with ultrasound (generally in 7-10 days) and serial bHCGrecommended.

Irregular Sac.
Hyperechoic collection within the sac.

A subchorionic haemorrhage is often seen, but unless large does not carry a poor prognosis.
Features which do predict poor outcome include:
• Fetal bradycardia : < 80 - 90 bpm• Small or Irregular Gestational Sac : MSD -
CRL < 5 mm• Large Subchorionic Haemorrhage


One important difference is to be deduced between an actual irregular sac & a sac which appears irregular due to Braxton-Hick’s contractions.
The former one, will not change its shape to become normal with time.

Refers to the presence of an open cervix in the context of bleeding in the first trimester of pregnancy.
Essentially, a threatened abortion progresses to an inevitable abortion if cervical dilatation occurs. Once tissue has passed through the cervical os, this will then be termed an incomplete abortion and ultimately a complete abortion.

Shows an empty
uterus with no
fetal components
or products of
conception

Retained Products of Conception, still seen within
the uterine / cervical cavity.

An anembryonicpregnancy may be diagnosed when there is no fetal pole identified on trans-vaginal scanning the size of the gestational sac is such that a fetal pole should be seen.
MSD ≥ 25 mm (by RCOG criteria)
There is little or no growth of the gestational sac between interval scans
Normally the MSD should increase by 1 mm per day
If MSD is too small to ascertain viability on the initial ultrasound, a follow up scan in 10-14 days should differentiate early pregnancy from a failed pregnancy


Other ancillary features include
Absent yolk sac when MSD > 8 mm
Poor decidual reaction : often < 2 mm
Irregular gestational sac shape
Abnormally low sac position

Ectopic pregnancy refers to the implantation of a fertilised ovum outside of the uterine cavity.
Risk factors : Any tubal abnormality that may prevent passage of the
zygote or result in the delayed transit Previous tubal pregnancy h/o tubal reconstructive surgery IUCD insertion Increased maternal age Increased parity Previous caesarean section

TUBAL ECTOPIC : 93 - 97%
Ampullary Ectopic : most common : ~ 70 % of tubal ectopics and ~ 65 - 68 % of all ectopics.
Isthmal Ectopic : ~ 12 % of tubal ectopics and ~ 11 % of all ectopics
Fimbrial Ectopic : ~ 11 % of tubal ectopics and ~ 10 % of all ectopics
ATYPICAL ECTOPIC PREGNANCIES Interstitial Ectopic - cornual ectopic : 3 - 4 % :
Ovarian Ectopic - ovarian pregnancy : 0.5 - 1%
Cervical Ectopic - cervical pregnancy : rare < 1 %
Scar Ectopic : site of previous Caesarian section scar : rare
Abdominal Ectopic : rare ( ~ 1.4%)
Specific signs include:1. Demonstration of the pseudosac2. Peritrophoblastic flow3. Demonstration of live embryo in the adnexa
Non specific signs include:1. Correlation with serum beta HCG levels2. Assessment of the suspected ectopic mass3. Ectopic tubal ring4. Free pelvic fluid

TVS must be the first line of imaging investigation. Because TVS allows for better visualization of the endometrium, endometrial canal and adnexa than TAS.
Pseudosac / pseudogestational sac / decidual cast : is an intrauterine fluid collection surrounded by single decidual layer as opposed to the two concentric rings of the double decidual sign.

Peritrophoblasticflow : colour flow doppler imaging helps in assessing the peritrophoblasticflow.It is high velocity, low resistance flow with low RI and PI.


Correlation with the serum beta HCG levels:Negative beta HCG excludes the presence of a live
pregnancy.Threshold level of beta HCG above which it is
always possible to identify a normal intrauterine gestational sac
TAS : above 1800mIU/mlTVS: 500 – 1000mIU/mlIf an intrauterine GS is not identified, ectopic
pregnancy becomes the diagnosis of exclusion.

Adnexal mass assessment :Conditions other than ectopic pregnancy
include:• Hemorrhagic corpus luteum cyst• Endometriosis• Abscess

Suspected ectopic mass should be assessed during TVS for:
• Local tenderness• Movement of the ectopic pregnancy separate
from the ovary as the probe pressure is applied ( specific for tubal pregnancy which is most common).


Free pelvic fluid : TVS is sensitive in detecting free pelvic fluid.The presence of the echogenic free fluid or blood
clots in the cul de sac, without sonographicevidence of an IUP, suggests EP.

Patients in whom the site of implantation has not been identified with certainty have been categorized as having PUL.
DIAGNOSTIC CRITERIA: Empty endometrial cavity with1. An inhomogeneous adnexal mass2. Extrauterine gestational sac with or without a
yolk sac and / or embryonic pole. Differentials include:1. Very early IUP2. Abnormal IUP3. Ectopic pregnancy

Diagnosis is made when a live embryo is demonstrated in the adnexa in a patient with an intrauterine gestational sac.
Suspected in patients undergoing ovulatoryinduction or IVF.


First trimester sonography plays an important role in establishing the location of the pregnancy and determining if the pregnancy is potentially viable.
Knowledge of the landmarks with respect to the appearance of structures appearing during first trimester are important in the triage of patients who present with pain and bleeding in the first trimester.

Dignostic ultrasoundCarol M Rumack Ultrasonography in obstetrics and
gynaecologyCallen

OPPORTUNITY IS MISSED BY MOST PEOPLE BECAUSE IT IS DRESSED IN OVERALLS AND LOOKS LIKE WORK!!!