iMAgES iN rESPirATOry MEDiCiNEdownloads.hindawi.com/journals/crj/2015/236130.pdf · 2019-07-31 ·...
3
Can Respir J Vol 22 No 3 May/June 2015 133 A 20-year-old Ecuadorian woman had a positive purified protein derivative (PPD) test during routine prenatal evaluation. A chest radiograph (CXR) performed at that time was normal. Treatment for latent tuberculosis infection was not initiated. She had an uneventful delivery and then presented more than one year later with cough, fever and night sweats. Posteroanterior and lateral CXR performed in the emergency department revealed atelectasis of the right upper lobe (RUL), with superomedial retraction of the minor fissure (Figure 1A and 1B). Sputum cultures for acid fast bacilli (AFB) subsequently grew Mycobacterium tuberculosis, and the patient was started on a multidrug regimen, which was narrowed once the organism was confirmed to be sensitive. To further evaluate the nature of her RUL atelectasis, com- puted tomography (CT) of the chest was performed following admin- istration of intravenous contrast, which was consistent with compression of the RUL bronchus by an adjacent mediastinal lymph node (Figure 1C and 1D). Bronchoscopic inspection undertaken to exclude neoplasia revealed a mass-like protrusion at the level of the RUL bronchial orifice that was covered with normal-appearing mucosa (Figure 1E and 1F). Endobronchial biopsies of this entity were negative for malignancy and granulomas. The patient’s RUL atelecta- sis was, thus, attributed to extrinsic obstruction by a tuberculous medi- astinal lymph node. ©2015 Pulsus Group Inc. All rights reserved Not your ‘garden variety’ atelectasis Justin Seashore MD 1 , Oleg Epelbaum MD 1,2 IMAGES IN RESPIRATORY MEDICINE 1 Department of Medicine and 2 Division of Pulmonary and Critical Care Medicine, Elmhurst Hospital Center, Icahn School of Medicine at Mount Sinai, New York, New York, USA Correspondence: Dr Justin Seashore,Elmherst Hospital Center, 79-01 Broadway, New York, New York 11373, USA. Telephone 718-334-3122, e-mail [email protected] Figure 1) A Posteroanterior chest radiograph showing right upper lobe (RUL) atelectasis with upward displacement of the minor fissure. B Lateral chest radiograph. C Computed tomography (CT) scan of the chest showing a mediastinal lymph node occupying the expected location of the RUL bronchus take-off (red arrow). Adjacent lymph node calcification is evident (blue arrow). There is resultant RUL atelectasis. D CT chest coronal reconstruction demonstrating obstruction at the level of the expected origin of the RUL bronchus (arrow). E Bronchoscopic image of the lesion at the level of the main carina. F Bronchoscopic image at the level of the right mainstem bronchus A B C D E F
Transcript of iMAgES iN rESPirATOry MEDiCiNEdownloads.hindawi.com/journals/crj/2015/236130.pdf · 2019-07-31 ·...

Can Respir J Vol 22 No 3 May/June 2015 133
A 20-year-old Ecuadorian woman had a positive purified protein derivative (PPD) test during routine prenatal evaluation. A chest
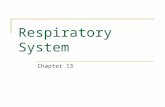
radiograph (CXR) performed at that time was normal. Treatment for latent tuberculosis infection was not initiated. She had an uneventful delivery and then presented more than one year later with cough, fever and night sweats. Posteroanterior and lateral CXR performed in the emergency department revealed atelectasis of the right upper lobe (RUL), with superomedial retraction of the minor fissure (Figure 1A and 1B). Sputum cultures for acid fast bacilli (AFB) subsequently grew Mycobacterium tuberculosis, and the patient was started on a multidrug regimen, which was narrowed once the organism was confirmed to be
sensitive. To further evaluate the nature of her RUL atelectasis, com-puted tomography (CT) of the chest was performed following admin-istration of intravenous contrast, which was consistent with compression of the RUL bronchus by an adjacent mediastinal lymph node (Figure 1C and 1D). Bronchoscopic inspection undertaken to exclude neoplasia revealed a mass-like protrusion at the level of the RUL bronchial orifice that was covered with normal-appearing mucosa (Figure 1E and 1F). Endobronchial biopsies of this entity were negative for malignancy and granulomas. The patient’s RUL atelecta-sis was, thus, attributed to extrinsic obstruction by a tuberculous medi-astinal lymph node.
©2015 Pulsus Group Inc. All rights reserved
Not your ‘garden variety’ atelectasisJustin Seashore MD1, Oleg Epelbaum MD1,2
iMAgES iN rESPirATOry MEDiCiNE
1Department of Medicine and 2Division of Pulmonary and Critical Care Medicine, Elmhurst Hospital Center, Icahn School of Medicine at Mount Sinai, New York, New York, USA
Correspondence: Dr Justin Seashore,Elmherst Hospital Center, 79-01 Broadway, New York, New York 11373, USA. Telephone 718-334-3122, e-mail [email protected]
Figure 1) A Posteroanterior chest radiograph showing right upper lobe (RUL) atelectasis with upward displacement of the minor fissure. B Lateral chest radiograph. C Computed tomography (CT) scan of the chest showing a mediastinal lymph node occupying the expected location of the RUL bronchus take-off (red arrow). Adjacent lymph node calcification is evident (blue arrow). There is resultant RUL atelectasis. D CT chest coronal reconstruction demonstrating obstruction at the level of the expected origin of the RUL bronchus (arrow). E Bronchoscopic image of the lesion at the level of the main carina. F Bronchoscopic image at the level of the right mainstem bronchus
A
B
C
D
E F

Images in Respiratory Medicine
Can Respir J Vol 22 No 3 May/June 2015134
KEY LEARNING POINTS
• Obstructive RUL atelectasis is most commonly caused by neoplasia, mainly primary lung malignancy or mucus impaction.
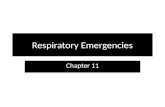
• When the cause of RUL atelectasis is a central lung tumour, one can often appreciate the ‘reverse S-sign of Golden’ on the posteroanterior chest radiograph (Figure 2).
• The anatomy of the right middle lobe (RML) bronchus renders it particularly vulnerable to chronic or recurrent benign atelectasis due to either extrinsic bronchial compression or intrinsic bronchial narrowing. This phenomenon has been termed ‘RML syndrome’ (1). No such predisposition is known to exist in the case of the RUL.
• One of the best-described causes of RML syndrome is extrinsic compression by a calcified tuberculous right hilar lymph node (Figure 3). While recognized in children with mediastinal lymphadenopathy from primary tuberculosis, RUL atelectasis caused by a tuberculous mediastinal lymph node in an adult with reactivation tuberculosis is unusual.
• RUL atelectasis due to inflammatory intrinsic bronchial narrowing caused by M pneumoniae has been reported recently, as has compression of the RUL bronchus by calcified lymphadenopathy from presumed blastomycosis (2,3). Our case similarly alerts the clinician about another ‘non-garden variety’ cause of RUL atelectasis in a young patient.
The ‘Images in Respiratory Medicine’ section of the Canadian Respiratory Journal aims to highlight the importance of visual interpretation, whether physiological, radiological, bronchoscopic, surgical/thorascopic or histological, in the diagnosis of chest diseases. Submissions should exemplify a classic, particularly dramatic or intriguing presentation of a disease while offering an important educational message to the reader (insightful diagnostic pearls or differential diagnosis, etc). This section is not intended to be a vehicle for publication of case reports (see the Clinical-Pathologic-Conferences for case-based leaning series).
REFERENCES1. Gudbjartsson T, Gudmundsson G. Middle lobe syndrome: A review
of clinicopathological features, diagnosis and treatment. Respiration 2012;84:80-6.
2. Miyashita N, Kawai Y, Akaike H, et al. Atelectasis caused by macrolide-resistant Mycoplasma pneumoniae pneumonia in an adult patient. J Infect Chemother 2013;19:1161-6.
3. A Gillson, A Tremblay. A recalcitrant foreign body. Can Respir J 2012;19:189.
Figure 2) The reverse S-sign of Golden. A central lung mass (orange) causing right upper lobe atelectasis (green arrow) with resultant concavity of the superolateral aspect of the minor fissure and convexity of its inferomedial aspect, which resembles a reverse letter ‘S’ (blue). Image courtesy of Dr Frank Gaillard and radiopaedia.org
Figure 3) Axial chest computed tomography image showing right middle lobe atelectasis due to bronchial compression caused by a calcified post-tuberculous right hilar lymph node

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com