III III SESSIONE: TUMORI TORACICI -...
68
III III SESSIONE: TUMORI TORACICI NUOVI DATI NSCLC B. Di Cocco UOC Oncologia Osp S.M. Goretti ASL Latina
Transcript of III III SESSIONE: TUMORI TORACICI -...
III III SESSIONE: TUMORI TORACICI
NUOVI DATI NSCLC
B. Di Cocco UOC Oncologia
Osp S.M. Goretti ASL Latina





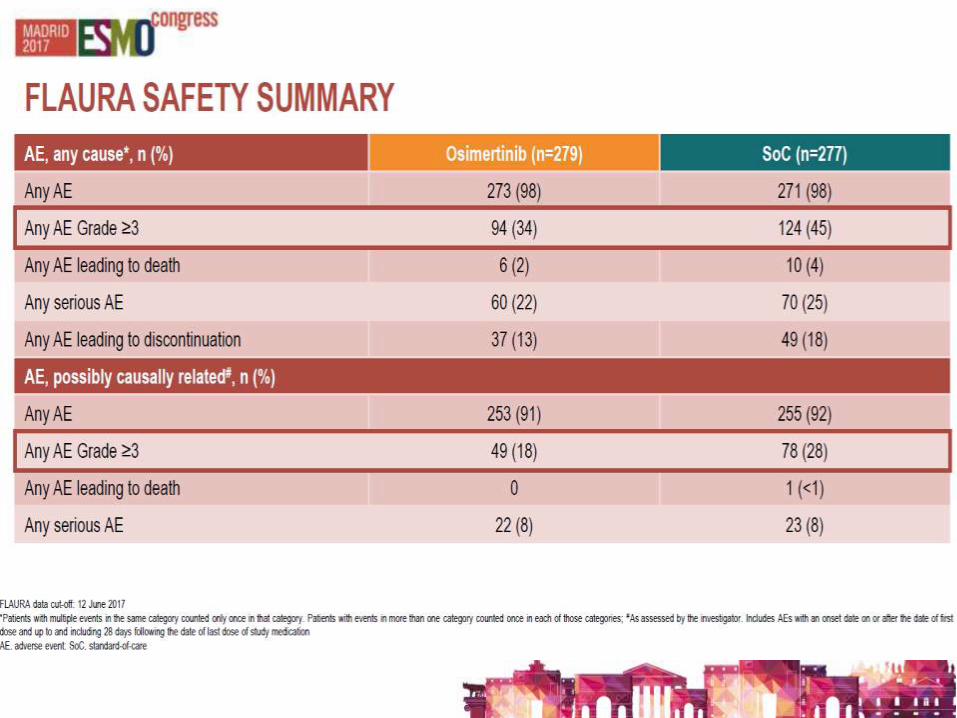
CheckMate 153: Continuous vs 1-Year Nivolumab
Study Design
• At database lock (May 15, 2017), minimum/median follow-up time post-randomization was 10.0/14.9 months
12
aConventional systemic therapies, excluding immuno-oncology therapies; bTreatment until PD, unacceptable toxicity, or withdrawal of consent; treatment beyond investigator-assessed PD permitted; cAll patients on treatment at 1 year were randomized regardless of response status; dPrimary endpoint was incidence of high-grade select treatment-related AEs1,2; eResponses were investigator-assessed every 8 weeks ± 5 days from week 9
1. Hussein M, et al. Oral presentation at IASLC 16th World Conference on Lung Cancer; September 6–9, 2015; Denver, CO, USA. Abstract ORAL02.02. 2. Waterhouse D, et al. Poster presentation at ASCO Annual Meeting; June 3–7, 2016; Chicago, IL, USA. Abstract 3059.
Exploratory endpointsd: safety/efficacye with continuous vs 1-year treatment, efficacy, other (eg, biomarkers, PK)
Key eligibility criteria
• Advanced/ metastatic NSCLC
• ≥1 prior systemic therapya
• ECOG PS 0−2
• Treated CNS metastases allowed
Stop nivolumab
Continuous nivolumab
Nivolumab
3 mg/kg IV Q2W
Treatment for 1 yearb
Rc
Nivolumab retreatment allowed at PD

CheckMate 153: Continuous vs 1-Year Nivolumab
Patient Flow and Analysis Populations
13
Stop nivolumab
Continuous nivolumab
1,245 patients treateda
220 patients on
treatment at
1 year
76 had response or SD
at randomizationc
87 had response or SD
at randomizationd
Rb
Efficacy analyses
aMain US cohort; 1,025 patients discontinued prior to 1 year due to progression, death, study withdrawal, toxicity, or other reasons; bAll 220 patients continuing on treatment at 1 year were randomized regardless of response status; 57 of these 220 patients had PD and were randomized as allowed per protocol; safety analyses were based on all 220 patients, 107 in the continuous arm and 113 in the stop arm; c8 patients discontinued treatment due to patient request or withdrawal of consent; d12 patients discontinued treatment due to patient request or withdrawal of consent

CheckMate 153: Continuous vs 1-Year Nivolumab
Baseline Patient Characteristics (Efficacy Analyses)a
14
Continuous treatment (n = 76) 1-year treatmentb (n = 87)
Median age, years (range) ≥70 years, %
67 (50−92) 41
67 (49−86) 40
Female, % 51 45
ECOG PS,c % 0−1 2
91 8
95 2
Current or former/never smoker, % 96/4 97/3
Squamous histology, % 34 47
PD-L1 status,d %
Quantifiable <1%e
≥1%e ≥50%e
53 32 68 28
60 25 75 23
Prior lines of therapy,f % 1 2 ≥3
41 33 26
40 28 29
CR or PR prior to randomization,g % 70 56
aPatients who did not have PD at randomization; bWith optional retreatment allowed at PD; cNot reported: continuous, n = 1; 1-year, n = 2; dUsing Dako PD-L1 IHC 28-8 pharmDx assay; ePercentage of patients with quantifiable PD-L1 expression; fNot reported: continuous, n = 0; 1-year, n = 3; gCRs: continuous, n = 8; 1-year, n = 2
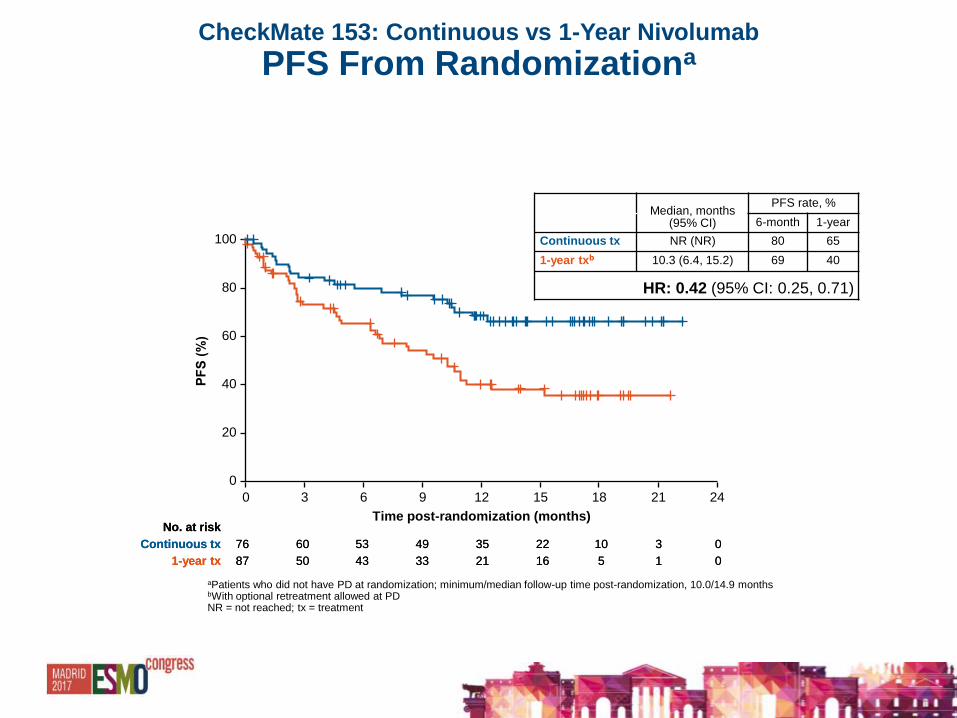
CheckMate 153: Continuous vs 1-Year Nivolumab
PFS From Randomizationa
15
aPatients who did not have PD at randomization; minimum/median follow-up time post-randomization, 10.0/14.9 months bWith optional retreatment allowed at PD NR = not reached; tx = treatment
Median, months (95% CI)
PFS rate, %
6-month 1-year
Continuous tx NR (NR) 80 65
1-year txb 10.3 (6.4, 15.2) 69 40
HR: 0.42 (95% CI: 0.25, 0.71)
No. at risk
1-year tx
Continuous tx
87 50 43 33 21 16 5 1 0
76 60 53 49 35 22 10 3 0
No. at risk
1-year tx
Continuous tx
87 50 43 33 21 16 5 1 0
76 60 53 49 35 22 10 3 0
Time post-randomization (months)
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24
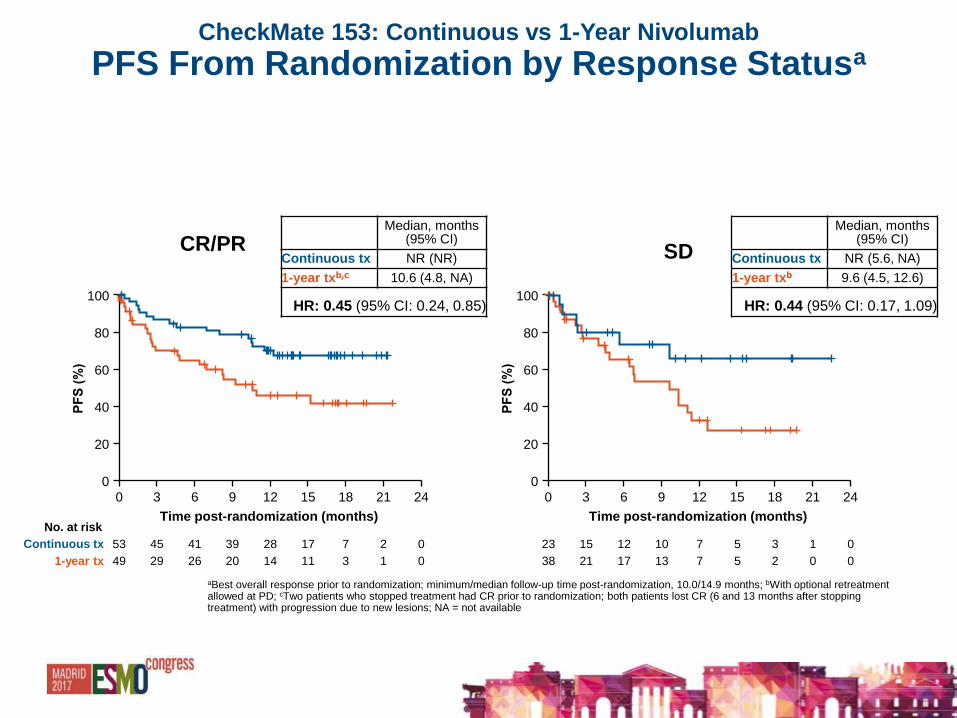
CheckMate 153: Continuous vs 1-Year Nivolumab
PFS From Randomization by Response Statusa
16
Median, months (95% CI)
Continuous tx NR (NR)
1-year txb,c 10.6 (4.8, NA)
HR: 0.45 (95% CI: 0.24, 0.85)
Median, months (95% CI)
Continuous tx NR (5.6, NA)
1-year txb 9.6 (4.5, 12.6)
HR: 0.44 (95% CI: 0.17, 1.09)
CR/PR SD
aBest overall response prior to randomization; minimum/median follow-up time post-randomization, 10.0/14.9 months; bWith optional retreatment allowed at PD; cTwo patients who stopped treatment had CR prior to randomization; both patients lost CR (6 and 13 months after stopping treatment) with progression due to new lesions; NA = not available
1-year tx 49 29 26 20 14 11 3 1 0
Continuous tx 53 45 41 39 28 17 7 2 0
No. at risk
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24
Time post-randomization (months)
38 21 17 13 7 5 2 0 0
23 15 12 10 7 5 3 1 0
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24
Time post-randomization (months)
n HR (95% CI)
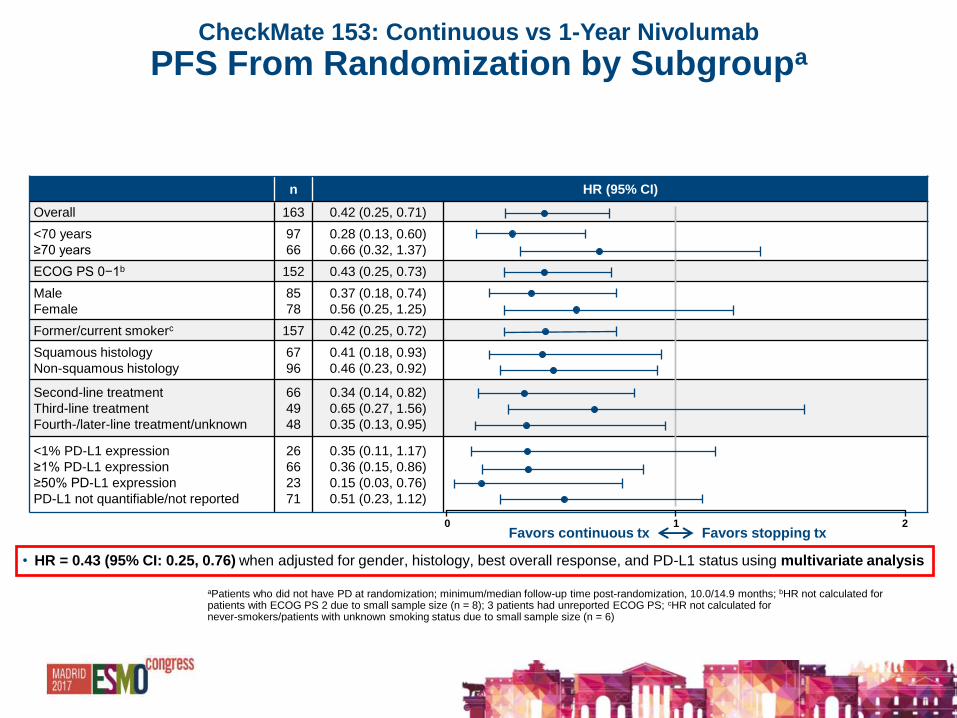
Overall 163 0.42 (0.25, 0.71)
<70 years
≥70 years
97
66
0.28 (0.13, 0.60)
0.66 (0.32, 1.37)
ECOG PS 0−1b 152 0.43 (0.25, 0.73)
Male
Female
85
78
0.37 (0.18, 0.74)
0.56 (0.25, 1.25)
Former/current smokerc 157 0.42 (0.25, 0.72)
Squamous histology
Non-squamous histology
67
96
0.41 (0.18, 0.93)
0.46 (0.23, 0.92)
Second-line treatment
Third-line treatment
Fourth-/later-line treatment/unknown
66
49
48
0.34 (0.14, 0.82)
0.65 (0.27, 1.56)
0.35 (0.13, 0.95)
<1% PD-L1 expression
≥1% PD-L1 expression
≥50% PD-L1 expression
PD-L1 not quantifiable/not reported
26
66
23
71
0.35 (0.11, 1.17)
0.36 (0.15, 0.86)
0.15 (0.03, 0.76)
0.51 (0.23, 1.12)
0 1 2 Favors continuous tx Favors stopping tx
CheckMate 153: Continuous vs 1-Year Nivolumab
PFS From Randomization by Subgroupa
17
• HR = 0.43 (95% CI: 0.25, 0.76) when adjusted for gender, histology, best overall response, and PD-L1 status using multivariate analysis
aPatients who did not have PD at randomization; minimum/median follow-up time post-randomization, 10.0/14.9 months; bHR not calculated for patients with ECOG PS 2 due to small sample size (n = 8); 3 patients had unreported ECOG PS; cHR not calculated for never-smokers/patients with unknown smoking status due to small sample size (n = 6)

CheckMate 153: Continuous vs 1-Year Nivolumab
OS From Randomizationa
18
aPatients who did not have PD at randomization; minimum/median follow-up time post-randomization, 10.0/14.9 months bWith optional retreatment allowed at PD
Median, months (95% CI)
OS rate, %
6-month 1-year
Continuous tx NR (NR) 97 88
1-year txb 23.2 (23.2, NA) 95 81
HR: 0.63 (95% CI: 0.33, 1.20)
74 72 67 62 41 29 7 2 0
79 74 70 61 38 23 4 0 0
No. at risk
1-year tx
Continuous tx
87
76
Time post-randomization (months)
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27

CheckMate 153: Continuous vs 1-Year Nivolumab
Retreatment in 1-Year Treatment Arm
19
aMain US cohort; 1,025 patients discontinued prior to 1 year due to progression, death, study withdrawal, toxicity, or other reasons; bAll 220 patients continuing on treatment at 1 year were randomized regardless of response status; 57 of these 220 patients had PD and were randomized as allowed per protocol; safety analyses were based on all 220 patients, 107 in the continuous arm and 113 in the stop arm; c8 patients discontinued treatment due to patient request or withdrawal of consent; d12 patients discontinued treatment due to patient request or withdrawal of consent
Stop
nivolumabd
Continuous
nivolumabc
1,245 patients
treateda
220 patients
on treatment
at 1 year
76 had response
or SD at
randomization
87 had response
or SD at
randomization
Rb
Efficacy analyses
43 (49%) had PD
after stopping
nivolumab
34 (79%) were
retreated with
nivolumab
Data at time of analysis (database lock May 15, 2017)
CheckMate 153: Continuous vs 1-Year Nivolumab
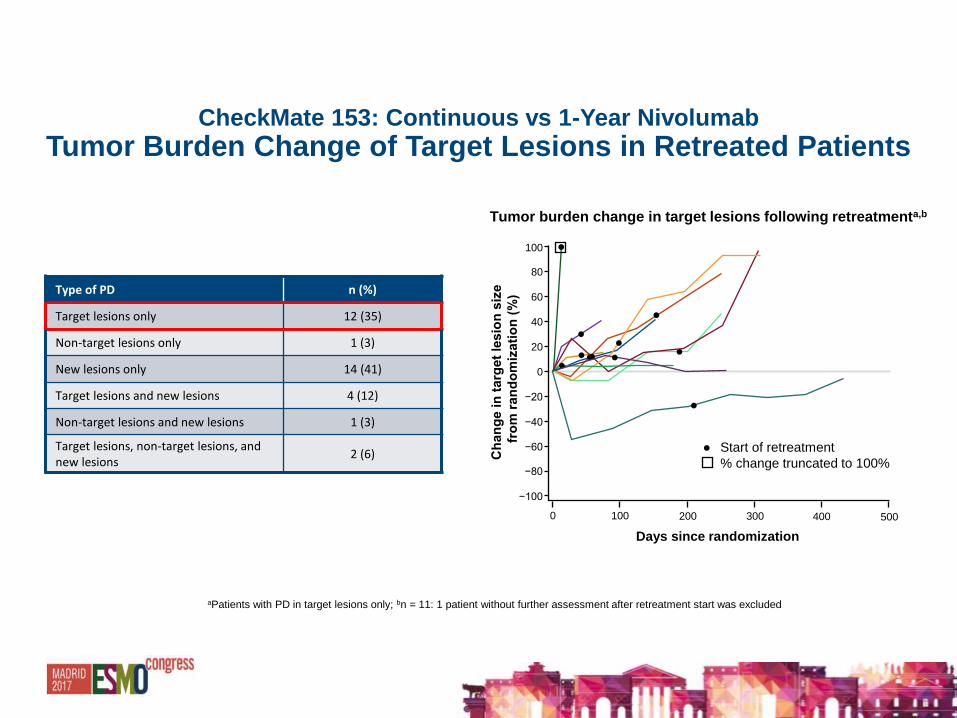
Tumor Burden Change of Target Lesions in Retreated Patients
20
aPatients with PD in target lesions only; bn = 11: 1 patient without further assessment after retreatment start was excluded
Type of PD n (%)
Target lesions only 12 (35)
Non-target lesions only 1 (3)
New lesions only 14 (41)
Target lesions and new lesions 4 (12)
Non-target lesions and new lesions 1 (3)
Target lesions, non-target lesions, and new lesions
2 (6)
Tumor burden change in target lesions following retreatmenta,b
● Start of retreatment
% change truncated to 100%
Days since randomization
−100
−80
−60
−40
−20
0
20
40
60
80
100
0 100 200 300 400 500
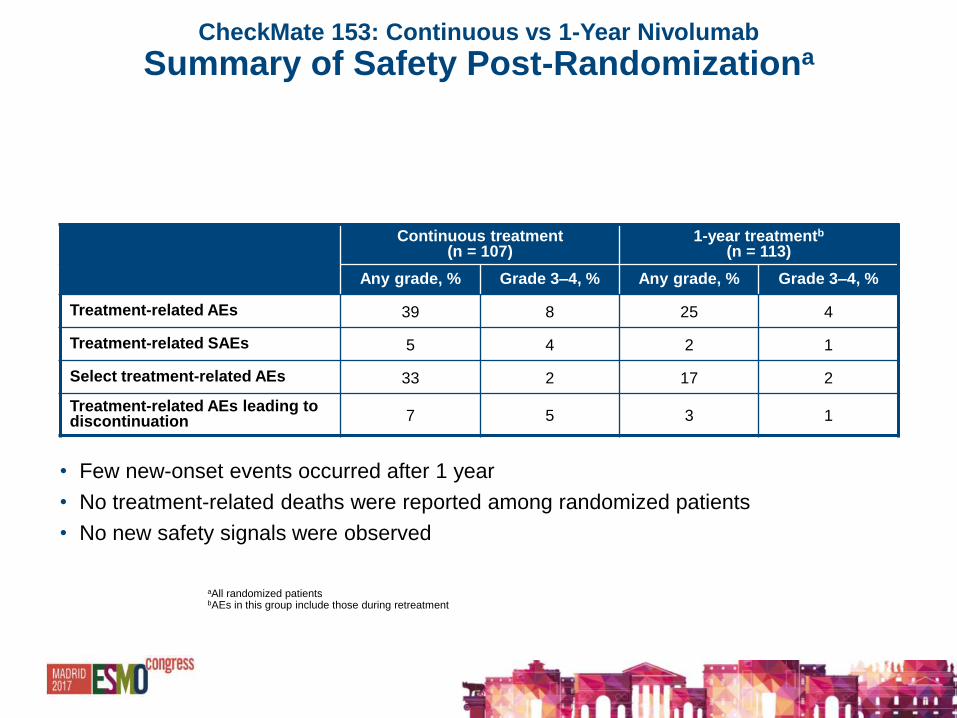
Continuous treatment (n = 107)
1-year treatmentb
(n = 113)
Any grade, % Grade 3–4, % Any grade, % Grade 3–4, %
Treatment-related AEs 39 8 25 4
Treatment-related SAEs 5 4 2 1
Select treatment-related AEs 33 2 17 2
Treatment-related AEs leading to discontinuation 7 5 3 1
CheckMate 153: Continuous vs 1-Year Nivolumab
Summary of Safety Post-Randomizationa
• Few new-onset events occurred after 1 year
• No treatment-related deaths were reported among randomized patients
• No new safety signals were observed
21
aAll randomized patients bAEs in this group include those during retreatment

CheckMate 153: Continuous vs 1-Year Nivolumab
Summary
• CheckMate 153 is the first randomized study to evaluate duration of therapy with
a PD-1/PD-L1 inhibitor
• Among patients still on nivolumab at 1 year, PFS was significantly improved for
those treated continuously vs stopping: PFS HR = 0.42 (95% CI: 0.25, 0.71)
• OS HR = 0.63 (95% CI: 0.33, 1.20), showing a trend favoring continuous
nivolumab; follow-up for OS is ongoing
• The frequency of treatment-related AEs was numerically higher with continuous
vs 1-year treatment, but overall, few new-onset events occurred after 1 year
22

Three-Year Follow-up From CheckMate 017/057: Nivolumab Versus Docetaxel in
Patients With Previously Treated Advanced Non-Small Cell Lung Cancer
• Enriqueta Felip,1 Scott Gettinger,2 Marco Angelo Burgio,3 Scott J. Antonia,4 Esther Holgado,5 David Spigel,6 Oscar Arrieta,7 Manuel Domine,8 Osvaldo Arén Frontera,9 Julie Brahmer,10 Laura Q. Chow,11 Lucio Crinò,3 Charles Butts,12 Bruno Coudert,13 Leora Horn,14 Martin Steins,15 William J. Geese,16 Ang Li,16 Diane Healey,16 Everett E. Vokes17
•1Hospital Universitari Vall d’Hebron, Barcelona, Spain; 2Yale Cancer Center, New Haven, CT, USA; 3IRCCS Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori, Meldola, Italy; 4H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL, USA; 5Hospital De Madrid, Norte Sanchinarro, Madrid, Spain; 6Sarah Cannon Research Institute/Tennessee Oncology, PLLC, Nashville, TN, USA; 7Instituto Nacional de Cancerología, Mexico City, Mexico; 8Fundación Jiménez Díaz, Madrid, Spain; 9Centro Internacional de Estudios Clinicos, Santiago, Chile; 10The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, MD, USA; 11University of Washington, Seattle, WA, USA; 12Cross Cancer Institute, Edmonton, AB, Canada; 13Centre Georges François Leclerc, Dijon, France; 14Vanderbilt-Ingram Cancer Center, Nashville, TN, USA; 15Thoraxklinik, Heidelberg University Hospital, Heidelberg, Germany; 16Bristol-Myers Squibb, Princeton, NJ, USA; 17University of Chicago Medicine & Biological Sciences, Chicago, IL, USA
Background
•Nivolumab, an anti–programmed death (PD)-1 antibody, is approved in many countries for the treatment of patients with advanced non-small cell lung cancer (NSCLC) and disease progression during or after platinum-based chemotherapy1,2
•Approval was based on data from 2 pivotal phase 3 trials in previously treated patients with squamous (SQ) NSCLC (CheckMate 017) or non-SQ NSCLC (CheckMate 057), which showed nivolumab significantly prolonged overall survival (OS) and had a favorable safety profile compared with docetaxel3,4
–Treatment benefit was observed in patients with SQ or non-SQ NSCLC, including those with <1% PD-1 ligand 1 (PD-L1) expression3-6; higher levels of PD-L1 expression were associated with a greater magnitude of benefit in non-SQ NSCLC4
•Here, we present updated efficacy and safety data from CheckMate 017 and CheckMate 057 based on >3 years of follow-up

CheckMate 017 and 057 study designs
aThe protocols of both studies were amended in September 2016, when minimum follow-up was approximately 2.5 years, allowing patients to switch to nivolumab 480 mg Q4W starting 2 weeks after their last 3-mg/kg Q2W dose; bAfter completion of the primary analyses,3,4 patients in the docetaxel arms who ended treatment at any time during the studies were allowed to cross over to nivolumab
ALK = anaplastic lymphoma kinase; ECOG PS = Eastern Cooperative Oncology Group performance status; EGFR = epidermal growth factor receptor; IV = intravenous; LCSS = Lung Cancer Symptom Scale; ORR = objective response rate; PFS = progression-free survival; Q3W = every 3 weeks; TKI = tyrosine kinase inhibitor
Nivolumab 3 mg/kg IV Q2W until progressive disease or
unacceptable toxicity (n = 292)
Docetaxel 75 mg/m2 IV Q3W until progressive disease or
unacceptable toxicityb
(n = 290)
Nivolumab 3 mg/kg IV Q2W until progressive disease or
unacceptable toxicity (n = 135)
CheckMate 017 (NCT01642004; N = 272)
CheckMate 057 (NCT01673867; N = 582)
Key eligibility criteria
• Stage IIIB/IV SQ NSCLC
• ECOG PS 0–1
• 1 prior platinum-based chemotherapy
• Pretreatment (archival or fresh) tumor
samples required for PD-L1 analysis
Key eligibility criteria
• Stage IIIB/IV non-SQ NSCLC
• ECOG PS 0–1
• 1 prior platinum-based chemotherapy
• Pretreatment (archival or fresh) tumor
samples required for PD-L1 analysis
• Prior maintenance therapy allowed
• Prior TKI therapy allowed for known ALK
translocation or EGFR mutation
Endpoints
• Primary
‒ OS
• Additional
‒ PFS
‒ ORR
‒ Efficacy by tumor PD-L1 expression
‒ Safety
‒ Quality of life (LCSS)
Optional switch to flat dose nivolumab 480 mg
Q4W allowed after September 2016a
Optional switch to flat dose nivolumab 480 mg
Q4W allowed after September 2016a
Docetaxel 75 mg/m2 IV Q3W until progressive disease or
unacceptable toxicityb
(n = 137)

OS (3 years’ minimum follow-up)
CI = confidence interval; HR = hazard ratio
292 194 148 112 82 58 49 39 7 0
290 195 112 67 46 35 26 16 1 0
135 86 57 38 31 26 21 16 8 0
137 69 33 17 11 10 8 7 3 0
CheckMate 057 (non-SQ NSCLC) CheckMate 017 (SQ NSCLC)
No. of patients at risk Nivolumab
Docetaxel
No. of patients at risk Nivolumab
Docetaxel
0 6 12 18 24 30 36 42 48 54
Δ10%
Nivolumab (n = 135) Docetaxel (n = 137)
1-y OS = 42%
2-y OS = 23% 3-y OS = 16% 1-y OS = 24%
2-y OS = 8% 3-y OS = 6%
HR (95% CI): 0.62 (0.48, 0.80)
100
80
60
40
20
0
Months
Δ18%
Δ15%
0 6 12 18 24 30 36 42 48 54 Months
1-y OS = 51%
2-y OS = 29% 3-y OS = 18%
1-y OS = 39%
2-y OS = 16% 3-y OS = 9%
Nivolumab (n = 292) Docetaxel (n = 290)
HR (95% CI): 0.73 (0.62, 0.88)
100
80
60
40
20
0
Δ12%
Δ13% Δ9%
3-year OS rates nivolumab vs docetaxel CheckMate 017 were 16% versus 6% CheckMate 057 were 18% versus 9%

PFSa (3 years’ minimum follow-up)
aInvestigator-assessed
NC = not calculable
292 82 47 39 29 20 18 10 2 0
290 89 22 7 4 3 1 0 0 0
135 48 24 17 16 13 10 7 3 0
137 27 8 1 0 0 0 0 0 0
CheckMate 017 (SQ NSCLC)
1-y PFS = 21% 2-y PFS = 16%
3-y PFS = 12%
1-y PFS = 7% 2-y PFS = NC 3-y PFS = NC
100
80
60
40
20
0 0 6 12 18 24 30 36 42 48 54
Months
Nivolumab (n = 135) Docetaxel (n = 137)
HR (95% CI): 0.63 (0.48, 0.82)
CheckMate 057 (non-SQ NSCLC)
1-y PFS = 19%
2-y PFS = 12% 3-y PFS = 10%
1-y PFS = 10% 2-y PFS = 2% 3-y PFS = <1%
100
80
60
40
20
0 0 6 12 18 24 30 36 42 48 54
Months
Nivolumab (n = 292) Docetaxel (n = 290)
HR (95% CI): 0.89 (0.74, 1.06)
No. of patients at risk Nivolumab
Docetaxel
No. of patients at risk Nivolumab
Docetaxel
3-year PFS rates nivolumab and docetaxel
CheckMate 017: 12% versus not calculable
CheckMate 057 and 10% versus <1%
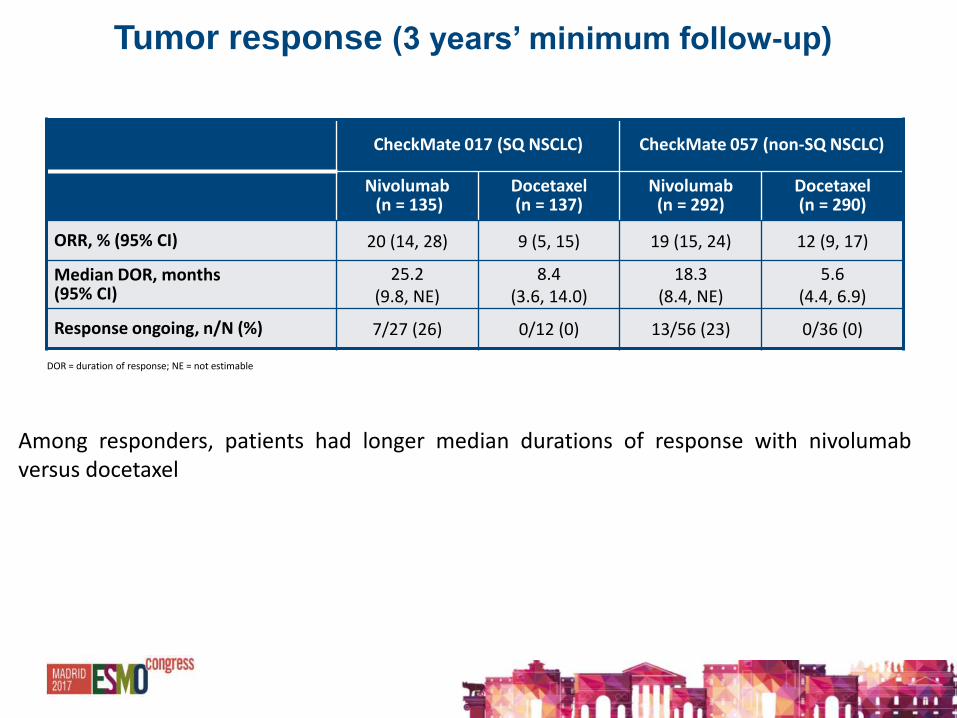
Tumor response (3 years’ minimum follow-up)
DOR = duration of response; NE = not estimable
CheckMate 017 (SQ NSCLC) CheckMate 057 (non-SQ NSCLC)
Nivolumab (n = 135)
Docetaxel (n = 137)
Nivolumab (n = 292)
Docetaxel (n = 290)
ORR, % (95% CI) 20 (14, 28) 9 (5, 15) 19 (15, 24) 12 (9, 17)
Median DOR, months (95% CI)
25.2 (9.8, NE)
8.4 (3.6, 14.0)
18.3 (8.4, NE)
5.6 (4.4, 6.9)
Response ongoing, n/N (%) 7/27 (26) 0/12 (0) 13/56 (23) 0/36 (0)
Among responders, patients had longer median durations of response with nivolumab versus docetaxel
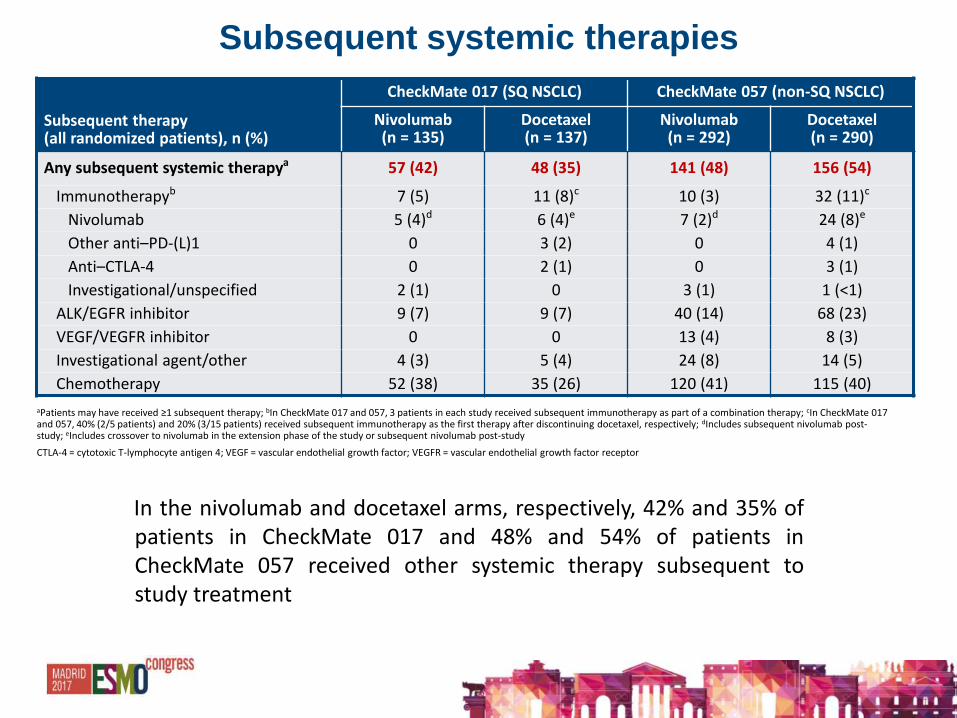
Subsequent systemic therapies
aPatients may have received ≥1 subsequent therapy; bIn CheckMate 017 and 057, 3 patients in each study received subsequent immunotherapy as part of a combination therapy; cIn CheckMate 017 and 057, 40% (2/5 patients) and 20% (3/15 patients) received subsequent immunotherapy as the first therapy after discontinuing docetaxel, respectively; dIncludes subsequent nivolumab post-study; eIncludes crossover to nivolumab in the extension phase of the study or subsequent nivolumab post-study
CTLA-4 = cytotoxic T-lymphocyte antigen 4; VEGF = vascular endothelial growth factor; VEGFR = vascular endothelial growth factor receptor
Subsequent therapy (all randomized patients), n (%)
CheckMate 017 (SQ NSCLC) CheckMate 057 (non-SQ NSCLC)
Nivolumab (n = 135)
Docetaxel (n = 137)
Nivolumab (n = 292)
Docetaxel (n = 290)
Any subsequent systemic therapya 57 (42) 48 (35) 141 (48) 156 (54)
Immunotherapyb 7 (5) 11 (8)c 10 (3) 32 (11)c
Nivolumab 5 (4)d 6 (4)e 7 (2)d 24 (8)e
Other anti–PD-(L)1 0 3 (2) 0 4 (1)
Anti–CTLA-4 0 2 (1) 0 3 (1)
Investigational/unspecified 2 (1) 0 3 (1) 1 (<1)
ALK/EGFR inhibitor 9 (7) 9 (7) 40 (14) 68 (23)
VEGF/VEGFR inhibitor 0 0 13 (4) 8 (3)
Investigational agent/other 4 (3) 5 (4) 24 (8) 14 (5)
Chemotherapy 52 (38) 35 (26) 120 (41) 115 (40)
In the nivolumab and docetaxel arms, respectively, 42% and 35% of patients in CheckMate 017 and 48% and 54% of patients in CheckMate 057 received other systemic therapy subsequent to study treatment
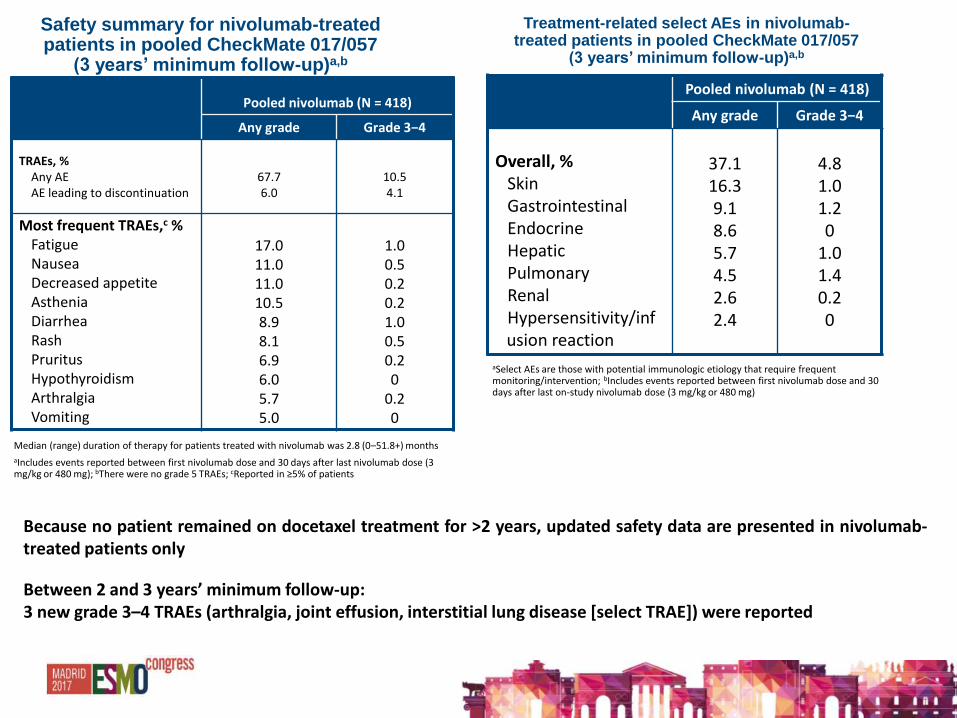
Pooled nivolumab (N = 418)
Any grade Grade 3−4
TRAEs, % Any AE AE leading to discontinuation
67.7 6.0
10.5 4.1
Most frequent TRAEs,c % Fatigue Nausea Decreased appetite Asthenia Diarrhea Rash Pruritus Hypothyroidism Arthralgia Vomiting
17.0 11.0 11.0 10.5 8.9 8.1 6.9 6.0 5.7 5.0
1.0 0.5 0.2 0.2 1.0 0.5 0.2 0
0.2 0
Safety summary for nivolumab-treated patients in pooled CheckMate 017/057
(3 years’ minimum follow-up)a,b
Median (range) duration of therapy for patients treated with nivolumab was 2.8 (0–51.8+) months
aIncludes events reported between first nivolumab dose and 30 days after last nivolumab dose (3 mg/kg or 480 mg); bThere were no grade 5 TRAEs; cReported in ≥5% of patients
Pooled nivolumab (N = 418)
Any grade Grade 3−4
Overall, %
Skin Gastrointestinal Endocrine Hepatic Pulmonary Renal Hypersensitivity/infusion reaction
37.1 16.3 9.1 8.6 5.7 4.5 2.6 2.4
4.8 1.0 1.2 0
1.0 1.4 0.2 0
Treatment-related select AEs in nivolumab-treated patients in pooled CheckMate 017/057
(3 years’ minimum follow-up)a,b
aSelect AEs are those with potential immunologic etiology that require frequent monitoring/intervention; bIncludes events reported between first nivolumab dose and 30 days after last on-study nivolumab dose (3 mg/kg or 480 mg)
Because no patient remained on docetaxel treatment for >2 years, updated safety data are presented in nivolumab-treated patients only
Between 2 and 3 years’ minimum follow-up: 3 new grade 3–4 TRAEs (arthralgia, joint effusion, interstitial lung disease [select TRAE]) were reported

Authors’ Conclusions
After 3 years’ minimum follow-up in the phase 3 CheckMate 017 and 057 studies:
• Nivolumab continued to demonstrate long-term OS and PFS benefit in patients with advanced SQ and non-SQ NSCLC
• 3-year OS rates with nivolumab were 16% in CheckMate 017 and 18% in CheckMate 057
• In CheckMate 017 and CheckMate 057, 26% and 23% of patients who responded to nivolumab, respectively, had ongoing tumor responses
• No new safety signals were identified for nivolumab and rates of TRAEs were similar to those seen at 2 years’ minimum follow-up

NSCLC: TARGET THERAPY


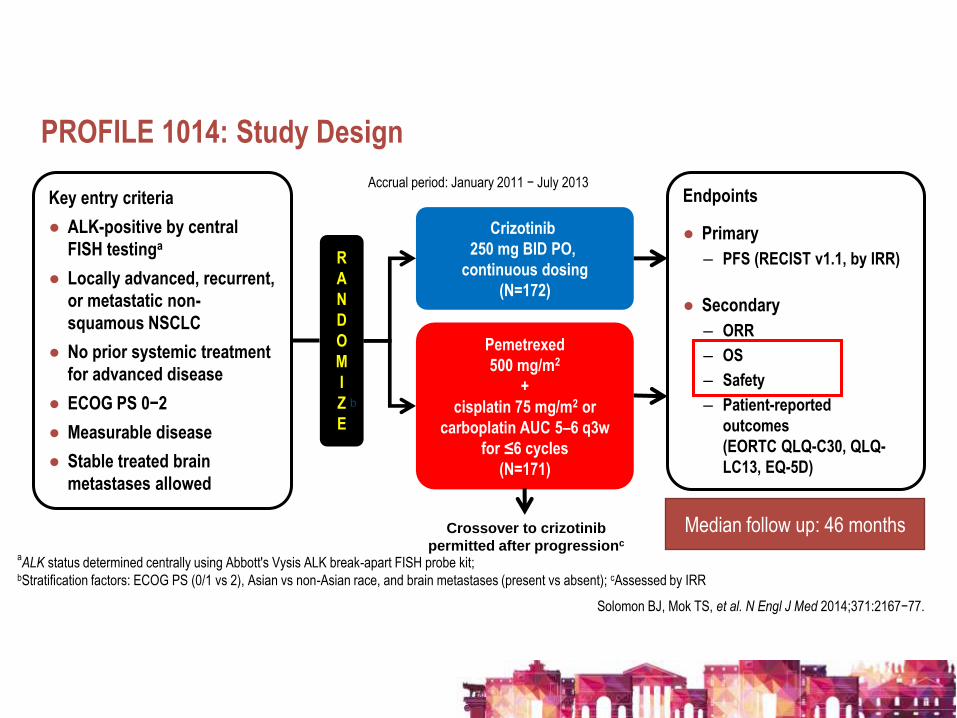
PROFILE 1014: Study Design
Solomon BJ, Mok TS, et al. N Engl J Med 2014;371:2167−77.
Key entry criteria
● ALK-positive by central
FISH testinga
● Locally advanced, recurrent,
or metastatic non-
squamous NSCLC
● No prior systemic treatment
for advanced disease
● ECOG PS 0−2
● Measurable disease
● Stable treated brain
metastases allowed
N=343
Crizotinib
250 mg BID PO,
continuous dosing
(N=172)
Pemetrexed
500 mg/m2
+
cisplatin 75 mg/m2 or
carboplatin AUC 5–6 q3w
for ≤6 cycles
(N=171)
Endpoints
● Primary
– PFS (RECIST v1.1, by IRR)
● Secondary
– ORR
– OS
– Safety
– Patient-reported
outcomes
(EORTC QLQ-C30, QLQ-
LC13, EQ-5D)
R
A
N
D
O
M
I
Z
E
aALK status determined centrally using Abbott's Vysis ALK break-apart FISH probe kit;
bStratification factors: ECOG PS (0/1 vs 2), Asian vs non-Asian race, and brain metastases (present vs absent); cAssessed by IRR
b
Accrual period: January 2011 − July 2013
Crossover to crizotinib
permitted after progressionc
Median follow up: 46 months

• PROFILE 1014 (Solomon et al NEJM 2014) was published after approximately 17 months of follow-up (data cutoff date 30 Nov 2013).
• Primary efficacy endpoint (superiority of crizotinib versus chemotherapy in terms of progression-free survival by IRR) was met: HR 0.454 (95% CI: 0.346, 0.596) and p-value <0.0001,
• Median PFS was 10.9 and 7.0 months for crizotinib and chemotherapy treatment, respectively
• ORR was significantly higher with crizotinib than with chemotherapy.
• 74% vs 45%, p<0.001
• With only 26% of all-cause deaths at data cutoff, median OS was not reached in either group at the time of first report.
• Here we report OS and safety of an additional 3 years of follow-up (LSLV 30 Nov 2016).
PROFILE 1014: Background
Solomon BJ, Mok TS, et al. N Engl J Med 2014;371:2167−77
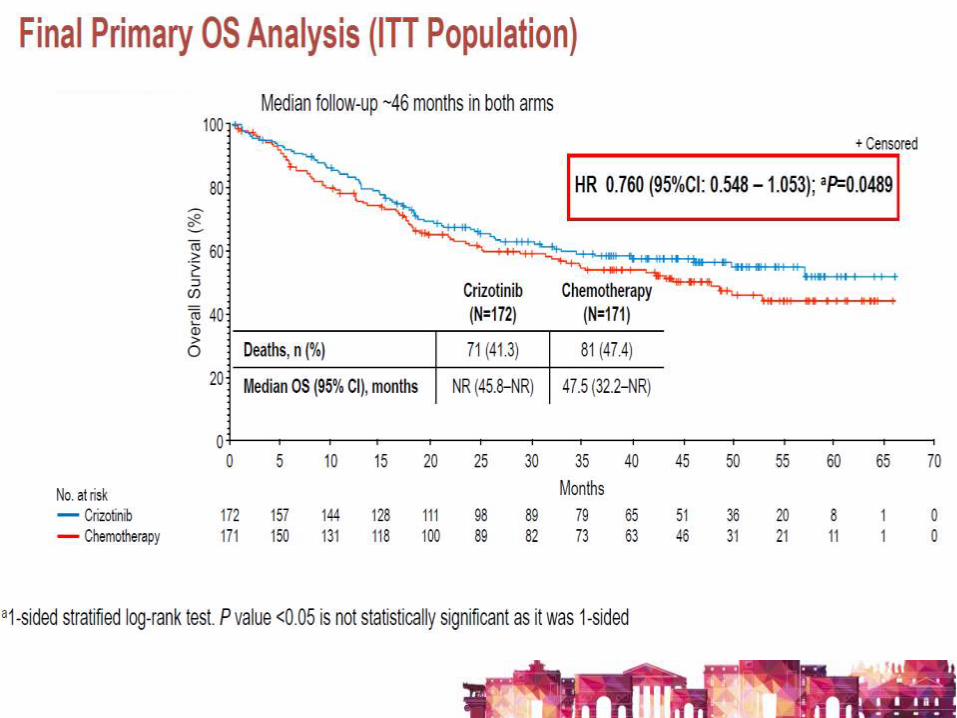


• With a median follow-up of approximately 46 months in both arms, this study has reported one of the highest 4 year survival rate to date for any study of TKIs in patients with Stage IV metastatic NSCLC.
• The difference in OS between crizotinib and chemotherapy arm (HR: 0.760 [95% CI: 0.548, 1.053]) did not reach statistical significance.
• After hypothetical adjustment for crossover (84.2% in chemotherapy arm and 19.2% in crizotinib arm), OS in the crizotinib arm could be significantly longer than in the chemotherapy arm (HR 0.346 [95% bootstrap CI: 0.081, 0.718] log-rank test approach).
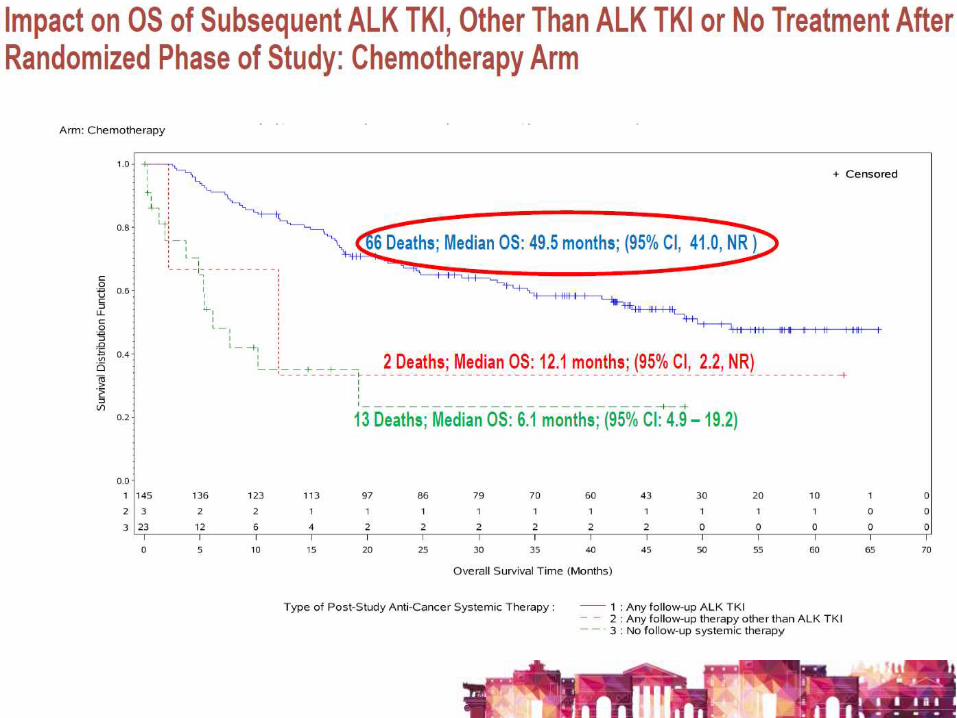
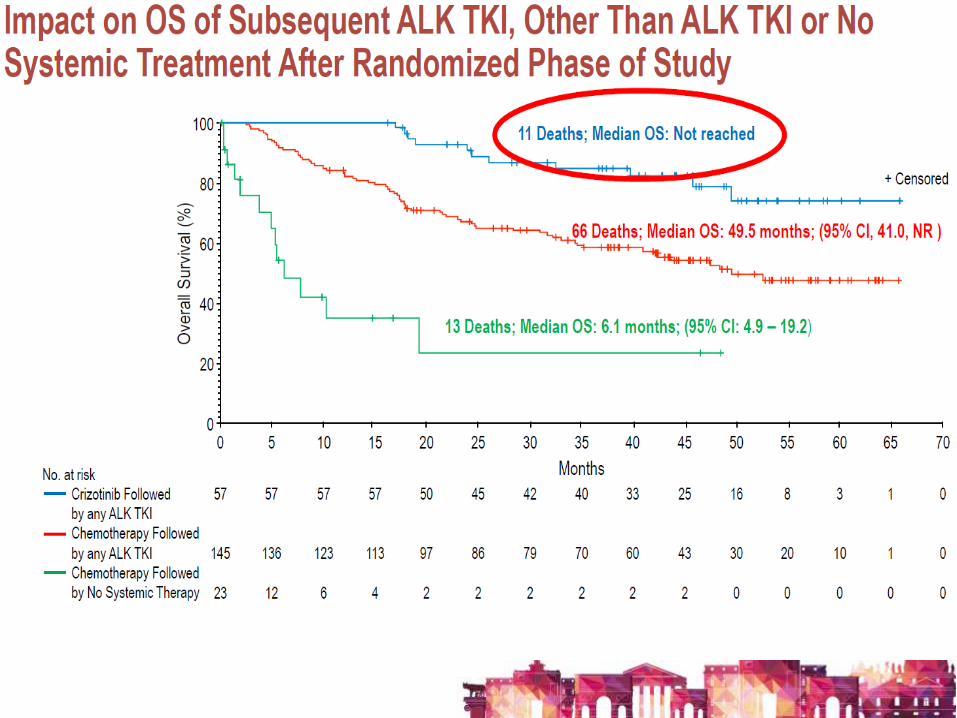
• Patients who received crizotinib followed by another ALK-TKI had the longest OS while patients randomized to chemotherapy followed by no ALK-TKI or other treatment had the worst OS.
• No unexpected toxicities were revealed with long-term crizotinib treatment.
Conclusions
ALECTINIB VS CRIZOTINIB IN TREATMENT-NAÏVE ALK+ NSCLC: CNS EFFICACY RESULTS FROM
THE ALEX STUDY
1Shirish Gadgeel, 2Solange Peters, 3Tony Mok, 4Alice T. Shaw, 5Dong-Wan Kim, 6Sai-Hong Ignatius Ou, 7Maurice Pérol, 8Rafal Dziadziuszko, 9Jin Seok Ahn, 10Rafael Rosell,
11Ali Zeaiter, 11Emmanuel Mitry, 11Eveline Nueesch, 11Bogdana Balas, 12D. Ross Camidge 1University of Michigan, Ann Arbor, MI, USA; 2Lausanne University Hospital, Lausanne, Switzerland; 3State Key Laboratory of South China, Chinese University
of Hong Kong, Shatin, New Territories, Hong Kong; 4Massachusetts General Hospital, Boston, MA, USA; 5Seoul National University Hospital, Seoul, South Korea; 6Chao Family Comprehensive Cancer Center, University of California, Irvine School of Medicine, Orange, CA, USA; 7Department of Medical Oncology,
Léon Bérard Cancer Center, Lyon, France; 8Department of Oncology and Radiotherapy, Medical University of Gdansk, Gdansk, Poland; 9Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea; 10Catalan Institute of Oncology, Barcelona, Spain;
11F. Hoffmann-La Roche Ltd, Basel, Switzerland; 12University of Colorado, Denver, CO, USA
52
52

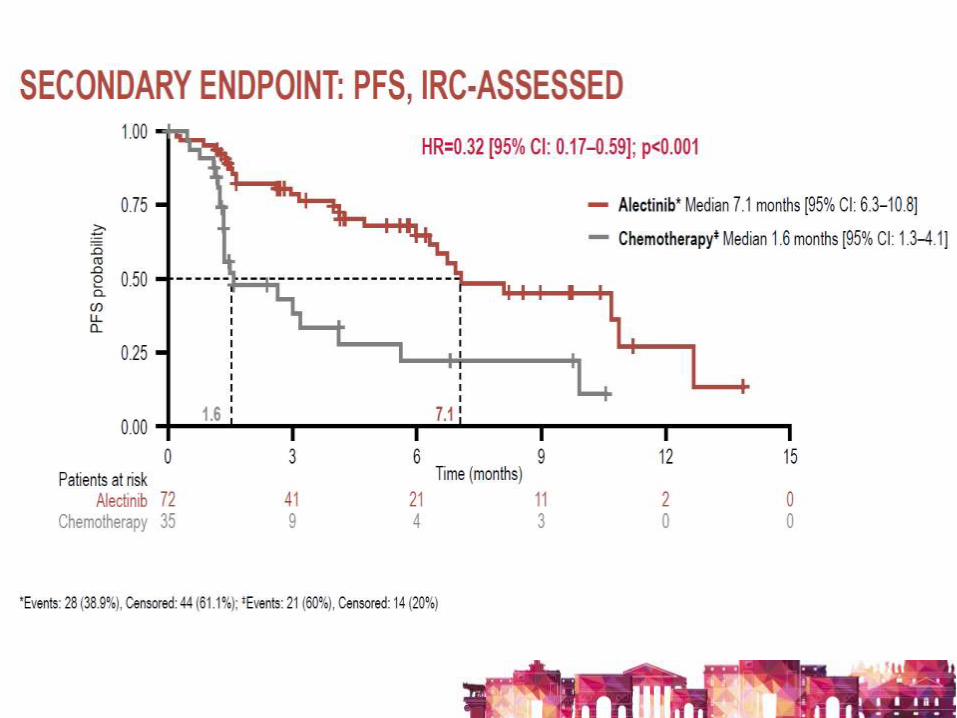
The primary endpoint of the study
was met:
HR 0.47 (95% CI 0.34–0.65) P<0.001
Median PFS with alectinib was not reached
compared with 11.1 months with crizotinib
53
*Isolated asymptomatic CNS progression, treatment until systemic or symptomatic CNS PD allowed BID = twice daily; DoR = duration of response; ECOG = Eastern Cooperative Oncology Group Performance Status; HR =hazard ratio; IHC = Immunohistochemistry; ORR = objective response rate; PD = disease progression; PFS = progression-free survival.
Alectinib 600mg BID (n=152)
Crizotinib 250mg BID (n=151)
R
1:1
• Stage IIIB/IV NSCLC
• ALK+ disease according to IHC test
• Treatment naïve
• ECOG PS 0–2
• Brain metastases permitted if asymptomatic
(n=303)
Until PD*,
toxicity, withdrawal
or death
Subsequent therapy
and survival
follow-up
Primary
endpoint
Investigator-assessed PFS in the ITT
population
Secondary
endpoints
Time to CNS progression, CNS ORR, CNS
DoR
(CNS endpoints were assessed by IRC)
Stratification
factors
ECOG PS (0/1 vs 2); Ethnicity (Asian vs non-
Asian); CNS metastases at baseline (presence
vs absence)
Peters, et al. NEJM 2017
All patients underwent restaging
chest/abdominal CT scans and brain imaging
every 8 weeks
ALEX STUDY DESIGN
• Median duration of follow-up: crizotinib arm 17.6 months (range: 0.3–27.0); alectinib arm 18.6 months (range: 0.5–29.0)
• Primary data cut-off: 9 February 2017
• CNS follow-up was conducted for all patients
• Lesions were documented by computed tomography scans, colour photography and MRI, brain scans, using RECIST v1.1



60
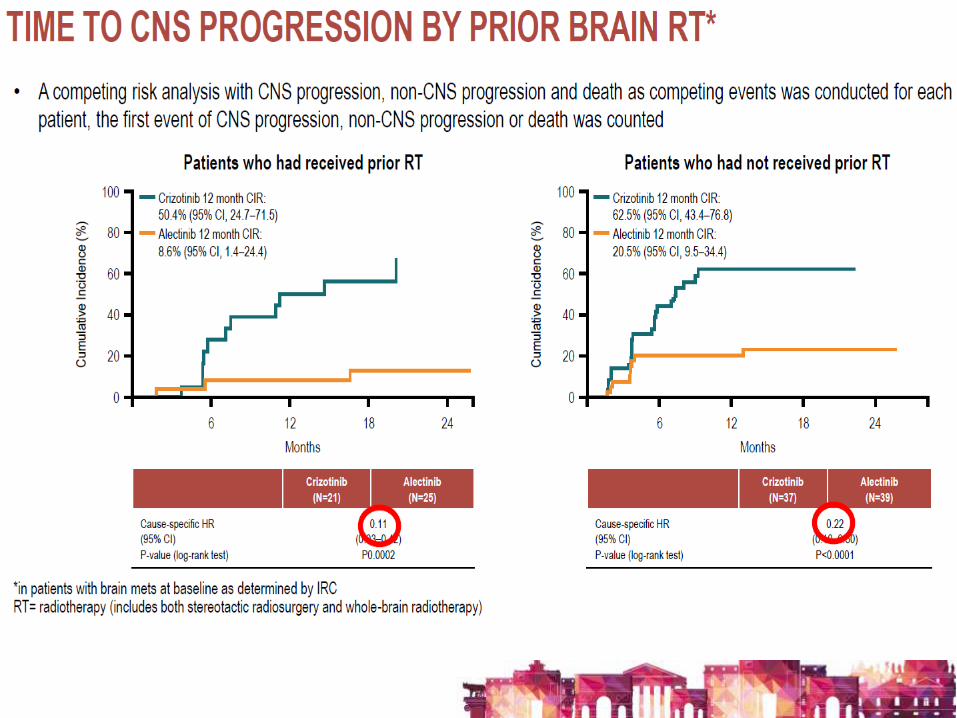
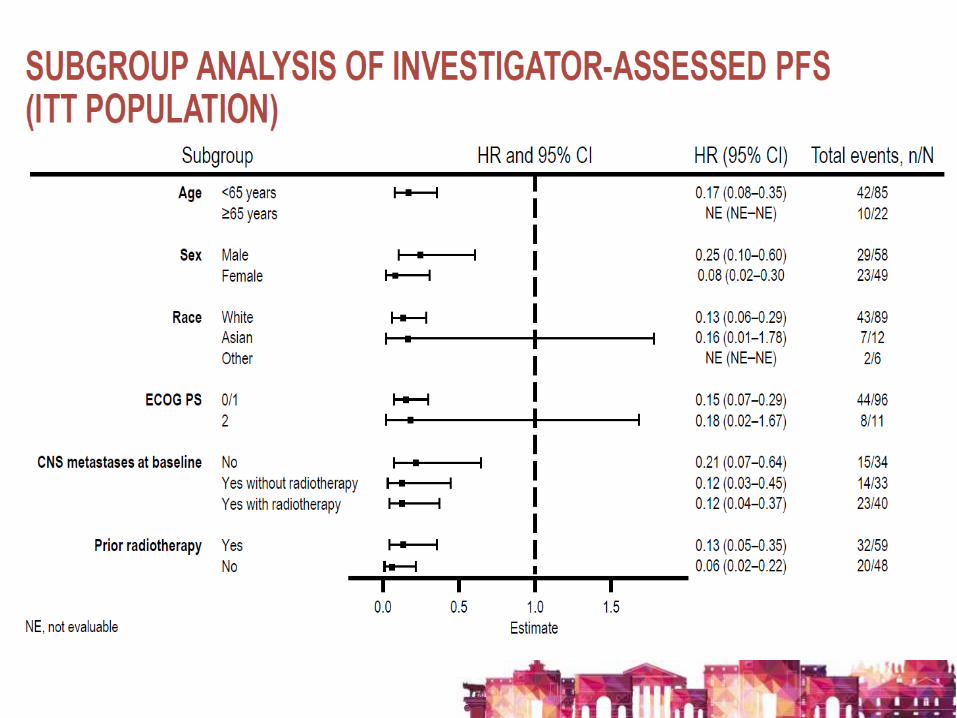
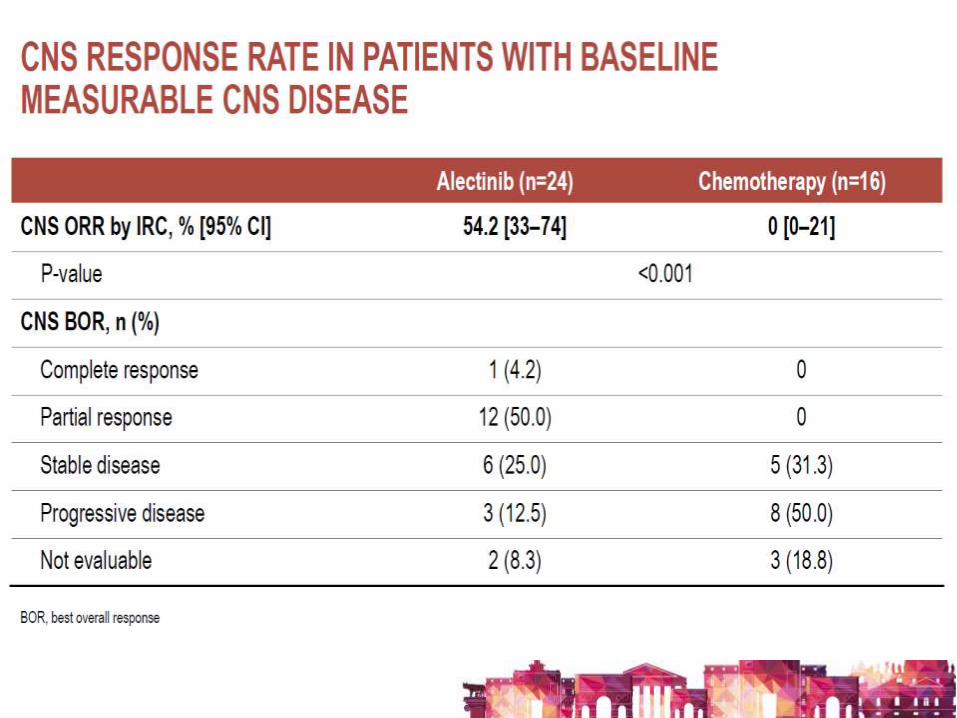
• Alectinib showed significantly superior CNS activity versus crizotinib in patients with CNS disease both with/without prior CNS RT across multiple CNS endpoints in previously untreated advanced ALK+ NSCLC
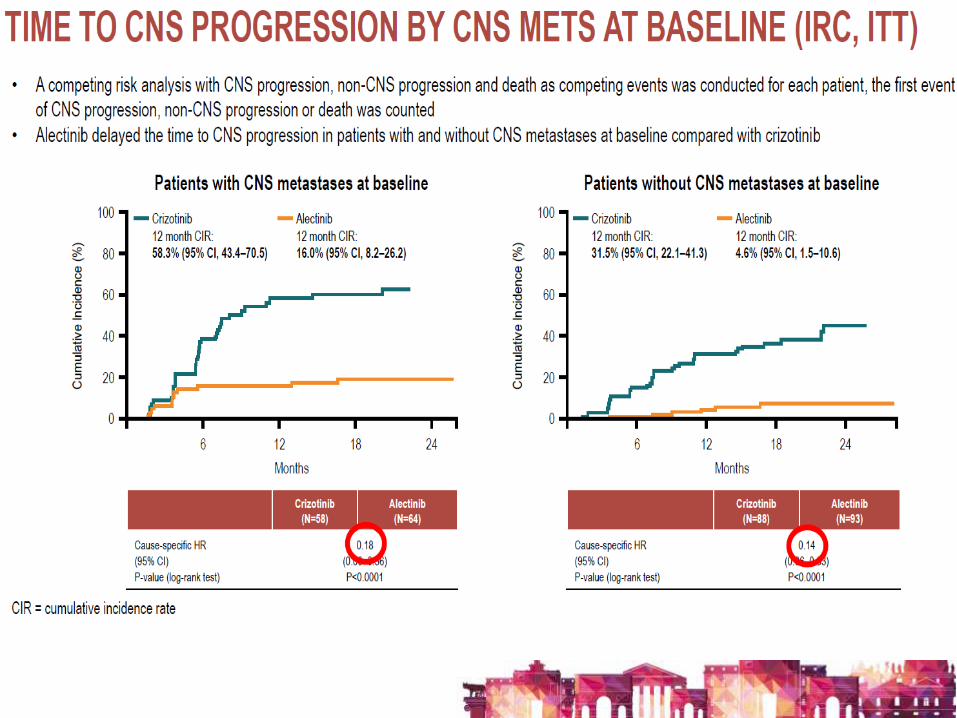
• alectinib significantly prolonged PFS in patients with and without CNS disease at baseline (HR 0.40, 95% CI 0.25–0.64; p<0.0001 and HR 0.51, 95% CI 0.33–0.80; p=0.0024, respectively) compared with crizotinib
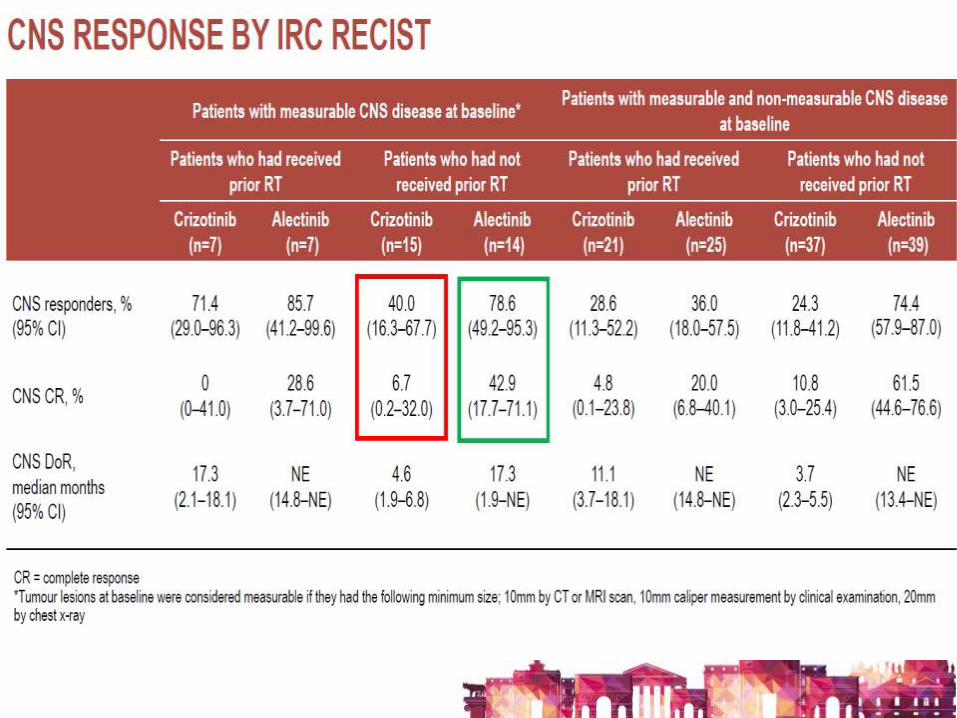
• alectinib significantly improved intracranial ORR compared with crizotinib, irrespective of RT (alectinib: 85.7% versus crizotinib: 71.4% and alectinib: 78.6% versus crizotinib: 40.0%)
• duration of CNS response with alectinib was longer in all patient subgroups than with crizotinib
• At 12 months, 31.3% of crizotinib vs 4.6% of alectinib patients had CNS metastases at the time of first progression suggesting alectinib is protective against the development of CNS progression
• Overall, these CNS results along with the systemic results consolidate alectinib as the new standard of care for patients with previously untreated, advanced ALK+ NSCLC
CONCLUSIONS
60 60


ACKNOWLEDGMENTS A special thanks to:
POMPERRA BELLINA CHEBORA ESMO 2017 (in alph. order: A.B., B.D.C., A.F.,T.F., L.P.,D.S., N.S., V.S. ET AL) Il Cremonese Jessica
grazie per l’attenzione!