Identifying and Preventing Adverse Drug Events … an average of 7.5lbs during freshman year ......
48
Jolene R. Bostwick, PharmD, BCPS, BCPP Clinical Associate Professor Associate Chair, Department of Clinical Pharmacy University of Michigan College of Pharmacy Clinical Pharmacist in Psychiatry University of Michigan Health System Identifying and Preventing Adverse Drug Events Associated with Psychotropic Medications
Transcript of Identifying and Preventing Adverse Drug Events … an average of 7.5lbs during freshman year ......

Jolene R. Bostwick, PharmD, BCPS, BCPPClinical Associate Professor Associate Chair, Department of Clinical PharmacyUniversity of Michigan College of PharmacyClinical Pharmacist in Psychiatry University of Michigan Health System
Identifying and Preventing Adverse Drug Events Associated with
Psychotropic Medications
Disclosure
I have NO actual or potential conflict of interest in relation to this educational activity or presentation.

Objectives
1. Identify key adverse drug events associated with psychotropic medications used to treat anxiety, depression, and ADHD
2. Describe potential strategies to mitigate adverse events associated with psychotropic medication use

BACKGROUND

ACHA Survey FindingsWithin the last 12 months, diagnosed or treated by a professional for
the following:
0
5
10
15
20
25
30
35
Attentiondeficit and
hyperactivitydisorder
Anxiety Depression Obsessivecompulsive
disorder
Panicattacks
FemaleMale
American College Health Association. American College Health Association-National College Health Assessment II: Reference Group Executive Summary Fall 2015. Hanover, MD: American College Health Association; 2016.Available at: http://www.acha-ncha.org/docs/NCHA-II%20FALL%202015%20REFERENCE%20GROUP%20EXECUTIVE%20SUMMARY.pdf

College Students Speak:a survey report on mental health (NAMI)
2724
12 116 6 5
105
1015202530
% of respondents
Adapted from: College Students Speak: a survey report on mental health. https://www.nami.org/getattachment/About-NAMI/Publications-Reports/Survey-Reports/College-Students-Speak_A-Survey-Report-on-Mental-Health-NAMI-2012.pdf
N=765

64%
36%
Are you no longer attending college because of a mental health related reason?"
YesNo
College Students Speak:a survey report on mental health (NAMI)

College Students Speak:a survey report on mental health (NAMI)
• When respondents were asked, – “what might have helped you stay in school?,”
• “managing side effects of medications.”– “what triggered your crisis?,”
• “medications stopped working.”
College Students Speak: a survey report on mental health. https://www.nami.org/getattachment/About-NAMI/Publications-Reports/Survey-Reports/College-Students-Speak_A-Survey-Report-on-Mental-Health-NAMI-2012.pdf
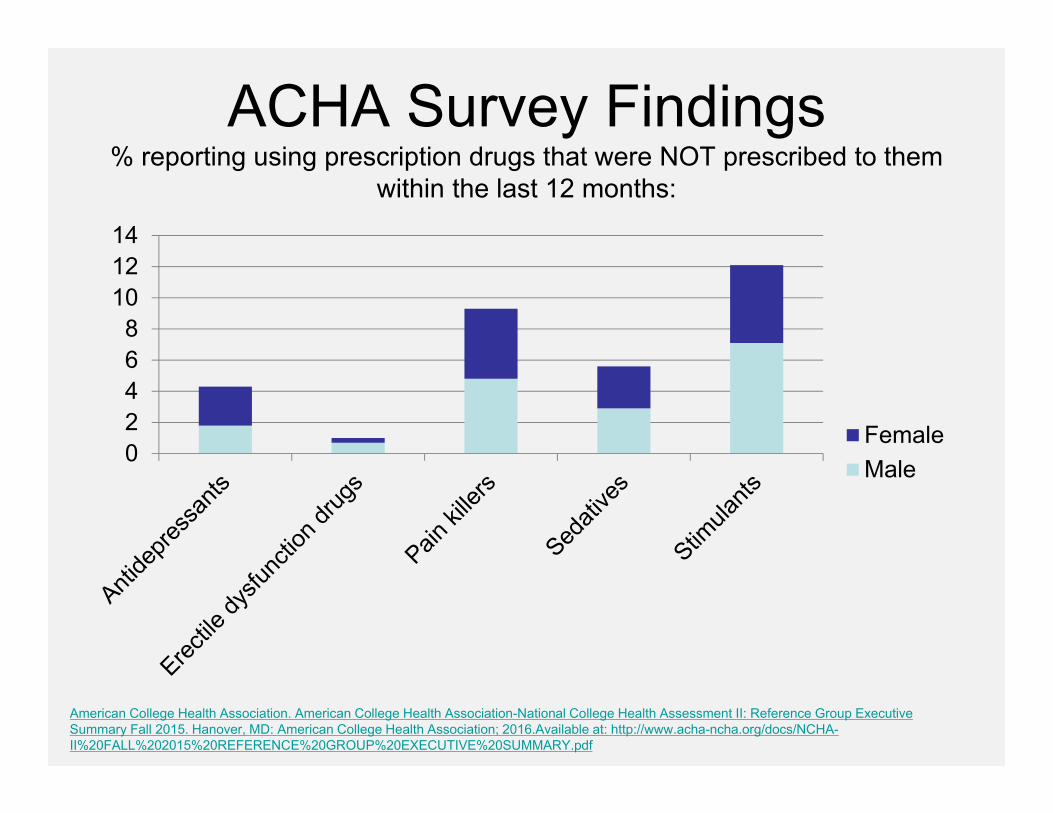
ACHA Survey Findings% reporting using prescription drugs that were NOT prescribed to them
within the last 12 months:
02468
101214
FemaleMale
American College Health Association. American College Health Association-National College Health Assessment II: Reference Group Executive Summary Fall 2015. Hanover, MD: American College Health Association; 2016.Available at: http://www.acha-ncha.org/docs/NCHA-II%20FALL%202015%20REFERENCE%20GROUP%20EXECUTIVE%20SUMMARY.pdf

Within the last 12 months, students reported the following top four factors affecting individual
academic performance
30.3
23.720.4
14.6
0
5
10
15
20
25
30
35
Stress Anxiety Sleep difficulties Depression
Percentage
American College Health Association. American College Health Association-National College Health Assessment II: Reference Group Executive Summary Fall 2015. Hanover, MD: American College Health Association; 2016.Available at: http://www.acha-ncha.org/docs/NCHA-II%20FALL%202015%20REFERENCE%20GROUP%20EXECUTIVE%20SUMMARY.pdf

Impact of Mental Illness on Performance and Cost
National Alliance on Mental Illness (NAMI) 2012
Poorer Academic Performance
• 64% of students with a mental health condition quit school for mental health related reasons
Increased Healthcare Costs
• Annual mental health expenditures in the United States are in the billions
• People with an anxiety disorder are more likely to utilize health care resources

Trends in Prescription Drug Use
Available at: http://www.cdc.gov/nchs/data/databriefs/db42.pdf. Accessed 4/25/16.

Trends in Prescription Drug Use
Available at: http://www.cdc.gov/nchs/data/databriefs/db42.pdf. Accessed 4/25/16.


Objectives
1. Identify key adverse drug events associated with psychotropic medications used to treat anxiety, depression, and ADHD
2. Describe potential strategies to mitigate adverse events associated with psychotropic medication use

Weight gain
Sexual dysfunction
Risk of seizures with bupropion + alcohol
Serotonin syndrome
Antidepressant discontinuation syndrome
Prescription drug misuse
Potential Adverse Events Associated with Psychotropic Medications

Patient CaseJoe is a 18 year old male with a history of severe and recurrent treatment resistant depression. He presents to the university clinic with suicidal ideation and is hospitalized for his current depressive episode. While hospitalized, his antidepressant regimen is changed.

Patient Case
Past medication trials include various antidepressants, one of which included mirtazapine and was associated with a significant amount of weight gain. Patient is no longer obese, as he has worked hard to reduce his weight. BMI=27.3.

Weight Gain
• Implications for college students– Body image and the “freshman 15”
• Meta-analysis of 5549 students found that 60.9% gained an average of 7.5lbs during freshman year
• Students continue to gain weight sophomore year
Vadeboncoeur C, et al. BMC Obes. 2015;2:22.Lloyd-Richardson EE, et al. Prev Med. 2009;48(3):256–261.


Antidepressants and Weight Gain
• Obesity is up to 3 times more common in psychiatric patients
• Medication induced or notable improvement in depressive symptoms?
• Short-term use of SSRI antidepressants (2-3 months) typically associated with little or no weight change
• Risk with mirtazapine ≥ paroxetine >>> fluoxetine > bupropion
Serretti A, et al. J Clin Psychiatry 2010;71(10):1259-1272.

Antidepressants and Weight Gain
Loss Modest Gain Gain Neutral
BupropionFluoxetine
CitalopramDuloxetineEscitalopramSertralineTrazodoneVenlafaxine
AmitriptylineImipramineMirtazapineParoxetinePhenelzine
FluvoxamineNefazodoneNortriptyline?
Schwartz TL, et al. Current Psychiatry 2007;6(5).

Patient Case
The patient inquires whether an antipsychotic would be a good option, as he has recently seen advertisements touting the benefits. How should you respond?A. NoB. YesC. Maybe - Let’s discuss the risks and
benefits…

Antipsychotics and Weight GainAntipsychotic Weight gain Diabetes DyslipidemiaAripiprazole - - -Asenapine -/+ - -Clozapine ++ ++ ++Iloperidone + - -Lurasidone - - -Olanzapine ++ ++ ++Paliperidone -/+ - -Quetiapine + + +Risperidone + + -Ziprasidone - - -
(-)low;(+)moderate; (++)high
Adapted from: PL Detail-Document, Comparison of Atypical Antipsychotics. Pharmacist’s Letter/Prescriber’s Letter. July 2015.

Recommended Metabolic Monitoring Parameters for Second Generation Antipsychotics
Parameters Baseline 4 & 8 weeks 12 weeks Quarterly Annually
Personal/Family History
x x
Weight (BMI) x x x xWaist Circumference
x x
Blood Pressure
x x x
Fasting Plasma Glucose or HbA1c
x x x
Fasting Lipid Panel
x x Every 5 years if wnl
Adapted from Diabetes Care 2004;27(2)596‐601
Patient Case
Assuming each of the following would be appropriate from a symptom management as well as past medication trial perspective, which of the of the following would be the most appropriate agent to consider next in Joe?
A. OlanzapineB. Paroxetine + aripiprazoleC. Fluoxetine and/or bupropionD. Mirtazapine

Mitigation Strategies• Inform patients that their appetite may be increased• Use weight neutral agents when possible• Monitor changes in weight at follow-up visits and
document these changes• Encourage diet and exercise – engage patient in
self-management• Discuss risks and benefits of treatment• Consider cognitive behavioral therapy • Place for weight-loss agents??
Antidepressants and Antipsychotics: Minimizing Weight Gain
Schwartz TL, et al. Current Psychiatry 2007;6(5).Bickerdike HJ et al. Diabetes Obes Metab 1999;1:207-14.

Weight gain
Sexual dysfunction
Risk of seizures with bupropion + alcohol
Serotonin syndrome
Antidepressant discontinuation syndrome
Prescription drug misuse
Potential Adverse Events Associated with Psychotropic Medications

Patient Case
Briana is a 23 year old female on multiple medications, including escitalopram 20 mg daily to manage her anxiety. It is working well to target her anxiety symptoms, however, she is concerned about her lack of interest in sexual activity. What are some potential management strategies?

Antidepressants and Sexual Dysfunction: Risk Factors
• Male• Increasing age• Lower academic achievement• Employment status other than full time• Poor physical health• Polypharmacy• Poor interpersonal relationships• CYP2D6 poor metabolizer status + treatment with
paroxetine• Others…
Baldwin DS, et al. CNS Drugs 2015;29:905-913.

Sexual Dysfunction• Common reason for non-adherence• May be due to:
– Side effect of psychotropic agent (impacts relapse rates by limiting dose/duration of treatment)
– Primary sexual disorder– Symptom of illness (medical or psychiatric)– Substance abuse– Psychosocial stressors– Other causes
Clayton AH, et al. J Sex Med 2009;6:1200-11.

Types of Sexual Dysfunction• Altered sexual desire/reduced libido
• Orgasmic and ejaculatory dysfunction– Anorgasmia– Hyperorgasmia– Painful orgasm and inhibited ejaculation
• Erectile problems– Erectile dysfunction– Priapism– Painful erection
• Reduced sexual satisfaction, issues with sexual arousal, lubrication, vaginismus, and dyspareunia
Taylor MJ et al. Cochrane Database of Systematic Reviews 2013, Issue 5. Art. No.: CD003382. DOI: 10.1002/14651858.CD003382.pub3.Baldwin DS, Foong T. Br J Psychiatry 2013;202:396-7

Risk of Sexual Dysfunction by Antidepressant
Risk Level Antidepressants Comments
Highest RiskCitalopram, fluoxetine,paroxetine, sertraline, venlafaxine
Rates approximately 65-80% of treated patients
High RiskFluvoxamine, escitalopram, duloxetine, phenelzine,imipramine
Significantly higher rates compared to placebo, but significantly less than the “highest risk” group, rates ranging from roughly 25-44%
Lowest Risk Bupropion, mirtazapine,nefazodone
Rates are lower or comparable to placebo (14.2%)
Serretti et al. J Clin Psychopharmacol 2009;29: 259-266.

Minimizing Sexual Dysfunction
• Watchful waiting• Modifying sexual technique• Individual and couple psychotherapy• Altering antidepressant use
– Reducing dose– Switching agents– Delaying use until after sexual activity
• Drug holidayTaylor MJ et al. Cochrane Database of Systematic Reviews 2013, Issue 5. Art. No.: CD003382. DOI: 10.1002/14651858.CD003382.pub3.

Minimizing Sexual Dysfunction
• Become skilled and comfortable discussing topic• Patient education when treatment initiated• Encourage reporting – inquire about concerns• Take patient concerns seriously, which may
include problems with desire, excitement, or orgasm
• Add an agent to manage symptoms
Clayton AH, et al. J Sex Med 2009;6:1200-11. Prabhakar D, et al. Current Psychiatry 2010;9(12):30-4.Nurnberg AG, et al. JAMA. 2008;300(4):395-404.Baldwin DS, Foong T. Br J Psychiatry. 2013;202:396-7

Pharmacologic Management Strategies• In men
– Sildenafil (3 studies, 255 participants) and tadalafil (1 study, 54 participants) better than placebo; treatment effect similar to those reported for erectile dysfunction due to other causes
– Higher dose bupropion (150 mg twice daily) beneficial (1 study, 234 participants)
• In women– Bupropion 150 mg twice daily better than
placebo (3 studies, 482 participants)– Additional published studies needed with
sildenafilTaylor MJ et al. Cochrane Database of Systematic Reviews 2013, Issue 5. Art. No.: CD003382. DOI: 10.1002/14651858.CD003382.pub3.

Patient Case
As previously described, what is likely the best strategy to try first to minimize sexual dysfunction that may be induced by escitalopram in Briana?A. Discontinue escitalopram and initiate
bupropionB. Consider a dose reductionC. Take a wait and see approachD. Add on sildenafil
Weight gain
Sexual dysfunction
Risk of seizures with bupropion + alcohol
Serotonin syndrome
Antidepressant discontinuation syndrome
Prescription drug misuse
Potential Adverse Events Associated with Psychotropic Medications
Patient CaseMessage from prescriber:“I treat a fair number of students and this question has come up several times for me. Regarding the use of bupropion, I wonder about this with students who drink alcohol. Some of them seem to binge drink on the weekends. Should I tell them not to take the bupropion if they are planning to drink or would it be better not to prescribe it for them at all? I am concerned about the fact that bupropion and alcohol use together could increase their risk for seizures.”

RecommendRecommend
Titrate up slowly
When possible, avoid high total daily doses (<400mg) and do NOT exceed recommended
maximum daily dose
Unless taking the XL formulation, avoid doses
>200mg at one time
Use lower doses if using as part of combination antidepressant
regimen
Avoid use in specific patients with predisposing
risk factors:
Avoid use in specific patients with predisposing
risk factors:
History or current excessive alcohol use
Abrupt alcohol cessation
Taking other medications that lower seizure threshold (e.g.
amphetamines)
History of head trauma
Bulimia nervosa
Bupropion and Seizure Risk
Tai M, et al. Current Psychiatry 2015;14(8):29-31, 43-46; Bupropion product labeling.

Patient CaseWhat would you recommend to this prescriber or do in this case? Tell them:A. The warning for risk of seizures is overstated,
you can prescribe without concernsB. Avoid bupropion only if the patient has a history
of an eating disorderC. Do not use bupropion in a patient at risk for binge
drinkingD. Evaluate on an individual basis; discuss risks
with patient; may avoid if high risk for binge drinking

Pain Relievers – Acetaminophen
• Commonly used OTC pain medication in the United States– Found in several products
• Knowledge gaps are common in the general population – Risk of adverse events is high
• Accidental and intentional overdose• Risk of liver damage with alcohol abuse
Concerns among college students

Pain Relievers – NSAIDs• Found in many OTC and Rx products lithium levels and renal lithium clearance– Even when one dose is used or when used PRN,
NSAIDs can significantly alter lithium levels
• Recommend:
BMJ 1991;302:1267-9Clin Pharmacokinet. 1995 Sep;29(3):172-91.J Clin Psychiatry 1987 Apr;48(4):161-3.
If possible, avoid newly starting NSAID therapy, even
PRN use
If possible, avoid newly starting NSAID therapy, even
PRN use
For patients that are receiving concurrent NSAID and lithium therapy, monitor
lithium levels every 4-5 days. Dose of lithium may need to be reduced if NSAID use is
chronic/long term
For patients that are receiving concurrent NSAID and lithium therapy, monitor
lithium levels every 4-5 days. Dose of lithium may need to be reduced if NSAID use is
chronic/long term
Educate patients on NSAID containing OTC products and
signs/symptoms of lithium toxicity
Educate patients on NSAID containing OTC products and
signs/symptoms of lithium toxicity

Weight gain
Sexual dysfunction
Risk of seizures with bupropion + alcohol
Serotonin syndrome
Antidepressant discontinuation syndrome
Prescription drug misuse
Potential Adverse Events Associated with Psychotropic Medications
Patient CaseEmily is a 20 year old female university studentpresenting to the university health clinic todaywith complaints of a migraine. She reportsthrobbing pain, sensitivity to light, nausea,vomiting, and lightheadedness. Her migraineshave been occurring about twice per month,each lasting 1 day. Her past medical historyincludes depression, and she is currentlytreated with sertraline 100 mg daily. She inquiresabout being prescribed a triptan, which has beenhelpful in the past, prior to her treatment with sertraline.

Triptans and Serotonin Syndrome
• FDA alert in 2006 warned about the possibility for serotonin syndrome when triptans are used concomitantly with SSRIs or SNRIs
• American Headache Society 2010: Position paper citing conflicting and insufficient data to support the FDA warning
Sclar DA, et al. Headache 2012;52:198-203.

Medications associated with Serotonin Syndrome
Boyer EW, Shannon M. N Engl J Med. 2005;352:1111-20.
Antidepressants
Valproic acid
Analgesics: meperidine, fentanyl, tramadol, pentazocine
Antiemetics: ondansetron, granisetron, metoclopramide
Antibiotics: linezolid, ritonavir
Dextromethorphan
Drugs of Abuse: MDMA/ecstasy, LSD
Dietary/Herbal Supplements: tryptophan, St. John’s Wort, Panax ginseng, Garcinia?
Lithium

MDMA
• Structurally related to both amphetamine and the hallucinogen mescaline
• Produces large increases in serotonin release mood elevation, feeling a sense of closeness to others, greater sociability, sharpened sensory perception, and extraversion
• Adverse effects related to excessive CNS and cardiovascular stimulation
Pharmacist 2006;25(9):684-9.