identifikasi tramadol

of 9
-
Upload
nazura-alias -
Category
Documents
-
view
236 -
download
0
Transcript of identifikasi tramadol
-
8/13/2019 identifikasi tramadol
1/9
Journal of An alytical Toxicology,Vol. 21, Novem ber/December1997
I d e n t i f i c a t i o n o f T r a m a d o l a n d i t s M e t a b o l i t e s i n B l o o d f r o mD r u g R e l a t e d D e a t h s a n d D r u g I m p a i r e d D r i v e r sKabrena E. Go er inger , Bar ry K. Logan, and Ga ry D . Chr is t ianWash ington Sta te Tox ico logy Depar tment o f Labora to ry Me d ic ine Un ivers it y o f W ash ing ton 220 3 A i rpor t Way SouthPark 90 /5 Su i te 360 Seat t le W ash ing ton 98134
bstractTramado l is a central ly acting, b inary analgesic ha t is neither anop ia te -der ived no r a non stero ida l an t i -in f lamm atory d rug and tha twas approved fo r use n the Un i ted S ta tes n 1995. I t is used ocontro l modera te pa in n chron ic pa in se t tings such asosteoa rthr i t is and postop erative cases. Use d n thera py as aracemic m ix tu re , the (+) -enant iomer w eak ly b inds to the p . -op io ldreceptor , and bo th enant iomers inh ib i t sero ton in andnorep inephr ine reuptake. T ramado l s m a jor ac t ive m etabo l ite ,O-desm ethyltramad ol (ODT ), sh ows higher aff in ity f or the ~t-op io id receptor and has tw ice the ana lges ic po tency o f the parentdrug . The synerg ism o f these e f fec ts contr ibu tes to t ramado i sana lgesic p roper ties wi th the (+) -enantiomer exh ib i t ing 10-foldhigher analgesic activ ity than th e (-)-enantiom er. Althoughtramado l w as in i t ia l ly thought to exh ib i t low abuse po ten t ia l,Or tho-McN ei l , the drug s manufac turer, recent ly repor ted a la rgenumb er o f adverse events a t t ribu ted to t ramado l inc lud ing abuseby opioid-de pend ent patients, a l lergic reactions, and seizures. Theh igh num ber o f adverse reac t ions has prompted the co mpan y toupdate the prescr ib ing in fo rmat ion fo r the drug . An ana ly t ica lmethod us ing gas chromatography-mass spectrometry (GC-M S)without der iva t iza t ion fo r the de terminat ion o f t ramado l and i tsme taboli tes is reported. An n-butyl ch lor ide extraction is fo l lowedby G C-MS a na lys is us ing a 5 pheny lmethy ls i licone co lum n(30 m x 0 .32-gm i .d .) . Ana lys is o f 12 b lood samples f romtrama dol-related deaths and four nonfata l intoxications involv ingt ramado l revea led concentra t ions rang ing f rom 0 .03 to 22 .59 m g/Lfor t ramado l , f rom 0 .02 to 1 .84 mg/L fo r OD T, and f rom 0 .01 to2 .08 m g/L fo r N-desmethy l t ramado l . Three deaths were c lear lya t t r ibu tab le to acu te morph ine tox ic i ty , one was a doxep inoverdose, and six were mu lt ip le drug overdoses. The role oft ramado l in each death is exp lo red .
I n t r o d u d i o nTramadol (Ultram Ortho-McN eil) is a centra lly acting, bi-nary analgesic that has be en available for use in Europe for sev-
Address or correspondence:Capt. KabrenaGoeringer, P.O. Box 13, USAFA, Colorad oSprings,CO 80840-0013.
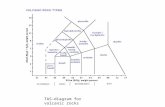
eral years, a l though i t was only approved for use in th e U nitedStates in 1995. I t is neither an opiate-der ived nor a non-s tero ida l an t i - inf lamm atory drug (1) . I t undergoe s N- an dO - d e m e t h y l a t i o n to N - d e s m e t h y l t r a m a d o l ( N D T ) a n dO-desmethyltramadol (ODT) (Figure 1) and is a racem ic drugbelieved to possess two modes of action. Both enantiomersinhib i t the reuptake of se ro tonin and norepinephr ine ; the(+)-enantiomer is mo re effective a t inhibiting the reuptake o fserotonin, whereas the ( - ) -enan tiom er more strongly inhibitsnorepinephrine reuptake (2 ) . The synergism of these effectscontr ibutes to tram ado rs analgesic properties; the (+)-enan-t iome r has b een show n to exhib i t 10- fo ld h ighe r ana lges icactivity than the ( - )-enantiomer.Tramadol was or iginally introduced in G ermany in the la te1970s by G ri~nenthal (Stolberg, G ermany) as a weak opioidwith an a typical c l inical profile (3) . The manufacturer c la imedthat the typical opioid side effects such as respira tory depres-sion or effects on smooth muscles could be lessened or avoidedaltogeth er if doses providing analgesic eff icacysimilar to tha tof meperidine w ere used. Because of the (+)-enantiomer s re l-atively low affinity for the I~-opioid eceptor, tramadol was alsooriginally thoug ht to have a low potentia l for abuse, tolerance,and dependence in treatmen t up to six months in length (4) . Infact , despite increasing c linical use , tramadol did no t becomepopular as a dru g of abuse unti l the ear ly 1990s, and a studypublished in 1993 found no signif icant abuse reported w itht ramadol (5) . In s tudies of phys ica l depend ence-produc ingcapacity, tramadol fa iled to suppress o r precipita te withdrawalin m or ph ine - de pe nde n t m ic e , r a t s , a nd r he sus m onke ys(3,6-8) . H owever , one study found that tramadol producedmild withdrawal signs when given to morphine-dependent,nonwithdrawn rhesus monkeys (8) . Other work showed thattramadol produced a mild degree of physical dependence af terrepeated administra tion to ra ts , mice, and rhesus monkeys asdemonstra ted by the exhibit ion of withdrawal signs followingopioid antagonist administra tion and abrupt drug termina-tion (3,7-9) . This may be because tramadol s active metabolite ,ODT, has up to 200 t imes high er aff inity for the I~-opioid re-ceptor and tw ice the analgesic potency of the p arent d rug.Studies that suggest tramadol may have abuse potentia l
Reproduction photocopying) f e ditorialcontentof this ournal s prohibitedwithoutpublisher s ermission. 5 2 9
-
8/13/2019 identifikasi tramadol
2/9
J o u rn a l o f A n a l y ti c a l T o x i c o l o g y , V o l . 2 1 , N o v e m b e r / D e c e m b e r 1 9 9 7
N HaCH3 CH3
HO . . . , ~ O C H 3 H O . . . , , ~ HH-I ,, ' H ,, '
el l3 H C H a C H aN-DesmethyltramadolNDT) O-DesmethyltramadolODT)
t
0 ~ 0 . . , , ~ O C H 3CH3N-Desmethyltramadol arbamateartifact
F i g u r e 1 . S tr u c tu r e s o f tr a m a d o l N D T a n d O D T .
I9 1
8
7 t
6
5 t
4
3
2
1 1
3 J 69 ." 9 9 . ~ i -~. . . . . . . . . . . . . . . . . . . . . . . i . . . .8,0 10.0 12.0 14.0
Time (rain)
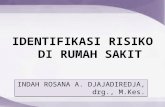
F i g u r e 2. G a s c h r o m a t o g r a p h ic s e p a r a ti o n o f tr a m a d o l N D T a n d O D T f ro m t h e i n te r n a l s t a n -d a r d s p a p a v e r i n e a n d d ip h e n y l a m i n e . P e a k d e n t if ic a t io n : 1 d i p h e n y l a m i n e ; 2 t ra m a d o l ;3 N - d e s m e t h y lt ra m a d o l ; 4 O - d e s m e t h y lt ra m a d o l ; 5 d i is o o c t y lp h t h a l a t e ; a n d 6 p a p a v e r in e .
have been performed. In three self-adminis tra-t ion s tud ies in l e fe tamine- t ra ined and d rug-na ive rhesu s monk eys , t ramad o l main ta ineddrug tak ing (8 ). Pres ton e t a l . (10 ) concludedtha t a l though the d rug does appear to havesome pote ntial for abuse, a m uc h larger dose oftramadol tha n m orph ine is required to produc esubjective effects n patients in a study of the ef-fects of tramadol in postaddicts to assist in itsabuse po tential assessment.Ortho-McNeil s recent le t ter (11) to heal thcare professionals across the U .S. provided newinfo rm at ion regard ing the po ten t ia l fo r abuse ,seizures, and anaphaylactoid reactions associ-a t e d w i t h t h e u s e o f t r a m a d o l . T h e l a r g enumber o f adverse even ts a t t r ibu ted to t ra -m a d o l h a s p ro m p t e d t h e c o m p a n y to u p d a t ethe pre scribing inform ation for Ultram. Specif-ica l ly , the new product in ser t spec i f ies tha tUltram is con traindicated in pat ients wit h pastor present his tories of addict ion to or depen-d e n c e o n o p i o i d s , t h o s e w i t h a l l e r g i e s t oUl t r a m o r o t h e r o p i o i d s , a n d t h o s e t a k i n gc o n c o m i t a n t m e d i c a t i o n s t h a t m a y r e d u c ethe se izure thresho ld, such as t r icyclic ant ide-p r e s s a n t s , o t h e r t r i c y c li c c o m p o u n d s , a n dselective sero toni n reuptake inhibitors (SSRIs).It is impo rtan t to consider t ram adol s abil i tyto inhib i t serotonin reuptake wh en prescribingthe d rug for pat ients already taking dru gs withsero ton erg ic activity. It is possible that subjectss tab il ized on SSRIs o r o ther an t idepressan tscould be susceptible to developing serotonintoxici ty up on s tart ing tramadol therapy. In ad-dition, it is highly probable tha t ODT, ram adol sact ive metaboli te, p lays a role in toxici ty inw h i c h h i g h c o n c e n t r a t i o n s o f t h e m e t a b o -l i te a r e p r e s e n t b e c a u s e o f e i t h e r s e ro t o n i ns y n d ro m e o r t r a m a d o l t o x i c i t y . ODT h a s ahig her affinity for the I~-opioid eceptor a nd hastwice the analgesic potency of t ramadol .Isoenzyme m etabo li sm i s a l so impo r tan t toconsider in tramadol-related fatalities. CYP2D6,the Cy tochrom e P-450 i so fo rm fo r wh ich m anyS S R I s a n d t r i c y c l i c a n t i d e p r e s s a n t s a r es u b s t r a t e s ( 1 2 - 14 ) , h a s b e e n s h o w n t o b eresponsible for the m etabo lism of t rama dol toODT. Conseq uently, com petitive inh ibition of2 D 6 r e s u l t i n g i n e n z y m e s a t u r a t i o n a n dsubs equ ent leng thened half-li fe and an increasei n p e a k p l a s m a c o n c e n t r a t i o n m a y o c c u r i ncases in w hich one o r m ore substrates for th isi s o e n z y m e a re p r e s e n t w i t h t r a m a d o l . S u c hintera ct ions can lead to toxic s ide effects thatmay play an imp ortan t role in t ramadol-relatedfatali t ies . The re are no known inducers of 2D6.I s o l a t i o n m e t h o d s fo r t r a m a d o l a n d i tsm e t a b o l i t e s f ro m b lo o d a n d u r i n e u s i n g g a s
5 3
-
8/13/2019 identifikasi tramadol
3/9
J our na l o f A na l y ti c a l T ox i c o l ogy , Vo l . 21 , N ov em ber /D ec ember 1997
c h r om a tog r a phy - m a ss spe c t r om e t r y ( G C - M S ) , G C w i thni t rogen-se lec t ive de tec t ion , and h igh-pe r forman ce l iquidchromatography (HPLC) were previously reported (15--19).How ever , a l l of the GC m ethod s involvedderivatization of a l l thre e compoun ds be-fore analysis. W e report ana lytical metho dsusin g GC-M S with out der ivatization fort h e d e t e r m i n a t i o n o f t r a m a d o l a n d i t smetaboli tes. This method was applied tocases of suspected drug-related deaths anddrug-impaired dr iving.
Materials and Methods
Tramadol, NDT, and ODT w ere gif ts f romR.W. Joh nsto n (Raritan, NJ) . One of theinternal standards, papaverine hy drochlo-r ide in GC -grade methanol, was obtainedf r om S igm a ( S t . L ou i s , M O ) . A l l o the rreagents were analytical grade or bettera nd w e r e ob t a ine d f r om F i she r ( S a n t aClara , CA).GC-M S was performed o n a 5890/5970GC-MS fro m Hew lett Packard (Palo Alto,CA) tha t w as operated in full-scan mod e.Chromatographic separation was achievedusing a 5 phenylmethylsil icone colum n(30 m x 0.32-1~m i.d., Econ ocap, A lltech,Deer fie ld , IL ) . Ana lyses were pe r formedwith the tempera ture programmed f rom80 to 295~ a t 15~ and he ld a t thef inal tem pera ture for 8 ra in .B l o o d s a m p l e s c o l l e c t e d a t a u t o p s yduring the investigation of 12 unrela tedfatalities we re each placed in separate 10-mL vials containing sodium f luoride andpo ta s s ium oxa l a t e ( V a c u ta ine r, B e c tonDickinson, Franklin Lakes, N ) . The sam-ples we re refr igerated un ti l analysis wasperformed. Most samp les were per ipheralblood, some w ere centra l blood, and som ewere n ot labeled as to collection si te .L i q u i d - l i q u i d e x t r a c t i o n s w e r e p e r -formed us ing a procedure based on tha tde sc r ibe d by F oe r s t e r a nd c o - w or ke r s(20,21) that was mo dified or general use inour laboratory for screening basic drugs.Blood (1 rnL), internal standard s (dipheny -larnine and pap averine, 100 I.tL of 1- and0.5-mg/L solutions, respectively) , and pH 9s a t u r a t e d p o t a s s i u m b o r a t e b u f f e r(1 mL) were mixed and ext rac ted wi thn-bu tyl chlor ide (3 mL) af ter centr ifugingat 2000 rpm for 5 ra in. The organic f ractionwas back extracted into 3M hydrochlor icacid (200 ILL), wh ich was the n basif ied
with con centra ted a m mo nium hydroxide and re-extracted intoc h lo r o f o r m ( 100 I ~L ) . T he c h lo r o f o r m f r a c t ion w a s t he nanalyzed by GC-MS.
32
28
24
2
16
12
8
4
36
32
28
24
2
16
12
8
4
58
... I7 7 1 7 1 3 5 2 6 3
. . . . . . . . _ . I ii . . . L I . . . . i . . . . . . . i . . ' . 9 i . . . . I . . . . i . . . . l . . . . i . . . . i 9 9 96 8 I 12 14 16 18 2 22 24 26
m z188
B
135
l T5 77 249. . . . . : , , ,, , , .. ] , ,L , .. .L : . : , ,, :. . . . . . . . . . . . . . . . . . . . . . . . . . [ . . . . .
5 7 9 11 13 15 17 19 21 23 25m z
5813000011000090000700005000030000i
[.5
C
77 121 249I . . . . . . . . . . . . . . . . . i L . I . . I .. , - - ,- - - . - , - - . , - - r - . , , , : , : : ' . , : : , , . ' r ' r ' ,
7 9 l l O 1 3 1 5 1 7 1 9 2 1 2 3 2 5m z
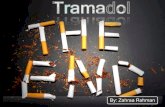
F i g u r e 3 . Mas s s pec t ra o f tr amado l A ) , N D T B) , and OD T C ) .
53
-
8/13/2019 identifikasi tramadol
4/9
J our na l o f Ana l y t ic a l T ox i c o logy Vo l . 21 N ov em ber /D ec ember 1997
Results
As shown in F igure 2 , t ram ado l , NDT, and ODT were re -solved from b oth internal s tandards, papaverine and diphenyl-am ine, in GC-M S analysis . The m etho d was not susceptible toi n t e r f e r e n c e f ro m o t h e r c o m m o n t h e ra p e u t i c d ru g s . M a s sspectra of the thre e analytes are show n in Figure 3 . Periodi-cal ly , variable a m oun ts of an art i fact of NDT appeared bo th ins a m p l e s f ro m p a t i e n t s a n d i n q u a n t i t a t i v e s t a n d a rd s w i t hmolecu lar ion rn z 261 ( the m olecu lar weigh t o f NDT is 249) .This was investigated by the d rug 's ma nuf actu rer (22), wh ichconduc ted p ro ton- and ~3C-nuclear mag net ic resonance spec-t roscopy o f the s tandard and c oncluded tha t the m z 261 peakcorresponds to a carbam ate der iva tive o f NDT, p resum ablyform ed in the inje ct ion port of the GC (Figure 4). The variablena tu re o f th i s phe nom enon m igh t a f fect re li abi li ty o f quan t i -tat ive resul ts fro m ND T. How ever, th is sh ould n ot affect in ter-preta t ion because NDT is an inactive m etaboli te.T h e GC -M S m e t h o d wa s l i n e a r fo r t r a m a d o l a n d b o t hmetabo l i t es over the range 0 .01-10 .00 mg/L wi th reg ress ioncoefficients for t ram adol , N DT, and ODT of 0 .996, 0 .99 3, and0.990, respect ively . For q uan ti tat ion, m z 58 was used fo r t ra -madoi an d ODT, and rn z 188 was use d for NDT. The fol lowingqualifying ions were used for each c om poun d: m z 135 and 263for t ramadol , m z 135 and 249 for ND T, and m z 121 and 249for ODT. Limits of detect ion (LOD) and qua nti tat ion (LOQ)were 0.01 and 0.02 rag/L, respectively,and w ere de term ined ac-co rd ing to a m ethod descr ibed by Jones and S chub er th (23) .Replicate analyses of t ramadol and metaboli te s tandards atconcen t ra t ions rang ing f rom 0 .01 to 10 .00 mg/L were per-formed, and the average con centra t ion and s tandard deviationdete rm ined from these results . Standard deviation was thenplot ted as a func tion of conce ntrat ion, and the y-intercept wastaken to be SD0. To de termine the LOD and LOQ fo r eachcom poun d, the e quations LOD = 3 x SD0 and LOQ = 8 x SD0
4500
3500 9
2500
150o ,
73
121
135
60 100
189
i g u r e 4 . M as s spec t r um o f N D T a r t i fac t .
were used . T ramado l and i t s metabo l i t es a re d i s t ingu ishedfrom a l l co mm on bas ic therapeu t ic d rugs , inc lud ing ant ide-pressants and analgesics , such as the t r icycl ics imipramine,des ip ramine , doxep in , no rdoxep in , ami t r ip ty l ine , and nor-trip tyline, an d the SSRIs (24). Co nce ntrat io ns of t rama dol ,metaboli tes , an d oth er drugs fou nd in each case, as w ell ascause and m ann er o f dea th , a re show n in Tab le I .
Discussion
I [ l 261
140 180 220 260m z
In clinical trials, peak-plasm a levels for trama dol an d ODT,wh ich were reached wi th in 2 and 3 h o f admin is t ra t ion o f asingle 100-rag dose, we re 0 .306 + 0 .078 an d 0.05 5 + 0 .020pg/m L, respect ively . W ithin 2 days of 100-mg Q.I.D. dosing,s teady-state t ram adol a nd ODT plasm a levels (0 .592 + 0 .177p.g/mL) have been rep orte d (1). Tramadol an d ODT have half-lives of 6.3 and 7.4 h, respectively, an d tramadol is 20 plasmabound. Sixty percen t of the dose s excreted in urine as metabo-l i tes , and the re st is el imin ated as u nch ang ed drug. The re hasbee n only one tramadol-related fatali ty reported in th e l i tera-ture, al thou gh the extent to which tramadol co ntributed to thedea th i s unc lear as h igh concen t ra t ions o f o ther d rugs wereprese nt (25). In tha t case, the autho rs suspected the involve-m en t o f sero ton in syndro me as a resu l t o f the moclobemide-clomipramine interact ion as has been previously reported (26).The au thors fu r ther sugges ted tha t t ramado l cou ld have had asynergis t ic effect on th e seroto nin syndro me because of i tsserotonin reuptak e-inhibi t ing abi l ity . Other fatali t ies involvingtramadol have occurred (27), al thou gh the cases have not beenpublished. The tramadol concentrat ions in these cases were2.7 and 1.3 rag/L; how ever, metabolite concentrations were no tmeasured, and i t is unkno w n if o th er drugs were involved.The presence of oth er drugs see m s to be typical of cases in-volving tramadol . For example, thre e drug-impaired drivers , all of w hom were found tohave thera peutic levels of t ramadol in theirblood, and one w ho had elevated trama dollevels in her urine, also had other drugsprese nt . Table II sum ma rizes these cases .As me n t io ned p rev ious ly , t ram ado l i s
metabolized to ODT by CYP2D6, and, assuch, i ts metabolism may be inhibi ted byt h e p re s e n c e o f o t h e r s u b s t ra t e s , wh i c hmay affect p lasm a levels of the paren t drug.The presence of such dru gs shou ld there-fore be taken into considerat ion in casesinvolving tramadol . The therap eutic effectof the drug m igh t be increased or decreasedby the presence of a 2D6 inhibi tor, as bothtramadol and ODT are pharmacological lyactive.Consequently , i t is impo rtant to considerODT l e ve ls wh e n i n t e rp re t i n g t r a m a d o llevels . Com paring the levels of the parentdru g and metaboli te m ay provide informa-t ion o n whe ther the d rug was ch ron ica l ly
53
-
8/13/2019 identifikasi tramadol
5/9
J o u r n a l o f A n a l y t i c a l T o x i c o l o g y , V o l . 2 1 , N o v e m b e r / D e c e m b e r 1 9 9 7
T a b l e I . C a s e I n f o r m a t i o n o n S u b j e c ts T e s t i n g P o s i t iv e f o r T r a m a d o lT * O D T N D T A l c o h o l C i rc u m s t a n c e s u r ro u n d i n g C a u s e o f M a n n e r fC a s e A g e G e n d e r m g / L ) m g / L ) m g / L ) g / lO O m L ) O t h e r d r u g u se de a th d e ath d e ath
I 1 8 F 0 . 0 3 0 . 0 6 0 . 11 n e g c a r b o n m o n o x i d e S u b j e c t w a s p o o r l y n o u r i s h e d S u d d e n c a r d i a c U n d e t e r m i n e d( < 5 % s a t) w / b e l o w n o r m a l e x e r c is e , H x d e a t h f ro mn i c o t in e J c o t i n in e o f a l c o h o l & d r u g a b u s e ; u n k n o w n e t io l o g y
b e c a m e s h o r t o f b r e a t h &c o l l a p s e d a f t e r m i l d e x e r t i o n ,u n a b l e t o b e r e s u s c i ta t e d
2 4 1 M 0 . 0 8 0 . 0 7 0 . 0 3 0 . 0 2 m o r p h i n e ( 0 . 1 8 ) H x o f d r u g a b u s e , o u n d A c u t e i n t r v e n o u s A c c i d e n t a ld e a d b y f r ie n d d u r i n g c a m p i n g n a m o t is mt r i p ; h a d i n g e s t e d a r g eq u a n t i t ie s o f a lc o h o l , h e r o i n , &p a i n m e d i c a t io n
3 4 8 M 0 . 4 1 0 . 0 4 0 . 2 7 n e g m o r p h i n e ( 0 . 1 4 ) H x o f d r u g a b u s e , d i e d A c u t e s u b s t a n c ep r o p o x y p h e n e ( 0 . 0 4 ) s u d d e n l y & u n e x p e c t e d l y a b u s en o r p r o p o x y p h e n e ( 0 . 2 3 )
4 5 4 /',4 0 . 0 5 0 . 0 4 0 . 0 1 0 . 0 6 m o r p h i n e ( 0 . 2 7 5 ) H x o f e m p h y s e m a & d r u g a b u s e ; A c u t e m o r p h i n ec o d e i n e ( 0 . 0 7 ) f o u n d d e a d w / d r u g p a r a p h e n a l i a i n to x i c a t io nn o r p r o p o x y p h e n e a t s c e n e ; a u t o p s y i n d in g s i n c lu d e( < 0 . 0 5 ) p u l m o n a r y e d e m a , a r t e ri o s c le r o s i s ,&n o r d i a z e p a m ( 0 . 1 6 ) a t h e r o s c l e ro s i s5 2 8 F 0 . 0 5 0 . 4 6 0 . 7 3 n e g d e x t r o m e t h o r p h a n H x o f d r u g a b u s e ; d i e d M u l ti p le d r u g( 0 .9 0 ) s u d d e n l y & u n e x p e c t e d l y a f t e r a b u s ep r o p o x y p h e n e ( 0 . 4 0 ) i n g e s t in gm o r p h i n e & v a r io u sn o r p r o p o x y p h e n e p a i n m e d i c a t io n s ; d r u g( 0 . 9 0 ) p a r a p h e n a l i a o u n d a t s c e n e ;m o r p h i n e ( < 0 . 0 2 5 ) a u t o p s y r e v e a le d p u lm o n a r y e d e m a
6 5 7 F 0 . 4 8 0 . 0 2 0 . 3 2 n e g d o x e p i n ( 1 0 . 0 0 ) H x o f d e p r e s s i o n ,o n m e d i c a t io n A c u t e d o x e p i nd e s m e t h y l d o x e p in f o r s a m e , o u n d d e c e a s e d a t h o m e ; o v e r d o s e( I . 4 ) e m p t y p i l l b o t t l e s ( d o x e p i n , p a x i l ,n i c o ti n e / c o ti n in e I o d in e ) f o u n d i n b e d r o o m
7 3 6 M 0 . 1 6 1 . 8 4 0 . 0 5 n e g a lp r a z o l a m ( 0 .1 1 ) H x o f b a c k p a i n , f o u n d d e a d i n A c u t e P r o b a b l yp r o p o x y p h e n e ( I . 9) p a r k e d m o t o r v e h i c le w / u p p e r c o m b i n a t io n d r u g a c c i d e n t a ln o r p r o p o x y p h e n e t o r s o s l u m p e d t o w a r d s p a s s e n g e r i n to x i c a t io n( 3 . 0 ) s e a t ; A m b i e n ( z o l p i d e m t a r t r a t e )f o u n d o n r ig h t p a s s e n g e r e a t
8 5 8 F 0 . 1 2 0 . 2 8 0 . 6 0 0 . 1 0 a m i tr ip t y li n e ( 0 . 1 3 ) S u b j e c t i e d a t h o m e a f t e r 2 d a y sn o r t ri p ty l in e ( < 0 . 1 ) d i s c h a r g e d r o m h o s p i t a l, o n
I n a p s i n e V g i v e n b y d a u g h t e r ,b u t i n v e s t i g a t o r su n a b l e t o f i n ds a m e ; c o ro n e r d e l a y e d d e c i s io nt o d o a u t o p s y , a n d b o d y n o t r e f ri g -e r a t e d s o m o d e r a t e ly d e c o m p o s e d
9 3 9 M 1 . 4 3 0 . 0 3 0 . 1 8 n e g a m i t ri p ty l in e ( 0 . 5 9 ) N o k n o w n m e d i c a l h i s to r y , o u n dn o r t ri p ty l in e ( 0 . 6 8 ) d e a d , f a c e d o w n , a t h o m e ;d i a z e p a m ( 0 . 2 7 ) p r e s c r ip t io n d r u g s i n c lu d e :n o r d i a z e p a m ( 0 . 1 9 ) p r e d n i s o n e d i a z e p a m , r a m a d o l ,
& m e t h o c a r b o n a l1 0 3 8 F 2 . 4 7 0 . 0 6 0 . 1 6 n e g a m i tr ip t y li n e ( 0 . 4 3 ) D i e d s u d d e n l y & u n e x p e c t e d l y ;
n o r t r i p t y li n e ( 0 . 7 1 ) R x i n c l u d e : u l t ra m ,h y d r o c o d o n e ( 0 . 0 7 ) a m i tr ip t y li n e , d e l t a z o n e , b u s p a r
1 1 3 2 M 2 2 . 5 9 0 . 3 4 2 . 0 8 0 . 0 2 p r o p r a n o l o l ( 3 . 9 0 ) A d m i t te d t o E R b e c a u s e o f m u l t ip l e M u l t ip l e d r u g S u i c i d ed e s i p r a m i n e ( I . 0 0 ) d r u g o v e r d o s e - - t r ic y c l ic & b e t a - o v e r d o s et r a z o d o n e ( 3 . 7 0 ) b l o c k e r , d i e d s h o r t ly a f t e r a d m i s s io n ;
H I V + ; R x i n c l u d e p r o p r a n o l o l , u l t r a m ,t r a z o d o n e , k l o n o p in , d e s i p r a m i n e ,
h y d r o x y z , l i t h o n a t e1 2 4 4 M 1 .1 3 0 . 4 6 0 . 3 0 . 1 4 n o r d ia z e p a m ( 0 . 2 0 ) R e l e a s e dr o m m e n t a l h o s p i t a l i n D e c a p i ta t io n S u i c i d e
c a r is o p r o d o l ( 2 . 7 0 ) m o r n i n g & w a l k e d t o t r a in t r a c k sm e p r o b a m a t e 5 . 9 0 ) a f t e r l e a v in g r ie n d ' s h o u s e ; p l a c e d
h e a d o n t r a c k s w h e n h e h e a r d r a inc o m i n g ; e n g i n e e r w a s u n a b l e t os t o p i n t im e
U n d e t e r m i n e d
U n d e t e r m i n e d
U n d e t e r m i n e d
U n d e t e r m i n e d
C o r o n a r y a r t e ry U n d e t e r m i n e dd i s e a s e , a l t h o u g hd e t e r m i n a t i o nm a d e b e f o rer e c e i p t o ft o x i c o l o g yr e s u l t sP o s i t i o n a l A c c i d e n t a la s p h y x i as e c o n d a r y oa c u t e d r u gi n t o x i c a t i o nA c u t e t ra m a d o l U n d e t e r m i n e di n t o x i c a t i o n
~ A b b r e v i a t io n s : T , tr a m a d o l ; O D T , O - d e s m e t h y l tr a m a d o l ; N D T , N - d e s m e t h y l tr a m a d o l ; H x , h i s to r y .
5 3 3
-
8/13/2019 identifikasi tramadol
6/9
or acutely ingested. I n addition, ODT contr ibute s to toxicity byway of i ts analgesic act ivity , wh ich is twice that of the pa rentcompound . I t s h igher ~-op io id recep to r a f f in i ty a l so con-tributes to toxicity throu gh depression of the ce ntral nervo ussystem.The role of t ramado l in fatali ties is d ifficul t to d eterm ine be-cause no fa ta l overdoses in w hich t ramado l a lone was p rese n thave been reported. H owever, an invest igat ion of the circ um -stances su rrou ndin g each case in th is s tudy provided invest i-gators with basel ine infor ma tion regard ing the blood levelsassociated with different types of fatal i t ies . No antemortemmedical evaluation was pe rform ed on any of the subjects de-scribed; therefore, consid erat ion of the role of seroto nin syn-drom e in these fatal i ties was based solely on th e pre sence orlack of seroton ergic act ivi ty of al l drugs present . T he thera -peutic and toxic ranges for drugs pre sent in the blood samplesand th eir relat ive abi li t ies to inh ibi t neurotra nsm it ter reuptakeand th e CYP450 isozyme(s) ( if known) for wh ich they are sub -strates (12-14,28-31) are sum m arized in Table III .
The low levels of t ram adol and rnetaboli tes in Case I ma keit unl ikely tha t the dru g played a role in th is death . Similarily ,the very low carbon monoxide levels rule o ut sm oke inhalationas a cause o f dea th . The t ru e cause o f the sub jec t s suddend e a t h r e m a i n s u n d e t e rm i n e d .Cases 2 , 3 , and 4 are clearly att r ibutable to acute m orp hineintoxicat ion (32). In each case, the m orph ine conc entrat io n isquite high, whereas the levels of other drug s present, includingt ramado l , a re wel l wi th in o r be low the therapeu t ic window.How ever, i t is possible that t ram adol m ay have contribu tedslightly to the se de aths beca use of its ~t-opioid eceptor affinity.The occ urren ce of sudd en death , as in Case 3 , and th e autopsyf ind ing o f pu lmonary edema, as in Case 4, a re bo th com mo n inm orph ine overdoses (33). I t is unclear how the se subjects ob-tained tramadol , al tho ugh the drug is not a scheduled narcotic.Tramadol s abuse poten tial was originally reported to be m uc hlower than tha t of mo rph ine (1). However, Ortho-McNeil s re-cent let ter to heal th care professionals providing addit ional
J o u r n a l o f A n a l y t i c a l To x i c o lo g y , V o l . 2 1 , N o v e m b e r / D e c e m b e r 1 9 9 7
inform ation on this subjec t reports 115 spontan eous domestica d v e r s e e v e n t s d e s c r i b e d a s d r u g a b u s e , d e p e n d e n c e ,withdrawal, or in tent ional overdose, not including cases ofaccidental overdose. Pat ients with a past or presen t his tory ofaddiction or depe nden ce on opioids acc ount for a ma jori ty ofthese reports (11). The fa ct that 4 of the 12 case s involvingt r a m a d o l r e p o r t e d h e re we re a l s o p o s i t i v e fo r m o rp h i n esuggests th at the ma nufacture r s conc erns are well founded.Morphine conc entrat ion s reported as less tha n 0 .025 I~g/mL,as in C ase 5 , me an tha t th e sample tes ted posi t ive, al thou gh thelevel is below the limit of quantitation of the analytical method.Blood mo rph in e leve ls in m orph in e-cause d dea ths can besignificantly lower when the survival period is longer than3 h (33).The tram adol level in Case 5 was low , but its effect, com binedwi th tha t o f ODT, may have con t r ibu ted to th e op io id e ffec t o fmo rph ine . Fur ther , the p resence o f dex t rome thorpha n andpropoxyphene, wh ich are both CYP2D6 substrates, ma y havecon t r ibu ted to decreased c learance o f t rama do l because o fc o m p e t i t i v e m e t a b o l i c i n h i b i t i o n , t h e re b y p ro l o n g i n g o renha ncing tramadol s effects . In addit ion, i t is conceivable thatt h e s e r o t o n i n r e u p t a k e - i n h i b i t i n g a b i l it y o f b o t h d ex -t ro m e t h o rp h a n a n d p ro p o x y p h e n e , c o m b i n e d wi t h t h a t o ftramad ol played a role in th is subject s death .Case 6 is clearly at t r ibutable to doxepin overdose. How ever,in te rac t ion f rom t ramad o l cou ld con t r ibu te to cause o f dea thbecause of the m oderate se rotonergic effect of both drug s. Theleve ls o f t ramado l and metabo l i t es a re wi th in therapeu t icranges , bu t co ncom i tan t admin is t ra tion wi th very h igh leve l sof doxepin may have contrib uted to serotonerg ic cris is , whichwas d ue to the chro notro pic and inotropic effects of serotonin,as well as the increased vasoconstriction produ ced by nore-pineph rine, angiotensin II , and his tamine (34).Case 7 is in terest ing in that , al though the t ramadol con-centrat ion is fairly low, the ODT conc entrat io n is extremelyh i g h , a n d p ro p o x y p h e n e a n d a l p ra z o l a m , wh i c h a r e b o t hCYP2D6 substrates , we re also pres ent in fairly high concen-
T a b l e I I . T r a m a d o l L e v e l s i n F o u r D r u g I m p a i r e d D r iv e r sS a m p l e T * O D T N D T l c o h o l
C a se g e G e n d e r t e s te d (mg/L) (mg/L) (mg/L) (g / lOOm L) O t h e r d r u g u s e C a s e h i s to r y1 44 M b lood 0 .07 0 .05 0 .09 neg coca ine
-
8/13/2019 identifikasi tramadol
7/9
J o u r n a l o f A n a l y t i c a l T o x i c o lo g y , V o l . 2 1 , N o v e m b e r / D e c e m b e r 1 9 9 7
t rat ions. Althou gh i t is possible th at a m etabolic in ter act iontook place, the l ikely explan ation is that th e sub ject ingested alarge bu t not fatal dose of t ram adol at an earl ier t im e. Acute,com bined -drug intoxicat ion seem s reasonable as a cause ofdea th .Case 8 was cert if ied as a natur al d eath before toxicologytest ing was complete. In reviewing the toxicologyresults, how-ever, i t is possible that ther e was som e serotonergic in teract ionbetween the d rugs p resen t tha t , toge ther wi th the a lcoho l ,may have been impor tan t .The very h igh t ramado l l eve l s and low metabo l i t e concen-t ra t ions in Case 9 po in t to an ac u te t ramado l inge s t ion in acom bined -drug overdose. Again, the effect of elevated conc en-trat ion s of several seroto nerg ic drugs tha t are also 2D6 sub-s t ra tes m ay have con t r ibu ted to the increased p lasma co ncen-trat ion s that p layed a ro le in th is fatal ity .The p resence o f ami t r ip ty l ine and hydrocodone , w h ich are
both substrates for CYP2D6, indicated a possible com peti t iveinh ib i t ion o f the i soenzyme. T he h igh concen t ra t ion o f t ra -m ado l relative to ODT also su pported this. It is also conceivablethat the combined serotonergic act ivi ty of amitriptyl ine and
tram adol was s ignificant in th is pe rson s death .In add i t ion to s ign i f ican t concen t ra t ions o f severa l sub-strates o f 2D6 in C ase 11, h igh levels of desipramine, an in-hibi tor of 2D6, we re also presen t . As in C ase 10, extremelyhigh levels of t ram adol relat ive to those o f its metabolites sup-por ted the p ossibility of comp etitive inhibition. It is likely th atthe sero tonerg ic ac tiv ity o f several d rug s p resen t in the sub-ject s b lood also played an im por tant role.The concen t ra t ions o f t ramado l and ODT in Case 12 arebo th wel l above the therapeu t ic range , and they , a long wi th thehigh blood alcohol level , ma y have contribute d to central n er-vous system depression. How ever, decapitat ion w as clearly thecause of death in th is case.In sum mary , t ramado l i s u sua lly p rese n t wi th an t idepres -san ts and /o r o the r op iates, bo th o f wh ich ca n in te rac t wi tht ramado l and i t s act ive m etabo l i te when th e d rug i s p resen t .ODT leve ls shou ld be taken in to cons idera t ion when in te r -p re t ing t ramado l concen t ra t ions , espec ia l ly when mo rph ine i salso present . The appearance of the two dru g interac t ions dis-cussed, the com petit ive inhib i t ion of CYP2D6 causing en zym esatu ra t ion and subsequ en t decreased c learance o f t ramado l
T a b l e I I I . P r o p e r t i e s o f D r u g s F o u n d i n P o s t m o r t e m B l o o d *T h e r a p e u t ic R e u p t a k e n h i b i ti o nc o n c e n t ra t io n T o x i c c o n c e n t r a t io nD r u g m g /L ) m g /L ) N E t D A S T
Alprazolam 0.02-0.04 >0.07 0 0 03A4, 2D6 minor)
Am itriptyl ine 0.06--0.22 >1.0 + 0 ++2D6,3A4 minor)
Codeine 0.03-0.3 4 1.00-8.80 0 0 02D6-to morphine)
Desipramine 0.01-0.2 8 1.20-15.00 +++ 0 03A4; nhibits 2D6)
Dextromethorpan 0.38 LOD = 0.5 g 0 0 +*2D6, 3A4 minor)
Doxepin 0.03-0.15 >0.1 + 0 +Diazepam 0.1-2.5 >1.5 0 0 02C19)
Hydrocodone 0.002-0.024 0.13-7.00 0 0 02D6)
Morphine 0.01-0.07 0.12--4.70 0 0 0Propoxyphene 0.05-0.75 1.0-2.0 + 0 +*2D6)
Propranolol 0.01-0.26 4.00-29 .00 0 0 02D6)
Tramadol 0.23-0 .77 LOD = 0.5 g + 0 +2D6)
Trazodone 0.49-I .60 >I 5.00 0 0 +
* Al l leve lscom e f rom Basel t and Crave y (32) except those o r t ramadol , wh ic h com e f rom the revised product inser t f rom O rtho-McNe i l (29) .+ Abb revia t ions and symbols: NE = no rep inephr ine; DA = dopam ine; ST = seroton in ; + to +++ = act ive to st rong ly act ive ; = weak ly act ive ; 0 = lacking.* Dextrom ethorphan s seroton in reuptake inh ib i t ing ab i l i ty is d iscussed in a paper by Sk ope t a l . (30)a nd that o f propoxyphene was reported by Codd et a l . (31) .
5 5
-
8/13/2019 identifikasi tramadol
8/9
potent ia l ly l eading to toxic s ide e f fects , and the comb ined sero-tonergic act iv i ty of two or more drugs should a l so be cons id-e r e d w he n i n te r pr e ti ng t r a m a do l l e v e l s. A t h i rd m e c ha n i s m o ftoxic ity in the subjects w ho had hi s tor ies of heart di sease m ayresul t f rom increased serotonin l eve l s. Un der norm al vascularcondi t ions , p late le t s re lease serotonin to promote vasodi la-t i o n a nd p l a t e le t a g g r e g a t io n , w h i c h c a us e v a s c u la r ho l e s a ndt e ar s to s ea l w i t h o u t c a u s i n g t h r o m b u s f o r m a t i o n 3 5 ) .However , in pat ients wi th vascular di sease , vasoconstr ic t ionc a n o c c u r w h e n s e r o t o n i n l e v e l s a r e i n c r e a s e d 3 6 ) . T h ec o m bi na t io n o f i ncr e a s ed s e r u m s e r o t o n i n l e v e ls , wh i c h a r edue to the p resence of serotonin reuptake inhibi t ing drug s , andt h e d e c r e a se d a b i li t y o f t h e e n d o t h e l i u m t o m e t a b o l i z es e r o t o n i n , wh i c h i s due t o i s c he m i c da m a g e , c o m po unds t hes e e m i n g l y c o n t r a d i c t o r y v a s o c o n s t r i c t i o n s e e n w i t h ada m a g e d e ndo t he l i um 2 9 ) .
ConclusionWe have descr ibed several fa ta li ties in w hich tramadol w asfound along with oth er drugs. I t is imperative that c l inic iansmaintain heightened awareness of the r isks associated withtramadol use to help m inim ize the prescr iption of medicationcombinations th at are l ikely to induce abno rmally high sero-tonergic activity or contr ibute to metabolic interactions orother ad verse reactions. Clinic ians and p hysicians should a lsowatch for evidence of tramadol abuse an d should a ttem pt todetermine if patients are taking other agents with ~-opioidreceptor aff inity. I t is h oped that these f indings will provide
guidance to toxicologists and pathologists in recognizing thepossibili ty of drug interactions involving tramadol, as w ell astramadol s contr ibution to heroin/m orph ine overdoses.
AcknowledgmentsWe gratefully acknow ledge the assistance of R.W. Johnsonchemists D. Xu, S. Chan , and T. W illiams for their help in e lu-cidating the s truc ture o f the N-desmethyltramadol ar t ifactthrough NMR and l iquid chromatographic-mass spectrometric
analysis, and we th ank the staff of the W ashington State Toxi-cology Laboratory for oth er d rug analyses performed in thesecases
References1 . Tox i -Lab A . New Drugs . Produc t lea f l e t (1995) .2. B. Dr iessen , W . Reiman , and H. Gier ts. In teract ion of the centra lana lges ic , tramado l , w i th the up take and re lease o f 5 -hyd roxy-tryptamine in the rat bra in in v i t ro . Bri t . J . Pharmac oL 108 :806-11(1993).3. E. Fr ider ichs, E. Felgenhauer, P. Jongsch aap, and G . Oster loh.Pharma co log ica l i nves t iga t i ons on ana lges ia and the deve lop -men t o f dependence and to le rance w i th t ramado l , a s t rong l yact ing analgesic. Arzne im. -Fo rsch . /D rug Res . 2 8 :1 2 2 - 3 4 ( 1 9 7 8 ) .5 6
Journal of Ana lytical Toxicology, V ol. 21, Novemb er/December 1997
4 . C .R . Lee , D . McT av i sh , and E .M. Sork in . Tramado l . A p re l im ina ryrev iew o f i t s pha rmacok ine t ic p roper t ies and the rapeu t i c po ten -t ia l i n acu te and ch ron i c pa in s ta tes . Drugs 4 6 :3 1 3 - 4 0 ( 1 9 9 3 ) .5 . W . K e u p . Missb rauchsmuste r b e i Abh~ng igke it yon A l koho l ,Med ikam en ten u nd Drogen-Frdhwam sys tem-Da ten f i J r d ie Bun-desrepub l ik Deu tsch land 1976-1990 . Lamb ertus Ver lag, Fre iburgim Bre i sgau , Germ any , 1993 , pp 48 -145 .6 . T . Murano , H . Yam amoto , Y . Endo , N . Okada , Y . Masud a , and I .Yano . S tud ies o f dependence on t ramado l i n ra ts . A r z n e i m . -Fo rsch . /D rug R es . 2 8 :1 5 2 - 5 8 ( 1 9 7 8 ) .7. J.E. Vi l larreal and M .H. Seevers. Evaluat ion of n ew com pound s formorph ine - l ike phys i ca l depen dence i n the Rhesus monkey . Na-t iona l Research Cou nc i l , C omm i ttee on Prob lems o f D rug D e-pendence . Proceed ings rom the 30 th mee t i ng . Na t i ona l Academ yo f Sc iences , W ash ing ton , D .C . , 1968 , Add endum 2 , pp 1 -15 .8 . T . Yanag ita . D rug dependence po ten t ia l o f 1 - (m-m ethoxypheny l ) -2 - (d ime thy laminomethy l ) -cyc lohexan- l -o l hyd ro ch lo r i de ( t ra -mado l ) tes ted i n monkeys . Arzne im. -Fo rsch . /D rug . Res . 28 :158-63 (1978) .9 . B . N i cke l and A . A led te r . Compara t i ve phys i ca l dependences tud ies in ra ts w i th f l up i r t i ne and op ia te recep to r s t imu la t inganalgesics. Postg rad . M ed . ] . 6 3 :4 1 - 4 3 ( 1 9 8 7 ) .10 . K .L . Pres ton , D .R . Jas insk i, and M . Tes ta . Abuse po ten t ia l andpharmaco log i ca l com par i son o f t ramado l and m orph ine . Drugand AIc . Dep . 2 7 :7 - 1 7 ( 1 9 9 1 ) .11 . T . G ibson . Le t te r f rom O r tho -M cN e i l , 1996 .12. R.J.Baldessar in i . Drugs and the treatm ent of psych iatr ic d isorders:depress ion and m an ia . In Goodm an Gi lman 's The Pharma co-log ica l Bas is of T herapeu t ics, 9 th ed . J .G. Hardma n and L .E . L im-b i rd , Eds . Mc Gra w H i l l , New York , NY, 1996 , pp 431-59 .13 . The Un i ted S ta tes Pharmaco pe ia l Conven t i on , Inc . U S P D I U p -da te vo l s . 1 and 2 . Un i ted S ta tes Pharmaco pe ia l Conven t i on ,Rockv i l l e , MD, 1995 .14 . N .L . Ke r ry , A .A . S omogy i , G. M ikus , and F. Bochner . Pr imaryand secondary ox ida t i ve me tabo l i sm o f dex t rometho rphan . Inv i vo s tud ies w i th fem a le Sprague-Dawley and Da rk Agou t i ra tl ive r m ic rosomes. Biochem. Pharmaco l . 45(4 ) 833 -39 (1993) .15 . Y .X . Yu , Y .Q . Yu , C .J . Zhang , and L . Shen . Ana lys i s o f t ramado land i ts me tabo l i tes i n h um an u ri ne . A c ta P h a r m . S i n . 28(5):379 -83 (1993) .16. B. EIs ing and G. Blasc hke. Achi ra l and ch i ra l h igh-pe rforman cel iqu id ch rom atograph ic determ inat ion of t rama dol and its ma jorme tabol i tes in ur ine after ora l adm in istrat ion of racem ic tra-mado l . J. Chromatogr. 6 1 2 :2 2 3 - 3 0 ( 1 9 9 3 ) .17. W . L intz, S. Er lacin, E. Frankus, and H. Urag g. Me tabol ism oftra-mado l i n man and an ima ls . Arzne im. -Fo rsch . 31(2 ) : 1932-43(1981).18. W . L intz and H. Urag g. Qu ant i ta t ive determ inat ion of t ramad ol inhuman se rum by gas ch romatog raphy /mass spec t romet ry . J. Chro-matogr. 341 : 65 -79 (1985) .19 . R . Becker and W. L in tz . De te rmina t i on o f tramado l i n hum anserum by cap i l la ry gas ch romatog raphy w i th n i trogen-se lec t i vedetect ion. J. Chromatogr. 3 7 7 :2 1 3 - 2 0 ( 1 9 8 6 ) .20. E .H . Foerster , D. H atchett , and J.C. Garr io t t . A rapid, compre-hensive screening procedure for basic drugs in b lood o r t issues bygas ch romatog raphy . J. Anal . Toxico l . 2 :5 0 - 5 5 ( 1 9 7 8 ) .21 . E .H . Foers te r and M .F. Mason . Pre l im ina ry resu l ts on the use o fn-buty l c h lor ide as an extractant in a drug screening proced ure.J. Forens ic Sci . 19(1 ) : 155 -61 (1974) .22. D. Xu, S. Cha n, and T. W i l liams. Personal com mu nicat ion, 1996.2 3 . A .W . J o n e s a n d J. S c h u b e r th . C o m p u te r - a i d e d h e a d s p a ceg a s c h r o m a t o g r a p h y a p p l i e d t o b l o o d - a l c o h o l a n a l y s i s :impor tance o f on l i ne p rocess con t ro l . J. Forensic 5ci . 34(5):1116-27 (1989) .24 . K .E . Goer inge r , B .K . Logan , and G .D . Chr i s t ian . A typ i ca l an t i de -pressants and the i r m etabol i tes in postmo rtem blood : a review ofthe l i terature and report o f cases. J. F orensic Sci . ( in press).25 . A .F . Hernandez , M .N . Mon te ro , A . P la , and E . V i ll anueva . Fa ta lmoc lobem ide ove rdose o r dea th caused by se ro ton in syndrome?J. Foren sic 5ci . 40(1 ) : 128 -30 (1995) .
-
8/13/2019 identifikasi tramadol
9/9
Journal of Ana lytical Toxicology, Vo l. 21, N ovember/Decem ber 199726 . O . S p igse t, T . M jo rnda l , and O. Lovhe im. Sero ton in syndromecaused by a moc lobem ide -c lomip ramine i n te rac t i on . Br Med J
3 6 : 2 4 8 ( I 993).27. J. Ol iver . Person al com mu nicat ion, 1995 .28. N. Rivers and B. Hom er. Po ssib le le thal react ion betwe en Nard i land dex t rometho rphan . Can M ed Assoc J 1 0 3 :8 5 ( 1 9 7 0 ) .29 . O r tho -M cN e i l . R ev i sed p roduc t i nse r t fo r U lt ram (1996) .30 . B .P . Skop , J .A . F inke l s te in , T .R . Mare th , M .R . Magoon , and T.M .Brown . Th e se ro ton in syndrome assoc ia ted w i th pa roxe t ine , anover- the-counter co ld rem edy, and vascular d isease. Am . ] . Em erg.Med 12(6): 642--44 (1994).31 . E .E . Codd , R .P . Schank , J .J . Schupsky , and R .B . Ra f fa . Se ro ton inand norep inephr ine uptake inh ib i t ing act iv i ty o f centra l ly act inganalgesics. PharmacoL Exp Ther 274(3 ) 1 263 -70 (1995) .32 . R .C . Base l t and R .H . Cravey . Disposi t ion of Toxic Drugs andChemicals in M an 4th ed. Chemical Toxico logy Inst i tu te, FosterCi ty, CA, 1995.
33 . J .C . Ga r r i o t t and W .Q. S tu rne r . Mo rph ine con cen t ra t ions andsurviva l per iods in acute hero in fa ta l i t ies. N Eng l J Med 2 8 9 :1276-78 (1973) .34 . B .N . Pr i cha rd and C .C . Smi th . Se ro ton in : recep to rs and ago-n i s t s - - s u m m a r y o f s y m p o s i u m . Cl in Phys io l B iochem8 s u p p l .3 ) : 1 2 0 - 2 8 ( 1 9 9 0 ).35 . S .M . Houran i and N .J . Cusack . Pharmaco log ica l recep to rs onblood p late lets. Pharmacol Rev 4 3 :2 4 3 - 9 8 ( 1 9 9 1 ) .36 . K . Sch ro r and M . Braun . P la te le ts as a sou rce o f vasoac t ivemed ia to rs . Stroke 21 : IV -32 -1V-35 (1990) .
Manuscr i p t rece i ved November 5 , 1996 ;rev i s ion rece i ved March 24 , 1997 .
5 7