ID Title Description Controls in place Director Healthcare ... · PDF filenot without its own...
22
ID Title Description Controls in place Director 502 Non compliance with the UK Blood Safety and Quality Regulations The Medicines and Healthcare Products Regulatory Agency (MHRA) is the competent authority who oversees the UKBSQR 2005. The UKBSQR 2005 insists that all staff involved in the collection of red cells from any authorised blood fridge must undergo Collection Competency Assessment. Levels of A&A competency assessment in blood collection processes remais less than 100% despite some areas desisting from this practice. Assessments require to be repeated every two years. There is restricted accessibility to blood fridges. Work is being done to re-establish network of trainers across the organisation who are capable of peer assessing collection competencies. Alison Graham 520 Medication errors due to medicines reconcilliation failure Failure to complete medicine reconciliation on admission and discharge could result in medication errors within both the hospital and community setting. Within the medical clerk in proforma and also the pre-op documentation medicines reconciliation form included for medicines reconciliation on admission. Awareness and training done for medical staff to complete. Work ongoing to progress and to improve process on discharge. Scottish Government CEL was published in September 2013 to take medicines reconciliation forward across Scotland. Work being undertaken to review this document and implement recommendations made. Michele Caldwell Healthcare Governance Committee
Transcript of ID Title Description Controls in place Director Healthcare ... · PDF filenot without its own...

ID Title Description Controls in place Director
502 Non compliance with the UK Blood Safety and Quality Regulations
The Medicines and Healthcare Products Regulatory Agency (MHRA) is the competent authority who oversees the UKBSQR 2005. The UKBSQR 2005 insists that all staff involved in the collection of red cells from any authorised blood fridge must undergo Collection Competency Assessment. Levels of A&A competency assessment in blood collection processes remais less than 100% despite some areas desisting from this practice. Assessments require to be repeated every two years.
There is restricted accessibility to blood fridges. Work is being done to re-establish network of trainers across the organisation who are capable of peer assessing collection competencies.
Alison Graham
520 Medication errors due to medicines reconcilliation failure
Failure to complete medicine reconciliation on admission and discharge could result in medication errors within both the hospital and community setting.
Within the medical clerk in proforma and also the pre-op documentation medicines reconciliation form included for medicines reconciliation on admission. Awareness and training done for medical staff to complete. Work ongoing to progress and to improve process on discharge. Scottish Government CEL was published in September 2013 to take medicines reconciliation forward across Scotland. Work being undertaken to review this document and implement recommendations made.
Michele Caldwell
Healthcare Governance Committee

ID Title Description Controls in place Director
511 Failure to implement all four new immunisation programmes successfully could cause failure to prevent childhood and adult commun
Risk that failure to implement programmes successfully, whilst maintaining high uptake in existing programmes, could cause a loss of confidence in immunisation programmes and reputational damage to the organisation. Whilst funding and GP negotiations for Year 1 have been agreed these are ongoing risks for future years and could jeopardise delivery of the programmes. One main ongoing risk for the programme is ensuring there is enough appropriately trained staff to safely deliver the programmes, in particular the seasonal flu extension over a short period of time to a large number of children. Risks attached regarding staffing for local co-ordination of programme. There is also a risk in ensuring sufficient vaccine storage and transportation to enable cold chain to be maintained.
Long established programmes in place to undertake, monitor and review childhood immunisation requirements for the population. Frequent local multi-disciplinary and multi-agency delivery group meetings. Oversight of immunisation programmes carried out as part of Public Health Governance. Representation on National Service Delivery Group with existing risk register. Local action plan regarding risks.
Carol Davidson

ID Title Description Controls in place Director
513 Junior Doctor August Changeover National data suggests that there is a small increased mortality rate associated with the changeover date (1st Wednesday in August) for training grade doctors. The increase in mortality is reported to be greatest in the sub group of patients admitted to general medicine. There are over 260 doctors in training working for NHS Ayrshire and Arran and the majority changeover between different Health Boards on this date.
All trainee doctors commencing in August attend generic hospital induction, which is repeated on three occasions to allow attendance by trainees commencing on nights or on leave. All trainees attend separate departmental induction which introduces them to the wider teams, their duties and responsibilities, local reporting systems, guidelines and protocols. Separate arrangements in place for trainees starting at different times, especially nights. Need to potetnially reduce elective services (e.g. clinics, theatres) highlighted through CD Forum and email communication to ensure that there is adequate consultant (or other doctor) presence on wards for emergency care while trainee doctors attend induction training. This is particularly highlighted within general/acute medicine where largest potential risk exists.
Alison Graham
515 NHS ADOC Service failure Continuing difficulty in filling standby and substantive shifts, particularly overnight shifts, resulting in risk to service continuity and patient safety along with reputational risk and risk of loss of public confidence. We continue to have to work right up to the last minute to fill shifts and are regularly left with some service deficit and no standby capacity. This risk will substantially increase over the winter months as winter activity and demand increases along with norovirus and flu outbreaks.
Enhanced payments for weekend shifts secured until February 2014. Improved working conditions including additional support for busier shifts, longer consultation times and flexible shift start and finish times being piloted. Major review and option appraisal underway to explore possible future models of care to guarantee sustainability. Short Life Working Group established and chaire by the Medical Director.
Alison Graham

ID Title Description Controls in place Director
529 Delays in patients receiving prescribed medication when using the HEPMA system due to delays in admission to PMS
The delay in admitting patients onto PMS which triggers the admission onto the JAC HEPMA system continues to cause difficulties in clinical areas. Several attempts to remedy the situation have been undertaken and the situation in the Medical Unit at Ayr has improved. Urology and Surgery at Ayr continue to report problems and have added this to their risk register. Delays in real time admission mean that patients cannot have medicines prescribed and administered.
Workaround to allow wards to admit direct to JAC. Repeated reminders to users to admit in real time.
Michele Caldwell
149 Breach Of Confidentiality / DPA Potential for a breach of confidentiality or a breach of the Data Protection Act to occur.
eLearning programme has been developed for staff to inform IG awareness and requirements of DPA. Induction for all new staff includes IG awareness. Audit of eSystems access currently underway.
Alison Graham
150 eHealth Security Insufficient IT security including physical and virus protection leading to possible denial of service with subsequent disruption to patient care, financial cost and reputational damage.
Network hardening exercise completed following Conficker virus outbreak New enhanced anti-virus protection installed with dedicated resource to monitor Memory Sticks monitoring in place New policies in place governing the use of memory sticks and other media by staff
John Wright
Information Governance Committee

ID Title Description Controls in place Director
178 Non - compliance with the Freedom of Information
Non-compliance with Freedom Of Information is a breach of the Act and may lead to potential ruling against NHS Ayrshire & Arran by the Information Commissioner
Protocol, policy and record keeping. We have a dedicated Freedom Of Information Officer with support within the Communications team to cover leave and illness. Regular reports to Information Governance and Directors as required.
John Burns
446 Infringement of Copyright Law by members of staff
Staff may copy,scan or otherwise reproduce items that are protected by the Copyright, Designs and Patents Act 1988
Notices placed beside photocopiers Guidance issued to staff outlining the NHS Scotland policy on copying
John Wright
506 Delays in, and the quality of, communication between primary and secondary care resulting in potential for harm
Current systems for communicating between primary and secondary care are suboptimal. GP colleagues have drawn attention to the poor quality of Immediate Discharge Letters and prescribing information. Also many Final Discharge Letters are never completed. Cardiology is particularly problematic but it is a widespread issue.
Current controls include the use of JAC HEPMA in the South, as a mechanism for IDLs and electronically produced drug summaries. Although not without its own problems, it is felt this system, if fully implemented in Ayrshire, would bring huge improvement in communication quality and timeliness.
Liz Moore

ID Title Description Controls in place Director
512 NHSGG&C Active Directory corruption incident occuring in NHS Ayrshire & Arran
Unknown root cause of IT incident in NHSGG&C relating to corruption of Microsoft Active Directory software and subsequent delay in routine recovery procedures
Current and up to date Active Directory recovery procedures which have been reviewed in light of NHSGG&C incident. Standby server prepared in event of need to perform an off network recovery. Existing backup policy in place includes 2 backups. Backup library for AD extended from 14 days to 30 days until root cause of NHSGG&C corruption is reported and fully understood. New hardware was procured for DNS system (the system which routes AD traffic) earlier this financial year and implementation of that hardware is underway. Update 3/12/13 - In addition further controls have been implemented which include staff to be supervised when performing AD tasks to reduce the risk of error, warning message implemented to warn staff that they are making a major AD change, full test restore successfully carried out. ADRAP arranged with Microsoft in January 2014.
John Wright
117 Financial deficit due to unbudgeted cost There is a risk that should equal pay claims be successful these are an unbudgeted cost leading to financial deficit
The Board is required to align with national approach to this financial and legal uncertainty. Equal Pay unit under CLO acts on behalf of all Boards.
Derek Lindsay
432 Insufficient annual funding allocation to address backlog maintenance/reduction in revenue funding and statutory compliance
Condition of premises are such that there is a risk of failure which could have an impact on business continuity and the provision of clinical services. Current estates budget allocation is insufficient to address backlog maintenance issues/statutory compliance and revenue funding.
Current budget allocated to premises/issues on a risk assessment basis. All other issues and costs are identified on the Estates Asset Management System (EAMS). Risk assessment and Justification detail attached.
John Wright
Performance Governance Committee

ID Title Description Controls in place Director
490 Public criticism by OSCR of how we spend endowment funds
Some historical practices around endowment funds are not in line with good practice for charities
New charter and operating procedure agreed by Endowment Trustees Endowment committee approves spend between £5K and £50K National guidance implemented locally.
Derek Lindsay
466 Failure of Disposal Programme achieve planned receipts for Capital developments such as NACH.
Properties on the A7AHB Disposal Programme have been identified where appropriate to be accrued against the North Ayrshire Community Hospital (NACH) within the Boards approved Capital Investment Plan. This means that any capital receipt derived from the sale of these premises will be directed back into the funding for the NACH Project. Currently there are eleven NHS properties with £8.7M of potential receipts attached to the NACH project. This income is expected to be split with £100k this financial year and the remaining due 2013/14. Due to current economic climate and failure of Banks to lend funds could result in not selling our properties or not receiving a good price in any sale
1. Property disposal strategy has recently been reviewed and updated. new agents appointed as to marketing. monitoring systems have been set up and are checked regularly. 2.Property Services are working with their agents to ensure the Board is best placed to achieve these sales. 3. Agents/advisers performance is being continually reviewed to ensure appropriate professional expertise is being procured. 4.Where sites are proving to be particularly challenging to market, Property Services have engaged with Scottish Futures Trust (SFT) and SGHSCD to seek additional funding that could be used to make the sites more marketable. 5.This new initiative is currently being developed with SFT's assistance with particular regard to Seafield House and the surplus land at Ayrshire Central, Irvine. The receipts from the sale of both premises are key to funding the NACH project. 6.Early discussions with SFT and SGHSCD to mitigate this risk by making properties more appealing to the market are already underway. 7.Independent expert advice from SFT has indicated that our Property Advisers are working well and that we are doing all that we can to achieve receipts.
John Wright

ID Title Description Controls in place Director
491 change fund investment does not result in a shift in the balance of care
Increasing elderly population results in demand on acute services and if new services introduced in the community do not reduce this then resources cannot be released from acute sector.
Targets associated with change fund include eliminating delayed discharges above 4 weeks then 2 weeks then altogether. Link investment in community services to planned bed closures to make them sustainable. Additional investment through LUCAP to reduce hospital admissions and provide more appropriate care.
Derek Lindsay
492 Efficiency savings signed up to are not then delivered
Delays in delivery of efficiency savings due to clinical/ staff/ public resistance which leaves a shortfall in efficiency savings programme for the year.
Monthly monitoring of efficiency savings, within directorate and by finance department CRES for 2013/14 mainly delivered
Derek Lindsay
493 A balanced budget cannot be set due insufficient efficiency savings identified
Increasingly difficult to release efficiency savings therefore identification of new savings before start of new financial year may not be sufficient to balance the budget.
Programme of service redesigns to deliver improvements. Monthly discussion at Corporate Management Team on progress on efficiency savings.
Derek Lindsay
494 Failing the legal Treatment Time Guarantee
Unable to find non-recurring funding to fund waiting list initiatives or private sector treatment.
DCAQ analysis to inform capacity and investment required. Using private sector in 2012/13 for orthopaedics catch up. Recurring funding provided for Orthopaedics. Other services covered by non-recurring funding.
Derek Lindsay
Staff Governance Committee

ID Title Description Controls in place Director
163 Failure of Building Utility Supplies and Services
Unforseen Failure of Electricity, Water or Gas leading to failure of Essential NHS Healthcare Building Infrastructure Utility Supplies and Services; Present the potential for the Organisation to fail to meet its corporate objectives. Encompassing the following risks:- 1. Service / Business interruption 2. Injury to patients/staff 3. Patient experience/outcome 4. Inspection/assessment/audit 5. Complaints/claims 6. Adverse publicity/reputation 7. Organisational/Personal security and equipment Estates Teams support the Board by carrying out the works, however, overall it’s an organisation wide risk.
Contingency plans for Utilities Power/Electricity, Gas and Water available by Sector Estates Teams. Risk assessment and Justification attached.
John Wright
219 Staff Health and numbers of staff absent from work due to ill health
Improvements in the health and wellbeing of staff are needed to support staff to have current and future healthy working lives. This will help to reduce the current high levels of sickness absence, which at times impacts on service delivery, quality of care and patient experience.
The Promoting Attendance project has been embedded within the new Staff Health Safety and Wellbeing Strategy. The HR and Partnership Leads have agreed a new Promoting Attendance and Wellbeing Policy and have developed a detailed action plan which focuses on long term absence and rehabilitation back to work and identifies interim milestones towards the national HEAT standard. Regular reporting on absence levels and progress against the action plan is given to the Health, Safety and Wellbeing Committee, the APF and Staff Governance Committee.
Patricia Leiser

ID Title Description Controls in place Director
417 Failure to comply with statutory regulations - Management of Occupational Road Risk
Failure to comply with the regulations could result in prosecution and adverse publicity.This includes car park management and access road management at the Board's main acute sites.
Legislation and Guidance provided by HSE. Local Policies and Procedures in place. Road risk action plan in place for the organisation as a whole. Crosshouse new traffic arrangements and traffic management plan now in place and workign well. A managed car parking scheme has been developed in partnership and approved by the Car Parking Policy Group and approved in principle by Corporate Management Team (CMT) subject to detailed implementation costs being developed amd submitted for approval in December 2013.
John Wright
308 Failure to comply with Fire Code Failure to have in place Fire Risk Assessments for all premises occupied by NHS Ayrshire & Arran, as required by the Fire (Scotland) Act 2005 and the Fire Safety (Scotland) Regulations 2006. Concerns raised as to Nominating officers being allocated for all bedded sites; training of 1/3 PARTIES ON OUR property/ in our facilities and their fire training; staff levels during out of hours periods and the impact upon local fire evacuation plans
Fire Risk Assessments which fulfill the necessary criteria have been undertaken in respect of 12 locations only (an additional 2 Risk Assessments are at present underway). With more than 80 premises within the Estates portfolio, the organization is currently in a position of statutory non-compliance in respect of more than 70 premises. Fire Safety Advisor group set up the oversee all board fire issues and to report to boards HAS Committee.
John Wright
ID Title Description Controls in place Director
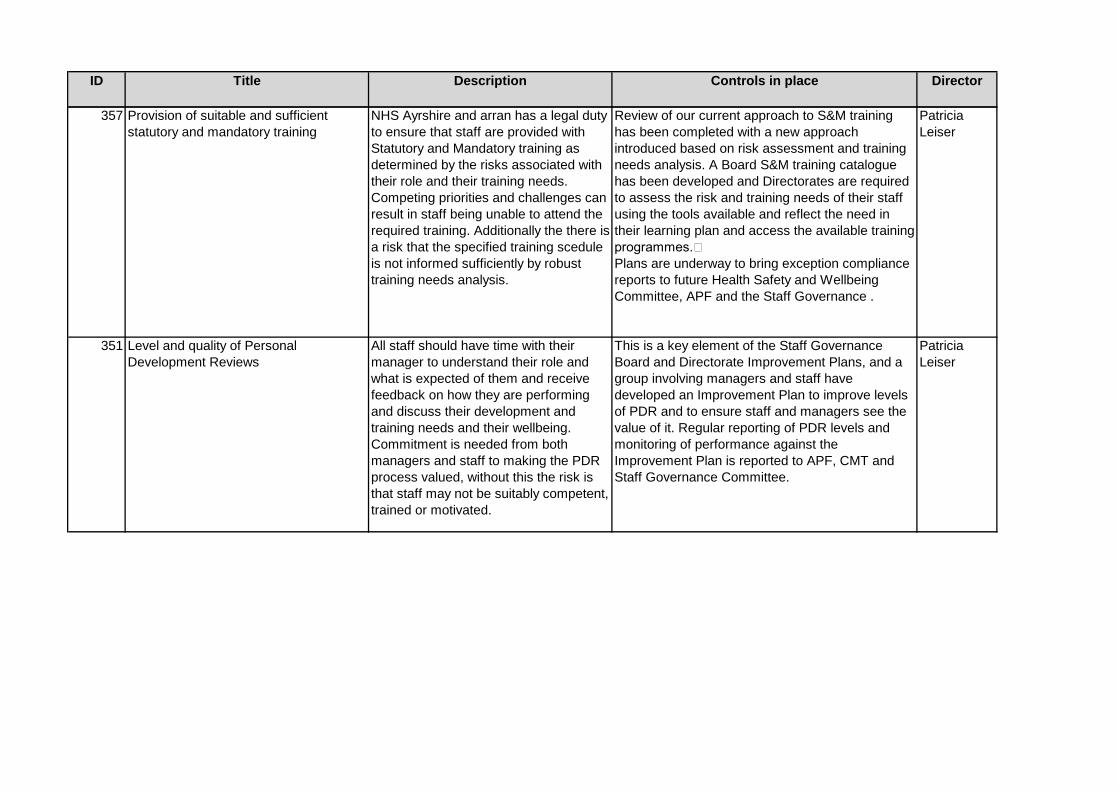
357 Provision of suitable and sufficient statutory and mandatory training
NHS Ayrshire and arran has a legal duty to ensure that staff are provided with Statutory and Mandatory training as determined by the risks associated with their role and their training needs. Competing priorities and challenges can result in staff being unable to attend the required training. Additionally the there is a risk that the specified training scedule is not informed sufficiently by robust training needs analysis.
Review of our current approach to S&M training has been completed with a new approach introduced based on risk assessment and training needs analysis. A Board S&M training catalogue has been developed and Directorates are required to assess the risk and training needs of their staff using the tools available and reflect the need in their learning plan and access the available training programmes. Plans are underway to bring exception compliance reports to future Health Safety and Wellbeing Committee, APF and the Staff Governance .
Patricia Leiser
351 Level and quality of Personal Development Reviews
All staff should have time with their manager to understand their role and what is expected of them and receive feedback on how they are performing and discuss their development and training needs and their wellbeing. Commitment is needed from both managers and staff to making the PDR process valued, without this the risk is that staff may not be suitably competent, trained or motivated.
This is a key element of the Staff Governance Board and Directorate Improvement Plans, and a group involving managers and staff have developed an Improvement Plan to improve levels of PDR and to ensure staff and managers see the value of it. Regular reporting of PDR levels and monitoring of performance against the Improvement Plan is reported to APF, CMT and Staff Governance Committee.
Patricia Leiser

Risk level (current)
Risk Owner
High risk Alison Graham
High risk Michele Caldwell

Risk level (current)
Risk Owner
Moderate risk
Carol Davidson

Risk level (current)
Risk Owner
High risk Alison Graham
High risk Alison Graham

Risk level (current)
Risk Owner
High risk Michele Caldwell
Moderate risk
Alison Graham
Moderate risk
John Wright

Risk level (current)
Risk Owner
Moderate risk
John Burns
Moderate risk
John Wright
High risk Liz Moore

Risk level (current)
Risk Owner
Moderate risk
John Wright
Moderate risk
Derek Lindsay
High risk John Wright

Risk level (current)
Risk Owner
Moderate risk
Derek Lindsay
High risk John Wright
Risk level (current)
Risk Owner
Moderate risk
Derek Lindsay
Moderate risk
Derek Lindsay
Moderate risk
Derek Lindsay
Moderate risk
Derek Lindsay

Risk level (current)
Risk Owner
Moderate risk
John Wright
VERYH Patricia Leiser

Risk level (current)
Risk Owner
Moderate risk
John Wright
High risk John Wright

Risk level (current)
Risk Owner
High risk Patricia Leiser
Moderate risk
Patricia Leiser