ics, College of Administrative Sciences and Economics ...alroth/papers/kidney.qje.pdforganized...
32
KIDNEY EXCHANGE* ALVIN E. ROTH TAYFUN SO ¨ NMEZ M. UTKU U ¨ NVER Most transplanted kidneys are from cadavers, but there are also many trans- plants from live donors. Recently, there have started to be kidney exchanges involving two donor-patient pairs such that each donor cannot give a kidney to the intended recipient because of immunological incompatibility, but each patient can receive a kidney from the other donor. Exchanges are also made in which a donor-patient pair makes a donation to someone waiting for a cadaver kidney, in return for the patient in the pair receiving high priority for a compatible cadaver kidney when one becomes available. There are stringent legal/ethical constraints on how exchanges can be conducted. We explore how larger scale exchanges of these kinds can be arranged efficiently and incentive compatibly, within existing constraints. The problem resembles some of the “housing” problems studied in the mechanism design literature for indivisible goods, with the novel feature that while live donor kidneys can be assigned simultaneously, cadaver kidneys cannot. In addition to studying the theoretical properties of the proposed kidney ex- change, we present simulation results suggesting that the welfare gains from larger scale exchange would be substantial, both in increased number of feasible live donation transplants, and in improved match quality of transplanted kidneys. I. INTRODUCTION Transplantation is the preferred treatment for the most se- rious forms of kidney disease. There are over 55,000 patients on the waiting list for cadaver kidneys in the United States, of whom almost 15,000 have been waiting more than three years. By way of comparison, in 2002 there were over 8,000 transplants of ca- daver kidneys performed in the United States. In the same year, * We thank Muriel Niederle, Erhan So ¨nmez, Stefanos Zenios, and the par- ticipants of the SITE 2003 Workshop on Matching Markets for their insightful comments and Hu ¨ seyin C ¸ ankaya for his help with the figures. After a first draft of this paper was completed, we also benefited from many helpful conversations with Dr. Frank Delmonico of the New England Organ Bank. So ¨nmez gratefully acknowledges the research support of Koc ¸Bank via the Koc ¸Bank scholar program and Turkish Academy of Sciences in the framework of the Young Scientist Award Program via grant TS/TU ¨ BA-GEBI ˙ P/2002-1-19. We also received support from a National Science Foundation grant through the National Bureau of Economic Research. All errors are our own responsibility. Email: [email protected]; address: Harvard University, Department of Econom- ics, Cambridge, MA 02138 and Harvard Business School, Boston, MA 02163. Email: [email protected]; address: Koc ¸ University, Department of Econom- ics, College of Administrative Sciences and Economics, Rumeli Feneri Yolu, Sarıyer, I ˙ stanbul, 34450, Turkey. Email: [email protected]; address: Koc ¸ University, Department of Econom- ics, College of Administrative Sciences and Economics, Rumeli Feneri Yolu, Sarıyer, I ˙ stanbul, 34450, Turkey. © 2004 by the President and Fellows of Harvard College and the Massachusetts Institute of Technology. The Quarterly Journal of Economics, May 2004 457
Transcript of ics, College of Administrative Sciences and Economics ...alroth/papers/kidney.qje.pdforganized...

KIDNEY EXCHANGE
ALVIN E ROTH
TAYFUN SONMEZ
M UTKU UNVER
Most transplanted kidneys are from cadavers but there are also many trans-plants from live donors Recently there have started to be kidney exchangesinvolving two donor-patient pairs such that each donor cannot give a kidney to theintended recipient because of immunological incompatibility but each patient canreceive a kidney from the other donor Exchanges are also made in which adonor-patient pair makes a donation to someone waiting for a cadaver kidney inreturn for the patient in the pair receiving high priority for a compatible cadaverkidney when one becomes available There are stringent legalethical constraintson how exchanges can be conducted We explore how larger scale exchanges ofthese kinds can be arranged efficiently and incentive compatibly within existingconstraints The problem resembles some of the ldquohousingrdquo problems studied in themechanism design literature for indivisible goods with the novel feature thatwhile live donor kidneys can be assigned simultaneously cadaver kidneys cannotIn addition to studying the theoretical properties of the proposed kidney ex-change we present simulation results suggesting that the welfare gains fromlarger scale exchange would be substantial both in increased number of feasiblelive donation transplants and in improved match quality of transplanted kidneys
I INTRODUCTION
Transplantation is the preferred treatment for the most se-rious forms of kidney disease There are over 55000 patients onthe waiting list for cadaver kidneys in the United States of whomalmost 15000 have been waiting more than three years By wayof comparison in 2002 there were over 8000 transplants of ca-daver kidneys performed in the United States In the same year
We thank Muriel Niederle Erhan Sonmez Stefanos Zenios and the par-ticipants of the SITE 2003 Workshop on Matching Markets for their insightfulcomments and Huseyin Cankaya for his help with the figures After a first draftof this paper was completed we also benefited from many helpful conversationswith Dr Frank Delmonico of the New England Organ Bank Sonmez gratefullyacknowledges the research support of KocBank via the KocBank scholar programand Turkish Academy of Sciences in the framework of the Young Scientist AwardProgram via grant TSTUBA-GEBIP2002-1-19 We also received support from aNational Science Foundation grant through the National Bureau of EconomicResearch All errors are our own responsibility
Email arothhbsedu address Harvard University Department of Econom-ics Cambridge MA 02138 and Harvard Business School Boston MA 02163
Email tsonmezkuedutr address Koc University Department of Econom-ics College of Administrative Sciences and Economics Rumeli Feneri YoluSarıyer Istanbul 34450 Turkey
Email uunverkuedutr address Koc University Department of Econom-ics College of Administrative Sciences and Economics Rumeli Feneri YoluSarıyer Istanbul 34450 Turkey
copy 2004 by the President and Fellows of Harvard College and the Massachusetts Institute ofTechnologyThe Quarterly Journal of Economics May 2004
457
about 3400 patients died while on the waiting list and another900 became too ill to be eligible for transplantation In addition totransplants of cadaver kidneys in 2002 there were also somewhatover 6000 transplants of kidneys from living donors a numberthat has been increasing steadily from year to year See Table I
There is thus a considerable shortage of kidneys comparedwith the demand However the substantial consensus in themedical community remains firmly opposed to allowing organsmdasheven cadaveric organsmdashto be bought and sold and this is a felonyunder the National Organ Transplant Act (NOTA) of 1984 andthe Uniform Anatomical Gift Act of 19871 The present paperconsiders ways to alleviate this shortage and improve patientwelfare within the constraints of the current social and legalenvironment
The National Organ Transplant Act of 1984 established theOrgan Procurement and Transplantation Network (OPTN) Run
1 There is however a steady stream of literature both by doctors and byeconomists considering how the shortage of organs might be alleviated by allow-ing their purchase and sale and what effects this might have See eg Nelson etal [1993] for an argument in favor of the status quo and eg Becker and Elias[2002] for an argument in favor of a market Recent Congressional testimonyendorsing the status quo but suggesting that empirical investigation of financialincentives might be in order can be found in Sade [2003]
TABLE IU S KIDNEY TRANSPLANTS
YearCadaveric
donorsCadaveric
transplantsLive
donorsAll wait-list
patientsNew wait-list
additions
1992 4276 7202 2535 22063 152241993 4609 7509 2851 24765 160901994 4797 7638 3009 27258 165381995 5003 7690 3377 30590 179031996 5038 7726 3649 34000 183281997 5083 7769 3912 37438 190671998 5339 8017 4361 40931 201911999 5386 8023 4552 43867 209862000 5490 8089 5324 47596 222692001 5528 8202 5924 51144 223492002 5630 8534 6233 54844 23494
The data for years 1992ndash2001 are constructed from the annual report of UNOSOPTN the data for 2002are constructed from the national database of UNOSOPTN National database numbers are slightly higherthan the annual report numbers due to continuous updating regarding previous years Number of registra-tions may have multiple counts of patients since one patient may have registered in multiple centers for thewait-list
458 QUARTERLY JOURNAL OF ECONOMICS
by the United Network for Organ Sharing (UNOS) it has devel-oped a centralized priority mechanism for the allocation of cadav-eric kidneys
Transplants from live donors generally have a higher chanceof success than those from cadavers The way such transplantsare typically arranged is that a patient identifies a healthy will-ing donor (a spouse for example) and if the transplant is feasibleon medical grounds it is carried out If the transplant from thewilling donor is not feasible the patient typically enters (or re-mains on) the queue for a cadaver kidney while the donor returnshome
Recently however in a small number of cases additionalpossibilities have been utilized when a transplant from a livedonor and the intended recipient is infeasible One of these calleda paired exchange involves two patient-donor couples for each ofwhom a transplant from donor to intended recipient is infeasiblebut such that the patient in each couple could feasibly receive atransplant from the donor in the other couple [Rapaport 1986Ross et al 1997] This pair of couples can then exchange donatedkidneys Compared with receiving cadaver kidneys at an un-known future time this improves the welfare of the patients Inaddition it relieves the demand on the supply of cadaver kidneysand thus potentially improves the welfare of those patients on thecadaver queue A small number of these two-couple operationshave been done and the transplantation community has issued aconsensus statement declaring them to be ethically acceptable[Abecassis et al 2000]2
Another possibility is an indirect exchange (or list exchange)involving an exchange between one incompatible patient-donorcouple and the cadaver queue [Ross and Woodle 2000] In thiskind of exchange the patient in the couple receives high priorityon the cadaver queue in return for the donation of his donorrsquoskidney to someone on the queue3 This improves the welfare ofthe patient in the couple compared with having a long wait for asuitable cadaver kidney and it benefits the recipient of the live
2 UNOS also published a legal opinion that such exchanges do not violatethe NOTA (httpwwwastsorgezefilesUNOSSection_301_NOTA_pdf)
3 Priority on the cadaver queue is actually a bit complex as queues areorganized regionally and consist of multiple queues on which priority is deter-mined by a scoring rule that gives points for how well matched the availablekidney is to each patient how long the patient has been waiting etc Giving highpriority on the queue could be implemented by giving an appropriate number ofpoints in the scoring rule
459KIDNEY EXCHANGE
kidney and others on the queue who benefit from the increase inkidney supply due to an additional living donor However Rossand Woodle note that this may have a negative impact on type Opatients already on the cadaver queue an issue studied by Ze-nios Woodle and Ross [2001] to which we shall return
In contrast to the system for cadaveric organs and despitethe growing interest in at least small-scale exchanges involvingliving donors there is no national system or even an organizedregistry at any level for managing exchanges of kidneys from livedonors However individual hospitals are beginning to thinkabout larger scale living donor exchanges As this paper wasbeing written the first three-couple kidney transplant exchangein the United States was reported at Johns Hopkins Comprehen-sive Transplant Center in Baltimore among three couples forwhom no two-couple transfer was feasible [Olson August 22003] In the present paper we will consider how such a system ofexchanges might be organized from the point of view of achievingefficiency and providing consistent incentives to patients donorsand doctors and what its welfare implications might be We willsee that the benefits of wider exchange accrue not only to theparties to the exchange The resulting increase in live organdonation also benefits patients waiting for cadaver kidneys in-cluding type O patients The design we propose is partly inspiredby the mechanism design literature on ldquohouse allocationrdquo and isintended to build on and complement the existing practices inkidney transplantation In this respect and others it is in themodern tradition of engineering economics (see Roth [2002]) asapplied to other problems of allocation such as labor marketclearinghouses (see Roth and Peranson [1999]) or auctions (seeMilgrom [2004]) in which practical implementation often in-volves incremental change in existing practices
II BACKGROUND
IIA Kidney Transplantation
End Stage Renal Disease (ESRD) is a fatal disease unlesstreated with dialysis or kidney transplantation Transplantationis the preferred treatment Two genetic characteristics play keyroles in the feasibility and success of a kidney transplant Thefirst is the ABO blood-type There are four blood types A B ABand O Absent other complications type O kidneys can be trans-
460 QUARTERLY JOURNAL OF ECONOMICS
planted into any patient type A or type B kidneys can be trans-planted into same type or type AB patients and type AB kidneyscan only be transplanted into type AB patients (So type O pa-tients can only receive type O kidneys) The second genetic char-acteristic is tissue type also known as HLA type HLA type is acombination of six proteins As the HLA mismatch between thedonor and the recipient increases the likelihood of graft (ietransplanted organ) survival decreases [Opelz 1997] HLA playsanother key role in transplantation through the pretransplantldquocrossmatchrdquo test Prior to transplantation the potential recipi-ent is tested for the presence of preformed antibodies againstHLA in the donor kidney The presence of antibodies called apositive crossmatch effectively rules out transplantation
When a cadaveric kidney becomes available for transplanta-tion the priority of each patient on the waiting list is determinedby a point system based on factors including the blood type HLAantigen-match time spent on the waiting list the region thekidney is harvested etc and the kidney is offered to the patientwith the highest priority If that patient declines the kidney isoffered to the patient with the next highest priority and so onLiving donor kidney grafts have superior survival rates (and theiravailability can also avoid the long waiting time for a cadaverkidney) However potential living donors can be eliminated fromconsideration due to incompatibility of the potential donor kidneywith the intended recipient
To minimize the elimination of physically eligible volunteerkidney donors on the basis of immunologic incompatibilities Ra-paport [1986] proposed the creation of a living donor pool forpaired exchange Ross et al [1997] again proposed to increase thesupply of living kidney donations by using kidneys from livingincompatible donors through an exchange arrangement betweentwo pairs In 2000 UNOS initiated pilot testing of such programs
Another exchange program is the indirect exchange program[Ross and Woodle 2000] a potential donor who is incompatiblewith his intended recipient donates his kidney to the cadavericwaiting list and his paired recipient will receive priority for thenext compatible cadaveric kidney There is widespread agree-ment in the transplantation community that indirect exchangecan harm type O patients who have no living donors First theywill be losing their priority to type O patients whose incompatibledonors donate to the cadaveric pool and second very few type Oliving kidneys will be offered to their pool since a type O donor can
461KIDNEY EXCHANGE
directly donate to his intended recipient unless there is a positivecrossmatch Despite this widespread concern many transplantcenters have also cautiously started pilot indirect exchange pro-grams since 2000 For example in UNOS Region 1 (New En-gland) consisting of fourteen transplant centers and two OrganProcurement Organizations four paired exchanges and seven-teen indirect exchanges have been conducted from 2001 through2003 (personal communication)
IIB Mechanism Design
We will extend results in the mechanism design literaturewhich we first quickly review Shapley and Scarf [1974] modeleda ldquohousing marketrdquo consisting of n agents each of whom is en-dowed with an indivisible good a ldquohouserdquo Each agent has pref-erences over all the houses and there is no money in the markettrade is feasible only in houses They attribute to David Gale theldquotop trading cyclerdquo algorithm that produces a house allocation inthe core of the market The algorithm works as follows eachagent points to her most preferred house (and each house pointsto its owner) There is at least one cycle in the resulting directedgraph In each such cycle the corresponding trades are carriedout ie each agent in the cycle receives the house she is pointingto and these agents and houses are removed from the marketThe process continues (with each agent pointing to her mostpreferred house that remains on the market) until no agentsremain and the final allocation is the one in which each agentreceives the house with which she left the market When allpreferences are strict the procedure yields a unique outcome[Roth and Postlewaite 1977] and truthful preference revelation isa dominant strategy [Roth 1982]
Note that paired kidney exchanges similarly seek the gainsfrom trade among patients with willing donors but (with therecent Johns Hopkins three-pair exchange being a notable excep-tion) mostly among just two pairs In the kidney exchange to beconsidered below if we consider exchange only among patientswith donors the properties of the housing market model essen-tially carry over unchanged if we assume that donorsrsquo prefer-ences are aligned with those of their intended recipient We willalso assume that all surgeries in a given cycle are carried outsimultaneously which is the current practice since a donorrsquoswillingness to donate a kidney might change once her intendedrecipient received a transplant
462 QUARTERLY JOURNAL OF ECONOMICS
However the kidney transplant environment consists notjust of patients with donors but also patients without donors andcadaver kidneys not tied to any specific patient Abdulkadirogluand Sonmez [1999] studied housing allocation on college cam-puses which is in some respects similar a set of rooms must beallocated to a set of students by a centralized housing office Someof the students are existing tenants each of whom already occu-pies a room and the rest of the students are newcomers Inaddition to occupied rooms there are vacant rooms Existingtenants are entitled to keep their current rooms but may alsoapply for other rooms Mechanisms used on a number of collegecampuses do not ensure the participation of existing tenants andresult in efficiency loss This is the motivation for the generali-zation of the top trading cycles (TTC) mechanism proposed byAbdulkadiroglu and Sonmez [1999] which they called you requestmy housemdashI get your turn (YRMH-IGYT) each student reportshis strict preferences over all rooms and an ordering of agents israndomly chosen For any given preference list and ordering theoutcome is obtained as follows (1) Assign the first student his topchoice the second student his top choice among the remainingrooms and so on until someone requests the room of an existingtenant who is yet to be served (2) Whenever that happens modifythe remainder of the ordering by moving the existing tenant to thebeginning of the line and proceed with the procedure (3) If at anypoint a cycle forms it is formed exclusively by existing tenantsand each of them requests the room of the tenant who is next inthe cycle In such cases remove all students in the cycle byassigning them the rooms they request and proceed with theprocedure The key innovation here is that an existing tenantwhose current room is requested is upgraded to the first place inthe line of agents remaining unassigned before his room is allo-cated As a result the YRMH-IGYT mechanism assures everyexisting tenant a room that is no worse than his own Thereforeexisting tenants do not have any reason not to enter the marketand consequently the eventual allocation is Pareto efficient Notethat the idea of upgrading an existing tenant whose current roomis requested to the top of the line was also invented by the trans-plantation community in the form of an indirect exchange pro-gram when a potential donor donates his kidney to the highestpriority patient on the waiting list his intended recipient isupgraded to the top of the waiting list
Note again that what prompted the introduction of simple
463KIDNEY EXCHANGE
kidney exchange programs was the loss of volunteer kidney do-nors because of immunologic incompatibilities Under these ex-change programs a potential donor who is incompatible with hisintended recipient is given the incentive to go ahead with thedonation because his donation makes it possible for his intendedrecipient to receive a compatible kidney Similarly the potentialefficiency loss in the campus housing problem is that some roomsmight fail to be traded even when welfare-enhancing trades arepossible The YRMH-IGYT is an attempt to address that problemin the housing context We next consider how it must be adaptedto kidney exchange
III KIDNEY EXCHANGE AND THE TOP TRADING CYCLES
AND CHAINS (TTCC) MECHANISM
While there are clear similarities between house allocationand kidney exchange there are also important differences Thecounterpart of an existing tenant and his room is a donor-recipi-ent pair which we denote by (kiti) We will often refer to donorki as kidney ki and recipient ti as patient ti In the context ofhouse allocation with existing tenants there are also newcomersnone of whom owns a specific house and vacant houses none ofwhich is owned by a specific student The counterpart of newcom-ers are patients who have no living donors and the counterpart ofvacant houses are cadaveric kidneys that are not targeted forspecific patients This analogy reveals one important differencebetween the two models in the house allocation model the set ofvacant houses is known In the kidney exchange problem it is notclear which cadaveric kidneys will be available when they will beavailable etc Therefore while occupied houses and vacant housesare simultaneously allocated under the YRMH-IGYT mechanismthis is not possible in the context of kidney exchange Insteadpatients with live donors who are not themselves allocated a livedonor kidney will be assigned to the cadaver queue (with a pri-ority reflecting whether their donorrsquos kidney was donated tosomeone on the queue)
Let K denote the set of living donor kidneys at a particulartime While patients and their doctors may define their prefer-ences over kidneys as they wish here we consider for specificitythe preferences that come from maximizing the probability of asuccessful transplant Given any patient part of K is outside thefeasible set due to ABO blood-type incompatibility or a positive
464 QUARTERLY JOURNAL OF ECONOMICS
crossmatch Among feasible kidneys HLA match [Opelz 1997]donor age kidney size etc play a significant role in the graftsurvival Therefore patients have heterogeneous preferences overcompatible kidneys In what follows we will consider all prefer-ences to be strict If only direct exchanges among donor-recipientpairs are considered one can directly use Galersquos Top TradingCycles mechanism However this will not allow for indirectexchanges We will need to modify the model and the mecha-nism to allow for this possibility Since the supply of specificcadaveric donor kidneys is not predictable a patient whowishes to trade his donorrsquos kidney in return for a priority in thecadaveric kidney waiting list is receiving a lottery Taking thisinto consideration the patient doctor and donor can decidewhether this option is acceptable and if so where it ranks inthe patientrsquos preferences
Given a patient ti let Ki K denote the set of living donorkidneys that are compatible with patient ti Let w denote theoption of entering the waiting list with priority reflecting thedonation of his donorrsquos kidney ki and Pi denote his strict prefer-ences over Ki kiw For our purposes the relevant part of Pi
is the ranking up to kidney ki or w whichever ranks higher Ifpatient ti ranks kidney ki at the top of his preferences thatmeans he and his donor do not wish to participate in an exchangeIf patient ti ranks ki on top of w that means he and his donor donot consider exchanging kidney ki with a priority in the cadaverickidney waiting list
We can now formalize a (static) kidney exchange problemconsisting of a set of donor-recipient pairs (k1t1) (kntn)a set of compatible kidneys Ki K k1 kn for eachpatient ti and a strict preference relation Pi over Ki kiw foreach patient ti The outcome of a kidney exchange problem is amatching of kidneyswait-list option to patients such that eachpatient ti is either assigned a kidney in Ki ki or the wait-listoption w and no kidney can be assigned to more than one patientalthough the wait-list option w can be assigned to several pa-tients A kidney exchange mechanism selects a matching for eachkidney exchange problem We are almost ready to introduce theTop Trading Cycles and Chains (TTCC) mechanism a generali-zation of the TTC mechanism for kidney exchange First we givea few definitions and observations to facilitate the description ofthe mechanism
465KIDNEY EXCHANGE
IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
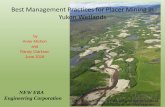
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

about 3400 patients died while on the waiting list and another900 became too ill to be eligible for transplantation In addition totransplants of cadaver kidneys in 2002 there were also somewhatover 6000 transplants of kidneys from living donors a numberthat has been increasing steadily from year to year See Table I
There is thus a considerable shortage of kidneys comparedwith the demand However the substantial consensus in themedical community remains firmly opposed to allowing organsmdasheven cadaveric organsmdashto be bought and sold and this is a felonyunder the National Organ Transplant Act (NOTA) of 1984 andthe Uniform Anatomical Gift Act of 19871 The present paperconsiders ways to alleviate this shortage and improve patientwelfare within the constraints of the current social and legalenvironment
The National Organ Transplant Act of 1984 established theOrgan Procurement and Transplantation Network (OPTN) Run
1 There is however a steady stream of literature both by doctors and byeconomists considering how the shortage of organs might be alleviated by allow-ing their purchase and sale and what effects this might have See eg Nelson etal [1993] for an argument in favor of the status quo and eg Becker and Elias[2002] for an argument in favor of a market Recent Congressional testimonyendorsing the status quo but suggesting that empirical investigation of financialincentives might be in order can be found in Sade [2003]
TABLE IU S KIDNEY TRANSPLANTS
YearCadaveric
donorsCadaveric
transplantsLive
donorsAll wait-list
patientsNew wait-list
additions
1992 4276 7202 2535 22063 152241993 4609 7509 2851 24765 160901994 4797 7638 3009 27258 165381995 5003 7690 3377 30590 179031996 5038 7726 3649 34000 183281997 5083 7769 3912 37438 190671998 5339 8017 4361 40931 201911999 5386 8023 4552 43867 209862000 5490 8089 5324 47596 222692001 5528 8202 5924 51144 223492002 5630 8534 6233 54844 23494
The data for years 1992ndash2001 are constructed from the annual report of UNOSOPTN the data for 2002are constructed from the national database of UNOSOPTN National database numbers are slightly higherthan the annual report numbers due to continuous updating regarding previous years Number of registra-tions may have multiple counts of patients since one patient may have registered in multiple centers for thewait-list
458 QUARTERLY JOURNAL OF ECONOMICS
by the United Network for Organ Sharing (UNOS) it has devel-oped a centralized priority mechanism for the allocation of cadav-eric kidneys
Transplants from live donors generally have a higher chanceof success than those from cadavers The way such transplantsare typically arranged is that a patient identifies a healthy will-ing donor (a spouse for example) and if the transplant is feasibleon medical grounds it is carried out If the transplant from thewilling donor is not feasible the patient typically enters (or re-mains on) the queue for a cadaver kidney while the donor returnshome
Recently however in a small number of cases additionalpossibilities have been utilized when a transplant from a livedonor and the intended recipient is infeasible One of these calleda paired exchange involves two patient-donor couples for each ofwhom a transplant from donor to intended recipient is infeasiblebut such that the patient in each couple could feasibly receive atransplant from the donor in the other couple [Rapaport 1986Ross et al 1997] This pair of couples can then exchange donatedkidneys Compared with receiving cadaver kidneys at an un-known future time this improves the welfare of the patients Inaddition it relieves the demand on the supply of cadaver kidneysand thus potentially improves the welfare of those patients on thecadaver queue A small number of these two-couple operationshave been done and the transplantation community has issued aconsensus statement declaring them to be ethically acceptable[Abecassis et al 2000]2
Another possibility is an indirect exchange (or list exchange)involving an exchange between one incompatible patient-donorcouple and the cadaver queue [Ross and Woodle 2000] In thiskind of exchange the patient in the couple receives high priorityon the cadaver queue in return for the donation of his donorrsquoskidney to someone on the queue3 This improves the welfare ofthe patient in the couple compared with having a long wait for asuitable cadaver kidney and it benefits the recipient of the live
2 UNOS also published a legal opinion that such exchanges do not violatethe NOTA (httpwwwastsorgezefilesUNOSSection_301_NOTA_pdf)
3 Priority on the cadaver queue is actually a bit complex as queues areorganized regionally and consist of multiple queues on which priority is deter-mined by a scoring rule that gives points for how well matched the availablekidney is to each patient how long the patient has been waiting etc Giving highpriority on the queue could be implemented by giving an appropriate number ofpoints in the scoring rule
459KIDNEY EXCHANGE
kidney and others on the queue who benefit from the increase inkidney supply due to an additional living donor However Rossand Woodle note that this may have a negative impact on type Opatients already on the cadaver queue an issue studied by Ze-nios Woodle and Ross [2001] to which we shall return
In contrast to the system for cadaveric organs and despitethe growing interest in at least small-scale exchanges involvingliving donors there is no national system or even an organizedregistry at any level for managing exchanges of kidneys from livedonors However individual hospitals are beginning to thinkabout larger scale living donor exchanges As this paper wasbeing written the first three-couple kidney transplant exchangein the United States was reported at Johns Hopkins Comprehen-sive Transplant Center in Baltimore among three couples forwhom no two-couple transfer was feasible [Olson August 22003] In the present paper we will consider how such a system ofexchanges might be organized from the point of view of achievingefficiency and providing consistent incentives to patients donorsand doctors and what its welfare implications might be We willsee that the benefits of wider exchange accrue not only to theparties to the exchange The resulting increase in live organdonation also benefits patients waiting for cadaver kidneys in-cluding type O patients The design we propose is partly inspiredby the mechanism design literature on ldquohouse allocationrdquo and isintended to build on and complement the existing practices inkidney transplantation In this respect and others it is in themodern tradition of engineering economics (see Roth [2002]) asapplied to other problems of allocation such as labor marketclearinghouses (see Roth and Peranson [1999]) or auctions (seeMilgrom [2004]) in which practical implementation often in-volves incremental change in existing practices
II BACKGROUND
IIA Kidney Transplantation
End Stage Renal Disease (ESRD) is a fatal disease unlesstreated with dialysis or kidney transplantation Transplantationis the preferred treatment Two genetic characteristics play keyroles in the feasibility and success of a kidney transplant Thefirst is the ABO blood-type There are four blood types A B ABand O Absent other complications type O kidneys can be trans-
460 QUARTERLY JOURNAL OF ECONOMICS
planted into any patient type A or type B kidneys can be trans-planted into same type or type AB patients and type AB kidneyscan only be transplanted into type AB patients (So type O pa-tients can only receive type O kidneys) The second genetic char-acteristic is tissue type also known as HLA type HLA type is acombination of six proteins As the HLA mismatch between thedonor and the recipient increases the likelihood of graft (ietransplanted organ) survival decreases [Opelz 1997] HLA playsanother key role in transplantation through the pretransplantldquocrossmatchrdquo test Prior to transplantation the potential recipi-ent is tested for the presence of preformed antibodies againstHLA in the donor kidney The presence of antibodies called apositive crossmatch effectively rules out transplantation
When a cadaveric kidney becomes available for transplanta-tion the priority of each patient on the waiting list is determinedby a point system based on factors including the blood type HLAantigen-match time spent on the waiting list the region thekidney is harvested etc and the kidney is offered to the patientwith the highest priority If that patient declines the kidney isoffered to the patient with the next highest priority and so onLiving donor kidney grafts have superior survival rates (and theiravailability can also avoid the long waiting time for a cadaverkidney) However potential living donors can be eliminated fromconsideration due to incompatibility of the potential donor kidneywith the intended recipient
To minimize the elimination of physically eligible volunteerkidney donors on the basis of immunologic incompatibilities Ra-paport [1986] proposed the creation of a living donor pool forpaired exchange Ross et al [1997] again proposed to increase thesupply of living kidney donations by using kidneys from livingincompatible donors through an exchange arrangement betweentwo pairs In 2000 UNOS initiated pilot testing of such programs
Another exchange program is the indirect exchange program[Ross and Woodle 2000] a potential donor who is incompatiblewith his intended recipient donates his kidney to the cadavericwaiting list and his paired recipient will receive priority for thenext compatible cadaveric kidney There is widespread agree-ment in the transplantation community that indirect exchangecan harm type O patients who have no living donors First theywill be losing their priority to type O patients whose incompatibledonors donate to the cadaveric pool and second very few type Oliving kidneys will be offered to their pool since a type O donor can
461KIDNEY EXCHANGE
directly donate to his intended recipient unless there is a positivecrossmatch Despite this widespread concern many transplantcenters have also cautiously started pilot indirect exchange pro-grams since 2000 For example in UNOS Region 1 (New En-gland) consisting of fourteen transplant centers and two OrganProcurement Organizations four paired exchanges and seven-teen indirect exchanges have been conducted from 2001 through2003 (personal communication)
IIB Mechanism Design
We will extend results in the mechanism design literaturewhich we first quickly review Shapley and Scarf [1974] modeleda ldquohousing marketrdquo consisting of n agents each of whom is en-dowed with an indivisible good a ldquohouserdquo Each agent has pref-erences over all the houses and there is no money in the markettrade is feasible only in houses They attribute to David Gale theldquotop trading cyclerdquo algorithm that produces a house allocation inthe core of the market The algorithm works as follows eachagent points to her most preferred house (and each house pointsto its owner) There is at least one cycle in the resulting directedgraph In each such cycle the corresponding trades are carriedout ie each agent in the cycle receives the house she is pointingto and these agents and houses are removed from the marketThe process continues (with each agent pointing to her mostpreferred house that remains on the market) until no agentsremain and the final allocation is the one in which each agentreceives the house with which she left the market When allpreferences are strict the procedure yields a unique outcome[Roth and Postlewaite 1977] and truthful preference revelation isa dominant strategy [Roth 1982]
Note that paired kidney exchanges similarly seek the gainsfrom trade among patients with willing donors but (with therecent Johns Hopkins three-pair exchange being a notable excep-tion) mostly among just two pairs In the kidney exchange to beconsidered below if we consider exchange only among patientswith donors the properties of the housing market model essen-tially carry over unchanged if we assume that donorsrsquo prefer-ences are aligned with those of their intended recipient We willalso assume that all surgeries in a given cycle are carried outsimultaneously which is the current practice since a donorrsquoswillingness to donate a kidney might change once her intendedrecipient received a transplant
462 QUARTERLY JOURNAL OF ECONOMICS
However the kidney transplant environment consists notjust of patients with donors but also patients without donors andcadaver kidneys not tied to any specific patient Abdulkadirogluand Sonmez [1999] studied housing allocation on college cam-puses which is in some respects similar a set of rooms must beallocated to a set of students by a centralized housing office Someof the students are existing tenants each of whom already occu-pies a room and the rest of the students are newcomers Inaddition to occupied rooms there are vacant rooms Existingtenants are entitled to keep their current rooms but may alsoapply for other rooms Mechanisms used on a number of collegecampuses do not ensure the participation of existing tenants andresult in efficiency loss This is the motivation for the generali-zation of the top trading cycles (TTC) mechanism proposed byAbdulkadiroglu and Sonmez [1999] which they called you requestmy housemdashI get your turn (YRMH-IGYT) each student reportshis strict preferences over all rooms and an ordering of agents israndomly chosen For any given preference list and ordering theoutcome is obtained as follows (1) Assign the first student his topchoice the second student his top choice among the remainingrooms and so on until someone requests the room of an existingtenant who is yet to be served (2) Whenever that happens modifythe remainder of the ordering by moving the existing tenant to thebeginning of the line and proceed with the procedure (3) If at anypoint a cycle forms it is formed exclusively by existing tenantsand each of them requests the room of the tenant who is next inthe cycle In such cases remove all students in the cycle byassigning them the rooms they request and proceed with theprocedure The key innovation here is that an existing tenantwhose current room is requested is upgraded to the first place inthe line of agents remaining unassigned before his room is allo-cated As a result the YRMH-IGYT mechanism assures everyexisting tenant a room that is no worse than his own Thereforeexisting tenants do not have any reason not to enter the marketand consequently the eventual allocation is Pareto efficient Notethat the idea of upgrading an existing tenant whose current roomis requested to the top of the line was also invented by the trans-plantation community in the form of an indirect exchange pro-gram when a potential donor donates his kidney to the highestpriority patient on the waiting list his intended recipient isupgraded to the top of the waiting list
Note again that what prompted the introduction of simple
463KIDNEY EXCHANGE
kidney exchange programs was the loss of volunteer kidney do-nors because of immunologic incompatibilities Under these ex-change programs a potential donor who is incompatible with hisintended recipient is given the incentive to go ahead with thedonation because his donation makes it possible for his intendedrecipient to receive a compatible kidney Similarly the potentialefficiency loss in the campus housing problem is that some roomsmight fail to be traded even when welfare-enhancing trades arepossible The YRMH-IGYT is an attempt to address that problemin the housing context We next consider how it must be adaptedto kidney exchange
III KIDNEY EXCHANGE AND THE TOP TRADING CYCLES
AND CHAINS (TTCC) MECHANISM
While there are clear similarities between house allocationand kidney exchange there are also important differences Thecounterpart of an existing tenant and his room is a donor-recipi-ent pair which we denote by (kiti) We will often refer to donorki as kidney ki and recipient ti as patient ti In the context ofhouse allocation with existing tenants there are also newcomersnone of whom owns a specific house and vacant houses none ofwhich is owned by a specific student The counterpart of newcom-ers are patients who have no living donors and the counterpart ofvacant houses are cadaveric kidneys that are not targeted forspecific patients This analogy reveals one important differencebetween the two models in the house allocation model the set ofvacant houses is known In the kidney exchange problem it is notclear which cadaveric kidneys will be available when they will beavailable etc Therefore while occupied houses and vacant housesare simultaneously allocated under the YRMH-IGYT mechanismthis is not possible in the context of kidney exchange Insteadpatients with live donors who are not themselves allocated a livedonor kidney will be assigned to the cadaver queue (with a pri-ority reflecting whether their donorrsquos kidney was donated tosomeone on the queue)
Let K denote the set of living donor kidneys at a particulartime While patients and their doctors may define their prefer-ences over kidneys as they wish here we consider for specificitythe preferences that come from maximizing the probability of asuccessful transplant Given any patient part of K is outside thefeasible set due to ABO blood-type incompatibility or a positive
464 QUARTERLY JOURNAL OF ECONOMICS
crossmatch Among feasible kidneys HLA match [Opelz 1997]donor age kidney size etc play a significant role in the graftsurvival Therefore patients have heterogeneous preferences overcompatible kidneys In what follows we will consider all prefer-ences to be strict If only direct exchanges among donor-recipientpairs are considered one can directly use Galersquos Top TradingCycles mechanism However this will not allow for indirectexchanges We will need to modify the model and the mecha-nism to allow for this possibility Since the supply of specificcadaveric donor kidneys is not predictable a patient whowishes to trade his donorrsquos kidney in return for a priority in thecadaveric kidney waiting list is receiving a lottery Taking thisinto consideration the patient doctor and donor can decidewhether this option is acceptable and if so where it ranks inthe patientrsquos preferences
Given a patient ti let Ki K denote the set of living donorkidneys that are compatible with patient ti Let w denote theoption of entering the waiting list with priority reflecting thedonation of his donorrsquos kidney ki and Pi denote his strict prefer-ences over Ki kiw For our purposes the relevant part of Pi
is the ranking up to kidney ki or w whichever ranks higher Ifpatient ti ranks kidney ki at the top of his preferences thatmeans he and his donor do not wish to participate in an exchangeIf patient ti ranks ki on top of w that means he and his donor donot consider exchanging kidney ki with a priority in the cadaverickidney waiting list
We can now formalize a (static) kidney exchange problemconsisting of a set of donor-recipient pairs (k1t1) (kntn)a set of compatible kidneys Ki K k1 kn for eachpatient ti and a strict preference relation Pi over Ki kiw foreach patient ti The outcome of a kidney exchange problem is amatching of kidneyswait-list option to patients such that eachpatient ti is either assigned a kidney in Ki ki or the wait-listoption w and no kidney can be assigned to more than one patientalthough the wait-list option w can be assigned to several pa-tients A kidney exchange mechanism selects a matching for eachkidney exchange problem We are almost ready to introduce theTop Trading Cycles and Chains (TTCC) mechanism a generali-zation of the TTC mechanism for kidney exchange First we givea few definitions and observations to facilitate the description ofthe mechanism
465KIDNEY EXCHANGE
IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

by the United Network for Organ Sharing (UNOS) it has devel-oped a centralized priority mechanism for the allocation of cadav-eric kidneys
Transplants from live donors generally have a higher chanceof success than those from cadavers The way such transplantsare typically arranged is that a patient identifies a healthy will-ing donor (a spouse for example) and if the transplant is feasibleon medical grounds it is carried out If the transplant from thewilling donor is not feasible the patient typically enters (or re-mains on) the queue for a cadaver kidney while the donor returnshome
Recently however in a small number of cases additionalpossibilities have been utilized when a transplant from a livedonor and the intended recipient is infeasible One of these calleda paired exchange involves two patient-donor couples for each ofwhom a transplant from donor to intended recipient is infeasiblebut such that the patient in each couple could feasibly receive atransplant from the donor in the other couple [Rapaport 1986Ross et al 1997] This pair of couples can then exchange donatedkidneys Compared with receiving cadaver kidneys at an un-known future time this improves the welfare of the patients Inaddition it relieves the demand on the supply of cadaver kidneysand thus potentially improves the welfare of those patients on thecadaver queue A small number of these two-couple operationshave been done and the transplantation community has issued aconsensus statement declaring them to be ethically acceptable[Abecassis et al 2000]2
Another possibility is an indirect exchange (or list exchange)involving an exchange between one incompatible patient-donorcouple and the cadaver queue [Ross and Woodle 2000] In thiskind of exchange the patient in the couple receives high priorityon the cadaver queue in return for the donation of his donorrsquoskidney to someone on the queue3 This improves the welfare ofthe patient in the couple compared with having a long wait for asuitable cadaver kidney and it benefits the recipient of the live
2 UNOS also published a legal opinion that such exchanges do not violatethe NOTA (httpwwwastsorgezefilesUNOSSection_301_NOTA_pdf)
3 Priority on the cadaver queue is actually a bit complex as queues areorganized regionally and consist of multiple queues on which priority is deter-mined by a scoring rule that gives points for how well matched the availablekidney is to each patient how long the patient has been waiting etc Giving highpriority on the queue could be implemented by giving an appropriate number ofpoints in the scoring rule
459KIDNEY EXCHANGE
kidney and others on the queue who benefit from the increase inkidney supply due to an additional living donor However Rossand Woodle note that this may have a negative impact on type Opatients already on the cadaver queue an issue studied by Ze-nios Woodle and Ross [2001] to which we shall return
In contrast to the system for cadaveric organs and despitethe growing interest in at least small-scale exchanges involvingliving donors there is no national system or even an organizedregistry at any level for managing exchanges of kidneys from livedonors However individual hospitals are beginning to thinkabout larger scale living donor exchanges As this paper wasbeing written the first three-couple kidney transplant exchangein the United States was reported at Johns Hopkins Comprehen-sive Transplant Center in Baltimore among three couples forwhom no two-couple transfer was feasible [Olson August 22003] In the present paper we will consider how such a system ofexchanges might be organized from the point of view of achievingefficiency and providing consistent incentives to patients donorsand doctors and what its welfare implications might be We willsee that the benefits of wider exchange accrue not only to theparties to the exchange The resulting increase in live organdonation also benefits patients waiting for cadaver kidneys in-cluding type O patients The design we propose is partly inspiredby the mechanism design literature on ldquohouse allocationrdquo and isintended to build on and complement the existing practices inkidney transplantation In this respect and others it is in themodern tradition of engineering economics (see Roth [2002]) asapplied to other problems of allocation such as labor marketclearinghouses (see Roth and Peranson [1999]) or auctions (seeMilgrom [2004]) in which practical implementation often in-volves incremental change in existing practices
II BACKGROUND
IIA Kidney Transplantation
End Stage Renal Disease (ESRD) is a fatal disease unlesstreated with dialysis or kidney transplantation Transplantationis the preferred treatment Two genetic characteristics play keyroles in the feasibility and success of a kidney transplant Thefirst is the ABO blood-type There are four blood types A B ABand O Absent other complications type O kidneys can be trans-
460 QUARTERLY JOURNAL OF ECONOMICS
planted into any patient type A or type B kidneys can be trans-planted into same type or type AB patients and type AB kidneyscan only be transplanted into type AB patients (So type O pa-tients can only receive type O kidneys) The second genetic char-acteristic is tissue type also known as HLA type HLA type is acombination of six proteins As the HLA mismatch between thedonor and the recipient increases the likelihood of graft (ietransplanted organ) survival decreases [Opelz 1997] HLA playsanother key role in transplantation through the pretransplantldquocrossmatchrdquo test Prior to transplantation the potential recipi-ent is tested for the presence of preformed antibodies againstHLA in the donor kidney The presence of antibodies called apositive crossmatch effectively rules out transplantation
When a cadaveric kidney becomes available for transplanta-tion the priority of each patient on the waiting list is determinedby a point system based on factors including the blood type HLAantigen-match time spent on the waiting list the region thekidney is harvested etc and the kidney is offered to the patientwith the highest priority If that patient declines the kidney isoffered to the patient with the next highest priority and so onLiving donor kidney grafts have superior survival rates (and theiravailability can also avoid the long waiting time for a cadaverkidney) However potential living donors can be eliminated fromconsideration due to incompatibility of the potential donor kidneywith the intended recipient
To minimize the elimination of physically eligible volunteerkidney donors on the basis of immunologic incompatibilities Ra-paport [1986] proposed the creation of a living donor pool forpaired exchange Ross et al [1997] again proposed to increase thesupply of living kidney donations by using kidneys from livingincompatible donors through an exchange arrangement betweentwo pairs In 2000 UNOS initiated pilot testing of such programs
Another exchange program is the indirect exchange program[Ross and Woodle 2000] a potential donor who is incompatiblewith his intended recipient donates his kidney to the cadavericwaiting list and his paired recipient will receive priority for thenext compatible cadaveric kidney There is widespread agree-ment in the transplantation community that indirect exchangecan harm type O patients who have no living donors First theywill be losing their priority to type O patients whose incompatibledonors donate to the cadaveric pool and second very few type Oliving kidneys will be offered to their pool since a type O donor can
461KIDNEY EXCHANGE
directly donate to his intended recipient unless there is a positivecrossmatch Despite this widespread concern many transplantcenters have also cautiously started pilot indirect exchange pro-grams since 2000 For example in UNOS Region 1 (New En-gland) consisting of fourteen transplant centers and two OrganProcurement Organizations four paired exchanges and seven-teen indirect exchanges have been conducted from 2001 through2003 (personal communication)
IIB Mechanism Design
We will extend results in the mechanism design literaturewhich we first quickly review Shapley and Scarf [1974] modeleda ldquohousing marketrdquo consisting of n agents each of whom is en-dowed with an indivisible good a ldquohouserdquo Each agent has pref-erences over all the houses and there is no money in the markettrade is feasible only in houses They attribute to David Gale theldquotop trading cyclerdquo algorithm that produces a house allocation inthe core of the market The algorithm works as follows eachagent points to her most preferred house (and each house pointsto its owner) There is at least one cycle in the resulting directedgraph In each such cycle the corresponding trades are carriedout ie each agent in the cycle receives the house she is pointingto and these agents and houses are removed from the marketThe process continues (with each agent pointing to her mostpreferred house that remains on the market) until no agentsremain and the final allocation is the one in which each agentreceives the house with which she left the market When allpreferences are strict the procedure yields a unique outcome[Roth and Postlewaite 1977] and truthful preference revelation isa dominant strategy [Roth 1982]
Note that paired kidney exchanges similarly seek the gainsfrom trade among patients with willing donors but (with therecent Johns Hopkins three-pair exchange being a notable excep-tion) mostly among just two pairs In the kidney exchange to beconsidered below if we consider exchange only among patientswith donors the properties of the housing market model essen-tially carry over unchanged if we assume that donorsrsquo prefer-ences are aligned with those of their intended recipient We willalso assume that all surgeries in a given cycle are carried outsimultaneously which is the current practice since a donorrsquoswillingness to donate a kidney might change once her intendedrecipient received a transplant
462 QUARTERLY JOURNAL OF ECONOMICS
However the kidney transplant environment consists notjust of patients with donors but also patients without donors andcadaver kidneys not tied to any specific patient Abdulkadirogluand Sonmez [1999] studied housing allocation on college cam-puses which is in some respects similar a set of rooms must beallocated to a set of students by a centralized housing office Someof the students are existing tenants each of whom already occu-pies a room and the rest of the students are newcomers Inaddition to occupied rooms there are vacant rooms Existingtenants are entitled to keep their current rooms but may alsoapply for other rooms Mechanisms used on a number of collegecampuses do not ensure the participation of existing tenants andresult in efficiency loss This is the motivation for the generali-zation of the top trading cycles (TTC) mechanism proposed byAbdulkadiroglu and Sonmez [1999] which they called you requestmy housemdashI get your turn (YRMH-IGYT) each student reportshis strict preferences over all rooms and an ordering of agents israndomly chosen For any given preference list and ordering theoutcome is obtained as follows (1) Assign the first student his topchoice the second student his top choice among the remainingrooms and so on until someone requests the room of an existingtenant who is yet to be served (2) Whenever that happens modifythe remainder of the ordering by moving the existing tenant to thebeginning of the line and proceed with the procedure (3) If at anypoint a cycle forms it is formed exclusively by existing tenantsand each of them requests the room of the tenant who is next inthe cycle In such cases remove all students in the cycle byassigning them the rooms they request and proceed with theprocedure The key innovation here is that an existing tenantwhose current room is requested is upgraded to the first place inthe line of agents remaining unassigned before his room is allo-cated As a result the YRMH-IGYT mechanism assures everyexisting tenant a room that is no worse than his own Thereforeexisting tenants do not have any reason not to enter the marketand consequently the eventual allocation is Pareto efficient Notethat the idea of upgrading an existing tenant whose current roomis requested to the top of the line was also invented by the trans-plantation community in the form of an indirect exchange pro-gram when a potential donor donates his kidney to the highestpriority patient on the waiting list his intended recipient isupgraded to the top of the waiting list
Note again that what prompted the introduction of simple
463KIDNEY EXCHANGE
kidney exchange programs was the loss of volunteer kidney do-nors because of immunologic incompatibilities Under these ex-change programs a potential donor who is incompatible with hisintended recipient is given the incentive to go ahead with thedonation because his donation makes it possible for his intendedrecipient to receive a compatible kidney Similarly the potentialefficiency loss in the campus housing problem is that some roomsmight fail to be traded even when welfare-enhancing trades arepossible The YRMH-IGYT is an attempt to address that problemin the housing context We next consider how it must be adaptedto kidney exchange
III KIDNEY EXCHANGE AND THE TOP TRADING CYCLES
AND CHAINS (TTCC) MECHANISM
While there are clear similarities between house allocationand kidney exchange there are also important differences Thecounterpart of an existing tenant and his room is a donor-recipi-ent pair which we denote by (kiti) We will often refer to donorki as kidney ki and recipient ti as patient ti In the context ofhouse allocation with existing tenants there are also newcomersnone of whom owns a specific house and vacant houses none ofwhich is owned by a specific student The counterpart of newcom-ers are patients who have no living donors and the counterpart ofvacant houses are cadaveric kidneys that are not targeted forspecific patients This analogy reveals one important differencebetween the two models in the house allocation model the set ofvacant houses is known In the kidney exchange problem it is notclear which cadaveric kidneys will be available when they will beavailable etc Therefore while occupied houses and vacant housesare simultaneously allocated under the YRMH-IGYT mechanismthis is not possible in the context of kidney exchange Insteadpatients with live donors who are not themselves allocated a livedonor kidney will be assigned to the cadaver queue (with a pri-ority reflecting whether their donorrsquos kidney was donated tosomeone on the queue)
Let K denote the set of living donor kidneys at a particulartime While patients and their doctors may define their prefer-ences over kidneys as they wish here we consider for specificitythe preferences that come from maximizing the probability of asuccessful transplant Given any patient part of K is outside thefeasible set due to ABO blood-type incompatibility or a positive
464 QUARTERLY JOURNAL OF ECONOMICS
crossmatch Among feasible kidneys HLA match [Opelz 1997]donor age kidney size etc play a significant role in the graftsurvival Therefore patients have heterogeneous preferences overcompatible kidneys In what follows we will consider all prefer-ences to be strict If only direct exchanges among donor-recipientpairs are considered one can directly use Galersquos Top TradingCycles mechanism However this will not allow for indirectexchanges We will need to modify the model and the mecha-nism to allow for this possibility Since the supply of specificcadaveric donor kidneys is not predictable a patient whowishes to trade his donorrsquos kidney in return for a priority in thecadaveric kidney waiting list is receiving a lottery Taking thisinto consideration the patient doctor and donor can decidewhether this option is acceptable and if so where it ranks inthe patientrsquos preferences
Given a patient ti let Ki K denote the set of living donorkidneys that are compatible with patient ti Let w denote theoption of entering the waiting list with priority reflecting thedonation of his donorrsquos kidney ki and Pi denote his strict prefer-ences over Ki kiw For our purposes the relevant part of Pi
is the ranking up to kidney ki or w whichever ranks higher Ifpatient ti ranks kidney ki at the top of his preferences thatmeans he and his donor do not wish to participate in an exchangeIf patient ti ranks ki on top of w that means he and his donor donot consider exchanging kidney ki with a priority in the cadaverickidney waiting list
We can now formalize a (static) kidney exchange problemconsisting of a set of donor-recipient pairs (k1t1) (kntn)a set of compatible kidneys Ki K k1 kn for eachpatient ti and a strict preference relation Pi over Ki kiw foreach patient ti The outcome of a kidney exchange problem is amatching of kidneyswait-list option to patients such that eachpatient ti is either assigned a kidney in Ki ki or the wait-listoption w and no kidney can be assigned to more than one patientalthough the wait-list option w can be assigned to several pa-tients A kidney exchange mechanism selects a matching for eachkidney exchange problem We are almost ready to introduce theTop Trading Cycles and Chains (TTCC) mechanism a generali-zation of the TTC mechanism for kidney exchange First we givea few definitions and observations to facilitate the description ofthe mechanism
465KIDNEY EXCHANGE
IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

kidney and others on the queue who benefit from the increase inkidney supply due to an additional living donor However Rossand Woodle note that this may have a negative impact on type Opatients already on the cadaver queue an issue studied by Ze-nios Woodle and Ross [2001] to which we shall return
In contrast to the system for cadaveric organs and despitethe growing interest in at least small-scale exchanges involvingliving donors there is no national system or even an organizedregistry at any level for managing exchanges of kidneys from livedonors However individual hospitals are beginning to thinkabout larger scale living donor exchanges As this paper wasbeing written the first three-couple kidney transplant exchangein the United States was reported at Johns Hopkins Comprehen-sive Transplant Center in Baltimore among three couples forwhom no two-couple transfer was feasible [Olson August 22003] In the present paper we will consider how such a system ofexchanges might be organized from the point of view of achievingefficiency and providing consistent incentives to patients donorsand doctors and what its welfare implications might be We willsee that the benefits of wider exchange accrue not only to theparties to the exchange The resulting increase in live organdonation also benefits patients waiting for cadaver kidneys in-cluding type O patients The design we propose is partly inspiredby the mechanism design literature on ldquohouse allocationrdquo and isintended to build on and complement the existing practices inkidney transplantation In this respect and others it is in themodern tradition of engineering economics (see Roth [2002]) asapplied to other problems of allocation such as labor marketclearinghouses (see Roth and Peranson [1999]) or auctions (seeMilgrom [2004]) in which practical implementation often in-volves incremental change in existing practices
II BACKGROUND
IIA Kidney Transplantation
End Stage Renal Disease (ESRD) is a fatal disease unlesstreated with dialysis or kidney transplantation Transplantationis the preferred treatment Two genetic characteristics play keyroles in the feasibility and success of a kidney transplant Thefirst is the ABO blood-type There are four blood types A B ABand O Absent other complications type O kidneys can be trans-
460 QUARTERLY JOURNAL OF ECONOMICS
planted into any patient type A or type B kidneys can be trans-planted into same type or type AB patients and type AB kidneyscan only be transplanted into type AB patients (So type O pa-tients can only receive type O kidneys) The second genetic char-acteristic is tissue type also known as HLA type HLA type is acombination of six proteins As the HLA mismatch between thedonor and the recipient increases the likelihood of graft (ietransplanted organ) survival decreases [Opelz 1997] HLA playsanother key role in transplantation through the pretransplantldquocrossmatchrdquo test Prior to transplantation the potential recipi-ent is tested for the presence of preformed antibodies againstHLA in the donor kidney The presence of antibodies called apositive crossmatch effectively rules out transplantation
When a cadaveric kidney becomes available for transplanta-tion the priority of each patient on the waiting list is determinedby a point system based on factors including the blood type HLAantigen-match time spent on the waiting list the region thekidney is harvested etc and the kidney is offered to the patientwith the highest priority If that patient declines the kidney isoffered to the patient with the next highest priority and so onLiving donor kidney grafts have superior survival rates (and theiravailability can also avoid the long waiting time for a cadaverkidney) However potential living donors can be eliminated fromconsideration due to incompatibility of the potential donor kidneywith the intended recipient
To minimize the elimination of physically eligible volunteerkidney donors on the basis of immunologic incompatibilities Ra-paport [1986] proposed the creation of a living donor pool forpaired exchange Ross et al [1997] again proposed to increase thesupply of living kidney donations by using kidneys from livingincompatible donors through an exchange arrangement betweentwo pairs In 2000 UNOS initiated pilot testing of such programs
Another exchange program is the indirect exchange program[Ross and Woodle 2000] a potential donor who is incompatiblewith his intended recipient donates his kidney to the cadavericwaiting list and his paired recipient will receive priority for thenext compatible cadaveric kidney There is widespread agree-ment in the transplantation community that indirect exchangecan harm type O patients who have no living donors First theywill be losing their priority to type O patients whose incompatibledonors donate to the cadaveric pool and second very few type Oliving kidneys will be offered to their pool since a type O donor can
461KIDNEY EXCHANGE
directly donate to his intended recipient unless there is a positivecrossmatch Despite this widespread concern many transplantcenters have also cautiously started pilot indirect exchange pro-grams since 2000 For example in UNOS Region 1 (New En-gland) consisting of fourteen transplant centers and two OrganProcurement Organizations four paired exchanges and seven-teen indirect exchanges have been conducted from 2001 through2003 (personal communication)
IIB Mechanism Design
We will extend results in the mechanism design literaturewhich we first quickly review Shapley and Scarf [1974] modeleda ldquohousing marketrdquo consisting of n agents each of whom is en-dowed with an indivisible good a ldquohouserdquo Each agent has pref-erences over all the houses and there is no money in the markettrade is feasible only in houses They attribute to David Gale theldquotop trading cyclerdquo algorithm that produces a house allocation inthe core of the market The algorithm works as follows eachagent points to her most preferred house (and each house pointsto its owner) There is at least one cycle in the resulting directedgraph In each such cycle the corresponding trades are carriedout ie each agent in the cycle receives the house she is pointingto and these agents and houses are removed from the marketThe process continues (with each agent pointing to her mostpreferred house that remains on the market) until no agentsremain and the final allocation is the one in which each agentreceives the house with which she left the market When allpreferences are strict the procedure yields a unique outcome[Roth and Postlewaite 1977] and truthful preference revelation isa dominant strategy [Roth 1982]
Note that paired kidney exchanges similarly seek the gainsfrom trade among patients with willing donors but (with therecent Johns Hopkins three-pair exchange being a notable excep-tion) mostly among just two pairs In the kidney exchange to beconsidered below if we consider exchange only among patientswith donors the properties of the housing market model essen-tially carry over unchanged if we assume that donorsrsquo prefer-ences are aligned with those of their intended recipient We willalso assume that all surgeries in a given cycle are carried outsimultaneously which is the current practice since a donorrsquoswillingness to donate a kidney might change once her intendedrecipient received a transplant
462 QUARTERLY JOURNAL OF ECONOMICS
However the kidney transplant environment consists notjust of patients with donors but also patients without donors andcadaver kidneys not tied to any specific patient Abdulkadirogluand Sonmez [1999] studied housing allocation on college cam-puses which is in some respects similar a set of rooms must beallocated to a set of students by a centralized housing office Someof the students are existing tenants each of whom already occu-pies a room and the rest of the students are newcomers Inaddition to occupied rooms there are vacant rooms Existingtenants are entitled to keep their current rooms but may alsoapply for other rooms Mechanisms used on a number of collegecampuses do not ensure the participation of existing tenants andresult in efficiency loss This is the motivation for the generali-zation of the top trading cycles (TTC) mechanism proposed byAbdulkadiroglu and Sonmez [1999] which they called you requestmy housemdashI get your turn (YRMH-IGYT) each student reportshis strict preferences over all rooms and an ordering of agents israndomly chosen For any given preference list and ordering theoutcome is obtained as follows (1) Assign the first student his topchoice the second student his top choice among the remainingrooms and so on until someone requests the room of an existingtenant who is yet to be served (2) Whenever that happens modifythe remainder of the ordering by moving the existing tenant to thebeginning of the line and proceed with the procedure (3) If at anypoint a cycle forms it is formed exclusively by existing tenantsand each of them requests the room of the tenant who is next inthe cycle In such cases remove all students in the cycle byassigning them the rooms they request and proceed with theprocedure The key innovation here is that an existing tenantwhose current room is requested is upgraded to the first place inthe line of agents remaining unassigned before his room is allo-cated As a result the YRMH-IGYT mechanism assures everyexisting tenant a room that is no worse than his own Thereforeexisting tenants do not have any reason not to enter the marketand consequently the eventual allocation is Pareto efficient Notethat the idea of upgrading an existing tenant whose current roomis requested to the top of the line was also invented by the trans-plantation community in the form of an indirect exchange pro-gram when a potential donor donates his kidney to the highestpriority patient on the waiting list his intended recipient isupgraded to the top of the waiting list
Note again that what prompted the introduction of simple
463KIDNEY EXCHANGE
kidney exchange programs was the loss of volunteer kidney do-nors because of immunologic incompatibilities Under these ex-change programs a potential donor who is incompatible with hisintended recipient is given the incentive to go ahead with thedonation because his donation makes it possible for his intendedrecipient to receive a compatible kidney Similarly the potentialefficiency loss in the campus housing problem is that some roomsmight fail to be traded even when welfare-enhancing trades arepossible The YRMH-IGYT is an attempt to address that problemin the housing context We next consider how it must be adaptedto kidney exchange
III KIDNEY EXCHANGE AND THE TOP TRADING CYCLES
AND CHAINS (TTCC) MECHANISM
While there are clear similarities between house allocationand kidney exchange there are also important differences Thecounterpart of an existing tenant and his room is a donor-recipi-ent pair which we denote by (kiti) We will often refer to donorki as kidney ki and recipient ti as patient ti In the context ofhouse allocation with existing tenants there are also newcomersnone of whom owns a specific house and vacant houses none ofwhich is owned by a specific student The counterpart of newcom-ers are patients who have no living donors and the counterpart ofvacant houses are cadaveric kidneys that are not targeted forspecific patients This analogy reveals one important differencebetween the two models in the house allocation model the set ofvacant houses is known In the kidney exchange problem it is notclear which cadaveric kidneys will be available when they will beavailable etc Therefore while occupied houses and vacant housesare simultaneously allocated under the YRMH-IGYT mechanismthis is not possible in the context of kidney exchange Insteadpatients with live donors who are not themselves allocated a livedonor kidney will be assigned to the cadaver queue (with a pri-ority reflecting whether their donorrsquos kidney was donated tosomeone on the queue)
Let K denote the set of living donor kidneys at a particulartime While patients and their doctors may define their prefer-ences over kidneys as they wish here we consider for specificitythe preferences that come from maximizing the probability of asuccessful transplant Given any patient part of K is outside thefeasible set due to ABO blood-type incompatibility or a positive
464 QUARTERLY JOURNAL OF ECONOMICS
crossmatch Among feasible kidneys HLA match [Opelz 1997]donor age kidney size etc play a significant role in the graftsurvival Therefore patients have heterogeneous preferences overcompatible kidneys In what follows we will consider all prefer-ences to be strict If only direct exchanges among donor-recipientpairs are considered one can directly use Galersquos Top TradingCycles mechanism However this will not allow for indirectexchanges We will need to modify the model and the mecha-nism to allow for this possibility Since the supply of specificcadaveric donor kidneys is not predictable a patient whowishes to trade his donorrsquos kidney in return for a priority in thecadaveric kidney waiting list is receiving a lottery Taking thisinto consideration the patient doctor and donor can decidewhether this option is acceptable and if so where it ranks inthe patientrsquos preferences
Given a patient ti let Ki K denote the set of living donorkidneys that are compatible with patient ti Let w denote theoption of entering the waiting list with priority reflecting thedonation of his donorrsquos kidney ki and Pi denote his strict prefer-ences over Ki kiw For our purposes the relevant part of Pi
is the ranking up to kidney ki or w whichever ranks higher Ifpatient ti ranks kidney ki at the top of his preferences thatmeans he and his donor do not wish to participate in an exchangeIf patient ti ranks ki on top of w that means he and his donor donot consider exchanging kidney ki with a priority in the cadaverickidney waiting list
We can now formalize a (static) kidney exchange problemconsisting of a set of donor-recipient pairs (k1t1) (kntn)a set of compatible kidneys Ki K k1 kn for eachpatient ti and a strict preference relation Pi over Ki kiw foreach patient ti The outcome of a kidney exchange problem is amatching of kidneyswait-list option to patients such that eachpatient ti is either assigned a kidney in Ki ki or the wait-listoption w and no kidney can be assigned to more than one patientalthough the wait-list option w can be assigned to several pa-tients A kidney exchange mechanism selects a matching for eachkidney exchange problem We are almost ready to introduce theTop Trading Cycles and Chains (TTCC) mechanism a generali-zation of the TTC mechanism for kidney exchange First we givea few definitions and observations to facilitate the description ofthe mechanism
465KIDNEY EXCHANGE
IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

planted into any patient type A or type B kidneys can be trans-planted into same type or type AB patients and type AB kidneyscan only be transplanted into type AB patients (So type O pa-tients can only receive type O kidneys) The second genetic char-acteristic is tissue type also known as HLA type HLA type is acombination of six proteins As the HLA mismatch between thedonor and the recipient increases the likelihood of graft (ietransplanted organ) survival decreases [Opelz 1997] HLA playsanother key role in transplantation through the pretransplantldquocrossmatchrdquo test Prior to transplantation the potential recipi-ent is tested for the presence of preformed antibodies againstHLA in the donor kidney The presence of antibodies called apositive crossmatch effectively rules out transplantation
When a cadaveric kidney becomes available for transplanta-tion the priority of each patient on the waiting list is determinedby a point system based on factors including the blood type HLAantigen-match time spent on the waiting list the region thekidney is harvested etc and the kidney is offered to the patientwith the highest priority If that patient declines the kidney isoffered to the patient with the next highest priority and so onLiving donor kidney grafts have superior survival rates (and theiravailability can also avoid the long waiting time for a cadaverkidney) However potential living donors can be eliminated fromconsideration due to incompatibility of the potential donor kidneywith the intended recipient
To minimize the elimination of physically eligible volunteerkidney donors on the basis of immunologic incompatibilities Ra-paport [1986] proposed the creation of a living donor pool forpaired exchange Ross et al [1997] again proposed to increase thesupply of living kidney donations by using kidneys from livingincompatible donors through an exchange arrangement betweentwo pairs In 2000 UNOS initiated pilot testing of such programs
Another exchange program is the indirect exchange program[Ross and Woodle 2000] a potential donor who is incompatiblewith his intended recipient donates his kidney to the cadavericwaiting list and his paired recipient will receive priority for thenext compatible cadaveric kidney There is widespread agree-ment in the transplantation community that indirect exchangecan harm type O patients who have no living donors First theywill be losing their priority to type O patients whose incompatibledonors donate to the cadaveric pool and second very few type Oliving kidneys will be offered to their pool since a type O donor can
461KIDNEY EXCHANGE
directly donate to his intended recipient unless there is a positivecrossmatch Despite this widespread concern many transplantcenters have also cautiously started pilot indirect exchange pro-grams since 2000 For example in UNOS Region 1 (New En-gland) consisting of fourteen transplant centers and two OrganProcurement Organizations four paired exchanges and seven-teen indirect exchanges have been conducted from 2001 through2003 (personal communication)
IIB Mechanism Design
We will extend results in the mechanism design literaturewhich we first quickly review Shapley and Scarf [1974] modeleda ldquohousing marketrdquo consisting of n agents each of whom is en-dowed with an indivisible good a ldquohouserdquo Each agent has pref-erences over all the houses and there is no money in the markettrade is feasible only in houses They attribute to David Gale theldquotop trading cyclerdquo algorithm that produces a house allocation inthe core of the market The algorithm works as follows eachagent points to her most preferred house (and each house pointsto its owner) There is at least one cycle in the resulting directedgraph In each such cycle the corresponding trades are carriedout ie each agent in the cycle receives the house she is pointingto and these agents and houses are removed from the marketThe process continues (with each agent pointing to her mostpreferred house that remains on the market) until no agentsremain and the final allocation is the one in which each agentreceives the house with which she left the market When allpreferences are strict the procedure yields a unique outcome[Roth and Postlewaite 1977] and truthful preference revelation isa dominant strategy [Roth 1982]
Note that paired kidney exchanges similarly seek the gainsfrom trade among patients with willing donors but (with therecent Johns Hopkins three-pair exchange being a notable excep-tion) mostly among just two pairs In the kidney exchange to beconsidered below if we consider exchange only among patientswith donors the properties of the housing market model essen-tially carry over unchanged if we assume that donorsrsquo prefer-ences are aligned with those of their intended recipient We willalso assume that all surgeries in a given cycle are carried outsimultaneously which is the current practice since a donorrsquoswillingness to donate a kidney might change once her intendedrecipient received a transplant
462 QUARTERLY JOURNAL OF ECONOMICS
However the kidney transplant environment consists notjust of patients with donors but also patients without donors andcadaver kidneys not tied to any specific patient Abdulkadirogluand Sonmez [1999] studied housing allocation on college cam-puses which is in some respects similar a set of rooms must beallocated to a set of students by a centralized housing office Someof the students are existing tenants each of whom already occu-pies a room and the rest of the students are newcomers Inaddition to occupied rooms there are vacant rooms Existingtenants are entitled to keep their current rooms but may alsoapply for other rooms Mechanisms used on a number of collegecampuses do not ensure the participation of existing tenants andresult in efficiency loss This is the motivation for the generali-zation of the top trading cycles (TTC) mechanism proposed byAbdulkadiroglu and Sonmez [1999] which they called you requestmy housemdashI get your turn (YRMH-IGYT) each student reportshis strict preferences over all rooms and an ordering of agents israndomly chosen For any given preference list and ordering theoutcome is obtained as follows (1) Assign the first student his topchoice the second student his top choice among the remainingrooms and so on until someone requests the room of an existingtenant who is yet to be served (2) Whenever that happens modifythe remainder of the ordering by moving the existing tenant to thebeginning of the line and proceed with the procedure (3) If at anypoint a cycle forms it is formed exclusively by existing tenantsand each of them requests the room of the tenant who is next inthe cycle In such cases remove all students in the cycle byassigning them the rooms they request and proceed with theprocedure The key innovation here is that an existing tenantwhose current room is requested is upgraded to the first place inthe line of agents remaining unassigned before his room is allo-cated As a result the YRMH-IGYT mechanism assures everyexisting tenant a room that is no worse than his own Thereforeexisting tenants do not have any reason not to enter the marketand consequently the eventual allocation is Pareto efficient Notethat the idea of upgrading an existing tenant whose current roomis requested to the top of the line was also invented by the trans-plantation community in the form of an indirect exchange pro-gram when a potential donor donates his kidney to the highestpriority patient on the waiting list his intended recipient isupgraded to the top of the waiting list
Note again that what prompted the introduction of simple
463KIDNEY EXCHANGE
kidney exchange programs was the loss of volunteer kidney do-nors because of immunologic incompatibilities Under these ex-change programs a potential donor who is incompatible with hisintended recipient is given the incentive to go ahead with thedonation because his donation makes it possible for his intendedrecipient to receive a compatible kidney Similarly the potentialefficiency loss in the campus housing problem is that some roomsmight fail to be traded even when welfare-enhancing trades arepossible The YRMH-IGYT is an attempt to address that problemin the housing context We next consider how it must be adaptedto kidney exchange
III KIDNEY EXCHANGE AND THE TOP TRADING CYCLES
AND CHAINS (TTCC) MECHANISM
While there are clear similarities between house allocationand kidney exchange there are also important differences Thecounterpart of an existing tenant and his room is a donor-recipi-ent pair which we denote by (kiti) We will often refer to donorki as kidney ki and recipient ti as patient ti In the context ofhouse allocation with existing tenants there are also newcomersnone of whom owns a specific house and vacant houses none ofwhich is owned by a specific student The counterpart of newcom-ers are patients who have no living donors and the counterpart ofvacant houses are cadaveric kidneys that are not targeted forspecific patients This analogy reveals one important differencebetween the two models in the house allocation model the set ofvacant houses is known In the kidney exchange problem it is notclear which cadaveric kidneys will be available when they will beavailable etc Therefore while occupied houses and vacant housesare simultaneously allocated under the YRMH-IGYT mechanismthis is not possible in the context of kidney exchange Insteadpatients with live donors who are not themselves allocated a livedonor kidney will be assigned to the cadaver queue (with a pri-ority reflecting whether their donorrsquos kidney was donated tosomeone on the queue)
Let K denote the set of living donor kidneys at a particulartime While patients and their doctors may define their prefer-ences over kidneys as they wish here we consider for specificitythe preferences that come from maximizing the probability of asuccessful transplant Given any patient part of K is outside thefeasible set due to ABO blood-type incompatibility or a positive
464 QUARTERLY JOURNAL OF ECONOMICS
crossmatch Among feasible kidneys HLA match [Opelz 1997]donor age kidney size etc play a significant role in the graftsurvival Therefore patients have heterogeneous preferences overcompatible kidneys In what follows we will consider all prefer-ences to be strict If only direct exchanges among donor-recipientpairs are considered one can directly use Galersquos Top TradingCycles mechanism However this will not allow for indirectexchanges We will need to modify the model and the mecha-nism to allow for this possibility Since the supply of specificcadaveric donor kidneys is not predictable a patient whowishes to trade his donorrsquos kidney in return for a priority in thecadaveric kidney waiting list is receiving a lottery Taking thisinto consideration the patient doctor and donor can decidewhether this option is acceptable and if so where it ranks inthe patientrsquos preferences
Given a patient ti let Ki K denote the set of living donorkidneys that are compatible with patient ti Let w denote theoption of entering the waiting list with priority reflecting thedonation of his donorrsquos kidney ki and Pi denote his strict prefer-ences over Ki kiw For our purposes the relevant part of Pi
is the ranking up to kidney ki or w whichever ranks higher Ifpatient ti ranks kidney ki at the top of his preferences thatmeans he and his donor do not wish to participate in an exchangeIf patient ti ranks ki on top of w that means he and his donor donot consider exchanging kidney ki with a priority in the cadaverickidney waiting list
We can now formalize a (static) kidney exchange problemconsisting of a set of donor-recipient pairs (k1t1) (kntn)a set of compatible kidneys Ki K k1 kn for eachpatient ti and a strict preference relation Pi over Ki kiw foreach patient ti The outcome of a kidney exchange problem is amatching of kidneyswait-list option to patients such that eachpatient ti is either assigned a kidney in Ki ki or the wait-listoption w and no kidney can be assigned to more than one patientalthough the wait-list option w can be assigned to several pa-tients A kidney exchange mechanism selects a matching for eachkidney exchange problem We are almost ready to introduce theTop Trading Cycles and Chains (TTCC) mechanism a generali-zation of the TTC mechanism for kidney exchange First we givea few definitions and observations to facilitate the description ofthe mechanism
465KIDNEY EXCHANGE
IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

directly donate to his intended recipient unless there is a positivecrossmatch Despite this widespread concern many transplantcenters have also cautiously started pilot indirect exchange pro-grams since 2000 For example in UNOS Region 1 (New En-gland) consisting of fourteen transplant centers and two OrganProcurement Organizations four paired exchanges and seven-teen indirect exchanges have been conducted from 2001 through2003 (personal communication)
IIB Mechanism Design
We will extend results in the mechanism design literaturewhich we first quickly review Shapley and Scarf [1974] modeleda ldquohousing marketrdquo consisting of n agents each of whom is en-dowed with an indivisible good a ldquohouserdquo Each agent has pref-erences over all the houses and there is no money in the markettrade is feasible only in houses They attribute to David Gale theldquotop trading cyclerdquo algorithm that produces a house allocation inthe core of the market The algorithm works as follows eachagent points to her most preferred house (and each house pointsto its owner) There is at least one cycle in the resulting directedgraph In each such cycle the corresponding trades are carriedout ie each agent in the cycle receives the house she is pointingto and these agents and houses are removed from the marketThe process continues (with each agent pointing to her mostpreferred house that remains on the market) until no agentsremain and the final allocation is the one in which each agentreceives the house with which she left the market When allpreferences are strict the procedure yields a unique outcome[Roth and Postlewaite 1977] and truthful preference revelation isa dominant strategy [Roth 1982]
Note that paired kidney exchanges similarly seek the gainsfrom trade among patients with willing donors but (with therecent Johns Hopkins three-pair exchange being a notable excep-tion) mostly among just two pairs In the kidney exchange to beconsidered below if we consider exchange only among patientswith donors the properties of the housing market model essen-tially carry over unchanged if we assume that donorsrsquo prefer-ences are aligned with those of their intended recipient We willalso assume that all surgeries in a given cycle are carried outsimultaneously which is the current practice since a donorrsquoswillingness to donate a kidney might change once her intendedrecipient received a transplant
462 QUARTERLY JOURNAL OF ECONOMICS
However the kidney transplant environment consists notjust of patients with donors but also patients without donors andcadaver kidneys not tied to any specific patient Abdulkadirogluand Sonmez [1999] studied housing allocation on college cam-puses which is in some respects similar a set of rooms must beallocated to a set of students by a centralized housing office Someof the students are existing tenants each of whom already occu-pies a room and the rest of the students are newcomers Inaddition to occupied rooms there are vacant rooms Existingtenants are entitled to keep their current rooms but may alsoapply for other rooms Mechanisms used on a number of collegecampuses do not ensure the participation of existing tenants andresult in efficiency loss This is the motivation for the generali-zation of the top trading cycles (TTC) mechanism proposed byAbdulkadiroglu and Sonmez [1999] which they called you requestmy housemdashI get your turn (YRMH-IGYT) each student reportshis strict preferences over all rooms and an ordering of agents israndomly chosen For any given preference list and ordering theoutcome is obtained as follows (1) Assign the first student his topchoice the second student his top choice among the remainingrooms and so on until someone requests the room of an existingtenant who is yet to be served (2) Whenever that happens modifythe remainder of the ordering by moving the existing tenant to thebeginning of the line and proceed with the procedure (3) If at anypoint a cycle forms it is formed exclusively by existing tenantsand each of them requests the room of the tenant who is next inthe cycle In such cases remove all students in the cycle byassigning them the rooms they request and proceed with theprocedure The key innovation here is that an existing tenantwhose current room is requested is upgraded to the first place inthe line of agents remaining unassigned before his room is allo-cated As a result the YRMH-IGYT mechanism assures everyexisting tenant a room that is no worse than his own Thereforeexisting tenants do not have any reason not to enter the marketand consequently the eventual allocation is Pareto efficient Notethat the idea of upgrading an existing tenant whose current roomis requested to the top of the line was also invented by the trans-plantation community in the form of an indirect exchange pro-gram when a potential donor donates his kidney to the highestpriority patient on the waiting list his intended recipient isupgraded to the top of the waiting list
Note again that what prompted the introduction of simple
463KIDNEY EXCHANGE
kidney exchange programs was the loss of volunteer kidney do-nors because of immunologic incompatibilities Under these ex-change programs a potential donor who is incompatible with hisintended recipient is given the incentive to go ahead with thedonation because his donation makes it possible for his intendedrecipient to receive a compatible kidney Similarly the potentialefficiency loss in the campus housing problem is that some roomsmight fail to be traded even when welfare-enhancing trades arepossible The YRMH-IGYT is an attempt to address that problemin the housing context We next consider how it must be adaptedto kidney exchange
III KIDNEY EXCHANGE AND THE TOP TRADING CYCLES
AND CHAINS (TTCC) MECHANISM
While there are clear similarities between house allocationand kidney exchange there are also important differences Thecounterpart of an existing tenant and his room is a donor-recipi-ent pair which we denote by (kiti) We will often refer to donorki as kidney ki and recipient ti as patient ti In the context ofhouse allocation with existing tenants there are also newcomersnone of whom owns a specific house and vacant houses none ofwhich is owned by a specific student The counterpart of newcom-ers are patients who have no living donors and the counterpart ofvacant houses are cadaveric kidneys that are not targeted forspecific patients This analogy reveals one important differencebetween the two models in the house allocation model the set ofvacant houses is known In the kidney exchange problem it is notclear which cadaveric kidneys will be available when they will beavailable etc Therefore while occupied houses and vacant housesare simultaneously allocated under the YRMH-IGYT mechanismthis is not possible in the context of kidney exchange Insteadpatients with live donors who are not themselves allocated a livedonor kidney will be assigned to the cadaver queue (with a pri-ority reflecting whether their donorrsquos kidney was donated tosomeone on the queue)
Let K denote the set of living donor kidneys at a particulartime While patients and their doctors may define their prefer-ences over kidneys as they wish here we consider for specificitythe preferences that come from maximizing the probability of asuccessful transplant Given any patient part of K is outside thefeasible set due to ABO blood-type incompatibility or a positive
464 QUARTERLY JOURNAL OF ECONOMICS
crossmatch Among feasible kidneys HLA match [Opelz 1997]donor age kidney size etc play a significant role in the graftsurvival Therefore patients have heterogeneous preferences overcompatible kidneys In what follows we will consider all prefer-ences to be strict If only direct exchanges among donor-recipientpairs are considered one can directly use Galersquos Top TradingCycles mechanism However this will not allow for indirectexchanges We will need to modify the model and the mecha-nism to allow for this possibility Since the supply of specificcadaveric donor kidneys is not predictable a patient whowishes to trade his donorrsquos kidney in return for a priority in thecadaveric kidney waiting list is receiving a lottery Taking thisinto consideration the patient doctor and donor can decidewhether this option is acceptable and if so where it ranks inthe patientrsquos preferences
Given a patient ti let Ki K denote the set of living donorkidneys that are compatible with patient ti Let w denote theoption of entering the waiting list with priority reflecting thedonation of his donorrsquos kidney ki and Pi denote his strict prefer-ences over Ki kiw For our purposes the relevant part of Pi
is the ranking up to kidney ki or w whichever ranks higher Ifpatient ti ranks kidney ki at the top of his preferences thatmeans he and his donor do not wish to participate in an exchangeIf patient ti ranks ki on top of w that means he and his donor donot consider exchanging kidney ki with a priority in the cadaverickidney waiting list
We can now formalize a (static) kidney exchange problemconsisting of a set of donor-recipient pairs (k1t1) (kntn)a set of compatible kidneys Ki K k1 kn for eachpatient ti and a strict preference relation Pi over Ki kiw foreach patient ti The outcome of a kidney exchange problem is amatching of kidneyswait-list option to patients such that eachpatient ti is either assigned a kidney in Ki ki or the wait-listoption w and no kidney can be assigned to more than one patientalthough the wait-list option w can be assigned to several pa-tients A kidney exchange mechanism selects a matching for eachkidney exchange problem We are almost ready to introduce theTop Trading Cycles and Chains (TTCC) mechanism a generali-zation of the TTC mechanism for kidney exchange First we givea few definitions and observations to facilitate the description ofthe mechanism
465KIDNEY EXCHANGE
IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

However the kidney transplant environment consists notjust of patients with donors but also patients without donors andcadaver kidneys not tied to any specific patient Abdulkadirogluand Sonmez [1999] studied housing allocation on college cam-puses which is in some respects similar a set of rooms must beallocated to a set of students by a centralized housing office Someof the students are existing tenants each of whom already occu-pies a room and the rest of the students are newcomers Inaddition to occupied rooms there are vacant rooms Existingtenants are entitled to keep their current rooms but may alsoapply for other rooms Mechanisms used on a number of collegecampuses do not ensure the participation of existing tenants andresult in efficiency loss This is the motivation for the generali-zation of the top trading cycles (TTC) mechanism proposed byAbdulkadiroglu and Sonmez [1999] which they called you requestmy housemdashI get your turn (YRMH-IGYT) each student reportshis strict preferences over all rooms and an ordering of agents israndomly chosen For any given preference list and ordering theoutcome is obtained as follows (1) Assign the first student his topchoice the second student his top choice among the remainingrooms and so on until someone requests the room of an existingtenant who is yet to be served (2) Whenever that happens modifythe remainder of the ordering by moving the existing tenant to thebeginning of the line and proceed with the procedure (3) If at anypoint a cycle forms it is formed exclusively by existing tenantsand each of them requests the room of the tenant who is next inthe cycle In such cases remove all students in the cycle byassigning them the rooms they request and proceed with theprocedure The key innovation here is that an existing tenantwhose current room is requested is upgraded to the first place inthe line of agents remaining unassigned before his room is allo-cated As a result the YRMH-IGYT mechanism assures everyexisting tenant a room that is no worse than his own Thereforeexisting tenants do not have any reason not to enter the marketand consequently the eventual allocation is Pareto efficient Notethat the idea of upgrading an existing tenant whose current roomis requested to the top of the line was also invented by the trans-plantation community in the form of an indirect exchange pro-gram when a potential donor donates his kidney to the highestpriority patient on the waiting list his intended recipient isupgraded to the top of the waiting list
Note again that what prompted the introduction of simple
463KIDNEY EXCHANGE
kidney exchange programs was the loss of volunteer kidney do-nors because of immunologic incompatibilities Under these ex-change programs a potential donor who is incompatible with hisintended recipient is given the incentive to go ahead with thedonation because his donation makes it possible for his intendedrecipient to receive a compatible kidney Similarly the potentialefficiency loss in the campus housing problem is that some roomsmight fail to be traded even when welfare-enhancing trades arepossible The YRMH-IGYT is an attempt to address that problemin the housing context We next consider how it must be adaptedto kidney exchange
III KIDNEY EXCHANGE AND THE TOP TRADING CYCLES
AND CHAINS (TTCC) MECHANISM
While there are clear similarities between house allocationand kidney exchange there are also important differences Thecounterpart of an existing tenant and his room is a donor-recipi-ent pair which we denote by (kiti) We will often refer to donorki as kidney ki and recipient ti as patient ti In the context ofhouse allocation with existing tenants there are also newcomersnone of whom owns a specific house and vacant houses none ofwhich is owned by a specific student The counterpart of newcom-ers are patients who have no living donors and the counterpart ofvacant houses are cadaveric kidneys that are not targeted forspecific patients This analogy reveals one important differencebetween the two models in the house allocation model the set ofvacant houses is known In the kidney exchange problem it is notclear which cadaveric kidneys will be available when they will beavailable etc Therefore while occupied houses and vacant housesare simultaneously allocated under the YRMH-IGYT mechanismthis is not possible in the context of kidney exchange Insteadpatients with live donors who are not themselves allocated a livedonor kidney will be assigned to the cadaver queue (with a pri-ority reflecting whether their donorrsquos kidney was donated tosomeone on the queue)
Let K denote the set of living donor kidneys at a particulartime While patients and their doctors may define their prefer-ences over kidneys as they wish here we consider for specificitythe preferences that come from maximizing the probability of asuccessful transplant Given any patient part of K is outside thefeasible set due to ABO blood-type incompatibility or a positive
464 QUARTERLY JOURNAL OF ECONOMICS
crossmatch Among feasible kidneys HLA match [Opelz 1997]donor age kidney size etc play a significant role in the graftsurvival Therefore patients have heterogeneous preferences overcompatible kidneys In what follows we will consider all prefer-ences to be strict If only direct exchanges among donor-recipientpairs are considered one can directly use Galersquos Top TradingCycles mechanism However this will not allow for indirectexchanges We will need to modify the model and the mecha-nism to allow for this possibility Since the supply of specificcadaveric donor kidneys is not predictable a patient whowishes to trade his donorrsquos kidney in return for a priority in thecadaveric kidney waiting list is receiving a lottery Taking thisinto consideration the patient doctor and donor can decidewhether this option is acceptable and if so where it ranks inthe patientrsquos preferences
Given a patient ti let Ki K denote the set of living donorkidneys that are compatible with patient ti Let w denote theoption of entering the waiting list with priority reflecting thedonation of his donorrsquos kidney ki and Pi denote his strict prefer-ences over Ki kiw For our purposes the relevant part of Pi
is the ranking up to kidney ki or w whichever ranks higher Ifpatient ti ranks kidney ki at the top of his preferences thatmeans he and his donor do not wish to participate in an exchangeIf patient ti ranks ki on top of w that means he and his donor donot consider exchanging kidney ki with a priority in the cadaverickidney waiting list
We can now formalize a (static) kidney exchange problemconsisting of a set of donor-recipient pairs (k1t1) (kntn)a set of compatible kidneys Ki K k1 kn for eachpatient ti and a strict preference relation Pi over Ki kiw foreach patient ti The outcome of a kidney exchange problem is amatching of kidneyswait-list option to patients such that eachpatient ti is either assigned a kidney in Ki ki or the wait-listoption w and no kidney can be assigned to more than one patientalthough the wait-list option w can be assigned to several pa-tients A kidney exchange mechanism selects a matching for eachkidney exchange problem We are almost ready to introduce theTop Trading Cycles and Chains (TTCC) mechanism a generali-zation of the TTC mechanism for kidney exchange First we givea few definitions and observations to facilitate the description ofthe mechanism
465KIDNEY EXCHANGE
IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

kidney exchange programs was the loss of volunteer kidney do-nors because of immunologic incompatibilities Under these ex-change programs a potential donor who is incompatible with hisintended recipient is given the incentive to go ahead with thedonation because his donation makes it possible for his intendedrecipient to receive a compatible kidney Similarly the potentialefficiency loss in the campus housing problem is that some roomsmight fail to be traded even when welfare-enhancing trades arepossible The YRMH-IGYT is an attempt to address that problemin the housing context We next consider how it must be adaptedto kidney exchange
III KIDNEY EXCHANGE AND THE TOP TRADING CYCLES
AND CHAINS (TTCC) MECHANISM
While there are clear similarities between house allocationand kidney exchange there are also important differences Thecounterpart of an existing tenant and his room is a donor-recipi-ent pair which we denote by (kiti) We will often refer to donorki as kidney ki and recipient ti as patient ti In the context ofhouse allocation with existing tenants there are also newcomersnone of whom owns a specific house and vacant houses none ofwhich is owned by a specific student The counterpart of newcom-ers are patients who have no living donors and the counterpart ofvacant houses are cadaveric kidneys that are not targeted forspecific patients This analogy reveals one important differencebetween the two models in the house allocation model the set ofvacant houses is known In the kidney exchange problem it is notclear which cadaveric kidneys will be available when they will beavailable etc Therefore while occupied houses and vacant housesare simultaneously allocated under the YRMH-IGYT mechanismthis is not possible in the context of kidney exchange Insteadpatients with live donors who are not themselves allocated a livedonor kidney will be assigned to the cadaver queue (with a pri-ority reflecting whether their donorrsquos kidney was donated tosomeone on the queue)
Let K denote the set of living donor kidneys at a particulartime While patients and their doctors may define their prefer-ences over kidneys as they wish here we consider for specificitythe preferences that come from maximizing the probability of asuccessful transplant Given any patient part of K is outside thefeasible set due to ABO blood-type incompatibility or a positive
464 QUARTERLY JOURNAL OF ECONOMICS
crossmatch Among feasible kidneys HLA match [Opelz 1997]donor age kidney size etc play a significant role in the graftsurvival Therefore patients have heterogeneous preferences overcompatible kidneys In what follows we will consider all prefer-ences to be strict If only direct exchanges among donor-recipientpairs are considered one can directly use Galersquos Top TradingCycles mechanism However this will not allow for indirectexchanges We will need to modify the model and the mecha-nism to allow for this possibility Since the supply of specificcadaveric donor kidneys is not predictable a patient whowishes to trade his donorrsquos kidney in return for a priority in thecadaveric kidney waiting list is receiving a lottery Taking thisinto consideration the patient doctor and donor can decidewhether this option is acceptable and if so where it ranks inthe patientrsquos preferences
Given a patient ti let Ki K denote the set of living donorkidneys that are compatible with patient ti Let w denote theoption of entering the waiting list with priority reflecting thedonation of his donorrsquos kidney ki and Pi denote his strict prefer-ences over Ki kiw For our purposes the relevant part of Pi
is the ranking up to kidney ki or w whichever ranks higher Ifpatient ti ranks kidney ki at the top of his preferences thatmeans he and his donor do not wish to participate in an exchangeIf patient ti ranks ki on top of w that means he and his donor donot consider exchanging kidney ki with a priority in the cadaverickidney waiting list
We can now formalize a (static) kidney exchange problemconsisting of a set of donor-recipient pairs (k1t1) (kntn)a set of compatible kidneys Ki K k1 kn for eachpatient ti and a strict preference relation Pi over Ki kiw foreach patient ti The outcome of a kidney exchange problem is amatching of kidneyswait-list option to patients such that eachpatient ti is either assigned a kidney in Ki ki or the wait-listoption w and no kidney can be assigned to more than one patientalthough the wait-list option w can be assigned to several pa-tients A kidney exchange mechanism selects a matching for eachkidney exchange problem We are almost ready to introduce theTop Trading Cycles and Chains (TTCC) mechanism a generali-zation of the TTC mechanism for kidney exchange First we givea few definitions and observations to facilitate the description ofthe mechanism
465KIDNEY EXCHANGE
IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

crossmatch Among feasible kidneys HLA match [Opelz 1997]donor age kidney size etc play a significant role in the graftsurvival Therefore patients have heterogeneous preferences overcompatible kidneys In what follows we will consider all prefer-ences to be strict If only direct exchanges among donor-recipientpairs are considered one can directly use Galersquos Top TradingCycles mechanism However this will not allow for indirectexchanges We will need to modify the model and the mecha-nism to allow for this possibility Since the supply of specificcadaveric donor kidneys is not predictable a patient whowishes to trade his donorrsquos kidney in return for a priority in thecadaveric kidney waiting list is receiving a lottery Taking thisinto consideration the patient doctor and donor can decidewhether this option is acceptable and if so where it ranks inthe patientrsquos preferences
Given a patient ti let Ki K denote the set of living donorkidneys that are compatible with patient ti Let w denote theoption of entering the waiting list with priority reflecting thedonation of his donorrsquos kidney ki and Pi denote his strict prefer-ences over Ki kiw For our purposes the relevant part of Pi
is the ranking up to kidney ki or w whichever ranks higher Ifpatient ti ranks kidney ki at the top of his preferences thatmeans he and his donor do not wish to participate in an exchangeIf patient ti ranks ki on top of w that means he and his donor donot consider exchanging kidney ki with a priority in the cadaverickidney waiting list
We can now formalize a (static) kidney exchange problemconsisting of a set of donor-recipient pairs (k1t1) (kntn)a set of compatible kidneys Ki K k1 kn for eachpatient ti and a strict preference relation Pi over Ki kiw foreach patient ti The outcome of a kidney exchange problem is amatching of kidneyswait-list option to patients such that eachpatient ti is either assigned a kidney in Ki ki or the wait-listoption w and no kidney can be assigned to more than one patientalthough the wait-list option w can be assigned to several pa-tients A kidney exchange mechanism selects a matching for eachkidney exchange problem We are almost ready to introduce theTop Trading Cycles and Chains (TTCC) mechanism a generali-zation of the TTC mechanism for kidney exchange First we givea few definitions and observations to facilitate the description ofthe mechanism
465KIDNEY EXCHANGE
IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

IIIA Cycles and w-Chains
The mechanism relies on an algorithm consisting of severalrounds In each round each patient ti points either toward akidney in Ki ki or toward w and each kidney ki points to itspaired recipient ti
A cycle is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to kidney k1 Cycles larger thana single pair are associated with direct exchanges very much likethe paired-kidney-exchange programs but may involve morethan two pairs so that patient t1 is assigned kidney k2 patient t2is assigned kidney k3 patient tm is assigned kidney k1Note that each kidney or patient can be part of at most one cycleand thus no two cycles intersect
A w-chain is an ordered list of kidneys and patients(k1t1k2t2 kmtm) such that kidney k1 points to patientt1 patient t1 points to kidney k2 kidney km points topatient tm and patient tm points to w We refer to the pair(kmtm) whose patient receives a cadaver kidney in a w-chain asthe head and the pair (k1t1) whose donor donates to someone onthe cadaver queue as the tail of the w-chain W-chains are asso-ciated with indirect exchanges but unlike in a cycle a kidney ora patient can be part of several w-chains One practical possibilityis choosing among w-chains with a well-defined chain selectionrule very much like the rules that establish priorities on thecadaveric waiting list The current pilot indirect exchange pro-grams in the United States choose the minimal w-chains consist-ing of a single donor-recipient pair but this may not be efficientSelection of longer w-chains will benefit other patients as welland therefore the choice of a chain selection rule has efficiencyimplications (see Theorem 1) Chain selection rules may also beused for specific policy objectives such as increasing the inflow oftype O living donor kidneys to the cadaveric waiting list When-ever w-chain (k1t1 kmtm) is selected in the algorithmpatient t1 is assigned kidney k2 patient t2 is assigned kidneyk3 patient tm1 is assigned kidney km patient tm receiveshigh priority for the next compatible kidney in the cadavericwaiting list and kidney k1 is offered either to the cadavericwaiting list or to another patient with a paired donor
466 QUARTERLY JOURNAL OF ECONOMICS
LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

LEMMA 1 Consider a graph in which both the patient and thekidney of each pair are distinct nodes as is the wait-listoption w Suppose that each patient points either toward akidney or w and each kidney points to its paired recipientThen either there exists a cycle or each pair is the tail ofsome w-chain
We can now introduce the TTCC mechanism Because the ex-change mechanism interacts with many parts of the kidney trans-plant environment it will clarify the discussion to start by indi-cating which parts of the environment we take as fixed for ourpresent purpose First we take the operation of the cadaverqueue as fixed The cadaver queue can be thought of as a stochas-tic arrival process of cadavers and patients interacting with ascoring rule that determines which patients are offered whichcadaver kidneys We also take as fixed how patients whose donorsdonate a kidney to someone on the queue are given high priorityon the queue eg by being given points in the scoring rule4 Wealso take as given the size of the live kidney exchange ie the setof patient-donor pairs is taken to be fixed In practice the set ofpatient-donor pairs will grow as the geographic area served bythe kidney exchange is increased or as the time between ex-changes is increased A larger pool of possible exchanges willincrease the potential efficiency gains that can be realized byexchange but will also increase the size of the trading cyclesw-chains that might be needed to achieve these efficiencies Wewill keep track of both of these when we report simulations Boththe operation of the cadaver queue and the frequency and scopeof the kidney exchange will influence patientsrsquo ldquoreservation util-ityrdquo ie how they compare various opportunities for direct orindirect exchange to the option of not making any exchange nowbut waiting for a future opportunity Patients can express thisreservation utility by where they rank their own donor in theirpreferences
4 Depending on how this priority is given patients may need to be aware ofthe current population of the queue to evaluate the desirability of the w optionLiran Einav and Muriel Niederle have shared with us interesting ideas about howto further model the desirability of the w option dynamically taking into accountthat others may enter the queue with high priority but we will not pursue thishere
467KIDNEY EXCHANGE
IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

IIIB The Exchange Mechanism
For the mechanism defined below we assume that when oneamong multiple w-chains must be selected a fixed chain selectionrule is invoked We will consider a number of such rules and theirimplications for incentives efficiency and equity
Throughout the procedure kidneys are assigned to patientsthrough a series of exchanges Some patients and their assignedkidneys will be immediately removed from the procedure whileothers will remain with their assignments but they will assume apassive role So at any point in the procedure some agents may nolonger be participants some participants will be active and theothers passive
For a given kidney exchange problem the TTCC mechanismdetermines the exchanges as follows
1 Initially all kidneys are available and all agents areactive At each stage of the procedure each remainingactive patient ti points to his most preferred remainingunassigned kidney or to the wait-list option w whicheveris more preferred each remaining passive patient contin-ues to point to his assignment and each remaining kidneyki points to its paired recipient ti
2 By Lemma 1 there is either a cycle or a w-chain or both(a) Proceed to Step 3 if there are no cycles Otherwise
locate each cycle and carry out the correspondingexchange (ie each patient in the cycle is assigned thekidney he is pointing to) Remove all patients in a cycletogether with their assignments
(b) Each remaining patient points to his top choice amongremaining kidneys and each kidney points to itspaired recipient Locate all cycles carry out the corre-sponding exchanges and remove them Repeat untilno cycle exists
3 If there are no pairs left we are done Otherwise byLemma 1 each remaining pair is the tail of a w-chainSelect only one of the chains with the chain selection ruleThe assignment is final for the patients in the selectedw-chain The chain selection rule also determines whetherthe selected w-chain is removed and the associated ex-changes are all immediately assigned (including the kid-ney at the tail which is designated to go to a patient on thecadaver queue) or if the selected w-chain is kept in the
468 QUARTERLY JOURNAL OF ECONOMICS
procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

procedure although each patient in it is passive hence-forth5
4 After a w-chain is selected new cycles may form RepeatSteps 2 and 3 with the remaining active patients andunassigned kidneys until no patient is left
At the end of the procedure each patient with a living donor isassigned a kidney (or a high priority place on the waiting list)However that does not necessarily mean each of these patientsreceives a transplant In particular a minimal cycle (kiti) con-sisting of a single patient-donor pair may be a pair that was notoffered a sufficiently desirable kidney in the current exchangeand chooses to wait in the hope of exchanging for a high qualityliving donor kidney the next time the exchange is run after newdonors have entered the system
EXAMPLE 1 Consider a kidney exchange problem with 12 pairs(k1t1) (k12t12) with preferences as follows
t1 k9 k10 k1 t7 k6 k1 k3 k9 k10 k1 wt2 k11 k3 k5 k6 k2 t8 k6 k4 k11 k2 k3 k8
t3 k2 k4 k5 k6 k7 k8 w t9 k3 k11 t4 k5 k9 k1 k8 k10 k3 w t10 k11 k1 k4 k5 k6 k7 wt5 k3 k7 k11 k4 k5 t11 k3 k6 k5 k11
t6 k3 k5 k8 k6 t12 k11 k3 k9 k8 k10 k12
Suppose that patients are ordered in a priority-list based ontheir indices starting with the patient with the smallestindex We use the following chain selection rule choose thelongest w-chain In case the longest w-chain is not uniquechoose the w-chain with the highest priority patient if thehighest priority patient is part of more than one choose thew-chain with the second highest priority patient and so onKeep the selected w-chains until the termination
The execution of the TTCC mechanism is given in FiguresIndashV
5 The relevance of the last point is the following whenever a w-chain(k1t1 kmtm) is selected even though the assignments of all patients in thew-chain are finalized the kidney k1 at the tail of the w-chain can be utilized in twopossible ways It can immediately be offered to the waiting list (in which case thew-chain is removed) or it may be made available to the remaining patients as theprocess continues and hence the selected w-chain may possibly grow later onalthough the patients already in it are not affected
469KIDNEY EXCHANGE
The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

The final matching is
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12
k9 k11 k2 k8 k7 k5 k6 k4 w k1 k3 k10
It is worth emphasizing that the chain selection policy doesnot affect a patient who is at the head of a chain Since he pointsto the wait-list option he will eventually be selected regardless ofthe chain selection rule However whether his intended donorrsquoskidney is offered to the cadaveric waiting list or another patientwith a living donor depends on the rule Depending on policypriorities one may consider adopting a number of alternativechain selection rules For example
a Choose minimal w-chains and remove themb (c) Choose the longest w-chain and remove it (keep it) If
the longest w-chain is not unique then use a tiebreaker tochoose among them
FIGURE IExample 1 Round 1
There is a single cycle C1 (k11t11k3t3k2t2) Remove the cycle by assigningk11 to t2 k3 to t11 and k2 to t3
470 QUARTERLY JOURNAL OF ECONOMICS
d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

d (e) Prioritize patient-donor pairs in a single list Choosethe w-chain starting with the highest priority pair andremove it (keep it)
A w-chain that is formed at an interim step of the procedure maygrow at subsequent steps unless it is removed hence the imme-diate removal of w-chains has a potential efficiency cost Thereforethe following ldquohybridrdquo of chain selection rules d and e may appeal tothose who wish to moderate the efficiency loss while increasing theinflow of type O living kidneys to the cadaveric waiting list
f Prioritize the patient-donor pairs so that pairs with type Odonor have higher priorities than those who do not Choosethe w-chain starting with the highest priority pair remove itin case the pair has a type O donor but keep it otherwise
IIIC Efficiency and Incentives
In what follows we will speak of Pareto efficiency in terms ofthe agents in the kidney exchange problem namely the paired
FIGURE IIExample 1 Round 2
Upon removing cycle C1 a new cycle C2 (k7t7k6t6k5t5) forms Remove itby assigning k7 to t5 k6 to t7 and k5 to t6
471KIDNEY EXCHANGE
patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

patients and donors who are available to participate in the kidneyexchange Given a kidney exchange problem a matching is Paretoefficient if there is no other matching that is weakly preferred byall patients and donors and strictly preferred by at least onepatient-donor pair A kidney exchange mechanism is efficient if italways selects a Pareto efficient matching among the participantspresent at any given time
THEOREM 1 Consider a chain selection rule such that any w-chainselected at a nonterminal round remains in the procedureand thus the kidney at its tail remains available for the nextround The TTCC mechanism implemented with any suchchain selection rule is efficient
Chain selection rules that remove a selected w-chain before ter-
FIGURE IIIExample 1 Round 3
No new cycle forms and hence each kidney-patient pair starts a w-chain Thelongest w-chains are W1 (k8t8k4t4k9t9) and W2 (k10t10k1t1k9t9)Since t1 the highest priority patient is in W2 but not in W1 choose and fix W2Assign w to t9 k9 to t1 and k1 to t10 but do not remove them Kidney k10 thekidney at the tail of W2 remains available for the next round
472 QUARTERLY JOURNAL OF ECONOMICS
mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

mination of the algorithm on the contrary may yield Pareto-inefficient outcomes
Roth [1982] showed for the housing model that truthful pref-erence revelation is a dominant strategy of the preference revela-tion game induced by the TTC mechanism and hence an agentcan never profit by misrepresenting his preferences Recall thatin the absence of indirect exchanges the static kidney exchangeproblem is a housing market and therefore the Roth [1982] resultimmediately applies6 When indirect exchanges are allowed
6 That is at any specific time a patient cannot receive a more preferredkidney by misrepresenting his preferences which include his option value for thepossibility that his donorrsquos kidney can be used in a future exchange We emphasizethat of course we speak of strategy-proofness in the limited strategy space thespace of stated preferences we have modeled for the kidney exchange problemThere may remain strategic issues associated with other aspects of the organtransplant process such as being registered at multiple transplant centers andhence appearing on multiple regional waiting lists
FIGURE IVExample 1 Round 4
Upon fixing the w-chain W2 a new cycle C3 (k4t4k8t8) forms Remove it byassigning k4 to t8 and k8 to t4
473KIDNEY EXCHANGE
whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

whether the TTCC mechanism is strategy-proof depends on thechoice of the chain selection rule
THEOREM 2 Consider the chain selection rules a d e and f TheTTCC mechanism implemented with any of these chain se-lection rules is strategy-proof
Among these four chain selection rules the last two areespecially appealing Rule e yields an efficient and strategy-proofmechanism whereas Rule f gives up efficiency in order to in-crease the inflow of type O kidneys to the cadaveric waiting listOn the negative side strategy-proofness of TTCC is lost if oneadopts a chain selection rule that chooses among the longestw-chains
EXAMPLE 2 Consider the problem in Example 1 but suppose thatpatient t4 misrepresents his preferences as P4
FIGURE VExample 1 Round 5
No new cycles form and the pair (k12t12) ldquojoinsrdquo W2 from its tail to form thelongest w-chain W3 (k12t12k10t10k1t1k9t9) Fix W3 and assign k10 to t12Since no patient is left w-chain W3 is removed and kidney k12 at its tail is offeredto the highest priority patient at the cadaveric waiting list
474 QUARTERLY JOURNAL OF ECONOMICS
k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

k5k1k9 improving the ranking of kidney k1 WhileRound 1 and Round 2 remain as in Example 1 Round 3changes and this time the longest w-chain at Round 3 isW4 (k8t8k4t4k1t1k9t9) Therefore patient t4 is as-signed kidney k1 instead of kidney k8 making his preferencemisrepresentation profitable
IV SIMULATIONS
The theoretical treatment of the TTCC mechanism makesclear that larger exchanges may yield welfare gains but it givesno idea of their magnitude The following simulations are meantas a first step in that direction and as a ldquoproof of conceptrdquo todemonstrate that the gains are potentially substantial We usedata where they exist eg on the likelihood of mismatches andpositive crossmatches (see Table II) Where no data existmdashon thewillingness of patients and donors to trade a live donation forpriority on the cadaver queuemdashwe do robustness checks by simu-lating a wide range of preferences
IVA Patient and Donor Characteristics
In addition to characteristics reported in Table II for theHLA characteristics of the population we use the distributionreported in Zenios [1996] using the UNOS registration data foryears between 1987 and 1991 We assume that all HLA proteinsand blood type are independently distributed following ZeniosFor simplicity we consider unrelated donor-patient pairs About253 percent all living-donor transplants were in this category in2001 We use UNOS data to find the conditional distribution ofthe age of a nonspousal unrelated donor given that he is an adultWe assume that HLA and blood-type characteristics of the donorhave the same distribution as the patientsrsquo the characteristics ofa nonspousal unrelated donor are independently distributed withthe patient and the characteristics of a spouse are independentlydistributed with the patient except his or her age We assumethat the spouse age is the same as the patient age
IVB Preference Construction
The preferences of patients are determined using the sur-vival analysis of grafts reported in Mandal et al [2003] Thisanalysis uses data obtained from first-time kidney-only trans-plants between 1995 and 1998 in the United States Renal Data
475KIDNEY EXCHANGE
System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

System (USRDS) database We assume that the utility function ofeach patient depends on the number of HLA mismatches ( x) andthe donor age ( y) In the ldquorationalrdquo preference construction fol-lowing Mandal et al we assume that each patient younger than60 has a utility function u( xy) 0514x y10 and eachpatient 60 and older has a utility function u( xy) 0510x y10 We also consider a ldquocautiousrdquo preference construction Un-der cautious preferences we assume that patient ti prefers donor
TABLE IIAMERICAN CAUCASIAN PATIENT AND LIVING DONOR CHARACTERISTIC
DISTRIBUTIONS USED IN SIMULATIONS
A Patient ABO blood type FrequencyO 456A 395B 111AB 38
B Patient gender FrequencyFemale 409Male 591
C Patient age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
D Unrelated living donors FrequencySpouse 535Other 465
E Living donor age Frequency18 5618ndash34 1335ndash49 34950ndash64 38964 76
F Positive crossmatch FrequencyFemale patientmdashhusband 333Other 111
The frequencies are obtained from the UNOS data for various years Patients are the new wait-listadditions recorded between January 1995 and April 2003 except the gender data The gender and livingdonor data were recorded between 1992 and 2001 Based on UNOSOPTN data and annual report as of7142003 retrieved from httpwwwoptnorg Positive crossmatch probability is reported by Zenios Woodleand Ross [2001]
476 QUARTERLY JOURNAL OF ECONOMICS
kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

kj Ki to his own donor ki only if kidney ki is not compatible withhim or if although kidney ki is compatible with him it has morethan an equivalent of one additional HLA mismatch than kidneykj has
Under both preference scenarios the wait-list option may ormay not be considered acceptable by a patient Since the expectedquality of HLA match is very low when a patient is given priorityin the waiting list and since the graft failure rates are signifi-cantly higher for cadaveric kidneys than living-donor kidneys weassume that a patient considers the wait-list option acceptableonly if his donor is not compatible with him We also assume thatthe patients who consider this option acceptable prefer any com-patible living-donor kidney to this option Because there are noreliable data available on the rate of patients who consider thisoption acceptable and because it depends on how priority is givenwe consider two treatments in which 0 percent and 40 percent ofthe patients with incompatible donors prefer the wait-list optionto their own donors
IVC Simulated Mechanisms
We consider four exchange mechanisms to contrast with theno-exchange regime (1) paired-kidney-exchange mechanism (2)TTC mechanism (3) paired and indirect exchange mechanismand (4) TTCC mechanism with the efficient and strategy-proofchain selection rule e In our simulations we randomly simulate asample of n donor-patient pairs using the population character-istics explained above Then we determine the preferences ofpatients over kidneys in the sample for each patient ti we firstcheck whether a donor kj is ABO-compatible If kj is ABO-com-patible then we check whether there is a positive crossmatchbetween ti and kj If they test negative for crossmatch then kj isin the compatible donor set Ki of patient ti After finding the setof compatible kidneys for each patient we obtain a preferenceordering on this set using the utility functions described aboveWe construct four sets of preferences for each patient using therational or cautious preference construction and assuming that 0percent or 40 percent of patients with incompatible donors con-sider the wait-list option acceptable We simulate each of the fivemechanisms under these four preference scenarios We use aMonte-Carlo simulation size of 100 trials for three different popu-lation sizes of 30 100 and 300 pairs
477KIDNEY EXCHANGE
IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

IVD Discussion of Results
The simulation results suggest that substantial gains in thenumber and match quality of transplanted kidneys might resultfrom adoption of the TTCC mechanism We report the details ofthis analysis in three tables The rows of the tables refer todifferent regimes under different preference constructions anddifferent population sizes
Table III reports the general patient statistics under eachregime The first column reports the total live donor transplantsas percentage of the population size which is the sum of the nexttwo columns transplants from own compatible donor and trans-plants from trades The fourth column is the percentage of pa-tients upgraded to the top of the wait-list through indirect ex-changes The fifth column reports the quality of matches in thelive donor transplants the lower the HLA mismatch is thehigher the odds of graft survival Standard errors are reportedbelow the estimates
In Table IV we report the effect of each regime on the wait-list additions for each blood type The columns are separated intotwo main groups The first group reports the net percentage ofpatients sent to the top of the wait-list due to indirect exchanges(the percentages are taken with respect to all paired patients)This is a net upgrade burden ie the difference between thepatients added at the top of the list and the living-donor kidneysmade available for the wait-list patients The second group re-ports (again as a percentage of all paired patients) the rate ofpaired patients who nonetheless are sent to the cadaveric waitinglist because the patient is not assigned a living-donor kidney
In Table V we report the sizes of cycles and w-chains undereach mechanism The columns are divided into two groups forcycles and w-chains Each group reports the number the averagelength the average maximum (per group over all 100 trials)length of cyclesw-chains and the length of the longest cyclew-chain encountered in all 100 trials The lengths of cyclesw-chainsare measured in pairs Standard errors are reported below theestimates
Next we highlight a number of these results1 A transition to the TTCC mechanism will significantly
improve the utilization rate of potential unrelated living-donor kidneys assuming a population size of 100 pairswhile approximately 55 percent of potential living-donor
478 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

TA
BL
EII
IN
UM
BE
RO
FT
RA
NS
PL
AN
TS
AN
DQ
UA
LIT
YO
FM
AT
CH
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
eT
otal
tran
s
Ow
ndo
nor
tran
s
Tra
de
Wai
t-li
stu
pgra
de
HL
Am
is
Wai
t-li
st0
All
Non
e54
83
(89
6)54
83
(89
6)0
(0)
0(0
)4
79(0
25)
All
Pai
red
685
0(9
90)
548
3(8
96)
136
7(9
40)
0(0
)4
78(0
24)
Rat
ion
alT
TC
824
7(1
014
)23
03
(94
4)59
43
(13
57)
0(0
)4
16(0
22)
n
30C
auti
ous
TT
C81
07
(10
02)
341
7(1
127
)46
90
(13
96)
0(0
)4
29(0
23)
Wai
t-li
st40
A
llP
aire
din
d68
50
(99
0)54
83
(89
6)13
67
(94
0)13
20
(67
3)4
78(0
24)
Rat
ion
alT
TC
Ce
847
0(8
49)
212
3(9
60)
634
7(1
239
)6
37(4
88)
417
(02
2)C
auti
ous
TT
CC
e83
57
(85
3)32
93
(10
98)
506
3(1
254
)6
13(4
39)
429
(02
2)
Wai
t-li
st0
All
Non
e54
79
(44
8)54
79
(44
8)0
(0)
0(0
)4
83(0
14)
All
Pai
red
735
9(4
97)
547
9(4
48)
188
0(3
81)
0(0
)4
82(0
11)
Rat
ion
alT
TC
878
5(4
54)
115
1(3
44)
763
4(5
45)
0(0
)3
72(0
10)
n
100
Cau
tiou
sT
TC
872
3(4
73)
240
1(4
48)
632
2(5
46)
0(0
)3
86(0
11)
Wai
t-li
st40
A
llP
aire
din
d73
59
(49
7)54
79
(44
8)18
80
(38
1)10
24
(30
7)4
82(0
11)
Rat
ion
alT
TC
Ce
894
4(3
85)
102
9(3
26)
791
5(4
40)
396
(19
7)3
71(0
10)
Cau
tiou
sT
TC
Ce
889
7(4
17)
228
1(4
83)
661
6(4
79)
472
(26
0)3
85(0
11)
Wai
t-li
st0
All
Non
e53
92
(28
2)53
92
(28
2)0
(0)
0(0
)4
81(0
08)
All
Pai
red
750
3(2
72)
539
2(2
82)
211
1(2
51)
0(0
)4
81(0
07)
Rat
ion
alT
TC
910
5(3
35)
572
(12
8)85
32
(36
1)0
(0)
329
(00
6)n
30
0C
auti
ous
TT
C90
86
(33
1)15
36
(22
0)75
51
(40
7)0
(0)
340
(00
6)W
ait-
list
40
All
Pai
red
ind
750
3(2
72)
539
2(2
82)
211
1(2
51)
977
(17
3)4
81(0
07)
Rat
ion
alT
TC
Ce
922
9(2
98)
500
(12
9)87
29
(30
5)3
02(1
36)
329
(00
6)C
auti
ous
TT
CC
e92
17
(29
3)14
42
(21
0)77
75
(32
6)3
19(1
40)
339
(00
6)
479KIDNEY EXCHANGE
TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

TA
BL
EIV
AB
OC
OM
PO
SIT
ION
OF
NE
TW
AIT
-LIS
TU
PG
RA
DE
SA
ND
OT
HE
RW
AIT
-LIS
TP
AT
IEN
TS
AS
PE
RC
EN
TA
GE
OF
N
30
N
100
AN
DN
30
0
Pop
si
zeP
ref
Exc
han
gere
gim
e
Net
wai
t-li
stu
pgra
des
O
ther
wai
t-li
stad
diti
ons
OA
BA
BT
otal
OA
BA
BT
otal
Wai
t-li
st0
All
Non
e0
00
00
288
310
13
577
043
451
7A
llP
aire
d0
00
00
245
04
072
800
1331
50
Rat
ion
alT
TC
00
00
012
47
317
177
013
175
3n
30
Cau
tiou
sT
TC
00
00
013
77
317
187
013
189
3W
ait-
list
40
All
Pai
red
ind
910
6
33
123
1
530
146
72
201
370
0718
30
Rat
ion
alT
TC
Ce
513
2
47
107
1
600
713
117
063
000
893
Cau
tiou
sT
TC
Ce
490
2
23
123
1
430
870
083
077
000
103
0
Wai
t-li
st0
All
Non
e0
00
00
276
411
18
586
053
452
1A
llP
aire
d0
00
00
218
92
901
570
0526
41
Rat
ion
alT
TC
00
00
09
301
900
910
0412
15
n
100
Cau
tiou
sT
TC
00
00
09
782
000
950
0412
77
Wai
t-li
st40
A
llP
aire
din
d8
25
527
1
70
128
013
42
162
108
005
161
7R
atio
nal
TT
CC
e3
49
117
1
07
125
05
710
460
420
016
60C
auti
ous
TT
CC
e4
21
156
1
12
153
05
500
410
400
006
31
Wai
t-li
st0
All
Non
e0
00
00
283
211
42
579
055
460
8A
llP
aire
d0
00
00
217
02
191
060
0224
97
Rat
ion
alT
TC
00
00
07
071
340
520
018
95n
30
0C
auti
ous
TT
C0
00
00
723
137
052
001
914
Wai
t-li
st40
A
llP
aire
din
d8
40
565
1
42
132
013
21
136
063
001
152
1R
atio
nal
TT
CC
e2
77
087
0
63
127
04
280
230
180
004
69C
auti
ous
TT
CC
e2
94
096
0
63
134
04
280
210
150
004
64
Net
wai
t-li
stu
pgra
des
isth
edi
ffer
ence
betw
een
the
nu
mbe
rof
upg
rade
dpa
tien
tsof
cert
ain
bloo
dty
pean
dth
en
um
ber
ofli
vedo
nor
kidn
eys
sen
tto
the
wai
t-li
stof
the
sam
ebl
ood
type
480 QUARTERLY JOURNAL OF ECONOMICS
TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

TA
BL
EV
PR
OP
ER
TIE
SO
FC
YC
LE
SA
ND
W-C
HA
INS
FO
RN
30
N
10
0A
ND
N
300
Pop
si
zeP
ref
Exc
han
gere
gim
e
Cyc
les
W-c
hai
ns
Nu
mbe
r
Len
gth
(as
pair
s)
Nu
mbe
r
Len
gth
(as
pair
s)
Mea
nM
ax
Lon
gest
Mea
nM
axL
onge
st
Wai
t-li
st0
All
Non
e16
45
(26
9)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
185
0(2
46)
111
(00
8)1
90(0
30)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C14
65
(22
2)2
95(0
43)
565
(11
5)9
0(0
)mdash
mdashmdash
n
30C
auti
ous
TT
C16
79
(27
1)2
59(0
41)
542
(11
7)10
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d18
50
(24
6)1
11(0
08)
190
(03
0)2
396
(20
2)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
133
7(2
50)
304
(04
7)5
65(1
15)
91
91(1
46)
186
(08
3)2
55(1
35)
7C
auti
ous
TT
CC
e15
74
(27
5)2
62(0
44)
542
(11
7)10
184
(13
2)1
81(0
68)
226
(10
1)6
Wai
t-li
st0
All
Non
e54
79
(44
8)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
641
9(4
33)
115
(00
3)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C36
53
(34
4)4
22(0
41)
101
4(1
65)
150
(0)
mdashmdash
mdashn
10
0C
auti
ous
TT
C45
53
(42
9)3
51(0
33)
982
(18
1)17
0(0
)mdash
mdashmdash
Wai
t-li
st40
A
llP
aire
din
d64
19
(43
3)1
15(0
03)
200
(00
0)2
102
4(3
07)
1(0
)1
(0)
1R
atio
nal
TT
CC
e32
91
(41
6)4
41(0
43)
101
4(1
65)
153
96(1
97)
240
(09
3)3
96(1
97)
11C
auti
ous
TT
CC
e42
00
(54
3)3
61(0
39)
982
(18
1)17
472
(26
0)2
17(0
65)
376
(16
4)10
Wai
t-li
st0
All
Non
e16
176
(84
7)1
(0)
1(0
)1
0(0
)mdash
mdashmdash
All
Pai
red
193
42(7
42)
116
(00
2)2
00(0
00)
20
(0)
mdashmdash
mdashR
atio
nal
TT
C79
54
(49
1)5
98(0
43)
168
4(2
41)
260
(0)
mdashmdash
mdashn
30
0C
auti
ous
TT
C10
214
(70
0)4
89(0
33)
160
0(2
00)
220
(0)
mdashmdash
mdashW
ait-
list
40
All
Pai
red
ind
193
42(7
42)
116
(00
2)2
00(0
00)
229
30
(51
8)1
(0)
1(0
)1
Rat
ion
alT
TC
Ce
711
7(5
88)
630
(04
6)16
84
(24
1)26
905
(40
7)2
88(0
78)
647
(24
0)15
Cau
tiou
sT
TC
Ce
937
6(7
51)
505
(03
3)16
00
(20
0)22
957
(42
0)2
65(0
72)
599
(22
3)12
Cyc
les
ofon
epa
irle
ngt
hw
ith
anin
com
pati
ble
don
or-p
atie
nt
pair
are
not
cou
nte
d
481KIDNEY EXCHANGE
kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

kidneys are utilized under the no-exchange regime thisrate increases to 735 percent under the paired-kidney-exchange and to 88ndash895 percent under the TTCC mech-anism The efficiency gain gets larger as the populationsize grows further
2 A transition to TTCC significantly decreases the HLAmismatch especially for the large populations
3 Under the TTCC mechanism averagemaximal sizes ofcyclesw-chains increase as the population grows al-though the increase is less than proportional
4 Type O patients without living donors benefit from theTTCC mechanism The TTCC mechanism significantlyreduces the incidence of type O patients with potentialdonors who are forced to rely on the cadaveric waiting listbecause of an incompatibility Consider a population sizeof 100 donor-recipient pairs (with the distribution of bloodtypes etc of the UNOS data set) When no exchange isallowed on average 276 type O patients who have awilling donor nevertheless join the waiting list for a ca-daver kidney because they are incompatible (by blood typeor positive crossmatch) with their donor This rate reducesto 219 under the paired-kidney-exchange and further to55ndash57 under the TTCC mechanism That means out of100 patients with living donors 162ndash164 patients with Oblood types drop out of competition for cadaver kidneys asa result of a change from paired-kidney-exchange to theTTCC mechanism The corresponding cost of this changeto type O patients with no living donors is that only35ndash42 type O patients with living donors are moved tothe head of the cadaver queue7 So the reduction in de-mand for O type cadaver kidneys is much larger than thenumber of patients who are inserted at the head of thequeue8
7 This benefitcost rate is significantly better than the benefitcost rate thatresults from a change from paired-kidney-exchange to pairedindirect-kidney-exchange because in an indirect exchange only occasionally will a type O livingdonor kidney be sent to the waiting list to compensate for the type O patient whoreceives priority on the queue In our simulations with 100 paired patients atransition from paired-kidney-exchange to pairedindirect-kidney-exchange drops2189ndash1342 847 patients from the waiting list at a cost of moving 825 pairedpatients to the head of the cadaver queue
8 We emphasize that the welfare implications of this for type O patients onthe cadaver queue is much clearer when we think of patients who enter the queueafter kidney exchange is already well established There can still be important
482 QUARTERLY JOURNAL OF ECONOMICS
More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

More detail on the simulations can be found in Roth Sonmez andUnver [2003]
V CONCLUSION
The TTCC mechanism is motivated by the present small-scale pilot paired and indirect kidney exchange programs Wehave concentrated here on its advantages over the simplest kindsof exchange But as we begin to talk with members of the trans-plantation community about first steps toward implementingsuch exchanges it is clear that there are obstacles to be overcomeSome are the same obstacles that have kept existing exchangeprograms very small Among these is the absence of registries ofincompatible or poorly matched patient-donor pairs9 Also ex-changes require coordination of multiple operating rooms andsurgical teams two for each patient-donor pair so larger ex-changes will require more coordination
As a registry starts to be assembled it may be that the maininitial advantage will simply be to allow paired exchanges to beconducted more often However as the registry grows larger andthe practical difficulties are overcome we have seen that therewill be additional benefits to be reaped from more flexible forms ofexchange that enlarge the set of possible exchanges Comparedwith simple paired and indirect exchanges the wider exchangeimplemented by the TTCC mechanism creates additional welfaregains in several ways First allowing longer cycles of exchangewill allow some transplantations that could not be arranged withpairwise exchanges and it will increase the scope for improvingthe quality of the resulting matches And by allowing more livedonations it will reduce the competition for cadaver kidneysSecond longer chains for combined indirect and paired exchange
welfare concerns about individual patients during the transition to an indirectexchange regime since an O type patient who has already been on the waiting listfor three years receives relatively less benefit from the reduction in new O typepatients joining the list than does a new patient but suffers increased waitingtime when an O type patient is given higher priority on the queue What thesimulations suggest is that once a kidney exchange regime is up and runningtype O patients without a living donor who enter the queue for a cadaver kidneywill be helped not harmed by the fact that exchanges are being made
9 Such a registry would need to include tissue typing data and presentmedical privacy laws mean that this will be difficult to collect ex post We havebegun exploratory discussions with our medical colleagues in New England aboutthe possibility of developing a program to identify incompatible and poorlymatched patient-donor pairs and collect tissue-typing data from potential donors
483KIDNEY EXCHANGE
will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

will allow an indirect exchange to benefit more than one patient-donor pair and by doing so will also increase the number of livedonations And third by increasing the number of O type patientswho can receive live donations and by managing the flow ofkidneys and patients to the cadaver queue this can be done inways that help O type patients who have no live donor10
In summary the design of practical exchange mechanisms isthe ldquoengineeringrdquo part of economic theory and must deal withconstraints omitted from more abstract endeavors The organiza-tion of a kidney exchange faces some of the most stringent con-straints we have encountered arising from sociallegalethicalconcerns as well as from the practical requirements of kidneytransplantation and patient care In the future some of thoseconstraints may be relaxed eg through advances in dealingwith immunological incompatibilities or in using xenotrans-plants (animal organs) to relieve the organ shortage or throughsome other way of radically increasing organ availability In themeantime increasing kidney exchange among willing donor-re-cipient pairs offers a way to benefit those pairs who are not wellmatched and by increasing live organ donation and reducingcompetition for cadaver organs also benefiting patients who donot have live donors This benefit is sufficiently widespread thatit helps even the most vulnerable patients the type O patientswithout a live donor
APPENDIX PROOFS
Proof of Lemma 1 Consider a graph where each patientpoints toward either a kidney or w and each kidney points to itspaired recipient Suppose that there is no cycle Consider anarbitrary pair (kiti) Start with kidney ki and follow the path inthe graph Since there are no cycles no kidney or patient can beencountered twice Hence by the finiteness of pairs the path will
10 To eliminate or reduce the adverse affect of indirect exchange programson patients with no living donors Zenios Woodle and Ross [2001] proposepreferential selection of O blood-type paired donors for patients with multiplepotential donors who wish to participate in indirect exchange programs Theirproposal is consistent with a direct extension of the TTCC mechanism to a modelwith multiple potential donors when the flexibility on chain selection is used toincrease the inflow of O blood-type kidneys to the cadaveric waiting list See RothSonmez and Unver [2003] for more on exchange when patients may have multiplepotential donors
484 QUARTERLY JOURNAL OF ECONOMICS
terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

terminate at w This is the w-chain initiated by pair (kiti) com-pleting the proof
Proof of Theorem 1 Let the TTCC mechanism be imple-mented with a chain selection rule such that any w-chain selectedat a nonterminal round remains in the procedure and the kidneyat its tail remains available for the next round Any patient whoseassignment is finalized in Round 1 has received his top choice andcannot be made better off Any patient whose assignment isfinalized in Round 2 has received his top choice among the kid-neys not already assigned as part of an exchange (since chains arenot removed so the kidney at their tail remains available) andcannot be made better off without hurting a patient whose as-signment was finalized in Round 1 Proceeding in a similar wayno patient can be made better off without hurting a patient whoseassignment is finalized in an earlier round Therefore TTCCmechanism selects a Pareto-efficient matching at any given timeprovided that w-chains are removed at the termination
We will prove Theorem 2 for the chain selection rule a and fora class of ldquopriority chain selection rulesrdquo that covers rules d e andf Under this class each ordering of patient-donor pairs togetherwith a fixed pair defines a chain selection rule and it is given asfollows order donor-patient pairs in a single priority list Fix apair (kjtj) Whenever a w-chain is to be selected select thew-chain starting with the highest priority pair (kiti) and removethe w-chain if the pair (kiti) has strictly higher priority than thefixed pair (kjtj) and keep it until termination otherwise
First we prove the following lemma which will be useful forthe proof of Theorem 2
LEMMA 2 Consider the TTCC mechanism implemented with apriority-based chain selection rule Fix the stated preferencesof all patients except patient ti at Pi Suppose that in thealgorithm the assignment of patient ti is finalized at Round sunder Pi and at Round s under Pi Suppose that s sThen the remaining active patients and unassigned kidneysat the beginning of Round s are the same whether patient tiannounces Pi or Pi
Proof of Lemma 2 Patient ti fails to participate in a cycle ora selected w-chain prior to Round s under either preferenceTherefore at any round prior to Round s not only the highestpriority active patient is the same whether patient ti announces
485KIDNEY EXCHANGE
Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

Pi or Pi but also the same cyclesw-chains form and in case thereare no cycles the same w-chain is selected whether patient ti
announces Pi or Pi Hence the remaining active patients andunassigned kidneys at the beginning of Round s are the samewhether patient ti announces Pi or Pi
Proof of Theorem 2 We first consider the chain selection rulea Recall that for each patient ti the relevant part of preferencePi is the ranking up to ki or w whichever is more preferredGiven the preference profile (Pi)i1
n construct a new preferenceprofile (Pi)i1
n as follows for each patient ti with kiPiw let Pi Pi For each patient ti with wPiki construct Pi from Pi byswapping the ranking of ki and w Note that kiPiw for eachpatient ti and because the relevant part of preferences are themore preferred of ki and w (kiti)i1
n (Pi)i1n is a housing
market Let denote the outcome of the TTC mechanism for thishousing market and construct matching v from matching asfollows if Pi Pi and (ti) ki then v(ti) w otherwisev(ti) (ti) The key observation is that v is the outcome of theTTCC mechanism when it is implemented with the minimalw-chain selecting chain selection rule Therefore by Roth [1982] apatient can never receive a more preferred kidney by a preferencemisrepresentation He can receive the wait-list option w by a mis-representation but cannot profit from it That is because the TTCCmechanism never assigns a patient a kidney that is inferior to wHence TTCC is strategy-proof with this choice of chain selectionrule
Next consider any of the priority-based chain selection rulesConsider a patient ti with true preferences Pi Fix an announcedpreference profile Pi for all other patients We want to show thatrevealing his true preferences Pi is at least as good as announcingany other preferences Pi under the TTCC mechanism Let s ands be the rounds at which patient ti leaves the algorithm under Pi
and Pi respectively We have two cases to consider
Case 1 s s By Lemma 2 the same kidneys remain in thealgorithm at the beginning of Round s whether patient ti an-nounces Pi or Pi Moreover patient ti is assigned his top choiceremaining at Round s under Pi Therefore his assignment underPi is at least as good as his assignment under Pi
486 QUARTERLY JOURNAL OF ECONOMICS
Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

Case 2 s s After announcing Pi the assignment ofpatient ti is finalized either by joining a cycle or by joining aselected w-chain We will consider the two cases separately
Case 2a The assignment of patient ti is finalized by joininga cycle under Pi
Let (k1t1k2 krti) be the cycle patient ti joins andthus k1 be the kidney he is assigned under Pi Next suppose thathe reveals his true preferences Pi Consider Round s By Lemma2 the same active patients and available kidneys remain at thebeginning of this round whether patient ti announces Pi or PiTherefore at Round s kidney k1 points to patient t1 patient t1
points to kidney k2 kidney kr points to patient ti Moreoverthey keep on doing so as long as patient ti remains Since patientti truthfully points to his best remaining choice at each round heeither receives a kidney better than kidney k1 or eventuallypoints to kidney k1 completes the formation of cycle(k1t1k2 krti) and gets assigned kidney k1
Case 2b The assignment of patient ti is finalized by joininga selected w-chain under Pi
Let (k1t1k2 krti trkr1 krmtrm) be the selectedw-chain patient ti joins where r 1 and m 0 under Pi Thereforeunder Pi patient ti is assigned the kidney kr1 if m 1 and thewait-list option w if m 0 Also note that given the considered classof priority-based chain selection rules pair (k1t1) is the highestpriority pair in Round s Next suppose that patient ti reveals histrue preferences Pi Consider Round s By Lemma 2 the same activepatients and available kidneys remain at the beginning of this roundwhether patient ti announces Pi or Pi We will complete the proof byshowing that upon announcing his truthful preferences Pi theassignment of patient ti is finalized in Round s and thus he isassigned his top choice available at the beginning of Round s recallthat for this case there is no cycle in Round s when patient tiannounces Pi Therefore when he announces his true preferences Pieither there is no cycle in Round s or there is one cycle that includeshim If it is the latter then his assignment is finalized in Round sand we are done Otherwise each pair initiates a w-chain by Lemma1 and one of these w-chains has to be selected By the choice of apriority-based chain selection rule this will be the w-chain thatstarts with the highest priority pair (k1t1) But the path startingwith kidney k1 passes through patient ti and therefore the selected
487KIDNEY EXCHANGE
w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS

w-chain includes patient ti Hence in this case as well his assign-ment is finalized in Round s completing the proof
HARVARD UNIVERSITY
KOC UNIVERSITY
KOC UNIVERSITY
REFERENCES
Abdulkadiroglu Atila and Tayfon Sonmez ldquoHouse Allocation with Existing Ten-antsrdquo Journal of Economic Theory LXXXVIII (1999) 233ndash260
Abecassis Michael et al The Journal of the American Medical AssociationCCLXXXIV (2002) 2919ndash2926
Becker Gary S and Julio J Elias ldquoIntroducing Incentives in the Market forLiving Organ Donationsrdquo Working paper University of Chicago 2002
Mandal Aloke K Jon J Snyder David T Gilbertson Allan J Collins andJohn R Silkensen ldquoDoes Cadaveric Donor Renal Transplantation Ever Pro-vide Better Outcomes Than Live-Donor Renal Transplantationrdquo Transplan-tation LXXV (2003) 494ndash500
Milgrom Paul Putting Auction Theory to Work (Cambridge University Press 2004)Nelson Edward W James E Childress Jennie Perryman Victor Robards Albert
Rowan Michael S Seely Sylvester Sterioff and Mary Rouelli SwansonldquoFinancial Incentives for Organ Donation A Report of the Payment Subcom-mitteerdquo United Network for Organ Sharing Ethics Committee 1993
Olson Elizabeth ldquoA Tale of 6 Kidneys or She Gave Him Her Love He Gave HerHis Kidneyrdquo New York Times Saturday August 2 A7 2003
Opelz Gerhard ldquoImpact of HLA Compatibility on Survival of Kidney Transplantsfrom Unrelated Live Donorsrdquo Transplantation LXIV (1997) 1473ndash1475
Rapaport Felix T ldquoThe Case for a Living Emotionally Related International KidneyDonor Exchange Registryrdquo Transplantation Proceedings XVIII (1986) 5ndash9
Ross Lainie Friedman David T Rubin Mark Siegler Michelle A JosephsonJ Richard Thistlethwaite Jr and E Steve Woodle ldquoEthics of a Paired-Kidney-Exchange Programrdquo The New England Journal of MedicineCCCXXXVI (1997) 1752ndash1755
Ross Lainie Friedman and E Steve Woodle ldquoEthical Issues in Increasing LivingKidney Donations by Expanding Kidney Paired Exchange Programsrdquo Trans-plantation LXIX (2002) 1539ndash1543
Roth Alvin E ldquoIncentive Compatibility in a Market with Indivisibilitiesrdquo Eco-nomics Letters IX (1982) 127ndash132
mdashmdash ldquoThe Economist as Engineer Game Theory Experimentation and Compu-tation as Tools for Design Economicsrdquo Econometrica LXX (2002) 1341ndash1378
Roth Alvin E and Elliot Peranson ldquoThe Redesign of the Matching Market forAmerican Physicians Some Engineering Aspects of Economic Designrdquo Ameri-can Economic Review LXXXIX (1999) 748ndash780
Roth Alvin E and Andrew Postlewaite ldquoWeak versus Strong Domination in aMarket with Indivisible Goodsrdquo Journal of Mathematical Economics IV(1977) 131ndash137
Roth Alvin E Tayfon Sonmez and M Utku Unver ldquoKidney Exchangerdquo NBERWorking Paper No 10002 September 2003
Sade R M ldquoAssessing Initiatives to Increase Organ Donationsrdquo Prepared WitnessTestimony The House Committee on Energy and Commerce W J ldquoBillyrdquoTauzin Chairman Subcommittee on Oversight and Investigations June 3 2003
Shapley Lloyd and Herbert Scarf ldquoOn Cores and Indivisibilityrdquo Journal ofMathematical Economics (1974) 23ndash28
Zenios Stefanos ldquoHealth Care Applications of Optimal Control Theoryrdquo PhDThesis Massachusetts Institute of Technology 1996
Zenios Stefanos E Steve Woodle and Lainie Friedman Ross ldquoPrimum nonNocere Avoiding Increased Waiting Times for Individual Racial and Blood-Type Subsets of Kidney Wait List Candidates in a Living DonorCadavericDonor Exchange Programrdquo Transplantation LXVI (2001) 406ndash407
488 QUARTERLY JOURNAL OF ECONOMICS