ICANL Final Report Compliance: The Definitive Guide & Checklist
14
The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance Engineered to comply with the strictest reporting standards published by MYOCARDIAL PERFUSION IMAGING FINAL REPORT Patient Name: DOE, JOHN D. Gender: M Date of Study: 4/2/2013 Date of birth: 6/28/1962 Age: 50 Medical Record #: 45869725 Ordering Physician: JANE INTERNIST, MD History: Chest Pain, Abn ECG, High Cholesterol, Hypertension, Positive Treadmill Test Indications: Assessment of chest pain, Positive ETT AUC: Appropriate use criteria met - Indication #38 NUCLEAR IMAGING PROTOCOL: Same Day Rest Stress 5.8 mCi of Tc-99m sestamibi was administered via IV injection at rest. Approximately 45 minutes afterwards, cardiac SPECT imaging was performed. A stress test was then performed and at peak exercise, 17.9 mCi of Tc-99m sestamibi was injected IV; approximately 45 minutes post injection, cardiac gated SPECT and prone cardiac gated SPECT imaging was performed. Attenuation correction was not used. STRESS PROTOCOL: Exercise Stress Test The patient exercised on a treadmill utilizing the Bruce protocol; they completed 11 minutes & 10 seconds, achieving approximately 12.9 METS. Baseline heart rate was measured at 62 bpm, and increased to 185 bpm at peak exercise; which is 108% of the maximum predicted heart rate. The heart rate response was normal. Baseline blood pressure was 142/78 mmHg and increased to 168/92 mmHg at peak exercise, which is a normal response to exercise. Resting ECG demonstrated normal sinus rhythm with diffuse non-specific ST-T wave abnormalities. During exercise, the ECG showed non-sustained V-tach. At peak stress, the ECG revealed downsloping ST-T depression of 1 - 1.5 mm. During exercise, Make Certain that Your Lab is ABSOLUTELY COMPLIANT with IAC Nuclear/PET Reporting Standards.
-
Upload
nuclearcardiologyreportscom-llc -
Category
Healthcare
-
view
930 -
download
12
description
To download this checklist, please go to: www.NuclearCardiologyReports.com/definitive-guide-checklist-icanl-report-compliance/ It is required by Medicare and insurance companies that our Nuclear Cardiology Labs are accredited in order to be reimbursed. ---------- It is widely known that one of the biggest reasons for negative accreditation decisions by IAC Nuclear/PET (ICANL) is a lack of compliance with their Final Report Standards. ---------- This clear, concise, and comprehensive breakdown of every component of the 2012 ICANL Final Report Standards will enable you to quickly and easily assess your Nuclear Cardiology Laboratory’s compliance or lack of compliance. ---------- Use this exhaustive checklist to easily determine whether or not your SPECT MPI Final Reports comply with ICANL Standards.
Transcript of ICANL Final Report Compliance: The Definitive Guide & Checklist

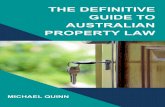
The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
Engineered to comply with the strictest reporting standards published by
MYOCARDIAL PERFUSION IMAGING FINAL REPORT
Patient Name: DOE, JOHN D. Gender: M Date of Study: 4/2/2013 Date of birth: 6/28/1962 Age: 50 Medical Record #: 45869725 Ordering Physician: JANE INTERNIST, MD History: Chest Pain, Abn ECG, High Cholesterol, Hypertension, Positive Treadmill Test Indications: Assessment of chest pain, Positive ETT AUC: Appropriate use criteria met - Indication #38
NUCLEAR IMAGING PROTOCOL: Same Day Rest Stress
5.8 mCi of Tc-99m sestamibi was administered via IV injection at rest. Approximately 45 minutes afterwards, cardiac SPECT imaging was performed. A stress test was then performed and at peak exercise, 17.9 mCi of Tc-99m sestamibi was injected IV; approximately 45 minutes post injection, cardiac gated SPECT and prone cardiac gated SPECT imaging was performed. Attenuation correction was not used.
STRESS PROTOCOL: Exercise Stress Test
The patient exercised on a treadmill utilizing the Bruce protocol; they completed 11 minutes & 10 seconds, achieving approximately 12.9 METS. Baseline heart rate was measured at 62 bpm, and increased to 185 bpm at peak exercise; which is 108% of the maximum predicted heart rate. The heart rate response was normal. Baseline blood pressure was 142/78 mmHg and increased to 168/92 mmHg at peak exercise, which is a normal response to exercise. Resting ECG demonstrated normal sinus rhythm with diffuse non-specific ST-T wave abnormalities. During exercise, the ECG showed non-sustained V-tach. At peak stress, the ECG revealed downsloping ST-T depression of 1 - 1.5 mm. During exercise,
Make Certain that Your Lab is
ABSOLUTELY COMPLIANT with IAC Nuclear/PET Reporting Standards.

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
2
Introduction:
The Template Reporting System by NuclearCardiologyReports.com is completely compliant with ICANL final report standards because it:
• is structured so that all ICANL required report elements are automaticallyincluded
• expresses every single report element in “Standardized Nomenclature”*• checks every report with over 100 error checks, ensuring ICANL reporting
compliance
• is updated with changing ICANL standards
*“Standardized Nomenclature” means according to the following documents:
(1) American Society of Nuclear Cardiology Reporting Standards
(2) ACC/AHA/ACR/ASE/ASNC/HRS/NASCI/RSNA/SAIP/SCAI/SCCT/SCMR/SIR 2008 Key Data Elements and Definitions for Cardiac Imaging
The report ... is the single most important part of the test… as it
communicates the result of the test to the patient’s health care provider(s).”**
… laboratories with a largernumber of reporting errors were
more likely to have delayed decisions, with provisional laboratories having fewer errors and those with granted status had no errors.”**
...there is no statistical difference in the average number of final
report errors between the 1st and 2nd times that nuclear cardiology labs apply for ICANL accreditation.” (paraphrase)**
... (the) majority of the laboratories were non-compliant with reporting standards, with
57.2% reporting at least one element of non-compliance.”**
Conclusions: Nuclear cardiology reports have a high degree of
non-compliance with the current ICANL standards.”**
** Quotes from: “The nuclear cardiology report: Problems, predictors, and improvement. A report from the ICANL database”, Tilkemeier P, Serber E, Farrell MB, Journal of Nuclear Cardiology 2011; DOI: 10.1007/s12350-011-9390-z.
GET STARTED WITH A FREE TRIAL NOW
It is required by Medicare and insurance companies that our Nuclear Cardiology Labs are accredited in order to be reimbursed.
It is widely known that one of the biggest reasons for negative accreditation decisions by IAC Nuclear/PET (ICANL) is a lack of compliance with their Final Report Standards. (See the quotes at right **)
This clear, concise, and comprehensive breakdown of every component of the 2012 ICANL Final Report Standards will enable you to quickly and easily assess your Nuclear Cardiology Laboratory’s compliance or lack of compliance.
Use this exhaustive checklist to easily determine whether or not your SPECT MPI Final Reports comply with ICANL Standards.
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
3
Top 18 ICANL Report Elements in Descending Order of Importance
# Required report componentMean
Importance Score
Definition
Does your lab’s report solution
always comply with this requirement?
1 Succinct impression1.0 Report must contain an accurate succinct impression (e.g., normal or abnormal) that clearly communicates the results
of the study YES NO
1.25 Quantification of myocardial perfusion defects in terms of location size, severity and type YES NO
1.42 Description of overall left ventricular function and regional abnormalities YES NO
1.75 Clinical indication and pertinent history leading to the performance of the examination YES NO
1.83 The final report must be transmitted to the referring healthcare provider within two working day YES NO
1.83 Use of appropriate reporting terminology and 17-segment model YES NO
2.0 Signature of the interpreting physician YES NO
2.17 Description of the procedure including type of examination, imaging protocol, imaging sequence and type of stress YES NO
2.5 Date the final report is reviewed signed and dated by the interpreting physician YES NO
2.5 Amount and route of administration of pharmacologic stress agent or other pharmaceuticals (e.g., aminophylline, PYP) YES NO
2.75 Exact dose of the administered radiopharmaceutical with one decimal point (i.e., XX.X mCi) YES NO
3.0 Demographic items such as facility identification and phone number YES NO
3.0 Lack of integration of imaging findings and stress data (exercise or pharmacologic) into the final imaging report YES NO
3.17 Requesting health care provider’s name YES NO
3.17 Patient’s age or date of birth YES NO
3.3 Patient’s gender YES NO
3.7 Route or method of administration of the radiopharmaceutical (i.e., intravenous) YES NO
2 Defect quantification
3 Wall motion findings
4 Indication
5 Timeliness
6 Nomenclature or standardization
7 Signature
8 Description of procedure
9 Date of report
10 Non-radioactive dose and route
11 Exact dose
12 Demographic items
13 Separate reports
14 Referring physician
15 Age/birth date
16 Gender
17 Route of administration of the RP
18 Typographical errors 3.9 Typing mistakes or errors YES NO
Note: Mean importance score: 1-5 scale (1 = very important, 5 = least important).
* This table is a compilation of Table 2 and Table 7 from this article: “The nuclear cardiology report: Problems, predictors, and improvement. A report from theICANL database.” Tilkemeier P, Serber E, Farrell MB, Journal of Nuclear Cardiology 2011; DOI: 10.1007/s12350-011-9390-z.
Overview:*
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
4
Comprehensive Breakdown of the Standards: ICANL Report Requirements Checklist for Your Lab
ICANL / IAC Nuclear Requirement
3.4.10A The final report must include a description of the results of the exam including pertinent positive and negative findings including:
Non-imaging data such as stress test responses and summarized findings (when applicable) Comment: Stress testing data reported must include patient response to stress (Rest and peak stress HR, rest and peak stress blood pressure, rest and peak stress ECG findings) stress symptoms, stress duration, percent of maximum predicted HR, reason for termination of stress, and timing of administration of radiopharmaceuticals as it relates to pharmaceutical or other stress administration. (3.4.10.1A)Itemized breakdown on next page
Always Compliant? YES NO Corrective Action(s) Needed: These report elements are included in every template.
Some values, such as timing of radiopharmaceutical administration as it relates to pharmacologic stress administration are usually set to default values (which can be quickly changed) per your normal protocols.
Image description, including:
location and types of findings
(including size/extent and severity/intensity of cardiac defects) (3.4.10.2A)
Recommendation:
The description should use standard nomenclature such as the 17-segment cardiac model for myocardial perfusion imaging.
If quantitative data is used, normal values should be reported. (3.4.13.2A)
Itemized breakdown on next page
This is where almost all Reporting Software fails.
Also, it is virtually impossible to get this correct using voice dictation / transcription.
To consistently describe perfusion, wall motion, and overall LV systolic function using appropriate standardized nomenclature requires the use of precisely programmed structured reporting software.
Always Compliant? YES NO Corrective Action(s) Needed:
The structure and error checking of our Image Interpretation User Interface ensures that every cardiac defect is described strictly according to ASNC standardized nomenclature*
For example perfusion defects are described by size (with guidelines for # of segments), severity, reversibility, and location (using the 17-segment cardiac model (larger defect areas, such as “inferior” may also be chosen if so desired)
Overall left ventricular systolic function is automatically described in accordance with LVEF percentage, or it may be manually characterized.
Quantitative sum scores and defect percentage extent are optional.
* Each and every report element in our reports complies withcurrent ASNC reporting standards:ASNC Imaging Guidelines For Nuclear Cardiology Procedures – 2009 Standardized reporting of radionuclide myocardial perfusion and function, Peter L. Tilkemeier, MD, C. David Cooke, MSEE, Gabriel B. Grossman, MD, PhD, Benjamin D. McCallister Jr, MD, and R. Parker Ward, MD
Does Your Current Final Report Solution Always Comply With This Requirement?
How the Template Reporting System Complies With This Requirement
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
5
3.4.10A (Continued) The final report must include a description of the results of the exam including pertinent positive and negative findings including:
ICANL / IAC Nuclear
Requirement
Does Your Current Final Report Solution Always Include These Report Elements? Does Your Current Solution Always Express These Report
Elements in ASNC Standardized Nomenclature?
Does the Template Reporting System Comply With This Requirement? What is the ASNC Standardized Nomenclature For These Report Elements?
3.4.10.1A
(Itemized)
Resting Heart Rate? YES NO _______________________
Peak Stress Heart Rate? YES NO _______________________
Rest Blood Pressure? YES NO _______________________
Peak Stress Blood Pressure? YES NO _______________________
Stress Symptoms? YES NO _______________________
Stress Duration? YES NO _______________________
% MPHR Achieved? YES NO _______________________
Reason for Termination of Stress? YES NO _______________________
Timing of Tracer Administration in Relation to Exercise or Pharmaceutical Stress Administration? YES NO ___________________
Summary of Stress Test? YES NO _______________________
Yes Error-checked for inclusion
Yes Error-checked for inclusion
Yes Error-checked for inclusion
Yes Error-checked for inclusion
Yes Error-checked for inclusion
Yes Error-checked for inclusion Yes Calculated automatically & error-checked for inclusion
Yes Error-checked for inclusion
Yes You choose your default timing of tracer admin; can change quickly via dropdown Yes Error-checked for inclusion. Also, a concise Stress Test Summary SECTION is
3.4.10.2A
(Itemized)
&
3.4.13.2A
(Standardized nomenclature
defined according to
ASNC Standards)
Perfusion Defects:
Size Expressed According to ASNC Nomenclature? YES NO
Severity Expressed According to ASNC Nomenclature? YES NO
Reversibility Expressed According to ASNC Nomenclature? YES NO
Location Expressed According to 17-segment model? YES NO
Wall Motion Defects:
Type Expressed According to ASNC Nomenclature? YES NO
Location Expressed According to 17-segment model? YES NO
Wall Thickening Defects:
Type Expressed According to ASNC Nomenclature? YES NO
Location Expressed According to 17-segment model? YES NO
Is Overall LV Systolic Function Accurately Expressed in Accordance with LVEF%? YES NO
Perfusion Defects: Yes Small, Medium, Large & Extensive; with definitions for # of segments which
constitute different sizes; TID included as well
Yes Mild, Mild to Moderate, Moderate, Moderate to Severe, Severe
Yes Reversible, Partially Reversible, Partially Fixed, Fixed, Mixed, Persistent
Yes All 17 segments are available to choose from, as well as more broadly definedregions (e.g. “Inferior”)
Wall Motion Defects: Yes Mild/Moderate/Severe Hypokinesis; Akinesis, Dyskinesis
Yes All 17 segments are available to choose from, as well as more broadly definedregions (e.g. “Global”, “Inferior”)
Wall Thickening Defects: Yes Mildly, Moderately, Severely Decreased Thickening
Yes All 17 segments are available to choose from, as well as more broadly definedregions (e.g. “Global”, “Inferior”)
Abnormal Overall LV Systolic Function is characterized automatically: Yes (EF = 50 - 70) = Normal (EF = 40 - 49) = Mildly impaired (EF = 30 - 39) = Moderately impaired (EF = less than 30%) = Severely impaired (EF = 71 Or greater) = Hyperdynamic
generated for ETT Nuclear Stress Tests for quick reference.
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
6
ICANL / IAC Nuclear Requirement Does Your Current Final Report Solution Always Comply With This Requirement?
How the Template Reporting System Complies With This Requirement
Identification of suboptimal or limited examinations and/ordeviations from standard protocols.
This may include attenuation (general soft tissue, breast, diaphragm), patient/organ motion (limb/body movement, upward creep of the heart), activity in nontarget organs (e.g., subdiaphragmatic activity on cardiac studies), or other imaging artifacts. (3.4.10.3A)
Always Compliant? YES NO
Corrective Action(s) Needed:
Overall study quality and up to 3 imaging artifacts per study may be chosen from prepopulated dropdowns.
Artifacts and deviations from standard protocols are quickly accommodated in your final reports For example, you can easily generate a report with no gated study and state that a patient’s A-Fib or frequent PVCs make the gated acquisition unobtainable. Or, you could qualify the gated study as possibly inaccurate due to A-Fib or frequent PVCs.
The presence of these data elements is error checked for.
An accurate, succinct impression (e.g., normal, abnormal, stable);
Comment: This must clearly communicate the result of the study and, when possible, answer the clinical question that was the cause for the examination. This final conclusion should resolve any inconsistencies or discrepancies (e.g., abnormal stress test with normal myocardial perfusion images) or provide guidance for further studies to do so. (3.4.11A )
Any need for additional studies based on the results of the procedure being reported. (3.4.12A)
Always Compliant? YES NO
Corrective Action(s) Needed:
The presence of a succinct overall impression is error checked for, and the Interpreting MD is notified if it is missing
Also, optional dropdowns are included with prepopulated common choices for “Answer the Clinical Question”, “Reconcile Disparate Stress Test and Imaging Findings”
Optional “Recommendations” dropdown addresses the need for any additional studies.
The final report must be reviewed and signed manually orelectronically by the interpreting qualified member of the medicalstaff.
Electronic signatures must be password protected and indicate they are electronically recorded.
Stamped signatures or signing by non-physician staff is unacceptable. (3.5.15A)
Always Compliant? YES NO
Corrective Action(s) Needed:
The Interpreting MD can enter their password to generate an electronic signature on the report.
If the report is to be printed and then faxed & scanned into an EHR, then we recommend that you manually sign.
If you electronically import your reports into your EHR, then use the password protected Electronic Signature & send the report via EHR task to Interpreting MD for final approval.
Very well-designed ...Quickly and easily produces complete, concise, well-organized and nice-looking reports that are free from errors. Very short learning curve. Single-page reports are quickly digestible and can’t get separated by referring providers’ offices.”
LEARN MORE about the Template Reporting System
Mark C. Goldberg, MD FACC Nuclear Interpreting Physician
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
7
ICANL / IAC Nuclear Requirement
3.4A (The) final report must be typed or computer generated and must accurately reflect the content and results of the study. This includes, but is not limited to:
identification of the name address and phone number of the facility; (3.4.1A)
Always Compliant? YES NO
Corrective Action(s) Needed:
We have a specific placeholder in the footer where you enter all of your laboratory’s required contact information.
patient’s first and last name gender and date of birth or age; (3.4.2A )
Always Compliant? YES NO
Corrective Action(s) Needed:
The presence of the NAME, GENDER, DATE OF BIRTH, and DATE OF STUDY fields are all error-checked for.
The patient’s AGE is computed, displayed, and used for calculating MPHR% achieved.
requesting health care provider’s name; (3.4.3A) Always Compliant? YES NO
Corrective Action(s) Needed:
You easily populate this dropdown with the names of your referring healthcare providers. Editing dropdowns is quick and easy.
The presence of this data element is error-checked for.
interpreting physician name; (3.4.4A) Always Compliant? YES NO
Corrective Action(s) Needed:
You easily populate this dropdown with the names of your Interpreting MDs.
The presence of this data element is error-checked for.
How the Template Reporting System Complies With This Requirement
Does Your Current Final Report Solution Always Comply With This Requirement?
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
8
ICANL / IAC Nuclear Requirement
date of the examination; (3.4.5A) Always Compliant? YES NO
Corrective Action(s) Needed:
You choose this from a “date-picker” calendar (usually you simply choose “today”).
The presence of this data element is error-checked for.
date report signed and approved by interpreting physician; (3.4.6A)
Always Compliant? YES NO
Corrective Action(s) Needed:
This defaults to today’s date when the MD completes the interpretation section and can be easily changed.
The presence of this data element is error-checked for.
clinical indications and pertinent history leading to the performance of the examination (e.g., medications, recent contrast, prior administration of radiopharmaceuticals, prior therapy which might affect radiopharmaceutical distribution, results of pertinent imaging studies and facility results); (3.4.7A)
Always Compliant? YES NO
Corrective Action(s) Needed:
All relevant conditions leading to the performance of the exam are included in the “History” and “Indications” dropdowns.
The “Indications” dropdowns are geared towards justifying the clinical need for the study, the reimbursbility of the study, and fulfillment of Appropriate Use Criteria.
The presence of these data elements is error checked for.
name of the procedure [type of examination(s)]; (3.4.8A) Always Compliant? YES NO
Corrective Action(s) Needed:
All Imaging Protocol Sections and Stress Sections are all clearly titled.
Simply set up your laboratory’s default templates so that these report section titles match the protocols described in your IAC Nuclear Policy and Procedure Manual.
How the Template Reporting System Complies With This Requirement
Does Your Current Final Report Solution Always Comply With This Requirement?
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
9
ICANL / IAC Nuclear Requirement
an adequate description of the procedure performed. The description must include the name of the procedure [type of the examination(s) or protocol].
It must also include the specific name specific amount and route of administration of any radioactive or non-radioactive material administered.
If applicable, the type of stress, pharmacologic agent, dose and route of administration must be described.
If applicable the type and use of attenuation correction must be specified (3.4.9A)
Always Compliant? YES NO
Corrective Action(s) Needed:
Did you know you can get dinged by a Recovery Audit Contractor for failing to document the route of administration of a radiopharmaceutical?
Every single report element mentioned here is included in all of our report templates. Dropdown values are prepopulated. The values that are always or almost always the same for every patient (route of administration, type of attenuation correction used, time between injection and imaging, type of imaging (SPECT, gated SPECT, prone, etc.) can be set to default values for your lab’s templates. You can quickly change these on an as-needed basis for unusual studies.
Also, quick choices for typical dosages of ancillary pharmaceuticals are available in dropdowns (100 mgs IV Aminophylline, .4 mgs sublingual Nitroglycerin, IV Lopressor, etc)
We focus on making software with:
A simple, quick and intuitive user interface
Error checking which allows for no omissions, no contradictions, noviolations of ICANL standards, and no departures from ASNC-standardized terminology
Sentence output that is totally accurate and grammatically perfect
Layout and design that presents relevant information in a quicklydigestible, visually appealing format for your referral base.
GET STARTED 100% Fully-Functioning, No-Risk
30-Day Trial
How the Template Reporting System Complies With This Requirement
Does Your Current Final Report Solution Always Comply With This Requirement?
Very helpful addition to our nuclear lab
It is intuitive to use, report creation is quick, andthe final report looks nice. … I would recommendthe software to any size physician group readingNuclear Cardiology studies to standardize thefinal report, which is the most important part of amyocardial perfusion study.
Chris Gilles MD ABNM Medical Director, ICANL Accredited Lab
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971
(All templates have been meticulously tested, improved, and tweaked on a daily basis, by the developer, over the course of 4 years in an ICANL accredited lab. There are absolutely no logical, grammatical, punctuation or sentence flow incongruities present in any of our templates.)

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
10
ICANL / IAC Nuclear Requirement
3.3A (The) final interpretation of examinations must be based on quality images/data as well as relevant clinical information. This includes, but is not limited to:
The Template Reporting System enables final interpretations to be based on all aspects of the patient / study
• The entire demographics, imaging protocol, and stress test sections of the report will be fully completed and viewable by the Interpreting MD when they open the final report to interpret the images
- If prior completion of the Stress section of the report is not possible due to time considerations, the Interpreting MD can easily glean relevant patient history and stress test results from our quicklydigestible comprehensive 1 page Stress Worksheet.
• Also, there is a “Technical” tab of the Image Interpretation User Interface in which the processing nuclear technologist describes the overall study quality, up to 3 artifacts, and a freetext area where theycan communicate with the Interpreting MD about any unusual or noteworthy aspects concerning the technical quality of the study. (All of these entries can be edited or erased by the Interpreting MD, and thefreetext comments never appear in the final report.)
Relevant clinical information (3.3.1A) Always Compliant? YES NO
Corrective Action(s) Needed:
Our clinical history dropdowns include just about every relevant condition seen over the course of 4 years in an IAC-Nuclear Accredited Nuclear Cardiology Lab. If you happen upon something odd, you can add it to the dropdown or type it in quickly.
Clinical indication/question (3.3.1A) Always Compliant? YES NO
Corrective Action(s) Needed:
Our Indications dropdowns include the history as above, plus other entries which are specifically geared towards phrasing things in away that justify the need for the study, justify reimbursement, and show how the indications meet Cardiac Radio Nuclide Imaging Appropriate Use Criteria (AUC).
Relevant patient response to stress (exercise or pharmacologic) or other pharmacologic intervention (including but not limited to symptoms, rest and stress heart rate/blood pressure data, rest and stress ECG findings etc., as appropriate for the type of stress or pharmacologic intervention).
This information must be included in the final report as noted in 3.4A. (3.3.2A)
Always Compliant? YES NO
Corrective Action(s) Needed:
All of these patient responses to stress are included in the stress worksheet, and are easily inputted into the final report These findings are already integrated into the final report by the time thNuclear Interpreting MD lays eyes on the images themselves.
He/she will open the final report in progress view the completed demographic, imaging protocol, and stress sections and THEN go on to interpret the nuclear images.
How the Template Reporting System Complies With This Requirement
Does Your Current Final Report Solution Always Comply With This Requirement?
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
11
ICANL / IAC Nuclear Requirement
Acceptable quality radionuclide images and/or derived quantitative data including acceptable: (3.3.3A)
count density (3.3.3.1A)
processing/filtering (3.3.3.2A
data display [includes image data (slice line-up, normalization, color, standardization, as relevant) and quantitative data (including ROI display, graphs, raw data, and calculated values, as relevant) (3.3.3.3A); and
lack of artifacts (e.g., patient motion, attenuation, subdiaphragmatic activity). (3.3.3.4A)
Always Compliant? YES NO
Corrective Action(s) Needed:
While our solution can’t directly improve the quality of your images, it does allow the nuclear medicine technologist who processed the study to select for the presence or absence of artifact(s), categorize the overall quality of the images, and leave freetext comments regarding the technical quality of the study for the Interpreting MD.
(These entries can be erased or overridden by the Interpreting MD and the freetext never finds its way into the final report)
Other relevant imaging modalities (i.e., echo/ultrasound, CT, MRI, etc.), if available. (3.3.4A)
Always Compliant? YES NO
Corrective Action(s) Needed:
Options in the History dropdowns are available for relevant pre-MPI imaging studies.
Comparison with prior nuclear medicine examinations when available. It is preferable that “no previous studies” be stated to document that there were none. (3.3.5A)
Always Compliant? YES NO
Corrective Action(s) Needed:
One simple dropdown click generates the “No previous studies available for comparison.” sentence in the IMPRESSION section.
(Note: since this is “preferable”, there is no error message generated should you choose not to include this element)
The integration of imaging and non-imaging information into a final impression that resolves any potential inconsistencies. (3.3.6A)
Always Compliant? YES NO
Corrective Action(s) Needed:
Prepopulated dropdown variables with common resolutions for inconsistent stress test and imaging results. (i.e. “Study is positive for evidence of reversible ischemia despite negative imaging findings due to the stress ECG findings.”)
You can also always enter any text you want, in the User Interface or in the final report – it s a Word document.
How the Template Reporting System Complies With This Requirement
Does Your Current Final Report Solution Always Comply With This Requirement?
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
12
ICANL / IAC Nuclear Requirement
Other IAC Nuclear Requirements relating to final reports:
Specific worksheets for non-imaging studies must be maintained as part of the facility records. (3.1.3A)
Always Compliant? YES NO
Corrective Action(s) Needed:
Comprehensive 1-page Stress Worksheet includes all relevant Stress Test Data (multiple pages tend to get separated and lost).
This Stress Worksheet is tightly coordinated to the Demographics and Stress Test section of our Report Templates for quick, accurate, and easy data entry.
The final report must be reviewed signed and dated manually or electronically by the interpreting qualified member of the medicalstaff.
Electronic signatures must be password protected and indicate that they are electronically recorded.
Stamped signatures or signing by non-physician staff is unacceptable.
Comment: In unusual circumstances, when the interpreting physician is not available, another qualified member of the medical staff may sign for them, if they choose to take such responsibility. (3.2.4A)
Always Compliant? YES NO
Corrective Action(s) Needed:
Interpreting MDs can Electronically sign Final Reports through the use of a password.
Note:
As always, it is the responsibility of your lab that your overall IT environment complies with HIPPA/HITECH.
If you are going to be first printing and then faxing, or printing and scanning your final reports it is recommended that you have the Interpreting MD physically sign and date the printed document, and then transmit it.
If you are going to import our reports into an EHR, you should use the electronic signature function, but send the report to the Interpreting MD in the EHR system for a final sign-off
The final signed report must be transmitted to the referring health care provider within two working days. (3.2.5A)
Always Compliant? YES NO
Corrective Action(s) Needed:
Using our recommended file management system there will always be an open folder called “Ready to be Read” and “Read” containing studies not yet transmitted on the Reading Room Computer.
The date of study is clearly visible as a part of the Final Report Filename, so it is easy to see at-a-glance if there are studies that are approaching the 2 working day deadline.
There must be a system for identification and retrieval of a patient’s prior similar studies for comparison. (3.2.6A)
Always Compliant? YES NO
Corrective Action(s) Needed:
While our solution can’t help with your image archives, there is quick and easy functionality for building sentences that compare the current study to previous studies in relevant terminology.
How the Template Reporting System Complies With This Requirement
Does Your Current Final Report Solution Always Comply With This Requirement?
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

The Definitive Guide and Checklist for IAC Nuclear | ICANL Final Report Standards Compliance
13
... a very well written and supported application that
makes … documentation for the signing physician easy, clear, concise and correctly communicated.
We have been extremely pleased with the software and would recommend … to anybody looking for an affordable solution for documentation.
We are very pleased with our choice."
-- Jeffrey Harris Lead Technical Analyst
SSM Integrated Health Technologies
Other Benefits of the Template Reporting System•
•
Perfect Spelling, Grammar, Punctuation & Sentence Flow
•
Fast and Easy: Simple, Quick & Intuitive User Interface
Visually Appealing, Quickly Digestible Reports Please Referring MDs
•
Professional Layout & Design. Comprehensive, Clear & Concise. Single-page Reports can't get separated by Referring MDs.
•
Extreme Attention to Detail Protects You from RACs, Shows Clinical Justification for the Test & Fulfillment of Appropriate Use Criteria
• Inexpensive: A Low One-Time Fee, No Recurring Payments
GET STARTED WITH A FREE TRIAL NOW
Your 30-day trial is:
• Free. No credit card required
• 100% fully functioning
• No risk. If you need the trial period extended, just contact us
• Easy to learn - Concise video tutorials on the website preciselydemonstrate every aspect of use & customization
•
Remote help is available for demonstration, training, andcustomization of your templates
•
You keep the final patient reports created during the trial period.Those are yours forever, even if you do not buy the software
Fast and super-easy to use after you’ve read about 7 studies
-- Mark C. Goldberg, MD FACC
Nuclear Interpreting Physician
www.NuclearCardiologyReports.com | [email protected] | Call or text: 1 (520) 429-9971

www.NuclearCardiologyReports.com [email protected]
Call or text: 1 (520) 429-9971
Share this Guide & Checklist on