IBS Presentation
32
1 IRRITABLE BOWEL SYNDROME IRRITABLE BOWEL SYNDROME (IBS) (IBS) Dr. Muhammad Imran Associate` Professor Medicine Services Institute of Medical Sciences Visiting Physician & Gastroenterologist
-
Upload
pk-doctors -
Category
Health & Medicine
-
view
8.700 -
download
2
description
A presentation on IBS, from P.S.F.P.
Transcript of IBS Presentation

1
IRRITABLE BOWEL SYNDROMEIRRITABLE BOWEL SYNDROME (IBS)(IBS)
Dr. Muhammad Imran
Associate` Professor MedicineServices Institute of Medical SciencesVisiting Physician & GastroenterologistServices Hospital, Lahore.

2
Functional bowel disorderFunctional bowel disorder
……. is a functional gastrointestinal . is a functional gastrointestinal disorder with symptoms attributable disorder with symptoms attributable to the mid or lower gastrointestinal to the mid or lower gastrointestinal tract. The symptoms include tract. The symptoms include abdominal pain, bloating or abdominal pain, bloating or distension and various symptoms of distension and various symptoms of disordered defecation.disordered defecation.
Thompson Thompson et alet al, 1992, 1992

3
IBS: HistoryIBS: History ‘…‘….occasional pain in the intestines and derangement of their .occasional pain in the intestines and derangement of their
powers of digestion, powers of digestion, with flatulence and a sense of suffocation’with flatulence and a sense of suffocation’
Practical remarks on the discrimination and successful Practical remarks on the discrimination and successful treatment of spasmodic stricture treatment of spasmodic stricture of the colonof the colon
‘…‘…. the bowels are at one time constipated, at . the bowels are at one time constipated, at another lax, in the same person.…’another lax, in the same person.…’
Cumming, 1849Cumming, 1849
Howship, 1830Howship, 1830
Powell, 1820Powell, 1820

4
IBS: HistoryIBS: History
‘…‘…. a tenacious mucus, which may be . a tenacious mucus, which may be slimy and gelatinous, like frog-spawn….’slimy and gelatinous, like frog-spawn….’
Mucous colitisMucous colitis
Neurogenic mucous colitisNeurogenic mucous colitisBockus Bockus et alet al, 1928, 1928
Hurst, 1921Hurst, 1921
Osler, 1892Osler, 1892

5
IBS: 1992IBS: 1992
……. a functional bowel disorder in which . a functional bowel disorder in which abdominal pain is associated with abdominal pain is associated with defecation or a change in bowel habitdefecation or a change in bowel habit, and , and with disordered defecation and with with disordered defecation and with distensiondistension..
Thompson Thompson et alet al, 1992, 1992

6
IBS: 1999IBS: 1999
……. comprises a group of functional bowel. comprises a group of functional boweldisorders in which abdominal discomfort or disorders in which abdominal discomfort or pain is associated with defecation or a pain is associated with defecation or a change in bowel habit, and with features of change in bowel habit, and with features of disordered defecation.disordered defecation.
Thompson Thompson et alet al, 1999, 1999

7

8
The Epidemiology of The Epidemiology of Irritable Bowel Syndrome Irritable Bowel Syndrome
(IBS)(IBS)

9
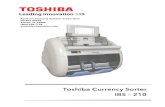
World Prevalence of IBSWorld Prevalence of IBS
Adapted from Camilleri M, et al. Aliment Pharmacol Ther. 1997;11:3.
Muller-Lisners et al. Digestion. 2001;64:200.
Canada
13.5%
US 10-20%
Peru
18%
Nigeria 30%
France 9.4%
UK 22%
Australia 12%
New Zealand 17%
China 23%
Japan 25%
Germany 12%

10
14%14%
14%14%
20%20%
9%9%7-8%7-8%
13%13%
13%13%
25%25%
10%10%
13%13%22%22% 9%9%
12%12%15%15%12%12% 17%17%
IBS: PrevalenceIBS: Prevalence

11
Disease prevalenceDisease prevalence
25% of patients examined by a G.P. suffer from a 25% of patients examined by a G.P. suffer from a gastrointestinal disorder, IBS being the most gastrointestinal disorder, IBS being the most
frequentfrequent
Source: American Gastroenterological Association Patients Care Committee, 1997

12
Prevalence of IBS

13
The Diagnosis of The Diagnosis of Irritable Bowel Syndrome Irritable Bowel Syndrome
(IBS)(IBS)

14
The The PositivePositive Diagnosis of IBS: Diagnosis of IBS:A Symptom-Based ApproachA Symptom-Based Approach
Adapted from Paterson et al. Adapted from Paterson et al. Can Med Assoc J.Can Med Assoc J. 1999;161:154. 1999;161:154.American Gastroenterological Association. American Gastroenterological Association. Gastroenterology.Gastroenterology. 1997;112:2120. 1997;112:2120.
Identify Current Primary SymptomIdentify Current Primary SymptomssIdentify Current Primary SymptomIdentify Current Primary Symptomss
Look for ‘Red Flags’ Based on:Look for ‘Red Flags’ Based on: HistoryHistory Physical examPhysical exam Laboratory testsLaboratory tests
Perform Selected PPerform Selected Physical andhysical and Diagnostic DiagnosticTTests ests to Rule Out Organic Diseaseto Rule Out Organic Disease
MakeMake a Positive Diagnosisa Positive Diagnosis
Abdominal pain / discomfort Bloating Constipation/Diarrhea
Abdominal pain / discomfort Bloating Constipation/Diarrhea

15
Identify Identify RRed ed FFlagslags
HistorHistoryy Unintentional weight lossUnintentional weight loss Onset in older patient (>50 Onset in older patient (>50
years)years) Family Family history ofhistory of cancercancer or IBD or IBD
Initial Initial llabsabs HGBHGB WBCWBC ESRESR Abnormal chemistryAbnormal chemistry TSHTSH
PhysicalPhysical Abnormal examsAbnormal exams Rectal bleeding / obstructionRectal bleeding / obstruction Positive flexible Positive flexible
sigmoidoscopy or sigmoidoscopy or colonoscopy (>50 years)colonoscopy (>50 years)
Adapted from a technical review. Adapted from a technical review. Gastroenterology.Gastroenterology. 1997;112:2120. 1997;112:2120.Paterson et al. Paterson et al. Can Med Assoc J.Can Med Assoc J. 1999;161:154. 1999;161:154.Camilleri et al. Camilleri et al. Aliment Pharmacol Ther.Aliment Pharmacol Ther. 1997;11:3. 1997;11:3.
Red FlagsRed Flags

16
The balance of IBS diagnosis

17
IBS: Rome criteria (1992)IBS: Rome criteria (1992)At least 3 months continuous or recurrent symptoms of:
1. abdominal pain or discomfort which is: a. relieved with defecation, b. and/or associated with a change in frequency of stool, c. and/or associated with a change in consistency of stool; and 2. two or more of the following, at least a quarter of occasions or days: a. altered stool frequency, b. altered stool form (lumpy/hard or loose/watery), c. altered stool passage (straining or urgency, feeling of
incomplete evacuation), d. passage of mucus, e. bloating or feeling of abdominal distension.
Thompson Thompson et alet al, 1992, 1992

18
IBS: Rome II criteria (1999)IBS: Rome II criteria (1999)
At least 12 weeks, which need not be consecutive, in the preceding 12 months of abdominal discomfortor pain that has two of three features:
relieved with defecation; and/or onset associated with a change in frequency of
stool; and/or onset associated with a change in form
(appearance) of stool.
Thompson Thompson et alet al, 1999, 1999

19
IBS: Rome II criteria (1999)IBS: Rome II criteria (1999)
The following symptoms cumulatively support the diagnosis of IBS:
abnormal stool frequency; abnormal stool form (lumpy/hard or loose/watery
stool); abnormal stool passage (straining, urgency, or
feeling of incomplete evacuation); passage of mucus; bloating or feeling of abdominal distension.
Thompson et al, 1999

20
Rome III – Irritable Bowel Rome III – Irritable Bowel SyndromeSyndrome
Diagnostic Criteria* for Irritable Bowel SyndromeDiagnostic Criteria* for Irritable Bowel Syndrome
Recurrent abdominal pain or discomfort** at least 3 days Recurrent abdominal pain or discomfort** at least 3 days per month in the last 3 months associated with 2 or more of per month in the last 3 months associated with 2 or more of the following:the following: Improvement with defecationImprovement with defecation Onset associated with a change in frequency of stoolOnset associated with a change in frequency of stool Onset associated with a change in form (appearance) of stoolOnset associated with a change in form (appearance) of stool
*Criteria fulfilled for the last 3 months with symptom onset at least 6 months*Criteria fulfilled for the last 3 months with symptom onset at least 6 months
prior to diagnosis.prior to diagnosis.
**Discomfort means an uncomfortable sensation not described as pain.**Discomfort means an uncomfortable sensation not described as pain.
Gastroenterology 2006;130:1480-1491Gastroenterology 2006;130:1480-1491

21
Rome III – Irritable Bowel SyndromeRome III – Irritable Bowel Syndrome
http://www.medscape.com/viewarticle/533460http://www.medscape.com/viewarticle/533460
Subtyping Irritable Bowel Syndrome (IBS)Subtyping Irritable Bowel Syndrome (IBS)
The Rome II committee subclassified IBS on the basis of expert The Rome II committee subclassified IBS on the basis of expert opinion and attempted to incorporate stool frequency, stool opinion and attempted to incorporate stool frequency, stool form, and defecation symptoms. form, and defecation symptoms.
In the Rome III the subclassification was revised to be based In the Rome III the subclassification was revised to be based solely on solely on stool consistencystool consistency, which has been supported by , which has been supported by recent studies.recent studies.
Subclassification of IBS is important because it would likely be Subclassification of IBS is important because it would likely be associated with different treatment choices and associated with different treatment choices and pathophysiologic mechanisms.pathophysiologic mechanisms.

22
Rome III – Irritable Bowel SyndromeRome III – Irritable Bowel Syndrome
Sub typing IBS by Predominant Stool PatternSub typing IBS by Predominant Stool Pattern
Gastroenterology 2006;130:1480-1491Gastroenterology 2006;130:1480-1491
Patients with IBS-M have both hard and loose stools over periods of hours or days, whereas IBS patients with alternating bowel habits change subtype over periods of weeks and months.

23
IBS: Further evaluationIBS: Further evaluation
SigmoidoscopySigmoidoscopy Examination of stoolExamination of stool Blood studiesBlood studies Imaging studiesImaging studies
Drossman, 1997; 1999

24
The Pathophysiology of The Pathophysiology of Irritable Bowel Syndrome Irritable Bowel Syndrome
(IBS)(IBS)

25
IBS: Evolving understandingIBS: Evolving understanding
1950 1960 1970 1980 1990 2000
Abnormal motor function
Visceral hyperalgesia
Brain-gut interaction
5-HT mediated visceralsensitivity and gut motility
Drossman et al, 1999

26
IBS PathophysiologyIBS Pathophysiology
Adapted from Camilleri and Choi. Adapted from Camilleri and Choi. Aliment Pharmacol Ther.Aliment Pharmacol Ther. 1997;11:3. 1997;11:3.
EnhancedEnhancedPerceptionPerception
Sympathetic Sympathetic
VagalVagalNucleiNuclei
5-HT5-HT
AlteredAlteredMotilityMotility
VisceralVisceralHypersensitivityHypersensitivity

27
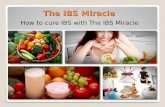
IBS: Quality of lifeIBS: Quality of lifeComparison with other diseasesComparison with other diseases
30
40
50
60
70
80
90
Physic
al fu
nctio
ning
Physic
al fu
nctio
ning
Role p
hysic
al
Role p
hysic
al
Body pai
n
Body pai
n
Gener
al h
ealth
Gener
al h
ealth
Vitalit
y
Vitalit
y
Social
funct
ionin
g
Social
funct
ionin
g
Role e
motio
nal
Role e
motio
nal
Men
tal h
ealth
Men
tal h
ealth
MeanMeanSF-36SF-36scorescore
National normativeNational normativevaluevalue
Diabetes type IIDiabetes type II
IBSIBS
Clinical depressionClinical depression
Wells Wells et alet al, 1997, 1997

28
IBS: Negative impact on IBS: Negative impact on quality of lifequality of life
Theoretical normative valueTheoretical normative value
Hahn Hahn et alet al, 1997, 1997
MeanMeanIBSQOLIBSQOL
scorescore
30
40
50
60
70
80
90
100
Emotio
nal
Emotio
nal
Men
tal h
ealth
Men
tal h
ealth
Sleep
Sleep
Energy
Energy
Physic
al fu
nctio
ning
Physic
al fu
nctio
ning
Diet
Diet
Social
role
Social
role
Physic
al ro
le
Physic
al ro
le
Sexual
rela
tions
Sexual
rela
tions
IBSIBS

29
The Management ofThe Management ofIrritable Bowel SyndromeIrritable Bowel Syndrome
(IBS)(IBS)

30
DOCTORDOCTOR
IBS: Patient's concernsIBS: Patient's concerns
What is IBS?What is IBS?
Do I haveDo I havecancer?cancer?
I can't lead I can't lead a normal lifea normal life
I can’t talk I can’t talk to anyoneto anyone about itabout it
Where is Where is the toilet?the toilet?
Can it be Can it be treated?treated?

31
TREATMENTTREATMENT
PATIENT EDUCATIONPATIENT EDUCATION DIETARY INTERVENTIONDIETARY INTERVENTION PHARMACOTHERAPYPHARMACOTHERAPY PSYCHOTHERAPY/COGNITIVE AND PSYCHOTHERAPY/COGNITIVE AND
BAHAVIOR THERAPYBAHAVIOR THERAPY HYPNOTHERAPYHYPNOTHERAPY

32
Drug Treatment of IBSDrug Treatment of IBSAbdominal pain/discomfortAbdominal pain/discomfort• Antispasmodics• Antidepressants
— TCAs/SSRIs
Bloating and distentionBloating and distention• Antiflatulents• Antispasmodics• Dietary modification
ConstipationConstipation• Fiber• Laxatives• PEG solutions
DiarrheaDiarrhea• Opioids—Loperamide
• Cholestyramine
AbdominalAbdominalpain/pain/
discomfortdiscomfort
Bloating/Bloating/distentiondistention
Altered bowelAltered bowelfunctionfunction
None of these medications effectively treat the multiple symptoms of IBS; they may exacerbate individual symptoms (eg, fiber and bloating, antispasmodic, constipation).