
IBD and Bone Health in Adults and Children - Imedex, LLCvid.imedex.com/pdf/5477/sylvester.pdf ·...
54
IBD and Bone Health in Adults and Children Francisco A. Sylvester, MD Associate Professor of Pediatrics
Transcript of IBD and Bone Health in Adults and Children - Imedex, LLCvid.imedex.com/pdf/5477/sylvester.pdf ·...

IBD and Bone Healthin Adults and Children
Francisco A. Sylvester, MDAssociate Professor of Pediatrics

GoalsT i b i b bi l• To review basic bone biology
• To understand the principles of DXA and its pitfalls
• To examine how IBD subverts normal bone function
• To review therapeutic options to increase BMD in patients with IBD

Bone And IBD
• Decreased bone mineral density– Males = Females– CD = UC (?)
• Fracture risk?– Vertebral fractures
Bernstein CN et al. Ann Intern Med 2000;133:795Bernstein CN et al. Gastroenterology 2003;124:795Heijckmann AC et al. Eur J Gastroenterol Hepatol 2008;20:740Semeao EJ et al. Gastroenterology 1997;112:1710Siffledeen JS et al. Clin Gastroenterol Hepatol 2007;5:721

Vertebral Fractures - IBD
Klaus J et al. Gut. 2002 Nov;51(5):654-8

Goal
To review basic bone biology

Compact Bone
Haversian System
Lamellae
Osteocytes
Periosteum
80% Bone Mass
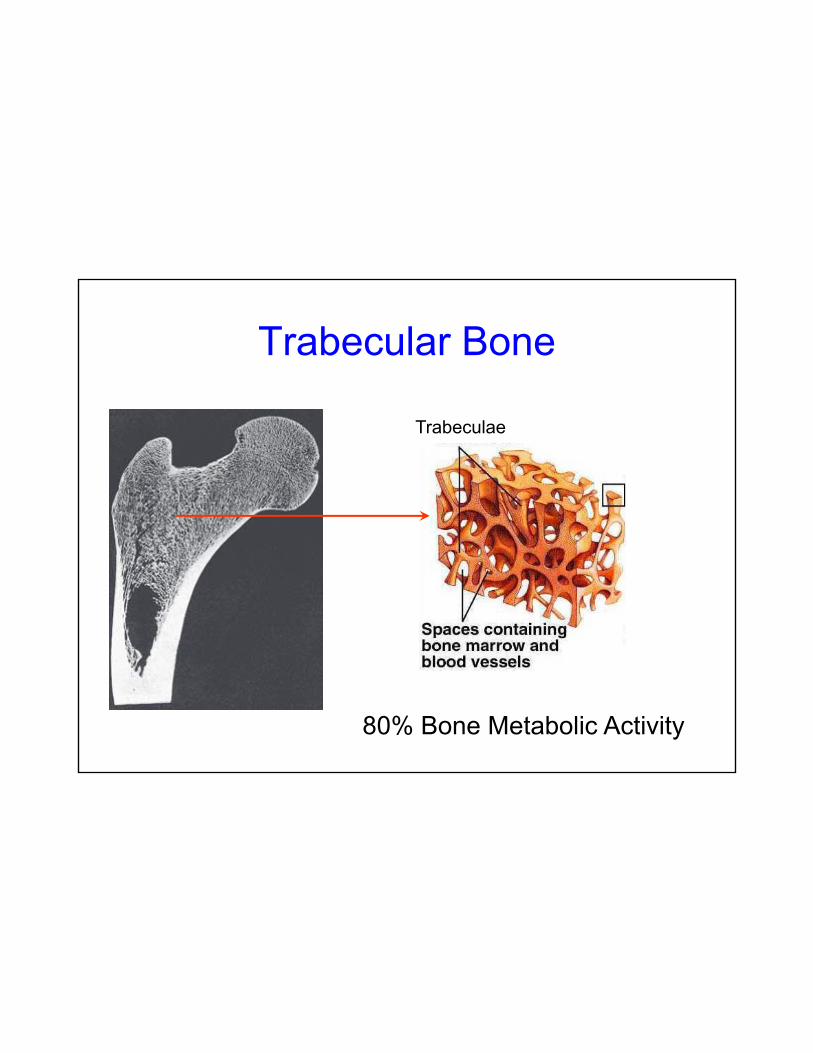
Trabecular Bone
Trabeculae
80% Bone Metabolic Activity
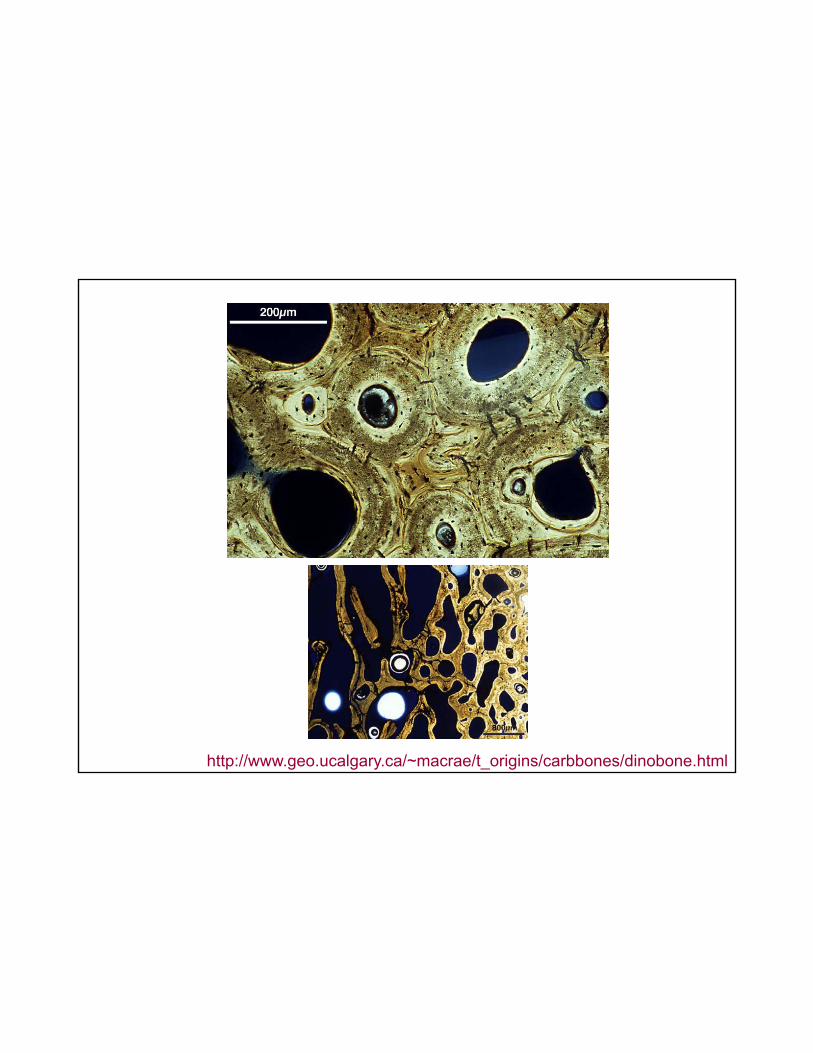
http://www.geo.ucalgary.ca/~macrae/t_origins/carbbones/dinobone.html

Osteoclasts
OC
OC
OC
OC
Sylvester FA, E Canalis 2006

Osteoblasts
E Canalis
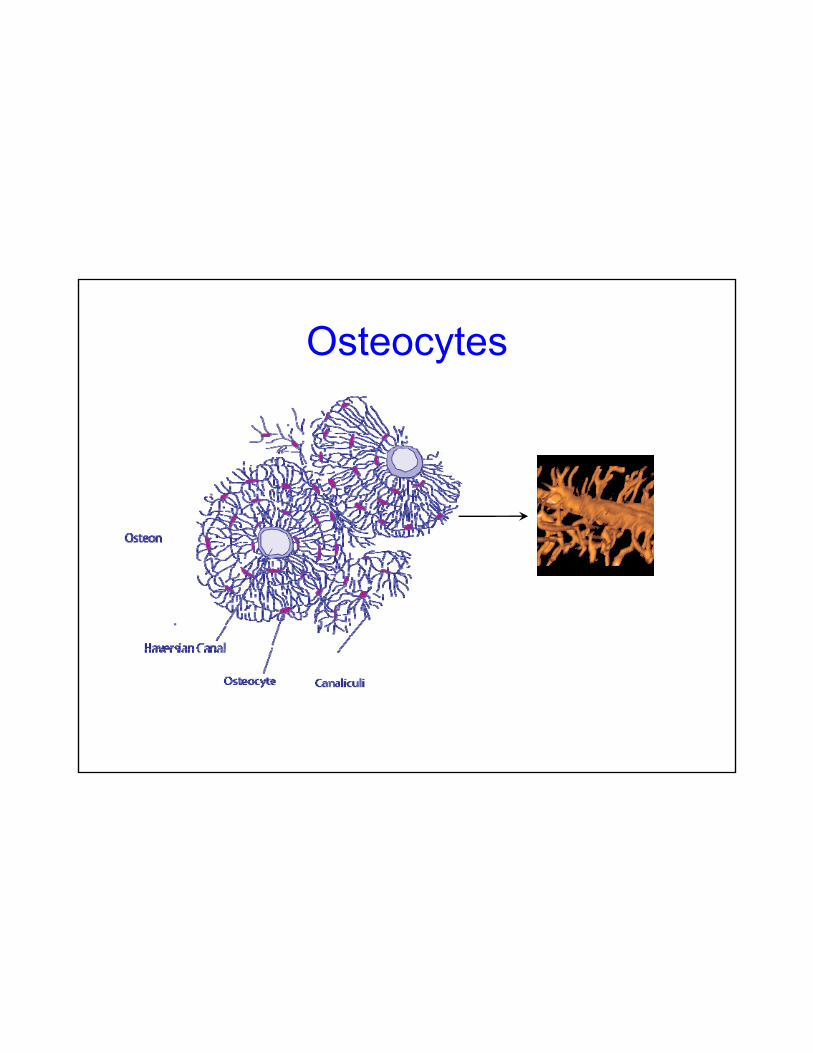
Osteocytes
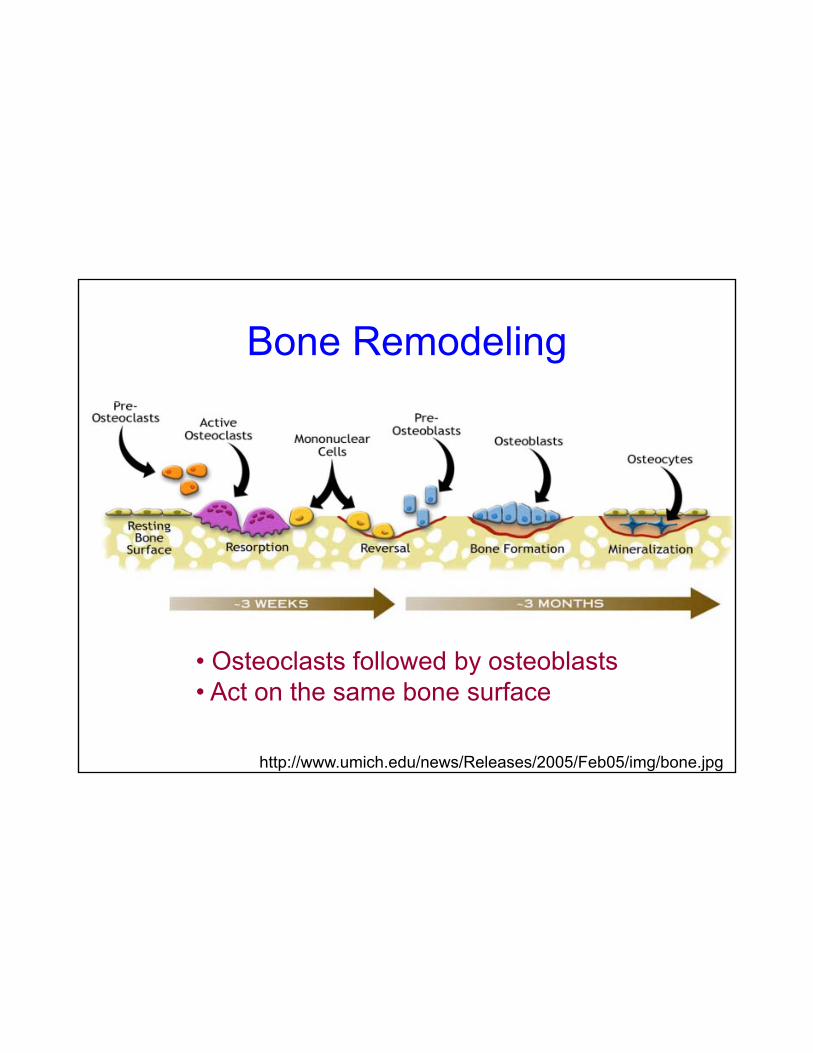
Bone Remodeling
• Osteoclasts followed by osteoblasts• Act on the same bone surface
http://www.umich.edu/news/Releases/2005/Feb05/img/bone.jpg
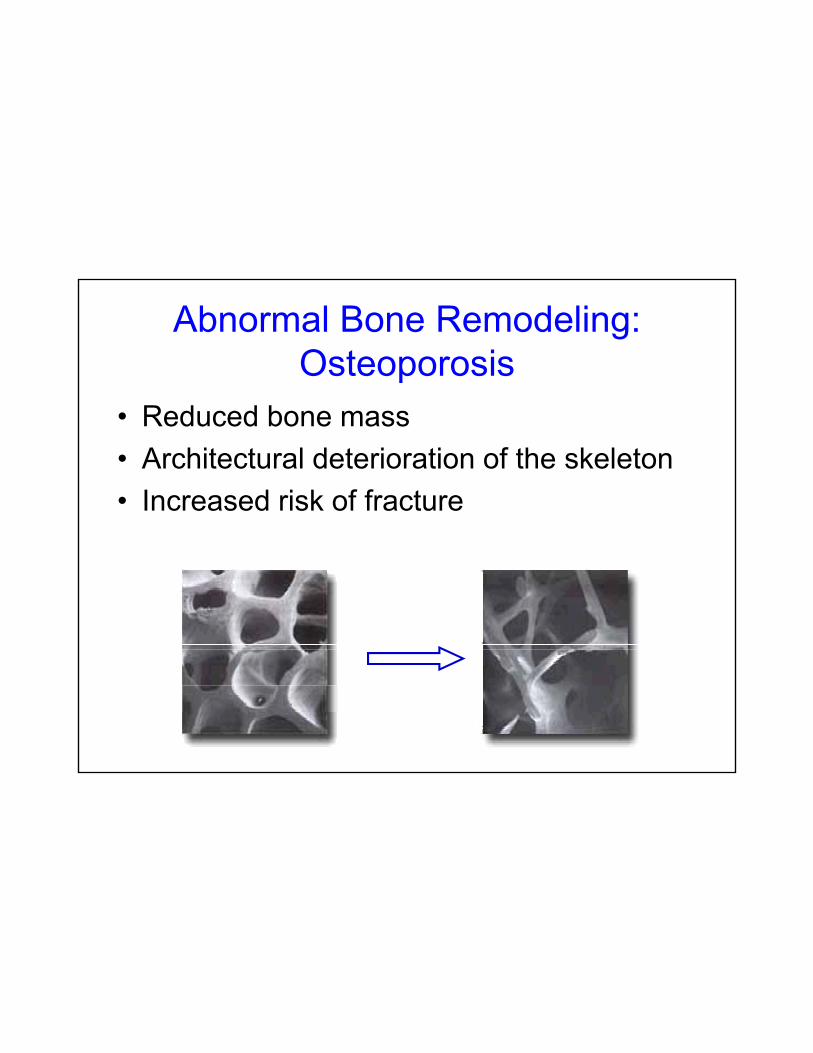
Abnormal Bone Remodeling: Osteoporosis
• Reduced bone mass• Architectural deterioration of the skeleton• Increased risk of fracture
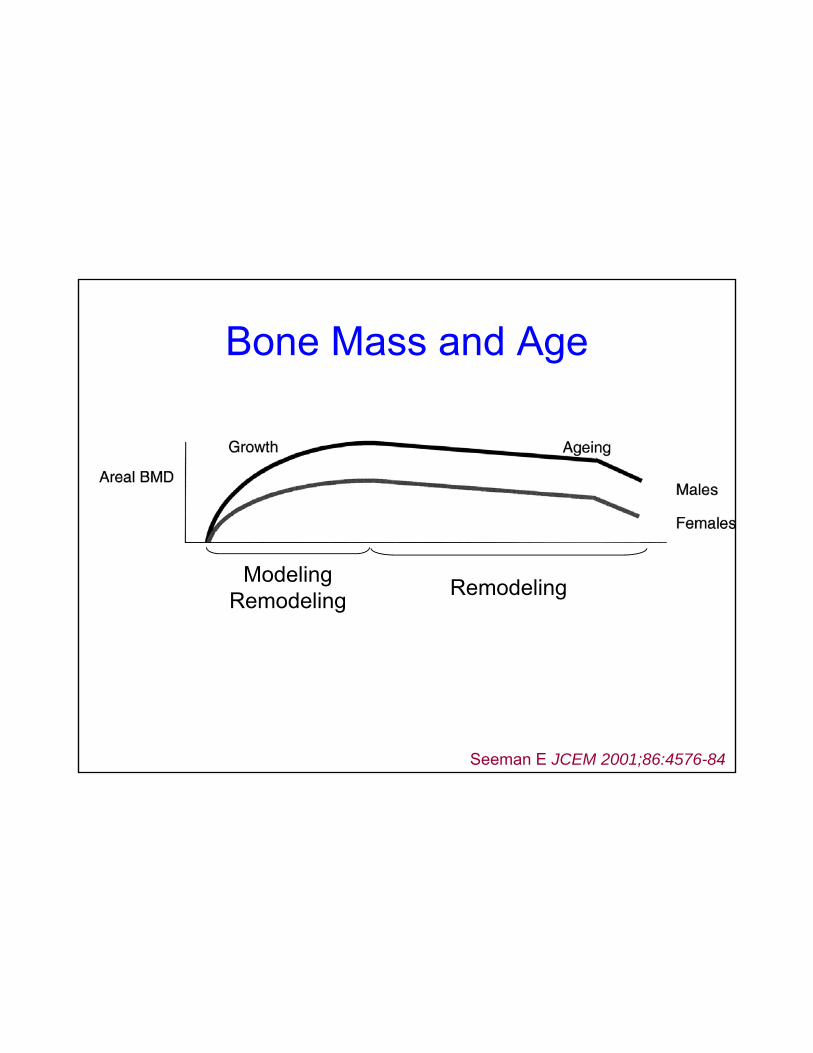
Bone Mass and Age
ModelingRemodeling Remodeling
Seeman E JCEM 2001;86:4576-84
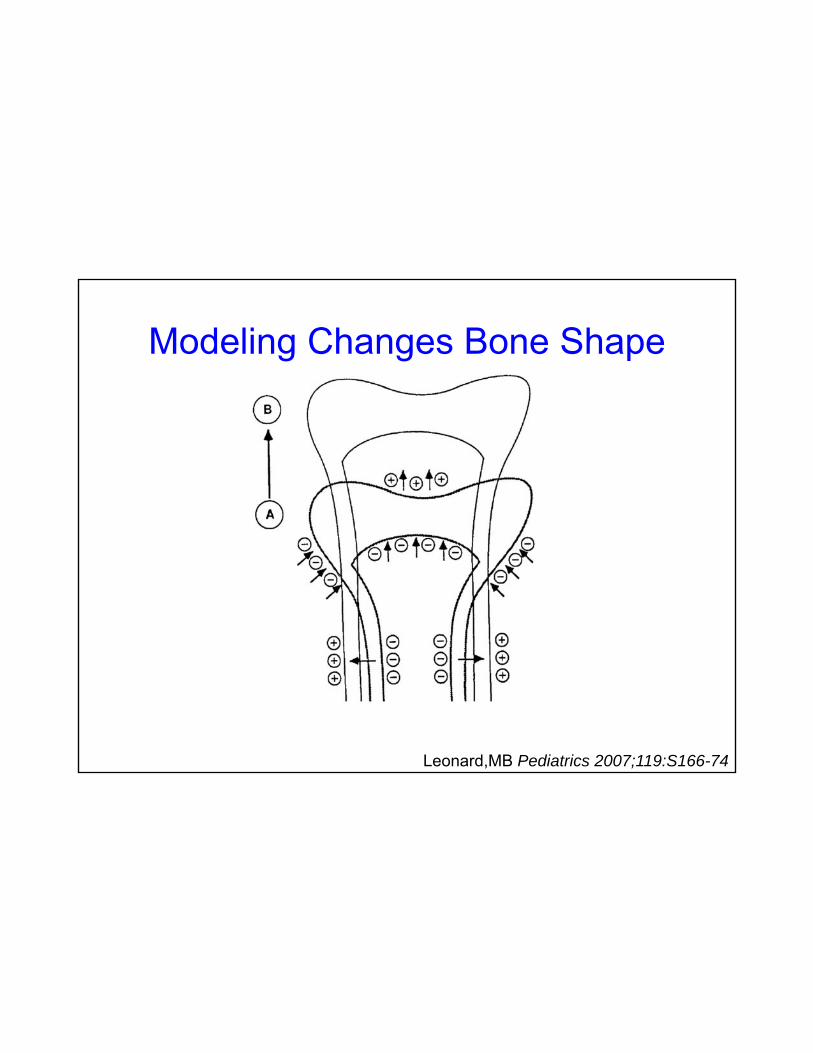
Modeling Changes Bone Shape
Leonard,MB Pediatrics 2007;119:S166-74

Determinants of Bone Mass
Inactivity
EndocrineDisorders Inflammation
GeneticsMedications
Poor Nutrition
ChronicIllness

Goal
To understand the principles of DXA and its pitfalls

DXA Technology
Patient
Detector (detects 2 tissue types - bone and soft tissue)
Photons
Patient
X-ray Source (produces 2 photon energies with different attenuation profiles)
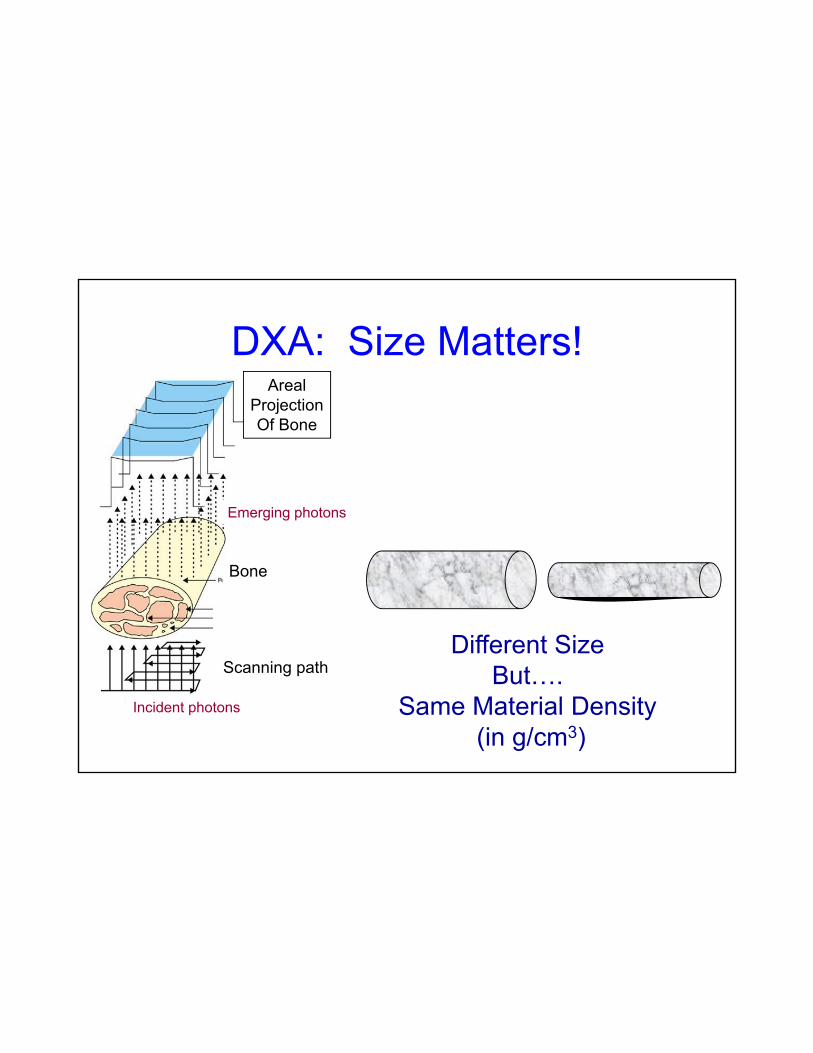
DXA: Size Matters!Areal
Projection
Emerging photons
ProjectionOf Bone
Bone
Different SizeScanning path
Incident photons
Different Size But….
Same Material Density (in g/cm3)
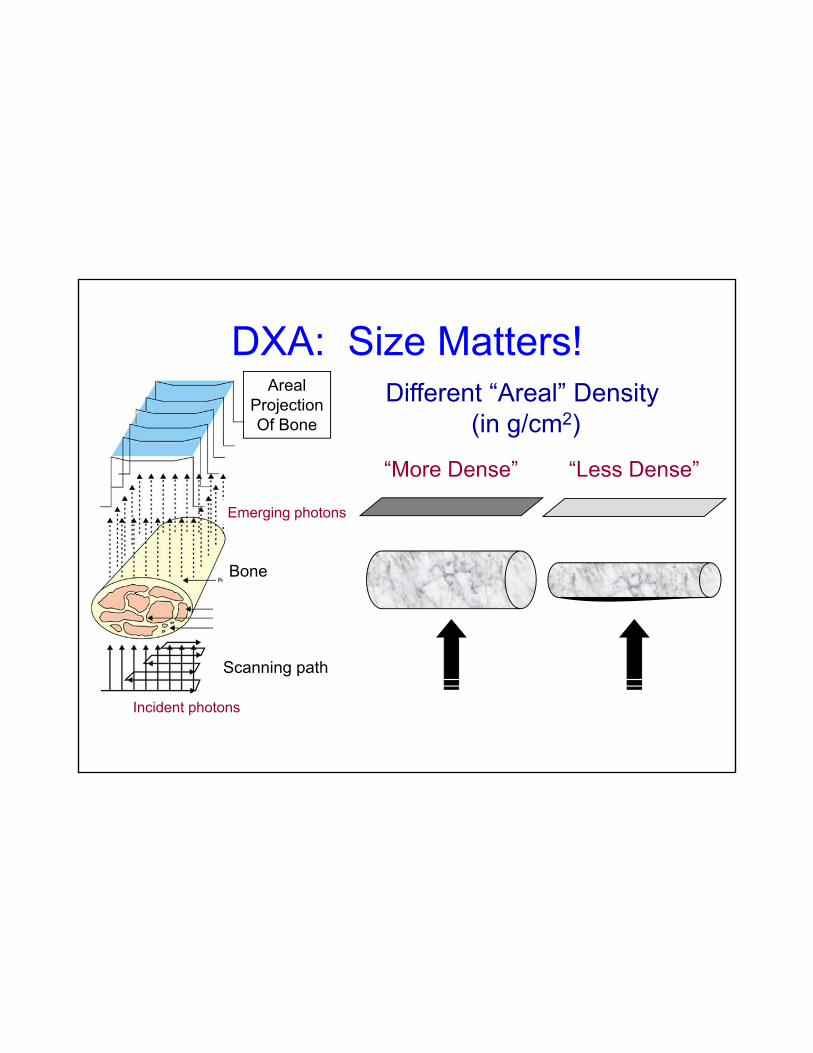
DXA: Size Matters!Areal
Projection Different “Areal” Density
Emerging photons
ProjectionOf Bone
“More Dense” “Less Dense”
y(in g/cm2)
Bone
Scanning path
Incident photons

Reporting DXAT- scores vs. Z-scores
= BMD (Observed – Normal for Age/Sex)SD
= BMD (Observed – Normal for Young Adult)SD

Definition of Osteoporosis
WHO d fi iti (2000) b d T• WHO definitions (2000) based on T-score– > -1 = Normal– < -1 but > -2.5 = Osteopenia– < -2.5 = Osteoporosis
• Only applicable to post-menopausal women
• Not intended as thresholds for treatment
• Not validated in patients with IBD
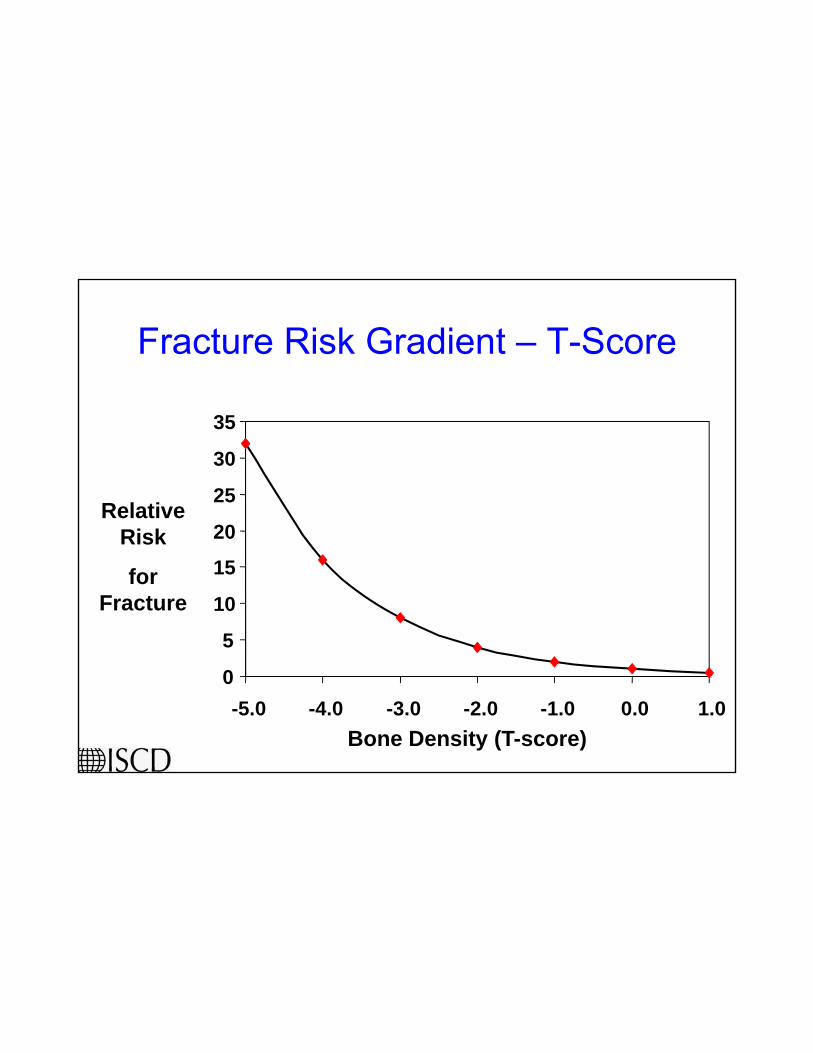
Fracture Risk Gradient – T-Score
Relative 20
25
30
35
Risk
for Fracture
5
10
15
20
Bone Density (T-score)
0-5.0 -4.0 -3.0 -2.0 -1.0 0.0 1.0
Age
8050
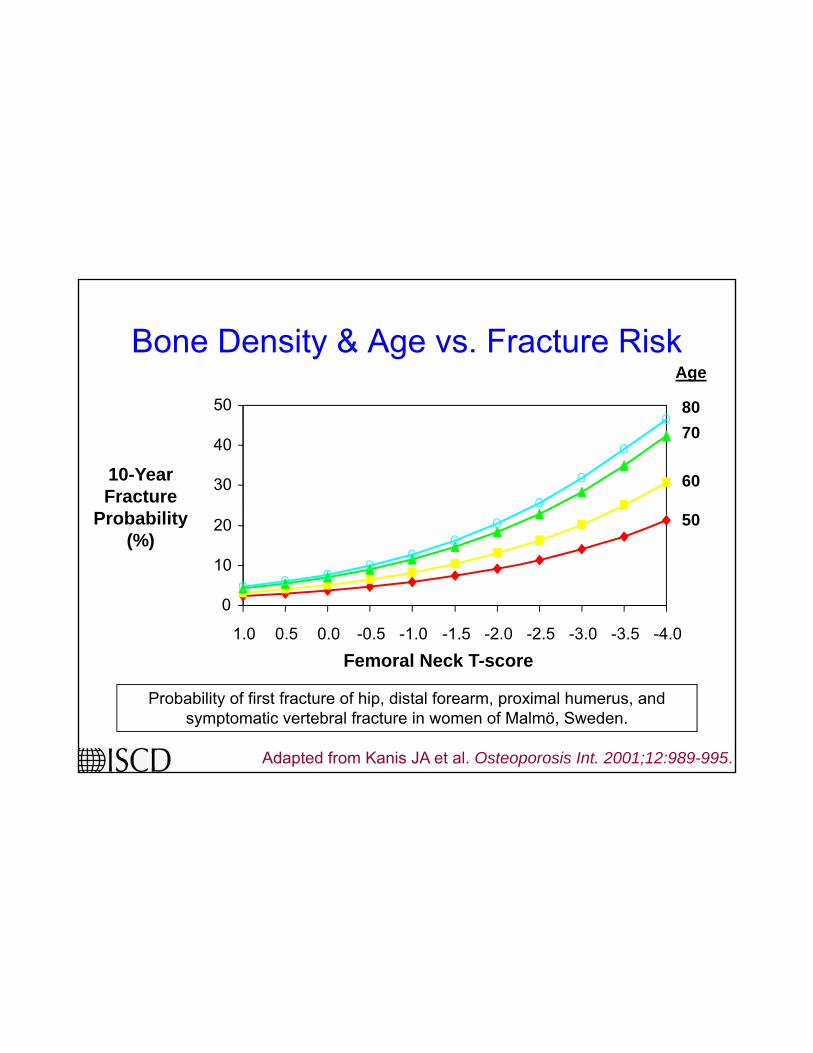
Bone Density & Age vs. Fracture Risk
10-Year Fracture
Probability
8070
60
5020
30
40
50
y(%)
0
10
20
1.0 0.5 0.0 -0.5 -1.0 -1.5 -2.0 -2.5 -3.0 -3.5 -4.0
Adapted from Kanis JA et al. Osteoporosis Int. 2001;12:989-995.
Probability of first fracture of hip, distal forearm, proximal humerus, and symptomatic vertebral fracture in women of Malmö, Sweden.
Femoral Neck T-score
Who Should Have DXA?
• Pre-existing fragility fracture• > 65 years of age• Patients with risk factors for low
BMD/f tBMD/fracture• Exposure to glucocorticoids ≥ 3 months• Consider repeating in 6 – 12 months
Lichtenstein GR et al. Inflamm Bowel Dis 2006;12:797-813
Vertebral Fractures – Crohn Disease
C ti l l f t b l• Cross-sectional prevalence of vertebral fractures
• 224 patients – 70 (36%) normal BMD70 (36%) normal BMD– 123 (51%) osteopenia– 31 (13%) osteoporosis
• Mean age 38.7± 11.8 y• 45 patients – 88 fractures
– 16 with normal BMD
Siffledeen J et al. Clin Gastroenterol Hepatol 2007;5:721-8

Goal
To examine how IBD subverts normal bone function
IBD - Bone
• Malnutrition• Malabsorption• Decreased physical
activityactivity• Delayed puberty• Medications• Inflammation

Hypothesis
IBD:A Gut BoneA Gut – Bone
Axis?

Gut – Bone Axis Candidates
• Immunological factors– Soluble factors– Cells (circulating/local)
• Nutritional deficiencies– Direct effects– Indirect effects
• Body compositionBody composition• Hormonal axes

Infliximab – Bone BiomarkersLuminal Crohn
Fistulizing Crohn
Franchimont N et al. Aliment Pharmacol Ther 2004;20:607
Pediatric Bone ≠ Adult Bone!
www.keithryan.com/Images/strongbaby.jpg

Effect of InfliximabREACH Study
100
140
1000
1400
1800BSAP (U/L) CTX (μg/μmol Cr)
20
60
Baseline Week 10
200
600
1000
Baseline Week 10
Thayu M et al. Bone 2007;40: 6(Supplement 1): S81
Baseline Week 10 Baseline Week 10
% Change 109 ± 97P<0.001
% Change 43 ± 78P<0.001
IBD - Infliximab – Bone
• Increased markers of bone formation• No effect on resorptive markers in adults• Increased bone turnover in children• Improved BMD
Franchimont N et al. Aliment Pharmacol Ther 2004;20:607.Ryan BM, et al. Aliment Pharmacol Ther 2004;20:851.Bernstein M, et al. Am J Gastroenterol 2005;100:2031.Abreu MT, et al. J Clin Gastroenterol 2006;40:55.Pazianas M, et al. Ann N Y Acad Sci 2006;1068:543Thayu M et al. Bone 2007;40: 6(Supplement 1): S81

Osteoclasts
OC
OC
OC
OC
Sylvester FA, E Canalis 2006
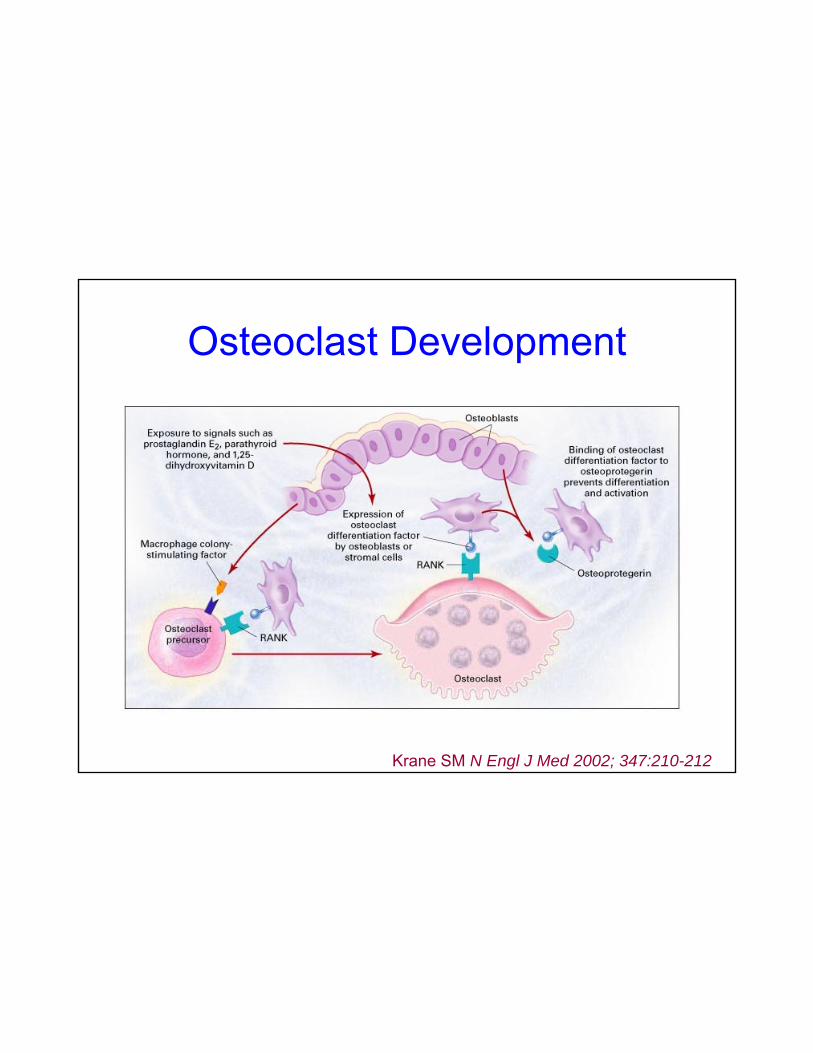
Osteoclast Development
Krane SM N Engl J Med 2002; 347:210-212

IBD – RANKL – OPG
M d t i i OPG/ RANKL• Modest increases in serum OPG/sRANKL
• OPG and BMD inversely correlated
In mice OPG increases BMD/treats colitis• In mice OPG increases BMD/treats colitis
• OPG is a regulator of intestinal immune responses
•Franchimont N et al. Clin Exp Immunol 2004;138:491-8•Vidal K et al. Am J Physiol Gastrointest Liver Physiol 2004;287:G836-44•Bernstein CN et al. Inflamm Bowel Dis 2005;11:325-30•Moschen AR et al. Gut 2005;54:479-87

OPG/RANKL in Children with IBD
Serum
234567
11.5
22.5
3* *
OPG (pmol/L) sRANKL (pmol/L)
012
00.5
Control
Sylvester FA et al. J Pediatr. 2006;148:461-466
Crohn

The Colon: A Source of OPG
Moschen, A R et al. Gut 2005;54:479-487
Macrophages/dendritic cells

Gut – Bone Axis:Indirect Effects?
Effect of Lean Body Mass
• Muscle strain drives bone formation
• LBM deficits present at diagnosis in IBD
• Persist despite weight gain/symptom improvement
Burnham JM et al. Am J Clin Nutr. 2005 Aug;82(2):413-20Sylvester FA et al. DDW 2007

Gut – Bone Axis – Indirect Effects
G th t ti• Growth stunting
• Nutrient intake/absorption/utilizationCalcium– Calcium
– Vitamin D– Vitamin K– Zinc

Immune FactorsT cells (INF- γ, RANKL) Cytokines (TNF-α, IL-6)
OPG
NutritionCalcium, vitamin D
Caloric/Protein intakeVitamin K/Others
HypogonadismIGF-I
InactivityLean tissue mass
Medications

Bone and IBD - Unknowns
• Disease duration?• Activity of disease?• Site of IBD involvement?• Small bowel surgery?• Diagnosis in childhood?• Skeletal site susceptibility?• Effect of remission?

P OCO
OHOH
P
R1
==Goal
OHOH R2To review therapeutic options to increase BMD in patients with IBD

Risk Factors – FractureModifiable
• Lifestyle factors• Low BMI• Risk of falling• Lifelong low Ca intake• Vitamin D deficiency/insufficiency• Use of glucocorticoids• Concurrent medical conditions

Calcium
• Women– Pregnant and nursing 1200 mg– 25-50 y 1000 mg
> 65 y 1500 mg– > 65 y 1500 mg
• Men– 25-65 y 1000 mg25 65 y 1000 mg– > 65 y 1500 mg
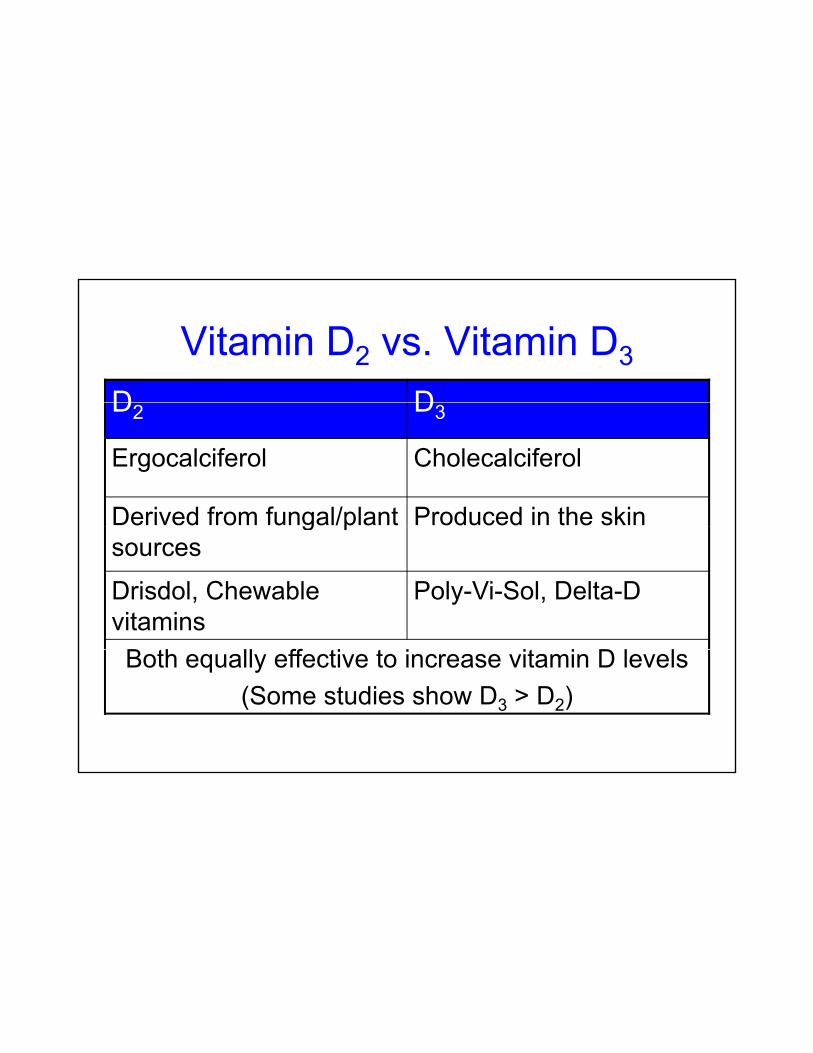
Vitamin D2 vs. Vitamin D3
D DD2 D3
Ergocalciferol Cholecalciferol
Derived from fungal/plant Produced in the sking psources
Drisdol, Chewable vitamins
Poly-Vi-Sol, Delta-D
B th ll ff ti t i it i D l lBoth equally effective to increase vitamin D levels(Some studies show D3 > D2)
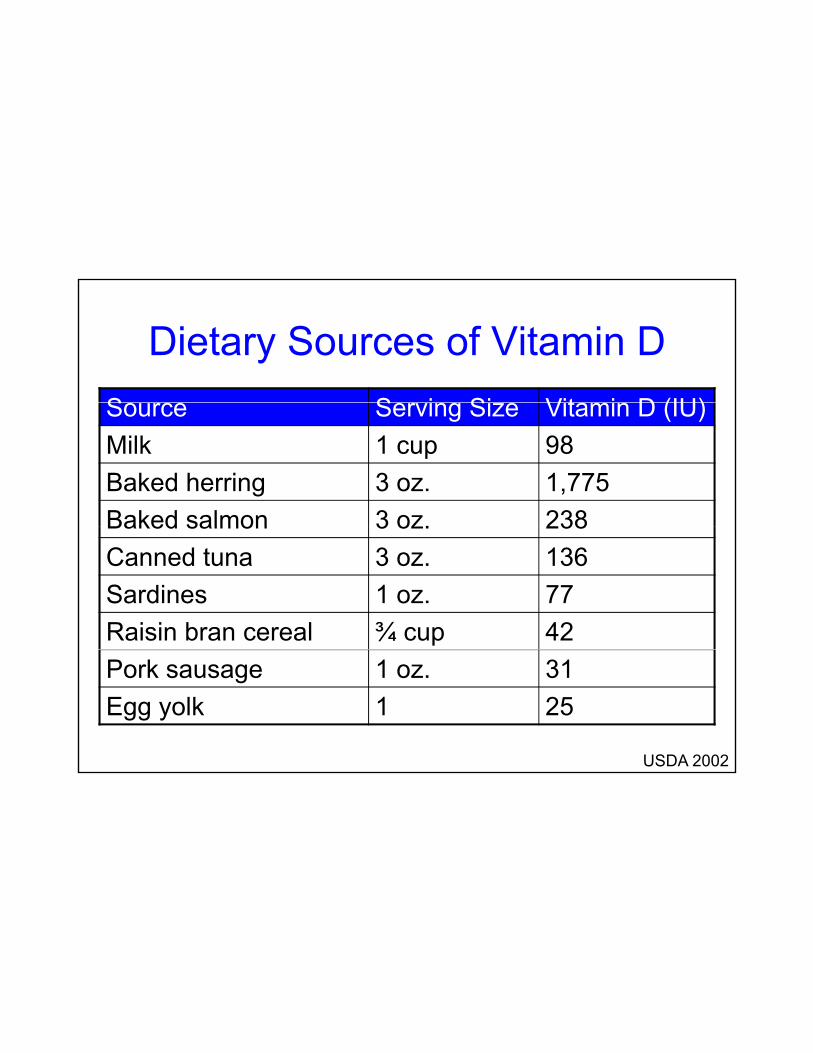
Dietary Sources of Vitamin DS S i Si Vit i D (IU)Source Serving Size Vitamin D (IU)Milk 1 cup 98Baked herring 3 oz. 1,775Baked salmon 3 oz. 238Baked salmon 3 oz. 238Canned tuna 3 oz. 136Sardines 1 oz. 77Raisin bran cereal ¾ cup 42Pork sausage 1 oz. 31Egg yolk 1 25
USDA 2002
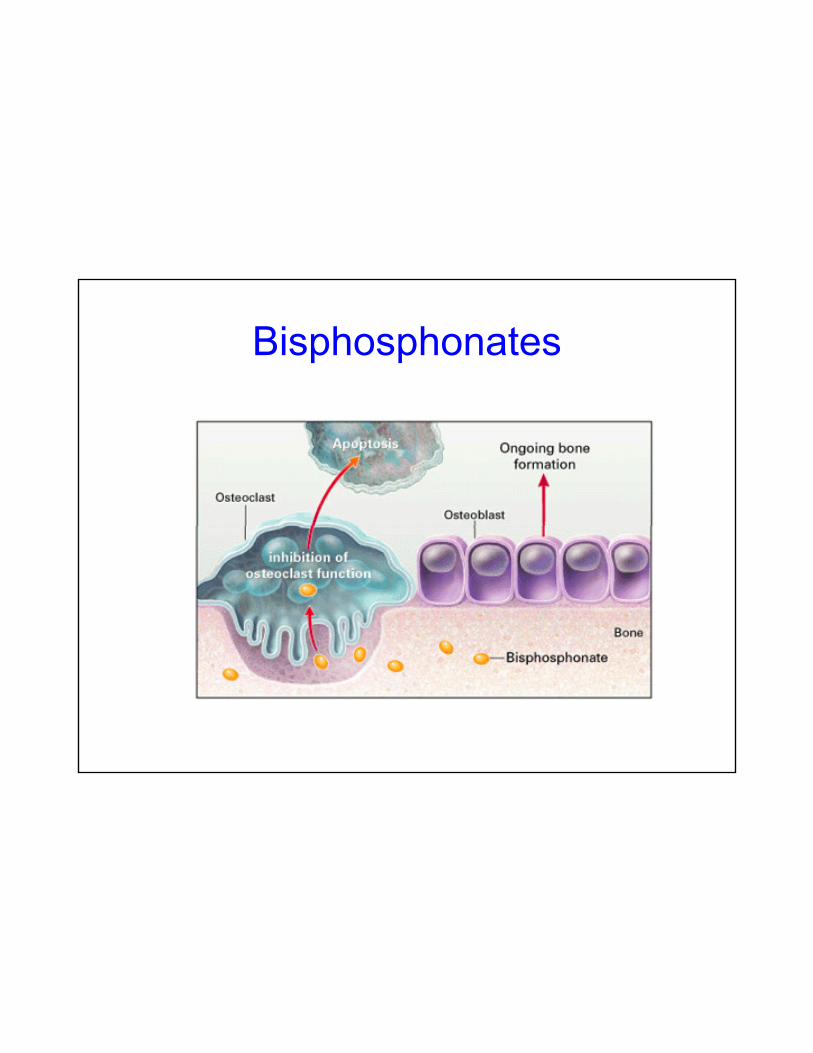
Bisphosphonates
The Future

Take Home Points
• Bone mass deficits occur in patients with IBD
Ri k f f t ildl i d• Risk of fractures mildly increased– Vertebral fracture prevalence?
M ltif t i l th i• Multifactorial pathogenesis
Take Home Points
• Bone mass can be measured by DXA– Be aware of pitfalls
Id tif d dd difi bl i k f t• Identify and address modifiable risk factors
• Control of inflammation, calcium/vitamin D, activity may increase bone massactivity may increase bone mass

Acknowledgements
NIH t R01 DK 066303• NIH grant R01-DK-066303 • Donaghue Foundation• CCMC • Dr Ernesto Canalis (Saint Francis• Dr. Ernesto Canalis (Saint Francis
Hospital & Medical Center)


















