Iabp pptx
48
IABP INTRA-AORTIC BALLOON COUNTERPULSATION Dr. VISHAL VANANI JASLOK HOSPITAL AND RESEARCH CENTRE APRIL 2015
-
Upload
vishal-vanani -
Category
Health & Medicine
-
view
107 -
download
0
Transcript of Iabp pptx

IABPINTRA-AORTIC BALLOON COUNTERPULSATION
Dr. VISHAL VANANIJASLOK HOSPITAL AND RESEARCH CENTRE
APRIL 2015

HISTORY
Kantrowitz described augmentation of coronary blood flow by retardation of the arterial pressure pulse in animal models in 1952.
In 1958, Harken suggested the removal of some of the blood volume via the femoral artery during systole and replacing it rapidly in diastole as a treatment for left ventricular (LV) failure, so called diastolic augmentation.

HISTORY
In the 1960s, Moulopoulos and colleagues from the Cleveland Clinic developed an experimental prototype of an IABP whose inflation and deflation were timed to the cardiac cycle.
In 1968, Kantrowitz reported improved systemic arterial pressure and urine output with the use of an IABP in two subjects with cardiogenic shock, one of who survived to hospital discharge.

HISTORY
Balloon catheters were 15 French and needed to be surgically grafted into the femoral arteries.
Percutaneous IABs in sizes 8.5-9.5 French (rather than 15 French used earlier) were introduced in 1979, and shortly after this, Bergman and colleagues described the first percutaneous insertion of IABP.
The first prefolded IAB was developed in 1986.

CARDIAC PHYSIOLOGY
PRELOAD
Preload refers to the amount of stretch on the ventricular myocardium prior to contraction.
Starling’s law described how an increase of volume in the ventricle at the end of diastole resulted in an increase in the volume of blood pumped out.
Preload is often referred to as “filling pressure”. Factors affecting preload include:
Aortic insufficiency Circulating blood volume Mitral valve disease Some medications (i.e. Vasoconstrictors, vasodilators)

AFTERLOAD
Afterload is the resistance that the heart must overcome in order to eject the blood volume from the left ventricle
Afterload takes several forms: The mass of blood that must be moved, measured by the
hematocrit Aortic end diastolic pressure (AEDP). Arteriole resistance
Afterload can be affected by: Aortic stenosis Arterial vasoconstrictors and vasodilators Hypertension Peripheral arterial constriction

OXYGEN CONSUMPTION
Myocardial Oxygen Consumption Depends on Systolic wall stress
Intra-ventricular pressure
Afterload
End diastolic volume
Wall thickness

HOW IABP HELPS?

IABP – HOW IT WORKS
A flexibile catheter – into the descending aorta. Correct positioning – Important When inflated, the balloon blocks 85-90% of the aorta.
This balloon displaces the blood that is in the aorta.
This is known as counter pulsation
This sudden inflation moves blood superiorly and inferiorly to the balloon.
When the balloon is suddenly deflated, the pressure within the aorta drops quickly.

WHY HELIUM?
Helium: Low Density Soluble

IABP – HOW IT HELPS
Inflation of the balloon occurs at the onset of diastole.
At that point, maximum aortic blood volume is available for displacement because the left ventricle has just finished contracting and is beginning to relax, and the aortic valve is closed.
The pressure wave that is created by inflation forces blood superiorly into the coronary arteries. This helps perfuse the heart.
Blood is also forced inferiorly increasing perfusion to distal organs (brain, kidneys, tissues, etc.)

IAB INFLATION
Balloon inflated during diastole Increasing aortic
pressure and
Increasing coronary blood flow
Increases Myocardial O2 delivery

IAB DEFLATED
The balloon remains inflated throughout diastole.
At the onset of systole, the balloon is rapidly deflated. The sudden loss of aortic pressure caused by the deflation reduces afterload.
The left ventricle does not have to generate as much pressure to achieve ejection since the blood has been forced from the aorta.
This lower ejection pressure reduces the amount of work the heart has to do resulting in lower myocardial oxygen demand.

Hemodynamic Effects of IABP
Aorta ↓ systolic pressure, ↑ diastolic pressure
Left ventricle↓ systolic pressure, ↓ end-diastolic
pressure,↓ volume, ↓ wall tension
Heart ↓ Afterload,↑ Cardiac Output, ↓ O2 Demand
Blood flow ↑ coronary blood flow

HEMODYNAMICS : Summary
Afterload
Myocardial oxygen demand
Coronary flow
Cardiac output

INDICATIONS
Refractory unstable angina Persistent myocardial
ischemia (preop or postop) Acute myocardial infarction Complications of acute MI Cardiogenic shock Refractory LV failure Acute MR and VSD Support for high-risk
catheterization or failed PCI Refractory ventricular
arrhythmias
As a bridge to cardiac transplantation
Support during transport Preoperative IABP (high-
risk patients) Cardiac surgery, High risk
CABG Weaning from
cardiopulmonary bypass Postcardiotomy LV systolic
failure unresponsive to inotropes

CONTRAINDICATIONS
Severe aortic insufficiency
Dissecting aortic aneurysm
Descending thoracic aortic atheroma
Aorto-iliac-femoral occlusive disease
Lower extremity ischemia
Dynamic LVOTO
Chronic end-stage heart disease with no anticipation of recovery
Aortic stents
End-stage cardiomyopathies
Severe atherosclerosis
End stage terminal disease
Abdominal aortic aneurysm
Uncontrolled sepsis
Severe peripheral vascular disease
Major arterial reconstruction surgery
Blood dyscrasias (Thrombocytopenia)

COMPLICATIONS
Transient loss of peripheral pulse
Limb ischaemia Thromboembolism Compartment syndrome Retroperitoneal hematoma Local vascular injury—false
aneurysm, haematoma, bleeding from the wound
Aortic perforation and/or dissection
Cardiac tamponade
Thrombocytopenia Infection / sepsis Malpositioning causing
cerebral or renal compromise
Renal failure and bowel ischemia
Heparin induced thrombocytopenia
Balloon rupture (can cause gas embolus)
Balloon entrapment

HOW TO INTRODUCE

IABP Kit Contents
Introducer needle Guide wire Vessel dilators Sheath IABP (34 or 40cc) Gas tubing 60-mL syringe Three-way stopcock Arterial pressure tubing
(not in kit)

IAB Sizing Chart

INSERTION TECHNIQUE
Percutaneous Sheath less With Sheath
Surgical insertion Femoral cut down Trans-thoracic

The IABP device has two major components:
1. A double-lumen 8.0-9.5 French catheter with a 25-50
ml balloon attached at its distal end; and
2. A console with a pump to drive the balloon.
The balloon is made of polyethylene and is inflated
with gas driven by the pump.

POSITIONING The end of the balloon should be just distal to the
takeoff of the left subclavian artery
Position should be confirmed by fluoroscopy or chest x-ray

HOW TO ADJUST IABP

OPERATION MODE

OPERATION MODES
AutomaticTracks cardiac cycle, cardiac rhythm and adjusts automatically
SemiautomaticOperator must adjust inflation & deflation
ManualOperator must adjust inflation & deflation & can set fixed rate

TRIGGER SOURCE
• During a cardiac arrest, the IABP can provide very effective perfusion in conjunction with external compressions.• Since there is no ECG signal and no
arterial pressure wave to trigger the pump, an internal trigger is selected.
• This trigger detects the flow of blood caused by compressions and inflates the balloon providing improved circulation.
• Good, consistent compressions are a must for this to work!

IAB FREQUENCY

AUGMENTATION

TIMINGS

TIMING OF COUNTER PULSATION
UASBP UASBP
ADBP
UADBPUADBP
ASBP
DABP

INTRAAORTIC BALLOON COUNTERPULSATION
Timing of inflation:
• First identify the dicrotic notch (when the aortic valve closes)
If inflation is too early the balloon inflates before the aortic valve closes and pumps blood backwards into the LV, and ↑ LVEDV & LVEDP, Increased left ventricular wall stress or afterload, Aortic regurgitation, Increased MV02 demand.
• If inflation is too late there will be sup-optimal coronary perfusion

INTRAAORTIC BALLOON COUNTERPULSATION
Early inflation:

INTRAAORTIC BALLOON COUNTERPULSATION
Late inflation:

INTRAAORTIC BALLOON COUNTERPULSATION
Timing of deflation:
• If deflation is too early there will be inadequate afterload reduction and sub-optimal coronary perfusion
• If deflation is too late the balloon remains inflated too long, causing ↑ afterload because the heart is trying to pump against an inflated balloon
INTRAAORTIC BALLOON COUNTERPULSATION
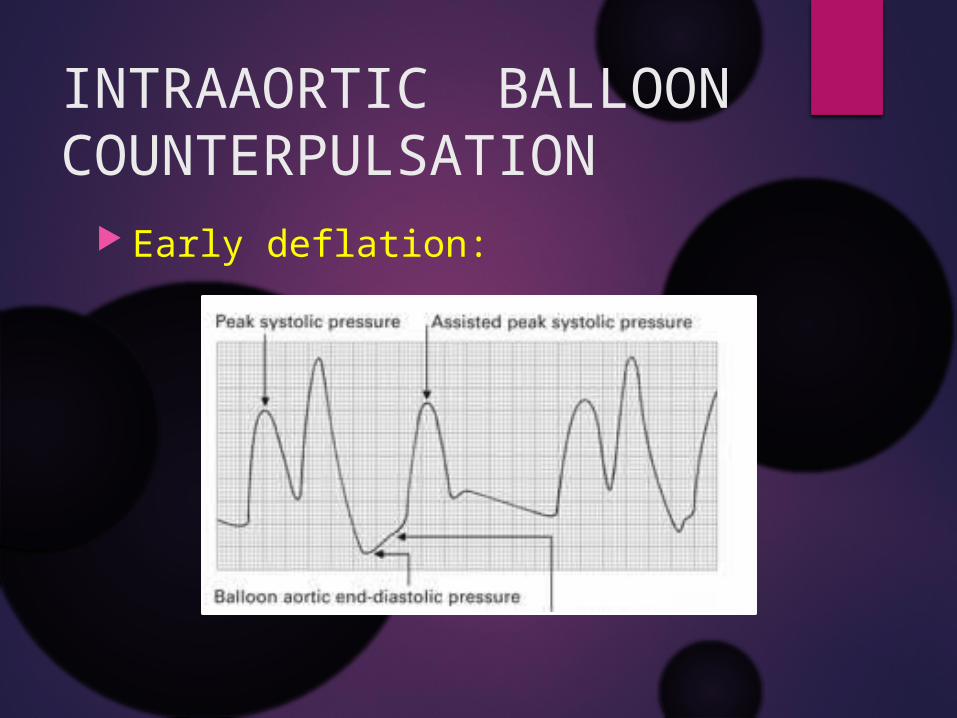
Early deflation:

EARLY DEFLATION
Waveform Characteristics: Assisted aortic end diastolic pressure may be ≤ the
unassisted aortic end diastolic pressure.
Assisted systolic pressure may rise.
Physiologic Effects: Sub-optimal coronary perfusion.
Potential for retrograde coronary and carotid blood flow.
Sub-optimal after load reduction & Increased MV02 demand.

INTRAAORTIC BALLOON COUNTERPULSATION
Late deflation:

LATE DEFLATION
Waveform Characteristics: Assisted aortic end diastolic pressure may be equal
to the unassisted aortic end diastolic pressure. Rate of rise of assisted systole is prolonged. Diastolic augmentation may appear widened.
Physiologic Effects: Afterload reduction is essentially absent. Increased MV02 consumption due to
The left ventricle ejecting against a greater resistance IAB may impede left ventricular ejection and increase
the afterload

MAINTENANCE CARE
Ankle flexion and extension one to two hourly
Use pressure relieving mattress Change ECG electrodes daily. Change occlusive dressing daily Secure balloon catheter at several points
along the limb.

OBSERVATIONS
Observe hourly at catheter insertion site For signs of bleeding Signs of infection Signs of blood in sheath
If blood or brown dust is observed within the lumen, immediately place the IABP on 'Standby'.
The catheter will have to be removed immediately.

OBSERVATIONS
Check hourly for left radial pulse Put SaO2 probe on left hand Assess the limb distal to the insertion One hourly Observe and record peripheral
pulses, capillary refill, skin, temperature Observe the waveform to ascertain that
the timing is correct

WEANING of IABP
Timing of weaning Patient should be stable for 24-48 hours
Decreasing inotropic support Decreasing pump ratio
From 1:1 to 1:2 or 1:3 Decrease augmentation Monitor patient closely
If patient becomes unstable, weaning should be immediately discontinued
IABP REMOVAL
Discontinue heparin six hours prior Check platelets and coagulation factors Deflate the balloon Apply manual pressure above and below IABP
insertion site Remove balloon while alternating pressure
above and below insertion site to expel clots Apply constant pressure to the insertion site
for a minimum of 30 minutes Check distal pulses frequently

KEY POINTS
The primary goal of intra-aortic balloon pump (IABP) treatment is to increase myocardial oxygen supply and decrease myocardial oxygen demand.
Decreased urine output after the insertion of IABP can occur because of juxta-renal balloon positioning.
Haemolysis from mechanical damage to red blood cells can reduce the haematocrit by up to 5%.
Suboptimal timing of inflation and deflation of the balloon produces haemodynamic instability.
An IABP is thrombogenic; always anticoagulate the patient.
Never switch the balloon off while in situ.

….THANK YOU….

![Intra-aortic balloon pump counterpulsation [IABP] for ...Intervention Review] Intra-aortic balloon pump counterpulsation (IABP) for myocardial infarction complicated by cardiogenic](https://static.fdocuments.in/doc/165x107/5b0c16167f8b9a8b038b916c/intra-aortic-balloon-pump-counterpulsation-iabp-for-intervention-review-intra-aortic.jpg)