
I NUOVI ANTICORPI ANTI-LINFOMA - Siematologia · I NUOVI ANTICORPI ANTI-LINFOMA ... Hodgkin’s...
39
I NUOVI ANTICORPI ANTI-LINFOMA PIER LUIGI ZINZANI Istituto di Ematologia e Oncologia “L. e A. Seràgnoli” Università degli Studi di Bologna Milano, 28 maggio 2007
-
Upload
vuongthuan -
Category
Documents
-
view
214 -
download
0
Transcript of I NUOVI ANTICORPI ANTI-LINFOMA - Siematologia · I NUOVI ANTICORPI ANTI-LINFOMA ... Hodgkin’s...
I NUOVI ANTICORPI
ANTI-LINFOMA
PIER LUIGI ZINZANI
Istituto di Ematologia e Oncologia
“L. e A. Seràgnoli”
Università degli Studi di Bologna
Milano, 28 maggio 2007
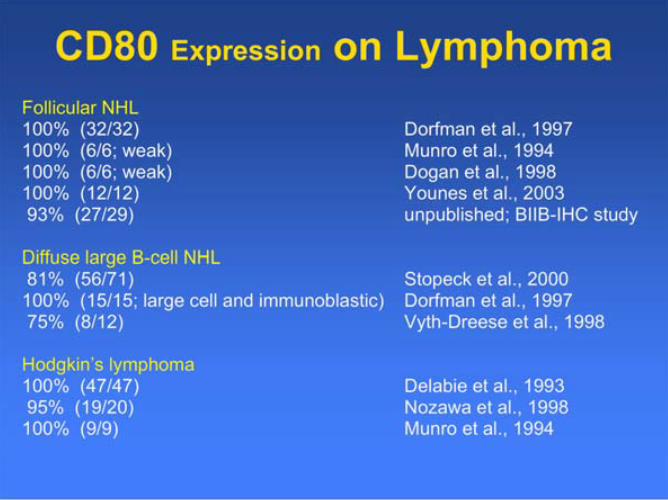
CD80 Expression on Lymphoma
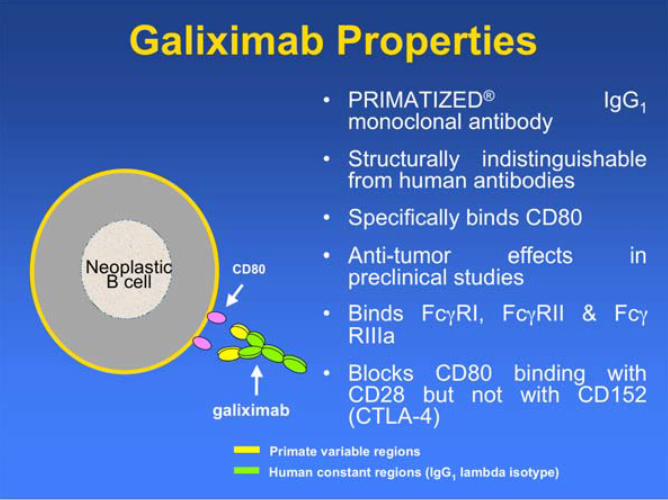
CD80NeoplasticB cell
Galiximab Properties
• PRIMATIZED® IgG1monoclonal antibody
• Structurally indistinguishablefrom human antibodies
• Specifically binds CD80
• Anti-tumor effects inpreclinical studies
• Binds Fc RI, Fc RII & FcRIIIa
• Blocks CD80 binding withCD28 but not with CD152(CTLA-4)
Primate variable regions
Human constant regions (IgG1 lambda isotype)
galiximab
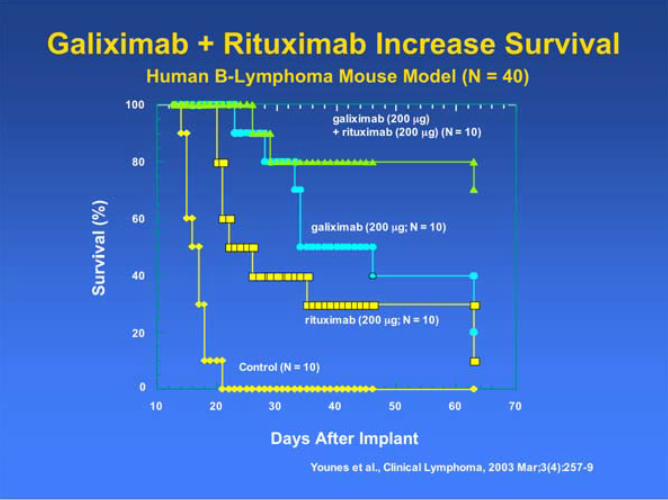
0
20
40
60
80
100
10 20 30 40 50 60 70
Days After Implant
Su
rviv
al
(%)
Control (N = 10)
rituximab (200 μg; N = 10)
galiximab (200 μg; N = 10)
galiximab (200 μg)
+ rituximab (200 μg) (N = 10)
Galiximab + Rituximab Increase Survival Human B-Lymphoma Mouse Model (N = 40)
Younes et al., Clinical Lymphoma, 2003 Mar;3(4):257-9
Galiximab Trials in Follicular
NHL
• Study 114-20: Galiximab monotherapy for
relapsed or refractory, follicular NHL
– Enrollment: Jan 2002 - Mar 2003
– 37 patients treated
• Study 114-21: Galiximab + rituximab for
relapsed or refractory, follicular NHL
– Enrollment: Nov 2002 - Mar 2004
– 73 patients treated
114-20: Galiximab Monotherapy
• Phase I/II, dose-escalation study of galiximab(125, 250, 375, or 500 mg/m2/wk x 4)
• Favorable safety profile
– Most common related AEs were fatigue, nausea, andheadache
• Tumor burden reductions in 46% of patients
• Overall response rate = 11% (4 of 37 patients)
– 375 mg/m2 (N = 21): 2 CRs, 1 PR
– 500 mg/m2 (N = 10): 1 PR
• PFS for responders: 11.2, 24.3+, 26.5, and 31 mos.Czuczman et al., J Clin Oncology, 2005
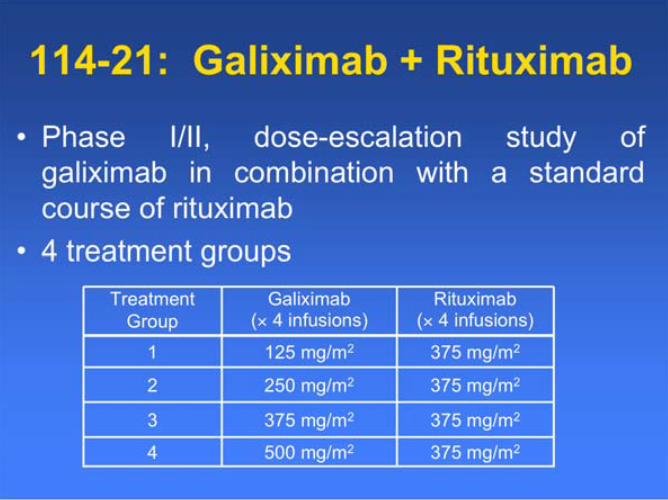
114-21: Galiximab + Rituximab
• Phase I/II, dose-escalation study of
galiximab in combination with a standard
course of rituximab
• 4 treatment groups
375 mg/m2375 mg/m23
375 mg/m2500 mg/m24
375 mg/m2250 mg/m22
375 mg/m2125 mg/m21
Rituximab( 4 infusions)
Galiximab( 4 infusions)
Treatment
Group
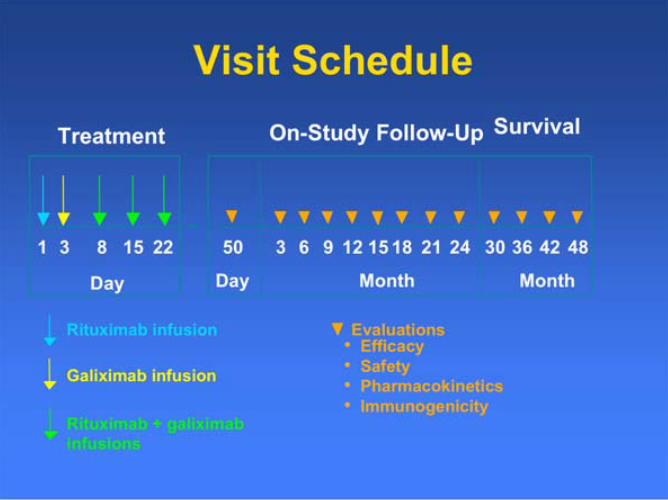
Visit Schedule
31 8
Day
15 22
Treatment
Rituximab infusion
Rituximab + galiximab
infusions
Galiximab infusion
On-Study Follow-Up
9 36 4815 4230
Month
123 6
Evaluations
18 21 2450
• Efficacy
• Safety
• Pharmacokinetics
• Immunogenicity
Survival
Day Month
Key Entrance Criteria
• Follicular lymphoma that has relapsed or hasfailed primary therapy
• Patients who received prior rituximab-containingtherapy had to respond with a TTP > 6 months
• WHO Performance Status < 2
• Acceptable hematologic status
– Hemoglobin > 8.0 g/dL
– ANC > 1500 cells/mm3
– Platelet count > 75,000 cells/mm3
Study Status
• 73 patients treated
• 64 treated at 500 mg/m2 galiximab + 375
mg/m2 rituximab weekly x 4
• Median follow up = 20.4 months
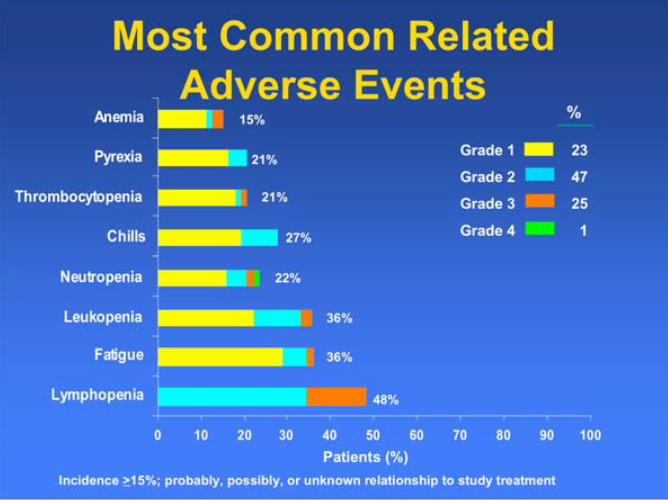
Most Common Related
Adverse Events
Incidence >15%; probably, possibly, or unknown relationship to study treatment
0 10 20 30 40 50 60 70 80 90 100
Lymphopenia
Fatigue
Leukopenia
Neutropenia
Chills
Thrombocytopenia
Pyrexia
Anemia 15%
Patients (%)
Grade 1
Grade 2
Grade 3
Grade 4
%
23
47
25
1
21%
21%
27%
22%
36%
36%
48%
Efficacy Results(500 mg/m2 Galiximab Group)
• Responses were evaluated using the
International Workshop Response Criteria
• Overall response rate = 64% (41 of 64
patients)
– 17% CR, 16% CRu, 31% PR
• Median PFS = 12.1 months (95% CI, 9.7
to 15.0 mo.)
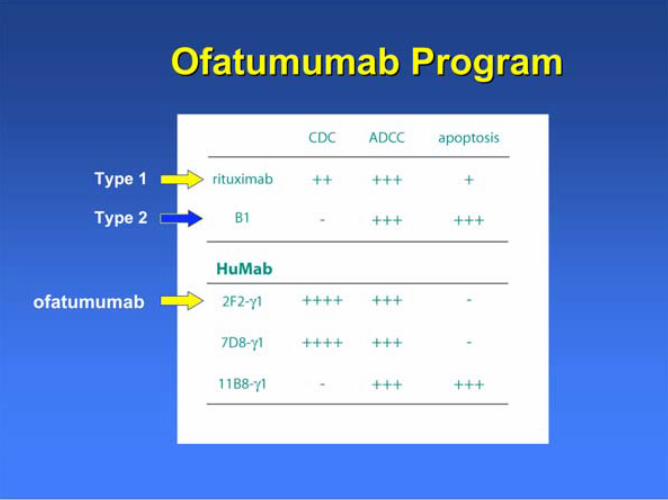
Ofatumumab ProgramOfatumumab Program
Type 1
Type 2
ofatumumab
OfatumumabOfatumumab
- Generated from Ig-Transgenic mice- Human IgG1,
- Excellent binding; slow off-rate
- Potent ADCC & CDC
Ofatumumab, a Novel Fully
Human Anti-CD20 Monoclonal
Antibody:
Results of a Phase I/II Trial in
Relapsed or Refractory Follicular Non-
Hodgkin’s Lymphoma
Study Hx-CD20-001
Objectives
To investigate the safety and efficacy ofofatumumab in patients with relapsed orrefractory follicular lymphoma grade 1-2
To determine the pharmacokinetics aftera single dose and after 4 doses ofofatumumab at weekly intervals
Design
An open label, dose-escalating, multicenter
clinical trial
4 cohorts of 10 patients
4 weekly i.v. infusions of 300, 500, 700 or 1000 mg
Patients were premedicated with oral
acetaminophen and i.v. antihistamine
In case of CTC grade 3 adverse events during
infusion i.v. glucocorticosteroids were given
Inclusion criteria
Relapsed or refractory follicular lymphomagrade 1-2, defined according to WHO
Lymphoma verified to be CD20+ from excisionallymph node biopsy
CT in screening phase showing:
2 or more clearly demarcated lesions with alargest diameter 1.5 cm, or
1 clearly demarcated lesion with a largestdiameter 2.0 cm
Age 18 years
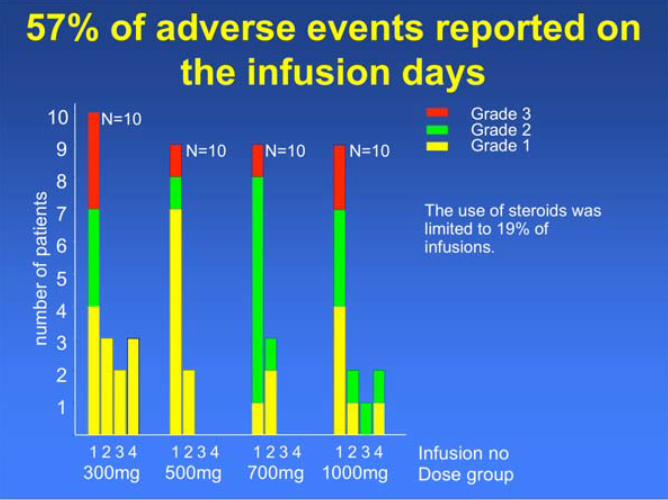
57% of adverse events reported on
the infusion days
The use of steroids waslimited to 19% ofinfusions.
N=10
N=10 N=10 N=10
Grade 3Grade 2Grade 1
nu
mb
er
of
pa
tie
nts
1
2
3
4
5
6
7
8
9
10
Infusion noDose group300mg 500mg 700mg 1000mg
1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4
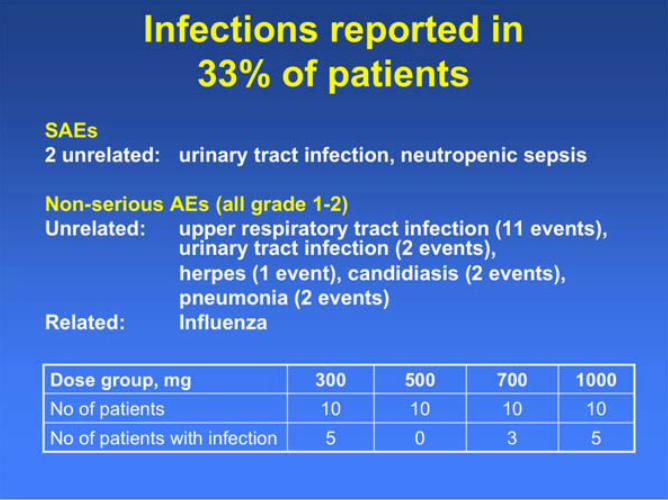
Infections reported in
33% of patients
SAEs
2 unrelated: urinary tract infection, neutropenic sepsis
Non-serious AEs (all grade 1-2)
Unrelated: upper respiratory tract infection (11 events),urinary tract infection (2 events),
herpes (1 event), candidiasis (2 events),
pneumonia (2 events)
Related: Influenza
5305No of patients with infection
10101010No of patients
1000700500300Dose group, mg
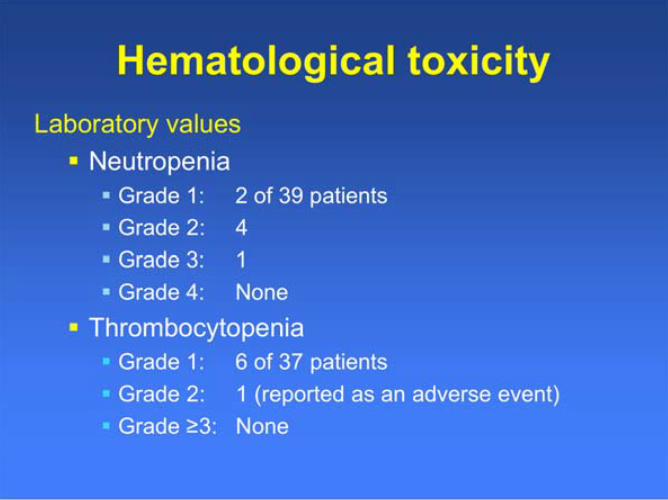
Hematological toxicity
Laboratory values
Neutropenia
Grade 1: 2 of 39 patients
Grade 2: 4
Grade 3: 1
Grade 4: None
Thrombocytopenia
Grade 1: 6 of 37 patients
Grade 2: 1 (reported as an adverse event)
Grade 3: None
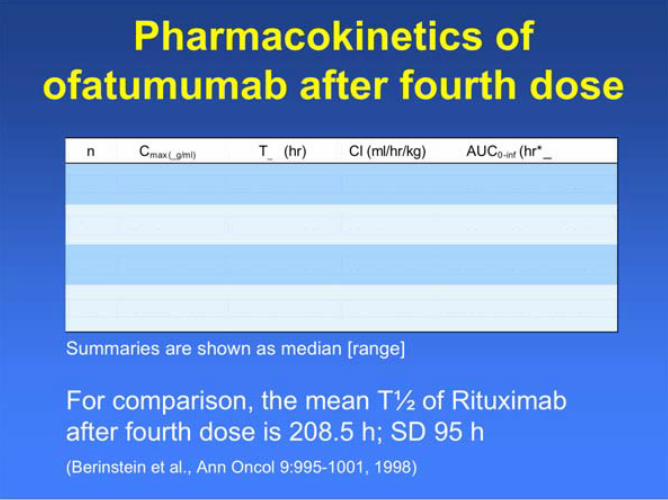
Pharmacokinetics of
ofatumumab after fourth dose
Summaries are shown as median [range]
For comparison, the mean T of Rituximab
after fourth dose is 208.5 h; SD 95 h
(Berinstein et al., Ann Oncol 9:995-1001, 1998)
n Cmax (_g/ml) T_ (hr) Cl (ml/hr/kg) AUC0-inf (hr*_g / m L )
1 0 1 2 9 [ 1 1 2 – 1 6 1 ] 4 4 6 [ 2 9 3 – 7 1 1 ] 9 [ 1 – 1 7 ] 7 4 6 1 6 [ 4 1 2 8 6 - 2 8 2 5 9 3 ]
9 1 8 5 [ 8 4 – 3 7 3 ] 3 0 3 [ 5 7 – 6 3 2 ] 1 6 [ 4 – 7 8 ] 5 3 2 6 1 [ 6 9 5 7 - 2 0 3 0 6 8 ]
9 3 5 5 [ 2 6 3 – 5 6 0 ] 3 2 2 [ 1 8 9 – 6 2 5 ] 1 0 [ 6 – 2 3 ] 1 8 5 2 5 1 [ 5 1 9 2 5 - 3 8 0 1 8 5 ]
1 0 6 1 0 [ 3 6 2 – 8 5 7 ] 5 6 7 [ 7 7 – 7 2 0 ] 3 [ 1 – 2 9 ] 6 4 4 0 8 0 [ 4 7 1 8 8 - 1 1 0 7 8 4 1 ]
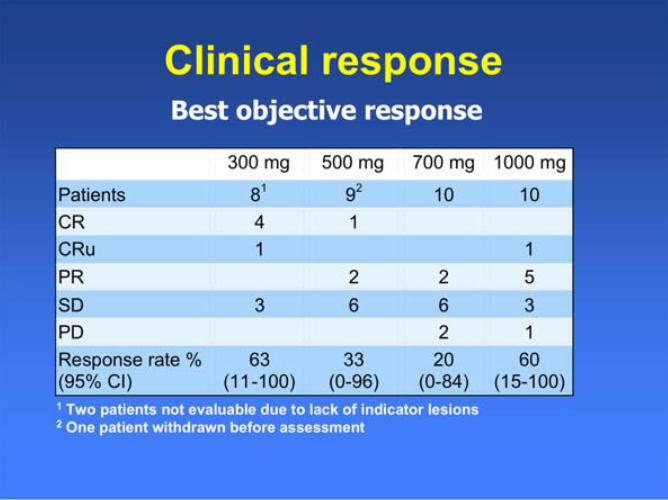
Clinical responseBest objective response
1 Two patients not evaluable due to lack of indicator lesions2 One patient withdrawn before assessment
300 mg 500 mg 700 mg 1000 mg
Patients 81 9
2 10 10
CR 4 1
CRu 1 1
PR 2 2 5
SD 3 6 6 3
PD 2 1
Response rate % (95% CI)
63 (11-100)
33 (0-96)
20 (0-84)
60 (15-100)
Objective responses in patients
previously treated with Rituximab
1 Davis et al., J Clin Oncol; 18: 3135-3143, 2000
9 of 14 (64%) evaluable patients treated withofatumumab after initial response to Rituximabachieved CR (3), CRu (1) or PR (5)
For comparison,
23 of 60 (38%) patients responded (10% CRand 28% PRs) after re-treatment withRituximab1
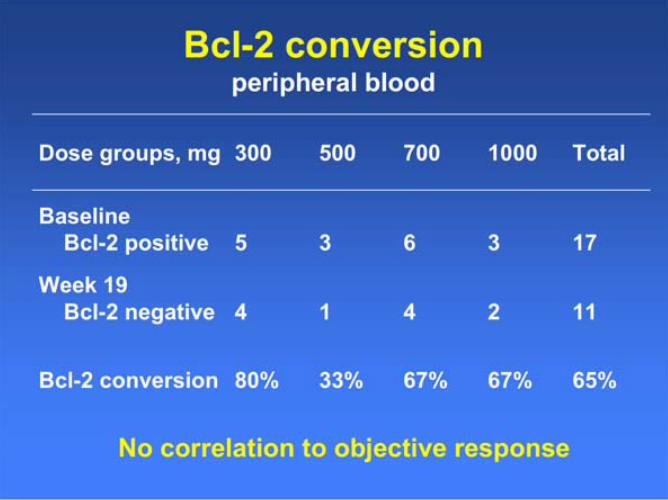
Bcl-2 conversionperipheral blood
65%67%67%33%80%Bcl-2 conversion
112414
Week 19
Bcl-2 negative
173635
Baseline
Bcl-2 positive
Total1000700500300Dose groups, mg
No correlation to objective response
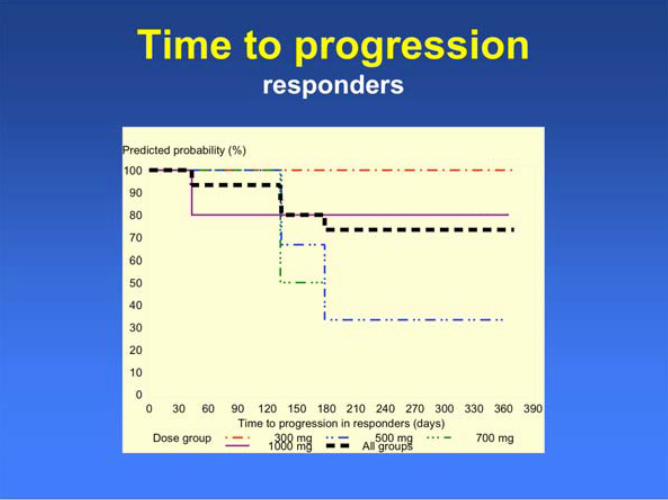
Time to progressionresponders
Predicted probability (%)
Dose group 300 mg 500 mg 700 mg1000 mg All groups
0
10
20
30
40
50
60
70
80
90
100
Time to progression in responders (days)
0 30 60 90 120 150 180 210 240 270 300 330 360 390
Conclusions
ofatumumab is well tolerated in patients withfollicular non-Hodgkin’s lymphoma’s
All dose levels caused immediate, profound and longlasting B-cell depletion
Objective responses achieved in all dose groups;response rate up to 63%
High objective response in patients previouslytreated with Rituximab
Bcl-2 conversion in the blood in 65% of evaluablepatients
The half-life of ofatumumab is greater than the half-life reported for Rituximab
Data strongly supports further development ofofatumumab in follicular lymphoma
Rationale for Targeting CD4 in CTCL
• CD4 is present on 90% of CTCL T cells
• CD4 expression is lineage-restricted
• CD4 expression is stable
• CD4 is involved in signaling
Zanolimumab
• High affinity, fully human monoclonal IgG1,
antibody (Kd = 5 x10-11 M)
• Activity– Antibody Dependent Cellular Cytotoxicity in vitro
– Depletion CD4+ T-cells in vivo
– The approximate half-life is 40 hours
• Blocks interaction between CD4 and MHC II
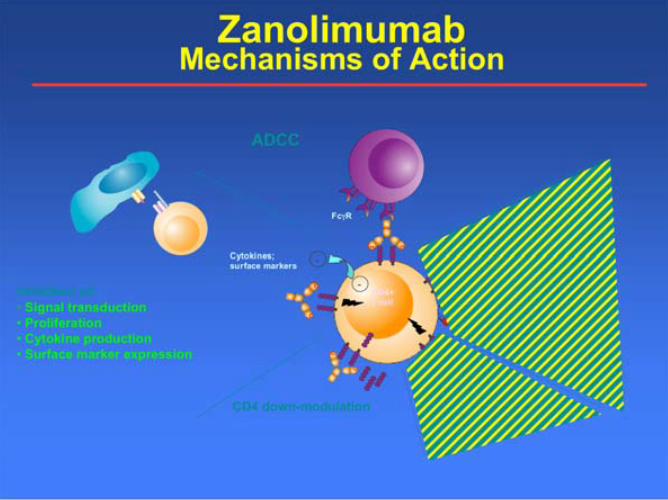
ZanolimumabMechanisms of Action
CD4 down-modulation
Inhibition of:
• Signal transduction
• Proliferation
• Cytokine production
• Surface marker expression
ADCC
CDC
Apoptosis
C1q
Fc R
-
Classical
pathway
Cytokines;
surface markers-
CD4+
T cell
Phase II TrialsRefractory Early and Advanced Stage CTCL
• Once weekly i.v. administration for 17 weeks conducted
between April 2003 – June 2004 in 47 CTCL patients
• Initial Regimen: 280 mg
• High Dose Regimen:
- 560 mg in early stage disease (HxCD4-007)
- 980 mg in advanced stage disease (HxCD4-008)
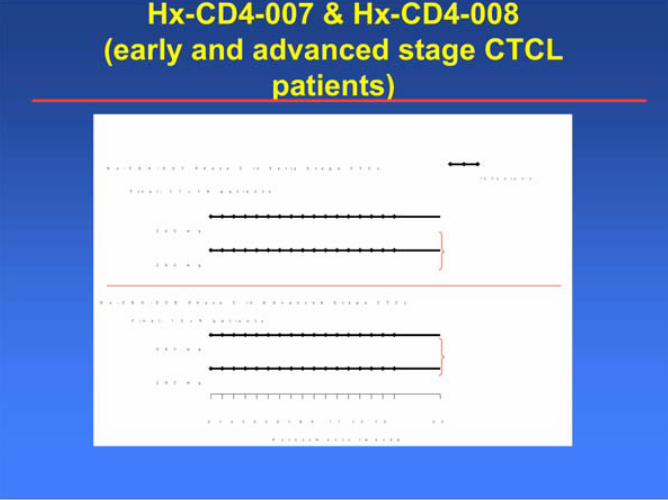
Hx-CD4-007 & Hx-CD4-008
(early and advanced stage CTCL
patients)
A s s e s s m e n t s ( w e e k s)
0 1 2 3 4 5 6 7 8 9 1 1 1 3 1 5 2 0
2 8 0 m g
5 6 0 m g
H x - C D 4 - 0 0 7 P h a s e 2 i n E a r l y S t a g e C T C L
F i n a l : 1 1 + 1 4 p a t i e n t s
2 8 0 m g
9 8 0 m g
H x - C D 4 - 0 0 8 P h a s e 2 i n A d v a n c e d S t a g e C T C L
F i n a l : 1 3 + 9 p a t i e n t s
I n f u s i o n s
17 weekly infusions
17 weekly infusions
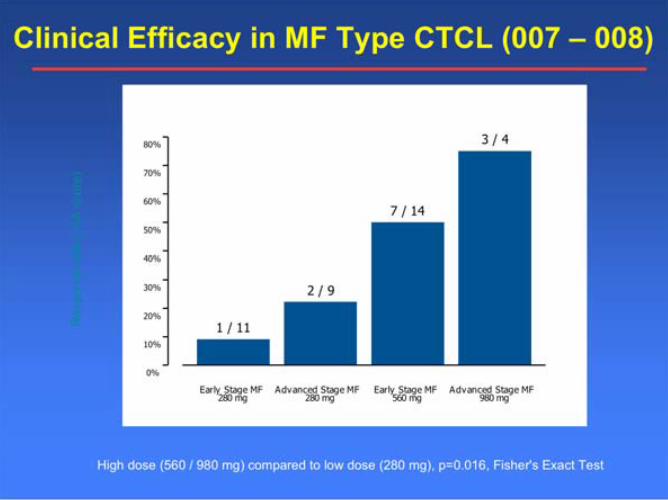
Clinical Efficacy in MF Type CTCL (007 – 008)
Early Stage MF280 mg
Advanced Stage MF280 mg
Early Stage MF560 mg
Advanced Stage MF980 mg
0%
10%
20%
30%
40%
50%
60%
70%
80%
1 / 11
2 / 9
7 / 14
3 / 4
Re
sp
on
se
ra
te (
CA
sco
re)
High dose (560 / 980 mg) compared to low dose (280 mg), p=0.016, Fisher's Exact Test
38 MF Patients
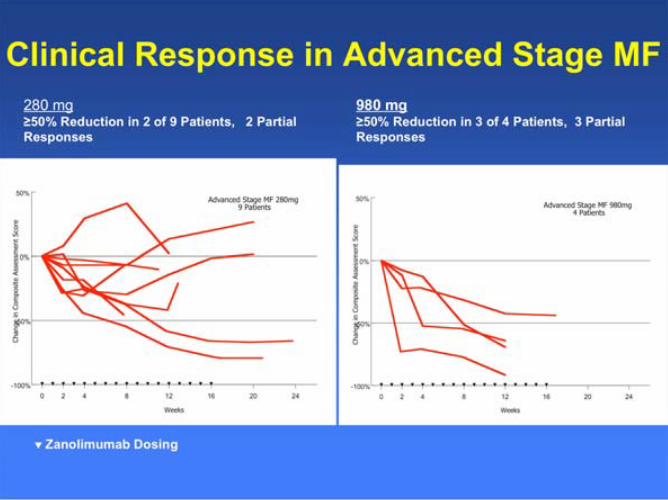
Clinical Response in Advanced Stage MF
280 mg50% Reduction in 2 of 9 Patients, 2 Partial
Responses
980 mg50% Reduction in 3 of 4 Patients, 3 Partial
Responses
Zanolimumab Dosing

Response in Stage IB Patient
280 mg
Baseline Week 2
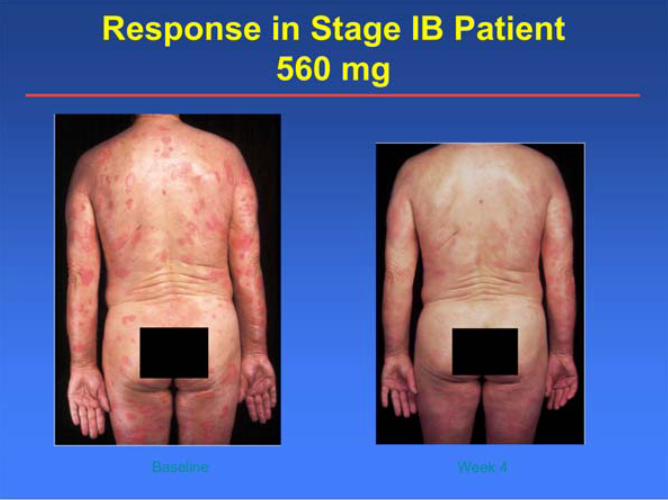
Response in Stage IB Patient
560 mg
Baseline Week 4

Response in Stage IVA Tumor Patient
980mg
Baseline Week 8
Most common AE in CTCL
• Grade 1-2 AE– Flu-like symptoms
– Pruritus
– Infections (no CMV reactivations)
– Eczema (dermatitis)
– Fatigue
– Headache
• SAEs (at 2 yrs follow-up)– 4 patients experienced 6 related SAEs in CTCL trials
4 Infections: Suspected wound infection, groininfection, peri-oral infection, CMV infection (11 monthsafter discontinuation of treatment)
2 cytokine release reactions
Current clinical development
status
• Zanolimumab is currently in phase III
clinical development for MF CD4+
CTCL
• Zanolimumab will soon be tested in
clinical trials as an add-on to standard
front-line combination chemotherapy in
NCTCL.


















