
I I - mvettathcts.com. Aeberhard.J.M. Badel.P. et al. Adult respiratory distress ... sponse syndrome...
23
MIMS HEART JOURNAL - 2004 JULY 01.. or as it is has been a field, which has seen umpteen this novel tool in our kitty. non-surgical PDA closure, which is very much in vogue now a days. Syndrome. not so long ago. reverse pacing which aims at correcting the intraventricular conduction delay and in treatment modality through one of the cases managed in our center. adults based on a wide range of published studies, guidelines and literature. much available in the Malabar region. I I Coronary Artery Bypass Grafting Bypass Surgery, commonly known, number of newer techniques and innovations and change of basic concepts creeping in and out. We were able to contribute to this surge of innovations in this field through our new invention – the “Vettath’s Anastamotic Obturator” (VAO) – a simple proximal anastamotic device for anastamosing vein grafts onto the aorta without using side clamp. The first article in this issue is a note on It is widely known that surgery starts were medicine fails. But today, newer developments in interventional technology have helped cardiologists pull back some of the surgeons’ domains into their repertoire. PDA and ASD are glorious examples of such lesions, which can and are being very effectively handled by Cardiologists today. We are having a feature on We bring to you some of the important aspects in the critical care of post cardiac surgical patients and a note on a pump associated postoperative problem – the Pump Lung Pump related problems have been a matter of concern and hence keeping away from the pump is a sensible fashion of the day. Beating Heart Surgery or Off Pump Coronary Artery Bypass (OPCAB) is a routine procedure. We bring you our experience on early Off Pump CABG in Acute Coronary Syndrome patients, a procedure which was considered impossible Pharmacotherapy for congestive cardiac failure aims at remodeling of the ventricles. But despite optimal medication a major portion of such patients get little benefit. Various treatment options for refractory cardiac failure have been described. Biventricular coordinating both the ventricles is one among them. We intend to bring you some facts about this We also bring you an elaborate review on Infective Endocarditis and its management in We sincerely do hope that this effort of ours, to transfer some of our limited knowledge in this field onto our peers in Kerala through the second edition of the MIMS Heart Journal will bear some fruit. We stress our commitment in providing you with outstanding information about the recent advances in Cardiovascular Sciences and related fields, which are very ED TOR AL
Transcript of I I - mvettathcts.com. Aeberhard.J.M. Badel.P. et al. Adult respiratory distress ... sponse syndrome...

12MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY13..
24 MIMS HEART JOURNAL - 2004 JULY
ation in patients who remain hypoxic despite PEEP.3. High frequency ventilation4. Airway pressure release ventilation5. Prone position6. Extracorporeal membrane oxygenation (ECMO).7. Partial liquid ventilationDrug like cyclooxygenase inhibitors, corticosteroids, nitric oxide,prostacyclin and surfactant have been tried with no conclusive benefit in ARDS. The role of pharmacological management is only supportive, apart from antibiotics to prevent secondary infection. From our practi-cal experience we found that pressure control ventilation with PEEP and inverse ratio ventilation improves the outcome in ARDS without much morbidity. Interesting feature in this patient were that drowsiness probably due to cerebral edema or hypoxia which was evident and effective diuresis inducing a negative balance of more then 7 litres over a period of 6 days helped in the speedy recovery. This shows that early detection and man-agement by appropriate Ventilatory strategies along with diuresis helps in recovery with out much morbidity in ‘Pump lung syndrome’.
REFERENCES
1. Amato, M.B.P, et al. Effect of protective ventilation strategy on mortality in the ARDS. N.Engl.j.Med 338 (6): 347-354, 1998.
2. Artigas, A., et al. The American-European consensus conference on ARDS part 2. Ventilatory, pharmacologic, supportive therapy, study design strate gies and issues related to recovery and remodeling, Intens. Care Med. 24:378- 398, 1998.
3. Marini. J.J. and Evans, T.W. Round table conference: Acute lung injury, 15th-17th March 1997 Brussels, Belgium. Intens. Care Med. 24:878-883, 1998.
4. Sessler, C.N.Mechanical ventilation of patients with acute lung injury. Crit. Care. Clin 14 (4): 707-729. 1998.
5. Zimmerman, J.L. and Hanania, N.A. Vasodilators in mechanical ventilation. Crit. Care. Clin 14 (4): 611-627, 1998
6. MooreFA, MooreEE. Evolving concepts in pathogenesis of post injury multiple organ failure. Surg clin North America 1995; 75:257-77.
7. Royston.D. Surgery with cardiopulmonary bypass and pulmonary inflammatory responses. Perfusion 1996: 11: 213-9.
8. Christenson.J.T. Aeberhard.J.M. Badel.P. et al. Adult respiratory distress syndrome after cardiac surgery. Cardio Vasc Surg 1996; 4:15-21.
He remained haemodynamically stable, very alert and was ambulated in ICU without any respiratory distress. By the end of 6 days, his fluid balance was –7430 ml. When he was transferred out of ICU, his weight has reduced to 80 kgs from 88 kgs.
Fig 3 CxR –acute phase of ARDSFig 4 CxR –recovery phase of ARDS
Serial-ABG REPORTSDay Preop 1st POD 5th POD 6th POD 7th POD 8th POD
PH 7.41 7.31 7.38 7.52 7.5 7.45
PO2 82 103.7 61.5 78.1 87.2 86.2
PCO2 40 52 36.1 34.8 36 39.4
BE -1.1 -0.6 -4.3 5.4 4.2 3.2
HCO3 28.5 23.5 31 29.3 28.3 27.3
FiO2 Room airNP4 l/min0.8 0.7 0.5 0.5
O2 Sat. 94.6 97.2 94.3 96.7 97.3 97
Remarks StablePCVentPCVentSIMV+PS
CONCLUSIONThere is considerable evidence that cardiopulmonary bypass is associated with deterioration of pulmonary function leading to acute lung injury (ALI) or ARDS. Mechanical ventilation plays an important role in reduc-ing the mortality rate of ARDS. Mortality is about 15 –30 % if only lung is involved and the rate increases upto 80% if 3 or more organs are involved. Ventillatory strategies used for ARDS (ARDS net).1. PEEP2. Low tidal volume 6-7 ml/kg to as low as 4 ml/kg to maintain plateau pressure <30-40cm H2O.3. Respiratory rate < 30/min4. FiO2 0.5 – 0.6
Different Ventillatory modes1. Pressure Control Ventilation- has advantage of higher mean airway pressure.2. Inverse ratio ventilation (IRV)- I: E ratio > 1 can improve oxygen
Cardiopulmonary bypass (CPB) is often followed by pulmonary dysfunc-tion and is also regarded as a risk factor for development of acute respi-ratory distress syndrome (ARDS). When pulmonary dysfunction cannot be directly attributed to a specific cause such as infection or ischemia, the concept of the “pump lung syndrome” or “systemic inflammatory re-sponse syndrome to CPB” is used as alternative explanation. Cardiopul-monary bypass is associated with a whole body inflammatory response, which involves activation of complement, leukocytes and endothelial cells , secretions of cytokines, proteases, arachidonic acid metabolites and oxygen free radicals. Leukocyte adhesion to microvascular endo-thelium, leukocyte extravasation and tissue damage are the final steps. Although the inflammatory response to cardiopulmonary bypass often remains at sub clinical levels, it can lead to major organ dysfunction and multiple organ failure. ARDS occurs in about 0.5 to 1.7% of patients undergoing open-heart surgery. We report a case of ARDS following on pump coronary artery bypass grafting .
CASE REPORT
A fifty-year-old male, weighing 88 kg, a known diabetic and chronic smoker, presented with exertional angina Class II. All his biochemical pa-rameters and ECG were normal. Chest X ray was normal (fig 1). Coronary angiogram revealed severe triple vessel disease i.e, proximal left anterior descending artery 90% stenosis, mid LAD after D1 95%, left circumflex 90% and right coronary artery (dominant) 70% stenosis. Echo showed normal LV function with ejection fraction of 61%. He was on carvedilol, diltiazem, sorbitrate and insulin. He was taken up for elective Coronary Artery Bypass Grafting.Premedicated with tablet diazepam 10 mg 2 hours before surgery. An-aesthesia induced with fentanyl, midazolam, thiopentone, pavulon, xy-locard and maintained with oxygen + air + intermittent isoflurane and fentanyl/midazolam/atracurium infusion. After heparinisation, CPB was instituted. CABG x 3 grafts done under warm blood cardioplegic arrest. Total CPB time was 73 minutes and aortic cross clamp time was 44 minutes. Came off bypass with minimal inotropic support. Elective ventilation continued and was extubated on
the next day morning. Chest x rays were within normal limits(fig 2). Inotropes were weaned off by 3rd postoperative day. Though patient was haemodynamically stable, he was very drowsy but arousable. He was drowsy even without any seda-tives. He could not be ambulated due to drowsiness.
On the 5th postoperative day, patient developed tachypnea, tachycardia, wheezing and a drop in saturation (SpO284-86%) with oxygen 10 L/min by mask. Chest X-ray showed me-diastinal widening with bilateral haziness (Fig 3). Arterial line and central venous catheter were inserted. ABG report showed hypoxia and hypercarbia (PO2- 65 mm Hg PCO2- 51.7 mm Hg). Cardac tam-ponade was suspected and was shifted to OT immediately for reexploration. After intuba-tion his lungs were found stiff on manual ventilation. The peak airway pressure was very high. Intraoperatively there was no evidence of tam-ponade. About 300 ml of serous fluid was removed from pleural cavities. Peroperatively the lung consistency was firm and turgid (boggy lung). Chest was closed with drains in situ.Post op ventilation continued on pressure controlled ventilation mode with the following settings: pressure control – 30 cm H2O, PEEP – 10 cm H2O, RR – 14/min, I: E ratio 1:1, FiO2- 0.8. The PaO2/ FiO2ratio was 78. Patient was on renal dose of dopamine, low dose adrenaline, lasix 1mg/hr, and aminophylline infusions. In 3 days, he had a negative balance of 3400 ml. His chest x-ray showed marked improvement (Fig 4). The PaO2 / FiO2 ratio improved from 78 to215.5. He was weaned off ventilator and extubated on the 4th day. All the infusions were stopped.
PUMP LUNG SYNDROME A case report
Fig 2 – Immediate post op CxR
Fig 1 - pre op CXR
Dr. Satheesh Kumar. N Cardiac Anaesthesiologist
mimslouranlfinal.indd 47/21/2004 11:07:55 PM
MIMS HEART JOURNAL - 2004 JULY 01..
or as it is has been a field, which has seen umpteen
this novel tool in our kitty.
non-surgical PDA closure, which is very much in vogue now a days.
Syndrome.
not so long ago. reverse
pacing which aims at correcting the intraventricular conduction delay and in
treatment modality through one of the cases managed in our center.
adults based on a wide range of published studies, guidelines and literature.
much available in the Malabar region.
I I
Coronary Artery Bypass Grafting Bypass Surgery, commonly known, number of newer techniques and innovations and change of basic concepts creeping in and out. We were able to contribute to this surge of innovations in this field through our new invention – the “Vettath’s
Anastamotic Obturator” (VAO) – a simple proximal anastamotic device for anastamosing vein grafts onto the aorta without using side clamp. The first article in this issue is a note on
It is widely known that surgery starts were medicine fails. But today, newer developments in interventional technology have helped cardiologists pull back some of the surgeons’ domains into their repertoire. PDA and ASD are glorious examples of such lesions, which can and are being very effectively handled by Cardiologists today. We are having a feature on
We bring to you some of the important aspects in the critical care of post cardiac surgical patients and a note on a pump associated postoperative problem – the Pump Lung
Pump related problems have been a matter of concern and hence keeping away from the pump is a sensible fashion of the day. Beating Heart Surgery or Off Pump Coronary Artery Bypass (OPCAB) is a routine procedure. We bring you our experience on early Off Pump CABG in Acute Coronary Syndrome patients, a procedure which was considered impossible
Pharmacotherapy for congestive cardiac failure aims at remodeling of the ventricles. But despite optimal medication a major portion of such patients get little benefit. Various treatment options for refractory cardiac failure have been described. Biventricular
coordinating both the ventricles is one among them. We intend to bring you some facts about this
We also bring you an elaborate review on Infective Endocarditis and its management in
We sincerely do hope that this effort of ours, to transfer some of our limited knowledge in this field onto our peers in Kerala through the second edition of the MIMS Heart Journal will bear some fruit. We stress our commitment in providing you with outstanding information about the recent advances in Cardiovascular Sciences and related fields, which are very
E D T O R A L

MIMS HEART JOURNAL - 2004 JULY 23..
14MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY11..
D E P A R T M E N T P R O F I L E
DEPARTMENT OFCARDIOVASCULAR & THORACIC SURGERY
Dr. Murali .P Vettath, MBBS, DNB, MChDr. Sheen Peeceeyen C.S, MBBS, MS, MChDr. Baburajan A.K, MBBS, DNB, MCh
DEPARTMENT OFCARDIAC ANAESTHESILOGY
Dr. A.V Kannan, MBBS, MD, FCACCDr. Satheesh Kumar.N, MBBS, MD
DEPARTMENT OFCARDIOLOGY
Dr. Ali Faizal, MBBS, MD, DMDr. Asish Kumar .M, MBBS, MD, DMDr. Dinesh Babu K.V, MBBS, MD, DMDr. Murali Krishna, MBBS, MD, DM
Infective Endocarditis, an infection of the inner walls of the cardiac cham-bers, valves, aortic root and prosthetic material is not an uncommon problem in our region. Advances in diagnosis and pharmacotherapy have changed the whole scenario since William Osler (1885) projected bacte-rial infection as the root cause, valvular heart disease as a predisposing factor and valvular incompetence and embolism as lethal complications of what he called Malignant Endocarditis. But even today, Infective En-docarditis carries a very high risk of morbidity and mortality. For bacterial endocarditis to occur there should be bacteremia, damaged endothelium vulnerable to infection, turbulence along haemodynamic path, and a virulent microorganism, which can overcome the natural defenses of the host or a host with a severely compromised immune system. Thus patients with acquired cardiac lesions like Rheumatic heart disease, degenerative valve disease or congenital lesions like Ventricular
Septal Defect, Tetralogy of Fallot, Congenital Aortic stenosis, complex cyanotic anomalies, Patent Ductus Arteriosus, Systemic to pulmonary arterial shunts etc. are prone for infective endocarditis. Recently intra-venous drug abuse is gaining more importance as a common cause for Infective endocarditis
The term infective endocarditis includes acute, subacute and chronic pro-cess of bacterial, viral, fungal or rickettsial aetiology. Acute endocarditis is a life threatening infection usually of normal heart valves, during the course of septicemia by virulent pyogenic microorganism such as hae-molytic Streptococci or Staphylococci. In subacute endocarditis, already damaged valves or other cardiac structures are secondarily infected.Acute native valve endocarditis accounts for 25% of Infective Endo-carditis. Severe sepsis, long term indwelling catheter, IV drug abuse and fungemia are predisposing factors. The usual affecting organism is Staphylococcus aureus. Other common organisms are Streptococcus viridans and Enterococci. The initial stage of valvular infection is surface vegetation – composed of platelets, fibrin and the causative microorganism. Organisms multiply within the vegetation and are thereby protected from the host defenses and antibiotics. They can be a source for repetitive bacteremia. Veg-etations are initially soft and friable and may embolise. They may also produce immune complex mediated and allergic vasculopathies. Large vegetation may become organized and calcified. Endocarditis is considered active surgically when surgery is performed in the presence of obvious local cardiac infection (active vegetation/ab-scess/sinus/fistulae) or when surgery is done while the patient is still on or within two weeks of termination of medical management for Infective Endocarditis. Endocarditis is considered healed when there is no active cardiac infection or inflammation, vegetation if present is endothelialised and abscess and sinus or fistulae if present are well organized.Surgical management of infective endocarditis was first reported by Kay et al (1961) in a patient with Tricuspid valve endocarditis and it was Wallace (1965) who first reported valve replacement as treatment for infective endocarditis.Early Diagnosis, effective management and prompt recognition of com-plication are essential to good patient outcome. For that general idea of the clinical presentation and diagnostic modalities are of great im-portance.
INFECTIVE ENDOCARDITIS - DIAGNOSIS AND MANAGEMENT IN ADULTS AN OVERVIEW
Dr. Sheen Peeceeyen. C.S Cardiac Surgeon
sizable proportion of patients with heart failure remain symptomatic and succumb to death, and hence additional treatment strategies like biven-tricular pacing have been developed.About 30 % of patients with chronic heart failure have intraventricular conduction delay such as left or right bundle branch block leading to loss of coordination of ventricular contraction. Such asynchrony is evident on the surface ECG as widening of QRS interval [> 120 m.sec]. This can impair the contractile reserve of the heart, and also enhance the severity of the functional mitral regurgitation. Intraventricular conduction delay has been associated with electrical instability and increased risk of sud-den death in patients with heart failure.
BENEFICIAL EFFECTS OF BIVENTRICULAR PACING: Short-term results of clinical trials with devices for atrial synchronized biventricular pacing to coordinate left and right ventricular contrac-tions are encouraging. Notable improvements in primary end points of NYHA functional class, six minutes walking distance and quality of life were constantly seen with cardiac resynchronization therapy [CRT]. In the recently published MIRACLE trial, the resynchronization group had significant improvement in peak oxygen consumption and total exercise time. Further, the left ventricular ejection fraction increased and the end-diastolic dimension, the magnitude of mitral regurgitation and the dura-tion of QRS all decreased in the resynchronization group. Biventricular pacing was associated with fewer hospital admissions and fewer days in the hospital for heart failure. The combined risk of a major clinical event [death or hospitalization for heart failure] was 40 % lower in the resynchronization group. In the study of Breithardt et al [JACC 2003 May 21, 41 [10]: 1852] cardiac resynchronization was associated with a significant reduction in severity of mitral regurgitation. The effective regurgitant orifice area decreased from 25 ± 19 mm to 13 ± 8 mm. This was directly related to an increase in left ventricular pressure rise [LV + dp/dt max]. Favourable effect on heart rate variability by resynchro-nization was shown by Adamson et al [circulation 2003 July 22; 108 (3) 266-9]. In the Ventak CHF study [Higgins SL et al JACC 2000 Sept; 36 (3)] synchronized biventricular pacing reduced the frequency of ICD therapies in patients receiving both the devices. Preliminary trial results show significant survival benefit when an ICD is combined with biven-tricular pacing and a 40 % reduction in hospitalization for heart failure.
ELIGIBLE PATIENT POPULATION:Patients with moderate-to-severe symptoms of heart failure [NYHA Class III or IV], left ventricular ejection fraction < 35 % and a wide QRS [> 130 m.sec] with left bundle branch block morphology are currently considered eligible for biventricular pacing. Heterogenous response to biventricular pacing has challenged the predictive accuracy of wide QRS complex in surface ECG for ventricular dyssynchrony. More sensitive tech-niques like Echocardiography with Tissue Doppler imaging to identify
regional delay in left ventricular contraction have been shown to better predict the responders from resynchronisation. [Makaryus AN et al Echo-cardiography] 2003 April 20 (3) 217-23.
TECHNIQUES & COMPLICATIONS:Prior to the procedure, a levophase of coronary angiogram is recorded to profile coronary sinus and cardiac veins. Device implantation is done in left infraclavicular pocket and venous access is obtained via subcla-vian vein puncture. Preformed sheaths in different curves are available to facilitate cannulation of the coronary sinus. With availability of over-the-wire leads, to enter the left cardiac vein, the technical success rate of CRT has improved. Placement of atrial and right ventricular leads are not different from the conventional pacemakers. The major complications associated with the procedure include dissection and perforation of the coronary sinus leading to hemopericardium, complete heart block, asys-tole, and arrhythmias. MIRACLE trial reported a technical failure rate of 8 % and major complications of 1-2 %, which include cardiac tamponade or cardiac arrest requiring resuscitation. Late dislodgment of left ventricu-lar lead can occur in as high as 6 % of patients.
FUTURE PERSPECTIVES:In considering devices for heart failure, the growing weight of evidence for biventricular pacing needs to be considered alongside the expand-ing indications for implantable cardioverter defibrillators. ICDs have been shown to significantly reduce the mortality and propensity for malignant ventricular arrhythmias in patients with left ventricular dysfunctions. Syn-chronized pacing can complement this effect by reducing the need for hospitalization for heart failure and the frequency of ICD therapies. Thus, patients with symptomatic heart failure due to ischemic cardiomyopathy and wide QRS complex, might be better served by a combined resynchro-nization pacer and defibrillator. However, the issue of cost effectiveness remains contentious and warrants further examination when long-term data are available.
REFERENCES: 1 Higgins SL, Yong P, Sheck D et al; biventricular pacing diminished the need for implantable cardioverter defibrillator therapy. Ventak CHF Investigators. J Am Coll Cardiol. 2000 Sep; 36 (3): 828-312 Young JB, Abraham WT, Smith AL et al; combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: the MIRACLE ICD Trial. JAMA. 2003 May 28; 289 (20): 2719-213 Makaryus AN, Arduini AD, Mallin J et al; echocardiographic features of pa-tients with heart failure who may benefit from biventricular pacing. Echocar-diography. 2003 Apr; 20(3) 217-234 Abraham WT., Fisher WG., Smith AL et al, Cardiac resynchronization in chronic heart failure. The MIRACLE study MEJM.
mimslouranlfinal.indd 5 7/21/2004 11:09:49 PM
02 MIMS HEART JOURNAL - 2004 JULY
Ii l t ti i
I I It t
Ii t
t
I I It wit i f lit t :
t
I I ITI DI I Ii
03
05
07
08 10
12
14 i i lati ly
t of thi li ti
i l i l t i ia
i it l li t
t ll t.in
C O N T E N T S
VETTATH’S ANASTAMOT C OBTURATOR A new prox ma anas amo c dev ce
NTENS VE CARE MANAGEMENT AFTER CARD AC SURGERY Where we s and oday
TRANS - CATHETER CLOSURE OF PATENT DUCTUS ARTER OSUS Ad eu o surgery
OPCAB FOR ACUTE CORONARY SYNDROME The way o go
CARD AC RESYNCHRON ZAT ON THERAPY A case repor h rev ew o era ure
PUMP LUNG SYNDROME A case repor
NFECT VE ENDOCARD S - AGNOS S AND MANAGEMENT N ADULTS An overv ew
For Pr vate C rcu on on
No Par s pub ca on may be reproduced by any means, nc ud ng e ec ron c med
Graph cs - Des gn - by nna ura wondders - ca cu
na ura y@sancharne

22 MIMS HEART JOURNAL - 2004 JULY
10MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY15..
MYCOTIC ANEURYSMS result from septic embolization of vegetation to vasa vasorum or intraluminal infective embolus with subsequent spread through the intima and outwards through the vessel wall. They occur mostly at arterial branching points as emboli are usually impacted at such points. Intracranial mycotic aneurysms are more common than ex-tracranial ones; which usually affect the visceral arteries and arteries to upper and lower limbs.The overall mortality rate in infective endocarditis patients with intra-cranial mycotic aneurysm is about 60%. Streptococci account for about 50% and Staphylococcus 10% of intracranial mycotic aneurysms. The distal MCA branches are more commonly affected. Intracranial mycotic aneurysms are multiple in about 20% of patients. Clinical presentation is highly variable.Routine screening is not required except when clinical findings are sug-gestive of an intracranial pathology. Contrast enhanced CT or Magnetic Resonance Angiography are useful in detecting these lesions but con-ventional four-vessel angiography still remains the diagnostic test of choice.Intracranial mycotic aneurysms (ICMA) may heal with medical therapy. Proximal aneurysms should be monitored with serial angiograms and CT as ligation of these may lead to severe neurological deficit. ICMA distal to major branching points may be ligated or excised. Some patients need both valve replacements and ICMA ligation. Bioprosthetic valve is prefer-able in such patients as anticoagulation can be avoided.
Extra-cranial mycotic aneurysms (ECMA) may present as tender pulsatile masses. Intra-thoracic or intra-abdominal ECMAs are asymptomatic until leakage or rupture occurs. Proximal and distal ligation of aneurysms and restoration of blood flow with autologous vein grafts through extra-ana-tomic site is the only hope for a radical cure.
SPLENIC ABSCESS in infective endocarditis may be caused either by an in-fected embolus or by bacterial seeding of a splenic infarct. Streptococcus viridans and Staphylococcus aureus accounts for around 40% of cases, enterococci 15%, gram-negative bacilli and fungi in <5%. Spleno-megaly is present only in about 30% and is not a reliable sign. Back, left flank, left upper quadrant pain or abdominal tenderness may be present. Persistent fever, bacteremia and sepsis may be suggestive of splenic abscess. Splenic rupture with hemorrhage is a rare complication. CT / MRI are the best diagnostic tests. Definitive treatment is splenectomy with appropriate antibiotics. Splenectomy should be performed before valve replacement, as the risk of prosthetic valve infection is very high with a splenic abscess.
PROPHYLAXIS AGAINST INFECTIVE ENDOCARDITISAntibiotic prophylaxis against infective endocarditis is recommended in a group of conditions, which carry with it a very high risk of playing a host to this dreaded disease. Patients with prosthetic heart valves, complex cyanotic congenital heart disease and previous history of infective endo-carditis carry a very high risk. Those with acquired lesions like rheumatic valve disease, hypertrophic cardiomyopathy (HCM), mitral valve prolapse with regurgitation, etc carry a moderate risk with them. Such patients need antibiotic prophylaxis while undergoing any invasive procedures like dental extraction or manipulation of the respiratory, genitourinary or gastrointestinal tracts.The standard general prophylaxis for patients at risk is Amoxicillin 2gm (50mg/kg in children) given orally one hour before the procedure. Those who are unable to take oral medications are given injection Ampicillin. Those allergic to penicillins are given either Clindamycin or Cephalexin or Cefadroxil or Azithromycin or Clarithromycin. An Aminoglycoside should be added to the above patients if they are undergoing procedures on the genitourinary or gastrointestinal tracts. Vancomycin with Gentamicin is preferred in patients who are allergic to penicillin.
CARDIAC RESYNCHRONIZATIONTHERAPY A case report with review of literature
CASE REPORT:Mr. R, a 36-year-old gentleman was diagnosed to have Hypertrophic Non-Obstructive Cardiomyopathy with LV systolic dysfunction. He pre-sented to us with worsening of dyspnea, orthopnea, and paroxysmal nocturnal dyspnoea . He had been symptomatic since the last 4 years and in NYHA functional class IV since 2 months. He had two episodes of syncope associated with palpitation during the previous 2 months. He was tachypnoeic on admission, heart rate was 56 beats /min, and blood pressure was 100/80 mmHg. Mean jugular venous pressure was not raised but ‘a’ wave was prominent. Apex beat was in the sixth intercostal space 1 cm outside the midclavicular line. First heart sound was soft, S2 was normally split, and LV S3 and S4 were prominent. Fine basal crepitations were present bilaterally. ECG showed sinus rhythm at 50 bpm, first degree AV block, and LBBB with a QRS duration of 240 m.sec. Chest X-ray showed grade III PVH, cardiomegaly, and mild pulmonary edema. All the routine hematological and biochemical parameters were normal. 2-D Echo Color Doppler examination showed asymmetrical sep-tal hypertrophy with global LV hypokinesis and LV ejection fraction of 35 % by Simpson’s method. There was moderate mitral regurgitation with MR jet area of 7 cm2. This gentleman had cardiac evaluation at another cardiac center in 10 months back. 24-hour Holter at that time showed one episode of non-sustained ventricular tachycardia and frequent multiform VPCs with cou-plets and bigeminy. Monomorphic sustained VT was inducible on electro-physiological testing. Angiography revealed normal coronary arteries. Patient was stabilized with I.V diuretics, Digoxin, ACE inhibitors, and supportive measures. The most appropriate therapeutic option was to provide an Implantable Cardioverter Device with biventricular pacing. However, since the patient could not afford the cost of an Implantable Cardioverter Device, the second best option of biventricular pacing with anti-arrhythmic drugs was discussed with the patient and relatives, to which they agreed.Patient was taken up for transvenous implantation of atrial synchronized biventricular pacing through a left infra-clavicular incision. Subclavian
puncture was done and coronary sinus was cannulated using the pre-formed sheath. A 6French balloon catheter was introduced through the coronary sinus sheath for venography. Attempts to negotiate the guide-wire in to the left cardiac vein were not successful. RA and RV apical leads were placed to which the pulse generator was connected and the wound closed. Subsequently, patient was taken for LV epicardial lead placement through left anterolateral thoracotomy. The proximal end of this lead was tun-neled to the infra-clavicular pocket and connected to the pulse generator. Pacemaker was programmed to biventricular pacing with an AV delay of 140 m.sec. Post-pacing ECG showed shortening of QRS duration to 130 m.sec, which is a significant indicator of response to therapy. Repeat Echocardiagraphic study revealed improvement in LV ejection fraction and reduction of MR jet area from 7 to 4 cm2.
REVIEW OF LITERATURE:INTRODUCTION:The pharmacotherapy of congestive heart failure is primarily based on antagonism of neurohormonal pathways namely, the sympathetic ner-vous system and the “renin-angiotensin-aldosterone axis”. Most of the drugs have been shown to reduce mortality and morbidity and in some cases they improve the underlying structural abnormalities of the heart by a process called reverse remodelling. Despite these therapeutic ad-vances,
Dr. Dinesh Babu .K.VCardiologist
2. Evidence of endocardial involvementA. Positive echocardiogram for IE defined as(i)Oscillating intracardiac mass on valve or supporting struc
tures, in the path of regurgitant jets, or on implanted material in the absence of an alternative anatomic explana tion, or(ii) Abscess, or(iii) New partial dehiscence of prosthetic valve
orB. New valvular regurgitation (worsening or changing of pre existing murmur not sufficient)
MINOR CRITERIA
1. Predisposition: predisposing heart condition or intravenous drug abuse2. Fever: temperature ≥38.0°C3. Vascular phenomena: major arterial emboli, septic pulmo nary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway lesions4. Immunologic phenomena: glomerulonephritis, Osler’s nodes, Roth spots, and rheumatoid factor5. Microbiological evidence: positive blood culture but does not meet a major criterion as noted above or serological evidence of active infection with organism consistent with IE6. Echocardiographic findings: consistent with IE but do not meet a major criterion as noted above.
Diagnosis of Definite Infective Endocarditis by Duke Criteria needs the presence of two major criteria or 1 major and 3 minor criteria or 5 minor criteria or pathological proof if IE. Those patients who do not meet the criteria for “Definite”Infective Endocarditis are labeled as “Probable” In-fective Endocarditis. Those patients whose symptoms reduce either with no treatment or within a short-term after diagnosis and those patients with no pathological evidence of infective endocarditis are labeled as rejected cases.The Duke Criteria is by far more specific and sensitive than the Beth Is-rael Criteria. Clinical suspicion of Infective Endocarditis may be raised by fever, other systemic symptoms along with physical findings like Osler’s nodes, petechiae, Janeway lesions, Roth spots, splenomegaly, newly di-agnosed clubbing and a new changing cardiac murmur. High index of suspicion in susceptible patients helps in diagnosing much before these findings set in. The offending organism can be demonstrated in 3 sets of blood cultures. (Each set with 1 aerobic and 1 anaerobic culture sample) obtained at intervals of more than one hour, within the first 24 hours is mandatory. 5 to 6 samples may be needed in some patients.
The diagnosis of infective endocarditis is straight forward in patients with the classical Oslerian manifestations of bacteremia or fungaemia, active valvulitis, peripheral emboli and immunologic vascular phenomena. In others, these classical findings may be few or absent as in Infective En-docarditis caused by Staphylococcus aureus infection of right sided heart valves or in patients where infective endocarditis is caused by the HACEK (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella) group of organisms. Immunologic vascular phenomenon is characteristic of subacute bacterial endocarditis. They are rarely seen in acute infective endocarditis on presentation, as the disease process is so rapid. Right-sided infective endocarditis does not produce peripheral embolism and immunological vascular phenomenon.This variability in clinical presentation of Infective Endocarditis warrants an optimal diagnostic strategy for early diagnosis. The Beth Israel criteria was proposed in 1981 by Van Reyn which was so stringent that only those patients confirmed pathologically were considered Definite Infec-tive Endocarditis patients and those with bacteremia, new valvular regur-gitation and vascular phenomenon were considered as Probable Infective Endocarditis patients. Durack et al from Duke University proposed the Modified Duke’s Criteria in 1994 incorporating Echocardiographic findings into the important di-agnostic parameters in Beth Israel Criteria. Moreover, intravenous drug abuse was recognized as an important cause for infective endocarditis in Duke’s criteria.The Duke’s clinical criteria stratified the various parameters into two broad groups – Major and Minor criteria as shown below.
MODIFIED DUKE’S CRITERIA FOR CLINICAL DIAGNOSIS OF INFECTIVE ENDOCARDITIS
MAJOR CRITERIA
1. Positive blood culture for IE A. Typical microorganism consistent with IE from 2 separate blood cultures as:(i) Viridans Streptococci, Streptococcus bovis, or HACEK group, or(ii) Community-acquired Staphylococcus aureus or entero cocci, in the absence of a primary focus
orB. Microorganisms consistent with IE from persistently positiveblood cultures defined as(i) ≥2 positive cultures of blood samples drawn >12 hours apart or(ii) All of 3 or a majority of ≥4 separate cultures of blood (with first and last sample drawn ≥1 hour apart)
mimslouranlfinal.indd 2 7/21/2004 11:03:23 PM
- 2004 03
INTRODUCTION
proximal anastomoses.
ses performed with our VAO.
placement to see if all the aortic layers were included.
VETTATH’S ANASTAMOTIC OBTURATOR (VAO)
that are 1 mm deep a 1.5 cm long.
aortic intima in the suture.
SURGICAL TECHNIQUE
or 6.0 polypropylene suture.
OUR EXPERIENCE OF 269 PROXIMAL ANASTOMOSES
. Chief Cardiac Surgeon
MIMS HEART JOURNAL JULY ..
With the advent of beating heart surgery, more than 50% of coronary artery bypass graft surgeries are performed in most coronary centers in India without the use of heart-lung machine. But the neurologic prob-lems caused by side clamping the aorta in performing the proximal anas-tomoses still remain. Hence, there has been a great deal of research to find an effective alternative to avoid side clamping the aorta. A couple of anastamotic devices have already arrived in the market, but since the costs of these devices are prohibitive, we designed our own device for
PATIENTS AND METHODS From July 2002 to July 2003, we performed 235 coronary artery bypass graft surgeries on the beating heart with 177 of these procedures performed off-pump and 58 of them carried out with pump assistance. Initially, proximal anastomoses of vein grafts were performed with aortic side clamp. Of late, all our top ends are being performed with VAO. 177 patients have had their proximal Saphenous Vein Graft (SVG) anastomo-
Before VAO was used on patients, it was tried for anastomosing vein grafts on the aortas and pulmonary arteries of various perfused animal heart models. The aortic and pulmonary artery pressures were maintained at 110 to 120 mm Hg systolic while these anastomoses were being per-formed. These conduits were then explanted and examined for suture
This metallic instrument is made of solid steel (Figure 1). It is 18 cm long and comes in small and medium sizes (5 mm and 6 mm in diameter respectively). The holding part is smooth. The inserting bit has a ridge 2.5 cm from the end (Figure 2). This 2mm ridge projects perpendicularly from the steel rod. There are 3 equidistant grooves in the inserting end
The ridge helps to prevent blood from spurting directly into the eye. The grooves allow the needle to pass through the rod and thereby include the
VAO allows us to anastamose the proximal ends of the vein grafts, before or after the distal anastomoses. The aortic site proposed for anastomosis marked with diathermy. Two 3-0 polypropylene purse-string sutures are applied 1 cm away from the site. The aorta is stabbed with a No.11 blade knife, and punched with 4mm or 4.5mm aortic punch (for 5-mm or 6-mm VAO), respectively. The punch hole is blocked with the left index finger. VAO is introduced and purse strings are tightened just enough to prevent excessive bleeding. Once the obturator is in and the snares are tightened, the proximal vein anastomoses is performed as usual with 5.0
VETTATH’S ANASTAMOTIC OBTURATOR
Dr. Murali P Vettath

MIMS HEART JOURNAL - 2004 JULY 21..
16MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY09..
About 5% of patients have “Culture Negative Endocarditis”, which usu-ally is due to inadvertent use of antibiotics prior to obtaining blood cul-ture samples (about 60%) or infection by pathogen difficult to isolate from blood culture. eg:- HACEK group, Bartonella species, a nutritionally variant streptococcus now classified as Abiotrophia species, Brucella spe-cies, Legionella species, Coxiella brunetti, Torpherema whipelli or fungi like Aspergillus which are never recovered from blood. These organisms need special methods and efforts from the microbiologist, to be traced and tackled appropriately.Echocardiography has an important role in diagnosing and assessing the severity of the disease and its complications, if any. Vegetation, abscess, new prosthetic valve dehiscence or new regurgitation are the four power-ful identifiers of infective endocarditis in the presence of other clinical parameters. Pathological consequences of infective endocarditis such as ventricular dysfunction,, ruptured chordae, shunts or fistulae may also be identified on echo. Echo may be useful in diagnosis of culture negative infective endocarditis or in the diagnosis of persistent bacteremia from an unidentified source. Trans Esophageal Echocardiography (TEE) has a much higher sensitivity and specificity than Transthoracic echocardiog-raphy (TTE) in diagnosing infective endocarditis. Moreover Transthoracic echocardiography alone cannot exclude prosthetic valve infection, peri-annular abscesses, fistula or leaflet perforation. All these are picked up better in Trans esophageal echocardiography. When both TTE and TEE are negative, the negative prediction value is about 95%. A repeat TEE in 7 to 10 days is needed in these patients labelled negative by Echo but with a high clinical suspicion of Infective Endocarditis. Follow-up Echo over the course and on completion of medical management is needed to assess the efficacy of therapy instituted.
MEDICAL MANAGEMENT OF INFECTIVE ENDOCARDITISThis is based on the invading organism. 80% of Infective Endocarditis are due to Streptococci and Staphylococci. Majority of native valve bacte-rial endocarditis is caused by Streptococci viridans (50%) and Staphy-lococcus aureus (20%). 80% of Tricuspid valve infection is caused by Staphylococcus aureus – as this is more common in IV drug abusers. Staphylococcus aureus is a frequent cause of infective endocarditis in diabetes mellitus too. Early prosthetic valve endocarditis, defined as en-docarditis during the first two months after surgery is frequently caused by Staphylococcus epidermidis. Late onset prosthetic valve infective en-docarditis usually is caused by Streptococcus viridans and Staphylococci. Enterococcal endocarditis associated with malignancy or manipulation of gastrointestinal or genitourinary tract is usually caused by Enterococcus faecium (90%). The HACEK groups are an important group, which causes large vegetation (>1 cm), large vessel emboli and Congestive Cardiac Failure (CCF). Fungi are another group, which produces large vegeta-tions. Candida is a common cause for Infective Endocarditis in IV drug
abusers and immunocompromised patients.
MEDICAL MANAGEMENT OF UNUSUALLY ENCOUNTERED MICROORGANISMSCOAGULASENEGATIVESTAPHYLOCOCCI: Increasing number of coagulase neg-ative Staphylococci infective endocarditis is being reported. An important subset of these patients, with infection of Staphylococcus lugdunensis is being identified. This is more virulent than other forms of coagulase negative Staphylococci, has high risk of paravalvular spread and meta-static distant organ seeding. This is susceptible to most antibiotics.
COXIELLABRUNETTI: The causative organism for Q fever usually affects prosthetic or previously damaged aortic or mitral valves. Infection is sub endothelial and vegetation is small and hence often missed. Doxycycline with Trimethoprim / Sulphamethoxazole, Rifampicin or Fluoroquinolones is the mainstay of therapy. The organism may remain dormant in tis-sues for a long time and hence drugs may be needed life long or for a minimum of three years.
BRUCELLA: This gram-negative bacillus which causes brucellosis can produce bulky vegetation on the previously damaged aortic and mitral valves followed commonly by valve destruction, perivalvar abscess and congestive heart failure. Doxycycline plus Streptomycin or Gentamicin or Trimethoprim /Sulphamethoxazole or Rifampicin is the drug of choice. Valve replacement is needed in most cases. Drugs should be continued for 2 to 10 months after valve replacement
CANDIDAANDASPERGILLUS: Cause majority of fungal Infective Endocardi-tis. Those with history of IV drug abuse, prosthetic valves replacements and long term central venous catheters are at high risk. Blood cultures are usually negative and vegetations bulky. Metastatic foci, perivalvar invasion and embolisation are common.Valve surgery is a must as Am-photericin B, the only fungicidal agent available and has poor penetra-tion into vegetation. Suppressive therapy with Imidazoles (Fluconazole) may be effective.
LEGIONELLA:Patients usually present with a long febrile illness, newly developed murmur and extremely high antibody titers. Most patients are prosthetic valve recipients. Embolism is rare. Parenteral Doxycycline or Erythromycin followed by prolonged oral therapy is effective. Valve re-placement is needed only if there is valvar incompetence.
PSEUDOMONASAERUGINOSAcauses Infective Endocarditis especially in IV drug abusers. Isolated right-sided Pseudomonas infective endocarditis can be medically managed with Piperacillin combined with an Aminoglycoside. Valve replacement is mandatory for left sided infective endocarditis.
of 0.5 to 1 mm; (vi) T inversion of > 1mm in leads with dominant R waves.Patients with chest pain probably non cardiac, one risk factor (not Diabe-tes Mellitus), flat T wave or < 1 mm inversion in leads with dominant R waves or normal ECG are considered to be carrying a low risk.Percutaneous intervention has proven to prevent irreversible myocardial damage. Cardiac catheterization, Angioplasty and CABG in ACS has in-creased considerably in the past two decades. In ACS, PTCA against the culprit lesion and antiplatelet therapy can be performed with an initial success rate of > 95%, although the incidence of procedure related complication is high, world wide.CABG is considered for patients with coronary lesion that are not suitable for or do not respond to catheter based reperfusion. The reported inci-dence of perioperative death is 4 % and MI is 10 % higher when CABG is performed urgently than semi urgently in ACS. Therefore, efforts should be made to stabilize the patients pharmacologically before emergency revascularization procedures are contemplated. Use of IABP aids as a bridge to Angioplasty or CABG in ACS patients.The need for revascularization is based on diagnosing the culprit lesion early. Various institutions adopt various protocols for coronary angiogra-phy (CAG)in ACS. Two strategies are generally followed- the early inva-sive strategy and the conservative strategy. The early invasive strategy incorporates coronary angiography for all sta-bilized patients within 48 hours of presentation. The conservative strat-egy prescribes angiography for high-risk patients (ie CHF, LVEF<50%, malignant arrhythmia, recurrent ischaemia, prior revascularization etc). Both early invasive and conservative strategies have been found to pro-duce similar clinical outcomes by the TIMI 2B and VANQUISH studyDecision about further proceedings is made based on the disease pattern revealed by CAG. Emergency surgical revascularization may be also need-ed in the setting of a failed thrombolysis or PTCA with acute occlusionThe morbidity of patients operated on after acute MI remains relatively high when compared to stabilized patients. This is mainly because, the adverse effect of CPB is poorly tolerated by a heart with an evolving MI. It is reasonable to think that keeping off the pump may be advantageous in this subgroup of patients.The optimal timing of surgery for ACS remains indecisive. Various studies have shown that the mortality rate of patients who underwent surgical revascularization within 48 hours of an acute MI was significantly higher compared to after 48 hours.A recent multi-center analysis has shown clearly that the perioperative mortality in acute MI patients declined considerably with the increasing time interval. The first 6 hours is said to be the most dangerous period with mortality of about 10%. The mortality depends not only on the tim-ing of surgical revascularization but also on the LV function, presence of haemodynamic stability and presence of collateral circulation.
Cardiopulmonary bypass (CPB) is a significant factor affecting the out-come in patients undergoing early CABG after ACS. Various studies have proven that the mortality rate is nearly 5 times higher in emergency CABG done on a stopped heart than on a beating heart. This deleterious effect of CPB is most evident in patients operated within 48 hours of an acute cardiac event.
OUR EXPERIENCE 306 CABGs were performed in our department during the period from July 2002 to October 2003. Out of these 46 were ACS patients who un-derwent emergency coronary angiography and were taken up for emer-gency surgical revascularisation. 6 of these patients had STEMI, 12 had NSTEMI, and the rest had unstable angina. 2 patients were referred to us for CABG after failed PTCA elsewhere. They were taken up on the second and third day post acute MI respectively.The patient age varied from 38 years to 76 years. 38 were males and 8 were females. All patients were diagnosed based on their ECG, Cardiac enzyme levels and trans-thoracic echocardiography. 2 patients had severe LV dysfunc-tion, 6 had moderate LV dysfunction and the rest had adequate LV func-tion. Every effort was made to stabilize the patients medically, so as to give at least a week’s time for the myocardium to recover from the acute insult. 14 patients needed emergency CABG before a week of the acute event. CABG in all the 46 patients, irrespective of the LV function and the time from the acute event were performed on beating heart. 6 patients needed minimal pump support due to haemodynamic compromise while positioning the heart for OPCAB. We had no perioperative MI or operative mortality. Postoperative ventilation, ICU stay, bleeding, enzyme levels, inotropic support and hospital stay were comparable to elective surgeries. All patients have been followed up till date and are maintaining good health.
CONCLUSIONAcute coronary syndrome is no longer a contraindication for surgical re-vascularisation. Off pump coronary artery bypass has contributed much to the results of CABG in the acute setting by taking the pump-associated complications away. Antiplatelet drugs, which cannot be weaned off in patients in an acute setting, do not contribute to perioperative blood loss in OPCAB patients, questioning the actual need for stopping antiplatelet drugs even before elective OPCAB. The results of surgical revasculariza-tion are rewarding if surgery can be prolonged at least for 3 days after an acute cardiac event.
The choice of the device for valve replacement depends on a variety of factors like risk of re-infection, ease of insertion, durability, need for an-ticoagulation, adequacy of removal of infected tissue etc. A homograft is preferred to a mechanical device considering the reduced risk for re-infec-tion and need for anticoagulation. Valve repair rather than replacement may be considered in some cases of healed mitral valve endocarditis with small vegetations and in intravenous drug abusers with tricuspid valve endocarditis.
MANAGEMENT OF COMPLICATIONS OF INFECTIVE ENDOCARDITISSepsis, congestive cardiac failure, embolism, periannular spread, mycotic aneurysm and spread of infection to other organs are the common com-plications of infective endocarditis. Certain factors likeprosthetic cardiac valves, left-sided endocarditis, Staphylococcus aureus IE,fungal IE, previ-ous IE, prolonged clinical symptoms (≥3 months), cyanotic congenital heart disease, patients with systemic to pulmonary shunts and those with poor clinical response to antimicrobial therapy are recognized to carry a high risk for developing complications in a patient with infective endo-carditis
CONGESTIVE CARDIAC FAILURE (CCF) : Congestive cardiac failure has the great-est impact on the prognosis of patients with infective endocarditis. Left sided endocarditis is more likely to develop CCF than right sided infective endocarditis. Aortic valve infective endocarditis is more likely to develop CCF (29%) than mitral valve (20%) or tricuspid valve (8%) infective endocarditis.Usually CCF develops insidiously with progressive worsening of valvular incompetence and ventricular dysfunction. CCF may also develop acutely as in acute rupture of chordae in mitral valve infective endocarditis, valve obstruction due to huge vegetation, prosthetic valve dehiscence, fistulae formation, valve leaflet perforation etc.CCF in infective endocarditis signifies a grave prognosis and is a predictor of poor outcome even after surgery.It is mandatory to operate on such patients at the earliest. Delay of sur-gery to extend preoperative antibiotic treatment carries with it the risk of permanent dysfunction. Class III or IV CCF has a very high risk for poor surgical outcome.
SYSTEMIC EMBOLIZATION : occur in 22 to 50% of cases of infective endocar-ditis. About 60 to 65% of embolic events occur in the CNS; with more than 95% of these in the Middle Cerebral Artery territory. Arterial beds in the lungs, coronaries, spleen, bowel and extremities are also very much prone. Left sided valveinfective endocarditis is more prone to give rise to emboli. Infective endocarditis due to Staphylococccus aureus, Candida, Abiotrophia species and HACEK organisms are important causative fac-tors. Most emboli are noted with two full weeks of treatment and the risk weans off gradually. Left sided vegetation especially of the mitral valve
and more than 1cm in size are at increased risk. Mitral valve vegeta-tions, irrespective of the size are associated with higher rates of embolism (25%) than aortic valve vegetation (10%). Anterior leaflet vegetation of mitral valve is more prone for embolisation, as the leaflet excursion occurs twice per heartbeat. Size and number of vegetations, number of valves involved and characteristics and mobility of vegetation are other less significant risk factors.Surgery to prevent further embolization is indicated if there has been two or more major embolic events. The advantage of prevention of further emboli exists only when surgery is done early in the course of Infective Endocarditis, when embolic rates are highest. Surgery should be consid-ered when large vegetation is detected on the mitral valve, particularly the anterior mitral leaflet. If inspite of adequate therapy, vegetation is found not to diminish in size or if it is still unstable on trans-esophageal echocar-diography, the risk of embolization is high and surgery may be indicated.
PERIANNULAR SPREAD OF INFECTIVE ENDOCARDITIS
Annular infection can break through and spread into nearby tissues, lead-ing to periannular ascess, pseudo aneurysm, sinuses or fistulae. Perian-nular spread predicts high mortality, and early need for cardiac surgery. Periannular spread complicates 10 to 40% of Infective Endocarditis. Aortic valve infective endocarditis is more prone to periannular spread than mitral or tricuspid valve infection. In prosthetic valve infective endo-carditis, periannular spread occurrence is very high (50 to 100%) as the primary infection is in the annulus and not the leaflets.Persistent bacteremia or fever, recurrent emboli, heart block, CCF or changes in characteristics of a murmur in a patient who is being inad-equately treated for infective endocarditis suggests possibility of perian-nular spread. TEE is the investigation of choice to look for and assess periannular spread.Surgery at the earliest is mandatory and includes drainage of abscess cavities, excision of necrotic tissue and closure of communicating tracts; apart from replacement of the infected valves. Grossly damaged perian-nular supporting tissues need major reconstruction using homograft.
mimslouranlfinal.indd 3 7/21/2004 11:05:55 PM
04 - 2004
rid of this.
recently described sutureless anastomotic device [Calafiore 2001].
studies of our patients in this series, to confirm their long-term patency.
REFERENCES
saphenous vein to the aorta. J Thorac Cardiovasc Surg 121:854-8.
Cardiology 80:215-25.
in 220 patients. J Thorac Cardiovasc Surg 110: 979-87.
in place with care, so as to avoid a purse string effect.
RESULTS
-
angiography after one year to assess the patencies of their grafts.
DISCUSSION
and the complexity of the surgical procedure [Mohan 1992].
such as those with post infarction angina and a low ejection fraction.
MIMS HEART JOURNAL JULY
Off-Pump coronary artery bypass grafting avoids extra corporeal circula-tion and has shown to reduce the clinically relevant morbidity, especially with regard to neurologic complications. Manipulating the ascending aorta by side-clamping is a definite risk factor and VAO helps us to get
Surgeon’s skill is an important factor in performing proximal anastamoses with VAO. One advantage here is that we can perform either the proximal or the distal anastamosis first, an option that is not possible with the
VAO device is made of steel, is reusable, and costs only US$ 10 to fab-ricate it. Side-clamping of the aorta can be avoided, and hence there is no need to bring down the systolic pressure below 100 mm Hg. There is no injury to the vein initima, because nothing is introduced into the vein. The suturing procedure takes not more than 10 minutes, and the learning curve is very short or negligible. VAO can also be used in calcified aortas if a small island of normal tissue is available. Our clinical results are excellent; we are now waiting of the one-year postoperative angiographic
1. Calafiore AM, Barel Y, Vitolla G, 2001. Early clinical experience with a new sutureless anastomotic device for proximal anastamosis of the
2. Mohan R, Amsel BJ, Walter PJ.1992. Coronary artery bypass in the elderly: a review of studies on patients older than 64, 69 or 74 years.
3. Moshkovitz Y, Luski A, Mohr R.1995. Coronary artery bypass without cardiopulmonary bypass: analysis of short-term and mid-term outcome
The sutures in the vein have to be inside out, and in the aorta, they have to be outside in. The aortic sutures are placed so that the needle passes through the aortic wall, goes into the groove of the Obturator, and comes out between the aorta and the metal, thus taking the intima. The sutures are placed all around the aortic punch hole and are loosely held. Once the suturing is complete, the obturator is removed, and the left index finger is positioned on the aortic punch hole to prevent bleeding. The loose sutures are pulled and tightened with a nerve hook. The assistant holds the two ends of the sutures firmly with controlled traction during this procedure. Once all of the sutures are in place, the two ends are tied snugly. The two snares on the purse string are removed, and they are tied
We have performed 269 proximal anastomoses on 177 patients. Initially, most were performed with proximal anastamosis first so that the flow in the vein grafts could be fully assessed. But with experience, we now do distal anastamosis first. We have had no postoperative ischemia, or perioperative infarction in any of our patients. We have had no perioperative mortality in our coronary patients. One patient presented with angina after 12 weeks, and check angiogram results showed a perfectly patent graft. We are planning to follow up these patients and to repeat coronary
With the present-day degree of myocardial protection and refinement in surgical technique, the mortality and morbidity of coronary artery surgery is related more to the co morbidities of patients than to cardiac function
Avoiding cardiopulmonary bypass [Moshkovitz 1995] has further con-tributed to the reduction of mortality and morbidity in high-risk patients,

20 MIMS HEART JOURNAL - 2004 JULY
08MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY17.
SURGICAL MANAGEMENT OF INFECTIVE ENDOCARDITISSurgery in patients with active native valve endocarditis is indicated in the presence of life threatening congestive heart failure or cardiogenic shock , embolic episodes, intractable arrythmias, progressive renal fail-ure, Staphylococcal or fungal endocarditis or uncontrolled sepsis, if the
patient has reasonable prospects of recovery with satisfactory quality of life after the operation. Surgery should not be delayed in the setting of Acute Infective Endocarditis when congestive heart failure intervenes. Surgery is not indicated if complications (severe embolic cerebral dam-age) or co-morbid conditions make the prospect of recovery remote. The indications for surgery for infective endocarditis in patients with stable haemodynamics are less clear. Surgical management of healed native valve endocarditis depends on the severity of the valvular lesion or the haemodynamic severity of the defect. Surgery is recommended in patients with annular or aortic ab-scesses, those with infections resistant to antibiotic therapy and those with fungal endocarditis. It is recognized that the presence of valvular vegetations poses a threat of embolic events. Echocardiography, espe-cially with transesophageal imaging, identifies vegetation and provides size estimation in many instances. Patients with a vegetation > 10 mm in diameter have a significantly higher incidence of embolization than those with a vegetation diameter < 10 mm, and this risk appears to be higher in patients with mitral valve endocarditis than aortic valve endocarditis. However, operation on the basis of vegetation size alone is controversial.Early prosthetic valve endocarditis patients need surgery if there is cardiac failure, valve obstruction due to vegetations or valve regurgitation or the causative organism is Staphylococcus. Late prosthetic valve endocarditis patients should be subjected to surgery if there is advanced heart failure or embolic episodes or continuing sepsis or if the offending organism is Staphylococcus. Patients with prosthetic valves receiving warfarin antico-agulation who develop endocarditis should have their warfarin discon-tinued and replaced with heparin. This recommendation is less related
to the possibility of haemorrhagic complications of endocarditis than the possibility of anticipating an urgent surgery. If surgery is required, the effects of warfarin will have dissipated and heparin can easily be re-versed. Likewise, aspirin, if part of the medical regimen, should also be discontinued. If neurological symptoms develop, anticoagulation should be discontinued until an intracranial haemorrhagic event is excluded by MRI or CT scanning.
RECOMMENDATIONS FOR SURGERY IN NATIVE VALVE ENDOCARDITIS
INDICATIONSAcute AR or MR with heart failure Acute AR with tachycardia and early closure of the mitral valve Fungal endocarditis Evidence of annular or aortic abscess, sinus or aortic true or false aneurysm Evidence of valve dysfunction and persistent infection after a prolonged period (7-10 days) of appropriate antibiotic therapy as indicated by presence of fever, leukocytosis and bacteremia, provided there are no non-cardiac causes forinfection Recurrent emboli after appropriate antibiotic therapy Infection with gram negative organisms or organisms with a poor response to antibiotics in patients with evidence of valve dysfunction Mobile vegetations > 10 mm
RECOMMENDATIONS FOR SURGERY IN PROSTHETIC VALVE ENDOCARDITIS
INDICATIONS Early prosthetic valve endocarditis (first two months or less after surgery) Heart failure with prosthetic valve dysfunction Fungal endocarditis Staphylococcal endocarditis not responding to antibiotic ther apy Evidence of paravalvular leak, annular or aortic abscess, sinus or aortic true or false aneurysm, fistula formation or new onset conduction disturbances Infection with gram negative organisms or organisms with poor response to antibiotics Persistent bacteremia after a prolonged course (7-10 days) of appropriate antibiotic therapy without non cardiac causes for bacteremia Recurrent peripheral embolus despite therapy
AntibioticDosageandRouteDurationCommentsAqueouscrystallinepenicillinGsodiumor
Ceftriaxonesodium
12-18millionU/24hIVeithercontinu-ouslyorin6equallydivideddoses.
2goncedailyIVorIM
4weeks
4weeks
Preferredinmostpatients>65yandthosewithimpairmentoftheeighthnerveorrenalfunction
AqueouscrystallinepenicillinGsodiumWith
Gentamycinsulfate
12-18millionU/24hIVeithercontinu-ouslyorin6equallydivideddoses.
1mg/kgIMorIVevery8h
2weeks
2weeks
Whenobtained1haftera20-30minIVinfusionorIMinjection.Serumconcentrationofgentamycinofapproximately3microg/mL,isdesirable;thoughconcentrationshouldbe<1microg/mL
Vancomycinhydrochloride30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
4weeksVancomycintherapyisrecommendedforpatientsallergictobetalactams;peakserumconcentrationofvanco-mycinshouldbeobtained1haftercompletionofinfusionandshouldbeintherangeof30-45microg/mLfortwicedailydosing.
ANTIBIOTICREGIMENFORBACTERIALENDOCARDITIS–AHAGUIDELINESNativevalveendocarditisinvolvingpenicillinsusceptibleStreptococcusviridansandStreptococcusbovis(MinimumInhibitoryConcentration<0.1microg/mL)
AntibioticDosageandRouteDurationComments
AqueouscrystallinepenicillinGsodium
WithGentamicinsulfate
18millionU/24hIVeithercontinuouslyorin6equallydivideddoses
1mg/kgIMorIVevery8h
4weeks
2weeks
Preferredinmostpatients>65yandthosewithimpairmentoftheeighthnerveorrenalfunction
Vancomycinhydrochloride30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
4weeksVancomycintherapyisrecommendedforpatientsallergictobetalactams.
NativevalveendocarditisinvolvingStreptococcusviridansandStreptococcusbovisRelativelyResistanttoPenicillinG(MinimumInhibitoryConcentration>0.1microg/mLand<0.5microg/mL)
Ischaemic Heart Disease is the most common cause of death worldwide. Though the death rate for coronary artery disease has decreased over the past few decades, the incidence has remained constant or increased. Acute Coronary Syndrome (ACS) is a new term that encompasses many permutations of acute ischaemic heart disease. Patients who present with signs or symptoms of acute ischaemic heart disease are now described as having Acute Coronary Syndrome.
The first step in evaluation is an ECG, which allows acute coronary syn-drome to be broadly grouped into two, based on the presence or absence of ST segment elevation. Those with ST elevation are labeled Acute Myo-cardial Infarction or ST elevation myocardial infarction (STEMI) and are eligible for thrombolysis. Non-ST elevation ACS encompasses a broader range of entities including rest angina, new onset angina, unstable an-gina, post infarction angina, variant angina and Non-STEMI. The final diagnosis depends on serial ECG evaluation and blood tests for various cardiac markers. Grouping all these under one umbrella emphasizes the urgent nature of the problem and provides a starting point for a series of decision making that rapidly determine the optimal line of manage-ment.
Today Non ST elevation ACS accounts for majority of coronary care unit admissions. Although majority of ACS patients stabilize, in-hospital Myo-cardial Infarction occurs in >10% and a few die suddenly. Various stud-ies have reported death rates between 2.9 to 4 %, reinfarction rate of 5 to 12 % and stroke rate of 0.4% to 0.9 % in ACS patients.
Morbidity and mortality can be reduced either by strategies for prevention of an acute cardiac event or by improved management. Primary preven-tion aims at reducing the risk factors like cholesterol, tobacco etc. Second-ary prevention focuses on early detection and treatment of asymptomatic disease by screening ECGs, good diabetic control etc. Tertiary prevention is the treatment which alters the course of clinical disease like coronary angioplasty or CABG. However, even the best of preventive strategies will not eliminate coronary artery disease and patients do and will continue to present with ACS, leaving cost effective therapeutic intervention which provide good long term clinical outcome as the only option left.Management of ACS depends on the risk stratification of such patients. Those patients with probable ACS undergo detailed history, clinical ex-amination and ECG. Based on the risk to which they are exposed, pa-tients are grouped into low, intermediate and high-risk groups. Low risk patients are managed in the OP department. Those with intermediate risk are given acute intensive care, stabilized and worked up for further management. Those with high risk are considered for early reperfusion therapy.Patients with high risk include (i) men> 60 years and women > 70 years with definite angina (ii) haemodynamic or ECG changes with pain (iii) marked symmetrical T wave inversion in precordial leads (iv) ST seg-ment elevation or depression of > 1mm (v) variant anginaThose with intermediate risk include (i) Men< 60 years and women < 70 years with definite angina; or Men > 60 years and women > 70 years with probable angina; (ii) Diabetes with two other risk factors (smoking, hypertension, elevated cholesterol); (iii) probable non-anginal pain in diabetes, (iv) extracardiac vascular diseases, (v) ST depression
OPCAB FOR ACUTE CORONARY SYNDROMETHE WAY TO GO
Dr. Baburajan. A.KCardaic Surgeon
mimslouranlfinal.indd 7 7/21/2004 11:13:21 PM
- 2004 05
role as an intensivist.
until the patient is safely transferred from the ICU to the ward.
are needed to bring them out safely.
MANAGEMENT AFTER CARDIAC SURGERY WHERE WE STAND TODAY
and reperfusion injury.
with CPB assistance.
(good diuresis.
in LV function.
MIMS HEART JOURNAL JULY ..
Postoperative care of cardiac surgery patient is as important as the intraoperative management. The cardiac anesthesiologist’s duty does not get over in the operation theater, but also continues in the postoperative period in the cardiac surgical ICU. In the ICU, the cardiac anaesthesiolo-gist closely monitors the vitals of the patient, achieves haemodynamic stability with appropriate use of inotropes or vasodilators, makes changes in the ventilator management as guided by the Arterial Blood Gas (ABG) reports and extubates the patient under optimal conditions. Hence his
In contrast to the general surgical patient, the cardiac surgical patient requires continuation of the invasive and non-invasive monitoring for at least another 24 – 48 hours after the extubation. The cardiac anaesthe-siologist along with the cardiac surgeon continues the postoperative care,
The current trend of coronary artery disease is taking a new turn with more and more younger age group of patients getting diffusely diseased pattern. Also post-infarction angina group patients are also taken up for surgery immediately after MI. Smoking from young age leads to badly affected lungs as evidenced by the less pul-monary reserve. These patients are prone for various complications and different strategies
POST INFARCT ANGINA PATIENTS The patients who had recent MI presenting with post infarction angina will require an-giographic evaluation and further intervention in the form of either angioplasty or CABG. The ACC guidelines recommend that CABG can be done safely 72 hours after MI. These patients present with angina after MI. Their LV function is not optimal and wall motion abnormalities, common. The induction of anaesthesia is more likely to produce hypotension, which may spi-
INTENSIVE CARE
ral down to a cardiac arrest. Heart lung machine is kept ready and the surgical team gets ready before the induction of anaesthesia. Intraopera-tively these patients are more prone for the development of arrhythmias
After coronary angiogram, femoral arterial sheath is kept in situ. A femo-ral venous sheath is also kept ready for temporary pacing. A 4-lumen central venous catheter is introduced through the internal jugular vein either in the cath lab or in the coronary care unit. Once the patient ar-rives the OR, the arterial line is connected to the femoral sheath and inotropes are connected to the central line. Induction of anaesthesia is done with utmost care to avoid hypotension. Anaesthetic agents causing myocardial depression are avoided. Coronary artery bypass grafting is done on beating heart either without the use of heart lung machine or
A pulmonary artery catheter with continuous cardiac output monitoring facility is used to guide the inotropes and vasopressors dosage. Intra aortic balloon pump will be required if the cardiac output remains low in spite of maximal inotropic therapy. Vasopressors are required if Systemic
vascular resistance (SVR) is low and the car-diac output is high with low arterial pressure. Urine output has to be monitored closely when vasopressors are used. A continuous infusion of furosemide is useful to reduce the Pulmo-nary vascular resistance PVR) and to maintain
We have operated on 46 patients with acute coronary syndrome with excellent results. Intra aortic balloon pump (IABP) was not required in any of these patients. Their cardiac output increased significantly in the postoperative period. Echocardiography done 1 week after the surgery showed significant improvement
Dr. A.V. Kannan Chief Cardiac Anaesthesiologist

MIMS HEART JOURNAL - 2004 JULY 19..
18 MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY07.
Antibiotic Dosage and Route Duration CommentsRegimen for methicillin-resistant staphylococcis
Vancomycin hydrochloride
With Rifampicin andWith Gentamycin sulphate
30mg/kg per 24 h IV in 2 equallydivided doses, not to exceed 2g/24 hunless serum levels are monitored300 mg orally every 8 h1.0 mg/kg IM or IV every 8 h
≥ 6 weeks
≥ 6 weeks2 weeks
Rifampicin increase the amount of warfarinsodium required for antithrombotic therapy
Regimen for methicillin-susceptible staphylococci
Nafcillin sodium or Oxacillin sodium
With Rifampicin andWith Gentamycin sulphate
2 g IV every 4 h
300 mg orally every 8 h1.0 mg/kg IM or IV every 8 h
≥ 6 weeks
≥ 6 weeks2 weeks
First-generation cephalolosporins or vanco-mycin should be used in patients allergic tobeta-lactam.Cephalosporins should be avoided inpatients with immediate-type hypersensitiv-ity to penicillin or with methicillin-resistantstaphylococci
Endocarditis due to staphylococcus in the presence of a Prosthetic Valve or other Prosthetic Material.
Antibiotic Dosage and Route Duration CommentsRegimen for methicillin-resistant staphylococcis
Ceftriaxone sodium
Ampicillin sodium
With gentamycin sulphate
2 g once daily IV or IM
12 g/ 24 h IV either continuously or in 6equally divided doses1 mg/kg IM or IV every 8 h
4 weeks
4 weeks
4 weeks
Cefotaxime sodium or other third-generationcephalosporins may be substituted
Therapy for Endocarditis due to HACEK microorganisms ( Haemophilus parainflenzae, Haemophilus aphrophilus, actinobacillus actinomy-cetemcomitans, Cardiobacterium Hominis, Eikenella corrodens and Kingella kingae
Antibiotic Dosage and Route Duration CommentsFungal Endocarditis
Amphotericin Bwith or withoutFlucytosine
1 mg/kg per day IV (total dose 2.0-2.5 g)
150 mg/kg per day PO in 4 divided doses
6-8 weeks
6-8 weeks
Culture-negative Endocarditis
Vancomycin plusgentamycin
15 mg/kg IV every 12 h1 mg/kg IM or IV every 8 h
6 weeks6 weeks
Fungal Endocarditis and Culture-Negative Endocarditis
Isolated Patent Ductus Arteriosus (PDA) is estimated to be present in one in 2000 term live births, accounting for about 5-10% of all types of Congenital Heart Diseases. The incidence in the preterm is higher.
Persistence of the ductus in the premature infant is due to physi-
ological developmental retardation. In the full-term infant, failure of the ductus to constrict postnatally is re-lated to a significant structural abnormality. The clinical features of Patent Ductus Arteriosus depend on the size of the communication, relationship between systemic and pulmonary vascular resistance and the ability of the myocardium to handle the extra volume load. INDICATION FOR CLOSUREPDA is an indication for closure; because of the risk of infective endo-carditis and the fact that the closure of PDA can be accomplished with virtually no risk. AGE AT CLOSURESpontaneous closure of PDA is unlikely beyond six months of age in term infants and 12 months of age in preterm infants. Such a cut-off is only arbitrary and closure is generally dictated by the clinical features conse-quent to the left to right shunt.Transcatheter closure has revolutionized management of PDA. In fact, PDA was the first lesion to be treated by transcatheter technique. The transcatheter closure has several advantages over surgical closure – less morbidity, absence of scar, comparable success rate and lack of anaes-thesia.
PROCEDUREThis is performed using conscious sedation in infants and young children, and local anaesthesia in older children and adults. Conscious sedation allows the child to return to full activity the following day. Closure can be accomplished with occluding coils or devices.A catheter is advanced from the femoral artery or the vein across the PDA. An occluding coil, made of stainless steel is placed in the PDA with a single coil loop on the pulmonary artery side and the remaining 3-4 loops in the ductal ampulla. Occasionally, multiple coils are required to achieve complete closure. The procedure success is 97% with no mortal-ity and no significant morbidity.The device we prefer is the Amplatzer Duct Occluder (ADO). This has
transformed percutaneous closure of large PDAs. The ADO is a self-expandable, highly elastic, mush-room shaped device, made from nitinol (Nickel-Titanium alloy) wire mesh. Dacron polyester fabric
sewn to the wire frame promotes thrombus formation The ADO has several desirable characteristics such as simplicity of use, ability to recapture and reposition the device, high (> 95%) complete closure rates and relatively small introducer sheath. Our patient age ranged from 1 year to 50 years and the size of the PDA from 2-6 mm. We prefer to deploy coils for small PDAs (<3mm) and the ADO for PDAs larger than 3mm. The procedural success has been 100% with no complications.As a matter of fact, with the introduction of the ADO, we have bid adieu to surgical closure for patent ductus arteriosus
TRANS CATHETER CLOSURE OF PATENTDUCTUS ARTERIOSUS WHERE WE STAND TODAY
Amplatzer Duct Occluder (ADO)
Coil closure of PDA
Dr. Asish Kumar.MCardiologist
AntibioticDosageandRouteDurationComments
AqueouscrystallinepenicillinGsodium
WithGentamycinsulfate
18-30millionU/24hIVeithercontinu-ouslyorin6equallydivideddoses
1mg/kgIMorIVevery8h
4-6weeks
4-6weeks
4-wktherapyrecommendedforpatientswithsymptoms<3monthsduration;6-wktherapyrecommendedforpatientswithsymptoms>3monthduration
Ampicillinsodium
WithGentamycinsulphate
12g/24hIVeithercontinuouslyorin6equallydivideddoses
1mg/kgIMorIVevery8h
4-6weeks
4-6weeks
Vancomycinhydrochloride
WithGentamycinsulphate
30mg/kgper24hin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
1mg/kgIMorIVevery8h
4-6weeks
4weeks
Vancomycintherapyisrecommendedforpatientsallergictobetalactams;cephalo-sporinsarenotacceptablealternativesforpatientsallergictopenicillin
StandardTherapyforEndocarditisDuetoEnterococci
AntibioticDosageandRouteDurationCommentsMethicillinsusceptiblestaphylococciRegimenfornon-betalactamallergicpatients
NafcillinsodiumorOxacillinsodium
WithoptionaladditionofGentamycinsulphate
2gevery4h
1mg/kgIMorIVevery8h
4-6weeks
3-5d
Benefitofadditionalaminoglycosideshasnotbeenestablished
Regimenforbetalactamallergicpatients
Cefazolin(orotherfirstgenerationcephalosporininequivalentdosages)
WithoptimaladditionofGentamycin
2gIVevery8h
1mg/kgIMorIVevery8h
4-6weeks
3-5d
Cephalosporinsshouldbeavoidedinpatientswithimmediatetypehypersensitiv-itytopenicillin)
Vancomycinhydrochloride30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
4-6weeksRecommendedforpatientsallergictopenicillin
Methicillin-resistantstaphylococci
Vancomycinhydrochloride30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
4-6weeks
EndocarditisduetostaphylococcusintheabsenceofProstheticMaterial
mimslouranlfinal.indd 6 7/21/2004 11:11:40 PM
- 2004
ARRHYTHMIAS
Occasionally Xylocard infusion is required to control them.
cardioversion.
hours.
albumin therapy may be indicated.
HAEMODYNAMIC MONITORING
blood flow and reduce the afterload of LV in necessary cases.
of postoperative bleeding due to inactive platelets is very high.
a coronary stent immediately after coronary angioplasty). The cardiac surgical ICU in MIMS has state of the art facilities 1. Motorized patient beds 2. Six channel modular monitors in each bed 3. Modern ventilators 4. Facilities for Non-Invasive ventilation 5. Vigilance monitor – continuous cardiac output monitoring 6. PiCCO continuous cardiac output monitoring 7. Syringe pumps for continuous infusion 8. Arterial blood gas analyzer with electrolytes and haematocrit measurement
able round the clock.
ing from the academic year 2003.
06 MIMS HEART JOURNAL JULY
Arrhythmias are common following cardiac surgery. Ventricular prema-ture contraction (VPC) is the most common arrhythmia and is usually due to hypokalemia. Following open heart surgery, the patients are prone for sodium retention and potassium excretion. In addition to this, diuretic therapy and insulin administration also lead to hypokalemia. These VPCs usually respond to potassium correction. When they persist even after the correction of potassium, 1-2 g of Magnesium is given over 30 min.
Atrial fibrillation is the second most common arrhythmia seen in our ICU. It is seen in about 8 % of our patients. The causes are hypoxemia, valve surgery, pneumothorax or haemothorax and preoperative AF. In-travenous infusion of amiodarone is our first line of management, which helps in achieving the sinus rhythm faster. In some patients, Digoxin and Magnesium sulphate are used along with Amiodarone. Rarely they need
VENTILATOR MANAGEMENT We practice “FAST TRACKING” in most of the patients after cardiac sur-gery. When the patient comes to ICU, he will be on SIMV mode and continuous infusion of sedative is given. A warming blanket is used, if the patient is hypothermic. Once the patient becomes fully warm, hae-modynamically stable and mediastinal drainage is minimal, sedation is stopped. The awake patient is kept on pressure support ventilation for a short while and extubated. This process usually takes about 4 – 6
If the patients are suspected to have pulmonary dysfunction or neurologi-cal dysfunction postoperatively, then they will be ventilated for a longer period. In case of acute lung injury (ALI) or adult respiratory distress syn-drome (ARDS), we use pressure-controlled ventilation to tide over the cri-sis along with aggressive diuretic therapy. Generally post cardiac surgical patients are prone for sodium and water retention and will require good dose of diuretics to drive fluid out of the interstitial space. Occasionally
All our patients have three channel ECG monitoring, invasive blood pres-sure monitoring, CVP monitoring, SpO2, ETCO2 and temperature moni-toring in the OT as well as in the ICU. When the patient is suspected to have low cardiac output syndrome, as seen by the requirement of high dose of inotropes, we resort to insertion of Swan Ganz catheter. A regu-lar pulmonary artery (PA) catheter gives systolic PA pressure, diastolic PA pressure and pulmonary capillary wedge pressure (PCWP). PCWP is indirectly indicative of left ventrcular end diastolic pressure (LVEDP). A thermodilution PA catheter is used to get more information like cardiac output, SVR and other derived parameters. We use a special PA catheter called ‘COMBO’ catheter, which gives continuous cardiac output. This is very useful in guiding us towards appropriate use of inotropes and va-sopressors. Intra Aortic Balloon Pump is used to augment the coronary
POSTOPERATIVE COAGULATION PROBLEMS In cardiac surgery, the coagulation system is the most affected one, after the heart. Every patient’s coagulation pathway is inhibited by the admin-istration of anticoagulant drug- heparin. When the patient is connected to cardiopulmonary bypass (CPB), blood is exposed to nonphysiological surfaces. CPB leads to platelet dysfunction in the postoperative period. If the patient is on anti-platelet drugs like aspirin or clopidogrel, the chance
With the recent development of off-pump (beating heart) coronary artery bypass grafting surgery, where heart lung machine is avoided, we ex-pect less coagulation problems. On the contrary, beating heart surgery leads to a procoagulant state and predisposes to the development of intra coronary thrombosis and graft occlusion in the immediate postoperative period. (This situation is analogous to the development of thrombosis in
9. Intra Aortic Balloon Pump (IABP) This infrastructure of international standards is supported by a team of cardiac surgeons, cardiac anaesthesiologists and other personnel avail-
PDCC in Cardiac Anaesthesia and Critical Care is a one year course start-

06MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY19..
18 MIMS HEART JOURNAL - 2004 JULY
AntibioticDosageandRouteDurationCommentsRegimenformethicillin-resistantstaphylococcis
Vancomycinhydrochloride
WithRifampicinandWithGentamycinsulphate
30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored300mgorallyevery8h1.0mg/kgIMorIVevery8h
≥6weeks
≥6weeks2weeks
Rifampicinincreasetheamountofwarfarinsodiumrequiredforantithrombotictherapy
Regimenformethicillin-susceptiblestaphylococci
NafcillinsodiumorOxacillinsodium
WithRifampicinandWithGentamycinsulphate
2gIVevery4h
300mgorallyevery8h1.0mg/kgIMorIVevery8h
≥6weeks
≥6weeks2weeks
First-generationcephalolosporinsorvanco-mycinshouldbeusedinpatientsallergictobeta-lactam.Cephalosporinsshouldbeavoidedinpatientswithimmediate-typehypersensitiv-itytopenicillinorwithmethicillin-resistantstaphylococci
EndocarditisduetostaphylococcusinthepresenceofaProstheticValveorotherProstheticMaterial.
AntibioticDosageandRouteDurationCommentsRegimenformethicillin-resistantstaphylococcis
Ceftriaxonesodium
Ampicillinsodium
Withgentamycinsulphate
2goncedailyIVorIM
12g/24hIVeithercontinuouslyorin6equallydivideddoses1mg/kgIMorIVevery8h
4weeks
4weeks
4weeks
Cefotaximesodiumorotherthird-generationcephalosporinsmaybesubstituted
TherapyforEndocarditisduetoHACEKmicroorganisms(Haemophilusparainflenzae,Haemophilusaphrophilus,actinobacillusactinomy-cetemcomitans,CardiobacteriumHominis,EikenellacorrodensandKingellakingae
AntibioticDosageandRouteDurationCommentsFungalEndocarditis
AmphotericinBwithorwithoutFlucytosine
1mg/kgperdayIV(totaldose2.0-2.5g)
150mg/kgperdayPOin4divideddoses
6-8weeks
6-8weeks
Culture-negativeEndocarditis
Vancomycinplusgentamycin
15mg/kgIVevery12h1mg/kgIMorIVevery8h
6weeks6weeks
FungalEndocarditisandCulture-NegativeEndocarditis
ARRHYTHMIAS Arrhythmias are common following cardiac surgery. Ventricular prema-ture contraction (VPC) is the most common arrhythmia and is usually due to hypokalemia. Following open heart surgery, the patients are prone for sodium retention and potassium excretion. In addition to this, diuretic therapy and insulin administration also lead to hypokalemia. These VPCs usually respond to potassium correction. When they persist even after the correction of potassium, 1-2 g of Magnesium is given over 30 min. Occasionally Xylocard infusion is required to control them.Atrial fibrillation is the second most common arrhythmia seen in our ICU. It is seen in about 8 % of our patients. The causes are hypoxemia, valve surgery, pneumothorax or haemothorax and preoperative AF. In-travenous infusion of amiodarone is our first line of management, which helps in achieving the sinus rhythm faster. In some patients, Digoxin and Magnesium sulphate are used along with Amiodarone. Rarely they need cardioversion.
VENTILATOR MANAGEMENTWe practice “FAST TRACKING” in most of the patients after cardiac sur-gery. When the patient comes to ICU, he will be on SIMV mode and continuous infusion of sedative is given. A warming blanket is used, if the patient is hypothermic. Once the patient becomes fully warm, hae-modynamically stable and mediastinal drainage is minimal, sedation is stopped. The awake patient is kept on pressure support ventilation for a short while and extubated. This process usually takes about 4 – 6 hours.If the patients are suspected to have pulmonary dysfunction or neurologi-cal dysfunction postoperatively, then they will be ventilated for a longer period. In case of acute lung injury (ALI) or adult respiratory distress syn-drome (ARDS), we use pressure-controlled ventilation to tide over the cri-sis along with aggressive diuretic therapy. Generally post cardiac surgical patients are prone for sodium and water retention and will require good dose of diuretics to drive fluid out of the interstitial space. Occasionally albumin therapy may be indicated.
HAEMODYNAMIC MONITORINGAll our patients have three channel ECG monitoring, invasive blood pres-sure monitoring, CVP monitoring, SpO2, ETCO2 and temperature moni-toring in the OT as well as in the ICU. When the patient is suspected to have low cardiac output syndrome, as seen by the requirement of high dose of inotropes, we resort to insertion of Swan Ganz catheter. A regu-lar pulmonary artery (PA) catheter gives systolic PA pressure, diastolic PA pressure and pulmonary capillary wedge pressure (PCWP). PCWP is indirectly indicative of left ventrcular end diastolic pressure (LVEDP). A thermodilution PA catheter is used to get more information like cardiac output, SVR and other derived parameters. We use a special PA catheter called ‘COMBO’ catheter, which gives continuous cardiac output. This is very useful in guiding us towards appropriate use of inotropes and va-sopressors. Intra Aortic Balloon Pump is used to augment the coronary blood flow and reduce the afterload of LV in necessary cases.
POSTOPERATIVE COAGULATION PROBLEMS In cardiac surgery, the coagulation system is the most affected one, after the heart. Every patient’s coagulation pathway is inhibited by the admin-istration of anticoagulant drug- heparin. When the patient is connected to cardiopulmonary bypass (CPB), blood is exposed to nonphysiological surfaces. CPB leads to platelet dysfunction in the postoperative period. If the patient is on anti-platelet drugs like aspirin or clopidogrel, the chance of postoperative bleeding due to inactive platelets is very high. With the recent development of off-pump (beating heart) coronary artery bypass grafting surgery, where heart lung machine is avoided, we ex-pect less coagulation problems. On the contrary, beating heart surgery leads to a procoagulant state and predisposes to the development of intra coronary thrombosis and graft occlusion in the immediate postoperative period. (This situation is analogous to the development of thrombosis in a coronary stent immediately after coronary angioplasty).The cardiac surgical ICU in MIMS has state of the art facilities1. Motorized patient beds2. Six channel modular monitors in each bed3. Modern ventilators 4. Facilities for Non-Invasive ventilation5. Vigilance monitor – continuous cardiac output monitoring6. PiCCO continuous cardiac output monitoring7. Syringe pumps for continuous infusion8. Arterial blood gas analyzer with electrolytes and haematocrit measurement 9. Intra Aortic Balloon Pump (IABP)This infrastructure of international standards is supported by a team of cardiac surgeons, cardiac anaesthesiologists and other personnel avail-able round the clock.PDCC in Cardiac Anaesthesia and Critical Care is a one year course start-ing from the academic year 2003.
Antibiotic Dosage and Route Duration Comments
Aqueous crystalline penicillin G sodium
WithGentamycin sulfate
18-30 million U/24 h IV either continu-ously or in 6 equally divided doses
1 mg/kg IM or IV every 8 h
4-6 weeks
4-6 weeks
4-wk therapy recommended for patientswith symptoms <3 months duration; 6-wktherapy recommended for patients withsymptoms >3 month duration
Ampicillin sodium
WithGentamycin sulphate
12g/24 h IV either continuously or in 6equally divided doses
1mg/kg IM or IV every 8 h
4-6 weeks
4-6 weeks
Vancomycin hydrochloride
WithGentamycin sulphate
30 mg/kg per 24 h in 2 equally divideddoses, not to exceed 2g/ 24 h unlessserum levels are monitored
1 mg/kg IM or IV every 8 h
4-6 weeks
4 weeks
Vancomycin therapy is recommended forpatients allergic to beta lactams; cephalo-sporins are not acceptable alternatives forpatients allergic to penicillin
Standard Therapy for Endocarditis Due to Enterococci
Antibiotic Dosage and Route Duration CommentsMethicillin susceptible staphylococciRegimen for non-beta lactam allergic patients
Nafcillin sodium or Oxacillin sodium
With optional addition of Gentamycin sulphate
2 g every 4 h
1 mg/kg IM or IV every 8 h
4-6 weeks
3-5 d
Benefit of additional aminoglycosides hasnot been established
Regimen for beta lactam allergic patients
Cefazolin (or other first generation cephalosporin inequivalent dosages)
With optimal addition of Gentamycin
2 g IV every 8 h
1 mg/kg IM or IV every 8 h
4-6 weeks
3-5 d
Cephalosporins should be avoided inpatients with immediate type hypersensitiv-ity to penicillin)
Vancomycin hydrochloride 30mg/kg per 24 h IV in 2 equallydivided doses, not to exceed 2g/24 hunless serum levels are monitored
4-6 weeks Recommended for patients allergic topenicillin
Methicillin-resistant staphylococci
Vancomycin hydrochloride 30mg/kg per 24 h IV in 2 equallydivided doses, not to exceed 2g/24 hunless serum levels are monitored
4-6 weeks
Endocarditis due to staphylococcus in the absence of Prosthetic Material
mimslouranlfinal.indd 67/21/2004 11:11:40 PM
- 2004 07.
Congenital Heart Diseases. The incidence in the preterm is higher.
lated to a significant structural abnormality.
load. INDICATION FOR CLOSURE
virtually no risk. AGE AT CLOSURE
quent to the left to right shunt.
thesia.
PROCEDURE
accomplished with occluding coils or devices.
ity and no significant morbidity.
nitinol alloy)
several desirable characteristics
introducer sheath.
with no complications.
to surgical closure for patent ductus arteriosus
DUCTUS ARTERIOSUS WHERE WE STAND TODAY
f PDA
MIMS HEART JOURNAL JULY
Isolated Patent Ductus Arteriosus (PDA) is estimated to be present in one in 2000 term live births, accounting for about 5-10% of all types of
Persistence of the ductus in the premature infant is due to physi-
ological developmental retardation. In the full-term infant, failure of the ductus to constrict postnatally is re-
The clinical features of Patent Ductus Arteriosus depend on the size of the communication, relationship between systemic and pulmonary vascular resistance and the ability of the myocardium to handle the extra volume
PDA is an indication for closure; because of the risk of infective endo-carditis and the fact that the closure of PDA can be accomplished with
Spontaneous closure of PDA is unlikely beyond six months of age in term infants and 12 months of age in preterm infants. Such a cut-off is only arbitrary and closure is generally dictated by the clinical features conse-
Transcatheter closure has revolutionized management of PDA. In fact, PDA was the first lesion to be treated by transcatheter technique. The transcatheter closure has several advantages over surgical closure – less morbidity, absence of scar, comparable success rate and lack of anaes-
This is performed using conscious sedation in infants and young children, and local anaesthesia in older children and adults. Conscious sedation allows the child to return to full activity the following day. Closure can be
A catheter is advanced from the femoral artery or the vein across the PDA. An occluding coil, made of stainless steel is placed in the PDA with a single coil loop on the pulmonary artery side and the remaining 3-4 loops in the ductal ampulla. Occasionally, multiple coils are required to achieve complete closure. The procedure success is 97% with no mortal-
The device we prefer is the Amplatzer Duct Occluder (ADO). This has transformed percutaneous closure of large PDAs. The ADO is a self-expandable, highly elastic, mush-room shaped device, made from
(Nickel-Titanium wire mesh. Dacron polyester fabric
sewn to the wire frame promotes thrombus formation The ADO has
such as simplicity of use, ability to recapture and reposition the device, high (> 95%) complete closure rates and relatively small
Our patient age ranged from 1 year to 50 years and the size of the PDA from 2-6 mm. We prefer to deploy coils for small PDAs (<3mm) and the ADO for PDAs larger than 3mm. The procedural success has been 100%
As a matter of fact, with the introduction of the ADO, we have bid adieu
TRANS CATHETER CLOSURE OF PATENT
Amplatzer Duct Occluder (ADO)
Coil closure o
Dr. Asish Kumar.M Cardiologist

20MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY05..
MIMS HEART JOURNAL - 2004 JULY 17.
Postoperative care of cardiac surgery patient is as important as the intraoperative management. The cardiac anesthesiologist’s duty does not get over in the operation theater, but also continues in the postoperative period in the cardiac surgical ICU. In the ICU, the cardiac anaesthesiolo-gist closely monitors the vitals of the patient, achieves haemodynamic stability with appropriate use of inotropes or vasodilators, makes changes in the ventilator management as guided by the Arterial Blood Gas (ABG) reports and extubates the patient under optimal conditions. Hence his role as an intensivist. In contrast to the general surgical patient, the cardiac surgical patient requires continuation of the invasive and non-invasive monitoring for at least another 24 – 48 hours after the extubation. The cardiac anaesthe-siologist along with the cardiac surgeon continues the postoperative care, until the patient is safely transferred from the ICU to the ward.The current trend of coronary artery disease is taking a new turn with more and more younger age group of patients getting diffusely diseased pattern. Also post-infarction angina group patients are also taken up for surgery immediately after MI. Smoking from young age leads to badly affected lungs as evidenced by the less pul-monary reserve. These patients are prone for various complications and different strategies are needed to bring them out safely.POST INFARCT ANGINA PATIENTS
The patients who had recent MI presenting with post infarction angina will require an-giographic evaluation and further intervention in the form of either angioplasty or CABG. The ACC guidelines recommend that CABG can be done safely 72 hours after MI. These patients present with angina after MI. Their LV function is not optimal and wall motion abnormalities, common. The induction of anaesthesia is more likely to produce hypotension, which may spi-
INTENSIVE CARE MANAGEMENT AFTER CARDIAC SURGERY WHERE WE STAND TODAY
ral down to a cardiac arrest. Heart lung machine is kept ready and the surgical team gets ready before the induction of anaesthesia. Intraopera-tively these patients are more prone for the development of arrhythmias and reperfusion injury.After coronary angiogram, femoral arterial sheath is kept in situ. A femo-ral venous sheath is also kept ready for temporary pacing. A 4-lumen central venous catheter is introduced through the internal jugular vein either in the cath lab or in the coronary care unit. Once the patient ar-rives the OR, the arterial line is connected to the femoral sheath and inotropes are connected to the central line. Induction of anaesthesia is done with utmost care to avoid hypotension. Anaesthetic agents causing myocardial depression are avoided. Coronary artery bypass grafting is done on beating heart either without the use of heart lung machine or with CPB assistance.A pulmonary artery catheter with continuous cardiac output monitoring facility is used to guide the inotropes and vasopressors dosage. Intra aortic balloon pump will be required if the cardiac output remains low in spite of maximal inotropic therapy. Vasopressors are required if Systemic
vascular resistance (SVR) is low and the car-diac output is high with low arterial pressure. Urine output has to be monitored closely when vasopressors are used. A continuous infusion of furosemide is useful to reduce the Pulmo-nary vascular resistance (PVR) and to maintain good diuresis.We have operated on 46 patients with acute coronary syndrome with excellent results. Intra aortic balloon pump (IABP) was not required in any of these patients. Their cardiac output increased significantly in the postoperative period. Echocardiography done 1 week after the surgery showed significant improvement in LV function.
Dr. A.V. KannanChief Cardiac Anaesthesiologist
SURGICAL MANAGEMENT OF INFECTIVE ENDOCARDITISSurgery in patients with active native valve endocarditis is indicated in the presence of life threatening congestive heart failure or cardiogenic shock , embolic episodes, intractable arrythmias, progressive renal fail-ure, Staphylococcal or fungal endocarditis or uncontrolled sepsis, if the
patient has reasonable prospects of recovery with satisfactory quality of life after the operation. Surgery should not be delayed in the setting of Acute Infective Endocarditis when congestive heart failure intervenes. Surgery is not indicated if complications (severe embolic cerebral dam-age) or co-morbid conditions make the prospect of recovery remote. The indications for surgery for infective endocarditis in patients with stable haemodynamics are less clear. Surgical management of healed native valve endocarditis depends on the severity of the valvular lesion or the haemodynamic severity of the defect. Surgery is recommended in patients with annular or aortic ab-scesses, those with infections resistant to antibiotic therapy and those with fungal endocarditis. It is recognized that the presence of valvular vegetations poses a threat of embolic events. Echocardiography, espe-cially with transesophageal imaging, identifies vegetation and provides size estimation in many instances. Patients with a vegetation > 10 mm in diameter have a significantly higher incidence of embolization than those with a vegetation diameter < 10 mm, and this risk appears to be higher in patients with mitral valve endocarditis than aortic valve endocarditis. However, operation on the basis of vegetation size alone is controversial.Early prosthetic valve endocarditis patients need surgery if there is cardiac failure, valve obstruction due to vegetations or valve regurgitation or the causative organism is Staphylococcus. Late prosthetic valve endocarditis patients should be subjected to surgery if there is advanced heart failure or embolic episodes or continuing sepsis or if the offending organism is Staphylococcus. Patients with prosthetic valves receiving warfarin antico-agulation who develop endocarditis should have their warfarin discon-tinued and replaced with heparin. This recommendation is less related
to the possibility of haemorrhagic complications of endocarditis than the possibility of anticipating an urgent surgery. If surgery is required, the effects of warfarin will have dissipated and heparin can easily be re-versed. Likewise, aspirin, if part of the medical regimen, should also be discontinued. If neurological symptoms develop, anticoagulation should be discontinued until an intracranial haemorrhagic event is excluded by MRI or CT scanning.
RECOMMENDATIONS FOR SURGERY IN NATIVE VALVE ENDOCARDITIS
INDICATIONSAcute AR or MR with heart failure Acute AR with tachycardia and early closure of the mitral valve Fungal endocarditis Evidence of annular or aortic abscess, sinus or aortic true or false aneurysm Evidence of valve dysfunction and persistent infection after a prolonged period (7-10 days) of appropriate antibiotic therapy as indicated by presence of fever, leukocytosis and bacteremia, provided there are no non-cardiac causes forinfection Recurrent emboli after appropriate antibiotic therapy Infection with gram negative organisms or organisms with a poor response to antibiotics in patients with evidence of valve dysfunction Mobile vegetations > 10 mm
RECOMMENDATIONS FOR SURGERY IN PROSTHETIC VALVE ENDOCARDITIS
INDICATIONS Early prosthetic valve endocarditis (first two months or less after surgery) Heart failure with prosthetic valve dysfunction Fungal endocarditis Staphylococcal endocarditis not responding to antibiotic ther apy Evidence of paravalvular leak, annular or aortic abscess, sinus or aortic true or false aneurysm, fistula formation or new onset conduction disturbances Infection with gram negative organisms or organisms with poor response to antibiotics Persistent bacteremia after a prolonged course (7-10 days) of appropriate antibiotic therapy without non cardiac causes for bacteremia Recurrent peripheral embolus despite therapy
Antibiotic Dosage and Route Duration CommentsAqueous crystalline penicillin G sodiumor
Ceftriaxone sodium
12-18 million U/24 h IV either continu-ously or in 6 equally divided doses.
2g once daily IV or IM
4 weeks
4 weeks
Preferred in most patients > 65 yand those with impairment of theeighth nerve or renal function
Aqueous crystalline penicillin G sodiumWith
Gentamycin sulfate
12-18 million U/24 h IV either continu-ously or in 6 equally divided doses.
1 mg/kg IM or IV every 8 h
2 weeks
2 weeks
When obtained 1 h after a 20-30min IV infusion or IM injection.Serum concentration of gentamycinof approximately 3 micro g/mL,is desirable; though concentrationshould be <1microg/mL
Vancomycin hydrochloride 30 mg/kg per 24 h IV in 2 equallydivided doses, not to exceed 2g/24 hunless serum levels are monitored
4 weeks Vancomycin therapy is recommendedfor patients allergic to beta lactams;peak serum concentration of vanco-mycin should be obtained 1 h aftercompletion of infusion and should bein the range of 30-45microg/mL fortwice daily dosing.
ANTIBIOTIC REGIMEN FOR BACTERIAL ENDOCARDITIS – AHA GUIDELINESNative valve endocarditis involving penicillin susceptible Streptococcus viridans and Streptococcus bovis (Minimum Inhibitory Concentration< 0.1 microg/mL)
Antibiotic Dosage and Route Duration Comments
Aqueous crystalline penicillin G sodium
WithGentamicin sulfate
18 million U/24 h IV either continuouslyor in 6 equally divided doses
1 mg/kg IM or IV every 8 h
4 weeks
2 weeks
Preferred in most patients > 65 y andthose with impairment of the eighth nerveor renal function
Vancomycin hydrochloride 30 mg/kg per 24 h IV in 2 equallydivided doses, not to exceed 2 g/24 hunless serum levels are monitored
4 weeks Vancomycin therapy is recommended forpatients allergic to beta lactams.
Native valve endocarditis involving Streptococcus viridans and Streptococcus bovis Relatively Resistant to Penicillin G (Minimum InhibitoryConcentration > 0.1 microg/mL and <0.5 microg/mL)
mimslouranlfinal.indd 77/21/2004 11:13:21 PM
08 - 2004MIMS HEART JOURNAL JULY
Dr. Baburajan. A.K Cardaic Surgeon OPCAB FOR
ACUTE CORONARY SYNDROME THE WAY TO GO
Ischaemic Heart Disease is the most common cause of death worldwide. Though the death rate for coronary artery disease has decreased over the past few decades, the incidence has remained constant or increased. Acute Coronary Syndrome (ACS) is a new term that encompasses many permutations of acute ischaemic heart disease. Patients who present with signs or symptoms of acute ischaemic heart disease are now described as having Acute Coronary Syndrome.
The first step in evaluation is an ECG, which allows acute coronary syn-drome to be broadly grouped into two, based on the presence or absence of ST segment elevation. Those with ST elevation are labeled Acute Myo-cardial Infarction or ST elevation myocardial infarction (STEMI) and are eligible for thrombolysis. Non-ST elevation ACS encompasses a broader range of entities including rest angina, new onset angina, unstable an-gina, post infarction angina, variant angina and Non-STEMI. The final diagnosis depends on serial ECG evaluation and blood tests for various cardiac markers. Grouping all these under one umbrella emphasizes the urgent nature of the problem and provides a starting point for a series of decision making that rapidly determine the optimal line of manage-ment.
Today Non ST elevation ACS accounts for majority of coronary care unit admissions. Although majority of ACS patients stabilize, in-hospital Myo-cardial Infarction occurs in >10% and a few die suddenly. Various stud-ies have reported death rates between 2.9 to 4 %, reinfarction rate of 5 to 12 % and stroke rate of 0.4% to 0.9 % in ACS patients.
Morbidity and mortality can be reduced either by strategies for prevention of an acute cardiac event or by improved management. Primary preven-tion aims at reducing the risk factors like cholesterol, tobacco etc. Second-ary prevention focuses on early detection and treatment of asymptomatic disease by screening ECGs, good diabetic control etc. Tertiary prevention is the treatment which alters the course of clinical disease like coronary angioplasty or CABG. However, even the best of preventive strategies will not eliminate coronary artery disease and patients do and will continue to present with ACS, leaving cost effective therapeutic intervention which provide good long term clinical outcome as the only option left. Management of ACS depends on the risk stratification of such patients. Those patients with probable ACS undergo detailed history, clinical ex-amination and ECG. Based on the risk to which they are exposed, pa-tients are grouped into low, intermediate and high-risk groups. Low risk patients are managed in the OP department. Those with intermediate risk are given acute intensive care, stabilized and worked up for further management. Those with high risk are considered for early reperfusion therapy. Patients with high risk include (i) men> 60 years and women > 70 years with definite angina (ii) haemodynamic or ECG changes with pain (iii) marked symmetrical T wave inversion in precordial leads (iv) ST seg-ment elevation or depression of > 1mm (v) variant angina Those with intermediate risk include (i) Men< 60 years and women < 70 years with definite angina; or Men > 60 years and women > 70 years with probable angina; (ii) Diabetes with two other risk factors (smoking, hypertension, elevated cholesterol); (iii) probable non-anginal pain in diabetes, (iv) extracardiac vascular diseases, (v) ST depression
04MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY21..
16 MIMS HEART JOURNAL - 2004 JULY
About 5% of patients have “Culture Negative Endocarditis”, which usu-ally is due to inadvertent use of antibiotics prior to obtaining blood cul-ture samples (about 60%) or infection by pathogen difficult to isolate from blood culture. eg:- HACEK group, Bartonella species, a nutritionally variant streptococcus now classified as Abiotrophia species, Brucella spe-cies, Legionella species, Coxiella brunetti, Torpherema whipelli or fungi like Aspergillus which are never recovered from blood. These organisms need special methods and efforts from the microbiologist, to be traced and tackled appropriately.Echocardiography has an important role in diagnosing and assessing the severity of the disease and its complications, if any. Vegetation, abscess, new prosthetic valve dehiscence or new regurgitation are the four power-ful identifiers of infective endocarditis in the presence of other clinical parameters. Pathological consequences of infective endocarditis such as ventricular dysfunction,, ruptured chordae, shunts or fistulae may also be identified on echo. Echo may be useful in diagnosis of culture negative infective endocarditis or in the diagnosis of persistent bacteremia from an unidentified source. Trans Esophageal Echocardiography (TEE) has a much higher sensitivity and specificity than Transthoracic echocardiog-raphy (TTE) in diagnosing infective endocarditis. Moreover Transthoracic echocardiography alone cannot exclude prosthetic valve infection, peri-annular abscesses, fistula or leaflet perforation. All these are picked up better in Trans esophageal echocardiography. When both TTE and TEE are negative, the negative prediction value is about 95%. A repeat TEE in 7 to 10 days is needed in these patients labelled negative by Echo but with a high clinical suspicion of Infective Endocarditis. Follow-up Echo over the course and on completion of medical management is needed to assess the efficacy of therapy instituted.
MEDICAL MANAGEMENT OF INFECTIVE ENDOCARDITISThis is based on the invading organism. 80% of Infective Endocarditis are due to Streptococci and Staphylococci. Majority of native valve bacte-rial endocarditis is caused by Streptococci viridans (50%) and Staphy-lococcus aureus (20%). 80% of Tricuspid valve infection is caused by Staphylococcus aureus – as this is more common in IV drug abusers. Staphylococcus aureus is a frequent cause of infective endocarditis in diabetes mellitus too. Early prosthetic valve endocarditis, defined as en-docarditis during the first two months after surgery is frequently caused by Staphylococcus epidermidis. Late onset prosthetic valve infective en-docarditis usually is caused by Streptococcus viridans and Staphylococci. Enterococcal endocarditis associated with malignancy or manipulation of gastrointestinal or genitourinary tract is usually caused by Enterococcus faecium (90%). The HACEK groups are an important group, which causes large vegetation (>1 cm), large vessel emboli and Congestive Cardiac Failure (CCF). Fungi are another group, which produces large vegeta-tions. Candida is a common cause for Infective Endocarditis in IV drug
abusers and immunocompromised patients.
MEDICAL MANAGEMENT OF UNUSUALLY ENCOUNTERED MICROORGANISMSCOAGULASE NEGATIVE STAPHYLOCOCCI: Increasing number of coagulase neg-ative Staphylococci infective endocarditis is being reported. An important subset of these patients, with infection of Staphylococcus lugdunensis is being identified. This is more virulent than other forms of coagulase negative Staphylococci, has high risk of paravalvular spread and meta-static distant organ seeding. This is susceptible to most antibiotics.
COXIELLA BRUNETTI : The causative organism for Q fever usually affects prosthetic or previously damaged aortic or mitral valves. Infection is sub endothelial and vegetation is small and hence often missed. Doxycycline with Trimethoprim / Sulphamethoxazole, Rifampicin or Fluoroquinolones is the mainstay of therapy. The organism may remain dormant in tis-sues for a long time and hence drugs may be needed life long or for a minimum of three years.
BRUCELLA : This gram-negative bacillus which causes brucellosis can produce bulky vegetation on the previously damaged aortic and mitral valves followed commonly by valve destruction, perivalvar abscess and congestive heart failure. Doxycycline plus Streptomycin or Gentamicin or Trimethoprim /Sulphamethoxazole or Rifampicin is the drug of choice. Valve replacement is needed in most cases. Drugs should be continued for 2 to 10 months after valve replacement
CANDIDA AND ASPERGILLUS : Cause majority of fungal Infective Endocardi-tis. Those with history of IV drug abuse, prosthetic valves replacements and long term central venous catheters are at high risk. Blood cultures are usually negative and vegetations bulky. Metastatic foci, perivalvar invasion and embolisation are common.Valve surgery is a must as Am-photericin B, the only fungicidal agent available and has poor penetra-tion into vegetation. Suppressive therapy with Imidazoles (Fluconazole) may be effective.
LEGIONELLA : Patients usually present with a long febrile illness, newly developed murmur and extremely high antibody titers. Most patients are prosthetic valve recipients. Embolism is rare. Parenteral Doxycycline or Erythromycin followed by prolonged oral therapy is effective. Valve re-placement is needed only if there is valvar incompetence.
PSEUDOMONAS AERUGINOSA causes Infective Endocarditis especially in IV drug abusers. Isolated right-sided Pseudomonas infective endocarditis can be medically managed with Piperacillin combined with an Aminoglycoside. Valve replacement is mandatory for left sided infective endocarditis.
The choice of the device for valve replacement depends on a variety of factors like risk of re-infection, ease of insertion, durability, need for an-ticoagulation, adequacy of removal of infected tissue etc. A homograft is preferred to a mechanical device considering the reduced risk for re-infec-tion and need for anticoagulation. Valve repair rather than replacement may be considered in some cases of healed mitral valve endocarditis with small vegetations and in intravenous drug abusers with tricuspid valve endocarditis.
MANAGEMENT OF COMPLICATIONS OF INFECTIVE ENDOCARDITISSepsis, congestive cardiac failure, embolism, periannular spread, mycotic aneurysm and spread of infection to other organs are the common com-plications of infective endocarditis. Certain factors likeprosthetic cardiac valves, left-sided endocarditis, Staphylococcus aureus IE,fungal IE, previ-ous IE, prolonged clinical symptoms (≥3 months), cyanotic congenital heart disease, patients with systemic to pulmonary shunts and those with poor clinical response to antimicrobial therapy are recognized to carry a high risk for developing complications in a patient with infective endo-carditis
CONGESTIVECARDIACFAILURE(CCF): Congestive cardiac failure has the great-est impact on the prognosis of patients with infective endocarditis. Left sided endocarditis is more likely to develop CCF than right sided infective endocarditis. Aortic valve infective endocarditis is more likely to develop CCF (29%) than mitral valve (20%) or tricuspid valve (8%) infective endocarditis.Usually CCF develops insidiously with progressive worsening of valvular incompetence and ventricular dysfunction. CCF may also develop acutely as in acute rupture of chordae in mitral valve infective endocarditis, valve obstruction due to huge vegetation, prosthetic valve dehiscence, fistulae formation, valve leaflet perforation etc.CCF in infective endocarditis signifies a grave prognosis and is a predictor of poor outcome even after surgery.It is mandatory to operate on such patients at the earliest. Delay of sur-gery to extend preoperative antibiotic treatment carries with it the risk of permanent dysfunction. Class III or IV CCF has a very high risk for poor surgical outcome.
SYSTEMICEMBOLIZATION: occur in 22 to 50% of cases of infective endocar-ditis. About 60 to 65% of embolic events occur in the CNS; with more than 95% of these in the Middle Cerebral Artery territory. Arterial beds in the lungs, coronaries, spleen, bowel and extremities are also very much prone. Left sided valveinfective endocarditis is more prone to give rise to emboli. Infective endocarditis due to Staphylococccus aureus, Candida, Abiotrophia species and HACEK organisms are important causative fac-tors. Most emboli are noted with two full weeks of treatment and the risk weans off gradually. Left sided vegetation especially of the mitral valve
and more than 1cm in size are at increased risk. Mitral valve vegeta-tions, irrespective of the size are associated with higher rates of embolism (25%) than aortic valve vegetation (10%). Anterior leaflet vegetation of mitral valve is more prone for embolisation, as the leaflet excursion occurs twice per heartbeat. Size and number of vegetations, number of valves involved and characteristics and mobility of vegetation are other less significant risk factors.Surgery to prevent further embolization is indicated if there has been two or more major embolic events. The advantage of prevention of further emboli exists only when surgery is done early in the course of Infective Endocarditis, when embolic rates are highest. Surgery should be consid-ered when large vegetation is detected on the mitral valve, particularly the anterior mitral leaflet. If inspite of adequate therapy, vegetation is found not to diminish in size or if it is still unstable on trans-esophageal echocar-diography, the risk of embolization is high and surgery may be indicated.
PERIANNULARSPREADOF INFECTIVE ENDOCARDITIS
Annular infection can break through and spread into nearby tissues, lead-ing to periannular ascess, pseudo aneurysm, sinuses or fistulae. Perian-nular spread predicts high mortality, and early need for cardiac surgery. Periannular spread complicates 10 to 40% of Infective Endocarditis. Aortic valve infective endocarditis is more prone to periannular spread than mitral or tricuspid valve infection. In prosthetic valve infective endo-carditis, periannular spread occurrence is very high (50 to 100%) as the primary infection is in the annulus and not the leaflets.Persistent bacteremia or fever, recurrent emboli, heart block, CCF or changes in characteristics of a murmur in a patient who is being inad-equately treated for infective endocarditis suggests possibility of perian-nular spread. TEE is the investigation of choice to look for and assess periannular spread.Surgery at the earliest is mandatory and includes drainage of abscess cavities, excision of necrotic tissue and closure of communicating tracts; apart from replacement of the infected valves. Grossly damaged perian-nular supporting tissues need major reconstruction using homograft.
Off-Pump coronary artery bypass grafting avoids extra corporeal circula-tion and has shown to reduce the clinically relevant morbidity, especially with regard to neurologic complications. Manipulating the ascending aorta by side-clamping is a definite risk factor and VAO helps us to get rid of this.Surgeon’s skill is an important factor in performing proximal anastamoses with VAO. One advantage here is that we can perform either the proximal or the distal anastamosis first, an option that is not possible with the recently described sutureless anastomotic device [Calafiore 2001]. VAO device is made of steel, is reusable, and costs only US$ 10 to fab-ricate it. Side-clamping of the aorta can be avoided, and hence there is no need to bring down the systolic pressure below 100 mm Hg. There is no injury to the vein initima, because nothing is introduced into the vein. The suturing procedure takes not more than 10 minutes, and the learning curve is very short or negligible. VAO can also be used in calcified aortas if a small island of normal tissue is available. Our clinical results are excellent; we are now waiting of the one-year postoperative angiographic studies of our patients in this series, to confirm their long-term patency.
REFERENCES1. Calafiore AM, Barel Y, Vitolla G, 2001. Early clinical experience with a new sutureless anastomotic device for proximal anastamosis of the saphenous vein to the aorta. J Thorac Cardiovasc Surg 121:854-8. 2. Mohan R, Amsel BJ, Walter PJ.1992. Coronary artery bypass in the elderly: a review of studies on patients older than 64, 69 or 74 years. Cardiology 80:215-25. 3. Moshkovitz Y, Luski A, Mohr R.1995. Coronary artery bypass without cardiopulmonary bypass: analysis of short-term and mid-term outcome in 220 patients. J Thorac Cardiovasc Surg 110: 979-87.
The sutures in the vein have to be inside out, and in the aorta, they have to be outside in. The aortic sutures are placed so that the needle passes through the aortic wall, goes into the groove of the Obturator, and comes out between the aorta and the metal, thus taking the intima. The sutures are placed all around the aortic punch hole and are loosely held. Once the suturing is complete, the obturator is removed, and the left index finger is positioned on the aortic punch hole to prevent bleeding. The loose sutures are pulled and tightened with a nerve hook. The assistant holds the two ends of the sutures firmly with controlled traction during this procedure. Once all of the sutures are in place, the two ends are tied snugly. The two snares on the purse string are removed, and they are tied in place with care, so as to avoid a purse string effect.
RESULTSWe have performed 269 proximal anastomoses on 177 patients. Initially, most were performed with proximal anastamosis first so that the flow in the vein grafts could be fully assessed. But with experience, we now do distal anastamosis first. We have had no postoperative ischemia, or peri-operative infarction in any of our patients. We have had no perioperative mortality in our coronary patients. One patient presented with angina after 12 weeks, and check angiogram results showed a perfectly patent graft. We are planning to follow up these patients and to repeat coronary angiography after one year to assess the patencies of their grafts.
DISCUSSIONWith the present-day degree of myocardial protection and refinement in surgical technique, the mortality and morbidity of coronary artery surgery is related more to the co morbidities of patients than to cardiac function and the complexity of the surgical procedure [Mohan 1992].Avoiding cardiopulmonary bypass [Moshkovitz 1995] has further con-tributed to the reduction of mortality and morbidity in high-risk patients, such as those with post infarction angina and a low ejection fraction.
mimslouranlfinal.indd 37/21/2004 11:05:55 PM
of 0.5 to 1 mm; (vi) T inversion of > 1mm in leads with dominant R waves. Patients with chest pain probably non cardiac, one risk factor (not Diabe-tes Mellitus), flat T wave or < 1 mm inversion in leads with dominant R waves or normal ECG are considered to be carrying a low risk. Percutaneous intervention has proven to prevent irreversible myocardial damage. Cardiac catheterization, Angioplasty and CABG in ACS has in-creased considerably in the past two decades. In ACS, PTCA against the culprit lesion and antiplatelet therapy can be performed with an initial success rate of > 95%, although the incidence of procedure related complication is high, world wide. CABG is considered for patients with coronary lesion that are not suitable for or do not respond to catheter based reperfusion. The reported inci-dence of perioperative death is 4 % and MI is 10 % higher when CABG is performed urgently than semi urgently in ACS. Therefore, efforts should be made to stabilize the patients pharmacologically before emergency revascularization procedures are contemplated. Use of IABP aids as a bridge to Angioplasty or CABG in ACS patients. The need for revascularization is based on diagnosing the culprit lesion early. Various institutions adopt various protocols for coronary angiogra-phy (CAG)in ACS. Two strategies are generally followed- the early inva-sive strategy and the conservative strategy. The early invasive strategy incorporates coronary angiography for all sta-bilized patients within 48 hours of presentation. The conservative strat-egy prescribes angiography for high-risk patients (ie CHF, LVEF<50%, malignant arrhythmia, recurrent ischaemia, prior revascularization etc). Both early invasive and conservative strategies have been found to pro-duce similar clinical outcomes by the TIMI 2B and VANQUISH study Decision about further proceedings is made based on the disease pattern revealed by CAG. Emergency surgical revascularization may be also need-ed in the setting of a failed thrombolysis or PTCA with acute occlusion The morbidity of patients operated on after acute MI remains relatively high when compared to stabilized patients. This is mainly because, the adverse effect of CPB is poorly tolerated by a heart with an evolving MI. It is reasonable to think that keeping off the pump may be advantageous in this subgroup of patients. The optimal timing of surgery for ACS remains indecisive. Various studies have shown that the mortality rate of patients who underwent surgical revascularization within 48 hours of an acute MI was significantly higher compared to after 48 hours. A recent multi-center analysis has shown clearly that the perioperative mortality in acute MI patients declined considerably with the increasing time interval. The first 6 hours is said to be the most dangerous period with mortality of about 10%. The mortality depends not only on the tim-ing of surgical revascularization but also on the LV function, presence of haemodynamic stability and presence of collateral circulation.
- 2004 09MIMS HEART JOURNAL JULY ..
Cardiopulmonary bypass (CPB) is a significant factor affecting the out-come in patients undergoing early CABG after ACS. Various studies have proven that the mortality rate is nearly 5 times higher in emergency CABG done on a stopped heart than on a beating heart. This deleterious effect of CPB is most evident in patients operated within 48 hours of an acute cardiac event.
OUR EXPERIENCE 306 CABGs were performed in our department during the period from July 2002 to October 2003. Out of these 46 were ACS patients who un-derwent emergency coronary angiography and were taken up for emer-gency surgical revascularisation. 6 of these patients had STEMI, 12 had NSTEMI, and the rest had unstable angina. 2 patients were referred to us for CABG after failed PTCA elsewhere. They were taken up on the second and third day post acute MI respectively. The patient age varied from 38 years to 76 years. 38 were males and 8 were females. All patients were diagnosed based on their ECG, Cardiac enzyme levels and trans-thoracic echocardiography. 2 patients had severe LV dysfunc-tion, 6 had moderate LV dysfunction and the rest had adequate LV func-tion. Every effort was made to stabilize the patients medically, so as to give at least a week’s time for the myocardium to recover from the acute insult. 14 patients needed emergency CABG before a week of the acute event. CABG in all the 46 patients, irrespective of the LV function and the time from the acute event were performed on beating heart. 6 patients needed minimal pump support due to haemodynamic compromise while positioning the heart for OPCAB. We had no perioperative MI or operative mortality. Postoperative ventilation, ICU stay, bleeding, enzyme levels, inotropic support and hospital stay were comparable to elective surgeries. All patients have been followed up till date and are maintaining good health.
CONCLUSION Acute coronary syndrome is no longer a contraindication for surgical re-vascularisation. Off pump coronary artery bypass has contributed much to the results of CABG in the acute setting by taking the pump-associated complications away. Antiplatelet drugs, which cannot be weaned off in patients in an acute setting, do not contribute to perioperative blood loss in OPCAB patients, questioning the actual need for stopping antiplatelet drugs even before elective OPCAB. The results of surgical revasculariza-tion are rewarding if surgery can be prolonged at least for 3 days after an acute cardiac event.

22MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY03..
INTRODUCTIONWith the advent of beating heart surgery, more than 50% of coronary artery bypass graft surgeries are performed in most coronary centers in India without the use of heart-lung machine. But the neurologic prob-lems caused by side clamping the aorta in performing the proximal anas-tomoses still remain. Hence, there has been a great deal of research to find an effective alternative to avoid side clamping the aorta. A couple of anastamotic devices have already arrived in the market, but since the costs of these devices are prohibitive, we designed our own device for proximal anastomoses.
PATIENTS AND METHODSFrom July 2002 to July 2003, we performed 235 coronary artery bypass graft surgeries on the beating heart with 177 of these procedures performed off-pump and 58 of them carried out with pump assistance. Initially, proximal anastomoses of vein grafts were performed with aortic side clamp. Of late, all our top ends are being performed with VAO. 177 patients have had their proximal Saphenous Vein Graft (SVG) anastomo-ses performed with our VAO.Before VAO was used on patients, it was tried for anastomosing vein grafts on the aortas and pulmonary arteries of various perfused animal heart models. The aortic and pulmonary artery pressures were maintained at 110 to 120 mm Hg systolic while these anastomoses were being per-formed. These conduits were then explanted and examined for suture placement to see if all the aortic layers were included.
VETTATH’S ANASTAMOTIC OBTURATOR (VAO)This metallic instrument is made of solid steel (Figure 1). It is 18 cm long and comes in small and medium sizes (5 mm and 6 mm in diameter respectively). The holding part is smooth. The inserting bit has a ridge 2.5 cm from the end (Figure 2). This 2mm ridge projects perpendicularly from the steel rod. There are 3 equidistant grooves in the inserting end that are 1 mm deep a 1.5 cm long. The ridge helps to prevent blood from spurting directly into the eye. The grooves allow the needle to pass through the rod and thereby include the aortic intima in the suture.
SURGICAL TECHNIQUEVAO allows us to anastamose the proximal ends of the vein grafts, before or after the distal anastomoses. The aortic site proposed for anastomosis marked with diathermy. Two 3-0 polypropylene purse-string sutures are applied 1 cm away from the site. The aorta is stabbed with a No.11 blade knife, and punched with 4mm or 4.5mm aortic punch (for 5-mm or 6-mm VAO), respectively. The punch hole is blocked with the left index finger. VAO is introduced and purse strings are tightened just enough to prevent excessive bleeding. Once the obturator is in and the snares are tightened, the proximal vein anastomoses is performed as usual with 5.0 or 6.0 polypropylene suture.
VETTATH’S ANASTAMOTIC OBTURATOR OUR EXPERIENCE OF 269 PROXIMAL ANASTOMOSES
Dr. Murali P. VettathChief Cardiac Surgeon
MIMS HEART JOURNAL - 2004 JULY 15..
MYCOTICANEURYSMSresult from septic embolization of vegetation to vasa vasorum or intraluminal infective embolus with subsequent spread through the intima and outwards through the vessel wall. They occur mostly at arterial branching points as emboli are usually impacted at such points. Intracranial mycotic aneurysms are more common than ex-tracranial ones; which usually affect the visceral arteries and arteries to upper and lower limbs.The overall mortality rate in infective endocarditis patients with intra-cranial mycotic aneurysm is about 60%. Streptococci account for about 50% and Staphylococcus 10% of intracranial mycotic aneurysms. The distal MCA branches are more commonly affected. Intracranial mycotic aneurysms are multiple in about 20% of patients. Clinical presentation is highly variable.Routine screening is not required except when clinical findings are sug-gestive of an intracranial pathology. Contrast enhanced CT or Magnetic Resonance Angiography are useful in detecting these lesions but con-ventional four-vessel angiography still remains the diagnostic test of choice.Intracranial mycotic aneurysms (ICMA) may heal with medical therapy. Proximal aneurysms should be monitored with serial angiograms and CT as ligation of these may lead to severe neurological deficit. ICMA distal to major branching points may be ligated or excised. Some patients need both valve replacements and ICMA ligation. Bioprosthetic valve is prefer-able in such patients as anticoagulation can be avoided.
Extra-cranial mycotic aneurysms (ECMA) may present as tender pulsatile masses. Intra-thoracic or intra-abdominal ECMAs are asymptomatic until leakage or rupture occurs. Proximal and distal ligation of aneurysms and restoration of blood flow with autologous vein grafts through extra-ana-tomic site is the only hope for a radical cure.
SPLENICABSCESSin infective endocarditis may be caused either by an in-fected embolus or by bacterial seeding of a splenic infarct. Streptococcus viridans and Staphylococcus aureus accounts for around 40% of cases, enterococci 15%, gram-negative bacilli and fungi in <5%. Spleno-megaly is present only in about 30% and is not a reliable sign. Back, left flank, left upper quadrant pain or abdominal tenderness may be present. Persistent fever, bacteremia and sepsis may be suggestive of splenic abscess. Splenic rupture with hemorrhage is a rare complication. CT / MRI are the best diagnostic tests. Definitive treatment is splenectomy with appropriate antibiotics. Splenectomy should be performed before valve replacement, as the risk of prosthetic valve infection is very high with a splenic abscess.
PROPHYLAXIS AGAINST INFECTIVE ENDOCARDITISAntibiotic prophylaxis against infective endocarditis is recommended in a group of conditions, which carry with it a very high risk of playing a host to this dreaded disease. Patients with prosthetic heart valves, complex cyanotic congenital heart disease and previous history of infective endo-carditis carry a very high risk. Those with acquired lesions like rheumatic valve disease, hypertrophic cardiomyopathy (HCM), mitral valve prolapse with regurgitation, etc carry a moderate risk with them. Such patients need antibiotic prophylaxis while undergoing any invasive procedures like dental extraction or manipulation of the respiratory, genitourinary or gastrointestinal tracts.The standard general prophylaxis for patients at risk is Amoxicillin 2gm (50mg/kg in children) given orally one hour before the procedure. Those who are unable to take oral medications are given injection Ampicillin. Those allergic to penicillins are given either Clindamycin or Cephalexin or Cefadroxil or Azithromycin or Clarithromycin. An Aminoglycoside should be added to the above patients if they are undergoing procedures on the genitourinary or gastrointestinal tracts. Vancomycin with Gentamicin is preferred in patients who are allergic to penicillin.
2. Evidence of endocardial involvementA. Positive echocardiogram for IE defined as(i)Oscillating intracardiac mass on valve or supporting struc
tures, in the path of regurgitant jets, or on implanted material in the absence of an alternative anatomic explana tion, or(ii) Abscess, or(iii) New partial dehiscence of prosthetic valve
orB. New valvular regurgitation (worsening or changing of pre existing murmur not sufficient)
MINOR CRITERIA
1. Predisposition: predisposing heart condition or intravenous drug abuse2. Fever: temperature ≥38.0°C3. Vascular phenomena: major arterial emboli, septic pulmo nary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway lesions4. Immunologic phenomena: glomerulonephritis, Osler’s nodes, Roth spots, and rheumatoid factor5. Microbiological evidence: positive blood culture but does not meet a major criterion as noted above or serological evidence of active infection with organism consistent with IE6. Echocardiographic findings: consistent with IE but do not meet a major criterion as noted above.
Diagnosis of Definite Infective Endocarditis by Duke Criteria needs the presence of two major criteria or 1 major and 3 minor criteria or 5 minor criteria or pathological proof if IE. Those patients who do not meet the criteria for “Definite”Infective Endocarditis are labeled as “Probable” In-fective Endocarditis. Those patients whose symptoms reduce either with no treatment or within a short-term after diagnosis and those patients with no pathological evidence of infective endocarditis are labeled as rejected cases.The Duke Criteria is by far more specific and sensitive than the Beth Is-rael Criteria. Clinical suspicion of Infective Endocarditis may be raised by fever, other systemic symptoms along with physical findings like Osler’s nodes, petechiae, Janeway lesions, Roth spots, splenomegaly, newly di-agnosed clubbing and a new changing cardiac murmur. High index of suspicion in susceptible patients helps in diagnosing much before these findings set in. The offending organism can be demonstrated in 3 sets of blood cultures. (Each set with 1 aerobic and 1 anaerobic culture sample) obtained at intervals of more than one hour, within the first 24 hours is mandatory. 5 to 6 samples may be needed in some patients.
The diagnosis of infective endocarditis is straight forward in patients with the classical Oslerian manifestations of bacteremia or fungaemia, active valvulitis, peripheral emboli and immunologic vascular phenomena. In others, these classical findings may be few or absent as in Infective En-docarditis caused by Staphylococcus aureus infection of right sided heart valves or in patients where infective endocarditis is caused by the HACEK (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella) group of organisms. Immunologic vascular phenomenon is characteristic of subacute bacterial endocarditis. They are rarely seen in acute infective endocarditis on presentation, as the disease process is so rapid. Right-sided infective endocarditis does not produce peripheral embolism and immunological vascular phenomenon.This variability in clinical presentation of Infective Endocarditis warrants an optimal diagnostic strategy for early diagnosis. The Beth Israel criteria was proposed in 1981 by Van Reyn which was so stringent that only those patients confirmed pathologically were considered Definite Infec-tive Endocarditis patients and those with bacteremia, new valvular regur-gitation and vascular phenomenon were considered as Probable Infective Endocarditis patients. Durack et al from Duke University proposed the Modified Duke’s Criteria in 1994 incorporating Echocardiographic findings into the important di-agnostic parameters in Beth Israel Criteria. Moreover, intravenous drug abuse was recognized as an important cause for infective endocarditis in Duke’s criteria.The Duke’s clinical criteria stratified the various parameters into two broad groups – Major and Minor criteria as shown below.
MODIFIED DUKE’S CRITERIA FOR CLINICAL DIAGNOSIS OF INFECTIVE ENDOCARDITIS
MAJOR CRITERIA
1. Positive blood culture for IE A. Typical microorganism consistent with IE from 2 separate blood cultures as:(i) Viridans Streptococci, Streptococcus bovis, or HACEK group, or(ii) Community-acquired Staphylococcus aureus or entero cocci, in the absence of a primary focus
orB. Microorganisms consistent with IE from persistently positiveblood cultures defined as(i) ≥2 positive cultures of blood samples drawn >12 hours apart or(ii) All of 3 or a majority of ≥4 separate cultures of blood (with first and last sample drawn ≥1 hour apart)
mimslouranlfinal.indd 27/21/2004 11:03:23 PM
10 - 2004MIMS HEART JOURNAL JULY
CARDIAC RESYNCHRONIZATION THERAPY A case report with review of literature
CASE REPORT: Mr. R, a 36-year-old gentleman was diagnosed to have Hypertrophic Non-Obstructive Cardiomyopathy with LV systolic dysfunction. He pre-sented to us with worsening of dyspnea, orthopnea, and paroxysmal nocturnal dyspnoea . He had been symptomatic since the last 4 years and in NYHA functional class IV since 2 months. He had two episodes of syncope associated with palpitation during the previous 2 months. He was tachypnoeic on admission, heart rate was 56 beats /min, and blood pressure was 100/80 mmHg. Mean jugular venous pressure was not raised but ‘a’ wave was prominent. Apex beat was in the sixth intercostal space 1 cm outside the midclavicular line. First heart sound was soft, S2 was normally split, and LV S3 and S4 were prominent. Fine basal crepitations were present bilaterally. ECG showed sinus rhythm at 50 bpm, first degree AV block, and LBBB with a QRS duration of 240 m.sec. Chest X-ray showed grade III PVH, cardiomegaly, and mild pulmonary edema. All the routine hematological and biochemical parameters were normal. 2-D Echo Color Doppler examination showed asymmetrical sep-tal hypertrophy with global LV hypokinesis and LV ejection fraction of 35 % by Simpson’s method. There was moderate mitral regurgitation with MR jet area of 7 cm2. This gentleman had cardiac evaluation at another cardiac center in 10 months back. 24-hour Holter at that time showed one episode of non-sustained ventricular tachycardia and frequent multiform VPCs with cou-plets and bigeminy. Monomorphic sustained VT was inducible on electro-physiological testing. Angiography revealed normal coronary arteries. Patient was stabilized with I.V diuretics, Digoxin, ACE inhibitors, and supportive measures. The most appropriate therapeutic option was to provide an Implantable Cardioverter Device with biventricular pacing. However, since the patient could not afford the cost of an Implantable Cardioverter Device, the second best option of biventricular pacing with anti-arrhythmic drugs was discussed with the patient and relatives, to which they agreed. Patient was taken up for transvenous implantation of atrial synchronized biventricular pacing through a left infra-clavicular incision. Subclavian
Dr. Dinesh Babu .K.V Cardiologist
puncture was done and coronary sinus was cannulated using the pre-formed sheath. A 6French balloon catheter was introduced through the coronary sinus sheath for venography. Attempts to negotiate the guide-wire in to the left cardiac vein were not successful. RA and RV apical leads were placed to which the pulse generator was connected and the wound closed. Subsequently, patient was taken for LV epicardial lead placement through left anterolateral thoracotomy. The proximal end of this lead was tun-neled to the infra-clavicular pocket and connected to the pulse generator. Pacemaker was programmed to biventricular pacing with an AV delay of 140 m.sec. Post-pacing ECG showed shortening of QRS duration to 130 m.sec, which is a significant indicator of response to therapy. Repeat Echocardiagraphic study revealed improvement in LV ejection fraction and reduction of MR jet area from 7 to 4 cm2.
REVIEW OF LITERATURE: INTRODUCTION: The pharmacotherapy of congestive heart failure is primarily based on antagonism of neurohormonal pathways namely, the sympathetic ner-vous system and the “renin-angiotensin-aldosterone axis”. Most of the drugs have been shown to reduce mortality and morbidity and in some cases they improve the underlying structural abnormalities of the heart by a process called reverse remodelling. Despite these therapeutic ad-vances,

02MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY23..
14 MIMS HEART JOURNAL - 2004 JULY
DEPARTMENTPROFILE
DEPARTMENTOFCARDIOVASCULAR&THORACICSURGERY
Dr.Murali.PVettath,MBBS,DNB,MChDr.SheenPeeceeyenC.S,MBBS,MS,MChDr.BaburajanA.K,MBBS,DNB,MCh
DEPARTMENTOFCARDIACANAESTHESILOGY
Dr.A.VKannan,MBBS,MD,FCACCDr.SatheeshKumar.N,MBBS,MD
DEPARTMENTOFCARDIOLOGY
Dr.AliFaizal,MBBS,MD,DMDr.AsishKumar.M,MBBS,MD,DMDr.DineshBabuK.V,MBBS,MD,DMDr.MuraliKrishna,MBBS,MD,DM
CONTENTS
VETTATH’SANASTAMOTICOBTURATORAnewproximalanastamoticdevice
INTENSIVECAREMANAGEMENTAFTERCARDIACSURGERYWherewestandtoday
TRANS-CATHETERCLOSUREOFPATENTDUCTUSARTERIOSUSAdieutosurgery
OPCABFORACUTECORONARYSYNDROMEThewaytogo
CARDIACRESYNCHRONIZATIONTHERAPYAcasereportwithreviewofliterature:
PUMPLUNGSYNDROMEAcasereport
INFECTIVEENDOCARDITIS-DIAGNOSISANDMANAGEMENTINADULTSAnoverview
03
05
07
0810
12
14ForPrivateCirculationonly
NoPartofthispublicationmaybereproducedbyanymeans,includingelectronicmedia
Graphics-Design-bynnaturalwondders-calicut
Infective Endocarditis, an infection of the inner walls of the cardiac cham-bers, valves, aortic root and prosthetic material is not an uncommon problem in our region. Advances in diagnosis and pharmacotherapy have changed the whole scenario since William Osler (1885) projected bacte-rial infection as the root cause, valvular heart disease as a predisposing factor and valvular incompetence and embolism as lethal complications of what he called Malignant Endocarditis. But even today, Infective En-docarditis carries a very high risk of morbidity and mortality. For bacterial endocarditis to occur there should be bacteremia, damaged endothelium vulnerable to infection, turbulence along haemodynamic path, and a virulent microorganism, which can overcome the natural defenses of the host or a host with a severely compromised immune system. Thus patients with acquired cardiac lesions like Rheumatic heart disease, degenerative valve disease or congenital lesions like Ventricular
Septal Defect, Tetralogy of Fallot, Congenital Aortic stenosis, complex cyanotic anomalies, Patent Ductus Arteriosus, Systemic to pulmonary arterial shunts etc. are prone for infective endocarditis. Recently intra-venous drug abuse is gaining more importance as a common cause for Infective endocarditis
The term infective endocarditis includes acute, subacute and chronic pro-cess of bacterial, viral, fungal or rickettsial aetiology. Acute endocarditis is a life threatening infection usually of normal heart valves, during the course of septicemia by virulent pyogenic microorganism such as hae-molytic Streptococci or Staphylococci. In subacute endocarditis, already damaged valves or other cardiac structures are secondarily infected.Acute native valve endocarditis accounts for 25% of Infective Endo-carditis. Severe sepsis, long term indwelling catheter, IV drug abuse and fungemia are predisposing factors. The usual affecting organism is Staphylococcus aureus. Other common organisms are Streptococcus viridans and Enterococci. The initial stage of valvular infection is surface vegetation – composed of platelets, fibrin and the causative microorganism. Organisms multiply within the vegetation and are thereby protected from the host defenses and antibiotics. They can be a source for repetitive bacteremia. Veg-etations are initially soft and friable and may embolise. They may also produce immune complex mediated and allergic vasculopathies. Large vegetation may become organized and calcified. Endocarditis is considered active surgically when surgery is performed in the presence of obvious local cardiac infection (active vegetation/ab-scess/sinus/fistulae) or when surgery is done while the patient is still on or within two weeks of termination of medical management for Infective Endocarditis. Endocarditis is considered healed when there is no active cardiac infection or inflammation, vegetation if present is endothelialised and abscess and sinus or fistulae if present are well organized.Surgical management of infective endocarditis was first reported by Kay et al (1961) in a patient with Tricuspid valve endocarditis and it was Wallace (1965) who first reported valve replacement as treatment for infective endocarditis.Early Diagnosis, effective management and prompt recognition of com-plication are essential to good patient outcome. For that general idea of the clinical presentation and diagnostic modalities are of great im-portance.
INFECTIVE ENDOCARDITIS - DIAGNOSIS AND MANAGEMENT IN ADULTSAN OVERVIEW
Dr. Sheen Peeceeyen. C.S Cardiac Surgeon
mimslouranlfinal.indd 57/21/2004 11:09:49 PM
- 2004 11
tricular pacing have been developed.
den death in patients with heart failure.
tricular pacing and a 40 % reduction in hospitalization for heart failure.
:
cardiography] 2003 April 20 (3) 217-23.
TECHNIQUES & COMPLICATIONS:
lar lead can occur in as high as 6 % of patients.
FUTURE PERSPECTIVES:
data are available.
REFERENCES:
Coll Cardiol. 2000 Sep; 36 (3): 828-31
diography. 2003 Apr; 20(3) 217-23
heart failure. The MIRACLE study MEJM.
MIMS HEART JOURNAL JULY ..
sizable proportion of patients with heart failure remain symptomatic and succumb to death, and hence additional treatment strategies like biven-
About 30 % of patients with chronic heart failure have intraventricular conduction delay such as left or right bundle branch block leading to loss of coordination of ventricular contraction. Such asynchrony is evident on the surface ECG as widening of QRS interval [> 120 m.sec]. This can impair the contractile reserve of the heart, and also enhance the severity of the functional mitral regurgitation. Intraventricular conduction delay has been associated with electrical instability and increased risk of sud-
BENEFICIAL EFFECTS OF BIVENTRICULAR PACING: Short-term results of clinical trials with devices for atrial synchronized biventricular pacing to coordinate left and right ventricular contrac-tions are encouraging. Notable improvements in primary end points of NYHA functional class, six minutes walking distance and quality of life were constantly seen with cardiac resynchronization therapy [CRT]. In the recently published MIRACLE trial, the resynchronization group had significant improvement in peak oxygen consumption and total exercise time. Further, the left ventricular ejection fraction increased and the end-diastolic dimension, the magnitude of mitral regurgitation and the dura-tion of QRS all decreased in the resynchronization group. Biventricular pacing was associated with fewer hospital admissions and fewer days in the hospital for heart failure. The combined risk of a major clinical event [death or hospitalization for heart failure] was 40 % lower in the resynchronization group. In the study of Breithardt et al [JACC 2003 May 21, 41 [10]: 1852] cardiac resynchronization was associated with a significant reduction in severity of mitral regurgitation. The effective regurgitant orifice area decreased from 25 ± 19 mm to 13 ± 8 mm. This was directly related to an increase in left ventricular pressure rise [LV + dp/dt max]. Favourable effect on heart rate variability by resynchro-nization was shown by Adamson et al [circulation 2003 July 22; 108 (3) 266-9]. In the Ventak CHF study [Higgins SL et al JACC 2000 Sept; 36 (3)] synchronized biventricular pacing reduced the frequency of ICD therapies in patients receiving both the devices. Preliminary trial results show significant survival benefit when an ICD is combined with biven-
ELIGIBLE PATIENT POPULATIONPatients with moderate-to-severe symptoms of heart failure [NYHA Class III or IV], left ventricular ejection fraction < 35 % and a wide QRS [> 130 m.sec] with left bundle branch block morphology are currently considered eligible for biventricular pacing. Heterogenous response to biventricular pacing has challenged the predictive accuracy of wide QRS complex in surface ECG for ventricular dyssynchrony. More sensitive tech-niques like Echocardiography with Tissue Doppler imaging to identify
regional delay in left ventricular contraction have been shown to better predict the responders from resynchronisation. [Makaryus AN et al Echo-
Prior to the procedure, a levophase of coronary angiogram is recorded to profile coronary sinus and cardiac veins. Device implantation is done in left infraclavicular pocket and venous access is obtained via subcla-vian vein puncture. Preformed sheaths in different curves are available to facilitate cannulation of the coronary sinus. With availability of over-the-wire leads, to enter the left cardiac vein, the technical success rate of CRT has improved. Placement of atrial and right ventricular leads are not different from the conventional pacemakers. The major complications associated with the procedure include dissection and perforation of the coronary sinus leading to hemopericardium, complete heart block, asys-tole, and arrhythmias. MIRACLE trial reported a technical failure rate of 8 % and major complications of 1-2 %, which include cardiac tamponade or cardiac arrest requiring resuscitation. Late dislodgment of left ventricu-
In considering devices for heart failure, the growing weight of evidence for biventricular pacing needs to be considered alongside the expand-ing indications for implantable cardioverter defibrillators. ICDs have been shown to significantly reduce the mortality and propensity for malignant ventricular arrhythmias in patients with left ventricular dysfunctions. Syn-chronized pacing can complement this effect by reducing the need for hospitalization for heart failure and the frequency of ICD therapies. Thus, patients with symptomatic heart failure due to ischemic cardiomyopathy and wide QRS complex, might be better served by a combined resynchro-nization pacer and defibrillator. However, the issue of cost effectiveness remains contentious and warrants further examination when long-term
1 Higgins SL, Yong P, Sheck D et al; biventricular pacing diminished the need for implantable cardioverter defibrillator therapy. Ventak CHF Investigators. J Am
2 Young JB, Abraham WT, Smith AL et al; combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: the MIRACLE ICD Trial. JAMA. 2003 May 28; 289 (20): 2719-21 3 Makaryus AN, Arduini AD, Mallin J et al; echocardiographic features of pa-tients with heart failure who may benefit from biventricular pacing. Echocar-
4 Abraham WT., Fisher WG., Smith AL et al, Cardiac resynchronization in chronic

MIMS HEART JOURNAL - 2004 JULY 13..
24MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY01..
ation in patients who remain hypoxic despite PEEP.3. High frequency ventilation4. Airway pressure release ventilation5. Prone position6. Extracorporeal membrane oxygenation (ECMO).7. Partial liquid ventilationDrug like cyclooxygenase inhibitors, corticosteroids, nitric oxide,prostacyclin and surfactant have been tried with no conclusive benefit in ARDS. The role of pharmacological management is only supportive, apart from antibiotics to prevent secondary infection. From our practi-cal experience we found that pressure control ventilation with PEEP and inverse ratio ventilation improves the outcome in ARDS without much morbidity. Interesting feature in this patient were that drowsiness probably due to cerebral edema or hypoxia which was evident and effective diuresis inducing a negative balance of more then 7 litres over a period of 6 days helped in the speedy recovery. This shows that early detection and man-agement by appropriate Ventilatory strategies along with diuresis helps in recovery with out much morbidity in ‘Pump lung syndrome’.
REFERENCES
1. Amato, M.B.P, et al. Effect of protective ventilation strategy on mortality in the ARDS. N.Engl.j.Med 338 (6): 347-354, 1998.
2. Artigas, A., et al. The American-European consensus conference on ARDS part 2. Ventilatory, pharmacologic, supportive therapy, study design strate gies and issues related to recovery and remodeling, Intens. Care Med. 24:378- 398, 1998.
3. Marini. J.J. and Evans, T.W. Round table conference: Acute lung injury, 15th-17th March 1997 Brussels, Belgium. Intens. Care Med. 24:878-883, 1998.
4. Sessler, C.N.Mechanical ventilation of patients with acute lung injury. Crit. Care. Clin 14 (4): 707-729. 1998.
5. Zimmerman, J.L. and Hanania, N.A. Vasodilators in mechanical ventilation. Crit. Care. Clin 14 (4): 611-627, 1998
6. MooreFA, MooreEE. Evolving concepts in pathogenesis of post injury multiple organ failure. Surg clin North America 1995; 75:257-77.
7. Royston.D. Surgery with cardiopulmonary bypass and pulmonary inflammatory responses. Perfusion 1996: 11: 213-9.
8. Christenson.J.T. Aeberhard.J.M. Badel.P. et al. Adult respiratory distress syndrome after cardiac surgery. Cardio Vasc Surg 1996; 4:15-21.
He remained haemodynamically stable, very alert and was ambulated in ICU without any respiratory distress. By the end of 6 days, his fluid balance was –7430 ml. When he was transferred out of ICU, his weight has reduced to 80 kgs from 88 kgs.
Fig 3 CxR –acute phase of ARDS Fig 4 CxR –recovery phase of ARDS
Serial-ABG REPORTSDay Preop 1st POD 5th POD 6th POD 7th POD 8th POD
PH 7.41 7.31 7.38 7.52 7.5 7.45
PO2 82 103.7 61.5 78.1 87.2 86.2
PCO2 40 52 36.1 34.8 36 39.4
BE -1.1 -0.6 -4.3 5.4 4.2 3.2
HCO3 28.5 23.5 31 29.3 28.3 27.3
FiO2 Room air NP4 l/min 0.8 0.7 0.5 0.5
O2 Sat. 94.6 97.2 94.3 96.7 97.3 97
Remarks Stable PCVent PCVent SIMV+PS
CONCLUSIONThere is considerable evidence that cardiopulmonary bypass is associated with deterioration of pulmonary function leading to acute lung injury (ALI) or ARDS. Mechanical ventilation plays an important role in reduc-ing the mortality rate of ARDS. Mortality is about 15 –30 % if only lung is involved and the rate increases upto 80% if 3 or more organs are involved. Ventillatory strategies used for ARDS (ARDS net).1. PEEP2. Low tidal volume 6-7 ml/kg to as low as 4 ml/kg to maintain plateau pressure <30-40cm H2O.3. Respiratory rate < 30/min4. FiO2 0.5 – 0.6
Different Ventillatory modes1. Pressure Control Ventilation- has advantage of higher mean airway pressure.2. Inverse ratio ventilation (IRV)- I: E ratio > 1 can improve oxygen
Coronary Artery Bypass Grafting or Bypass Surgery, as it is commonly known, has been a field, which has seen umpteen number of newer techniques and innovations and change of basic concepts creeping in and out. We were able to contribute to this surge of innovations in this field through our new invention – the “Vettath’s
Anastamotic Obturator” (VAO) – a simple proximal anastamotic device for anastamosing vein grafts onto the aorta without using side clamp. The first article in this issue is a note on this novel tool in our kitty.It is widely known that surgery starts were medicine fails. But today, newer developments in interventional technology have helped cardiologists pull back some of the surgeons’ domains into their repertoire. PDA and ASD are glorious examples of such lesions, which can and are being very effectively handled by Cardiologists today. We are having a feature on non-surgical PDA closure, which is very much in vogue now a days.We bring to you some of the important aspects in the critical care of post cardiac surgical patients and a note on a pump associated postoperative problem – the Pump Lung Syndrome. Pump related problems have been a matter of concern and hence keeping away from the pump is a sensible fashion of the day. Beating Heart Surgery or Off Pump Coronary Artery Bypass (OPCAB) is a routine procedure. We bring you our experience on early Off Pump CABG in Acute Coronary Syndrome patients, a procedure which was considered impossible not so long ago.Pharmacotherapy for congestive cardiac failure aims at reverse remodeling of the ventricles. But despite optimal medication a major portion of such patients get little benefit. Various treatment options for refractory cardiac failure have been described. Biventricular pacing which aims at correcting the intraventricular conduction delay and in coordinating both the ventricles is one among them. We intend to bring you some facts about this treatment modality through one of the cases managed in our center.We also bring you an elaborate review on Infective Endocarditis and its management in adults based on a wide range of published studies, guidelines and literature. We sincerely do hope that this effort of ours, to transfer some of our limited knowledge in this field onto our peers in Kerala through the second edition of the MIMS Heart Journal will bear some fruit. We stress our commitment in providing you with outstanding information about the recent advances in Cardiovascular Sciences and related fields, which are very much available in the Malabar region.
EDITORIAL
mimslouranlfinal.indd 4 7/21/2004 11:07:55 PM
12 - 2004
pump coronary artery bypass grafting .
CASE REPORT
Artery Bypass Grafting.
fentanyl/midazolam/atracurium infusion.
were
was
to drowsiness.
a drop in saturation (SpO284-
ponade was suspect
Chest was closed with drains in situ.
2
2 2 2 / FiO2 ratio
2 / FiO2 ventilator and extubated on the 4th day. All the infusions were stopped.
SYNDROME A case report
Fig 2 – Immediate post op CxR
Fig 1 - pre op CXR
MIMS HEART JOURNAL JULY
Cardiopulmonary bypass (CPB) is often followed by pulmonary dysfunc-tion and is also regarded as a risk factor for development of acute respi-ratory distress syndrome (ARDS). When pulmonary dysfunction cannot be directly attributed to a specific cause such as infection or ischemia, the concept of the “pump lung syndrome” or “systemic inflammatory re-sponse syndrome to CPB” is used as alternative explanation. Cardiopul-monary bypass is associated with a whole body inflammatory response, which involves activation of complement, leukocytes and endothelial cells , secretions of cytokines, proteases, arachidonic acid metabolites and oxygen free radicals. Leukocyte adhesion to microvascular endo-thelium, leukocyte extravasation and tissue damage are the final steps. Although the inflammatory response to cardiopulmonary bypass often remains at sub clinical levels, it can lead to major organ dysfunction and multiple organ failure. ARDS occurs in about 0.5 to 1.7% of patients undergoing open-heart surgery. We report a case of ARDS following on
A fifty-year-old male, weighing 88 kg, a known diabetic and chronic smoker, presented with exertional angina Class II. All his biochemical pa-rameters and ECG were normal. Chest X ray was normal (fig 1). Coronary angiogram revealed severe triple vessel disease i.e, proximal left anterior descending artery 90% stenosis, mid LAD after D1 95%, left circumflex 90% and right coronary artery (dominant) 70% stenosis. Echo showed normal LV function with ejection fraction of 61%. He was on carvedilol, diltiazem, sorbitrate and insulin. He was taken up for elective Coronary
Premedicated with tablet diazepam 10 mg 2 hours before surgery. An-aesthesia induced with fentanyl, midazolam, thiopentone, pavulon, xy-locard and maintained with oxygen + air + intermittent isoflurane and
After heparinisation, CPB was instituted. CABG x 3 grafts done under warm blood cardioplegic arrest. Total CPB time was 73 minutes and aortic cross clamp time was 44 minutes. Came off bypass with minimal inotropic support. Elective ventilation continued and was extubated on
the next day morning. Chest x rays within normal limits(fig 2).
Inotropes were weaned off by 3rd postoperative day. Though patient
haemodynamically stable, he was very drowsy but arousable. He was drowsy even without any seda-tives. He could not be ambulated due
On the 5th postoperative day, patient developed tachypnea, tachycardia, wheezing and
86%) with oxygen 10 L/min by mask. Chest X-ray showed me-diastinal widening with bilateral haziness (Fig 3). Arterial line and central venous catheter were inserted. ABG report showed hypoxia and hypercarbia (PO2- 65 mm Hg PCO2- 51.7 mm Hg). Cardac tam-
ed and was shifted to OT immediately for reexploration. After intuba-tion his lungs were found stiff on manual ventilation. The peak airway pressure was very high. Intraoperatively there was no evidence of tam-ponade. About 300 ml of serous fluid was removed from pleural cavities. Peroperatively the lung consistency was firm and turgid (boggy lung).
Post op ventilation continued on pressure controlled ventilation mode with the following settings: pressure control – 30 cm H O, PEEP – 10 cm H O, RR – 14/min, I: E ratio 1:1, FiO - 0.8. The PaOwas 78. Patient was on renal dose of dopamine, low dose adrenaline, lasix 1mg/hr, and aminophylline infusions. In 3 days, he had a negative balance of 3400 ml. His chest x-ray showed marked improvement (Fig 4). The PaO ratio improved from 78 to215.5. He was weaned off
PUMP LUNG Dr. Satheesh Kumar. N Cardiac Anaesthesiologist
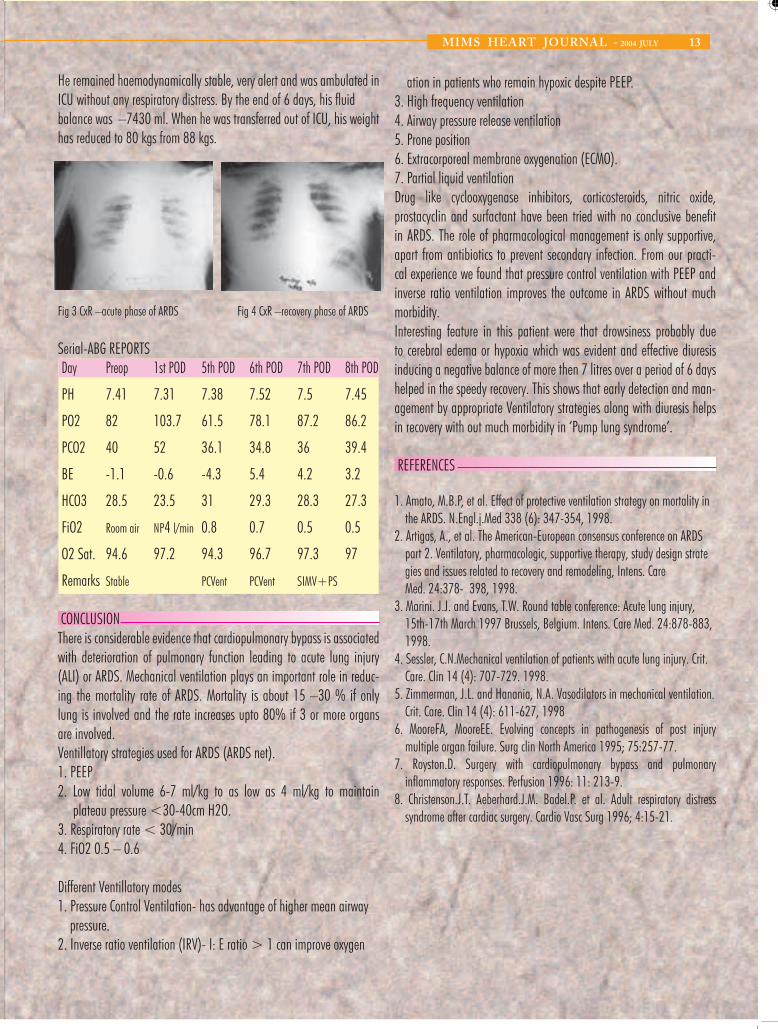
12 MIMS HEART JOURNAL - 2004 JULY
24MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY01..
Coronary Artery Bypass Grafting or Bypass Surgery, as it is commonly known, has been a field, which has seen umpteen number of newer techniques and innovations and change of basic concepts creeping in and out. We were able to contribute to this surge of innovations in this field through our new invention – the “Vettath’s
Anastamotic Obturator” (VAO) – a simple proximal anastamotic device for anastamosing vein grafts onto the aorta without using side clamp. The first article in this issue is a note on this novel tool in our kitty.It is widely known that surgery starts were medicine fails. But today, newer developments in interventional technology have helped cardiologists pull back some of the surgeons’ domains into their repertoire. PDA and ASD are glorious examples of such lesions, which can and are being very effectively handled by Cardiologists today. We are having a feature on non-surgical PDA closure, which is very much in vogue now a days.We bring to you some of the important aspects in the critical care of post cardiac surgical patients and a note on a pump associated postoperative problem – the Pump Lung Syndrome. Pump related problems have been a matter of concern and hence keeping away from the pump is a sensible fashion of the day. Beating Heart Surgery or Off Pump Coronary Artery Bypass (OPCAB) is a routine procedure. We bring you our experience on early Off Pump CABG in Acute Coronary Syndrome patients, a procedure which was considered impossible not so long ago.Pharmacotherapy for congestive cardiac failure aims at reverse remodeling of the ventricles. But despite optimal medication a major portion of such patients get little benefit. Various treatment options for refractory cardiac failure have been described. Biventricular pacing which aims at correcting the intraventricular conduction delay and in coordinating both the ventricles is one among them. We intend to bring you some facts about this treatment modality through one of the cases managed in our center.We also bring you an elaborate review on Infective Endocarditis and its management in adults based on a wide range of published studies, guidelines and literature. We sincerely do hope that this effort of ours, to transfer some of our limited knowledge in this field onto our peers in Kerala through the second edition of the MIMS Heart Journal will bear some fruit. We stress our commitment in providing you with outstanding information about the recent advances in Cardiovascular Sciences and related fields, which are very much available in the Malabar region.
EDITORIAL
Cardiopulmonary bypass (CPB) is often followed by pulmonary dysfunc-tion and is also regarded as a risk factor for development of acute respi-ratory distress syndrome (ARDS). When pulmonary dysfunction cannot be directly attributed to a specific cause such as infection or ischemia, the concept of the “pump lung syndrome” or “systemic inflammatory re-sponse syndrome to CPB” is used as alternative explanation. Cardiopul-monary bypass is associated with a whole body inflammatory response, which involves activation of complement, leukocytes and endothelial cells , secretions of cytokines, proteases, arachidonic acid metabolites and oxygen free radicals. Leukocyte adhesion to microvascular endo-thelium, leukocyte extravasation and tissue damage are the final steps. Although the inflammatory response to cardiopulmonary bypass often remains at sub clinical levels, it can lead to major organ dysfunction and multiple organ failure. ARDS occurs in about 0.5 to 1.7% of patients undergoing open-heart surgery. We report a case of ARDS following on pump coronary artery bypass grafting .
CASE REPORT
A fifty-year-old male, weighing 88 kg, a known diabetic and chronic smoker, presented with exertional angina Class II. All his biochemical pa-rameters and ECG were normal. Chest X ray was normal (fig 1). Coronary angiogram revealed severe triple vessel disease i.e, proximal left anterior descending artery 90% stenosis, mid LAD after D1 95%, left circumflex 90% and right coronary artery (dominant) 70% stenosis. Echo showed normal LV function with ejection fraction of 61%. He was on carvedilol, diltiazem, sorbitrate and insulin. He was taken up for elective Coronary Artery Bypass Grafting.Premedicated with tablet diazepam 10 mg 2 hours before surgery. An-aesthesia induced with fentanyl, midazolam, thiopentone, pavulon, xy-locard and maintained with oxygen + air + intermittent isoflurane and fentanyl/midazolam/atracurium infusion. After heparinisation, CPB was instituted. CABG x 3 grafts done under warm blood cardioplegic arrest. Total CPB time was 73 minutes and aortic cross clamp time was 44 minutes. Came off bypass with minimal inotropic support. Elective ventilation continued and was extubated on
the next day morning. Chest x rays were within normal limits(fig 2). Inotropes were weaned off by 3rd postoperative day. Though patient was haemodynamically stable, he was very drowsy but arousable. He was drowsy even without any seda-tives. He could not be ambulated due to drowsiness.
On the 5th postoperative day, patient developed tachypnea, tachycardia, wheezing and a drop in saturation (SpO284-86%) with oxygen 10 L/min by mask. Chest X-ray showed me-diastinal widening with bilateral haziness (Fig 3). Arterial line and central venous catheter were inserted. ABG report showed hypoxia and hypercarbia (PO2- 65 mm Hg PCO2- 51.7 mm Hg). Cardac tam-ponade was suspected and was shifted to OT immediately for reexploration. After intuba-tion his lungs were found stiff on manual ventilation. The peak airway pressure was very high. Intraoperatively there was no evidence of tam-ponade. About 300 ml of serous fluid was removed from pleural cavities. Peroperatively the lung consistency was firm and turgid (boggy lung). Chest was closed with drains in situ.Post op ventilation continued on pressure controlled ventilation mode with the following settings: pressure control – 30 cm H2O, PEEP – 10 cm H2O, RR – 14/min, I: E ratio 1:1, FiO2 - 0.8. The PaO2 / FiO2 ratio was 78. Patient was on renal dose of dopamine, low dose adrenaline, lasix 1mg/hr, and aminophylline infusions. In 3 days, he had a negative balance of 3400 ml. His chest x-ray showed marked improvement (Fig 4). The PaO2 / FiO2 ratio improved from 78 to215.5. He was weaned off ventilator and extubated on the 4th day. All the infusions were stopped.
PUMP LUNG SYNDROMEA case report
Fig 2 – Immediate post op CxR
Fig 1 - pre op CXR
Dr. Satheesh Kumar. N Cardiac Anaesthesiologist
mimslouranlfinal.indd 4 7/21/2004 11:07:55 PM
- 2004 13
3. High frequency ventilation 4. Airway pressure release ventilation
6. Extracorporeal membrane oxygenation (ECMO).
Drug like nitric oxide,
morbidity.
REFERENCES
the ARDS. N.Engl.j.Med 338 (6): 347-354, 1998.
gies and issues related to recovery and remodeling, Intens. Care Med. 24:378- 398, 1998.
15th-17th March 1997 Brussels, Belgium. Intens. Care Med. 24:878-883, 1998.
4. Sessler, C.N.Mechanical ventilation of patients with acute lung injury. Crit. Care. Clin 14 (4): 707-729. 1998.
Crit. Care. Clin 14 (4): 611-627, 1998
multiple organ failure. Surg clin North America 1995; 75:257-77. 7. with and pulmonary
ICU without any respiratory distress. By the end of 6 days, his fluid
has reduced to 80 kgs from 88 kgs.
Fig 3 CxR –acute phase of ARDS Fig 4 CxR –recovery phase of ARDS
Serial-ABG REPORTS Day 1st POD 5th POD 6th POD 7th POD 8th POD
PH 7.41 7.31 7.38 7.52 7.5 7.45
PO2 82 103.7 61.5 78.1 87.2 86.2
PCO2 40 52 36.1 34.8 36 39.4
BE -1.1 -0.6 -4.3 5.4 4.2 3.2
HCO3 28.5 23.5 31 29.3 28.3 27.3
FiO2 Room air NP4 l/min 0.8 0.7 0.5 0.5
O2 Sat. 94.6 97.2 94.3 96.7 97.3 97
Remarks Stable SIMV+PS
CONCLUSION
are involved.
1. PEEP
plateau pressure <30-40cm H2O. 3. Respiratory rate < 30/min 4. FiO2 0.5 – 0.6
pressure. 2. Inverse ratio ventilation (IRV)- I: E ratio > 1 can improve oxygen
MIMS HEART JOURNAL JULY ..
ation in patients who remain hypoxic despite PEEP.
5. Prone position
7. Partial liquid ventilation cyclooxygenase inhibitors, corticosteroids,
prostacyclin and surfactant have been tried with no conclusive benefit in ARDS. The role of pharmacological management is only supportive, apart from antibiotics to prevent secondary infection. From our practi-cal experience we found that pressure control ventilation with PEEP and inverse ratio ventilation improves the outcome in ARDS without much
Interesting feature in this patient were that drowsiness probably due to cerebral edema or hypoxia which was evident and effective diuresis inducing a negative balance of more then 7 litres over a period of 6 days helped in the speedy recovery. This shows that early detection and man-agement by appropriate Ventilatory strategies along with diuresis helps in recovery with out much morbidity in ‘Pump lung syndrome’.
1. Amato, M.B.P, et al. Effect of protective ventilation strategy on mortality in
2. Artigas, A., et al. The American-European consensus conference on ARDS part 2. Ventilatory, pharmacologic, supportive therapy, study design strate
3. Marini. J.J. and Evans, T.W. Round table conference: Acute lung injury,
5. Zimmerman, J.L. and Hanania, N.A. Vasodilators in mechanical ventilation.
6. MooreFA, MooreEE. Evolving concepts in pathogenesis of post injury
Royston.D. Surgery cardiopulmonary bypass inflammatory responses. Perfusion 1996: 11: 213-9.
8. Christenson.J.T. Aeberhard.J.M. Badel.P. et al. Adult respiratory distress syndrome after cardiac surgery. Cardio Vasc Surg 1996; 4:15-21.
He remained haemodynamically stable, very alert and was ambulated in
balance was –7430 ml. When he was transferred out of ICU, his weight
Preop
PCVent PCVent
There is considerable evidence that cardiopulmonary bypass is associated with deterioration of pulmonary function leading to acute lung injury (ALI) or ARDS. Mechanical ventilation plays an important role in reduc-ing the mortality rate of ARDS. Mortality is about 15 –30 % if only lung is involved and the rate increases upto 80% if 3 or more organs
Ventillatory strategies used for ARDS (ARDS net).
2. Low tidal volume 6-7 ml/kg to as low as 4 ml/kg to maintain
Different Ventillatory modes 1. Pressure Control Ventilation- has advantage of higher mean airway

02MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY23..
MIMS HEART JOURNAL - 2004 JULY 11..
DEPARTMENTPROFILE
DEPARTMENTOFCARDIOVASCULAR&THORACICSURGERY
Dr.Murali.PVettath,MBBS,DNB,MChDr.SheenPeeceeyenC.S,MBBS,MS,MChDr.BaburajanA.K,MBBS,DNB,MCh
DEPARTMENTOFCARDIACANAESTHESILOGY
Dr.A.VKannan,MBBS,MD,FCACCDr.SatheeshKumar.N,MBBS,MD
DEPARTMENTOFCARDIOLOGY
Dr.AliFaizal,MBBS,MD,DMDr.AsishKumar.M,MBBS,MD,DMDr.DineshBabuK.V,MBBS,MD,DMDr.MuraliKrishna,MBBS,MD,DM
CONTENTS
VETTATH’SANASTAMOTICOBTURATORAnewproximalanastamoticdevice
INTENSIVECAREMANAGEMENTAFTERCARDIACSURGERYWherewestandtoday
TRANS-CATHETERCLOSUREOFPATENTDUCTUSARTERIOSUSAdieutosurgery
OPCABFORACUTECORONARYSYNDROMEThewaytogo
CARDIACRESYNCHRONIZATIONTHERAPYAcasereportwithreviewofliterature:
PUMPLUNGSYNDROMEAcasereport
INFECTIVEENDOCARDITIS-DIAGNOSISANDMANAGEMENTINADULTSAnoverview
03
05
07
0810
12
14ForPrivateCirculationonly
NoPartofthispublicationmaybereproducedbyanymeans,includingelectronicmedia
Graphics-Design-bynnaturalwondders-calicut
sizable proportion of patients with heart failure remain symptomatic and succumb to death, and hence additional treatment strategies like biven-tricular pacing have been developed.About 30 % of patients with chronic heart failure have intraventricular conduction delay such as left or right bundle branch block leading to loss of coordination of ventricular contraction. Such asynchrony is evident on the surface ECG as widening of QRS interval [> 120 m.sec]. This can impair the contractile reserve of the heart, and also enhance the severity of the functional mitral regurgitation. Intraventricular conduction delay has been associated with electrical instability and increased risk of sud-den death in patients with heart failure.
BENEFICIAL EFFECTS OF BIVENTRICULAR PACING: Short-term results of clinical trials with devices for atrial synchronized biventricular pacing to coordinate left and right ventricular contrac-tions are encouraging. Notable improvements in primary end points of NYHA functional class, six minutes walking distance and quality of life were constantly seen with cardiac resynchronization therapy [CRT]. In the recently published MIRACLE trial, the resynchronization group had significant improvement in peak oxygen consumption and total exercise time. Further, the left ventricular ejection fraction increased and the end-diastolic dimension, the magnitude of mitral regurgitation and the dura-tion of QRS all decreased in the resynchronization group. Biventricular pacing was associated with fewer hospital admissions and fewer days in the hospital for heart failure. The combined risk of a major clinical event [death or hospitalization for heart failure] was 40 % lower in the resynchronization group. In the study of Breithardt et al [JACC 2003 May 21, 41 [10]: 1852] cardiac resynchronization was associated with a significant reduction in severity of mitral regurgitation. The effective regurgitant orifice area decreased from 25 ± 19 mm to 13 ± 8 mm. This was directly related to an increase in left ventricular pressure rise [LV + dp/dt max]. Favourable effect on heart rate variability by resynchro-nization was shown by Adamson et al [circulation 2003 July 22; 108 (3) 266-9]. In the Ventak CHF study [Higgins SL et al JACC 2000 Sept; 36 (3)] synchronized biventricular pacing reduced the frequency of ICD therapies in patients receiving both the devices. Preliminary trial results show significant survival benefit when an ICD is combined with biven-tricular pacing and a 40 % reduction in hospitalization for heart failure.
ELIGIBLE PATIENT POPULATION:Patients with moderate-to-severe symptoms of heart failure [NYHA Class III or IV], left ventricular ejection fraction < 35 % and a wide QRS [> 130 m.sec] with left bundle branch block morphology are currently considered eligible for biventricular pacing. Heterogenous response to biventricular pacing has challenged the predictive accuracy of wide QRS complex in surface ECG for ventricular dyssynchrony. More sensitive tech-niques like Echocardiography with Tissue Doppler imaging to identify
regional delay in left ventricular contraction have been shown to better predict the responders from resynchronisation. [Makaryus AN et al Echo-cardiography] 2003 April 20 (3) 217-23.
TECHNIQUES & COMPLICATIONS:Prior to the procedure, a levophase of coronary angiogram is recorded to profile coronary sinus and cardiac veins. Device implantation is done in left infraclavicular pocket and venous access is obtained via subcla-vian vein puncture. Preformed sheaths in different curves are available to facilitate cannulation of the coronary sinus. With availability of over-the-wire leads, to enter the left cardiac vein, the technical success rate of CRT has improved. Placement of atrial and right ventricular leads are not different from the conventional pacemakers. The major complications associated with the procedure include dissection and perforation of the coronary sinus leading to hemopericardium, complete heart block, asys-tole, and arrhythmias. MIRACLE trial reported a technical failure rate of 8 % and major complications of 1-2 %, which include cardiac tamponade or cardiac arrest requiring resuscitation. Late dislodgment of left ventricu-lar lead can occur in as high as 6 % of patients.
FUTURE PERSPECTIVES:In considering devices for heart failure, the growing weight of evidence for biventricular pacing needs to be considered alongside the expand-ing indications for implantable cardioverter defibrillators. ICDs have been shown to significantly reduce the mortality and propensity for malignant ventricular arrhythmias in patients with left ventricular dysfunctions. Syn-chronized pacing can complement this effect by reducing the need for hospitalization for heart failure and the frequency of ICD therapies. Thus, patients with symptomatic heart failure due to ischemic cardiomyopathy and wide QRS complex, might be better served by a combined resynchro-nization pacer and defibrillator. However, the issue of cost effectiveness remains contentious and warrants further examination when long-term data are available.
REFERENCES: 1 Higgins SL, Yong P, Sheck D et al; biventricular pacing diminished the need for implantable cardioverter defibrillator therapy. Ventak CHF Investigators. J Am Coll Cardiol. 2000 Sep; 36 (3): 828-312 Young JB, Abraham WT, Smith AL et al; combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: the MIRACLE ICD Trial. JAMA. 2003 May 28; 289 (20): 2719-213 Makaryus AN, Arduini AD, Mallin J et al; echocardiographic features of pa-tients with heart failure who may benefit from biventricular pacing. Echocar-diography. 2003 Apr; 20(3) 217-234 Abraham WT., Fisher WG., Smith AL et al, Cardiac resynchronization in chronic heart failure. The MIRACLE study MEJM.
mimslouranlfinal.indd 57/21/2004 11:09:49 PM
14 - 2004
docarditis carries a very high risk of morbidity and mortality.
Infective endocarditis
damaged valves or other cardiac structures are secondarily infected.
viridans and Enterococci.
vegetation may become organized and calcified.
and abscess and sinus or fistulae if present are well organized.
infective endocarditis.
portance.
INFECTIVE ENDOCARDITIS
AN OVERVIEW
MIMS HEART JOURNAL JULY
Infective Endocarditis, an infection of the inner walls of the cardiac cham-bers, valves, aortic root and prosthetic material is not an uncommon problem in our region. Advances in diagnosis and pharmacotherapy have changed the whole scenario since William Osler (1885) projected bacte-rial infection as the root cause, valvular heart disease as a predisposing factor and valvular incompetence and embolism as lethal complications of what he called Malignant Endocarditis. But even today, Infective En-
For bacterial endocarditis to occur there should be bacteremia, damaged endothelium vulnerable to infection, turbulence along haemodynamic path, and a virulent microorganism, which can overcome the natural defenses of the host or a host with a severely compromised immune system. Thus patients with acquired cardiac lesions like Rheumatic heart disease, degenerative valve disease or congenital lesions like Ventricular
Septal Defect, Tetralogy of Fallot, Congenital Aortic stenosis, complex cyanotic anomalies, Patent Ductus Arteriosus, Systemic to pulmonary arterial shunts etc. are prone for infective endocarditis. Recently intra-venous drug abuse is gaining more importance as a common cause for
The term infective endocarditis includes acute, subacute and chronic pro-cess of bacterial, viral, fungal or rickettsial aetiology. Acute endocarditis is a life threatening infection usually of normal heart valves, during the course of septicemia by virulent pyogenic microorganism such as hae-molytic Streptococci or Staphylococci. In subacute endocarditis, already
Acute native valve endocarditis accounts for 25% of Infective Endo-carditis. Severe sepsis, long term indwelling catheter, IV drug abuse and fungemia are predisposing factors. The usual affecting organism is Staphylococcus aureus. Other common organisms are Streptococcus
The initial stage of valvular infection is surface vegetation – composed of platelets, fibrin and the causative microorganism. Organisms multiply within the vegetation and are thereby protected from the host defenses and antibiotics. They can be a source for repetitive bacteremia. Veg-etations are initially soft and friable and may embolise. They may also produce immune complex mediated and allergic vasculopathies. Large
Endocarditis is considered active surgically when surgery is performed in the presence of obvious local cardiac infection (active vegetation/ab-scess/sinus/fistulae) or when surgery is done while the patient is still on or within two weeks of termination of medical management for Infective Endocarditis. Endocarditis is considered healed when there is no active cardiac infection or inflammation, vegetation if present is endothelialised
Surgical management of infective endocarditis was first reported by Kay et al (1961) in a patient with Tricuspid valve endocarditis and it was Wallace (1965) who first reported valve replacement as treatment for
Early Diagnosis, effective management and prompt recognition of com-plication are essential to good patient outcome. For that general idea of the clinical presentation and diagnostic modalities are of great im-
- DIAGNOSIS AND MANAGEMENT IN ADULTS
Dr. Sheen Peeceeyen. C.S Cardiac Surgeon

22MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY03..
INTRODUCTIONWith the advent of beating heart surgery, more than 50% of coronary artery bypass graft surgeries are performed in most coronary centers in India without the use of heart-lung machine. But the neurologic prob-lems caused by side clamping the aorta in performing the proximal anas-tomoses still remain. Hence, there has been a great deal of research to find an effective alternative to avoid side clamping the aorta. A couple of anastamotic devices have already arrived in the market, but since the costs of these devices are prohibitive, we designed our own device for proximal anastomoses.
PATIENTS AND METHODSFrom July 2002 to July 2003, we performed 235 coronary artery bypass graft surgeries on the beating heart with 177 of these procedures performed off-pump and 58 of them carried out with pump assistance. Initially, proximal anastomoses of vein grafts were performed with aortic side clamp. Of late, all our top ends are being performed with VAO. 177 patients have had their proximal Saphenous Vein Graft (SVG) anastomo-ses performed with our VAO.Before VAO was used on patients, it was tried for anastomosing vein grafts on the aortas and pulmonary arteries of various perfused animal heart models. The aortic and pulmonary artery pressures were maintained at 110 to 120 mm Hg systolic while these anastomoses were being per-formed. These conduits were then explanted and examined for suture placement to see if all the aortic layers were included.
VETTATH’S ANASTAMOTIC OBTURATOR (VAO)This metallic instrument is made of solid steel (Figure 1). It is 18 cm long and comes in small and medium sizes (5 mm and 6 mm in diameter respectively). The holding part is smooth. The inserting bit has a ridge 2.5 cm from the end (Figure 2). This 2mm ridge projects perpendicularly from the steel rod. There are 3 equidistant grooves in the inserting end that are 1 mm deep a 1.5 cm long. The ridge helps to prevent blood from spurting directly into the eye. The grooves allow the needle to pass through the rod and thereby include the aortic intima in the suture.
SURGICAL TECHNIQUEVAO allows us to anastamose the proximal ends of the vein grafts, before or after the distal anastomoses. The aortic site proposed for anastomosis marked with diathermy. Two 3-0 polypropylene purse-string sutures are applied 1 cm away from the site. The aorta is stabbed with a No.11 blade knife, and punched with 4mm or 4.5mm aortic punch (for 5-mm or 6-mm VAO), respectively. The punch hole is blocked with the left index finger. VAO is introduced and purse strings are tightened just enough to prevent excessive bleeding. Once the obturator is in and the snares are tightened, the proximal vein anastomoses is performed as usual with 5.0 or 6.0 polypropylene suture.
VETTATH’S ANASTAMOTIC OBTURATOR OUR EXPERIENCE OF 269 PROXIMAL ANASTOMOSES
Dr. Murali P. VettathChief Cardiac Surgeon
10 MIMS HEART JOURNAL - 2004 JULY
MYCOTICANEURYSMSresult from septic embolization of vegetation to vasa vasorum or intraluminal infective embolus with subsequent spread through the intima and outwards through the vessel wall. They occur mostly at arterial branching points as emboli are usually impacted at such points. Intracranial mycotic aneurysms are more common than ex-tracranial ones; which usually affect the visceral arteries and arteries to upper and lower limbs.The overall mortality rate in infective endocarditis patients with intra-cranial mycotic aneurysm is about 60%. Streptococci account for about 50% and Staphylococcus 10% of intracranial mycotic aneurysms. The distal MCA branches are more commonly affected. Intracranial mycotic aneurysms are multiple in about 20% of patients. Clinical presentation is highly variable.Routine screening is not required except when clinical findings are sug-gestive of an intracranial pathology. Contrast enhanced CT or Magnetic Resonance Angiography are useful in detecting these lesions but con-ventional four-vessel angiography still remains the diagnostic test of choice.Intracranial mycotic aneurysms (ICMA) may heal with medical therapy. Proximal aneurysms should be monitored with serial angiograms and CT as ligation of these may lead to severe neurological deficit. ICMA distal to major branching points may be ligated or excised. Some patients need both valve replacements and ICMA ligation. Bioprosthetic valve is prefer-able in such patients as anticoagulation can be avoided.
Extra-cranial mycotic aneurysms (ECMA) may present as tender pulsatile masses. Intra-thoracic or intra-abdominal ECMAs are asymptomatic until leakage or rupture occurs. Proximal and distal ligation of aneurysms and restoration of blood flow with autologous vein grafts through extra-ana-tomic site is the only hope for a radical cure.
SPLENICABSCESSin infective endocarditis may be caused either by an in-fected embolus or by bacterial seeding of a splenic infarct. Streptococcus viridans and Staphylococcus aureus accounts for around 40% of cases, enterococci 15%, gram-negative bacilli and fungi in <5%. Spleno-megaly is present only in about 30% and is not a reliable sign. Back, left flank, left upper quadrant pain or abdominal tenderness may be present. Persistent fever, bacteremia and sepsis may be suggestive of splenic abscess. Splenic rupture with hemorrhage is a rare complication. CT / MRI are the best diagnostic tests. Definitive treatment is splenectomy with appropriate antibiotics. Splenectomy should be performed before valve replacement, as the risk of prosthetic valve infection is very high with a splenic abscess.
PROPHYLAXIS AGAINST INFECTIVE ENDOCARDITISAntibiotic prophylaxis against infective endocarditis is recommended in a group of conditions, which carry with it a very high risk of playing a host to this dreaded disease. Patients with prosthetic heart valves, complex cyanotic congenital heart disease and previous history of infective endo-carditis carry a very high risk. Those with acquired lesions like rheumatic valve disease, hypertrophic cardiomyopathy (HCM), mitral valve prolapse with regurgitation, etc carry a moderate risk with them. Such patients need antibiotic prophylaxis while undergoing any invasive procedures like dental extraction or manipulation of the respiratory, genitourinary or gastrointestinal tracts.The standard general prophylaxis for patients at risk is Amoxicillin 2gm (50mg/kg in children) given orally one hour before the procedure. Those who are unable to take oral medications are given injection Ampicillin. Those allergic to penicillins are given either Clindamycin or Cephalexin or Cefadroxil or Azithromycin or Clarithromycin. An Aminoglycoside should be added to the above patients if they are undergoing procedures on the genitourinary or gastrointestinal tracts. Vancomycin with Gentamicin is preferred in patients who are allergic to penicillin.
CARDIAC RESYNCHRONIZATIONTHERAPYA case report with review of literature
CASE REPORT:Mr. R, a 36-year-old gentleman was diagnosed to have Hypertrophic Non-Obstructive Cardiomyopathy with LV systolic dysfunction. He pre-sented to us with worsening of dyspnea, orthopnea, and paroxysmal nocturnal dyspnoea . He had been symptomatic since the last 4 years and in NYHA functional class IV since 2 months. He had two episodes of syncope associated with palpitation during the previous 2 months. He was tachypnoeic on admission, heart rate was 56 beats /min, and blood pressure was 100/80 mmHg. Mean jugular venous pressure was not raised but ‘a’ wave was prominent. Apex beat was in the sixth intercostal space 1 cm outside the midclavicular line. First heart sound was soft, S2 was normally split, and LV S3 and S4 were prominent. Fine basal crepitations were present bilaterally. ECG showed sinus rhythm at 50 bpm, first degree AV block, and LBBB with a QRS duration of 240 m.sec. Chest X-ray showed grade III PVH, cardiomegaly, and mild pulmonary edema. All the routine hematological and biochemical parameters were normal. 2-D Echo Color Doppler examination showed asymmetrical sep-tal hypertrophy with global LV hypokinesis and LV ejection fraction of 35 % by Simpson’s method. There was moderate mitral regurgitation with MR jet area of 7 cm2. This gentleman had cardiac evaluation at another cardiac center in 10 months back. 24-hour Holter at that time showed one episode of non-sustained ventricular tachycardia and frequent multiform VPCs with cou-plets and bigeminy. Monomorphic sustained VT was inducible on electro-physiological testing. Angiography revealed normal coronary arteries. Patient was stabilized with I.V diuretics, Digoxin, ACE inhibitors, and supportive measures. The most appropriate therapeutic option was to provide an Implantable Cardioverter Device with biventricular pacing. However, since the patient could not afford the cost of an Implantable Cardioverter Device, the second best option of biventricular pacing with anti-arrhythmic drugs was discussed with the patient and relatives, to which they agreed.Patient was taken up for transvenous implantation of atrial synchronized biventricular pacing through a left infra-clavicular incision. Subclavian
puncture was done and coronary sinus was cannulated using the pre-formed sheath. A 6French balloon catheter was introduced through the coronary sinus sheath for venography. Attempts to negotiate the guide-wire in to the left cardiac vein were not successful. RA and RV apical leads were placed to which the pulse generator was connected and the wound closed. Subsequently, patient was taken for LV epicardial lead placement through left anterolateral thoracotomy. The proximal end of this lead was tun-neled to the infra-clavicular pocket and connected to the pulse generator. Pacemaker was programmed to biventricular pacing with an AV delay of 140 m.sec. Post-pacing ECG showed shortening of QRS duration to 130 m.sec, which is a significant indicator of response to therapy. Repeat Echocardiagraphic study revealed improvement in LV ejection fraction and reduction of MR jet area from 7 to 4 cm2.
REVIEW OF LITERATURE:INTRODUCTION:The pharmacotherapy of congestive heart failure is primarily based on antagonism of neurohormonal pathways namely, the sympathetic ner-vous system and the “renin-angiotensin-aldosterone axis”. Most of the drugs have been shown to reduce mortality and morbidity and in some cases they improve the underlying structural abnormalities of the heart by a process called reverse remodelling. Despite these therapeutic ad-vances,
Dr. Dinesh Babu .K.VCardiologist
mimslouranlfinal.indd 27/21/2004 11:03:23 PM
The diagnosis of infective endocarditis is straight forward in patients with the classical Oslerian manifestations of bacteremia or fungaemia, active valvulitis, peripheral emboli and immunologic vascular phenomena. In others, these classical findings may be few or absent as in Infective En-docarditis caused by Staphylococcus aureus infection of right sided heart valves or in patients where infective endocarditis is caused by the HACEK (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella) group of organisms. Immunologic vascular phenomenon is characteristic of subacute bacterial endocarditis. They are rarely seen in acute infective endocarditis on presentation, as the disease process is so rapid. Right-sided infective endocarditis does not produce peripheral embolism and immunological vascular phenomenon. This variability in clinical presentation of Infective Endocarditis warrants an optimal diagnostic strategy for early diagnosis. The Beth Israel criteria was proposed in 1981 by Van Reyn which was so stringent that only those patients confirmed pathologically were considered Definite Infec-tive Endocarditis patients and those with bacteremia, new valvular regur-gitation and vascular phenomenon were considered as Probable Infective Endocarditis patients. Durack et al from Duke University proposed the Modified Duke’s Criteria in 1994 incorporating Echocardiographic findings into the important di-agnostic parameters in Beth Israel Criteria. Moreover, intravenous drug abuse was recognized as an important cause for infective endocarditis in Duke’s criteria. The Duke’s clinical criteria stratified the various parameters into two broad groups – Major and Minor criteria as shown below.
MODIFIED DUKE’S CRITERIA FOR CLINICAL DIAGNOSIS OF INFECTIVE ENDOCARDITIS
MAJOR CRITERIA
1. Positive blood culture for IE A. Typical microorganism consistent with IE from 2 separate blood cultures as: (i) Viridans Streptococci, Streptococcus bovis, or HACEK
group, or (ii) Community-acquired Staphylococcus aureus or entero
cocci, in the absence of a primary focus or B. Microorganisms consistent with IE from persistently positive blood cultures defined as (i) ≥2 positive cultures of blood samples drawn
>12 hours apart or (ii) All of 3 or a majority of ≥4 separate cultures of blood
(with first and last sample drawn ≥1 hour apart)
- 2004 15MIMS HEART JOURNAL JULY ..
2. Evidence of endocardial involvementA. Positive echocardiogram for IE defined as (i)Oscillating intracardiac mass on valve or supporting struc
tures, in the path of regurgitant jets, or on implanted material in the absence of an alternative anatomic explana tion, or
(ii) Abscess, or(iii) New partial dehiscence of prosthetic valve
or B. New valvular regurgitation (worsening or changing of pre existing murmur not sufficient)
MINOR CRITERIA
1. Predisposition: predisposing heart condition or intravenous drug abuse
2. Fever: temperature ≥38.0°C3. Vascular phenomena: major arterial emboli, septic pulmo
nary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway lesions
4. Immunologic phenomena: glomerulonephritis, Osler’s nodes, Roth spots, and rheumatoid factor
5. Microbiological evidence: positive blood culture but does not meet a major criterion as noted above or serological evidence of active infection with organism consistent with IE
6. Echocardiographic findings: consistent with IE but do not meet a major criterion as noted above.
Diagnosis of Definite Infective Endocarditis by Duke Criteria needs the presence of two major criteria or 1 major and 3 minor criteria or 5 minor criteria or pathological proof if IE. Those patients who do not meet the criteria for “Definite”Infective Endocarditis are labeled as “Probable” In-fective Endocarditis. Those patients whose symptoms reduce either with no treatment or within a short-term after diagnosis and those patients with no pathological evidence of infective endocarditis are labeled as rejected cases. The Duke Criteria is by far more specific and sensitive than the Beth Is-rael Criteria. Clinical suspicion of Infective Endocarditis may be raised by fever, other systemic symptoms along with physical findings like Osler’s nodes, petechiae, Janeway lesions, Roth spots, splenomegaly, newly di-agnosed clubbing and a new changing cardiac murmur. High index of suspicion in susceptible patients helps in diagnosing much before these findings set in. The offending organism can be demonstrated in 3 sets of blood cultures. (Each set with 1 aerobic and 1 anaerobic culture sample) obtained at intervals of more than one hour, within the first 24 hours is mandatory. 5 to 6 samples may be needed in some patients.
04MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY21..
MIMS HEART JOURNAL - 2004 JULY 09..
of 0.5 to 1 mm; (vi) T inversion of > 1mm in leads with dominant R waves.Patients with chest pain probably non cardiac, one risk factor (not Diabe-tes Mellitus), flat T wave or < 1 mm inversion in leads with dominant R waves or normal ECG are considered to be carrying a low risk.Percutaneous intervention has proven to prevent irreversible myocardial damage. Cardiac catheterization, Angioplasty and CABG in ACS has in-creased considerably in the past two decades. In ACS, PTCA against the culprit lesion and antiplatelet therapy can be performed with an initial success rate of > 95%, although the incidence of procedure related complication is high, world wide.CABG is considered for patients with coronary lesion that are not suitable for or do not respond to catheter based reperfusion. The reported inci-dence of perioperative death is 4 % and MI is 10 % higher when CABG is performed urgently than semi urgently in ACS. Therefore, efforts should be made to stabilize the patients pharmacologically before emergency revascularization procedures are contemplated. Use of IABP aids as a bridge to Angioplasty or CABG in ACS patients.The need for revascularization is based on diagnosing the culprit lesion early. Various institutions adopt various protocols for coronary angiogra-phy (CAG)in ACS. Two strategies are generally followed- the early inva-sive strategy and the conservative strategy. The early invasive strategy incorporates coronary angiography for all sta-bilized patients within 48 hours of presentation. The conservative strat-egy prescribes angiography for high-risk patients (ie CHF, LVEF<50%, malignant arrhythmia, recurrent ischaemia, prior revascularization etc). Both early invasive and conservative strategies have been found to pro-duce similar clinical outcomes by the TIMI 2B and VANQUISH studyDecision about further proceedings is made based on the disease pattern revealed by CAG. Emergency surgical revascularization may be also need-ed in the setting of a failed thrombolysis or PTCA with acute occlusionThe morbidity of patients operated on after acute MI remains relatively high when compared to stabilized patients. This is mainly because, the adverse effect of CPB is poorly tolerated by a heart with an evolving MI. It is reasonable to think that keeping off the pump may be advantageous in this subgroup of patients.The optimal timing of surgery for ACS remains indecisive. Various studies have shown that the mortality rate of patients who underwent surgical revascularization within 48 hours of an acute MI was significantly higher compared to after 48 hours.A recent multi-center analysis has shown clearly that the perioperative mortality in acute MI patients declined considerably with the increasing time interval. The first 6 hours is said to be the most dangerous period with mortality of about 10%. The mortality depends not only on the tim-ing of surgical revascularization but also on the LV function, presence of haemodynamic stability and presence of collateral circulation.
Cardiopulmonary bypass (CPB) is a significant factor affecting the out-come in patients undergoing early CABG after ACS. Various studies have proven that the mortality rate is nearly 5 times higher in emergency CABG done on a stopped heart than on a beating heart. This deleterious effect of CPB is most evident in patients operated within 48 hours of an acute cardiac event.
OUR EXPERIENCE 306 CABGs were performed in our department during the period from July 2002 to October 2003. Out of these 46 were ACS patients who un-derwent emergency coronary angiography and were taken up for emer-gency surgical revascularisation. 6 of these patients had STEMI, 12 had NSTEMI, and the rest had unstable angina. 2 patients were referred to us for CABG after failed PTCA elsewhere. They were taken up on the second and third day post acute MI respectively.The patient age varied from 38 years to 76 years. 38 were males and 8 were females. All patients were diagnosed based on their ECG, Cardiac enzyme levels and trans-thoracic echocardiography. 2 patients had severe LV dysfunc-tion, 6 had moderate LV dysfunction and the rest had adequate LV func-tion. Every effort was made to stabilize the patients medically, so as to give at least a week’s time for the myocardium to recover from the acute insult. 14 patients needed emergency CABG before a week of the acute event. CABG in all the 46 patients, irrespective of the LV function and the time from the acute event were performed on beating heart. 6 patients needed minimal pump support due to haemodynamic compromise while positioning the heart for OPCAB. We had no perioperative MI or operative mortality. Postoperative ventilation, ICU stay, bleeding, enzyme levels, inotropic support and hospital stay were comparable to elective surgeries. All patients have been followed up till date and are maintaining good health.
CONCLUSIONAcute coronary syndrome is no longer a contraindication for surgical re-vascularisation. Off pump coronary artery bypass has contributed much to the results of CABG in the acute setting by taking the pump-associated complications away. Antiplatelet drugs, which cannot be weaned off in patients in an acute setting, do not contribute to perioperative blood loss in OPCAB patients, questioning the actual need for stopping antiplatelet drugs even before elective OPCAB. The results of surgical revasculariza-tion are rewarding if surgery can be prolonged at least for 3 days after an acute cardiac event.
The choice of the device for valve replacement depends on a variety of factors like risk of re-infection, ease of insertion, durability, need for an-ticoagulation, adequacy of removal of infected tissue etc. A homograft is preferred to a mechanical device considering the reduced risk for re-infec-tion and need for anticoagulation. Valve repair rather than replacement may be considered in some cases of healed mitral valve endocarditis with small vegetations and in intravenous drug abusers with tricuspid valve endocarditis.
MANAGEMENT OF COMPLICATIONS OF INFECTIVE ENDOCARDITISSepsis, congestive cardiac failure, embolism, periannular spread, mycotic aneurysm and spread of infection to other organs are the common com-plications of infective endocarditis. Certain factors likeprosthetic cardiac valves, left-sided endocarditis, Staphylococcus aureus IE,fungal IE, previ-ous IE, prolonged clinical symptoms (≥3 months), cyanotic congenital heart disease, patients with systemic to pulmonary shunts and those with poor clinical response to antimicrobial therapy are recognized to carry a high risk for developing complications in a patient with infective endo-carditis
CONGESTIVECARDIACFAILURE(CCF): Congestive cardiac failure has the great-est impact on the prognosis of patients with infective endocarditis. Left sided endocarditis is more likely to develop CCF than right sided infective endocarditis. Aortic valve infective endocarditis is more likely to develop CCF (29%) than mitral valve (20%) or tricuspid valve (8%) infective endocarditis.Usually CCF develops insidiously with progressive worsening of valvular incompetence and ventricular dysfunction. CCF may also develop acutely as in acute rupture of chordae in mitral valve infective endocarditis, valve obstruction due to huge vegetation, prosthetic valve dehiscence, fistulae formation, valve leaflet perforation etc.CCF in infective endocarditis signifies a grave prognosis and is a predictor of poor outcome even after surgery.It is mandatory to operate on such patients at the earliest. Delay of sur-gery to extend preoperative antibiotic treatment carries with it the risk of permanent dysfunction. Class III or IV CCF has a very high risk for poor surgical outcome.
SYSTEMICEMBOLIZATION: occur in 22 to 50% of cases of infective endocar-ditis. About 60 to 65% of embolic events occur in the CNS; with more than 95% of these in the Middle Cerebral Artery territory. Arterial beds in the lungs, coronaries, spleen, bowel and extremities are also very much prone. Left sided valveinfective endocarditis is more prone to give rise to emboli. Infective endocarditis due to Staphylococccus aureus, Candida, Abiotrophia species and HACEK organisms are important causative fac-tors. Most emboli are noted with two full weeks of treatment and the risk weans off gradually. Left sided vegetation especially of the mitral valve
and more than 1cm in size are at increased risk. Mitral valve vegeta-tions, irrespective of the size are associated with higher rates of embolism (25%) than aortic valve vegetation (10%). Anterior leaflet vegetation of mitral valve is more prone for embolisation, as the leaflet excursion occurs twice per heartbeat. Size and number of vegetations, number of valves involved and characteristics and mobility of vegetation are other less significant risk factors.Surgery to prevent further embolization is indicated if there has been two or more major embolic events. The advantage of prevention of further emboli exists only when surgery is done early in the course of Infective Endocarditis, when embolic rates are highest. Surgery should be consid-ered when large vegetation is detected on the mitral valve, particularly the anterior mitral leaflet. If inspite of adequate therapy, vegetation is found not to diminish in size or if it is still unstable on trans-esophageal echocar-diography, the risk of embolization is high and surgery may be indicated.
PERIANNULARSPREADOF INFECTIVE ENDOCARDITIS
Annular infection can break through and spread into nearby tissues, lead-ing to periannular ascess, pseudo aneurysm, sinuses or fistulae. Perian-nular spread predicts high mortality, and early need for cardiac surgery. Periannular spread complicates 10 to 40% of Infective Endocarditis. Aortic valve infective endocarditis is more prone to periannular spread than mitral or tricuspid valve infection. In prosthetic valve infective endo-carditis, periannular spread occurrence is very high (50 to 100%) as the primary infection is in the annulus and not the leaflets.Persistent bacteremia or fever, recurrent emboli, heart block, CCF or changes in characteristics of a murmur in a patient who is being inad-equately treated for infective endocarditis suggests possibility of perian-nular spread. TEE is the investigation of choice to look for and assess periannular spread.Surgery at the earliest is mandatory and includes drainage of abscess cavities, excision of necrotic tissue and closure of communicating tracts; apart from replacement of the infected valves. Grossly damaged perian-nular supporting tissues need major reconstruction using homograft.
Off-Pump coronary artery bypass grafting avoids extra corporeal circula-tion and has shown to reduce the clinically relevant morbidity, especially with regard to neurologic complications. Manipulating the ascending aorta by side-clamping is a definite risk factor and VAO helps us to get rid of this.Surgeon’s skill is an important factor in performing proximal anastamoses with VAO. One advantage here is that we can perform either the proximal or the distal anastamosis first, an option that is not possible with the recently described sutureless anastomotic device [Calafiore 2001]. VAO device is made of steel, is reusable, and costs only US$ 10 to fab-ricate it. Side-clamping of the aorta can be avoided, and hence there is no need to bring down the systolic pressure below 100 mm Hg. There is no injury to the vein initima, because nothing is introduced into the vein. The suturing procedure takes not more than 10 minutes, and the learning curve is very short or negligible. VAO can also be used in calcified aortas if a small island of normal tissue is available. Our clinical results are excellent; we are now waiting of the one-year postoperative angiographic studies of our patients in this series, to confirm their long-term patency.
REFERENCES1. Calafiore AM, Barel Y, Vitolla G, 2001. Early clinical experience with a new sutureless anastomotic device for proximal anastamosis of the saphenous vein to the aorta. J Thorac Cardiovasc Surg 121:854-8. 2. Mohan R, Amsel BJ, Walter PJ.1992. Coronary artery bypass in the elderly: a review of studies on patients older than 64, 69 or 74 years. Cardiology 80:215-25. 3. Moshkovitz Y, Luski A, Mohr R.1995. Coronary artery bypass without cardiopulmonary bypass: analysis of short-term and mid-term outcome in 220 patients. J Thorac Cardiovasc Surg 110: 979-87.
The sutures in the vein have to be inside out, and in the aorta, they have to be outside in. The aortic sutures are placed so that the needle passes through the aortic wall, goes into the groove of the Obturator, and comes out between the aorta and the metal, thus taking the intima. The sutures are placed all around the aortic punch hole and are loosely held. Once the suturing is complete, the obturator is removed, and the left index finger is positioned on the aortic punch hole to prevent bleeding. The loose sutures are pulled and tightened with a nerve hook. The assistant holds the two ends of the sutures firmly with controlled traction during this procedure. Once all of the sutures are in place, the two ends are tied snugly. The two snares on the purse string are removed, and they are tied in place with care, so as to avoid a purse string effect.
RESULTSWe have performed 269 proximal anastomoses on 177 patients. Initially, most were performed with proximal anastamosis first so that the flow in the vein grafts could be fully assessed. But with experience, we now do distal anastamosis first. We have had no postoperative ischemia, or peri-operative infarction in any of our patients. We have had no perioperative mortality in our coronary patients. One patient presented with angina after 12 weeks, and check angiogram results showed a perfectly patent graft. We are planning to follow up these patients and to repeat coronary angiography after one year to assess the patencies of their grafts.
DISCUSSIONWith the present-day degree of myocardial protection and refinement in surgical technique, the mortality and morbidity of coronary artery surgery is related more to the co morbidities of patients than to cardiac function and the complexity of the surgical procedure [Mohan 1992].Avoiding cardiopulmonary bypass [Moshkovitz 1995] has further con-tributed to the reduction of mortality and morbidity in high-risk patients, such as those with post infarction angina and a low ejection fraction.
mimslouranlfinal.indd 37/21/2004 11:05:55 PM
16 - 2004
and tackled appropriately.
assess the efficacy of therapy instituted.
MEDICAL MANAGEMENT OF INFECTIVE ENDOCARDITIS
–
abusers and immunocompromised patients.
MEDICAL MANAGEMENT OF UNUSUALLY ENCOUNTERED MICROORGANISMS COAGULASE N S :
static distant organ seeding. This is susceptible to most antibiotics.
C :
/
minimum of three years.
BRUCELLA :
for 2 to 10 months after valve replacement
C A :
may be effective.
LEGIONELLA :
placement is needed only if there is valvar incompetence.
P
MIMS HEART JOURNAL JULY
About 5% of patients have “Culture Negative Endocarditis”, which usu-ally is due to inadvertent use of antibiotics prior to obtaining blood cul-ture samples (about 60%) or infection by pathogen difficult to isolate from blood culture. eg:- HACEK group, Bartonella species, a nutritionally variant streptococcus now classified as Abiotrophia species, Brucella spe-cies, Legionella species, Coxiella brunetti, Torpherema whipelli or fungi like Aspergillus which are never recovered from blood. These organisms need special methods and efforts from the microbiologist, to be traced
Echocardiography has an important role in diagnosing and assessing the severity of the disease and its complications, if any. Vegetation, abscess, new prosthetic valve dehiscence or new regurgitation are the four power-ful identifiers of infective endocarditis in the presence of other clinical parameters. Pathological consequences of infective endocarditis such as ventricular dysfunction,, ruptured chordae, shunts or fistulae may also be identified on echo. Echo may be useful in diagnosis of culture negative infective endocarditis or in the diagnosis of persistent bacteremia from an unidentified source. Trans Esophageal Echocardiography (TEE) has a much higher sensitivity and specificity than Transthoracic echocardiog-raphy (TTE) in diagnosing infective endocarditis. Moreover Transthoracic echocardiography alone cannot exclude prosthetic valve infection, peri-annular abscesses, fistula or leaflet perforation. All these are picked up better in Trans esophageal echocardiography. When both TTE and TEE are negative, the negative prediction value is about 95%. A repeat TEE in 7 to 10 days is needed in these patients labelled negative by Echo but with a high clinical suspicion of Infective Endocarditis. Follow-up Echo over the course and on completion of medical management is needed to
This is based on the invading organism. 80% of Infective Endocarditis are due to Streptococci and Staphylococci. Majority of native valve bacte-rial endocarditis is caused by Streptococci viridans (50%) and Staphy-lococcus aureus (20%). 80% of Tricuspid valve infection is caused by Staphylococcus aureus as this is more common in IV drug abusers. Staphylococcus aureus is a frequent cause of infective endocarditis in diabetes mellitus too. Early prosthetic valve endocarditis, defined as en-docarditis during the first two months after surgery is frequently caused by Staphylococcus epidermidis. Late onset prosthetic valve infective en-docarditis usually is caused by Streptococcus viridans and Staphylococci. Enterococcal endocarditis associated with malignancy or manipulation of gastrointestinal or genitourinary tract is usually caused by Enterococcus faecium (90%). The HACEK groups are an important group, which causes large vegetation (>1 cm), large vessel emboli and Congestive Cardiac Failure (CCF). Fungi are another group, which produces large vegeta-tions. Candida is a common cause for Infective Endocarditis in IV drug
EGATIVE TAPHYLOCOCCI Increasing number of coagulase neg-ative Staphylococci infective endocarditis is being reported. An important subset of these patients, with infection of Staphylococcus lugdunensis is being identified. This is more virulent than other forms of coagulase negative Staphylococci, has high risk of paravalvular spread and meta-
OXIELLA BRUNETTI The causative organism for Q fever usually affects prosthetic or previously damaged aortic or mitral valves. Infection is sub endothelial and vegetation is small and hence often missed. Doxycycline with Trimethoprim Sulphamethoxazole, Rifampicin or Fluoroquinolones is the mainstay of therapy. The organism may remain dormant in tis-sues for a long time and hence drugs may be needed life long or for a
This gram-negative bacillus which causes brucellosis can produce bulky vegetation on the previously damaged aortic and mitral valves followed commonly by valve destruction, perivalvar abscess and congestive heart failure. Doxycycline plus Streptomycin or Gentamicin or Trimethoprim /Sulphamethoxazole or Rifampicin is the drug of choice. Valve replacement is needed in most cases. Drugs should be continued
ANDIDA AND SPERGILLUS Cause majority of fungal Infective Endocardi-tis. Those with history of IV drug abuse, prosthetic valves replacements and long term central venous catheters are at high risk. Blood cultures are usually negative and vegetations bulky. Metastatic foci, perivalvar invasion and embolisation are common.Valve surgery is a must as Am-photericin B, the only fungicidal agent available and has poor penetra-tion into vegetation. Suppressive therapy with Imidazoles (Fluconazole)
Patients usually present with a long febrile illness, newly developed murmur and extremely high antibody titers. Most patients are prosthetic valve recipients. Embolism is rare. Parenteral Doxycycline or Erythromycin followed by prolonged oral therapy is effective. Valve re-
SEUDOMONAS AERUGINOSA causes Infective Endocarditis especially in IV drug abusers. Isolated right-sided Pseudomonas infective endocarditis can be medically managed with Piperacillin combined with an Aminoglycoside. Valve replacement is mandatory for left sided infective endocarditis.

20MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY05..
08 MIMS HEART JOURNAL - 2004 JULY
Postoperative care of cardiac surgery patient is as important as the intraoperative management. The cardiac anesthesiologist’s duty does not get over in the operation theater, but also continues in the postoperative period in the cardiac surgical ICU. In the ICU, the cardiac anaesthesiolo-gist closely monitors the vitals of the patient, achieves haemodynamic stability with appropriate use of inotropes or vasodilators, makes changes in the ventilator management as guided by the Arterial Blood Gas (ABG) reports and extubates the patient under optimal conditions. Hence his role as an intensivist. In contrast to the general surgical patient, the cardiac surgical patient requires continuation of the invasive and non-invasive monitoring for at least another 24 – 48 hours after the extubation. The cardiac anaesthe-siologist along with the cardiac surgeon continues the postoperative care, until the patient is safely transferred from the ICU to the ward.The current trend of coronary artery disease is taking a new turn with more and more younger age group of patients getting diffusely diseased pattern. Also post-infarction angina group patients are also taken up for surgery immediately after MI. Smoking from young age leads to badly affected lungs as evidenced by the less pul-monary reserve. These patients are prone for various complications and different strategies are needed to bring them out safely.POST INFARCT ANGINA PATIENTS
The patients who had recent MI presenting with post infarction angina will require an-giographic evaluation and further intervention in the form of either angioplasty or CABG. The ACC guidelines recommend that CABG can be done safely 72 hours after MI. These patients present with angina after MI. Their LV function is not optimal and wall motion abnormalities, common. The induction of anaesthesia is more likely to produce hypotension, which may spi-
INTENSIVE CARE MANAGEMENT AFTER CARDIAC SURGERY WHERE WE STAND TODAY
ral down to a cardiac arrest. Heart lung machine is kept ready and the surgical team gets ready before the induction of anaesthesia. Intraopera-tively these patients are more prone for the development of arrhythmias and reperfusion injury.After coronary angiogram, femoral arterial sheath is kept in situ. A femo-ral venous sheath is also kept ready for temporary pacing. A 4-lumen central venous catheter is introduced through the internal jugular vein either in the cath lab or in the coronary care unit. Once the patient ar-rives the OR, the arterial line is connected to the femoral sheath and inotropes are connected to the central line. Induction of anaesthesia is done with utmost care to avoid hypotension. Anaesthetic agents causing myocardial depression are avoided. Coronary artery bypass grafting is done on beating heart either without the use of heart lung machine or with CPB assistance.A pulmonary artery catheter with continuous cardiac output monitoring facility is used to guide the inotropes and vasopressors dosage. Intra aortic balloon pump will be required if the cardiac output remains low in spite of maximal inotropic therapy. Vasopressors are required if Systemic
vascular resistance (SVR) is low and the car-diac output is high with low arterial pressure. Urine output has to be monitored closely when vasopressors are used. A continuous infusion of furosemide is useful to reduce the Pulmo-nary vascular resistance (PVR) and to maintain good diuresis.We have operated on 46 patients with acute coronary syndrome with excellent results. Intra aortic balloon pump (IABP) was not required in any of these patients. Their cardiac output increased significantly in the postoperative period. Echocardiography done 1 week after the surgery showed significant improvement in LV function.
Dr. A.V. KannanChief Cardiac Anaesthesiologist
SURGICAL MANAGEMENT OF INFECTIVE ENDOCARDITISSurgery in patients with active native valve endocarditis is indicated in the presence of life threatening congestive heart failure or cardiogenic shock , embolic episodes, intractable arrythmias, progressive renal fail-ure, Staphylococcal or fungal endocarditis or uncontrolled sepsis, if the
patient has reasonable prospects of recovery with satisfactory quality of life after the operation. Surgery should not be delayed in the setting of Acute Infective Endocarditis when congestive heart failure intervenes. Surgery is not indicated if complications (severe embolic cerebral dam-age) or co-morbid conditions make the prospect of recovery remote. The indications for surgery for infective endocarditis in patients with stable haemodynamics are less clear. Surgical management of healed native valve endocarditis depends on the severity of the valvular lesion or the haemodynamic severity of the defect. Surgery is recommended in patients with annular or aortic ab-scesses, those with infections resistant to antibiotic therapy and those with fungal endocarditis. It is recognized that the presence of valvular vegetations poses a threat of embolic events. Echocardiography, espe-cially with transesophageal imaging, identifies vegetation and provides size estimation in many instances. Patients with a vegetation > 10 mm in diameter have a significantly higher incidence of embolization than those with a vegetation diameter < 10 mm, and this risk appears to be higher in patients with mitral valve endocarditis than aortic valve endocarditis. However, operation on the basis of vegetation size alone is controversial.Early prosthetic valve endocarditis patients need surgery if there is cardiac failure, valve obstruction due to vegetations or valve regurgitation or the causative organism is Staphylococcus. Late prosthetic valve endocarditis patients should be subjected to surgery if there is advanced heart failure or embolic episodes or continuing sepsis or if the offending organism is Staphylococcus. Patients with prosthetic valves receiving warfarin antico-agulation who develop endocarditis should have their warfarin discon-tinued and replaced with heparin. This recommendation is less related
to the possibility of haemorrhagic complications of endocarditis than the possibility of anticipating an urgent surgery. If surgery is required, the effects of warfarin will have dissipated and heparin can easily be re-versed. Likewise, aspirin, if part of the medical regimen, should also be discontinued. If neurological symptoms develop, anticoagulation should be discontinued until an intracranial haemorrhagic event is excluded by MRI or CT scanning.
RECOMMENDATIONS FOR SURGERY IN NATIVE VALVE ENDOCARDITIS
INDICATIONSAcute AR or MR with heart failure Acute AR with tachycardia and early closure of the mitral valve Fungal endocarditis Evidence of annular or aortic abscess, sinus or aortic true or false aneurysm Evidence of valve dysfunction and persistent infection after a prolonged period (7-10 days) of appropriate antibiotic therapy as indicated by presence of fever, leukocytosis and bacteremia, provided there are no non-cardiac causes forinfection Recurrent emboli after appropriate antibiotic therapy Infection with gram negative organisms or organisms with a poor response to antibiotics in patients with evidence of valve dysfunction Mobile vegetations > 10 mm
RECOMMENDATIONS FOR SURGERY IN PROSTHETIC VALVE ENDOCARDITIS
INDICATIONS Early prosthetic valve endocarditis (first two months or less after surgery) Heart failure with prosthetic valve dysfunction Fungal endocarditis Staphylococcal endocarditis not responding to antibiotic ther apy Evidence of paravalvular leak, annular or aortic abscess, sinus or aortic true or false aneurysm, fistula formation or new onset conduction disturbances Infection with gram negative organisms or organisms with poor response to antibiotics Persistent bacteremia after a prolonged course (7-10 days) of appropriate antibiotic therapy without non cardiac causes for bacteremia Recurrent peripheral embolus despite therapy
Ischaemic Heart Disease is the most common cause of death worldwide. Though the death rate for coronary artery disease has decreased over the past few decades, the incidence has remained constant or increased. Acute Coronary Syndrome (ACS) is a new term that encompasses many permutations of acute ischaemic heart disease. Patients who present with signs or symptoms of acute ischaemic heart disease are now described as having Acute Coronary Syndrome.
The first step in evaluation is an ECG, which allows acute coronary syn-drome to be broadly grouped into two, based on the presence or absence of ST segment elevation. Those with ST elevation are labeled Acute Myo-cardial Infarction or ST elevation myocardial infarction (STEMI) and are eligible for thrombolysis. Non-ST elevation ACS encompasses a broader range of entities including rest angina, new onset angina, unstable an-gina, post infarction angina, variant angina and Non-STEMI. The final diagnosis depends on serial ECG evaluation and blood tests for various cardiac markers. Grouping all these under one umbrella emphasizes the urgent nature of the problem and provides a starting point for a series of decision making that rapidly determine the optimal line of manage-ment.
Today Non ST elevation ACS accounts for majority of coronary care unit admissions. Although majority of ACS patients stabilize, in-hospital Myo-cardial Infarction occurs in >10% and a few die suddenly. Various stud-ies have reported death rates between 2.9 to 4 %, reinfarction rate of 5 to 12 % and stroke rate of 0.4% to 0.9 % in ACS patients.
Morbidity and mortality can be reduced either by strategies for prevention of an acute cardiac event or by improved management. Primary preven-tion aims at reducing the risk factors like cholesterol, tobacco etc. Second-ary prevention focuses on early detection and treatment of asymptomatic disease by screening ECGs, good diabetic control etc. Tertiary prevention is the treatment which alters the course of clinical disease like coronary angioplasty or CABG. However, even the best of preventive strategies will not eliminate coronary artery disease and patients do and will continue to present with ACS, leaving cost effective therapeutic intervention which provide good long term clinical outcome as the only option left.Management of ACS depends on the risk stratification of such patients. Those patients with probable ACS undergo detailed history, clinical ex-amination and ECG. Based on the risk to which they are exposed, pa-tients are grouped into low, intermediate and high-risk groups. Low risk patients are managed in the OP department. Those with intermediate risk are given acute intensive care, stabilized and worked up for further management. Those with high risk are considered for early reperfusion therapy.Patients with high risk include (i) men> 60 years and women > 70 years with definite angina (ii) haemodynamic or ECG changes with pain (iii) marked symmetrical T wave inversion in precordial leads (iv) ST seg-ment elevation or depression of > 1mm (v) variant anginaThose with intermediate risk include (i) Men< 60 years and women < 70 years with definite angina; or Men > 60 years and women > 70 years with probable angina; (ii) Diabetes with two other risk factors (smoking, hypertension, elevated cholesterol); (iii) probable non-anginal pain in diabetes, (iv) extracardiac vascular diseases, (v) ST depression
OPCAB FOR ACUTE CORONARY SYNDROMETHE WAY TO GO
Dr. Baburajan. A.KCardaic Surgeon
mimslouranlfinal.indd 77/21/2004 11:13:21 PM
- 2004 17.MIMS HEART JOURNAL JULY
ANTIBIOTIC REGIMEN FOR BACTERIAL ENDOCARDITIS – AHA GUIDELINES Native valve endocarditis involving penicillin susceptible Streptococcus viridans and Streptococcus bovis (Minimum Inhibitory Concentration < 0.1 microg/mL)
Antibiotic Dosage and Route Duration Comments Aqueous crystalline penicillin G sodium 12-18 million U/24 h IV either continu- 4 weeks Preferred in most patients > 65 y or ously or in 6 equally divided doses. and those with impairment of the
eighth nerve or renal function Ceftriaxone sodium 2g once daily IV or IM 4 weeks
Aqueous crystalline penicillin G sodium With
12-18 million U/24 h IV either continu-ously or in 6 equally divided doses.
2 weeks When obtained 1 h after a 20-30 min IV infusion or IM injection. Serum concentration of gentamycin
Gentamycin sulfate 1 mg/kg IM or IV every 8 h 2 weeks of approximately 3 micro g/mL, is desirable; though concentration should be <1microg/mL
Vancomycin hydrochloride 30 mg/kg per 24 h IV in 2 equally divided doses, not to exceed 2g/24 h unless serum levels are monitored
4 weeks Vancomycin therapy is recommended for patients allergic to beta lactams; peak serum concentration of vanco-mycin should be obtained 1 h after completion of infusion and should be in the range of 30-45microg/mL for twice daily dosing.
Native valve endocarditis involving Streptococcus viridans and Streptococcus bovis Relatively Resistant to Penicillin G (Minimum Inhibitory Concentration > 0.1 microg/mL and <0.5 microg/mL)
Antibiotic Dosage and Route Duration Comments
Aqueous crystalline penicillin G sodium 18 million U/24 h IV either continuously 4 weeks Preferred in most patients > 65 y and or in 6 equally divided doses those with impairment of the eighth nerve
With or renal function Gentamicin sulfate 1 mg/kg IM or IV every 8 h 2 weeks
Vancomycin hydrochloride 30 mg/kg per 24 h IV in 2 equally divided doses, not to exceed 2 g/24 h unless serum levels are monitored
4 weeks Vancomycin therapy is recommended for patients allergic to beta lactams.
06MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY19..
MIMS HEART JOURNAL - 2004 JULY 07.
AntibioticDosageandRouteDurationCommentsRegimenformethicillin-resistantstaphylococcis
Vancomycinhydrochloride
WithRifampicinandWithGentamycinsulphate
30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored300mgorallyevery8h1.0mg/kgIMorIVevery8h
≥6weeks
≥6weeks2weeks
Rifampicinincreasetheamountofwarfarinsodiumrequiredforantithrombotictherapy
Regimenformethicillin-susceptiblestaphylococci
NafcillinsodiumorOxacillinsodium
WithRifampicinandWithGentamycinsulphate
2gIVevery4h
300mgorallyevery8h1.0mg/kgIMorIVevery8h
≥6weeks
≥6weeks2weeks
First-generationcephalolosporinsorvanco-mycinshouldbeusedinpatientsallergictobeta-lactam.Cephalosporinsshouldbeavoidedinpatientswithimmediate-typehypersensitiv-itytopenicillinorwithmethicillin-resistantstaphylococci
EndocarditisduetostaphylococcusinthepresenceofaProstheticValveorotherProstheticMaterial.
AntibioticDosageandRouteDurationCommentsRegimenformethicillin-resistantstaphylococcis
Ceftriaxonesodium
Ampicillinsodium
Withgentamycinsulphate
2goncedailyIVorIM
12g/24hIVeithercontinuouslyorin6equallydivideddoses1mg/kgIMorIVevery8h
4weeks
4weeks
4weeks
Cefotaximesodiumorotherthird-generationcephalosporinsmaybesubstituted
TherapyforEndocarditisduetoHACEKmicroorganisms(Haemophilusparainflenzae,Haemophilusaphrophilus,actinobacillusactinomy-cetemcomitans,CardiobacteriumHominis,EikenellacorrodensandKingellakingae
AntibioticDosageandRouteDurationCommentsFungalEndocarditis
AmphotericinBwithorwithoutFlucytosine
1mg/kgperdayIV(totaldose2.0-2.5g)
150mg/kgperdayPOin4divideddoses
6-8weeks
6-8weeks
Culture-negativeEndocarditis
Vancomycinplusgentamycin
15mg/kgIVevery12h1mg/kgIMorIVevery8h
6weeks6weeks
FungalEndocarditisandCulture-NegativeEndocarditis
ARRHYTHMIAS Arrhythmias are common following cardiac surgery. Ventricular prema-ture contraction (VPC) is the most common arrhythmia and is usually due to hypokalemia. Following open heart surgery, the patients are prone for sodium retention and potassium excretion. In addition to this, diuretic therapy and insulin administration also lead to hypokalemia. These VPCs usually respond to potassium correction. When they persist even after the correction of potassium, 1-2 g of Magnesium is given over 30 min. Occasionally Xylocard infusion is required to control them.Atrial fibrillation is the second most common arrhythmia seen in our ICU. It is seen in about 8 % of our patients. The causes are hypoxemia, valve surgery, pneumothorax or haemothorax and preoperative AF. In-travenous infusion of amiodarone is our first line of management, which helps in achieving the sinus rhythm faster. In some patients, Digoxin and Magnesium sulphate are used along with Amiodarone. Rarely they need cardioversion.
VENTILATOR MANAGEMENTWe practice “FAST TRACKING” in most of the patients after cardiac sur-gery. When the patient comes to ICU, he will be on SIMV mode and continuous infusion of sedative is given. A warming blanket is used, if the patient is hypothermic. Once the patient becomes fully warm, hae-modynamically stable and mediastinal drainage is minimal, sedation is stopped. The awake patient is kept on pressure support ventilation for a short while and extubated. This process usually takes about 4 – 6 hours.If the patients are suspected to have pulmonary dysfunction or neurologi-cal dysfunction postoperatively, then they will be ventilated for a longer period. In case of acute lung injury (ALI) or adult respiratory distress syn-drome (ARDS), we use pressure-controlled ventilation to tide over the cri-sis along with aggressive diuretic therapy. Generally post cardiac surgical patients are prone for sodium and water retention and will require good dose of diuretics to drive fluid out of the interstitial space. Occasionally albumin therapy may be indicated.
HAEMODYNAMIC MONITORINGAll our patients have three channel ECG monitoring, invasive blood pres-sure monitoring, CVP monitoring, SpO2, ETCO2 and temperature moni-toring in the OT as well as in the ICU. When the patient is suspected to have low cardiac output syndrome, as seen by the requirement of high dose of inotropes, we resort to insertion of Swan Ganz catheter. A regu-lar pulmonary artery (PA) catheter gives systolic PA pressure, diastolic PA pressure and pulmonary capillary wedge pressure (PCWP). PCWP is indirectly indicative of left ventrcular end diastolic pressure (LVEDP). A thermodilution PA catheter is used to get more information like cardiac output, SVR and other derived parameters. We use a special PA catheter called ‘COMBO’ catheter, which gives continuous cardiac output. This is very useful in guiding us towards appropriate use of inotropes and va-sopressors. Intra Aortic Balloon Pump is used to augment the coronary blood flow and reduce the afterload of LV in necessary cases.
POSTOPERATIVE COAGULATION PROBLEMS In cardiac surgery, the coagulation system is the most affected one, after the heart. Every patient’s coagulation pathway is inhibited by the admin-istration of anticoagulant drug- heparin. When the patient is connected to cardiopulmonary bypass (CPB), blood is exposed to nonphysiological surfaces. CPB leads to platelet dysfunction in the postoperative period. If the patient is on anti-platelet drugs like aspirin or clopidogrel, the chance of postoperative bleeding due to inactive platelets is very high. With the recent development of off-pump (beating heart) coronary artery bypass grafting surgery, where heart lung machine is avoided, we ex-pect less coagulation problems. On the contrary, beating heart surgery leads to a procoagulant state and predisposes to the development of intra coronary thrombosis and graft occlusion in the immediate postoperative period. (This situation is analogous to the development of thrombosis in a coronary stent immediately after coronary angioplasty).The cardiac surgical ICU in MIMS has state of the art facilities1. Motorized patient beds2. Six channel modular monitors in each bed3. Modern ventilators 4. Facilities for Non-Invasive ventilation5. Vigilance monitor – continuous cardiac output monitoring6. PiCCO continuous cardiac output monitoring7. Syringe pumps for continuous infusion8. Arterial blood gas analyzer with electrolytes and haematocrit measurement 9. Intra Aortic Balloon Pump (IABP)This infrastructure of international standards is supported by a team of cardiac surgeons, cardiac anaesthesiologists and other personnel avail-able round the clock.PDCC in Cardiac Anaesthesia and Critical Care is a one year course start-ing from the academic year 2003.
Isolated Patent Ductus Arteriosus (PDA) is estimated to be present in one in 2000 term live births, accounting for about 5-10% of all types of Congenital Heart Diseases. The incidence in the preterm is higher.
Persistence of the ductus in the premature infant is due to physi-
ological developmental retardation. In the full-term infant, failure of the ductus to constrict postnatally is re-lated to a significant structural abnormality. The clinical features of Patent Ductus Arteriosus depend on the size of the communication, relationship between systemic and pulmonary vascular resistance and the ability of the myocardium to handle the extra volume load. INDICATION FOR CLOSUREPDA is an indication for closure; because of the risk of infective endo-carditis and the fact that the closure of PDA can be accomplished with virtually no risk. AGE AT CLOSURESpontaneous closure of PDA is unlikely beyond six months of age in term infants and 12 months of age in preterm infants. Such a cut-off is only arbitrary and closure is generally dictated by the clinical features conse-quent to the left to right shunt.Transcatheter closure has revolutionized management of PDA. In fact, PDA was the first lesion to be treated by transcatheter technique. The transcatheter closure has several advantages over surgical closure – less morbidity, absence of scar, comparable success rate and lack of anaes-thesia.
PROCEDUREThis is performed using conscious sedation in infants and young children, and local anaesthesia in older children and adults. Conscious sedation allows the child to return to full activity the following day. Closure can be accomplished with occluding coils or devices.A catheter is advanced from the femoral artery or the vein across the PDA. An occluding coil, made of stainless steel is placed in the PDA with a single coil loop on the pulmonary artery side and the remaining 3-4 loops in the ductal ampulla. Occasionally, multiple coils are required to achieve complete closure. The procedure success is 97% with no mortal-ity and no significant morbidity.The device we prefer is the Amplatzer Duct Occluder (ADO). This has
transformed percutaneous closure of large PDAs. The ADO is a self-expandable, highly elastic, mush-room shaped device, made from nitinol (Nickel-Titanium alloy) wire mesh. Dacron polyester fabric
sewn to the wire frame promotes thrombus formation The ADO has several desirable characteristics such as simplicity of use, ability to recapture and reposition the device, high (> 95%) complete closure rates and relatively small introducer sheath. Our patient age ranged from 1 year to 50 years and the size of the PDA from 2-6 mm. We prefer to deploy coils for small PDAs (<3mm) and the ADO for PDAs larger than 3mm. The procedural success has been 100% with no complications.As a matter of fact, with the introduction of the ADO, we have bid adieu to surgical closure for patent ductus arteriosus
TRANS CATHETER CLOSURE OF PATENTDUCTUS ARTERIOSUSWHERE WE STAND TODAY
Amplatzer Duct Occluder (ADO)
Coil closure of PDA
Dr. Asish Kumar.MCardiologist
mimslouranlfinal.indd 67/21/2004 11:11:40 PM
- 2004
tibiotic te ti ts
talli icilli i
With t i lfate
illi / I it til i ll ivi
/ I I
t f ti ts wit t t ti ; t f ti t ith
t t ti
icilli i
With t i l te
/ I it ti l ill ivi
/ I I
i l i
With t i l te
/ i ll ivit t / l
l l it
/ I I
in t i fti t ll ic t ta l t ; l
i t t l lt ti fti t ll ic t icillin
St f iti t t i
tibiotic te ti ts thicilli tibl t l i i f ta l t ll i ti ts
fcilli i illi i
Wit ti l iti f t i l te / I I
fit of iti l i l it t li
i f ta l t ll i ti ts
f lin ( t fi t ti l in in i l t )
Wit ti l iti f t in
I
/ I I
l i l i in ti t ith i iate t iti
ity t icillin)
i l i / IV i lly divi t t /
l l l it
f ti t ll ic to icillin
thicilli ist t st l i
i l i / IV i lly divi t t /
l l l it
iti t t l in t f t ti t ial
18 MIMS HEART JOURNAL JULY
An Dosage and Rou Dura on Commen
Aqueous crys ne pen n G sod um
Gen amyc n su
18-30 m on U 24 h V e her con nu-ous y or n 6 equa y d ded doses
1 mg kg M or V every 8 h
4-6 weeks
4-6 weeks
4-wk herapy recommended or pa enh symp oms <3 mon hs dura on 6-wk
herapy recommended or pa en s wsymp oms >3 mon h dura on
Amp n sod um
Gen amyc n su pha
12g 24 h V e her con nuous y or n 6 equa y d ded doses
1mg kg M or V every 8 h
4-6 weeks
4-6 weeks
Vancomyc n hydroch or de
Gen amyc n su pha
30 mg kg per 24 h n 2 equa y d ded doses, no o exceed 2g 24 h un ess serum eve s are mon ored
1 mg kg M or V every 8 h
4-6 weeks
4 weeks
Vancomyc herapy s recommended or pa en s a erg o be ac ams cepha o-spor ns are no accep ab e a erna ves or pa en s a erg o pen
andard Therapy or Endocard s Due o En erococc
An Dosage and Rou Dura on CommenMe n suscep e s aphy ococcReg men or non-be ac am a erg c pa en
Na n sod um or Oxac n sod um
h op ona add on o Gen amyc n su pha
2 g every 4 h
1 mg kg M or V every 8 h
4-6 weeks
3-5 d
Bene add ona am nog ycos des has no been es ab shed
Reg men or be ac am a erg c pa en
Ce azo or o her rs genera on cepha osporequ va en dosages
h op ma add on o Gen amyc
2 g V every 8 h
1 mg kg M or V every 8 h
4-6 weeks
3-5 d
Cepha ospor ns shou d be avo ded pa en s w mmed ype hypersens v-
o pen
Vancomyc n hydroch or de 30mg kg per 24 h n 2 equaded doses, no o exceed 2g 24 h
un ess serum eve s are mon ored
4-6 weeks Recommended or pa en s a ergpen
Me n-res an aphy ococc
Vancomyc n hydroch or de 30mg kg per 24 h n 2 equaded doses, no o exceed 2g 24 h
un ess serum eve s are mon ored
4-6 weeks
Endocard s due o s aphy ococcus he absence o Pros he c Ma er

06 MIMS HEART JOURNAL - 2004 JULY
18 MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY07.
ARRHYTHMIAS Arrhythmias are common following cardiac surgery. Ventricular prema-ture contraction (VPC) is the most common arrhythmia and is usually due to hypokalemia. Following open heart surgery, the patients are prone for sodium retention and potassium excretion. In addition to this, diuretic therapy and insulin administration also lead to hypokalemia. These VPCs usually respond to potassium correction. When they persist even after the correction of potassium, 1-2 g of Magnesium is given over 30 min. Occasionally Xylocard infusion is required to control them.Atrial fibrillation is the second most common arrhythmia seen in our ICU. It is seen in about 8 % of our patients. The causes are hypoxemia, valve surgery, pneumothorax or haemothorax and preoperative AF. In-travenous infusion of amiodarone is our first line of management, which helps in achieving the sinus rhythm faster. In some patients, Digoxin and Magnesium sulphate are used along with Amiodarone. Rarely they need cardioversion.
VENTILATOR MANAGEMENTWe practice “FAST TRACKING” in most of the patients after cardiac sur-gery. When the patient comes to ICU, he will be on SIMV mode and continuous infusion of sedative is given. A warming blanket is used, if the patient is hypothermic. Once the patient becomes fully warm, hae-modynamically stable and mediastinal drainage is minimal, sedation is stopped. The awake patient is kept on pressure support ventilation for a short while and extubated. This process usually takes about 4 – 6 hours.If the patients are suspected to have pulmonary dysfunction or neurologi-cal dysfunction postoperatively, then they will be ventilated for a longer period. In case of acute lung injury (ALI) or adult respiratory distress syn-drome (ARDS), we use pressure-controlled ventilation to tide over the cri-sis along with aggressive diuretic therapy. Generally post cardiac surgical patients are prone for sodium and water retention and will require good dose of diuretics to drive fluid out of the interstitial space. Occasionally albumin therapy may be indicated.
HAEMODYNAMIC MONITORINGAll our patients have three channel ECG monitoring, invasive blood pres-sure monitoring, CVP monitoring, SpO2, ETCO2 and temperature moni-toring in the OT as well as in the ICU. When the patient is suspected to have low cardiac output syndrome, as seen by the requirement of high dose of inotropes, we resort to insertion of Swan Ganz catheter. A regu-lar pulmonary artery (PA) catheter gives systolic PA pressure, diastolic PA pressure and pulmonary capillary wedge pressure (PCWP). PCWP is indirectly indicative of left ventrcular end diastolic pressure (LVEDP). A thermodilution PA catheter is used to get more information like cardiac output, SVR and other derived parameters. We use a special PA catheter called ‘COMBO’ catheter, which gives continuous cardiac output. This is very useful in guiding us towards appropriate use of inotropes and va-sopressors. Intra Aortic Balloon Pump is used to augment the coronary blood flow and reduce the afterload of LV in necessary cases.
POSTOPERATIVE COAGULATION PROBLEMS In cardiac surgery, the coagulation system is the most affected one, after the heart. Every patient’s coagulation pathway is inhibited by the admin-istration of anticoagulant drug- heparin. When the patient is connected to cardiopulmonary bypass (CPB), blood is exposed to nonphysiological surfaces. CPB leads to platelet dysfunction in the postoperative period. If the patient is on anti-platelet drugs like aspirin or clopidogrel, the chance of postoperative bleeding due to inactive platelets is very high. With the recent development of off-pump (beating heart) coronary artery bypass grafting surgery, where heart lung machine is avoided, we ex-pect less coagulation problems. On the contrary, beating heart surgery leads to a procoagulant state and predisposes to the development of intra coronary thrombosis and graft occlusion in the immediate postoperative period. (This situation is analogous to the development of thrombosis in a coronary stent immediately after coronary angioplasty).The cardiac surgical ICU in MIMS has state of the art facilities1. Motorized patient beds2. Six channel modular monitors in each bed3. Modern ventilators 4. Facilities for Non-Invasive ventilation5. Vigilance monitor – continuous cardiac output monitoring6. PiCCO continuous cardiac output monitoring7. Syringe pumps for continuous infusion8. Arterial blood gas analyzer with electrolytes and haematocrit measurement 9. Intra Aortic Balloon Pump (IABP)This infrastructure of international standards is supported by a team of cardiac surgeons, cardiac anaesthesiologists and other personnel avail-able round the clock.PDCC in Cardiac Anaesthesia and Critical Care is a one year course start-ing from the academic year 2003.
Isolated Patent Ductus Arteriosus (PDA) is estimated to be present in one in 2000 term live births, accounting for about 5-10% of all types of Congenital Heart Diseases. The incidence in the preterm is higher.
Persistence of the ductus in the premature infant is due to physi-
ological developmental retardation. In the full-term infant, failure of the ductus to constrict postnatally is re-lated to a significant structural abnormality. The clinical features of Patent Ductus Arteriosus depend on the size of the communication, relationship between systemic and pulmonary vascular resistance and the ability of the myocardium to handle the extra volume load. INDICATION FOR CLOSUREPDA is an indication for closure; because of the risk of infective endo-carditis and the fact that the closure of PDA can be accomplished with virtually no risk. AGE AT CLOSURESpontaneous closure of PDA is unlikely beyond six months of age in term infants and 12 months of age in preterm infants. Such a cut-off is only arbitrary and closure is generally dictated by the clinical features conse-quent to the left to right shunt.Transcatheter closure has revolutionized management of PDA. In fact, PDA was the first lesion to be treated by transcatheter technique. The transcatheter closure has several advantages over surgical closure – less morbidity, absence of scar, comparable success rate and lack of anaes-thesia.
PROCEDUREThis is performed using conscious sedation in infants and young children, and local anaesthesia in older children and adults. Conscious sedation allows the child to return to full activity the following day. Closure can be accomplished with occluding coils or devices.A catheter is advanced from the femoral artery or the vein across the PDA. An occluding coil, made of stainless steel is placed in the PDA with a single coil loop on the pulmonary artery side and the remaining 3-4 loops in the ductal ampulla. Occasionally, multiple coils are required to achieve complete closure. The procedure success is 97% with no mortal-ity and no significant morbidity.The device we prefer is the Amplatzer Duct Occluder (ADO). This has
transformed percutaneous closure of large PDAs. The ADO is a self-expandable, highly elastic, mush-room shaped device, made from nitinol (Nickel-Titanium alloy) wire mesh. Dacron polyester fabric
sewn to the wire frame promotes thrombus formation The ADO has several desirable characteristics such as simplicity of use, ability to recapture and reposition the device, high (> 95%) complete closure rates and relatively small introducer sheath. Our patient age ranged from 1 year to 50 years and the size of the PDA from 2-6 mm. We prefer to deploy coils for small PDAs (<3mm) and the ADO for PDAs larger than 3mm. The procedural success has been 100% with no complications.As a matter of fact, with the introduction of the ADO, we have bid adieu to surgical closure for patent ductus arteriosus
TRANS CATHETER CLOSURE OF PATENTDUCTUS ARTERIOSUS WHERE WE STAND TODAY
Amplatzer Duct Occluder (ADO)
Coil closure of PDA
Dr. Asish Kumar.MCardiologist
AntibioticDosageandRouteDurationComments
AqueouscrystallinepenicillinGsodium
WithGentamycinsulfate
18-30millionU/24hIVeithercontinu-ouslyorin6equallydivideddoses
1mg/kgIMorIVevery8h
4-6weeks
4-6weeks
4-wktherapyrecommendedforpatientswithsymptoms<3monthsduration;6-wktherapyrecommendedforpatientswithsymptoms>3monthduration
Ampicillinsodium
WithGentamycinsulphate
12g/24hIVeithercontinuouslyorin6equallydivideddoses
1mg/kgIMorIVevery8h
4-6weeks
4-6weeks
Vancomycinhydrochloride
WithGentamycinsulphate
30mg/kgper24hin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
1mg/kgIMorIVevery8h
4-6weeks
4weeks
Vancomycintherapyisrecommendedforpatientsallergictobetalactams;cephalo-sporinsarenotacceptablealternativesforpatientsallergictopenicillin
StandardTherapyforEndocarditisDuetoEnterococci
AntibioticDosageandRouteDurationCommentsMethicillinsusceptiblestaphylococciRegimenfornon-betalactamallergicpatients
NafcillinsodiumorOxacillinsodium
WithoptionaladditionofGentamycinsulphate
2gevery4h
1mg/kgIMorIVevery8h
4-6weeks
3-5d
Benefitofadditionalaminoglycosideshasnotbeenestablished
Regimenforbetalactamallergicpatients
Cefazolin(orotherfirstgenerationcephalosporininequivalentdosages)
WithoptimaladditionofGentamycin
2gIVevery8h
1mg/kgIMorIVevery8h
4-6weeks
3-5d
Cephalosporinsshouldbeavoidedinpatientswithimmediatetypehypersensitiv-itytopenicillin)
Vancomycinhydrochloride30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
4-6weeksRecommendedforpatientsallergictopenicillin
Methicillin-resistantstaphylococci
Vancomycinhydrochloride30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
4-6weeks
EndocarditisduetostaphylococcusintheabsenceofProstheticMaterial
mimslouranlfinal.indd 6 7/21/2004 11:11:40 PM
- 2004 19
tibiotic te ti ts i f thicilli ist t st l is
i l i
Wit if iciWit t i l te
/ IV i lly divi t t /
l l l itll
/ I IRif icin i t t of f in
i i f tit tic t
i f thicilli tibl t l i
fcilli i illi i
Wit if iciWit t i l te
I
ll/ I I
Fi t ti lol ii l i ti t ll ic to
t l tl i l i in
ti t ith i iat t itiity t icilli it thicilli ist t st l i
iti t t l in t f t ti l t t i t ial.
tibiotic te ti ts i f thicilli ist t st l is
ftri i
icilli i
Wit t i l te
ily I IM
/ I it ti l ill ivi/ I I
fot i i t thi til i titut
f iti t i i ( il infl il il ti ill tit i i t i ini i ll i ll i
tibiotic te ti ts l itis
t iciwit it t Fl t i
/ IV (total )
/ i ivi
lt ti itis
i lt in
/ I/ I I
l iti lt ti itis
MIMS HEART JOURNAL JULY ..
An Dosage and Rou Dura on CommenReg men or me n-res an aphy ococc
Vancomyc n hydroch or de
h R amp n and h Gen amyc n su pha
30mg kg per 24 h n 2 equaded doses, no o exceed 2g 24 h
un ess serum eve s are mon ored 300 mg ora y every 8 h 1.0 mg kg M or V every 8 h
≥ 6 weeks
≥ 6 weeks 2 weeks
amp ncrease he amoun war arsod um requ red or an hrombo herapy
Reg men or me n-suscep e s aphy ococc
Na n sod um or Oxac n sod um
h R amp n and h Gen amyc n su pha
2 g V every 4 h
300 mg ora y every 8 h 1.0 mg kg M or V every 8 h
≥ 6 weeks
≥ 6 weeks 2 weeks
rs -genera on cepha ospor ns or vanco-myc n shou d be used n pa en s a ergbe a- ac am. Cepha ospor ns shou d be avo ded pa en s w mmed e- ype hypersens v-
o pen n or w h me n-res anaphy ococc
Endocard s due o s aphy ococcus he presence o a Pros he c Va ve or o her Pros het c Ma er
An Dosage and Rou Dura on CommenReg men or me n-res an aphy ococc
Ce axone sod um
Amp n sod um
h gen amyc n su pha
2 g once da V or
12 g 24 h V e her con nuous y or n 6 equa y d ded doses 1 mg kg M or V every 8 h
4 weeks
4 weeks
4 weeks
Ce ax me sod um or o her rd-genera on cepha ospor ns may be subs ed
Therapy or Endocard s due o HACEK m croorgan sms Haemoph us para enzae, Haemoph us aphroph us, ac nobac us ac nomy-ce emcom tans, Card obac er um Hom s, E kene a corrodens and K nge a k ngae
An Dosage and Rou Dura on CommenFunga Endocard
Ampho er n B h or w hou
ucy os ne
1 mg kg per day dose 2.0-2.5 g
150 mg kg per day PO n 4 d ded doses
6-8 weeks
6-8 weeks
Cu ure-nega ve Endocard
Vancomyc n p us gen amyc
15 mg kg V every 12 h 1 mg kg M or V every 8 h
6 weeks 6 weeks
Funga Endocard s and Cu ure-Nega ve Endocard

MIMS HEART JOURNAL - 2004 JULY 05..
08MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY17.
Postoperative care of cardiac surgery patient is as important as the intraoperative management. The cardiac anesthesiologist’s duty does not get over in the operation theater, but also continues in the postoperative period in the cardiac surgical ICU. In the ICU, the cardiac anaesthesiolo-gist closely monitors the vitals of the patient, achieves haemodynamic stability with appropriate use of inotropes or vasodilators, makes changes in the ventilator management as guided by the Arterial Blood Gas (ABG) reports and extubates the patient under optimal conditions. Hence his role as an intensivist. In contrast to the general surgical patient, the cardiac surgical patient requires continuation of the invasive and non-invasive monitoring for at least another 24 – 48 hours after the extubation. The cardiac anaesthe-siologist along with the cardiac surgeon continues the postoperative care, until the patient is safely transferred from the ICU to the ward.The current trend of coronary artery disease is taking a new turn with more and more younger age group of patients getting diffusely diseased pattern. Also post-infarction angina group patients are also taken up for surgery immediately after MI. Smoking from young age leads to badly affected lungs as evidenced by the less pul-monary reserve. These patients are prone for various complications and different strategies are needed to bring them out safely.POST INFARCT ANGINA PATIENTS
The patients who had recent MI presenting with post infarction angina will require an-giographic evaluation and further intervention in the form of either angioplasty or CABG. The ACC guidelines recommend that CABG can be done safely 72 hours after MI. These patients present with angina after MI. Their LV function is not optimal and wall motion abnormalities, common. The induction of anaesthesia is more likely to produce hypotension, which may spi-
INTENSIVE CARE MANAGEMENT AFTER CARDIAC SURGERYWHERE WE STAND TODAY
ral down to a cardiac arrest. Heart lung machine is kept ready and the surgical team gets ready before the induction of anaesthesia. Intraopera-tively these patients are more prone for the development of arrhythmias and reperfusion injury.After coronary angiogram, femoral arterial sheath is kept in situ. A femo-ral venous sheath is also kept ready for temporary pacing. A 4-lumen central venous catheter is introduced through the internal jugular vein either in the cath lab or in the coronary care unit. Once the patient ar-rives the OR, the arterial line is connected to the femoral sheath and inotropes are connected to the central line. Induction of anaesthesia is done with utmost care to avoid hypotension. Anaesthetic agents causing myocardial depression are avoided. Coronary artery bypass grafting is done on beating heart either without the use of heart lung machine or with CPB assistance.A pulmonary artery catheter with continuous cardiac output monitoring facility is used to guide the inotropes and vasopressors dosage. Intra aortic balloon pump will be required if the cardiac output remains low in spite of maximal inotropic therapy. Vasopressors are required if Systemic
vascular resistance (SVR) is low and the car-diac output is high with low arterial pressure. Urine output has to be monitored closely when vasopressors are used. A continuous infusion of furosemide is useful to reduce the Pulmo-nary vascular resistance (PVR) and to maintain good diuresis.We have operated on 46 patients with acute coronary syndrome with excellent results. Intra aortic balloon pump (IABP) was not required in any of these patients. Their cardiac output increased significantly in the postoperative period. Echocardiography done 1 week after the surgery showed significant improvement in LV function.
Dr. A.V. KannanChief Cardiac Anaesthesiologist
AntibioticDosageandRouteDurationCommentsAqueouscrystallinepenicillinGsodiumor
Ceftriaxonesodium
12-18millionU/24hIVeithercontinu-ouslyorin6equallydivideddoses.
2goncedailyIVorIM
4weeks
4weeks
Preferredinmostpatients>65yandthosewithimpairmentoftheeighthnerveorrenalfunction
AqueouscrystallinepenicillinGsodiumWith
Gentamycinsulfate
12-18millionU/24hIVeithercontinu-ouslyorin6equallydivideddoses.
1mg/kgIMorIVevery8h
2weeks
2weeks
Whenobtained1haftera20-30minIVinfusionorIMinjection.Serumconcentrationofgentamycinofapproximately3microg/mL,isdesirable;thoughconcentrationshouldbe<1microg/mL
Vancomycinhydrochloride30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
4weeksVancomycintherapyisrecommendedforpatientsallergictobetalactams;peakserumconcentrationofvanco-mycinshouldbeobtained1haftercompletionofinfusionandshouldbeintherangeof30-45microg/mLfortwicedailydosing.
ANTIBIOTICREGIMENFORBACTERIALENDOCARDITIS–AHAGUIDELINESNativevalveendocarditisinvolvingpenicillinsusceptibleStreptococcusviridansandStreptococcusbovis(MinimumInhibitoryConcentration<0.1microg/mL)
AntibioticDosageandRouteDurationComments
AqueouscrystallinepenicillinGsodium
WithGentamicinsulfate
18millionU/24hIVeithercontinuouslyorin6equallydivideddoses
1mg/kgIMorIVevery8h
4weeks
2weeks
Preferredinmostpatients>65yandthosewithimpairmentoftheeighthnerveorrenalfunction
Vancomycinhydrochloride30mg/kgper24hIVin2equallydivideddoses,nottoexceed2g/24hunlessserumlevelsaremonitored
4weeksVancomycintherapyisrecommendedforpatientsallergictobetalactams.
NativevalveendocarditisinvolvingStreptococcusviridansandStreptococcusbovisRelativelyResistanttoPenicillinG(MinimumInhibitoryConcentration>0.1microg/mLand<0.5microg/mL)
Ischaemic Heart Disease is the most common cause of death worldwide. Though the death rate for coronary artery disease has decreased over the past few decades, the incidence has remained constant or increased. Acute Coronary Syndrome (ACS) is a new term that encompasses many permutations of acute ischaemic heart disease. Patients who present with signs or symptoms of acute ischaemic heart disease are now described as having Acute Coronary Syndrome.
The first step in evaluation is an ECG, which allows acute coronary syn-drome to be broadly grouped into two, based on the presence or absence of ST segment elevation. Those with ST elevation are labeled Acute Myo-cardial Infarction or ST elevation myocardial infarction (STEMI) and are eligible for thrombolysis. Non-ST elevation ACS encompasses a broader range of entities including rest angina, new onset angina, unstable an-gina, post infarction angina, variant angina and Non-STEMI. The final diagnosis depends on serial ECG evaluation and blood tests for various cardiac markers. Grouping all these under one umbrella emphasizes the urgent nature of the problem and provides a starting point for a series of decision making that rapidly determine the optimal line of manage-ment.
Today Non ST elevation ACS accounts for majority of coronary care unit admissions. Although majority of ACS patients stabilize, in-hospital Myo-cardial Infarction occurs in >10% and a few die suddenly. Various stud-ies have reported death rates between 2.9 to 4 %, reinfarction rate of 5 to 12 % and stroke rate of 0.4% to 0.9 % in ACS patients.
Morbidity and mortality can be reduced either by strategies for prevention of an acute cardiac event or by improved management. Primary preven-tion aims at reducing the risk factors like cholesterol, tobacco etc. Second-ary prevention focuses on early detection and treatment of asymptomatic disease by screening ECGs, good diabetic control etc. Tertiary prevention is the treatment which alters the course of clinical disease like coronary angioplasty or CABG. However, even the best of preventive strategies will not eliminate coronary artery disease and patients do and will continue to present with ACS, leaving cost effective therapeutic intervention which provide good long term clinical outcome as the only option left.Management of ACS depends on the risk stratification of such patients. Those patients with probable ACS undergo detailed history, clinical ex-amination and ECG. Based on the risk to which they are exposed, pa-tients are grouped into low, intermediate and high-risk groups. Low risk patients are managed in the OP department. Those with intermediate risk are given acute intensive care, stabilized and worked up for further management. Those with high risk are considered for early reperfusion therapy.Patients with high risk include (i) men> 60 years and women > 70 years with definite angina (ii) haemodynamic or ECG changes with pain (iii) marked symmetrical T wave inversion in precordial leads (iv) ST seg-ment elevation or depression of > 1mm (v) variant anginaThose with intermediate risk include (i) Men< 60 years and women < 70 years with definite angina; or Men > 60 years and women > 70 years with probable angina; (ii) Diabetes with two other risk factors (smoking, hypertension, elevated cholesterol); (iii) probable non-anginal pain in diabetes, (iv) extracardiac vascular diseases, (v) ST depression
OPCAB FOR ACUTE CORONARY SYNDROMETHE WAY TO GO
Dr. Baburajan. A.KCardaic Surgeon
mimslouranlfinal.indd 7 7/21/2004 11:13:21 PM
20 - 2004
SURGICAL MANAGEMENT OF INFECTIVE ENDOCARDITIS
haemodynamics are less clear.
controversial.
MRI or CT scanning.
RECOMMENDATIONS FOR SURGERY IN NATIVE VALVE ENDOCARDITIS
INDICATIONS
Fungal endocarditis Evidence of annular or aortic abscess, sinus or aortic true or false aneurysm Evidence of valve dysfunction and persistent infection after a prolonged period (7-10 days) of appropriate antibiotic therapy as indicated by presence of fever, leukocytosis and bacteremia, provided there are no non-cardiac causes for infection Recurrent emboli after appropriate antibiotic therapy Infection with gram negative organisms or organisms with a poor response to antibiotics in patients with evidence of valve dysfunction Mobile vegetations > 10 mm
RECOMMENDATIONS FOR SURGERY IN PROSTHETIC VALVE ENDOCARDITIS
INDICATIONS Early prosthetic valve endocarditis (first two months or less after surgery) Heart failure with prosthetic valve dysfunction Fungal endocarditis Staphylococcal endocarditis not responding to antibiotic ther apy
sinus or aortic true or false aneurysm, fistula formation or new onset conduction disturbances Infection with gram negative organisms or organisms with poor response to antibiotics
of appropriate antibiotic therapy without non cardiac causes for bacteremia Recurrent peripheral embolus despite therapy
MIMS HEART JOURNAL JULY
Surgery in patients with active native valve endocarditis is indicated in the presence of life threatening congestive heart failure or cardiogenic shock , embolic episodes, intractable arrythmias, progressive renal fail-ure, Staphylococcal or fungal endocarditis or uncontrolled sepsis, if the
patient has reasonable prospects of recovery with satisfactory quality of life after the operation. Surgery should not be delayed in the setting of Acute Infective Endocarditis when congestive heart failure intervenes. Surgery is not indicated if complications (severe embolic cerebral dam-age) or co-morbid conditions make the prospect of recovery remote. The indications for surgery for infective endocarditis in patients with stable
Surgical management of healed native valve endocarditis depends on the severity of the valvular lesion or the haemodynamic severity of the defect. Surgery is recommended in patients with annular or aortic ab-scesses, those with infections resistant to antibiotic therapy and those with fungal endocarditis. It is recognized that the presence of valvular vegetations poses a threat of embolic events. Echocardiography, espe-cially with transesophageal imaging, identifies vegetation and provides size estimation in many instances. Patients with a vegetation > 10 mm in diameter have a significantly higher incidence of embolization than those with a vegetation diameter < 10 mm, and this risk appears to be higher in patients with mitral valve endocarditis than aortic valve endocarditis. However, operation on the basis of vegetation size alone is
Early prosthetic valve endocarditis patients need surgery if there is cardiac failure, valve obstruction due to vegetations or valve regurgitation or the causative organism is Staphylococcus. Late prosthetic valve endocarditis patients should be subjected to surgery if there is advanced heart failure or embolic episodes or continuing sepsis or if the offending organism is Staphylococcus. Patients with prosthetic valves receiving warfarin antico-agulation who develop endocarditis should have their warfarin discon-tinued and replaced with heparin. This recommendation is less related
to the possibility of haemorrhagic complications of endocarditis than the possibility of anticipating an urgent surgery. If surgery is required, the effects of warfarin will have dissipated and heparin can easily be re-versed. Likewise, aspirin, if part of the medical regimen, should also be discontinued. If neurological symptoms develop, anticoagulation should be discontinued until an intracranial haemorrhagic event is excluded by
Acute AR or MR with heart failure Acute AR with tachycardia and early closure of the mitral valve
Evidence of paravalvular leak, annular or aortic abscess,
Persistent bacteremia after a prolonged course (7-10 days)

04 MIMS HEART JOURNAL - 2004 JULY
16MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY09..
About 5% of patients have “Culture Negative Endocarditis”, which usu-ally is due to inadvertent use of antibiotics prior to obtaining blood cul-ture samples (about 60%) or infection by pathogen difficult to isolate from blood culture. eg:- HACEK group, Bartonella species, a nutritionally variant streptococcus now classified as Abiotrophia species, Brucella spe-cies, Legionella species, Coxiella brunetti, Torpherema whipelli or fungi like Aspergillus which are never recovered from blood. These organisms need special methods and efforts from the microbiologist, to be traced and tackled appropriately.Echocardiography has an important role in diagnosing and assessing the severity of the disease and its complications, if any. Vegetation, abscess, new prosthetic valve dehiscence or new regurgitation are the four power-ful identifiers of infective endocarditis in the presence of other clinical parameters. Pathological consequences of infective endocarditis such as ventricular dysfunction,, ruptured chordae, shunts or fistulae may also be identified on echo. Echo may be useful in diagnosis of culture negative infective endocarditis or in the diagnosis of persistent bacteremia from an unidentified source. Trans Esophageal Echocardiography (TEE) has a much higher sensitivity and specificity than Transthoracic echocardiog-raphy (TTE) in diagnosing infective endocarditis. Moreover Transthoracic echocardiography alone cannot exclude prosthetic valve infection, peri-annular abscesses, fistula or leaflet perforation. All these are picked up better in Trans esophageal echocardiography. When both TTE and TEE are negative, the negative prediction value is about 95%. A repeat TEE in 7 to 10 days is needed in these patients labelled negative by Echo but with a high clinical suspicion of Infective Endocarditis. Follow-up Echo over the course and on completion of medical management is needed to assess the efficacy of therapy instituted.
MEDICAL MANAGEMENT OF INFECTIVE ENDOCARDITISThis is based on the invading organism. 80% of Infective Endocarditis are due to Streptococci and Staphylococci. Majority of native valve bacte-rial endocarditis is caused by Streptococci viridans (50%) and Staphy-lococcus aureus (20%). 80% of Tricuspid valve infection is caused by Staphylococcus aureus – as this is more common in IV drug abusers. Staphylococcus aureus is a frequent cause of infective endocarditis in diabetes mellitus too. Early prosthetic valve endocarditis, defined as en-docarditis during the first two months after surgery is frequently caused by Staphylococcus epidermidis. Late onset prosthetic valve infective en-docarditis usually is caused by Streptococcus viridans and Staphylococci. Enterococcal endocarditis associated with malignancy or manipulation of gastrointestinal or genitourinary tract is usually caused by Enterococcus faecium (90%). The HACEK groups are an important group, which causes large vegetation (>1 cm), large vessel emboli and Congestive Cardiac Failure (CCF). Fungi are another group, which produces large vegeta-tions. Candida is a common cause for Infective Endocarditis in IV drug
abusers and immunocompromised patients.
MEDICAL MANAGEMENT OF UNUSUALLY ENCOUNTERED MICROORGANISMSCOAGULASENEGATIVESTAPHYLOCOCCI: Increasing number of coagulase neg-ative Staphylococci infective endocarditis is being reported. An important subset of these patients, with infection of Staphylococcus lugdunensis is being identified. This is more virulent than other forms of coagulase negative Staphylococci, has high risk of paravalvular spread and meta-static distant organ seeding. This is susceptible to most antibiotics.
COXIELLABRUNETTI: The causative organism for Q fever usually affects prosthetic or previously damaged aortic or mitral valves. Infection is sub endothelial and vegetation is small and hence often missed. Doxycycline with Trimethoprim / Sulphamethoxazole, Rifampicin or Fluoroquinolones is the mainstay of therapy. The organism may remain dormant in tis-sues for a long time and hence drugs may be needed life long or for a minimum of three years.
BRUCELLA: This gram-negative bacillus which causes brucellosis can produce bulky vegetation on the previously damaged aortic and mitral valves followed commonly by valve destruction, perivalvar abscess and congestive heart failure. Doxycycline plus Streptomycin or Gentamicin or Trimethoprim /Sulphamethoxazole or Rifampicin is the drug of choice. Valve replacement is needed in most cases. Drugs should be continued for 2 to 10 months after valve replacement
CANDIDAANDASPERGILLUS: Cause majority of fungal Infective Endocardi-tis. Those with history of IV drug abuse, prosthetic valves replacements and long term central venous catheters are at high risk. Blood cultures are usually negative and vegetations bulky. Metastatic foci, perivalvar invasion and embolisation are common.Valve surgery is a must as Am-photericin B, the only fungicidal agent available and has poor penetra-tion into vegetation. Suppressive therapy with Imidazoles (Fluconazole) may be effective.
LEGIONELLA:Patients usually present with a long febrile illness, newly developed murmur and extremely high antibody titers. Most patients are prosthetic valve recipients. Embolism is rare. Parenteral Doxycycline or Erythromycin followed by prolonged oral therapy is effective. Valve re-placement is needed only if there is valvar incompetence.
PSEUDOMONASAERUGINOSAcauses Infective Endocarditis especially in IV drug abusers. Isolated right-sided Pseudomonas infective endocarditis can be medically managed with Piperacillin combined with an Aminoglycoside. Valve replacement is mandatory for left sided infective endocarditis.
of 0.5 to 1 mm; (vi) T inversion of > 1mm in leads with dominant R waves.Patients with chest pain probably non cardiac, one risk factor (not Diabe-tes Mellitus), flat T wave or < 1 mm inversion in leads with dominant R waves or normal ECG are considered to be carrying a low risk.Percutaneous intervention has proven to prevent irreversible myocardial damage. Cardiac catheterization, Angioplasty and CABG in ACS has in-creased considerably in the past two decades. In ACS, PTCA against the culprit lesion and antiplatelet therapy can be performed with an initial success rate of > 95%, although the incidence of procedure related complication is high, world wide.CABG is considered for patients with coronary lesion that are not suitable for or do not respond to catheter based reperfusion. The reported inci-dence of perioperative death is 4 % and MI is 10 % higher when CABG is performed urgently than semi urgently in ACS. Therefore, efforts should be made to stabilize the patients pharmacologically before emergency revascularization procedures are contemplated. Use of IABP aids as a bridge to Angioplasty or CABG in ACS patients.The need for revascularization is based on diagnosing the culprit lesion early. Various institutions adopt various protocols for coronary angiogra-phy (CAG)in ACS. Two strategies are generally followed- the early inva-sive strategy and the conservative strategy. The early invasive strategy incorporates coronary angiography for all sta-bilized patients within 48 hours of presentation. The conservative strat-egy prescribes angiography for high-risk patients (ie CHF, LVEF<50%, malignant arrhythmia, recurrent ischaemia, prior revascularization etc). Both early invasive and conservative strategies have been found to pro-duce similar clinical outcomes by the TIMI 2B and VANQUISH studyDecision about further proceedings is made based on the disease pattern revealed by CAG. Emergency surgical revascularization may be also need-ed in the setting of a failed thrombolysis or PTCA with acute occlusionThe morbidity of patients operated on after acute MI remains relatively high when compared to stabilized patients. This is mainly because, the adverse effect of CPB is poorly tolerated by a heart with an evolving MI. It is reasonable to think that keeping off the pump may be advantageous in this subgroup of patients.The optimal timing of surgery for ACS remains indecisive. Various studies have shown that the mortality rate of patients who underwent surgical revascularization within 48 hours of an acute MI was significantly higher compared to after 48 hours.A recent multi-center analysis has shown clearly that the perioperative mortality in acute MI patients declined considerably with the increasing time interval. The first 6 hours is said to be the most dangerous period with mortality of about 10%. The mortality depends not only on the tim-ing of surgical revascularization but also on the LV function, presence of haemodynamic stability and presence of collateral circulation.
Cardiopulmonary bypass (CPB) is a significant factor affecting the out-come in patients undergoing early CABG after ACS. Various studies have proven that the mortality rate is nearly 5 times higher in emergency CABG done on a stopped heart than on a beating heart. This deleterious effect of CPB is most evident in patients operated within 48 hours of an acute cardiac event.
OUR EXPERIENCE 306 CABGs were performed in our department during the period from July 2002 to October 2003. Out of these 46 were ACS patients who un-derwent emergency coronary angiography and were taken up for emer-gency surgical revascularisation. 6 of these patients had STEMI, 12 had NSTEMI, and the rest had unstable angina. 2 patients were referred to us for CABG after failed PTCA elsewhere. They were taken up on the second and third day post acute MI respectively.The patient age varied from 38 years to 76 years. 38 were males and 8 were females. All patients were diagnosed based on their ECG, Cardiac enzyme levels and trans-thoracic echocardiography. 2 patients had severe LV dysfunc-tion, 6 had moderate LV dysfunction and the rest had adequate LV func-tion. Every effort was made to stabilize the patients medically, so as to give at least a week’s time for the myocardium to recover from the acute insult. 14 patients needed emergency CABG before a week of the acute event. CABG in all the 46 patients, irrespective of the LV function and the time from the acute event were performed on beating heart. 6 patients needed minimal pump support due to haemodynamic compromise while positioning the heart for OPCAB. We had no perioperative MI or operative mortality. Postoperative ventilation, ICU stay, bleeding, enzyme levels, inotropic support and hospital stay were comparable to elective surgeries. All patients have been followed up till date and are maintaining good health.
CONCLUSIONAcute coronary syndrome is no longer a contraindication for surgical re-vascularisation. Off pump coronary artery bypass has contributed much to the results of CABG in the acute setting by taking the pump-associated complications away. Antiplatelet drugs, which cannot be weaned off in patients in an acute setting, do not contribute to perioperative blood loss in OPCAB patients, questioning the actual need for stopping antiplatelet drugs even before elective OPCAB. The results of surgical revasculariza-tion are rewarding if surgery can be prolonged at least for 3 days after an acute cardiac event.
Off-Pump coronary artery bypass grafting avoids extra corporeal circula-tion and has shown to reduce the clinically relevant morbidity, especially with regard to neurologic complications. Manipulating the ascending aorta by side-clamping is a definite risk factor and VAO helps us to get rid of this.Surgeon’s skill is an important factor in performing proximal anastamoses with VAO. One advantage here is that we can perform either the proximal or the distal anastamosis first, an option that is not possible with the recently described sutureless anastomotic device [Calafiore 2001]. VAO device is made of steel, is reusable, and costs only US$ 10 to fab-ricate it. Side-clamping of the aorta can be avoided, and hence there is no need to bring down the systolic pressure below 100 mm Hg. There is no injury to the vein initima, because nothing is introduced into the vein. The suturing procedure takes not more than 10 minutes, and the learning curve is very short or negligible. VAO can also be used in calcified aortas if a small island of normal tissue is available. Our clinical results are excellent; we are now waiting of the one-year postoperative angiographic studies of our patients in this series, to confirm their long-term patency.
REFERENCES1. Calafiore AM, Barel Y, Vitolla G, 2001. Early clinical experience with a new sutureless anastomotic device for proximal anastamosis of the saphenous vein to the aorta. J Thorac Cardiovasc Surg 121:854-8. 2. Mohan R, Amsel BJ, Walter PJ.1992. Coronary artery bypass in the elderly: a review of studies on patients older than 64, 69 or 74 years. Cardiology 80:215-25. 3. Moshkovitz Y, Luski A, Mohr R.1995. Coronary artery bypass without cardiopulmonary bypass: analysis of short-term and mid-term outcome in 220 patients. J Thorac Cardiovasc Surg 110: 979-87.
The sutures in the vein have to be inside out, and in the aorta, they have to be outside in. The aortic sutures are placed so that the needle passes through the aortic wall, goes into the groove of the Obturator, and comes out between the aorta and the metal, thus taking the intima. The sutures are placed all around the aortic punch hole and are loosely held. Once the suturing is complete, the obturator is removed, and the left index finger is positioned on the aortic punch hole to prevent bleeding. The loose sutures are pulled and tightened with a nerve hook. The assistant holds the two ends of the sutures firmly with controlled traction during this procedure. Once all of the sutures are in place, the two ends are tied snugly. The two snares on the purse string are removed, and they are tied in place with care, so as to avoid a purse string effect.
RESULTSWe have performed 269 proximal anastomoses on 177 patients. Initially, most were performed with proximal anastamosis first so that the flow in the vein grafts could be fully assessed. But with experience, we now do distal anastamosis first. We have had no postoperative ischemia, or peri-operative infarction in any of our patients. We have had no perioperative mortality in our coronary patients. One patient presented with angina after 12 weeks, and check angiogram results showed a perfectly patent graft. We are planning to follow up these patients and to repeat coronary angiography after one year to assess the patencies of their grafts.
DISCUSSIONWith the present-day degree of myocardial protection and refinement in surgical technique, the mortality and morbidity of coronary artery surgery is related more to the co morbidities of patients than to cardiac function and the complexity of the surgical procedure [Mohan 1992].Avoiding cardiopulmonary bypass [Moshkovitz 1995] has further con-tributed to the reduction of mortality and morbidity in high-risk patients, such as those with post infarction angina and a low ejection fraction.
mimslouranlfinal.indd 3 7/21/2004 11:05:55 PM
The choice of the device for valve replacement depends on a variety of factors like risk of re-infection, ease of insertion, durability, need for an-ticoagulation, adequacy of removal of infected tissue etc. A homograft is preferred to a mechanical device considering the reduced risk for re-infec-tion and need for anticoagulation. Valve repair rather than replacement may be considered in some cases of healed mitral valve endocarditis with small vegetations and in intravenous drug abusers with tricuspid valve endocarditis.
MANAGEMENT OF COMPLICATIONS OF INFECTIVE ENDOCARDITIS Sepsis, congestive cardiac failure, embolism, periannular spread, mycotic aneurysm and spread of infection to other organs are the common com-plications of infective endocarditis. Certain factors likeprosthetic cardiac valves, left-sided endocarditis, Staphylococcus aureus IE,fungal IE, previ-ous IE, prolonged clinical symptoms (≥3 months), cyanotic congenital heart disease, patients with systemic to pulmonary shunts and those with poor clinical response to antimicrobial therapy are recognized to carry a high risk for developing complications in a patient with infective endo-carditis
CONGESTIVE CARDIAC FAILURE (CCF) : Congestive cardiac failure has the great-est impact on the prognosis of patients with infective endocarditis. Left sided endocarditis is more likely to develop CCF than right sided infective endocarditis. Aortic valve infective endocarditis is more likely to develop CCF (29%) than mitral valve (20%) or tricuspid valve (8%) infective endocarditis. Usually CCF develops insidiously with progressive worsening of valvular incompetence and ventricular dysfunction. CCF may also develop acutely as in acute rupture of chordae in mitral valve infective endocarditis, valve obstruction due to huge vegetation, prosthetic valve dehiscence, fistulae formation, valve leaflet perforation etc. CCF in infective endocarditis signifies a grave prognosis and is a predictor of poor outcome even after surgery. It is mandatory to operate on such patients at the earliest. Delay of sur-gery to extend preoperative antibiotic treatment carries with it the risk of permanent dysfunction. Class III or IV CCF has a very high risk for poor surgical outcome.
SYSTEMIC EMBOLIZATION : occur in 22 to 50% of cases of infective endocar-ditis. About 60 to 65% of embolic events occur in the CNS; with more than 95% of these in the Middle Cerebral Artery territory. Arterial beds in the lungs, coronaries, spleen, bowel and extremities are also very much prone. Left sided valveinfective endocarditis is more prone to give rise to emboli. Infective endocarditis due to Staphylococccus aureus, Candida, Abiotrophia species and HACEK organisms are important causative fac-tors. Most emboli are noted with two full weeks of treatment and the risk weans off gradually. Left sided vegetation especially of the mitral valve
- 2004 21MIMS HEART JOURNAL JULY ..
and more than 1cm in size are at increased risk. Mitral valve vegeta-tions, irrespective of the size are associated with higher rates of embolism (25%) than aortic valve vegetation (10%). Anterior leaflet vegetation of mitral valve is more prone for embolisation, as the leaflet excursion occurs twice per heartbeat. Size and number of vegetations, number of valves involved and characteristics and mobility of vegetation are other less significant risk factors. Surgery to prevent further embolization is indicated if there has been two or more major embolic events. The advantage of prevention of further emboli exists only when surgery is done early in the course of Infective Endocarditis, when embolic rates are highest. Surgery should be consid-ered when large vegetation is detected on the mitral valve, particularly the anterior mitral leaflet. If inspite of adequate therapy, vegetation is found not to diminish in size or if it is still unstable on trans-esophageal echocar-diography, the risk of embolization is high and surgery may be indicated.
PERIANNULAR SPREAD OF INFECTIVE ENDOCARDITIS
Annular infection can break through and spread into nearby tissues, lead-ing to periannular ascess, pseudo aneurysm, sinuses or fistulae. Perian-nular spread predicts high mortality, and early need for cardiac surgery. Periannular spread complicates 10 to 40% of Infective Endocarditis. Aortic valve infective endocarditis is more prone to periannular spread than mitral or tricuspid valve infection. In prosthetic valve infective endo-carditis, periannular spread occurrence is very high (50 to 100%) as the primary infection is in the annulus and not the leaflets. Persistent bacteremia or fever, recurrent emboli, heart block, CCF or changes in characteristics of a murmur in a patient who is being inad-equately treated for infective endocarditis suggests possibility of perian-nular spread. TEE is the investigation of choice to look for and assess periannular spread. Surgery at the earliest is mandatory and includes drainage of abscess cavities, excision of necrotic tissue and closure of communicating tracts; apart from replacement of the infected valves. Grossly damaged perian-nular supporting tissues need major reconstruction using homograft.

MIMS HEART JOURNAL - 2004 JULY 03..
INTRODUCTIONWith the advent of beating heart surgery, more than 50% of coronary artery bypass graft surgeries are performed in most coronary centers in India without the use of heart-lung machine. But the neurologic prob-lems caused by side clamping the aorta in performing the proximal anas-tomoses still remain. Hence, there has been a great deal of research to find an effective alternative to avoid side clamping the aorta. A couple of anastamotic devices have already arrived in the market, but since the costs of these devices are prohibitive, we designed our own device for proximal anastomoses.
PATIENTS AND METHODSFrom July 2002 to July 2003, we performed 235 coronary artery bypass graft surgeries on the beating heart with 177 of these procedures performed off-pump and 58 of them carried out with pump assistance. Initially, proximal anastomoses of vein grafts were performed with aortic side clamp. Of late, all our top ends are being performed with VAO. 177 patients have had their proximal Saphenous Vein Graft (SVG) anastomo-ses performed with our VAO.Before VAO was used on patients, it was tried for anastomosing vein grafts on the aortas and pulmonary arteries of various perfused animal heart models. The aortic and pulmonary artery pressures were maintained at 110 to 120 mm Hg systolic while these anastomoses were being per-formed. These conduits were then explanted and examined for suture placement to see if all the aortic layers were included.
VETTATH’S ANASTAMOTIC OBTURATOR (VAO)This metallic instrument is made of solid steel (Figure 1). It is 18 cm long and comes in small and medium sizes (5 mm and 6 mm in diameter respectively). The holding part is smooth. The inserting bit has a ridge 2.5 cm from the end (Figure 2). This 2mm ridge projects perpendicularly from the steel rod. There are 3 equidistant grooves in the inserting end that are 1 mm deep a 1.5 cm long. The ridge helps to prevent blood from spurting directly into the eye. The grooves allow the needle to pass through the rod and thereby include the aortic intima in the suture.
SURGICAL TECHNIQUEVAO allows us to anastamose the proximal ends of the vein grafts, before or after the distal anastomoses. The aortic site proposed for anastomosis marked with diathermy. Two 3-0 polypropylene purse-string sutures are applied 1 cm away from the site. The aorta is stabbed with a No.11 blade knife, and punched with 4mm or 4.5mm aortic punch (for 5-mm or 6-mm VAO), respectively. The punch hole is blocked with the left index finger. VAO is introduced and purse strings are tightened just enough to prevent excessive bleeding. Once the obturator is in and the snares are tightened, the proximal vein anastomoses is performed as usual with 5.0 or 6.0 polypropylene suture.
VETTATH’S ANASTAMOTIC OBTURATOROUR EXPERIENCE OF 269 PROXIMAL ANASTOMOSES
Dr. Murali P. VettathChief Cardiac Surgeon
10MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY15..
CARDIAC RESYNCHRONIZATIONTHERAPY A case report with review of literature
CASE REPORT:Mr. R, a 36-year-old gentleman was diagnosed to have Hypertrophic Non-Obstructive Cardiomyopathy with LV systolic dysfunction. He pre-sented to us with worsening of dyspnea, orthopnea, and paroxysmal nocturnal dyspnoea . He had been symptomatic since the last 4 years and in NYHA functional class IV since 2 months. He had two episodes of syncope associated with palpitation during the previous 2 months. He was tachypnoeic on admission, heart rate was 56 beats /min, and blood pressure was 100/80 mmHg. Mean jugular venous pressure was not raised but ‘a’ wave was prominent. Apex beat was in the sixth intercostal space 1 cm outside the midclavicular line. First heart sound was soft, S2 was normally split, and LV S3 and S4 were prominent. Fine basal crepitations were present bilaterally. ECG showed sinus rhythm at 50 bpm, first degree AV block, and LBBB with a QRS duration of 240 m.sec. Chest X-ray showed grade III PVH, cardiomegaly, and mild pulmonary edema. All the routine hematological and biochemical parameters were normal. 2-D Echo Color Doppler examination showed asymmetrical sep-tal hypertrophy with global LV hypokinesis and LV ejection fraction of 35 % by Simpson’s method. There was moderate mitral regurgitation with MR jet area of 7 cm2. This gentleman had cardiac evaluation at another cardiac center in 10 months back. 24-hour Holter at that time showed one episode of non-sustained ventricular tachycardia and frequent multiform VPCs with cou-plets and bigeminy. Monomorphic sustained VT was inducible on electro-physiological testing. Angiography revealed normal coronary arteries. Patient was stabilized with I.V diuretics, Digoxin, ACE inhibitors, and supportive measures. The most appropriate therapeutic option was to provide an Implantable Cardioverter Device with biventricular pacing. However, since the patient could not afford the cost of an Implantable Cardioverter Device, the second best option of biventricular pacing with anti-arrhythmic drugs was discussed with the patient and relatives, to which they agreed.Patient was taken up for transvenous implantation of atrial synchronized biventricular pacing through a left infra-clavicular incision. Subclavian
puncture was done and coronary sinus was cannulated using the pre-formed sheath. A 6French balloon catheter was introduced through the coronary sinus sheath for venography. Attempts to negotiate the guide-wire in to the left cardiac vein were not successful. RA and RV apical leads were placed to which the pulse generator was connected and the wound closed. Subsequently, patient was taken for LV epicardial lead placement through left anterolateral thoracotomy. The proximal end of this lead was tun-neled to the infra-clavicular pocket and connected to the pulse generator. Pacemaker was programmed to biventricular pacing with an AV delay of 140 m.sec. Post-pacing ECG showed shortening of QRS duration to 130 m.sec, which is a significant indicator of response to therapy. Repeat Echocardiagraphic study revealed improvement in LV ejection fraction and reduction of MR jet area from 7 to 4 cm2.
REVIEW OF LITERATURE:INTRODUCTION:The pharmacotherapy of congestive heart failure is primarily based on antagonism of neurohormonal pathways namely, the sympathetic ner-vous system and the “renin-angiotensin-aldosterone axis”. Most of the drugs have been shown to reduce mortality and morbidity and in some cases they improve the underlying structural abnormalities of the heart by a process called reverse remodelling. Despite these therapeutic ad-vances,
Dr. Dinesh Babu .K.VCardiologist
2. Evidence of endocardial involvementA. Positive echocardiogram for IE defined as(i)Oscillating intracardiac mass on valve or supporting struc
tures, in the path of regurgitant jets, or on implanted material in the absence of an alternative anatomic explana tion, or(ii) Abscess, or(iii) New partial dehiscence of prosthetic valve
orB. New valvular regurgitation (worsening or changing of pre existing murmur not sufficient)
MINOR CRITERIA
1. Predisposition: predisposing heart condition or intravenous drug abuse2. Fever: temperature ≥38.0°C3. Vascular phenomena: major arterial emboli, septic pulmo nary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway lesions4. Immunologic phenomena: glomerulonephritis, Osler’s nodes, Roth spots, and rheumatoid factor5. Microbiological evidence: positive blood culture but does not meet a major criterion as noted above or serological evidence of active infection with organism consistent with IE6. Echocardiographic findings: consistent with IE but do not meet a major criterion as noted above.
Diagnosis of Definite Infective Endocarditis by Duke Criteria needs the presence of two major criteria or 1 major and 3 minor criteria or 5 minor criteria or pathological proof if IE. Those patients who do not meet the criteria for “Definite”Infective Endocarditis are labeled as “Probable” In-fective Endocarditis. Those patients whose symptoms reduce either with no treatment or within a short-term after diagnosis and those patients with no pathological evidence of infective endocarditis are labeled as rejected cases.The Duke Criteria is by far more specific and sensitive than the Beth Is-rael Criteria. Clinical suspicion of Infective Endocarditis may be raised by fever, other systemic symptoms along with physical findings like Osler’s nodes, petechiae, Janeway lesions, Roth spots, splenomegaly, newly di-agnosed clubbing and a new changing cardiac murmur. High index of suspicion in susceptible patients helps in diagnosing much before these findings set in. The offending organism can be demonstrated in 3 sets of blood cultures. (Each set with 1 aerobic and 1 anaerobic culture sample) obtained at intervals of more than one hour, within the first 24 hours is mandatory. 5 to 6 samples may be needed in some patients.
The diagnosis of infective endocarditis is straight forward in patients with the classical Oslerian manifestations of bacteremia or fungaemia, active valvulitis, peripheral emboli and immunologic vascular phenomena. In others, these classical findings may be few or absent as in Infective En-docarditis caused by Staphylococcus aureus infection of right sided heart valves or in patients where infective endocarditis is caused by the HACEK (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella) group of organisms. Immunologic vascular phenomenon is characteristic of subacute bacterial endocarditis. They are rarely seen in acute infective endocarditis on presentation, as the disease process is so rapid. Right-sided infective endocarditis does not produce peripheral embolism and immunological vascular phenomenon.This variability in clinical presentation of Infective Endocarditis warrants an optimal diagnostic strategy for early diagnosis. The Beth Israel criteria was proposed in 1981 by Van Reyn which was so stringent that only those patients confirmed pathologically were considered Definite Infec-tive Endocarditis patients and those with bacteremia, new valvular regur-gitation and vascular phenomenon were considered as Probable Infective Endocarditis patients. Durack et al from Duke University proposed the Modified Duke’s Criteria in 1994 incorporating Echocardiographic findings into the important di-agnostic parameters in Beth Israel Criteria. Moreover, intravenous drug abuse was recognized as an important cause for infective endocarditis in Duke’s criteria.The Duke’s clinical criteria stratified the various parameters into two broad groups – Major and Minor criteria as shown below.
MODIFIED DUKE’S CRITERIA FOR CLINICAL DIAGNOSIS OF INFECTIVE ENDOCARDITIS
MAJOR CRITERIA
1. Positive blood culture for IE A. Typical microorganism consistent with IE from 2 separate blood cultures as:(i) Viridans Streptococci, Streptococcus bovis, or HACEK group, or(ii) Community-acquired Staphylococcus aureus or entero cocci, in the absence of a primary focus
orB. Microorganisms consistent with IE from persistently positiveblood cultures defined as(i) ≥2 positive cultures of blood samples drawn >12 hours apart or(ii) All of 3 or a majority of ≥4 separate cultures of blood (with first and last sample drawn ≥1 hour apart)
mimslouranlfinal.indd 2 7/21/2004 11:03:23 PM
22 - 2004
MYCOTIC ANEURYSMS
upper and lower limbs.
is highly variable.
choice.
able in such patients as anticoagulation can be avoided.
tomic site is the only hope for a radical cure.
SPLENIC ABSCESS
CT /
with a splenic abscess.
or gastrointestinal tracts.
preferred in patients who are allergic to penicillin.
MIMS HEART JOURNAL JULY
result from septic embolization of vegetation to vasa vasorum or intraluminal infective embolus with subsequent spread through the intima and outwards through the vessel wall. They occur mostly at arterial branching points as emboli are usually impacted at such points. Intracranial mycotic aneurysms are more common than ex-tracranial ones; which usually affect the visceral arteries and arteries to
The overall mortality rate in infective endocarditis patients with intra-cranial mycotic aneurysm is about 60%. Streptococci account for about 50% and Staphylococcus 10% of intracranial mycotic aneurysms. The distal MCA branches are more commonly affected. Intracranial mycotic aneurysms are multiple in about 20% of patients. Clinical presentation
Routine screening is not required except when clinical findings are sug-gestive of an intracranial pathology. Contrast enhanced CT or Magnetic Resonance Angiography are useful in detecting these lesions but con-ventional four-vessel angiography still remains the diagnostic test of
Intracranial mycotic aneurysms (ICMA) may heal with medical therapy. Proximal aneurysms should be monitored with serial angiograms and CT as ligation of these may lead to severe neurological deficit. ICMA distal to major branching points may be ligated or excised. Some patients need both valve replacements and ICMA ligation. Bioprosthetic valve is prefer-
Extra-cranial mycotic aneurysms (ECMA) may present as tender pulsatile masses. Intra-thoracic or intra-abdominal ECMAs are asymptomatic until leakage or rupture occurs. Proximal and distal ligation of aneurysms and restoration of blood flow with autologous vein grafts through extra-ana-
in infective endocarditis may be caused either by an in-fected embolus or by bacterial seeding of a splenic infarct. Streptococcus viridans and Staphylococcus aureus accounts for around 40% of cases, enterococci 15%, gram-negative bacilli and fungi in <5%. Spleno-megaly is present only in about 30% and is not a reliable sign. Back, left flank, left upper quadrant pain or abdominal tenderness may be present. Persistent fever, bacteremia and sepsis may be suggestive of splenic abscess. Splenic rupture with hemorrhage is a rare complication.
MRI are the best diagnostic tests. Definitive treatment is splenectomy with appropriate antibiotics. Splenectomy should be performed before valve replacement, as the risk of prosthetic valve infection is very high
PROPHYLAXIS AGAINST INFECTIVE ENDOCARDITIS Antibiotic prophylaxis against infective endocarditis is recommended in a group of conditions, which carry with it a very high risk of playing a host to this dreaded disease. Patients with prosthetic heart valves, complex cyanotic congenital heart disease and previous history of infective endo-carditis carry a very high risk. Those with acquired lesions like rheumatic valve disease, hypertrophic cardiomyopathy (HCM), mitral valve prolapse with regurgitation, etc carry a moderate risk with them. Such patients need antibiotic prophylaxis while undergoing any invasive procedures like dental extraction or manipulation of the respiratory, genitourinary
The standard general prophylaxis for patients at risk is Amoxicillin 2gm (50mg/kg in children) given orally one hour before the procedure. Those who are unable to take oral medications are given injection Ampicillin. Those allergic to penicillins are given either Clindamycin or Cephalexin or Cefadroxil or Azithromycin or Clarithromycin. An Aminoglycoside should be added to the above patients if they are undergoing procedures on the genitourinary or gastrointestinal tracts. Vancomycin with Gentamicin is
02 MIMS HEART JOURNAL - 2004 JULY
14MIMSHEARTJOURNAL - 2004 JULYMIMSHEARTJOURNAL - 2004 JULY11..
C O N T E N T S
VETTATH’S ANASTAMOTIC OBTURATORA new proximal anastamotic device
INTENSIVE CARE MANAGEMENT AFTER CARDIAC SURGERYWhere we stand today
TRANS - CATHETER CLOSURE OF PATENT DUCTUS ARTERIOSUSAdieu to surgery
OPCAB FOR ACUTE CORONARY SYNDROMEThe way to go
CARDIAC RESYNCHRONIZATION THERAPYA case report with review of literature:
PUMP LUNG SYNDROMEA case report
INFECTIVE ENDOCARDITIS - DIAGNOSIS AND MANAGEMENT IN ADULTSAn overview
03
05
07
0810
12
14For Private Circulation only
No Part of this publication may bereproduced by any means,including electronic media
Graphics - Design - bynnatural wondders - calicut
Infective Endocarditis, an infection of the inner walls of the cardiac cham-bers, valves, aortic root and prosthetic material is not an uncommon problem in our region. Advances in diagnosis and pharmacotherapy have changed the whole scenario since William Osler (1885) projected bacte-rial infection as the root cause, valvular heart disease as a predisposing factor and valvular incompetence and embolism as lethal complications of what he called Malignant Endocarditis. But even today, Infective En-docarditis carries a very high risk of morbidity and mortality. For bacterial endocarditis to occur there should be bacteremia, damaged endothelium vulnerable to infection, turbulence along haemodynamic path, and a virulent microorganism, which can overcome the natural defenses of the host or a host with a severely compromised immune system. Thus patients with acquired cardiac lesions like Rheumatic heart disease, degenerative valve disease or congenital lesions like Ventricular
Septal Defect, Tetralogy of Fallot, Congenital Aortic stenosis, complex cyanotic anomalies, Patent Ductus Arteriosus, Systemic to pulmonary arterial shunts etc. are prone for infective endocarditis. Recently intra-venous drug abuse is gaining more importance as a common cause for Infective endocarditis
The term infective endocarditis includes acute, subacute and chronic pro-cess of bacterial, viral, fungal or rickettsial aetiology. Acute endocarditis is a life threatening infection usually of normal heart valves, during the course of septicemia by virulent pyogenic microorganism such as hae-molytic Streptococci or Staphylococci. In subacute endocarditis, already damaged valves or other cardiac structures are secondarily infected.Acute native valve endocarditis accounts for 25% of Infective Endo-carditis. Severe sepsis, long term indwelling catheter, IV drug abuse and fungemia are predisposing factors. The usual affecting organism is Staphylococcus aureus. Other common organisms are Streptococcus viridans and Enterococci. The initial stage of valvular infection is surface vegetation – composed of platelets, fibrin and the causative microorganism. Organisms multiply within the vegetation and are thereby protected from the host defenses and antibiotics. They can be a source for repetitive bacteremia. Veg-etations are initially soft and friable and may embolise. They may also produce immune complex mediated and allergic vasculopathies. Large vegetation may become organized and calcified. Endocarditis is considered active surgically when surgery is performed in the presence of obvious local cardiac infection (active vegetation/ab-scess/sinus/fistulae) or when surgery is done while the patient is still on or within two weeks of termination of medical management for Infective Endocarditis. Endocarditis is considered healed when there is no active cardiac infection or inflammation, vegetation if present is endothelialised and abscess and sinus or fistulae if present are well organized.Surgical management of infective endocarditis was first reported by Kay et al (1961) in a patient with Tricuspid valve endocarditis and it was Wallace (1965) who first reported valve replacement as treatment for infective endocarditis.Early Diagnosis, effective management and prompt recognition of com-plication are essential to good patient outcome. For that general idea of the clinical presentation and diagnostic modalities are of great im-portance.
INFECTIVE ENDOCARDITIS - DIAGNOSIS AND MANAGEMENT IN ADULTS AN OVERVIEW
Dr. Sheen Peeceeyen. C.S Cardiac Surgeon
sizable proportion of patients with heart failure remain symptomatic and succumb to death, and hence additional treatment strategies like biven-tricular pacing have been developed.About 30 % of patients with chronic heart failure have intraventricular conduction delay such as left or right bundle branch block leading to loss of coordination of ventricular contraction. Such asynchrony is evident on the surface ECG as widening of QRS interval [> 120 m.sec]. This can impair the contractile reserve of the heart, and also enhance the severity of the functional mitral regurgitation. Intraventricular conduction delay has been associated with electrical instability and increased risk of sud-den death in patients with heart failure.
BENEFICIAL EFFECTS OF BIVENTRICULAR PACING: Short-term results of clinical trials with devices for atrial synchronized biventricular pacing to coordinate left and right ventricular contrac-tions are encouraging. Notable improvements in primary end points of NYHA functional class, six minutes walking distance and quality of life were constantly seen with cardiac resynchronization therapy [CRT]. In the recently published MIRACLE trial, the resynchronization group had significant improvement in peak oxygen consumption and total exercise time. Further, the left ventricular ejection fraction increased and the end-diastolic dimension, the magnitude of mitral regurgitation and the dura-tion of QRS all decreased in the resynchronization group. Biventricular pacing was associated with fewer hospital admissions and fewer days in the hospital for heart failure. The combined risk of a major clinical event [death or hospitalization for heart failure] was 40 % lower in the resynchronization group. In the study of Breithardt et al [JACC 2003 May 21, 41 [10]: 1852] cardiac resynchronization was associated with a significant reduction in severity of mitral regurgitation. The effective regurgitant orifice area decreased from 25 ± 19 mm to 13 ± 8 mm. This was directly related to an increase in left ventricular pressure rise [LV + dp/dt max]. Favourable effect on heart rate variability by resynchro-nization was shown by Adamson et al [circulation 2003 July 22; 108 (3) 266-9]. In the Ventak CHF study [Higgins SL et al JACC 2000 Sept; 36 (3)] synchronized biventricular pacing reduced the frequency of ICD therapies in patients receiving both the devices. Preliminary trial results show significant survival benefit when an ICD is combined with biven-tricular pacing and a 40 % reduction in hospitalization for heart failure.
ELIGIBLE PATIENT POPULATION:Patients with moderate-to-severe symptoms of heart failure [NYHA Class III or IV], left ventricular ejection fraction < 35 % and a wide QRS [> 130 m.sec] with left bundle branch block morphology are currently considered eligible for biventricular pacing. Heterogenous response to biventricular pacing has challenged the predictive accuracy of wide QRS complex in surface ECG for ventricular dyssynchrony. More sensitive tech-niques like Echocardiography with Tissue Doppler imaging to identify
regional delay in left ventricular contraction have been shown to better predict the responders from resynchronisation. [Makaryus AN et al Echo-cardiography] 2003 April 20 (3) 217-23.
TECHNIQUES & COMPLICATIONS:Prior to the procedure, a levophase of coronary angiogram is recorded to profile coronary sinus and cardiac veins. Device implantation is done in left infraclavicular pocket and venous access is obtained via subcla-vian vein puncture. Preformed sheaths in different curves are available to facilitate cannulation of the coronary sinus. With availability of over-the-wire leads, to enter the left cardiac vein, the technical success rate of CRT has improved. Placement of atrial and right ventricular leads are not different from the conventional pacemakers. The major complications associated with the procedure include dissection and perforation of the coronary sinus leading to hemopericardium, complete heart block, asys-tole, and arrhythmias. MIRACLE trial reported a technical failure rate of 8 % and major complications of 1-2 %, which include cardiac tamponade or cardiac arrest requiring resuscitation. Late dislodgment of left ventricu-lar lead can occur in as high as 6 % of patients.
FUTURE PERSPECTIVES:In considering devices for heart failure, the growing weight of evidence for biventricular pacing needs to be considered alongside the expand-ing indications for implantable cardioverter defibrillators. ICDs have been shown to significantly reduce the mortality and propensity for malignant ventricular arrhythmias in patients with left ventricular dysfunctions. Syn-chronized pacing can complement this effect by reducing the need for hospitalization for heart failure and the frequency of ICD therapies. Thus, patients with symptomatic heart failure due to ischemic cardiomyopathy and wide QRS complex, might be better served by a combined resynchro-nization pacer and defibrillator. However, the issue of cost effectiveness remains contentious and warrants further examination when long-term data are available.
REFERENCES: 1 Higgins SL, Yong P, Sheck D et al; biventricular pacing diminished the need for implantable cardioverter defibrillator therapy. Ventak CHF Investigators. J Am Coll Cardiol. 2000 Sep; 36 (3): 828-312 Young JB, Abraham WT, Smith AL et al; combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: the MIRACLE ICD Trial. JAMA. 2003 May 28; 289 (20): 2719-213 Makaryus AN, Arduini AD, Mallin J et al; echocardiographic features of pa-tients with heart failure who may benefit from biventricular pacing. Echocar-diography. 2003 Apr; 20(3) 217-234 Abraham WT., Fisher WG., Smith AL et al, Cardiac resynchronization in chronic heart failure. The MIRACLE study MEJM.
mimslouranlfinal.indd 5 7/21/2004 11:09:49 PM
MIMS HEART JOURNAL - 2004 JULY 23..
I
li tat
j
t
li i li
ili i
D E P A R T M E N T P R O F L E
DEPARTMENT OF CARDIOVASCULAR & THORACIC SURGERY
Dr. Mura .P Vet h, MBBS, DNB, MCh Dr. Sheen Peeceeyen C.S, MBBS, MS, MCh Dr. Babura an A.K, MBBS, DNB, MCh
DEPARTMENT OF CARDIAC ANAESTHESILOGY
Dr. A.V Kannan, MBBS, MD, FCACC Dr. Sa heesh Kumar.N, MBBS, MD
DEPARTMENT OF CARDIOLOGY
Dr. A Fa za , MBBS, MD, DM Dr. As sh Kumar .M, MBBS, MD, DM Dr. D nesh Babu K.V, MBBS, MD, DM Dr. Mura Kr shna, MBBS, MD, DM















![ODOT- PDA intro.ppt [Read-Only] · PDA ConclusionsPDA Conclusions • PDA with CAPWAP evaluates capacity at low cost for driven piles, drilled shafts, & augercast piles • PDA gives](https://static.fdocuments.in/doc/165x107/5e80a08e0838cb51cc1301e3/odot-pda-introppt-read-only-pda-conclusionspda-conclusions-a-pda-with-capwap.jpg)