Hypothermic Coronary Venous Phased Retroperfusion: A ......anaerobic metabolism and ischemic...
12
Hypothermic Coronary Venous Phased Retroperfusion: A Closed-chest Treatment of Acute Regional Myocardial Ischemia SAMUEL MEERBAUM, PH.D., ROBERTO V. HAENDCHEN, M.D., ELIOT CORDAY, M.D., MOYSEY POVZHITKOV, M.D., MICHAEL C. FISHBEIN, M.D., JACOB Y-RIT, M.D., TZU-WANG LANG, M.D., TAKAHISA UCHIYAMA, M.D., NOBORU AoSAKI, M.D., AND JEFFREY BROFFMAN, B.A. SUMMARY Hypothermic synchronized retroperfusion (HSRP) was applied in closed-chest dogs after acute coronary occlusion to determine whether this intervention can significantly retard the otherwise rapidly developing irreversible ischemic injury. The left anterior descending coronary artery (LAD) was occluded for 3 hours in 22 dogs and for 6 hours in 16 dogs. Starting 30 minutes after occlusion, HSRP was applied during maintained coronary occlusion in 21 dogs. The remaining dogs served as untreated controls. Arterial blood was cooled to 20°C and retroperfused in diastole into the regional coronary veins. Hemodynamics, contrast cine- angiography and two-dimensional echocardiography were measured sequentially. Glycogen-depleted ischemic areas and necrotic zones were delineated in transverse slices of the left ventricle. Untreated control dogs further deteriorated; in contrast, HSRP between 30 minutes and 3- or 6-hour LAD occlusion significantly reduced the rate-pressure product (21.3 ± 4.0% or 26.8 ± 8.2%) and left ventricular end-diastolic pressure (39.5 ± 9.5% or 51.4 ± 7.7%) and increased ejection fraction (28 ± 17% and 33 ± 2.0%). HSRP caused no arrhythmias and led to much less necrosis of ischemic myocardium in the treated 3- or 6-hour occlusion series (7.4 ± 2.7% or 28.9 ± 12.6%) than in respective untreated controls (47.1 ± 8.9% and 72.3 ± 5.9%). Moderately hypothermic closed-chest phased retroperfusion appears to protect reversibly injured ischemic myocardium and improve cardiac function. Such treatment may be particularly suitable in the earliest stages of evolving myocardial infarction, when maintenance of myocardial viability is essential for preservation of jeopardized myocardium while awaiting coronary bypass revascularization or nonsurgical thrombolytic reperfusion. APPLICATION of hypothermia during periods of ischemia or anoxia is a well-established procedure in cardiac surgery. Surgical research suggests that hypo- thermia, often combined with cardioplegia, repre- sents an appropriate perioperative treatment capable of extending myocardial viability if it is instituted before irreversible damage ensues. Modes of global or regional application, the degree of hypothermia, and its effectiveness alone or in conjunction with various infusion protocols have been investigated. Although cooling-induced slowing of cellular me- tabolism may be beneficial during acute myocardial ischemia,' prompt clinical application of regional car- diac hypothermic treatment presents difficulties, and methods have not been adequately evaluated. Stable levels of myocardial cooling can be achieved in the From the Department of Medicine, Division of Cardiology, and the Department of Pathology, Cedars-Sinai Medical Center; and the Department of Medicine, UCLA School of Medicine, Los Angeles, California. Supported in part by grants HL-14644-08 and HL-17651-06, NHLBI, NIH; the Ahmanson Foundation; the W.M. Keck Foun- dation; the Lillian D. Truyens Foundation; Mrs. Anna Bing Arnold; Ms. Joan and Mrs. Pearl Borinstein; Mr. and Mrs. E.E. Fogelson; Mr. and Mrs. Ira Gershwin; Mr. and Mrs. Edward Mitchell; Mr. and Mrs. Abe Lipsey; and Mrs. Rita Schreiber, Los Angeles, California. Address for correspondence: Samuel Meerbaum, Ph.D., Cedars- Sinai Medical Center, Halper Research Building, 8700 Beverly Boulevard, Los Angeles, California 90048. Received June 3, 1981; revision accepted October 14, 1981. Circulation 65, No. 7, 1982. closed chest after a cool-down period of 2-3 hours, using externally applied or systemically administered whole-body hypothermia,1 2 and recent investigations reported that such an approach improved cardiac function and reduced infarct size." 3 However, a delay of even 2 hours after an acute coronary occlusion may result in substantial irreversible damage.4' 1 There- fore, we examined closed-chest intracoronary tech- niques aimed at rapidly instituted regional hypo- thermia to an acutely underperfused ischemic zone. Antegrade intracoronary delivery of cooled arterial blood beyond a coronary obstruction is one method for extending ischemic tissue viability. We chose the more practicable coronary venous retrograde route to promptly produce hypothermia in an acutely ischemic segment of the left ventricle, hoping to enhance the safety and effectiveness of closed-chest synchronized retroperfusion.67 Our objective has been to develop a prompt hypothermic assist capable of significantly extending viability and enhancing function of jeo- pardized acutely ischemic myocardium. We report an exploratory experimental study of hypothermic retro- perfusion applied in the earliest stage after acute cor- onary occlusion.8' 9 Methods The study was performed in 38 healthy closed-chest mongrel dogs that weighed 25-35 kg. Each dog was placed on a special table to facilitate echocardio- graphic, fluoroscopic and cineangiographic studies. 1435 by guest on October 4, 2017 http://circ.ahajournals.org/ Downloaded from
Transcript of Hypothermic Coronary Venous Phased Retroperfusion: A ......anaerobic metabolism and ischemic...

Hypothermic Coronary Venous PhasedRetroperfusion: A Closed-chest Treatmentof Acute Regional Myocardial Ischemia
SAMUEL MEERBAUM, PH.D., ROBERTO V. HAENDCHEN, M.D., ELIOT CORDAY, M.D.,
MOYSEY POVZHITKOV, M.D., MICHAEL C. FISHBEIN, M.D., JACOB Y-RIT, M.D.,
TZU-WANG LANG, M.D., TAKAHISA UCHIYAMA, M.D., NOBORU AoSAKI, M.D.,AND JEFFREY BROFFMAN, B.A.
SUMMARY Hypothermic synchronized retroperfusion (HSRP) was applied in closed-chest dogs afteracute coronary occlusion to determine whether this intervention can significantly retard the otherwise rapidlydeveloping irreversible ischemic injury. The left anterior descending coronary artery (LAD) was occluded for 3hours in 22 dogs and for 6 hours in 16 dogs. Starting 30 minutes after occlusion, HSRP was applied duringmaintained coronary occlusion in 21 dogs. The remaining dogs served as untreated controls. Arterial blood wascooled to 20°C and retroperfused in diastole into the regional coronary veins. Hemodynamics, contrast cine-angiography and two-dimensional echocardiography were measured sequentially. Glycogen-depleted ischemicareas and necrotic zones were delineated in transverse slices of the left ventricle.
Untreated control dogs further deteriorated; in contrast, HSRP between 30 minutes and 3- or 6-hour LADocclusion significantly reduced the rate-pressure product (21.3 ± 4.0% or 26.8 ± 8.2%) and left ventricularend-diastolic pressure (39.5 ± 9.5% or 51.4 ± 7.7%) and increased ejection fraction (28 ± 17% and 33 ±2.0%). HSRP caused no arrhythmias and led to much less necrosis of ischemic myocardium in the treated 3- or
6-hour occlusion series (7.4 ± 2.7% or 28.9 ± 12.6%) than in respective untreated controls (47.1 ± 8.9% and72.3 ± 5.9%).
Moderately hypothermic closed-chest phased retroperfusion appears to protect reversibly injured ischemicmyocardium and improve cardiac function. Such treatment may be particularly suitable in the earliest stagesof evolving myocardial infarction, when maintenance of myocardial viability is essential for preservation ofjeopardized myocardium while awaiting coronary bypass revascularization or nonsurgical thrombolyticreperfusion.
APPLICATION of hypothermia during periods ofischemia or anoxia is a well-established procedure incardiac surgery. Surgical research suggests that hypo-thermia, often combined with cardioplegia, repre-sents an appropriate perioperative treatment capableof extending myocardial viability if it is institutedbefore irreversible damage ensues. Modes of global orregional application, the degree of hypothermia, andits effectiveness alone or in conjunction with variousinfusion protocols have been investigated.
Although cooling-induced slowing of cellular me-tabolism may be beneficial during acute myocardialischemia,' prompt clinical application of regional car-diac hypothermic treatment presents difficulties, andmethods have not been adequately evaluated. Stablelevels of myocardial cooling can be achieved in the
From the Department of Medicine, Division of Cardiology, andthe Department of Pathology, Cedars-Sinai Medical Center; andthe Department of Medicine, UCLA School of Medicine, LosAngeles, California.
Supported in part by grants HL-14644-08 and HL-17651-06,NHLBI, NIH; the Ahmanson Foundation; the W.M. Keck Foun-dation; the Lillian D. Truyens Foundation; Mrs. Anna Bing Arnold;Ms. Joan and Mrs. Pearl Borinstein; Mr. and Mrs. E.E. Fogelson;Mr. and Mrs. Ira Gershwin; Mr. and Mrs. Edward Mitchell; Mr.and Mrs. Abe Lipsey; and Mrs. Rita Schreiber, Los Angeles,California.
Address for correspondence: Samuel Meerbaum, Ph.D., Cedars-Sinai Medical Center, Halper Research Building, 8700 BeverlyBoulevard, Los Angeles, California 90048.
Received June 3, 1981; revision accepted October 14, 1981.Circulation 65, No. 7, 1982.
closed chest after a cool-down period of 2-3 hours,using externally applied or systemically administeredwhole-body hypothermia,1 2 and recent investigationsreported that such an approach improved cardiacfunction and reduced infarct size." 3 However, a delayof even 2 hours after an acute coronary occlusion mayresult in substantial irreversible damage.4' 1 There-fore, we examined closed-chest intracoronary tech-niques aimed at rapidly instituted regional hypo-thermia to an acutely underperfused ischemic zone.Antegrade intracoronary delivery of cooled arterial
blood beyond a coronary obstruction is one methodfor extending ischemic tissue viability. We chose themore practicable coronary venous retrograde route topromptly produce hypothermia in an acutely ischemicsegment of the left ventricle, hoping to enhance thesafety and effectiveness of closed-chest synchronizedretroperfusion.67 Our objective has been to develop aprompt hypothermic assist capable of significantlyextending viability and enhancing function of jeo-pardized acutely ischemic myocardium. We report anexploratory experimental study of hypothermic retro-perfusion applied in the earliest stage after acute cor-onary occlusion.8' 9
MethodsThe study was performed in 38 healthy closed-chest
mongrel dogs that weighed 25-35 kg. Each dog wasplaced on a special table to facilitate echocardio-graphic, fluoroscopic and cineangiographic studies.
1435
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

VOL 65, No 7, JUNE 1982
Anesthesia was induced by administering sodium pen-tobarbital (35 mg/kg i.v.) 20 minutes after 1 mg/kg ofi.m. morphine sulfate. Heparin (10,000 IU i.v.) wasgiven before instrumentation, followed by 3000 IUevery 3 hours. Supplemental pentobarbital was ad-ministered when required. Saline was drip-infused at arate of 150 ml/hour.A #4F intracoronary double-lumen balloon catheter
was introduced under fluoroscopic control into the leftanterior descending coronary artery (LAD), and theballoon was inflated for acute coronary occlusion at asite distal to the first diagonal branch of the LAD.After catheterization and completion of instrumenta-tion, the preparation was allowed to stabilize for 30minutes. Before occlusion and subsequently at regularpostocclusion intervals up to 3 or 6 hours, aorticroot, left ventricular (LV) and distal LAD coronarypressures were measured with Statham P23Db trans-ducers. ECGs and blood pressures were recorded(Model V12, Electronics for Medicine, Honeywell).Magnified LV end-diastolic pressure, along with LVdP/dt derived by electrical differentiation, were alsomonitored. Cardiac output was measured by thermo-dilution (American Edwards Laboratories). BloodPo2, Pco2 and pH were monitored by sampling fromthe aortic root and through the central lumen of theLAD catheter. Temperatures were recorded in theclosed-chest dog study at three sites: at the extra-corporeal synchronized retroperfusion (SRP) pump,in the dog's rectum and within the LAD distal to theballoon occlusion.
Synchronized Retroperfusion SystemAn experimental closed-chest SRP system7 was
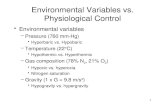
modified to incorporate cooling of the pumped blood(fig. 1). Arterial blood was shunted from the dog'sbrachial or carotid artery into a phased gas-actuatedbladder pump synchronized by conventional counter-pulsation ECG-triggering (Phased Shift BalloonPump, A. Kantrowitz). The arterial blood was pro-pelled forward in diastole for ischemic zone retro-infusion, and flow was stopped in systole to facilitatenormal coronary venous drainage. A single-lumenautoinflatable balloon catheter was used to achieveretrograde diastolic infusion through the regionalgreat cardiac vein subserving the occluded LAD. Theballoon inflated rapidly when catheter intraluminalpressure was generated during diastolic retroinfusion;this compartmentalized the great cardiac vein in dias-tole, so that retroinfusate was effectively directed tothe ischemic region, with minimal bypassing to thecoronary sinus. The balloon collapsed promptly whenretroinfusion ceased at the onset of systole to permitcoronary venous blood drainage around the retro-perfusion catheter into the coronary sinus. Coronarycontrast venography confirmed the rapidity of thisphasic action; it demonstrated extensive diastolicpenetration of retroinfusate into the plexus of smallcoronary veins located within the region distal to LADocclusion, as well as effective emptying in systolethrough the major coronary veins.
Arterial blood was cooled by passing a coiled can-
FIGURE 1. Hypothermic synchronized retroperfusion(HSRP). Arterial blood is shuntedfrom the aortic arch andthen cooled and delivered into the synchronized bladderpump. In diastole, blood is propelled into the balloon-tippedsynchronized retroperfusion (SRP) catheter and through itinto the regional coronary veins. Forwardflow stops in sys-tole, causing the balloon of the SRP catheter to promptlycollapse and allowing coronary venous drainage around thecatheter into the coronary sinuis. The system also providesmeasurement of infusate pressure andflow. SRP treatmentis applied through the great cardiac vein and the anterior in-terventricular (AI) vein to perfuse myocardium madeacutely ischemic by intracoronary balloon occlusion of theleft anterior descending (LAD) coronary artery. EM = elec-tromagnetic.
nula through ice water to maintain an infusion tem-perature of 20°C at the external SRP pump (fig.1). Resulting myocardial temperatures were not mea-sured directly in this closed-chest dog study, but intra-vascular blood temperature distal to the LAD occlu-sion was monitored by a thermistor passed into theischemic zone through the central lumen of the intra-coronary balloon catheter. Retrograde blood flow ratewas measured with an electromagnetic flowmeter(model ABC- 1000B, Omnicraft). To maintain re-gional coronary vein pressures well below 50 mm Hgat any time, a requirement derived from previous ex-perience,6 7 mean retroperfusion flow rate was kept inthe range of 60-80 ml/min, as measured with an elec-tromagnetic probe in the hypothermic synchronizedretroperfusion (HSRP) system (fig. 1).
Measurement of LV FunctionLV ejection fraction was measured by contrast cine-
angiography or two-dimensional echocardiography(2D echo) (model 850A, Advanced TechnologyLaboratories). Because of its noninvasive characterand comprehensive imaging of the left ventricle, 2Decho was also used to sequentially quantitate changesin global and regional cardiac function resulting fromthe HSRP intervention. Several short-axis and onelong-axis 2D echo sections of the left ventricle wereimaged. LV volumes and ejection fractions could bereconstructed from 2D echo section areas and LVlength, in a manner described and validated.10 Endo-
CIRCULATION1436
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

HYPOTHERMIC RETROPERFUSION/Meerbaum et al.
cardial outlines of the ventricular lumen were planim-etered to compute the sectional systolic fractional areachange (FAC), an index of regional contractile func-tion. Further subdivision of sections into eight sectorswas carried out in a standardized manner using thecenter of the lumen and internal landmarks of the leftventricle. FAC was then computed for each of theeight segments to assess function in ischemic and non-ischemic zones.
Pathologic StudyAt the time of sacrifice, the hearts were promptly
(less than 60 seconds) excised, and cut as rapidly aspossible from apex to base into five to seven trans-verse slices (of 0.8-1.0 cm thick). Alternate slices wereeither incubated in triphenyl tetrazolium chloride(TTC) or immersed into Carnoy's solution, a non-aqueous, volatile fixative that preserves tissue gly-cogen. TTC served for macroscopic determination ofinfarct size,'1--' and periodic Acid-Schiff (PAS)-stained sections of myocardium fixed in Carnoy'ssolution demonstrated glycogen loss, characterizinganaerobic metabolism and ischemic injury.14'19 TheTCC-stained slices were fixed in formalin and photo-graphed. Carnoy-fixed slices were cleared in cedar-wood oil and embedded in paraffin. Then whole mountgiaht histologic sections of each slice were cut fromthe slab surface adjacent to that of the neighboringTTC-stained slice. This section was stained forglycogen by the PAS method. The regions that areglycogen-depleted (i.e., ischemic) fail to stain.20 Theextent of both the necrotic zone in TTC-stained slicesand the ischemic zone in adjacent PAS-stained sec-tions were measured by planimetry.2" 22 Thus, the ex-tent of necrosis could be compared with the extent ofischemia in both control dogs and in treated dogs.Electron microscopic study of TTC-delineated zonesin LV slabs has confirmed that this macroscopic tech-nique appropriately defines irreversible injury at 3hours after occlusion or even earlier.'1 In selectedanimals, coronary venous retroinfusion of colloidalcarbon was used to check whether the retroperfusateentered into the ischemic zone microvasculature.
Data AnalysisStatistical evaluation was applied by unpaired t
tests to compare the changes induced by HSRP(between 30 minutes and 3 or 6 hours after LADocclusion) vs the spontaneous alterations during thesame periods of untreated coronary occlusion.
ResultsEffects ofHSRP Applied from 30 to 180 or from30 to 360 Minutes After LAD Occlusion
HemodynamicsIn the 3-hour series, there were no significant differ-
ences in hemodynamics between treated and un-treated dogs before or 30 minutes and 3 hours afterocclusion. Compared with the untreated controls,which exhibited a further drop in LV stroke volumeand increased the rate-pressure product, LV end-dia-stolic pressure and systemic vascular resistance,
HSRP applied between 30 and 180 minutes signifi-cantly lowered the double product (21.3 ± 4.0%), LVend-diastolic pressure (39.4 ± 9.5%) and systemic vas-cular resistance (12.5 ± 5.9%), while increasing LVstroke volume (4.5 + 8.3%). Other differences werenonsignificant.Comparing HSRP vs controls in the extended
series, heart rate decreased 8.1 ± 7.0%, vs an increaseof 27.1 ± 5.8%; mean aortic pressure was reduced by21.5 ± 3.6%, vs a decrease of 12.1 ± 6.3%; the doubleproduct dropped 26.8 ± 8.2%, vs an increase of 16.8 ±9.2%, and LV end-diastolic pressure dropped 51.4 ±7.7%, vs a slight reduction of 6.3 ± 13.7% (fig. 2).Differences in other measurements were not signifi-cant.HSRP caused no arrhythmias. The only instances
of premature ventricular complexes occurred in bothtreated and untreated dogs very early after the cor-onary occlusion (within the 30-minute LAD occlusionperiod).
Closed-chest Temperature MeasurementsAfter a reduction of 0.67 ± 0.22°C durirng the first
30 minutes ofLAD occlusion, temperature distal to theballoon occlusion dropped rapidly with HSRP by 4.85± 0.79°C. This was significant compared with agradual decrease by 2.04 ± 0.42°C measured rectally.The LAD temperature level remained substantiallyabove the 20°C level instituted at the extracorporealHSRP pump, indicating moderate myocardial hypo-thermia. Recent measurements with implanted ther-mistors in two dogs indicated that during the HSRPtreatment, subepicardial temperatures in the ischemicand nonischemic zones decreased at most by severaldegrees, and did not drop below 30°C. These mea-surements appear consistent with moderate hypo-thermia and small myocardial temperature gradients.
L V FunctionFigure 3 shows the sequential cineangiographic
measurements of LV ejection fraction in untreatedand treated dogs with a 3-hour LAD occlusion. Therewere no differences between the series before and 30minutes after LAD occlusion, but HSRP resulted in asignificant (though partial) return of global LV func-tion.
Figure 4 illustrates the type of computer-assisted 2D echo quantitation of papillary level LV short-axiscross sections performed in the control state and aftercoronary occlusion. Normal contraction with uni-form inward wall motion, evident before coronaryocclusion, changed promptly to distinctly deranged(akinetic or dyskinetic) anterior and anteroseptal wallmotion, with some hypofunction in more remote seg-ments. This dysfunction persisted in the absence oftreatment, whereas in the HSRP-treated dogs, con-traction tended to return toward normal despite main-tained LAD occlusion.
Sequential reconstructive 2D echo studies of LVvolumes, stroke volumes and ejection fraction wereperformed in all dogs with a 6-hour LAD occlusion.Figures 5 and 6 are a comparison of HSRP vs control
1437
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

VOL 65, No 7, JUNE 1982
series and show a major reduction of both end-dia-stolic and end-systolic LV volumes by the HSRPtreatment, resulting in a significant increase in LVejection fraction between 30 minutes and 6 hours. Incontrast, volumes remained elevated and ejection frac-tion decreased further in untreated controls.
Detailed analysis of 2D echo short-axis cross-sec-tions at different levels of the left ventricle yieldedfurther data on HSRP effects. At the higher level ofthe left ventricles, sectional cardiac function wasreturned to normal by the HSRP treatment. At thelowest level, function was improved, but remainedbelow control (fig. 7). In untreated dogs, 6
140-F-
I 120_
100 L80 _
E 15000F0 _
x 11000
7000 _
4000 -
> 3000_cn
2000L
.-_-e
0I l, \
I I I IControl 30min. 1.5hr. 3hr. 4.,
100
80
60
40
20
0
= CONTROL (N=9)r7 r "
'IL*
r'HSRP (N= 13)pc 05 relative to 30min
occlusion
Ie
CONTROL 30 min 3 hrocclusion occlusion
hours of FIGURE 3. Left ventricular (LV) ejection fraction (%) inuntreated and hypothermic synchronized retroperfusion
- °.. (HSRP)-treated dogs with 3 hours of coronary occlusion0, - '(LV angiography). There were no statistical differences in
ejection fraction in preocclusion control and 30 minutesafter occlusion (before HSRP in treated dogs). In controldogs, ejection fraction remained depressed or decreasedfurther between 30 minutes and 3 hours, while HSRP sig-nificantly increased global L V performance.
or coronary occlusion led to progressively more func-tional derangements. Segmental analysis of the lowpapillary muscle level 2D echo section showed thatHSRP distinctly improved contraction in the anterior
..- 4* ischemic region, in sharp contrast with persisting dys-kinesis in untreated controls (fig. 8A). The remotenonischemic posterior wall, which showed hypo-kinesis in control occlusions, demonstrated signifi-cantly improved contraction with HSRP (fig. 8B).Thus, cardiac function in the HSRP series was sig-
* nificantly enhanced between 30 minutes and 6 hours,but deteriorated further in the untreated controls.
I J However, LV function was usually not fully restored5hr. 6 hr. by HSRP to the preocclusion level.
A O
CORONARY OCCLUSION PathologySample photographs of LV slabs studied for is-
chemia and necrosis are presented in figures 9 and 10.Figure 9 illustrates the extent of both glycogen-de-pleted and necrotic zones in adjacent low papillarymuscle level slabs of an untreated control dog, sacri-
FIGURE 2. (top) Heart rate (HR), the product ofHR andmean aortic blood pressure (HR X AoPm) and systemicvascular resistance (SVR) vs time for eight dogs with un-
10- treated (open circles) and hypothermic synchronized retro-' - __- - - -o perfusion (HSRP, solid circles)-treated 6-hour coronary
--occlusions. There were no statistically significant differ-ences in the control state or 30 minutes after occlusion.HSRP, initiated after the 30-minute coronary occlusionmeasurements, and maintained throughout the 6-hourocclusion period, significantly lowered heart rate and HR X
'_ AoPm. SVR was significantly lower in the treated series at4.5 hour after occlusion. (bottom) Left ventricular end-dia-stolic pressure (L VEDP), LV stroke work (SW) and max-
l l I imal LV rate of rise (LV dP/dt) vs coronary occlusion.trol 30min. 1.5hr. 3hr. 4.5hr. 6hr. HSRP caused a significant drop in L VEDP compared with
I I untreated dogs. There were no statistical differences in SWCORONARY OCCLUSION and LV dP/dt.
0lLLJ
I
16
12
8
4
rF
503 40cn
3020
1800 -
1400 L
1000_
4-0.~0-J
Cont
II-
1438 CIRCULATION
I
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

HYPOTHERMIC RETROPERFUSION/Meerbaum et al.
CONTROL STATE
EDA=20.85socm ESA-10.91 FAC=47.7
30 MIN LAD OCCLUSION
EDA = 20.43sQ cm ESA = 16.79 FAC =17.8
FIGURE 4. Computer-assisted two-dimensional echocardiographic quantitation of left ventricular (L V)function in a short-axis cross-sectional image at the low L V level. In this view, the septum is on the left andtop, and anterior wall at the bottom, and the posterior aspect on the right. Analysis was performed bothbefore and 30 minutes after acute occlusion of the left anterior descending (LAD) coronary artery. EDA =diastolic intraluminal section area; ESA - systolic area; and FA C = percent systolic fractional area change.Diastolic and systolic area centers are close to each other in the control state in the presence of essentiallyuniform' inward wall motion, but deviate during coronary occlusion in view ofmajor segmental dyssynergy.Using standardized subdivision' into eight sectors, analysis ofsegmental FA C shows dyskinesis in the antero-septal ischemic region, with progressively less regional dysfunction in more distant segments. Hypokinesisappears to be due to the broad'impact of LAD occlusion on function at the low level of the ventricle.
ficed 6 hours after coronary occlusion. The size ofnecrotic and ischemic areas are similar. Figure 10shows, in a similar manner, an HSRP-treated dog.There is a marked difference in that necrosis is minor
100 -0-- o
> _0 UNTREATED (N=d,D 80 _. HSRP (N=8)
W * p < 0560 .p< .001
60*70 - -0-
ci 50 -
w/30 ;
20
1. I l I
Control 30min 1;5hr 3hr. 4.5hr 6hr.
CORONARY OCCLUSKON
FIGURE 5. Two-dimensional echocardiographic analysisof left ventricular end-diastolic volume (EDV), end-systolicvolume (ESV) and stroke volume (SV) throughout the 6-hour experiments. There are no statistical differences be-tween the untreated and treated series either before or 30minutes after occlusion. In contrast with untreated dogs, sig-nificant differences developed after 1.5 hours, with hypo-thermic synchronized retroperfusion (HSRP) sharply reduc-ing both EDV and ESV. SV increased at 6 hours.
and limited to subendocardium, while the zone ofglycogen depletion exhibits a patchy character. HSRPappeared to protect most of the ischemic myocar-dium over the experimental coronary occlusion peri-ods, whereas absence of treatment resulted in exten-sive necrosis within the ischemic zone.
Statistical evaluation of the 3-hour occlusion path-ologic data is shown in figures 11 and 12, whichare comparisons of untreated controls with.-HSRP-
706050
L, 40LUj3020100
D] UNTREATED (N=8)2 HSRP SN=8)* p<.0l** p<.00I
Control 30 mim 3 hr. 6 hr.
CORONARY OCCLUSION-
FIGURE 6. Left ventricular (L V) volumes determined bytwo-dimensional echocardiography were used to computethe global percent ejection fraction- (L VEF). Over 6 hours ofuntreated coronary occlusion, L VEF dropped progressivelyand substantially. Hypo'thermic synchronized retroper-fusion (HSRP) begun after 30 minutes of occlusion led to asignificant improvement in LVEF.
1439
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

VOL 65, No 7, JUNE 1982
D UNTREATED (N=8)0 HSRP (N=8)
** p<.001
60
50
40
30
20
10
o
*T
Control 30 min 3 hr. 6 hr.
CORONARY OCCLUSION
FIGURE 7. The effects of hypothermic synchronized retro-perfusion (HSRP) on regional left ventricular functionstudied by two-dimensional echocardiography at the highpapillary muscle level, which corresponds to the moderatelyischemic zone near the left anterior descending coronary
artery occlusion site. HSRP totally reversed the moderatedysfunction noted 30 minutes after occlusion, in contrastwith persisting major reduction in sectional systolic fractionarea change (FAC) in untreated dogs with 6 hours of cor-
onary occlusion.
treated dogs. While the difference in the overall size ofischemic zones at the low papillary level was not sig-nificant (fig. 11), treated dogs did show a smaller andmore patchy glycogen depletion. In sharp contrastwith untreated controls, HSRP-treated dogs showedless necrosis, expressed either as percent of respectiveischemic area (fig. 11) or as percent of left ventricle(fig. 12). Similar pathologic data were obtained in the6-hour occlusion series (figs. 13 and 14). Myocardialnecrosis was not fully averted by HSRP (particularlyat the apex of the left ventricle), but salvage or exten-sion of myocardial viability was highly significantcompared with 6-hour untreated coronary occlusion(fig. 14).
Figure 15 illustrates the penetration of retroinfusedcolloidal carbon into capillary vessels within the is-chemic region, confirming prior indications that SRPdoes indeed provide retrograde delivery of perfusate tothe severely jeopardized myocardium23
Comparison Between HSRP and SRPEven though substantial experience with SRP has
been reported,ff" additional comparative data were
obtained in the current study in five dogs applyingSRP alone (without hypothermia) from 30 minutes to6 hours after coronary occlusion. Intermediate effectsbetween untreated control and HSRP were generallynoted. Thus, SRP alone differed from HSRP between30 minutes and 6 hours: LV ejection fraction in-creased 5.2 ± 17.4% vs 32.6 ± 2.0% (decrease by 31.6± 6.9% in untreated controls); double product de-creased only 9.1 + 13.7% vs 26.8 8.2% (16.8 ± 9.2%increase in controls); LV end-diastolic pressure was
reduced 18.3 ± 10.2% vs 51.4 + 7.7% (6.3 ± 13.8% incontrols); systemic vascular resistance decreased 1.5
12.2% vs an increase of 22.4 ± 12.9% in HSRP
(25.0 ± 11.4% increase in controls). Hypothermiaappeared to counteract the often observed reduction invascular resistance with SRP. Infarction with SRPalone was substantially less than in untreated con-trols, but substantially greater than in the HSRPseries (58.2 ± 42.8% vs 28.9 ± 12.6% of ischemiczone).
DiscussionSRP per se is associated with distinct bene.fits,6 but
HSRP was more effective in extending the viability ofseverely jeopardized myocardium and significantlyimproving cardiac function. These benefits probably
50
40
30
e 20
< o
-10
-20
60
11
50
40
30
20
10
0
Control
UNTREATED (N =8'
HSRP (N=8)* p < 01
i i
30 min 3 hr. 6hr.
CORONARY OCCLUSION
UNTREATED (N =8)
0 HSRP (N=8)
* p<.0i** p<.001
Control 30min 3 hr. 6 hr.
CORONARY OCCLUSION
FIGURE 8. (top) Two-dimensional echocardiographicanalysis of low left ventricular section (much below the leftanterior descending coronary artery occlusion site) is-chemic segment, with segmental function expressed as per-
cent systolic fractional area change (FA C). Without treat-ment, coronary occlusion caused severe dysfunction thatprogressed to frank dyskinesis. In contrast, hypothermicsynchronized retroperfusion (HSRP) resulted in a sharp risein contraction, reaching a level only moderately below thecontrol state. (bottom) Echocardiographic quantitation ofpercent systolic FAC in a remote (only moderately in-volved) segment of a low left ventricular short-axis section.Hypocontraction during coronary occlusion was unalteredwithout treatment but reversed with HSRP.
.,
1440 CIRCULATION
T
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

HYPOTHERMIC RETROPERFUSION/Meerbaum et al.
:a
FIGURE 9. Control dog killed 6 hours after coronaryocclusion. Giant histologic section stained with PAS forglycogen (A), and surface of adjacent gross slice of myo-cardium stained with triphenyltetrazolium chloride (TTC)to demonstrate necrosis (B). The necrotic zone, which failsto stain with TTC, is almost as large as the glycogen-depleted ischemic zone (A).
reflect synergistic effects of enhanced ischemic tissueperfusion by SRP,24 along with reduction of cellularmetabolism and oxygen demands due to lowering ofmyocardial temperatures.25, 25
Although not systematically measured in thisclosed-chest preparation, limited data with implantedmyocardial thermistors indicated that the retro-gradely applied hypothermia was distributed and didnot reduce regional myocardial temperature below30°C. The resulting relatively small temperaturegradients may explain why no arrhythmias were en-
countered in our study. Intravascular temperature dis-tal to the coronary artery occlusion provided indirectdata suggesting an early but moderate degree ofregional myocardial cooling when the retrogradelydelivered blood temperature was lowered to 20°C atthe extracorporeal SRP pump.The hemodynamic changes and improvements in
FIGURE 10. Treated dog killed 6 hours after coronaryocclusion. Giant histologic section stained with PAS forglycogen (A), and surface of adjacent gross slice of myo-cardium stained with TTC to demonstrate necrosis (B).There is no myocardium that fails to stain, indicating thatno necrosis is present. In this example, when compared tothe previous control, glycogen loss is also less extensive andpatchy.
LV function with HSRP are generally in accord withprevious investigations of SRP,6 except that the sig-nificant drop in systemic vascular resistance usuallyobserved with SRP alone appeared to be reduced orabsent with HSRP. The addition of hypothermia wasbeneficial and had no deleterious effects.
Coronary venous retroperfusion is a particularlyattractive approach when there is poor access toan acutely ischemic region of the heart.27-30 Global in-terruption of coronary venous drainage can be dele-terious and cause a high degree of tissue edema, whichimpedes the retrograde retroperfusion.31 32 Severalinvestigators have used a regionally administered retro-perfusion;33 3" however, the infusion still required per-manent occlusion of the regional coronary vein, pre-cluding appropriate drainage flow. To resolve thislimitation, our SRP system applies retroperfusion indiastole while facilitating coronary venous drainageduring systole.6 I This phasic system appears to min-imize vascular congestion, myocardial edema and
1441
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

VOL 65, No 7, JUNE 1982
El CONTROLS (N-9)
3 HSRP (N= 13)* p<.OOI relative to
control series
NECROTIC ZONE(% of Ischemic zone)
FIGURE 11. Pathologic data on ischemic and necroticzones in a midpapillary level left ventricular slab after 3-hour left anterior descending coronary artery, occlusionwithout and with hypothermic Synchronized retroperfusion(HSRP). Expressed as percent of the slab area, the ischemiczone after 2½12 hours ofHSRP was only slightly reduced butgenerally of a patchy character, compared with a contigu-ous ischemic zone in untreated dogs. Note the dramaticdifference in extent of necrosis, only 7.4 ± 2.7% with HSRPcompared with 47.1 ± 8.9% in untreated control occlusions.
hemorrhages. The benefits demonstrated. in our SRPstudies, have been corroborated37 38 and revealed thatischemic zone myocardial.perfusion is significantly in-creased.39 Retroinfusate penetration into the capillarymicrocirculation was also demonstrated in our studyusing colloidal carbon.The rationale for supplemental myocardial hypo-
thermia was to maintain viability and protect jeopard-ized tissue by reducing cellular metabolism.40 49 Theeffects of myoc'ardial cooling on perfusion, functionand tissue viability have been the subject of intensivestudy, primarily in the arrested heart, in relation to es-tablished cardiac surgical procedures without or withcardioplegic solutions. Profound cooling could lead to
I El CONTROLS (N=9)
E HSRP (N=13)* p < .001 relative to
control series
li
FIGURE 12. Infarct size after 3 hours of left anterior de-scending coronary artery occlusion was 9.3% of the left ven-
tricle in the absence of treatment and presented often as new
transmural necrosis. With hypothermic synchronized retro-perfusion (HSRP) applied between 30 minutes and 3 hoursafter occlusion, the size ofinfarction was less than S% of theleft ventricle, mostly in the subendocardial region.
,J 80'r,< 70u
2 60IL'D 50
O 40
O 30(I)0 20cr-ui 10I0z
0
iH
L] UNTREATED (N- 8)2 HSRP (N=8)* p<05** p<.01 -- .T *I~~~~~~~
C
MID-LV SLAB APICAL SLAB TOTAL LVFIGURE 13. Extent ofnecrosis as percent ofischemic areasin middle and apical left ventricular (L V) slabs, as well as inthe total left ventricle, after 6 hours of untreated or hypo-thermic synchronized retroperfusion (HSRP)-treated cor-onary occlusion. HSRP reduced necrosis significantly in themid-L V slab and in the left ventricle as a whole. Reductionin necrosis by HSRP did not reach significance (comparedwith untreated dogs) in the apical slab.
arrhythmias or result in ventricular fibrillation.49 Withmoderate cooling, heart rate and myocardial oxygenconsumption are reduced.43 7 Contractility and sys-temic vascular resistance might increase as a result of
16 r
14 F
12 F
-loLL-
80
6H
4
2
0
D UNTREATED (N=8)
E HSRP (N=8)* p <.001
*
a-
ISCHEMIA NECROSISFIGURE 14. Size of ischemic and necrotic areas expressedas percent of the left ventricle (L V). As was the case after 3hours occlusion (fig. 15), the ischemic zone was generallypatchy after hypothermic synchronized retroperfusion(HSRP) but not significantly decreased in extent. In con-trast, a significant reduction in necrosis was noted after 6-hour HSRP-treated coronary occlusion. The relatively smallinfarct size in the 6-hour control series (10% of LV) is at-tributable to the site of left anterior descending coronaryartery occlusion and dog-to-dog variability, emphasizing theneed to relate necrosis to the ischemic zone.
100
80
60
40
20
0ISCHEMIC ZONE(/ of Slob area)
10 r
8
6
4
2
0
-^
1442 CIRCULATION
r
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

HYPOTHERMIC RETROPERFUSION/Meerbaum et al.
~~~ ~~ ~~~~ if .z ...X
FIGURE 15. Glycogen-depleted ischemic myocardium afterinfusion of colloidal carbon by means of hypothermic syn-
chronized retroperfusion. Microscopic sections show col-loidal carbon within veins (short arrows) and capillaries(long arrows), providing morphologic confirmation of entryof retroperfusate into the ischemic zone. PAS stain; originalmagnification X 160.
hypothermia,42' 46 and myocardial perfusion increaseor decrease, depending on whether the physiologicstate was normotensive, or else exhibited high heartrates and severely depressed blood pressure.47 48 He-moconcentration has been reported, particularly atprofound levels of global hypothermia.49To clarify the contribution of hypothermia in
HSRP, we repeated, during the course of this investi-gation, a limited SRP study without the cooling. Sig-nificant lowering of heart rates and double product byhypothermia further improved LV function and de-creased myocardial necrosis. The optimal level ofregional hypothermia and mode of retrograde coolingapplication are not known. Treatment effectivenessdepends, of course, on the time it is begun relative tothe progression from reversible to irreversible myo-cardial injury.
System Limitations and Need For DevelopmentSRP catheterization of the coronary sinus and great
cardiac vein is usually completed within 10-15 min-utes, and no serious problems were encountered instudies in about 500 dogs. Insertion of the SRP cath-eter into the regional anterior interventricular veinwas avoided, in view of acute angles and potentialtrauma. Practical anatomic considerations somewhatlimit the specificity of location of the retrograde cor-onary venous infusions. But, while the efficiency ofretrograde delivery to a specific region of the heart isinherently limited, the existence of coronary veno-
venous shunting is useful in distributing flows to differ-
ent regions of the heart and minimizing potentiallydamaging buildup of intravascular pressure. Anischemic zone distal to the left circumflex coronaryartery occlusion can be treated by coronary sinusHSRP. Right coronary occlusions were not studied.The maximal possible efficiency of SRP delivery is
believed to be 50-60%.39 As long as the induced pres-sure and flow within the coronary veins do not exceed50 mm Hg and 80 ml/min, respectively, experience inour laboratory indicates insignificant damage to theheart from SRP. Long-term application of nonsyn-chronized retroperfusion may require maintenance ofeven lower pressures within the coronary veins.50 Themean regional coronary venous pressure during ourstudies was generally less than 30 mm Hg. While cor-onary venous retroinfusion pressures and flows mustbe limited, several investigators have noted a preferen-tial retroinfusate delivery to the ischemic region23 andendocardium '"
Effective diastolic retrograde delivery of hypother-mia into the ischemic myocardium might be achievedthrough intramural channels even in the absenceof transcapillary perfusion. Because of the distribut-ing effects of coronary venovenous shunts, thecooled myocardium encompasses portions of the non-ischemic zone, and ventricular temperature gradientsare thus minimized. Profound HSRP cooling mighthave to be avoided to exclude arrhythmias. Furtherexperimental study should evaluate retrograde hypo-thermia applied after longer periods of coronaryocclusion and during only partly effective interven-tions.
Adequacy of Measurements For Assessment of theInterventionOne of the principal end points of this study was
the extent of necrosis developed within the inducedacutely ischemic territory. Recent histologic and elec-tron microscopic validations in our laboratory,25 con-firm the ability of quantitating the zone of irreversibleinjury with TTC after coronary occlusion periods of 3hours or shorter. Compared with untreated controlswith a similar period and level of coronary occlusion,HSRP generally resulted in only minor necrosis.To avoid dog-to-dog variability and erroneous con-
clusions from experimental studies of proposed treat-ments of acute ischemia, myocardial infarction mustbe related to a zone at risk, usually defined as the areawith a severe perfusion deficit due to coronary ob-struction. The TTC-delineated area of necrosis in LVsections was related to a posttreatment area of myo-cardial glycogen depletion in equivalent adjacentsurfaces. This zone depends on the primary underper-fusion as well as on spontaneous or imposed altera-tions in oxygen demands.8 Glycogen loss is an earlyand reliable index of acute myocardial ischemia and areturn of glycogen is delayed substantially even whenperfusion is reestablished. A practical experimentalmethod has been devised to delineate the zone ofglycogen depletion in LV slabs obtained from treatedor untreated dogs.9 This method is admittedly new andhas not been fully explored. A particular limitation,
1443
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

VOL 65, No 7, JUNE 1982
shared by some other methods, is that measurementsare performed only at the end of the experiment. Ourobservations of a patchy treated vs contiguous un-treated zone of glycogen depletion illustrated thatsuch a delineation may well change due to alterationsin myocardial perfusion or oxygen demands, occur-
ring spontaneously or as a result of treatment. If thesechanges differ widely from dog to dog, then themethod may have serious limitations. In acute experi-ments such as those of the current study, changes inthe supply zone and oxygen demands are relativelysmall, but an optimal technique would establishchanges in the risk zone throughout the study of thetreatment.
Sequential single-plane contrast cineangiographyappeared satisfactory for global measurements of LVfunction. However, the echocardiographic methodwas preferred because it is noninvasive and providescomprehensive imaging of the left ventricle for com-
puter-assisted analysis of ischemic and nonischemicsegments. HSRP significantly improved global LVfunction, although the dysfunction caused by coronaryocclusion was not fully reversed in the 3- or 6-hourperiod. Ischemic segmental function was enhanced byHSRP, whereas in untreated dogs similar segmentsusually remained severely depressed. These 2D echostudies of the extent of dysfunction were compatiblewith autopsy findings.The primary hemodynamic effect of HSRP was
to decrease heart rate and rate-pressure product, as
might be expected with hypothermia alone. HSRP didnot cause arrhythmias, and transient premature ven-tricular complexes encountered in the dogs usually oc-curred shortly after the coronary occlusion, beforetreatment.
Clinical ImplicationsAt this stage of development, HSRP might best be
viewed as an important adjunct of either surgical ornonsurgical reperfusion techniques, which criticallydepend on support of circulation and myocardialpreservation during the earliest phase of acute myo-cardial infarction. An example of the latter is therecently introduced coronary thrombolytic pro-cedure, which may benefit from effective interim sup-port to maintain cardiac function and myocardial via-bility.52
Pharmacologic agents have been combined withSRP treatment53 and a limited experimental study hasdemonstrated that great cardiac vein retroperfusionwith streptokinase resulted in early and reliable lysisof a thrombolotic occlusion within the LAD."HSRP may provide stabilization during threaten-
ing ischemic heart conditions and perioperative orpostsurgical cardiac support. Cardiac derangementsin evolving shock states or arrhythmias might also bealleviated by retrogradely supplying oxygenatedblood, substrates, drugs or hypothermia into the in-volved ischemic segment.
AcknowledgmentThe authors gratefully acknowledge the technical assistance of
Myles Prevost and Xaviar Escudero. We thank Valida Gaskin for
her assistance with pathology studies, Barbara Voigt for secretarialassistance and Jeanne Bloom for editorial assistance.
References1.Abenschein DR, Tacker WA Jr, Babbs CF: Protection of is-
chemic myocardium by whole body hypothermia after cor-onary artery occlusion in dogs. Am Heart J 96: 772, 1978
2. Tyers GFO, Williams EH, Hughes HC, Waldhauser JA: Op-timal myocardial hypothermia at 10 to 15°C. Surg Forum 26:233, 1976
3. Saito Y, Yasutomi N, Nomura Y, Yamamoto T, Sakuyama K,Koide T, Tanimoto M, Yamasaki K, Ohgami T, Ando H,Yamane K, Kawai Y, Ohyanagi M, Iwasaki T, Yorifuji S:Protection of ischemic myocardium by whole-body hypother-mia after acute coronary occlusion in the closed chest dog. JpnCirc J 44: 169, 1980
4. Maroko PR, Libby P, Ginks WR, Bloor CM, Shell WE, SobelBE, Ross J Jr: Coronary artery reperfusion. I. Early effects onlocal myocardial function and the extent of myocardial ne-crosis. J Clin Invest 51: 2710, 1972
5. Reimer KA, Lowe JE, Rasmussen MM, Jennings RB: Thewavefront phenomenon of ischemic cell death. Myocardial in-farct size vs duration of coronary occlusion in dogs. Circula-tion 56: 786, 1977
6. Meerbaum S, Lang TW, Osher JV, Hashimoto K, Lewis GW,Feldstein C, Corday E: Diastolic retroperfusion of acutely is-chemic myocardium. Am J Cardiol 37: 588, 1976
7. Farcot JC, Meerbaum S, Lang TW, Kaplan L, Corday E: Syn-chronized retroperfusion of coronary veins for circulatory sup-port of jeopardized ischemic myocardium. Am J Cardiol 41:1191, 1978
8. Meerbaum S, Uchiyama T, Lang TW, Broffman J, Haend-chen R, Rit J, Fishbein M, Corday E: Reduction of myocardialnecrosis by closed chest regional hypothermic retroperfusionearly after coronary occlusion. (abstr) Circulation 62 (supplIII): III-316, 1980
9. Haendchen R, Aosaki N, Uchiyama T, Escudero X, BroffmanJ: Hypothermic retroperfusion treatment of acute myocardialischemia: effects on cardiac function and infarct size. (abstr)Am J Cardiol 47: 436, 1981
10. Gueret P, Meerbaum S, Wyatt HL, Uchiyama T, Lang TW,Corday E: Two-dimensional echocardiographic quantitation ofleft ventricular volumes and ejection fraction. Importance ofaccounting for dyssynergy in short-axis reconstruction models.Circulation 62: 1308, 1980
11. Fishbein MC, Meerbaum S, Rit J, Lando U, Kanmatsuse K,Mercier JC, Corday E, Ganz W: Early phase acute myocardialinfarct size quantitation: validation of the triphenyl tetrazoli-um chloride tissue enzyme staining technique. Am Heart J 101:593, 1981
12. Sandritter HW, Jestadt R: Triphenyltetrazoiumchlorid (TTC)als Reduktionsindidator zur makroskopischen diagnose desfrischen Herzinfarktes. Verh Dsch Ges Pathol 41: 165, 1958
13. Lie JT, Pairolero PC, Holley KE, Titus JL: Macroscopic en-zyme-mapping verification of large, homogeneous, experi-mental myocardial infarcts of predictable size and location indogs. J Thorac Cardiovasc Surg 65: 599, 1975
14. Meyer DK, Purdy FA: Cardiac glycogen of rats during andfollowing acute anoxia. Am J Physiol 200: 860, 1961
15. Weissler AM, Kruger FA, Baba N, Scarpelli DG, LeightonRF, Gallimore JK: Role of anaerobic metabolism in the preser-vation of functional capacity and structure of anoxic myocar-dium. J Clin Invest 47: 403, 1968
16. Jennings RB, Ganote CE, Reimer KA: Ischemic tissue injury.Am J Pathol 81: 179, 1975
17. Kent SP, Diseker M: Early myocardial ischemia. Study ofhistochemical changes in dogs. Lab Invest 4: 398, 1955
18. Klionsky B: Myocardial ischemia and early infarction. A histo-chemical study. Am J Pathol 36: 575, 1960
19. Sommers HM, Jennings RB: Experimental acute myocardialinfarction. Histologic and histochemical studies of early myo-cardial infarcts induced by temporary or permanent occlusionof a coronary artery. Lab Invest 13: 1491, 1964
20. Fishbein MC, Hare CA, Gissen SA, Spadaro J, Maclean D,Maroko PR: Identification and quantification of histochemicalborder zones during the evolution of myocardial infarction in
1444 CIRCULATION
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

HYPOTHERMIC RETROPERFUSION/Meerbaum et al.
the rat. Cardiovasc Res 19: 41, 198021. Boor PJ, Reynolds ES: A simple planimetric method for deter-
mination of left ventricular mass and necrotic myocardial massin postmortem hearts. Am J Clin Pathol 86: 387, 1977
22. Boor PJ, Reynolds ES: Myocardial infarct size: clinicopatho-logic agreement and discordance. Hum Pathol 6: 685, 1977
23. Meerbaum S, Lang TW, Broffman J, Uchiyama T, Haend-chen R, Povzhitkov M, Corday E: Lysis of a coronary arterythrombus by coronary venous streptokinase retroinfusion.(abstr). Clin Res 28: 222A, 1981
24. Farcot JC, Berdeaux A, Barry M, Rigaud M, Bardet J, Giudi-celli JF, Bourdarias JP: Regional blood flow redistribution bysynchronized retroperfusion (SRP) treatment of acute caninemyocardial ischemia. (abstr) Circulation 62 (suppl III): III-316,1980
25. Delin NA, Pollack L, Kjartansson KB, Worthington GS: Car-diac performance in hypothermia. An experimental study of leftventricular power, oxygen consumption and efficiency in dogs. JThorac Cardiovasc Surg 47: 774, 1964
26. Delin NA, Pollack L, Kgartansson KB, Schenk WG: Cardiacperformance in hypothermia: an experimental study of left ven-tricular power, oxygen consumption and efficiency in dogs. JThorac Cardiovasc Surg 47: 774, 1964
27. Beck CS, Stanton E, Batiuchok W, Leiter E: Revasculariza-tion of the heart by graft of systemic artery into coronary sinus.JAMA 137: 436, 1948
28. Beck CS, Leighniner DS: Operations for coronary artery dis-ease. JAMA 13: 1226, 1954
29. Feil H: Clinical appraisal of the Beck operation. Ann Surg 118:807, 1943
30. Hammond GL, Davies AL, Austen WG Jr: Retrograde cor-onary sinus perfusion: a method of myocardial protection in thedog during left coronary artery occlusion. Ann Surg 166: 39,1967
31. Eckstein RW, Hornberger C, Sano T: Acute effects of ele-vation of coronary sinus pressure. Circulation 7: 422, 1953
32. Bakst AA, Costas-Durieux J, Goldberg H, Bailey CP: Protec-tion of the heart by arterialization of the coronary sinus. II.Coronary flow in dogs with aorto-coronary sinus anastomosis. JThorac Cardiovasc Surg 27: 442, 1954
33. Andreadis P, Natsikas N, Arealis E, Lazarides DP: The aorto-coronary venous anastomosis in experimental acute myocar-dial ischemia. Vasc Surg 8: 45, 1974
34. Bhayana JN, Olsen DB, Bryne JP, Kolff WJ: Reversal of myo-cardial ischemia by arterialization of the coronary vein. JThorac Cardiovasc Surg 67: 125, 1974
35. Benedict JS, Buhl TL, Henney RP: Cardiac vein myocardial re-vascularization. An experimental study and report of 3 clinicalcases. Ann Thorac Surg 20: 550, 1975
36. Gott VL, Gonzales JL, Zuhdi MN, Varco RL, Lillehei CW:Retrograde perfusion of the coronary sinus for direct aortic sur-gery. Surg Gynecol Obstet 104: 319, 1957
37. Gundry SR, Goldfaden DM, Seipp HW, Solomon RE, JonesM: Diastolic retroperfusion of acutely ischemic myocardiumutilizing a balloon tipped coronary vein catheter. (abstr) Cir-culation 62 (suppl III): III-3 16, 1980
38. Smith GT, Geary GG, Blanchard W, McNamara JJ: Reduc-tion in infarct size by synchronized selective coronary venousretroperfusion of arterialized blood. Am J Cardiol 48: 1064,1982
39. Berdeaux A, Farcot JC, Bourdarias JP, Barry M, Bardet J,Giudicelli JF: Effects of diastolic synchronized retroperfusionon regional coronary blood flow in experimental myocardial is-chemia. Am J Cardiol 47: 1033, 1981
40. Freese JW, Lesage AM, Young WG Jr, Sealy WC: The effectof core induced hypothermia of 25 and 7°C on dogs with myo-cardial infarction. Trans Am Soc Artif Intern Organs 6: 218,1960
41. Kuhn LW, Weiser FM, D'Aria J, Apter R: Hemodynamic andmetabolic effects of hypothermia and extracorporeal circula-tion in experimental myocardial infarction and shock. Circ Res10: 916, 1962
42. Kuhn LA, Apter R, Weinrauch H, Jacobson TE, Meltzer L:Hemodynamic and metabolic effects of the skin and blood-stream cooling in experimental myocardial infarction withshock. Am J Cardiol 12: 795, 1963
43. Bergmann SR, Torres JC, Angelakos ET: The effect of mod-erate hypothermia after acute coronary occlusion in dogs. FedProc 36: 620, 1977
44. Moutitzen CV, Anderson MN: Mechanisms of ventricularfibrillation during hypothermia. J Thorac Cardiovasc Surg 51:585, 1966
45. Blair E: Clinical Hypothermia. New York, McGraw-Hill, 196446. Goldberg LI: Effect of hypothermia on contractility of the in-
tact dog heart. Am J Physiol 194: 92, 195847. Hardin RA, Scott JB, Haddy FJ: Effect of cardiac cooling on
coronary vascular resistance in normothermic dogs. Am JPhysiol 199: 163, 1960
48. Mangardi JL, Aiken JE, Behrer A, Foche JE: Coronary bloodflow during moderate and profound hypothermia. J Cardio-vasc Res 6: 349, 1966
49. Rand P, Lacombe E, Hunt H, Austin W: Viscosity of normalhuman blood under normothermic and hypothermic condi-tions. J Appl Physiol 19: 117, 1964
50. Toscano MF, Kampman KM, Beere PA, Bates RJ, Demos SS,Anagnostopoulos CE: Retrograde coronary venous perfusion atlow pressure. Bull Tex Heart Inst 7: 41, 1980
51. Lolley DM, Hewitt RL: Myocardial distribution of asanguine-ous solutions retroperfused under low pressure through the cor-onary sinus. J Cardiovasc Surg 21: 287, 1980
52. Ganz W, Buchbinder N, Marcus H, Mondkar A, Maddahi J,Charuzi Y, O'Connor L, Shell W, Fishbein MC, Kass R,Miyamoto A, Swan HJC: Intracoronary thrombolysis in evolv-ing myocardial infarction. Am Heart J 101: 4, 1981
53. Povzhitkov M, Haendchen RB, Meerbaum S, Fishbein MC, Y-Rit J, Corday, E: Protective effect of coronary venous prosta-glandin E1 retroperfusion during acute myocardial ischemia(abstr). Am J Cardiol. In press
54. Meerbaum S, Povzhitkov M, Haendchen RV, Broffman J,Lang TW, Corday E: Coronary artery thrombolyis by strepto-kinase coronary venous retroinfusion or systemic administra-tion (abstr). Am J Cardiol. In press
1445
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

Uchiyama, N Aosaki and J BroffmanS Meerbaum, R V Haendchen, E Corday, M Povzhitkov, M C Fishbein, J Y-Rit, T W Lang, T
regional myocardial ischemia.Hypothermic coronary venous phased retroperfusion: a closed-chest treatment of acute
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1982 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.65.7.1435
1982;65:1435-1445Circulation.
http://circ.ahajournals.org/content/65/7/1435the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from