Hypolipidemic Drugs. HYPERLIPIDEMIA Plasma lipids are transported in complexes called lipoproteins....
20
Hypolipidemic Drugs
-
Upload
douglas-kelley -
Category
Documents
-
view
219 -
download
0
Transcript of Hypolipidemic Drugs. HYPERLIPIDEMIA Plasma lipids are transported in complexes called lipoproteins....

Hypolipidemic Drugs

HYPERLIPIDEMIA
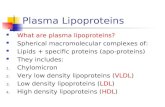
Plasma lipids are transported in complexes called lipoproteins.
Metabolic disorders that involve elevations in any lipoprotein species are termed hyperlipoproteinemias or hyperlipidemias.
Hyperlipemia: indicates increased levels of triglycerides.

HYPERLIPIDEMIA
The two major clinical sequelae of hyperlipidemias Atherosclerosis: Atherosclerosis is the
leading cause of death for both genders in the USA and other Western countries.
Acute pancreatitis: Occurs in patients with marked hyperlipemia. Control of triglycerides can prevent recurrent attacks of this life-threatening disease.

Atherosclerosis Lipoproteins that contain apolipoprotein (apo) B-100 carry lipids into the
artery wall. These are low-density lipoproteins (LDL), intermediate-density lipoproteins (IDL), very-low-density lipoproteins (VLDL), and lipoprotein(a) (Lp[a]).
Cellular components in atherosclerotic plaques include foam cells, which are transformed macrophages and smooth muscle cells filled with cholesteryl esters.
These cellular alterations result from endocytosis of modified lipoproteins via at least four species of scavenger receptors.
Chemical modification of lipoproteins by free radicals creates ligands for these receptors.
The atheroma growth: the accumulation of foam cells, collagen, fibrin, and frequently calcium. slowly occlude coronary vessels, rupture of unstable atheromatous plaques, activation of platelets and formation of occlusive thrombi.
The leading cause of death.!!

Atherosclerosis
High-density lipoproteins (HDL) exert several anti atherogenic effects.
They participate in removing of cholesterol from the artery wall and inhibit the oxidation of atherogenic lipoproteins.
Low levels of HDL (hypoalphalipoproteinemia) are an independent risk factor for atherosclerotic disease.
Cigarette smoking is a major risk factor for coronary disease. It is associated with; reduced levels of HDL, inhibiting of cholesterol removal from the artery wall, cytotoxic effects on the endothelium, increased oxidation of lipoproteins, and stimulation of thrombogenesis.
Diabetes, also a major risk factor, is another source of oxidative stress.

Atherosclerosis Normal coronary arteries can dilate in response to ischemia,
increasing delivery of oxygen to the myocardium. This process is mediated by nitric oxide, acting upon smooth muscle
cells of the arterial media. This function is impaired by atherogenic lipoproteins, thus
aggravating ischemia. Reducing levels of atherogenic lipoproteins and inhibiting their
oxidation restores endothelial function. Because atherogenesis is multifactorial, therapy should be directed
toward all modifiable risk factors. Atherogenesis is a dynamic process. Quantitative angiographic trials have demonstrated net regression
of plaques during aggressive lipid-lowering therapy. Clinical trials have shown significant reduction in mortality from new
coronary events and in all-cause mortality.

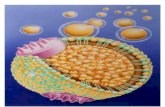
Schematic Illustration of a Lipoprotein Particle
TG: TrigiglyceridesCE: Cholesteryl esthers
Lipoproteins have hydrophobic core regions containing cholesteryl esters and triglycerides surrounded by unesterified cholesterol, phospholipids, and apoproteins. Certain lipoproteins contain very high-molecular-weight apoproteins (B type) that exist in two forms: B-48, formed in the intestine and found in chylomicrons and their remnants; and B-100, synthesized in liver and found in VLDL, VLDL remnants (IDL), LDL (formed from VLDL), and Lp(a) lipoproteins.



apo C

THE PRIMARY HYPERTRIGLYCERIDEMIAS
Hypertriglyceridemia is associated with increased risk of coronary disease.
VLDL and IDL have been found in atherosclerotic plaques. These patients tend to have cholesterol-rich VLDL of small particle
diameter. Hypertriglyceridemic patients with coronary disease or risk
equivalents should be treated aggressively. Patients with triglycerides above 700 mg/dL should be treated to
prevent acute pancreatitis because the LPL clearance mechanism is saturated at about this level.

Primary Chylomicronemia
Chylomicrons are not present in the serum of normal individuals who have fasted 10 hours.
The recessive traits of deficiency of lipoprotein lipase or its cofactor are usually associated with severe lipemia (2000-2500 mg/dL of triglycerides when the patient is consuming a typical American diet).
These disorders might not be diagnosed until an attack of acute pancreatitis occurs.
Patients may have eruptive xanthomas, hepatosplenomegaly, hypersplenism, and lipid-laden foam cells in bone marrow, liver, and spleen.
Marked restriction of total dietary fat is the basis of effective long-term treatment.
Niacin or a fibrate may be of some benefit if VLDL levels are increased.




DRUGS USED IN HYPERLIPIDEMIA
HMG-CoA reductase inhibitorsLovastatin, atorvastatin, fluvastatin,
pravastatin, simvastatin, rosuvastatin Niacin Fibric Acid Derivatives
Gemfibrozil, fenofibrate, clofibrate Bile acid-binding Resins
Colestipol, cholestyramine, colesevelam Inhibitors of Intestinal sterol absorption
Ezetimibe

HMG-CoA reductase inhibitors(3-Hydroxy-3-methylglutaryl-coenzyme A )
These compounds are structural analogs of HMG-CoA.
They are most effective in reducing LDL. Other effects include decreased oxidative stress
and vascular inflammation with increased stability of atherosclerotic lesions.
It has become standard practice to initiate reductase inhibitor therapy immediately after acute coronary syndromes, irrespective of lipid levels.

HMG-CoA reductase inhibitors(3-Hydroxy-3-methylglutaryl-coenzyme A )
Reductase inhibitors are useful alone or with resins, niacin, or ezetimibe in reducing levels of LDL.
Women who are pregnant, lactating, or likely to become pregnant should not be given these agents.
Use in children is restricted to those with special indications (homozygous familial hypercholesterolemia, heterozygous familial hypercholesterolemia).
Elevations of serum aminotransferase activity (up to three times normal) occur in some patients. Sign of hepatotoxicity.

Inhibitors of Intestinal sterol absorption Ezetimibe is the first member of a group of drugs that
inhibit intestinal absorption of phytosterols and cholesterol.
Its primary clinical effect is reduction of LDL levels. Ezetimibe is a selective inhibitor of intestinal absorption
of cholesterol and phytosterols. A transport protein, NPC1L1, appears to be the target of
the drug. It is effective even in the absence of dietary cholesterol
because it inhibits reabsorption of cholesterol excreted in the bile.
Average reduction in LDL cholesterol with ezetimibe alone in patients with primary hypercholesterolemia is about 18%, with minimal increases in HDL cholesterol.
Ezetimibe is synergistic with reductase inhibitors, producing decreases as great as 25% in LDL cholesterol.

Acronyms Apo Apolipoprotein CETP Cholesteryl ester transfer protein CK Creatine kinase HDL High-density lipoproteins HMG-CoA 3-Hydroxy-3-methylglutaryl-coenzyme A IDL Intermediate-density lipoproteins LCAT Lecithin:cholesterol acyltransferase LDL Low-density lipoproteins Lp(a) Lipoprotein(a) LPL Lipoprotein lipase PPAR-a Peroxisome proliferator-activated receptor-
alpha VLDL Very-low-density lipoproteins