
Hypofractionated Radiotherapy for breast cancer: Updated .... DR TABASSUM... · Associate Professor...
36
Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial Centre Mumbai, INDIA 2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 [email protected]
Transcript of Hypofractionated Radiotherapy for breast cancer: Updated .... DR TABASSUM... · Associate Professor...
Hypofractionated Radiotherapy for breast cancer: Updated evidence
Tabassum Wadasadawala Associate Professor of Radiation Oncology
Tata Memorial Centre
Mumbai, INDIA
2rd Bangladesh Breast Cancer Conference, Dhaka, December 2017
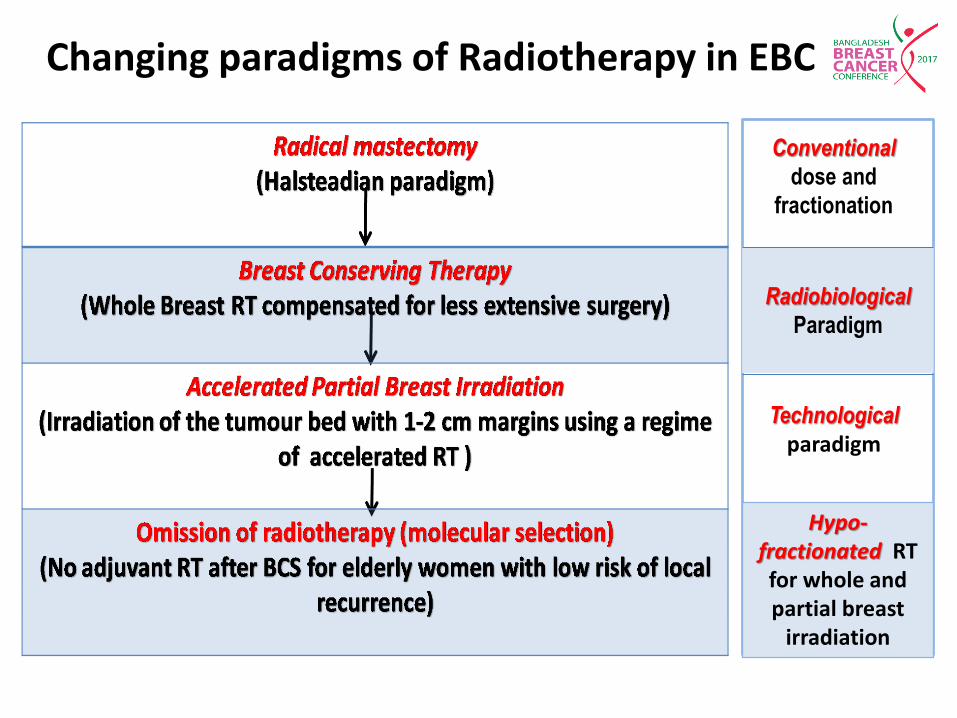
Changing paradigms of Radiotherapy in EBC
Radiobiological
Paradigm
Technological
paradigm
Hypo-fractionated RT for whole and partial breast
irradiation
Conventional
dose and
fractionation
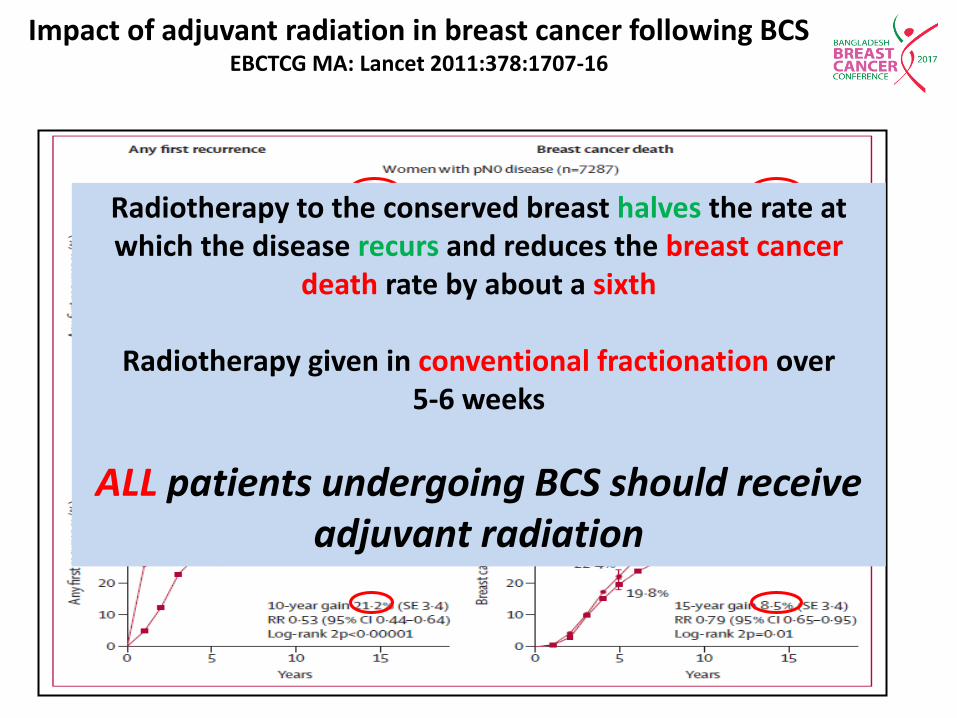
Impact of adjuvant radiation in breast cancer following BCS EBCTCG MA: Lancet 2011:378:1707-16
Radiotherapy to the conserved breast halves the rate at which the disease recurs and reduces the breast cancer
death rate by about a sixth
Radiotherapy given in conventional fractionation over 5-6 weeks
ALL patients undergoing BCS should receive adjuvant radiation
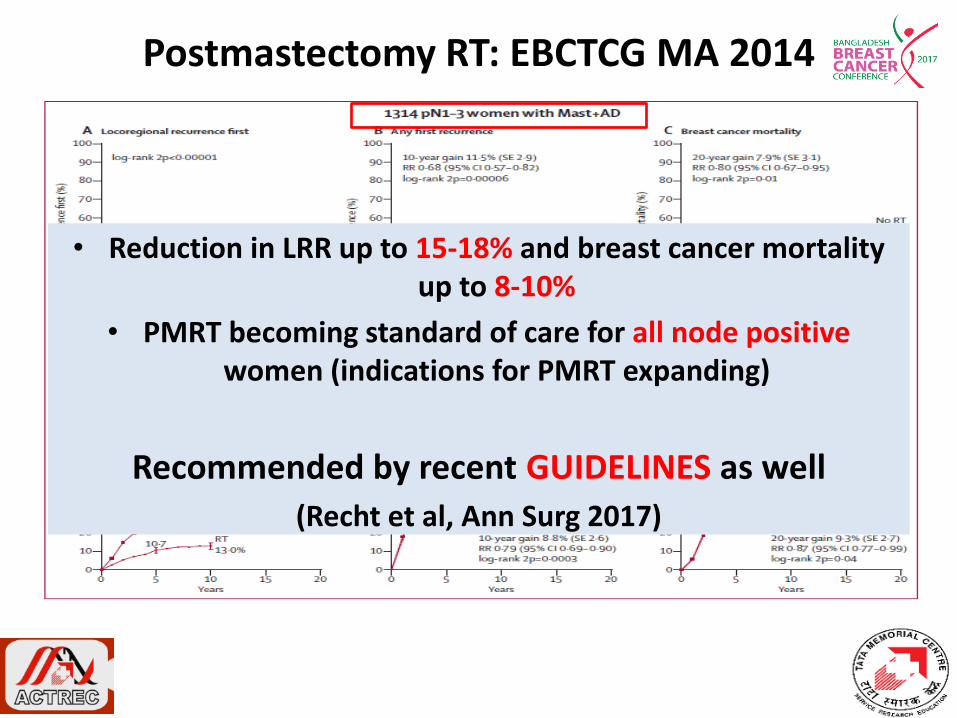
Postmastectomy RT: EBCTCG MA 2014
• Reduction in LRR up to 15-18% and breast cancer mortality up to 8-10%
• PMRT becoming standard of care for all node positive women (indications for PMRT expanding)
Recommended by recent GUIDELINES as well
(Recht et al, Ann Surg 2017)
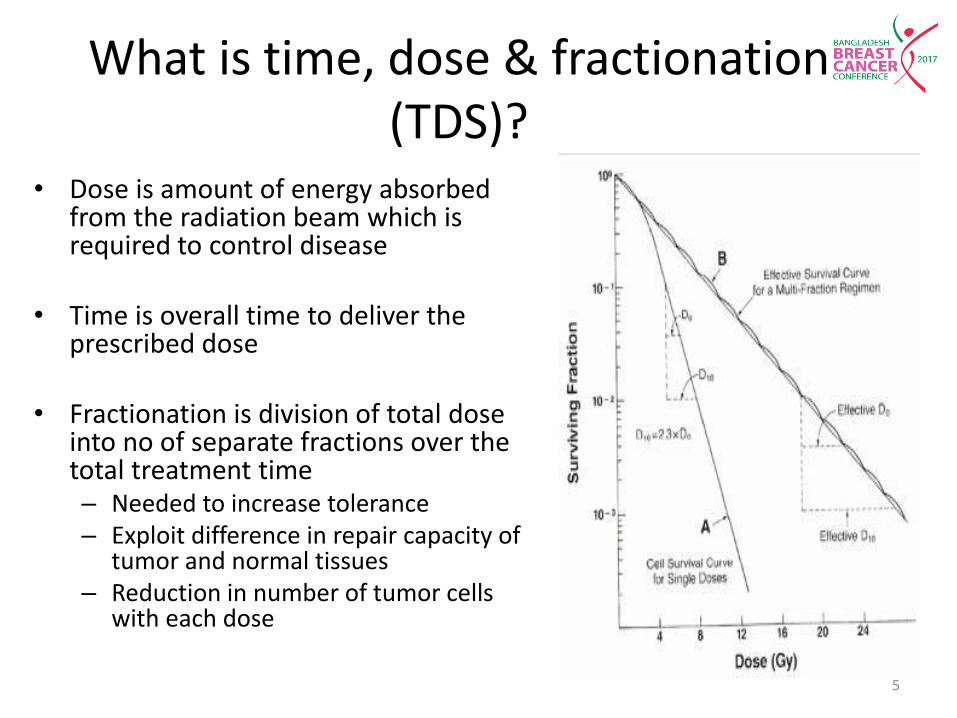
What is time, dose & fractionation (TDS)?
• Dose is amount of energy absorbed from the radiation beam which is required to control disease
• Time is overall time to deliver the prescribed dose
• Fractionation is division of total dose
into no of separate fractions over the total treatment time – Needed to increase tolerance – Exploit difference in repair capacity of
tumor and normal tissues – Reduction in number of tumor cells
with each dose
5
Conventional Hypofractionation
• Daily , 5-6 weeks
• 5 fractions per week
• 1.8-2.0 Gy per fraction
• Pros and cons:
– Effective (most commonly practiced)
– Evidence based
– Inconvenient (5-6 weeks)
– Significant acute/late toxicity
• Daily, 2-4 weeks
• 2-5 fractions per week
• >2 Gy per fraction
• Reduction in total dose
• Pros and cons:
– Shortening of overall treatment time
– Resource sparing
– Cost effective
– Less acute and late toxicity
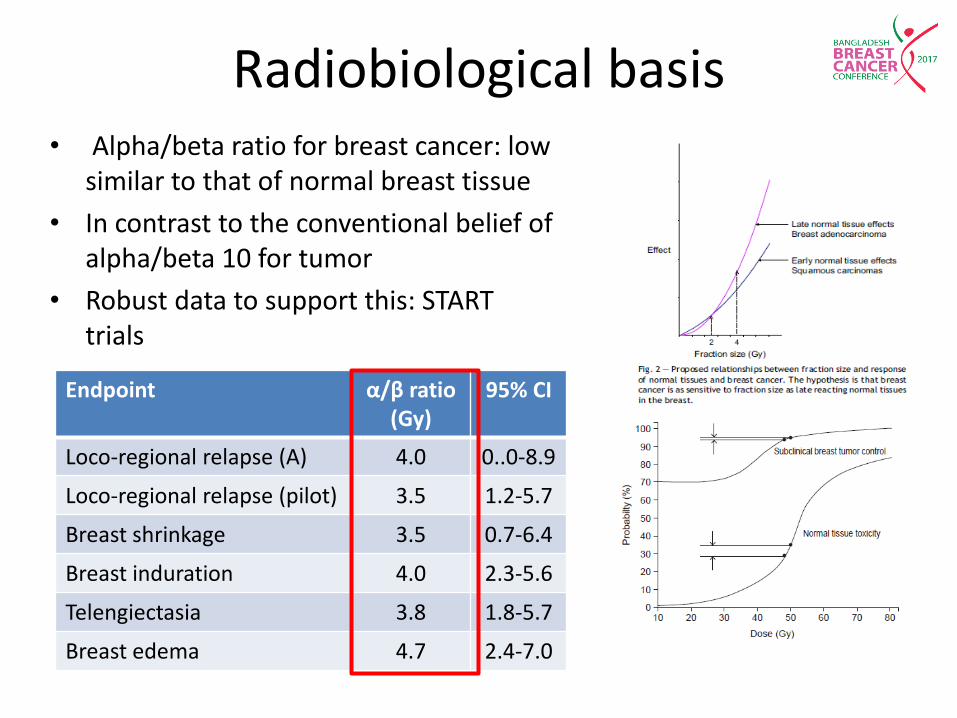
Radiobiological basis • Alpha/beta ratio for breast cancer: low
similar to that of normal breast tissue
• In contrast to the conventional belief of alpha/beta 10 for tumor
• Robust data to support this: START trials
Endpoint α/β ratio (Gy)
95% CI
Loco-regional relapse (A) 4.0 0..0-8.9
Loco-regional relapse (pilot) 3.5 1.2-5.7
Breast shrinkage 3.5 0.7-6.4
Breast induration 4.0 2.3-5.6
Telengiectasia 3.8 1.8-5.7
Breast edema 4.7 2.4-7.0
When, Whom & How
• Hypofractionated radiotherapy: – Whole breast
– Partial breast
– Simultaneous integrated boost
• Accelerated partial breast irradiation: – Interstitial brachytherapy
– External beam
– Intra-operative
– Balloon brachytherapy
8
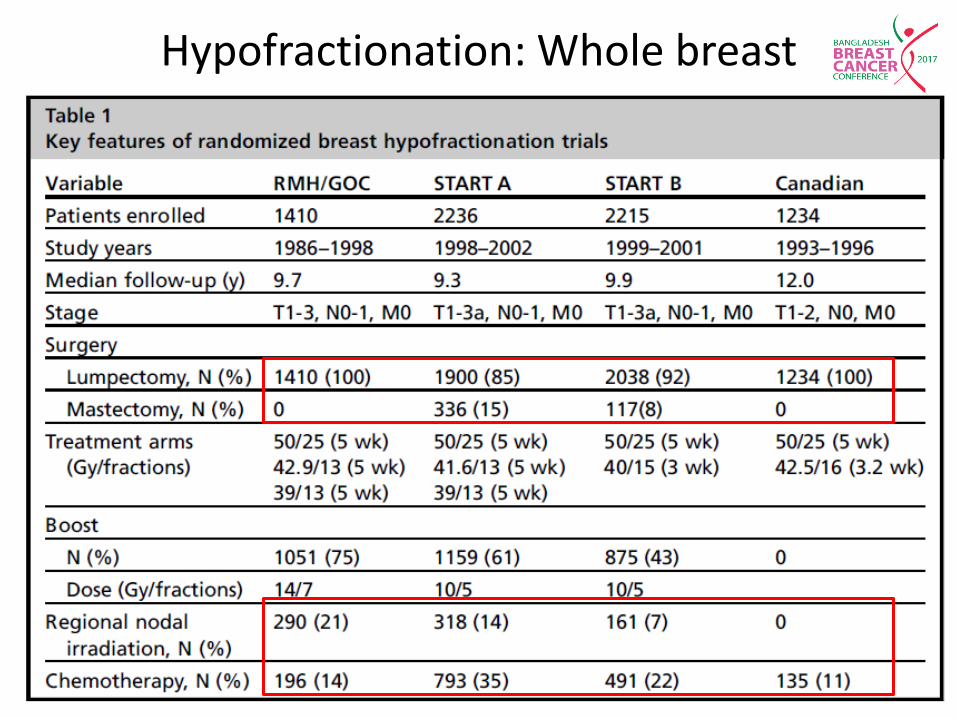
Hypofractionation: Whole breast
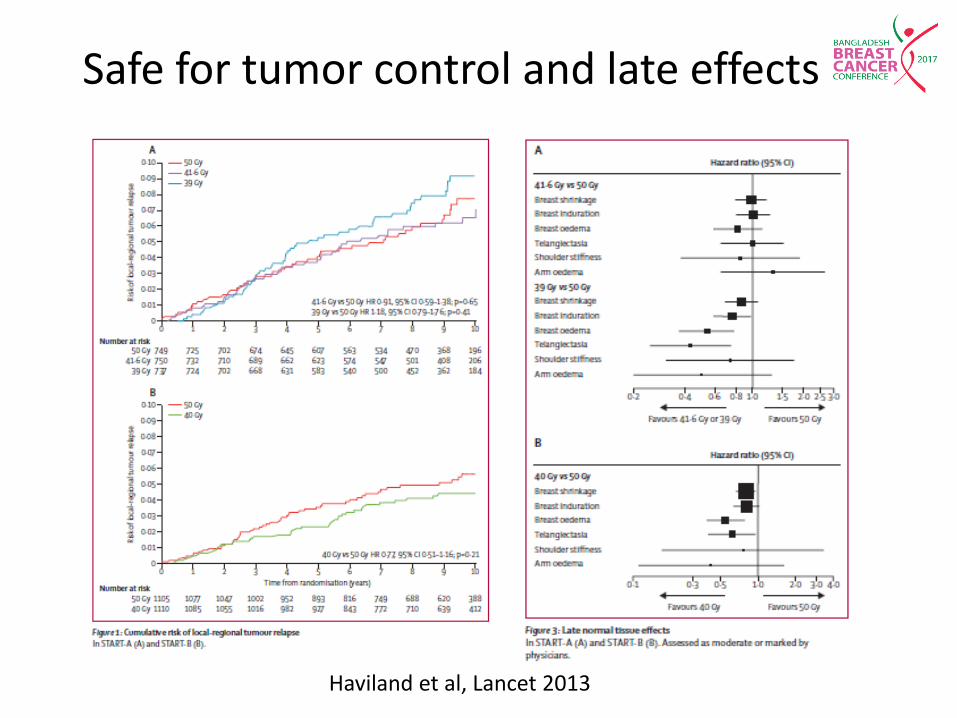
Safe for tumor control and late effects
Haviland et al, Lancet 2013
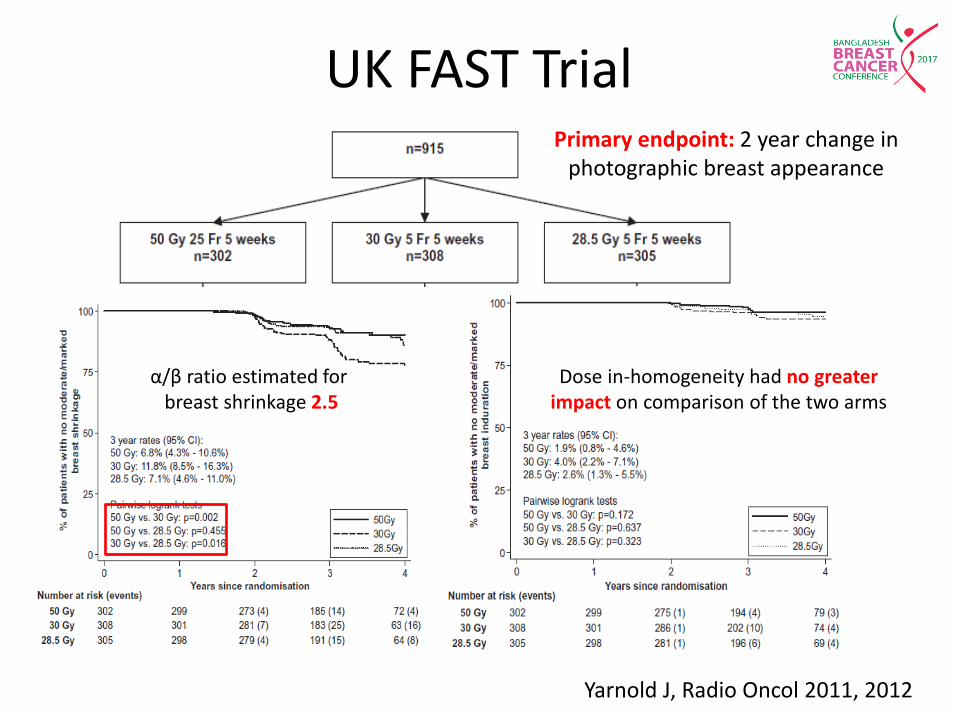
UK FAST Trial
Yarnold J, Radio Oncol 2011, 2012
α/β ratio estimated for breast shrinkage 2.5
Dose in-homogeneity had no greater impact on comparison of the two arms
Primary endpoint: 2 year change in photographic breast appearance
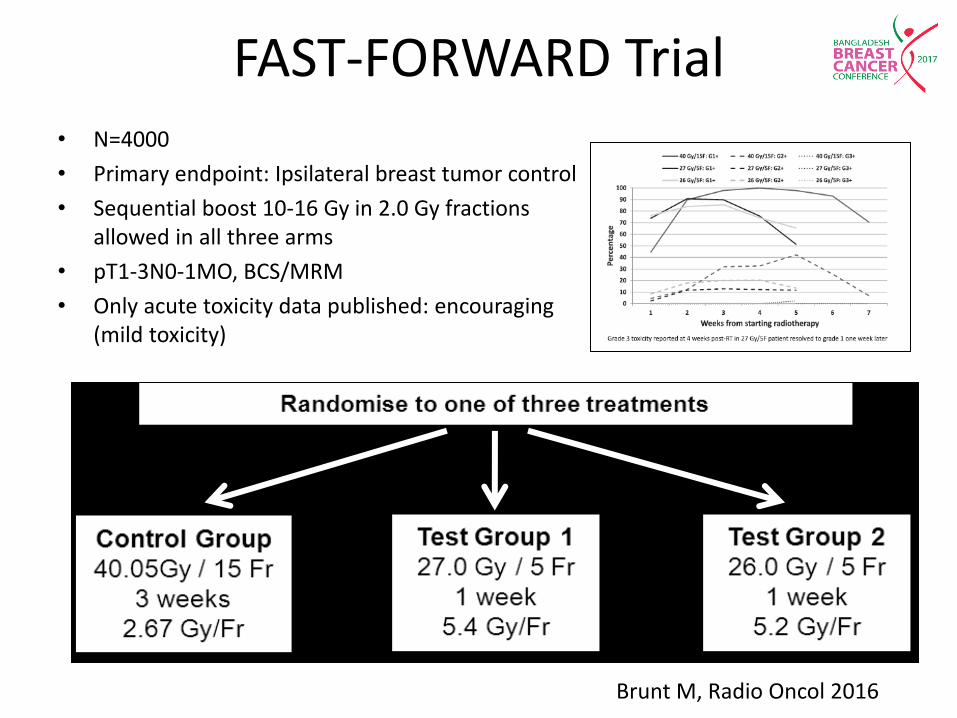
FAST-FORWARD Trial • N=4000
• Primary endpoint: Ipsilateral breast tumor control
• Sequential boost 10-16 Gy in 2.0 Gy fractions allowed in all three arms
• pT1-3N0-1MO, BCS/MRM
• Only acute toxicity data published: encouraging (mild toxicity)
Brunt M, Radio Oncol 2016
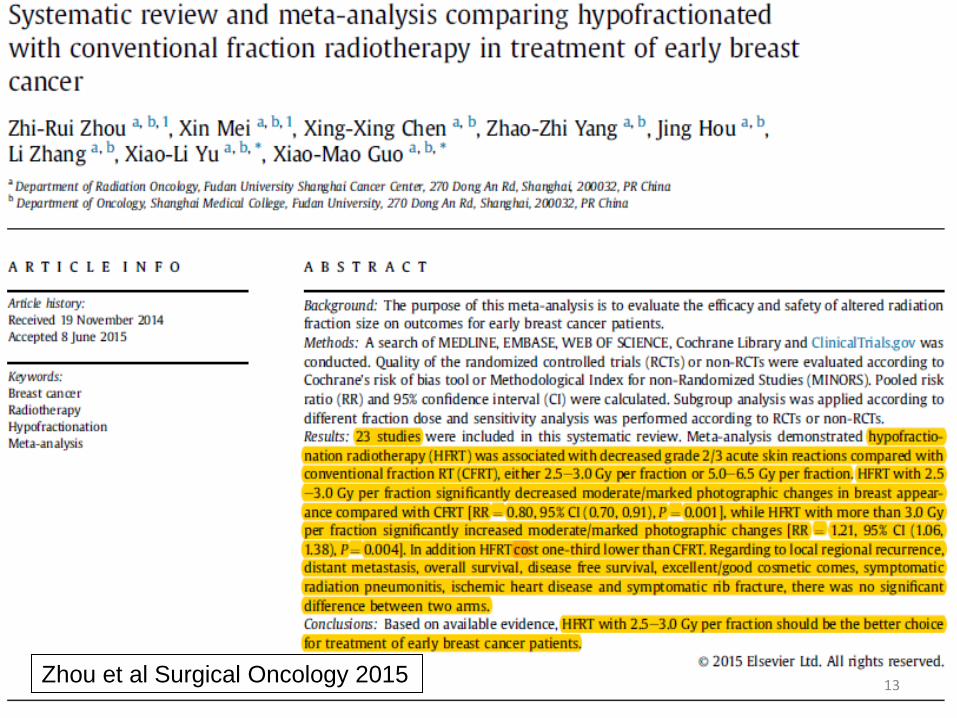
Zhou et al Surgical Oncology 2015 13
Concerns with hypo-fractionation • Recommends HFRT for ≥ 50 years, BCS, T1-2N0, not
receiving chemotherapy
• ‘Choosing Wisely’ campaign by the ASTRO • Is HFRT safe for:
– Young women – High grade tumors – Large breast size – Patients receiving systemic chemotherapy – Pure DCIS – Regional nodal irradiation – Post-mastectomy women – Lung and heart
14
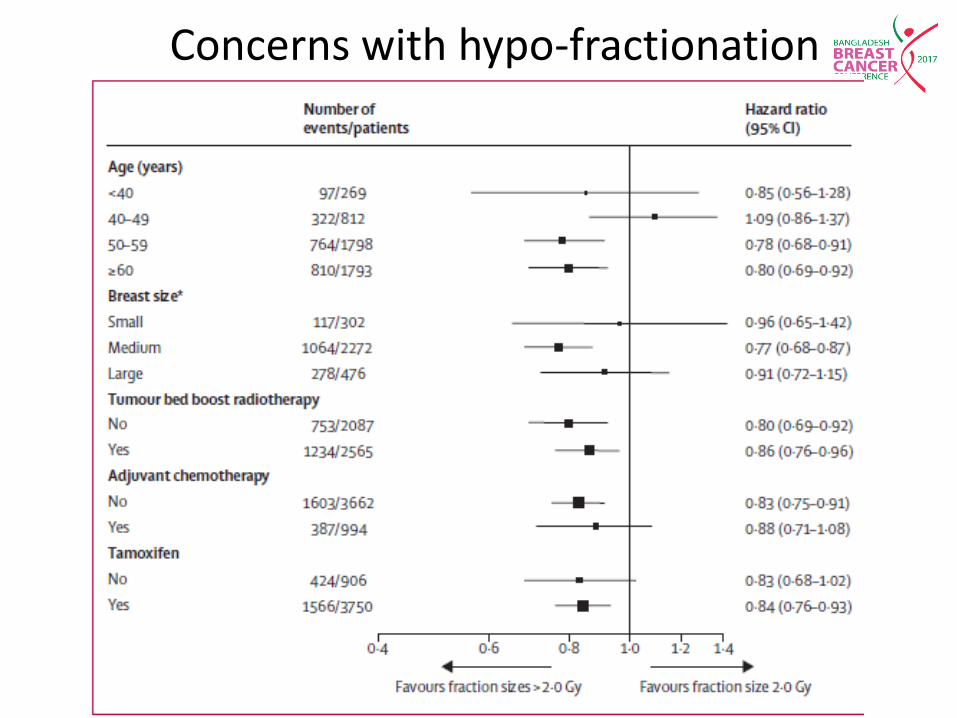
Concerns with hypo-fractionation
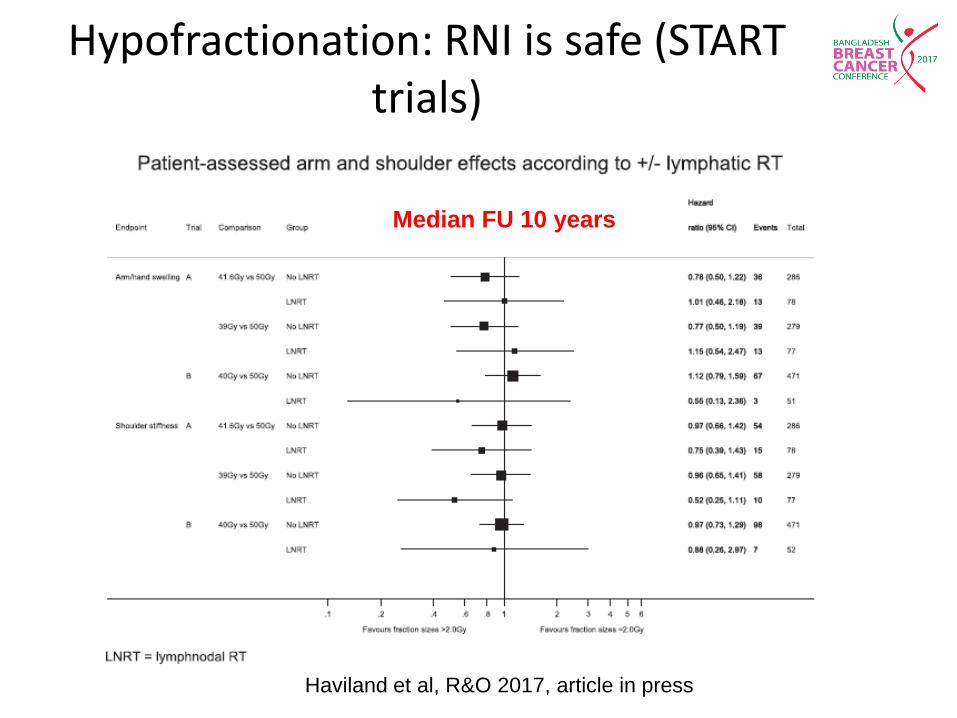
Hypofractionation: RNI is safe (START trials)
Haviland et al, R&O 2017, article in press
Median FU 10 years
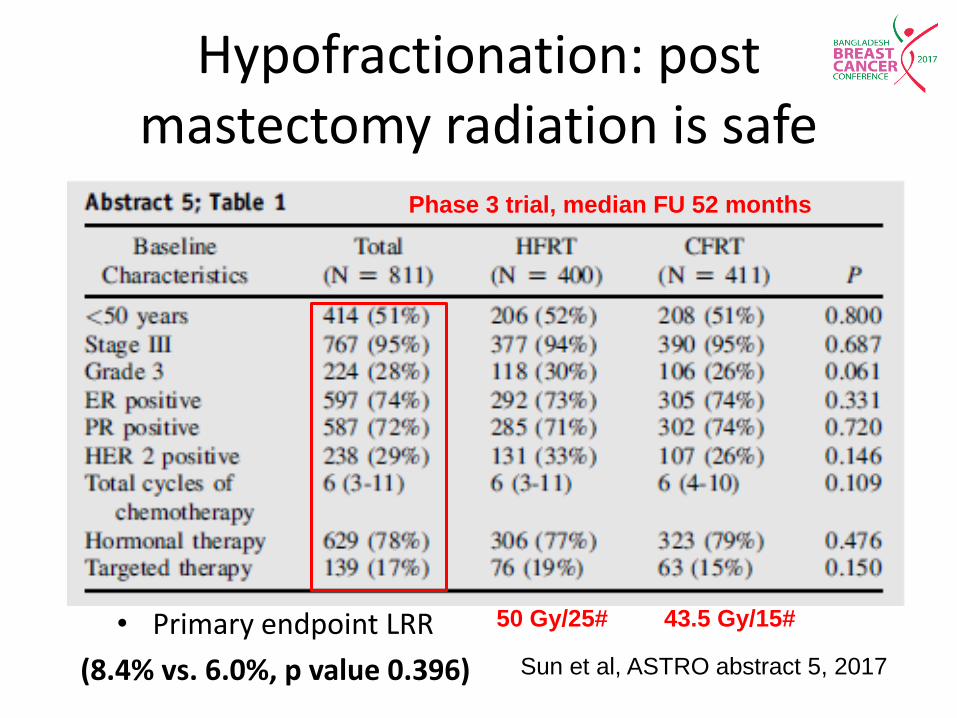
Hypofractionation: post mastectomy radiation is safe
Sun et al, ASTRO abstract 5, 2017
Phase 3 trial, median FU 52 months
50 Gy/25# 43.5 Gy/15# • Primary endpoint LRR
(8.4% vs. 6.0%, p value 0.396)
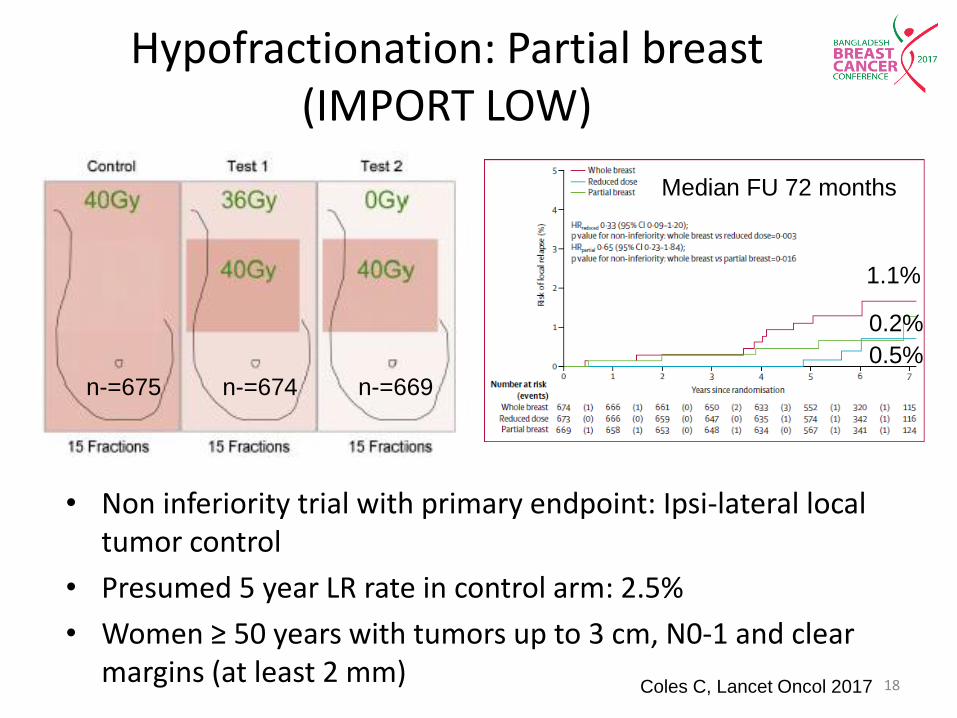
Hypofractionation: Partial breast (IMPORT LOW)
• Non inferiority trial with primary endpoint: Ipsi-lateral local tumor control
• Presumed 5 year LR rate in control arm: 2.5%
• Women ≥ 50 years with tumors up to 3 cm, N0-1 and clear margins (at least 2 mm)
Coles C, Lancet Oncol 2017 18
n-=675 n-=674 n-=669
1.1%
0.2%
0.5%
Median FU 72 months
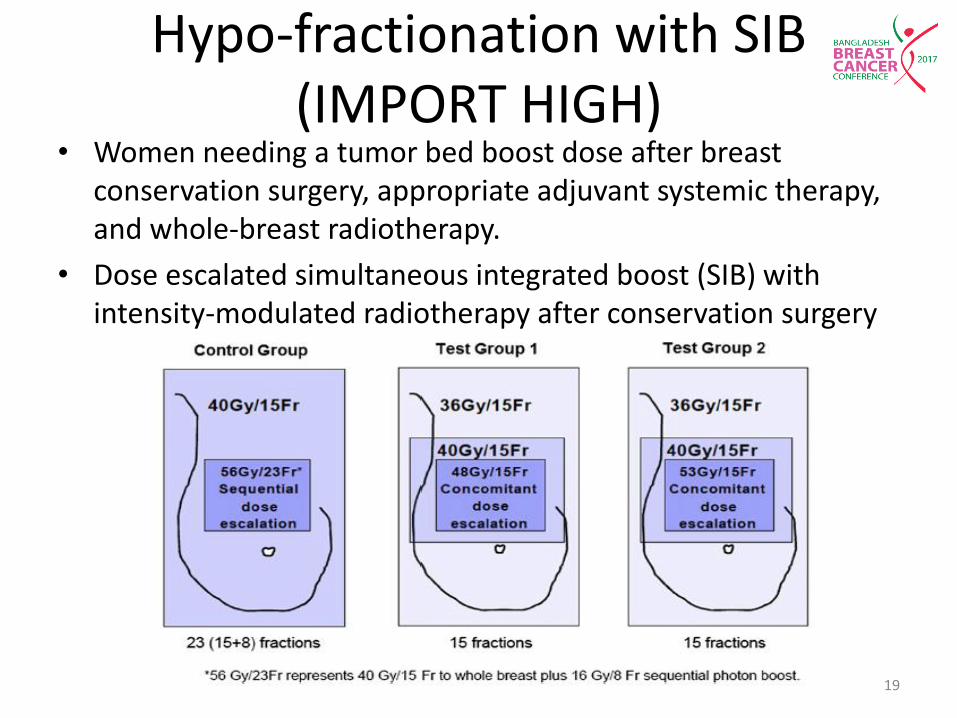
Hypo-fractionation with SIB (IMPORT HIGH)
• Women needing a tumor bed boost dose after breast conservation surgery, appropriate adjuvant systemic therapy, and whole-breast radiotherapy.
• Dose escalated simultaneous integrated boost (SIB) with intensity-modulated radiotherapy after conservation surgery
19

Conclusions: Hypofractionation
• Hypo-fractionation is here to stay
• Safe
• Effective
• Randomized studies confirm α∕β ratios between 3-4
• However, it is also advisable to evaluate the safety of this approach in our own patient population
20
Rationale for Accelerated Partial Breast Irradiation: 15-30% drop out rate after BCT
• Lack of commitment to usual 5-6 weeks course of adjuvant RT
• Lack of access (distance, transport) (Athas et al: JNCI 92:269-271, 2000)
• Logistics (ambulatory status, social support, temporary loss of employment)
• Prolonged waiting time
• Physician bias
• Availability of expertise & facility
• Cost
• Patient age (Ballard et al: JNCI 88:716-725, 1996)
• Fear of radiation treatment
Women opt for mastectomy though eligible for BCS or never receive RT after BCS even in the west
Lazovich DA, JAMA, 1991
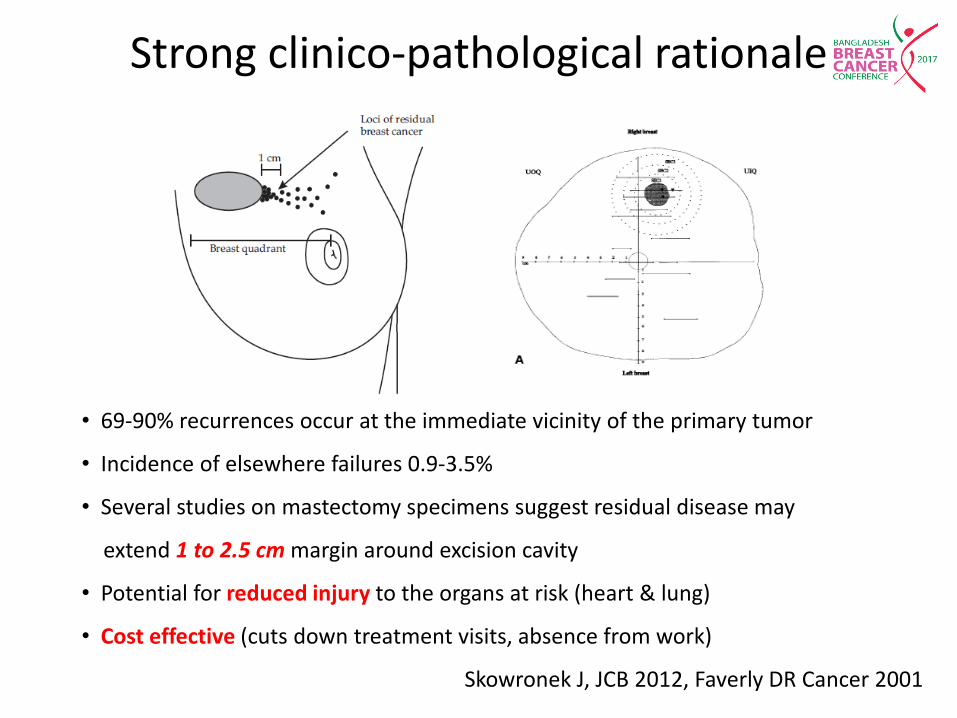
Strong clinico-pathological rationale
• 69-90% recurrences occur at the immediate vicinity of the primary tumor
• Incidence of elsewhere failures 0.9-3.5%
• Several studies on mastectomy specimens suggest residual disease may
extend 1 to 2.5 cm margin around excision cavity
• Potential for reduced injury to the organs at risk (heart & lung)
• Cost effective (cuts down treatment visits, absence from work)
Skowronek J, JCB 2012, Faverly DR Cancer 2001
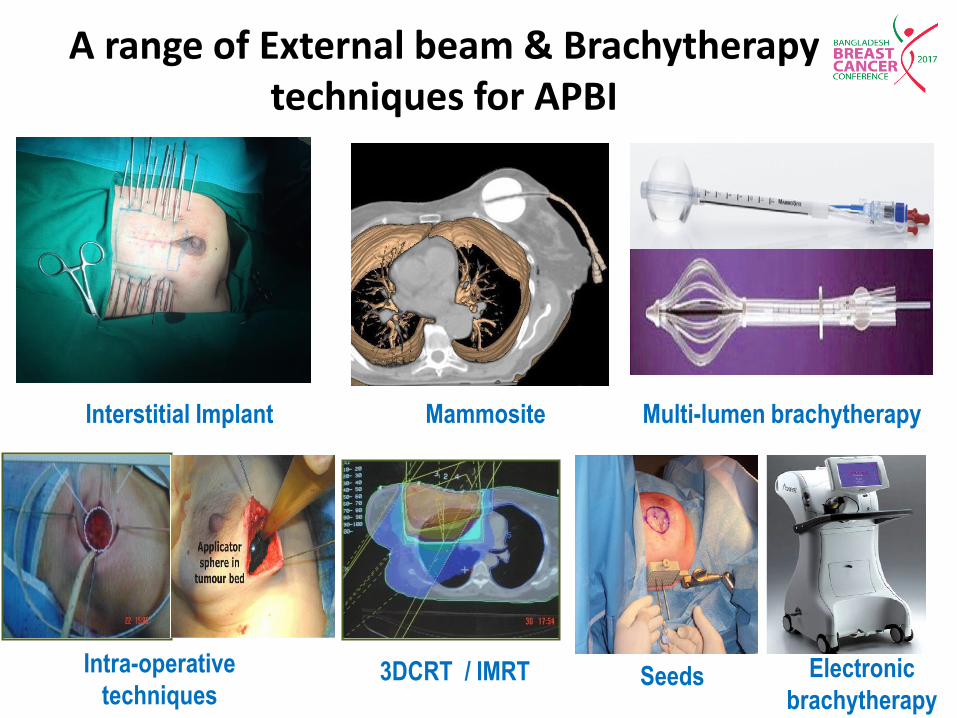
Interstitial Implant Mammosite Multi-lumen brachytherapy
Intra-operative
techniques 3DCRT / IMRT
A range of External beam & Brachytherapy techniques for APBI
Seeds Electronic
brachytherapy

APPROPRIATE SELECTION OF TECHNIQUE AND CASE: CRITICAL
R SARIN, NATURE CLINICAL PRACTICE ONCOLOGY, 2005
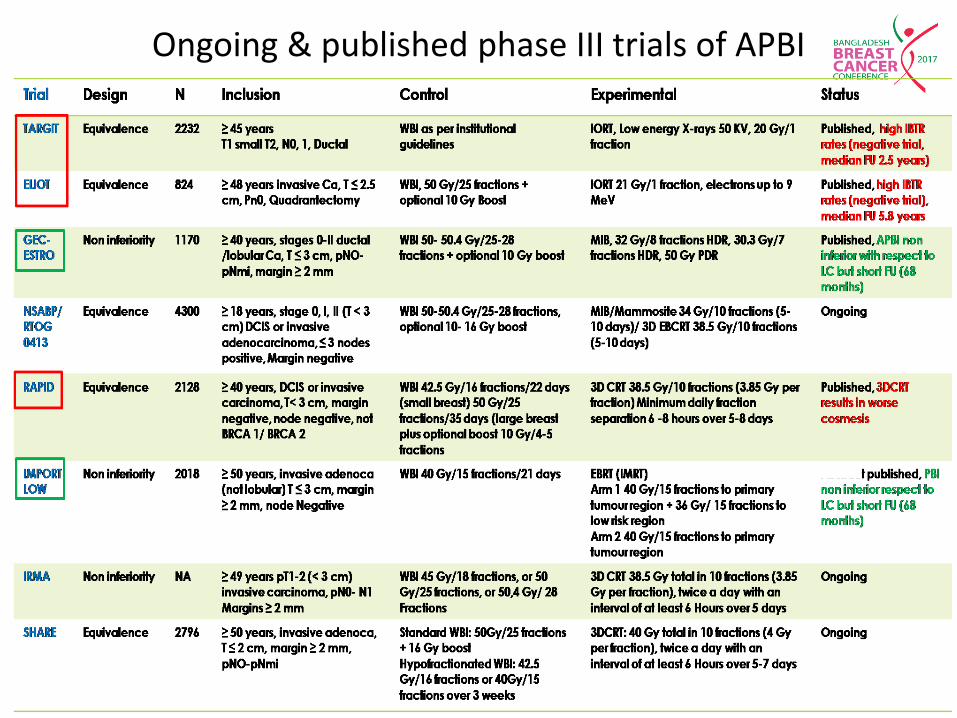
Ongoing & published phase III trials of APBI

APBI: RECOMMENDATIONS

Author (ref) N Technique Median FU
(months)
Tsize
(Median)
Histology ASTRO CS group (Percent/LR) p value
Suitable Cautionary Unsuitable
Ferraro DJ,
2012
202 IBT 64 1.0 cm IDC/DCIS/
ILC
28.7% 51.5% 19.8% NS at 5 years, ASTRO
CS failed to predict LR,
LRR or DFS Overall 3.0%
Wilkinson
JB*, 2012
1813 All except
IORT
60.6 1.0 cm IDC/DCIS 36.5%
2.5%
46.9%
3.3%
16.7%
4.6%
NS at 5 years
Vicini FA
2011
199 IBT 133 NR IDC 47.7%
2.6%
31.7%
7.8%
20.6%
2.5%
NS at 10 years,
ASTRO CS did
not predict LR MacHaffie DR,
2011
136 MammoSite 60 1.0 cm IDC/DCIS
24.6%
1.6%
42.2%
4.8%
33.2%
6.6%
NS at 5 years
TMH, 2014 112 IBT 125 2.0 cm IDC 24.5%
0.0%
59.8%
7.4%
15.7%
6.2%
10 year LR not as
per ASTRO CS
group
ASTRO-CS (TMH data): Does not predict risk of LR
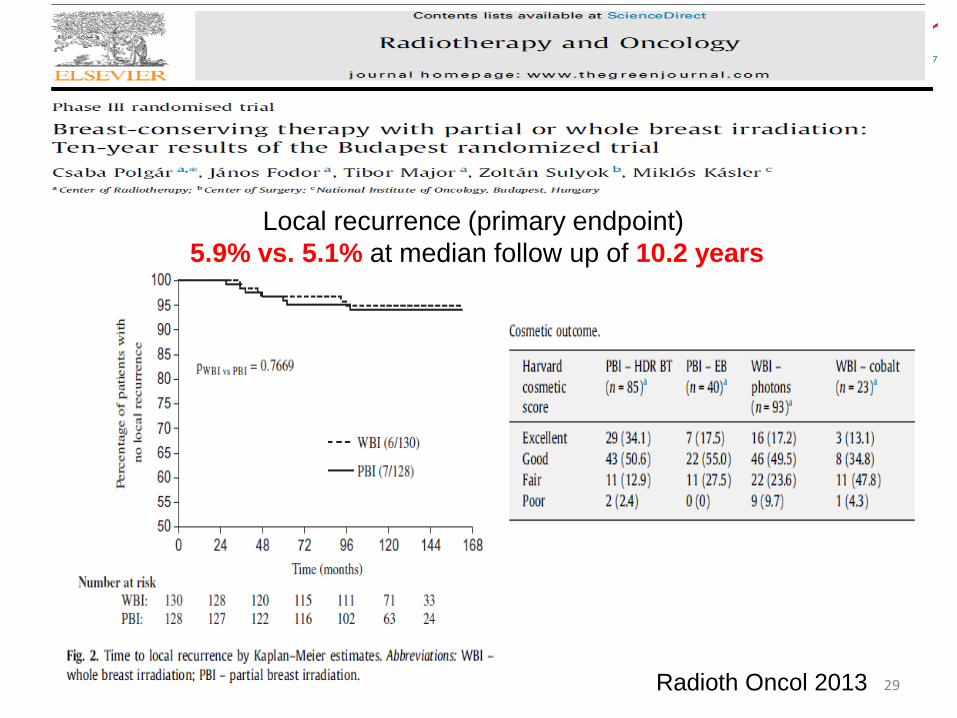
Radioth Oncol 2013 29
Local recurrence (primary endpoint)
5.9% vs. 5.1% at median follow up of 10.2 years
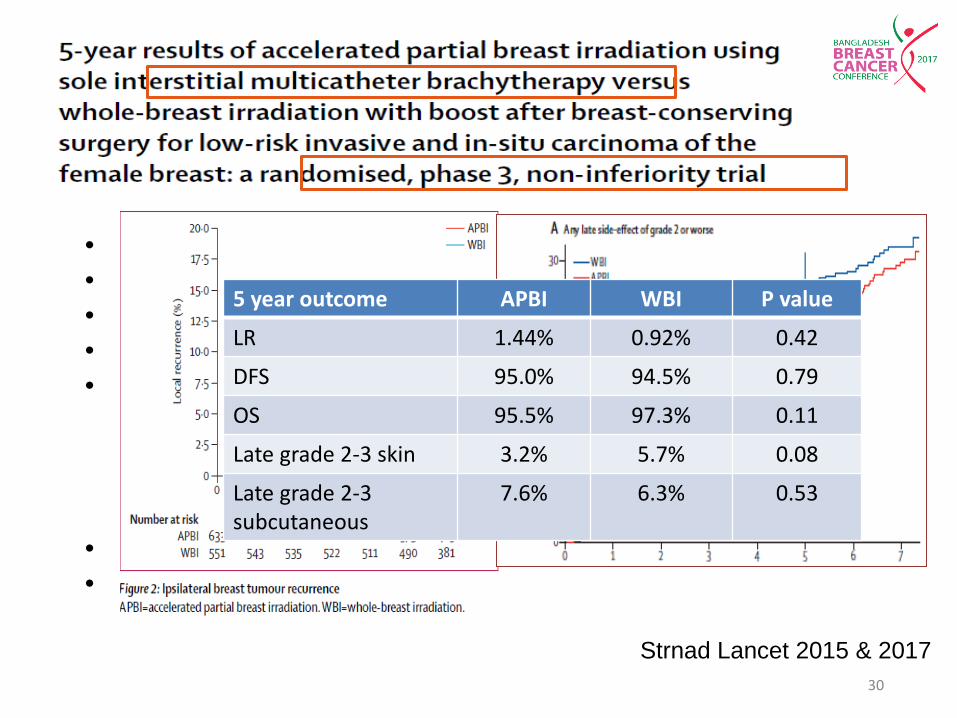
• N=1184, • Duration: 2004-2009 • GEC-ESTRO Study • Conventional WBI + TBB vs. APBI using exclusively MIB • Inclusion criteria:
– ≥40 yrs, pTis or pT1–2a (≤3 cm diameter), – pN0/pNmi, and M0 – Local excision least 2 mm margins (ILC or DCIS, at least 5 mm), – No LVSI
• Median follow-up was 6.6 yrs • Median age 62 years
Strnad Lancet 2015 & 2017
30
5 year outcome APBI WBI P value
LR 1.44% 0.92% 0.42
DFS 95.0% 94.5% 0.79
OS 95.5% 97.3% 0.11
Late grade 2-3 skin 3.2% 5.7% 0.08
Late grade 2-3 subcutaneous
7.6% 6.3% 0.53

• 4 studies 5415patients (2 RCTs and 2 non-RCTs)
• IBTR significantly higher IORT vs WBI (RR 2.83)
• Overall mortality did not differ significantly
• Prudent selection of suitable patients with low risk of LR necessary
31
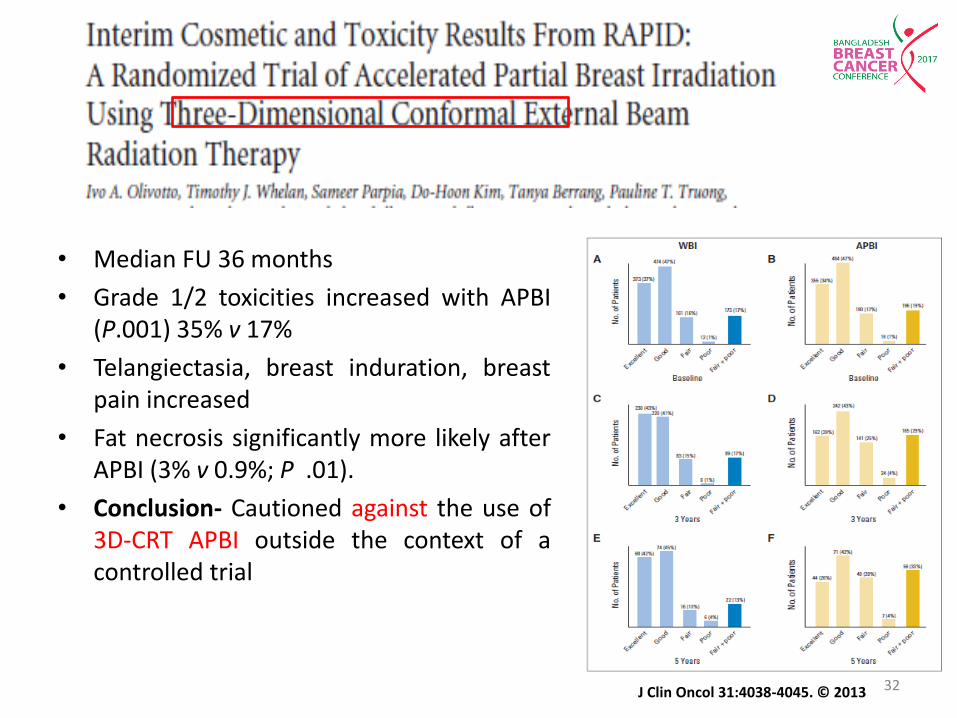
• Median FU 36 months
• Grade 1/2 toxicities increased with APBI (P.001) 35% v 17%
• Telangiectasia, breast induration, breast pain increased
• Fat necrosis significantly more likely after APBI (3% v 0.9%; P .01).
• Conclusion- Cautioned against the use of 3D-CRT APBI outside the context of a controlled trial
J Clin Oncol 31:4038-4045. © 2013 32
• Increase in dose conformity with more normal tissue sparing.
• >40 yrs, ≤25 mm
• 30 Gy to tumour bed in five non consecutive #
• 520 patients 2004-2013
• Median follow-up of 5.0 years
• IBTR rate was 1.5% in both
• 5-year OS 96.6% for WBI vs 99.4% for APBI
• Better results considering acute (p = 0.0001), late (p = 0.004), and cosmetic outcome (p = 0.045)with APBI
European Journal of Cancer (2015)
33

• Increase in dose conformity with more normal tissue sparing.
• >40 yrs, ≤25 mm
• 30 Gy to tumour bed in five non consecutive #
• 520 patients 2004-2013
• Median follow-up of 5.0 years
• IBTR rate was 1.5% in both
• 5-year OS 96.6% for WBI vs 99.4% for APBI
• Better results considering acute (p = 0.0001), late (p = 0.004), and cosmetic outcome (p = 0.045)with APBI
European Journal of Cancer (2015)
34
Conclusion: APBI
• Randomized and prospective data from interstitial brachytherapy series: reassuring and can be considered standard in selected women
• A word of caution for intra-operative techniques
• IMRT better than 3DCRT for APBI
• ASTRO-CS not useful for patient selection
35
THANK YOU FOR YOUR KIND ATTENTION


















