
HYPERTENSIVE DRUG THERAPY Goodman & Gilman, 11th ed., pp. 845-869 Katzung 9th ed., pp. 160-183 JAMA...
55
HYPERTENSIVE DRUG THERAPY Goodman & Gilman, 11th ed., pp. 845-869 Katzung 9th ed., pp. 160- 183 JAMA 289:2560-2572, 2003
-
Upload
thomasine-whitehead -
Category
Documents
-
view
220 -
download
2
Transcript of HYPERTENSIVE DRUG THERAPY Goodman & Gilman, 11th ed., pp. 845-869 Katzung 9th ed., pp. 160-183 JAMA...

HYPERTENSIVE DRUG THERAPY
Goodman & Gilman, 11th ed., pp. 845-869
Katzung 9th ed., pp. 160-183
JAMA 289:2560-2572, 2003

Blood Pressure
• Normotension defined as < 120/80 and > 100/60
• Prehypertension defined as 120-140/80-90
•Hypertension defined as > 140/90
» i. stage 1 140-160/90-100
» ii. stage 2 > 160/100
Control of Blood Pressure BP = (SV)
(HR) (TPR)•Sympathetic Nervous System
– Raises Stroke volume via ß1 receptor activation
– Raises Heart Rate via ß1 receptor activation
– Raises Resistance via receptor activation
Control of Blood Pressure BP = (SV)
(HR) (TPR)•Renin-angiotensin system
– Vasopressor system with salt-retaining effects
– Raises resistance via Angiotensin (AT1) receptor activation
•Plasma volume - affects stroke volume

Sites of action of Antihypertensive
agents• Diuretics (Thiazides, Loop Diuretics, Potassium sparing)
• ß Blockers (Propranolol and other “olols”)
• Renin angiotensin disrupters (ACE inhibitors, angiotensin receptor blockers)
• Calcium channel blockers (Nifedipine etc.)

Sites of action of Antihypertensive agents (cont)
blockers (Terazosin and other “azosins”)
Arteriole-selective vasodilators (Hydralazine, Diazoxide, Minoxidil etc)
Norepinephrine depleting agents (Guanethidine, Reserpine, Guanadrel)
agonists ( methyl dopa, clonidine, others)
Sites of action of Antihypertensive agents (cont)
Ganglionic Blockers (nicotinic receptor antagonist-Trimethaphan)
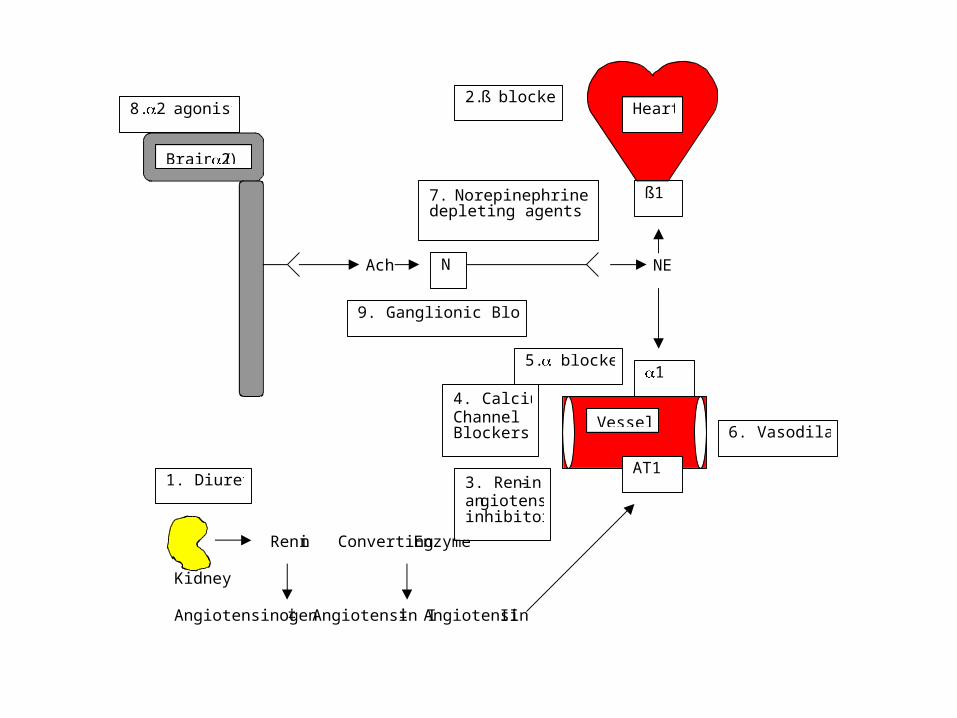
Ach NE
Renin Converting Enzyme Kidney Angiotensinogen ‡ Angiotensin I ‡ Angiotensin II
ß1
1
Brain (2)
Heart
Vessel
N
AT1 1. Diuretics 3. Renin-
angiotensin inhibitors
4. Calcium Channel Blockers
5. blockers
6. Vasodilators
7. Norepinephrine depleting agents
2. ß blockers 8. 2 agonists
9. Ganglionic Blockers
Ideal anti-hypertensive agent
•Decreases systolic/diastolic pressure
•Does not alter cardiac output maintenance
•Does not cause orthostatic hypotension
•Does not produce major changes in regional blood flow
Ideal anti-hypertensive agent
•Is not subject to the development of tolerance
•Is easy to administer to facilitate patient compliance
•Has no limiting side effects or toxicity
• Thiazide diuretics, beta blockers, renin angiotensin system inhibitors and calcium channel antagonists are considered to be closest to ideal

Diuretics
• decrease Na+ and blood volume so pressure is more dependent on vascular resistance. Therefore, they potentiate the antihypertensive effects of other agents reducing TPR, particularly converting enzyme inhibitors or angiotensin receptor blockers.

Diuretics
• Thiazide diuretics • Loop diuretics• Potassium - sparing diuretics

Thiazide diuretics
• HYDROCHLOROTHIAZIDE (Microzide), Chlorothiazide (Diuril), Polythiazide (Renese), CHLORTHALIDONE (Chlorthalidone), indapamide (Lozol), Metalozone (Mykrox)

Thiazide diuretics
•Increase Na+ excretion and reduce plasma volume but these effects can be separated from the antihypertensive action
•Should usually be the first drugs used for hypertension therapy
•Decrease total peripheral resistance through vasodilator action on smooth muscle (activate a potassium channel to hyperpolarize smooth muscle)
Thiazide diuretics • Can cause hypokalemia, hyperglycemia (activate potassium channel in ß cells of pancreas to hyperpolarize & reduce insulin secretion) and hyperuricemia (gout)
• Considered to be excellent choices for the generic hypertensive and hypertension in African Americans and elderly- compelling indication for use in hypertension associated with: heart failure; diabetes, prevention against stroke
• Considered to be a poor choice in patients with gout or hyponatremia (no longer considered dangerous in diabetes mellitus even though they suppress insulin)

Loop diuretics
•FUROSEMIDE, ethacrynic acid, bumetanide - not used much in hypertension
•Decrease in BP correlates with loss in body weight

Potassium - sparing diuretics
•Spironolactone (Aldactone) and Eplerenone (Inspra) are aldosterone receptor antagonists
•TRIAMTERENE (Dyrenium) and Amiloride (Midamor) inhibit Na+ channels (ENaC) resulting in reduced K+ and H+ loss in the distal tubule of kidney
•Decrease potassium loss during diuretic therapy
Potassium - sparing diuretics
•Spironolactone & Eplerenone used to treat primary aldosteronism
•Can cause severe hyperkalemia
•Compelling use for Spironolactone or Eplerenone in hypertension associated with heart failure or post-myocardial infarction

ß adrenergic blockers - Act to decrease cardiac output
•Non selective
•ß1 selective
•Partial agonists•Combined alpha & ß blockade

ß adrenergic blockers
• Non selective
– PROPRANOLOL (Inderal), NADOLOL (Corguard), pindolol (Visken), penbutolol, (Levatol), bisoprolol (Zabeta)
– Produce negative inotropic and chronotropic effects and little orthostatic hypotension
– Disadvantages are reflex vasoconstriction, fluid retention and efficacy is dependent on adrenergic tone & can produce bronchospasm in asthmatics, hypoglycemia in diabetics and hypertension in pheochromocytoma
ß adrenergic blockers
ß1 selective
– METOPROLOL (Lopressor), ATENOLOL (Tenormin), acebutolol, (Sectral), and betaxolol (Kerlone)
– Advantages and disadvantages are the same as those for non-selective beta antagonists except that ß1 antagonists are less likely to produce asthma, hypoglycemia in a diabetic or hypertension in pheochromocytoma

ß adrenergic blockers
•Partial agonists (pindolol, acebutolol, penbutolol) are less likely to lower heart rate and they are vasodilators (called intrinsic sympathomimetic activity)
•Combined alpha & ß blockade- Labetalol (Normodyne, Trandate) and Carvedilol (Coreg)
ß adrenergic blockers
– compelling indication for ß blocker use in treating hypertension associated with heart failure, angina pectoris, post-myocardial infarction, and diabetes mellitus. Good in hypertension associated with migraine headache, atrial tachycardia, hyperthyroidism or tremor

ß adrenergic blockers
• ß blockers are poor choices in hypertension associated with asthma, depression, heart block; most recent guidelines do not include peripheral vascular disease or diabetes mellitus or hyperlipidemia

Renin dependent antihypertensives
• Converting Enzyme Inhibitors• Angiotensin receptor antagonists• Renin inhibitor • Less effective in African-Americans than diuretics or calcium channel antagonists
• Angiotensin receptor blocking agents and converting enzyme inhibitors are essentially equivalent

Converting Enzyme Inhibitors
• CAPTOPRIL (Capoten) , ENALAPRIL (Vasotec), LISINOPRIL (Prinivil, Zestrin) , fosinopril (Monopril) , ramipril (Altace), benazopril, (Lotensin), Perindopril (Aceon), quinapril (Accupril), moexepril, (Univsasc), trandolapril (Mavik)
• Decrease TPR• renal protective in patients with diabetes mellitus or chronic renal disease
• Disadvantages are cough, angioedema, nephropathies, leukopenia and agranulocytosis; teratogenic effects-avoid in pregnancy

Converting Enzyme Inhibitors
• diuretics markedly potentiate anti-hypertensive effects (Na & volume depletion makes blood pressure more dependent on renin-angiotensin system)
• less effective in African-Americans than diuretics or calcium channel blockers
• Compelling indication for treatment of hypertension associated with diabetes mellitus, chronic kidney disease, congestive heart failure or left ventricular dysfunction, post myocardial infarction and danger of stroke
Angiotensin receptor antagonists
•Losartan,(Cozaar), Valsartan (Diovan); Irbesartan (Avapro); Candesartan (Atacand); Telmisartan (Micardis); Eprosartan (Teveten), Irbesartan (Avapro), Olmesartan (Benicar))
•Apparently do not cause cough, as Captopril et al. do (don’t potentiate kinins)

Renin Inhibitor
•Aliskerin (Tekturna)– Blocks formation of angiotensin I by inhibiting renin
– Approved for use in 2007– Side effects are diarrhea, rash and hyperkalemia
– More expensive than other renin-angiotensin inhibitors
– Significance as an antihypertensive not established yet
Calcium Channel Blocking Agents
• inhibit voltage sensitive calcium channels (usually L channels) to reduce calcium entry into smooth muscle

Calcium Channel Blocking Agents (cont)
• VERAPAMIL (Calan, Isoptin etc); DILTIAZEM (Cardizem); Nicardipine (Cardene); NIFEDIPINE (Procardia, Adalat)- only extended release forms; short-acting forms are reported to increase mortality
• Others include amlodipine (Norvasc), felodipine (Plendil), Isradipine (Dynacirc), Nisoldipine (Sular)
• Actions are to vasodilate (reduce TPR)– 1. DILTIAZEM and VERAPAMIL contraindicated with ß blockers (they suppress cardiac contractions, as ß blockers do)

Calcium Channel Blocking Agents (cont)
•Considered to be a good choice in hypertensive African Americans and a compelling choice in hypertension associated with angina pectoris or diabetes mellitus
•A major side effect is edema
•T channel inhibitor- Mibefradil (Posicor)- blocks T channels to decrease resistance and blood pressure

Peripherally acting adrenergic antagonists
• PRAZOSIN (Minipress), doxazosin (Cardura) and TERAZOSIN (Hytrin)
• Act to dilate arterioles by blocking the constrictor effect of catecholamines
• Produce orthostatic and exertion related hypotension - block venoconstriction
• Act to decrease TPR blockers are considered good choices in hypertension associated with prostatic hypertrophy (they attenuate the
hypertrophy)
Direct acting vasodilators
•Arteriole - Specific•Arteriolar and Venodilators

Arteriole - Specific
Hydralazine (Apresoline)• Decreases TPR but doesn't produce much orthostatic hypotension (veins are not dilated)
• Disadvantage is reflex tachycardia and fluid retention
• Given orally, Metabolized by liver (highly variable)
• Side effects are palpitations, headache - usually prevented by ß blockade; also a lupus-like syndrome
• parenteral drug of choice for pregnancy-induced hypertension

Arteriole - Specific
Minoxidil (Loniten; Rogaine)– Similar to hydralazine in mechanism, use, and side effects but doesn't produce the lupus syndrome
– Hypertrichosis (hair growth) is a common side effect (used topically for hair growth)
– Usually reserved for severe, resistant hypertension
– Diazoxide (Hyperstat IV) Thiazide-like vasodilator not mentioned in JNC VII report (JAMA article)

Arteriolar and Venodilators
Nitroprusside (Nipride)
– Mechanism is to rapidly dilate both veins and arteries (elevates cGMP concentrations in smooth muscle by activating guanylyl cyclase)
– Blood pressure can be reduced to any level
– Only given i.v., short term treatment
– Used in surgical hypotension, hypertensive crisis, dissecting aneurysms, heart failure, ergot poisoning

Norepinephrine depleting agents
•Reserpine (Serpasil), guanethidine (Ismelin), guanadrel (Hylorel).
•Decrease total peripheral resistance and cardiac output with little reflex tachycardia
•Disadvantages are an initially elevated BP, bradycardia, postural hypotension, fluid retention, and efficacy dependent on sympathetic tone
•No compelling reason to use these agents
Centrally acting 2
agonists• methyldopa (Aldomet), clonidine (Catapress) guanabenz (Wytensin), guanfacine (Tenex)
• Mechanism of action is to inhibit sympathetic nerve activity via activation of 2 receptors- decrease both TPR and Cardiac Output
• methyl-dopa - Drug of choice in pregnancy-induced hypertension (the only compelling reason for its use)
• Advantages of these drugs include a decrease in TPR but negligible orthostatic hypotension
• Some disadvantages are fluid retention and efficacy is dependent on sympathetic tone [depression]

Ganglionic (nicotinic receptor) blockers • Mecamylamine (Inversine), Trimethaphan (Arfonad) and Hexamethonium
• Block autonomic ganglia, therefore decrease sympathetic tone on vessels
• Were used in hypertensive crises and to produce surgical hypotension but no compelling rationale for use (no longer manufactured in USA)
• Enormous number of side effects discourage the use of these drugs
Specific Treatment
• Essential hypertension (from JAMA 289: 2560-2572, 2003)
• Renal hypertension - cure is surgery or angioplasty but can be controlled with CAPTOPRIL, ENALAPRIL, etc. (these agents can cause renal failure in this condition)
• Pheochromocytoma - BP can be controlled with phentolamine or phenoxybenzamine ( blockers), surgical removal is cure
• Hypertensive crisis –treat with rapid acting vasodilator (nitroprusside, LABETALOL)
• Pregnancy-induced hypertension- -methyldopa (aldomet) is preferred agent; Hydralazine (Apresoline) is a good alternative and preferred parenteral agent
Essential hypertension
• If prehypertensive, treat with lifestyle modifications but not drugs unless they have diabetes meillitus or chronic kidney disease
• If stage I hypertensive (140-160/90-100), encourage lifestyle modification and initiate drug therapy, preferably a thiazide diuretic
• If stage II hypertension (>160/100), encourage lifestyle modifications but start drug therapy usually with 2 agents, including a thiazide diuretic in combination with a renin-angiotensin system disruptor (ACE inhibitor or angiotensin receptor blocker), ß blocker, or calcium channel blocker.
• If response still inadequate, add a second or third agent from a different class


Compelling reasons for antihypertensive use
• Thiazide diuretics- Congestive heart failure; diabetes mellitus; prevention of stroke
• Spironolactone/Eplerenone- Congestive heart failure; after a myocardial infarction
• Propranolol (ß blockers)- Congestive heart failure; Angina pectoris; after a myocardial infarction; diabetes mellitus
• Renin-angiotensin disrupters- Diabetes mellitus; Chronic kidney disease; Congestive heart failure; after myocardial infarction; prevention of stroke
• Calcium channel blockers (nifedipine etc)- Angina pectoris; Diabetes mellitus


Conditions precluding use of certain
antihypertensive agents
• Thiazide diuretics (Hydrochlorothiazide et al.)- hyponatremia; gout
• Propranolol (ß blockers)- Asthma; depression; heart block

Hypertensive conditions in which a
certain antihypertensive is
good• Propranolol (ß blockers)- migraine headache; atrial tachycardia; hyperthyroidism; tremor
• Nifedipine (Calcium channel blockers)- African Americans
• Terazosin (Alpha 1 blockers)- prostatic hypertrophy
• Hydralazine- pregnancy-induced hypertension
• Alpha methyl DOPA- pregnancy-induced hypertension

A male 36 year old patient has a blood pressure of 144/96. He is training for a marathon. Which of the following is the best treatment for his hypertension:
• Enalapril • Hydrochlorothiazide• Nifedipine• Propranolol• Spironolactone

A 35 year old male diabetic patient has a blood pressure of 140/90 with proteinuria. Which of the following would be the most
appropriate treatment:
a) Enalaprilb) Hydrochlorothiazidec) Hydralazined) Nifedipinee) Propranolol

A 55 year old male patient has a blood pressure of 145/95 with chest pain upon
physical exertion. Which of the following would you give:
a) Enalaprilb) Hydrochlorothiazidec) Hydralazined) Nifedipinee) Propranolol

A 55 year old male patient has a blood pressure of 150/98. He had a myocardial
infarction two weeks earlier. Which of the following would you give to treat his
hypertension:
a) Enalaprilb) Hydrochlorothiazidec) Hydralazined) Nifedipinee) Propranolol

A 55 year old female patient has a blood pressure of 150/98. She has a history of migraine headaches. Which of the following would you give to treat her hypertension:
a) Enalaprilb) Hydrochlorothiazidec) Hydralazined) Nifedipinee) Propranolol
A 63 year old male patient has a blood pressure of 145/95. He has been studying to be a pianist and complains about tremor while
performing. How would you treat his hypertension:
a) Enalaprilb) Hydrochlorothiazidec) Nifedipined) Propranolole) Spironolactone

A 58 year old female patient has a blood pressure of 130/88 after treatment with one antihypertensive agent. She recently is suffering acute attacks of gout. Which of the following antihypertensive treatment is
most likely to be the cause:a) Enalaprilb) Hydrochlorothiazidec) Nifedipined) Propranolole) Spironolactone
A 48 year old female patient has a blood pressure of 128/93 after treatment with one antihypertensive agent. She is an asthmatic and is suffering from a dramatic increase in the frequency of asthmatic attacks. Which of the following antihypertensive treatment is
most likely to be the cause:a) Enalaprilb) Hydrochlorothiazidec) Nifedipined) Propranolole) Spironolactone


















