Lessons from Hypertension guidelines : Treatment Of Hypertension.
description

Hypertension TreatmentHypertension TreatmentA TransAtlantic viewA TransAtlantic view
Arterial Hypertension 2014
José R. González JuanateyCardiology Department and ICCU
University Hospital Santiago de Compostela. Spain

Disclosures:Research Grants: AZ, Boehringer Ingelheim, Pfizer, Novartis, Daichii-Sankyo, Sanofi-Aventis, Bayer, MSD.Consultant/Honorarium. AZ, Boehringer-Ingelheim, Bayer, Pfizer, BMS, MSD, Daichii-Sankyo, Servier.

J.R.G. JUANATEY C.H.U.Santiago
HT- 2014. A transAtlantic view
Epidemiology
HT and Risk Stratification
New Guidelines and Therapeutic Objectives
New Guidelines and Drug Selection

J.R.G. JUANATEY C.H.U.Santiago
HT Epidemiology
.30 – 45 % of adult population (> 1.500 million persons)

J.R.G. JUANATEY C.H.U.Santiago
World’s biggest killers World’s biggest killers –– CVD retain top spotCVD retain top spot

J.R.G. JUANATEY C.H.U.Santiago
HT- 2014. A transAtlantic view
Epidemiology
HT and Risk Stratification
New Guidelines and Therapeutic Objectives
New Guidelines and Drug Selection

J.R.G. JUANATEY C.H.U.Santiago
Office and ambulatory HT mmHgCategory SBP DBP
Office ≥ 140 y/o ≥ 90
ABPM
Day (activity) ≥ 135 y/o ≥ 85
Night (rest) ≥ 120 y/o ≥ 70
24-hours ≥ 130 y/o ≥ 80
In-home ≥ 135 y/o ≥ 85
JNC VIII / ASH ESC / ESH 2013

J.R.G. JUANATEY C.H.U.Santiago
EVALUATING THE PATIENTEVALUATING THE PATIENTHistory. History. Important previous events include:Important previous events include:Stroke, TIA, CAD, HF or symptoms of left vemtricular dysfunction, CKD, Stroke, TIA, CAD, HF or symptoms of left vemtricular dysfunction, CKD, Pripheral artery disease, Diabetes, Sleep apnea, ask about other risk Pripheral artery disease, Diabetes, Sleep apnea, ask about other risk factors and concurrent drugs.factors and concurrent drugs.Physical Examination.Physical Examination.Measuring BP; weight, height and BMI, waist circumference, signs of HF, Measuring BP; weight, height and BMI, waist circumference, signs of HF, neuro examination, optic fundi (if possible), peri-ocular xantomas, neuro examination, optic fundi (if possible), peri-ocular xantomas, peripheral pulses.peripheral pulses.
TESTSTESTSBlood Sample: Blood Sample: electrolytes, Fasting glucose, serum creatinine and electrolytes, Fasting glucose, serum creatinine and BUN, Lipids, Hb/hematocrit, liver function tests.BUN, Lipids, Hb/hematocrit, liver function tests.Urine Sample: Urine Sample: Albuminuria, red and white cells.Albuminuria, red and white cells.
ECG. ECG. All patientsAll patientsECHOCARDIOGRAMECHOCARDIOGRAM. , if available, can be helpful . , if available, can be helpful …., although this …., although this test is not routine in hypertensive patientstest is not routine in hypertensive patients
2013

J.R.G. JUANATEY C.H.U.Santiago
Test CV predictive value Availability Reproducibility Cost-effect
ESC/ESH 2013. ESC/ESH 2013.
Guidelines Markers of organ damageGuidelines Markers of organ damage

J.R.G. JUANATEY C.H.U.Santiago
Factores de riesgo (FRCV)Lesión de órgano diana (LOD)
Enfermedad cardiovascular (ECV)
No otros factores de riesgo
1 – 2 factores de riesgo
≥ 3 factores de riesgo
LOD, IRC 3 o Diabetes
ECV sintomática, IRC ≥ 4 o Diabetes con LOD/FRCV
Presión arterial (mmHg)
Normal altaPAS 130 – 139o PAD 85-89
HTA grado 1PAS 140 – 159o PAD 90-99
HTA grado 2PAS 160 – 179o PAD 100-109
HTA grado 3PAS ≥ 180
o PAD ≥ 110
Bajo riesgo
Bajo riesgo
Alto riesgo
Alto riesgo
Alto riesgo
Alto riesgo
Alto riesgo
Alto riesgo
Muy alto riesgo Muy alto riesgo Muy alto riesgo Muy alto riesgo
Moderado riesgo
Moderado riesgo Moderado a alto riesgo
Moderado a alto riesgo
Alto a muyalto riesgo
Bajo a moderado riesgo
Moderado a alto riesgo
JNC VIII / ASH ESC / ESH 2013

J.R.G. JUANATEY C.H.U.Santiago
HT- 2014. A transAtlantic view
Epidemiology
HT and Risk Stratification
New Guidelines and Therapeutic Objectives
New Guidelines and Drug Selection

J.R.G. JUANATEY C.H.U.Santiago
JNC VIII / ASH ESC / ESH 2013
JAMA 2013 / AJH 2013
Eur Heart J / J Hypertens 2013
< 140/90 mmHg
< 140/90 mmHg in diabetes and chronic renal failure
“…it may be prudent to recommend lowering SBP/DBP to values < 140/90 mmHg in all hypertensive patients…” “…<140/85 mmHg in diabetes…”

J.R.G. JUANATEY C.H.U.Santiago
Blood Pressure Goal in Patientes with HT
Recomendaciones Clase Nivel
Presión arterial sistólica < 140 mmHg
pacientes con riesgo cardiovascular bajo-moderado I B
pacientes con diabetes I A
pacientes con ictus previo o ataque isquémico transitorio IIa B
pacientes con cardiopatía isquémica IIa B
pacientes con insuficiencia renal, diabética o no diabética IIa B
Ancianos (< 80 años) con PAS ≥ 160 mmHg, objetivo PAS entre 140 y 150 mmHg
I A
Ancianos (< 80 años) en buena forma física < 140 mmHg IIb C
Ancianos (> 80 años) con PAS ≥ 160 mmHg, objetivo PAS entre 140 y 150 mmHg, si están en buenas condiciones
I B
Presión arterial diastólica < 90 mmHg; en diabéticos < 85 mmHg. Valores PAD 80-85 mmHg son seguros y bien tolerados
I A
ESC / ESH 2013

J.R.G. JUANATEY C.H.U.Santiago
PatientsPatients BPBP
Adults Aged > 18 yAdults Aged > 18 y > 140 / 90 mmHg OBPOBP
Age Age >> 80 y 80 y > 150 / 90 mmHg OBPOBP
High Risk (DM, CKD)High Risk (DM, CKD) > 140 / 90 mmHg OBPOBP
2013Blood Pressure >140/90 in Adults Aged >18 years
(For age >80 years, pressure >150/90 or >140/90 if high risk (DM, CKD
Start Lifestyle Changes(Lose weight, reduce dietary salt and alcohol, stop
smoking)

J.R.G. JUANATEY C.H.U.Santiago
Recommendation 1Recommendation 1In the general population In the general population aged aged 60 years or older, 60 years or older, initiate pharmacologic treatment to lower BP initiate pharmacologic treatment to lower BP at SBP of at SBP of 150 mm Hg or higher150 mm Hg or higher or DBP of 90 mm Hg or higher or DBP of 90 mm Hg or higher and treat to goal SBP lower than 150 mm Hg and goal and treat to goal SBP lower than 150 mm Hg and goal DBP lower than 90 mm Hg.DBP lower than 90 mm Hg.Strong recommendation Strong recommendation –– Grade A Grade ARecommendation 2Recommendation 2In the general population younger than 60 years In the general population younger than 60 years initiate pharmacologic treatment to lower BP at DBP of initiate pharmacologic treatment to lower BP at DBP of 90 mm Hg or higher and treat to goal DBP of lower 90 mm Hg or higher and treat to goal DBP of lower than 90 mm Hg than 90 mm Hg For ages 30-59 years: For ages 30-59 years: Strong recommendation Strong recommendation –– Grade AGrade AFor ages 18-29 years: For ages 18-29 years: Expert opinion Expert opinion –– Grade E Grade ERecommendation 3Recommendation 3In the general population younger than 60 years In the general population younger than 60 years initiate pharmacologic treatment to lower BP at SBP of initiate pharmacologic treatment to lower BP at SBP of 140 mm Hg or higher and treat to goal SBP of lower 140 mm Hg or higher and treat to goal SBP of lower than 140 mm Hg than 140 mm Hg Expert opinion Expert opinion –– Grade E Grade E

J.R.G. JUANATEY C.H.U.Santiago
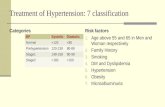
Metaregression of Treatment-induced Systolic BP Changes with Stroke and Myocardial InfarctionMetaregression of Treatment-induced Systolic BP Changes with Stroke and Myocardial InfarctionMetaregression of Treatment-induced Systolic BP Changes with Stroke and Myocardial InfarctionMetaregression of Treatment-induced Systolic BP Changes with Stroke and Myocardial Infarction
Reboldi, Gentile, Angeli, Ambrosio, Mancia, Verdecchia, 2010Reboldi, Gentile, Angeli, Ambrosio, Mancia, Verdecchia, 2010
Stroke Myocardialinfarction
3.003.002.752.752.502.502.252.25
2.002.001.751.75
1.501.50
1.251.25
1.001.00
0.750.75
0.500.50
0.250.25
Rel
ativ
e ris
kR
elat
ive
risk
SBP difference between randomized groups (mmHg)SBP difference between randomized groups (mmHg)-6-6 -4-4 -2-2 00 22 44 66 88 1010 1212 1414 1616 1818 2020 -6-6 -4-4 -2-2 00 22 44 66 88 1010 1212 1414 1616 1818 2020
3.003.002.752.752.502.502.252.25
2.002.001.751.75
1.501.50
1.251.25
1.001.00
0.750.75
0.500.50
0.250.25
ABCD-N More vs LessABCD-N More vs Less
SYST-EUR DiabSYST-EUR Diab
ACCORD BPACCORD BPUKPDS 38UKPDS 38
FACETFACET
MOSES-DiabMOSES-Diab
JMIC-B-DiabJMIC-B-Diab
HOPE-DiabHOPE-DiabIDNT/CCB -PLBIDNT/CCB -PLB
PROGRESS-DiabPROGRESS-Diab
SHEP-DiabSHEP-Diab
EUROPA-DiabEUROPA-Diab
ABCD-HABCD-HMore vs LessMore vs Less
ACTION-DiabACTION-Diab
ABCD/NormABCD/Norm
ABCD/HTABCD/HT
IDNT/ARB-CCBIDNT/ARB-CCB
IDNT/ARB-PLBIDNT/ARB-PLB
ADVANCEADVANCE
ASCOT-DiabASCOT-Diab
HOT-DM More vs LessHOT-DM More vs Less
DETAILDETAIL
DETAILDETAIL
ALLHAT/ACE-CCB-DiabALLHAT/ACE-CCB-Diab
STOP2/CCB-BB-DiabSTOP2/CCB-BB-DiabLIFE-DiabLIFE-Diab
INVEST-DiabINVEST-DiabIINSIGHT-DiabIINSIGHT-Diab
ALLHAT/CCB-D-DiabALLHAT/CCB-D-DiabSTOP2/ACE-BB-DiabSTOP2/ACE-BB-Diab
RENAALRENAALDIABHYCARDIABHYCARCAPPP-DiabCAPPP-Diab
ALLHAT/ACE-D-DiabALLHAT/ACE-D-DiabUKPDS 39UKPDS 39
STOP2/ACE-CCB-DiabSTOP2/ACE-CCB-Diab
ABCD-N More vs LessABCD-N More vs Less
ACCORD BPACCORD BP
UKPDS 38UKPDS 38
FACETFACET
JMIC-B-DiabJMIC-B-Diab
HOPE-DiabHOPE-Diab
IDNT/ARB-CCBIDNT/ARB-CCB
EUROPA-DiabEUROPA-Diab
ACTION-DiabACTION-Diab
ABCD/NormABCD/Norm
ABCD/HTABCD/HT
IDNT/ARB-CCBIDNT/ARB-CCB
IDNT/ARB-PLBIDNT/ARB-PLB
ADVANCEADVANCE
ASCOT-DiabASCOT-Diab
HOT-DM More vs LessHOT-DM More vs Less
DETAILDETAILSTOP2/CCB-BB-DiabSTOP2/CCB-BB-Diab
LIFE-DiabLIFE-Diab
INVEST-DiabINVEST-Diab
STOP2/ACE-BB-DiabSTOP2/ACE-BB-DiabRENAALRENAAL
DIABHYCARDIABHYCAR
CAPPP-DiabCAPPP-Diab
UKPDS 39UKPDS 39
STOP2/ACE-CCB-DiabSTOP2/ACE-CCB-Diab
ATLANTIS/1.25ATLANTIS/1.25
ATLANTIS/5ATLANTIS/5
ABCD-H More vs LessABCD-H More vs Less

J.R.G. JUANATEY C.H.U.Santiago
CV Event Incidence in Relation to Mean FU Systolic BP (up to 1st event) in VALUE
Mancia et al., 2010Mancia et al., 2010
MIMIMIMI StrokeStrokeStrokeStroke
0
4
8
12
16
20
0
2
4
6
8
10
2.212.21 1.761.762.642.64
4.034.03
6.816.81
9.369.36
11.7211.72
17.4217.42
4.924.92
3.933.933.273.27
4.514.51
6.976.97
8.188.188.708.70
5.435.43
<120<120 120-120-<130<130
130-130-<140<140
140-140-<150<150
150-150-<160<160
160-160-<170<170
170-170-<180<180
≥≥180180
SBP (mmHg)SBP (mmHg)
<120<120 120-120-<130<130
130-130-<140<140
140-140-<150<150
150-150-<160<160
160-160-<170<170
170-170-<180<180
≥≥180180
SBP (mmHg)SBP (mmHg)
%% %%

J.R.G. JUANATEY C.H.U.Santiago
Incidence and Incidence and Unadjusted CV Risk of Events Unadjusted CV Risk of Events in Deciles of In-treatment SBPin Deciles of In-treatment SBP
Incidence and Incidence and Unadjusted CV Risk of Events Unadjusted CV Risk of Events in Deciles of In-treatment SBPin Deciles of In-treatment SBP
Una
djus
ted
risk
of e
vent
s (%
)U
nadj
uste
d ris
k of
eve
nts
(%)
HR
(95% C
I)H
R (95%
CI)
On-treatment SBP (mmHg)On-treatment SBP (mmHg)U
nadj
uste
d ris
k of
eve
nts
(%)
Una
djus
ted
risk
of e
vent
s (%
)
HR
(95% C
I)H
R (95%
CI)
Myocardial infarctionMyocardial infarctionMyocardial infarctionMyocardial infarction StrokeStrokeStrokeStroke
Sleight, et al., J Hypert 2009; 27: 1360-1369Sleight, et al., J Hypert 2009; 27: 1360-1369
112 121 126 130 133 136 140 144 149 160 0
5
10
0
1
2
112 121 126 130 133 136 140 144 149 160 0
5
10
0
2
4
6
On-treatment SBP (mmHg)On-treatment SBP (mmHg)