
HYPERTENSION in ADPKD Sabine Karam M.D.. Introduction ADPKD is the most common life-threatening...
34
HYPERTENSION in ADPKD Sabine Karam M.D.
-
Upload
abraham-anderson -
Category
Documents
-
view
221 -
download
0
Transcript of HYPERTENSION in ADPKD Sabine Karam M.D.. Introduction ADPKD is the most common life-threatening...

HYPERTENSION in ADPKDSabine Karam M.D.
IntroductionADPKD is the most common life-threatening
single-gene disease
It affects over 12 million people worldwide
Fourth leading cause of end-stage renal disease (ESRD) in the US
Hypertension identified as a factor associated with progression to ESRD
HYPERTENSION in ADPKDOccurs in 50-75% of patients prior to the onset
of marked renal insufficiency
Early high incidence correlated with renal structural abnormalities
Most important potentially treatable variable
Important risk factor for cardiovascular death, the most frequent cause of mortality in ADPKD patients
JASN. 2001.Jan;12(1):194-200
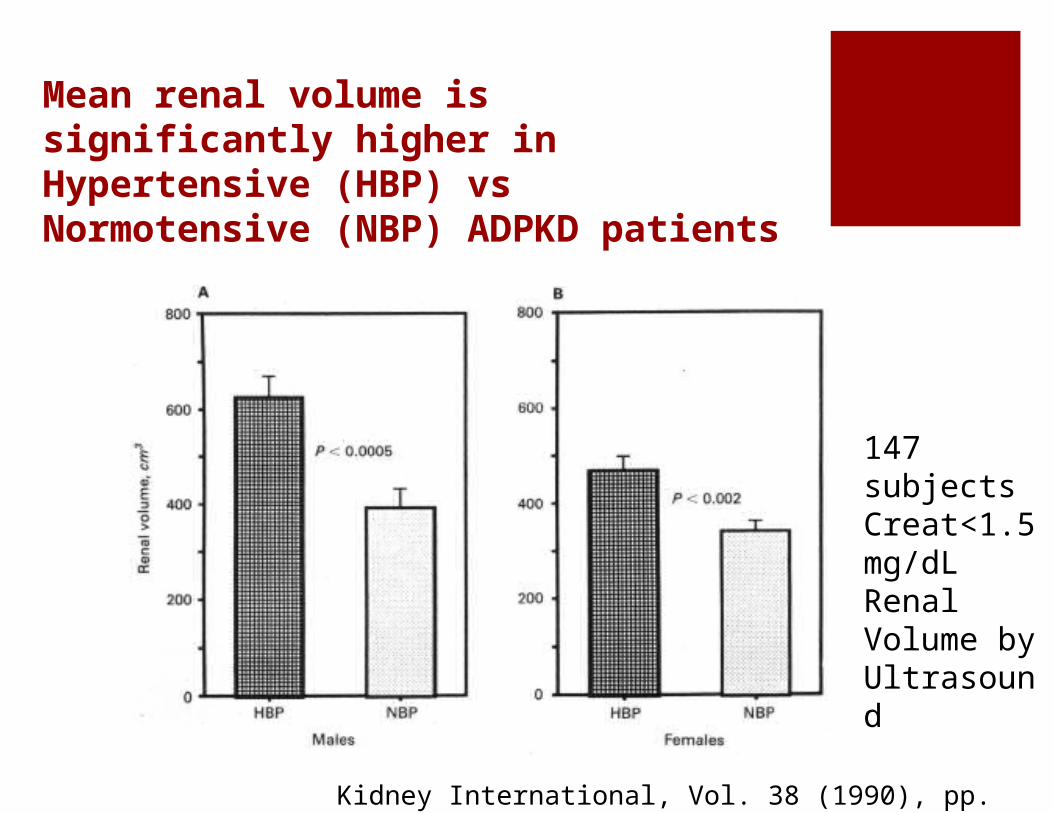
Mean renal volume is significantly higher in Hypertensive (HBP) vs Normotensive (NBP) ADPKD patients
Kidney International, Vol. 38 (1990), pp. 1177—1180
147 subjectsCreat<1.5 mg/dLRenal Volume by Ultrasound
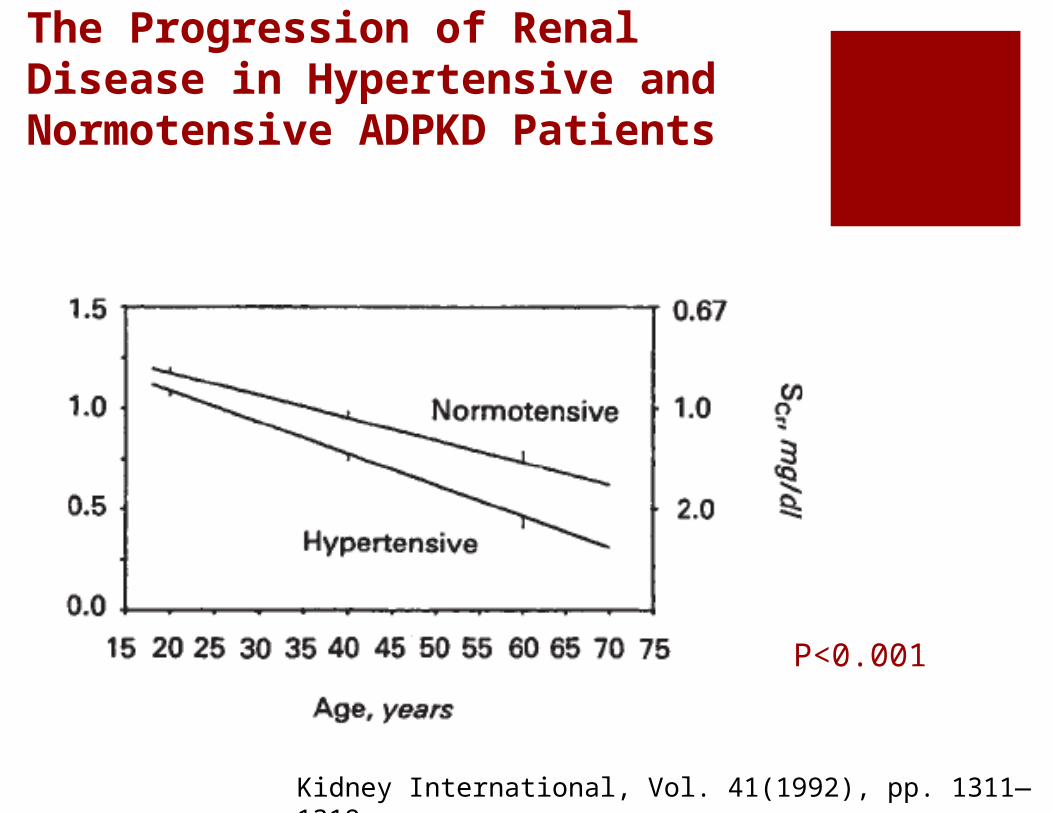
The Progression of Renal Disease in Hypertensive and Normotensive ADPKD Patients
Kidney International, Vol. 41(1992), pp. 1311—1319
P<0.001
Does the choice of the
agent matter?

Mean PRA and plasma aldosterone concentration in 14 patients with HTN and ADPKD vs 9 patients with essential hypertension before and after 50 mg of captopril
NEJM.1990;323:1091-6
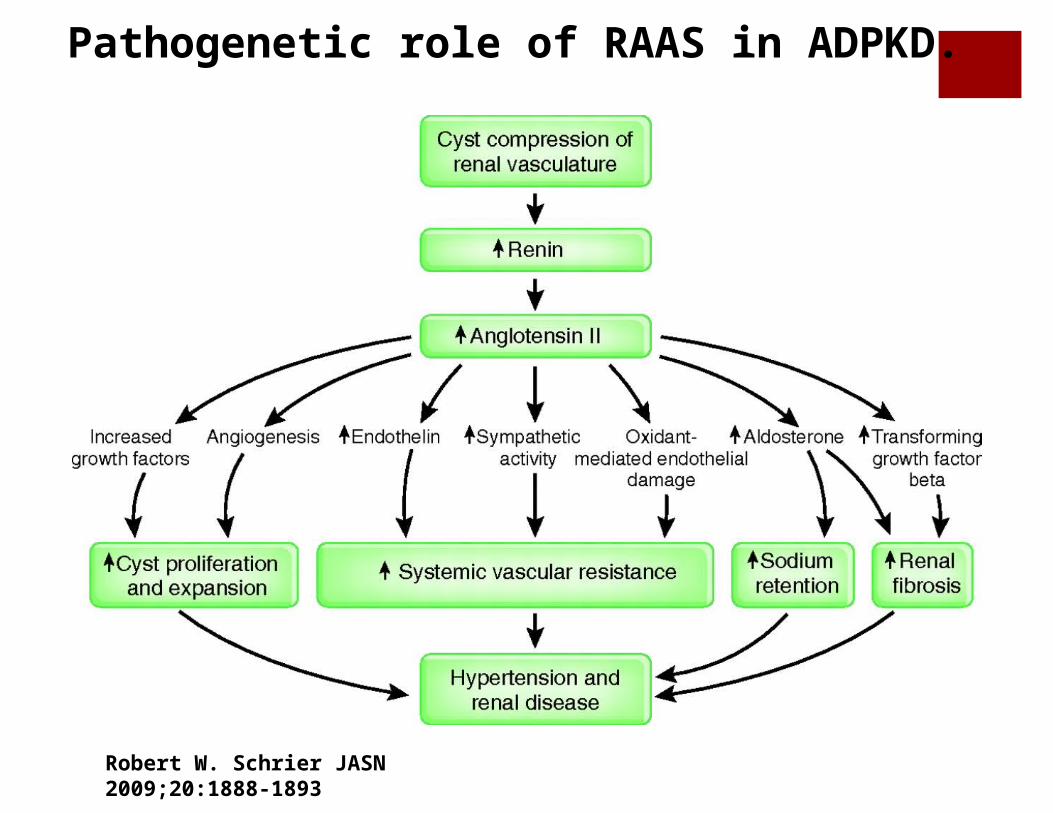
Pathogenetic role of RAAS in ADPKD.
Robert W. Schrier JASN 2009;20:1888-1893
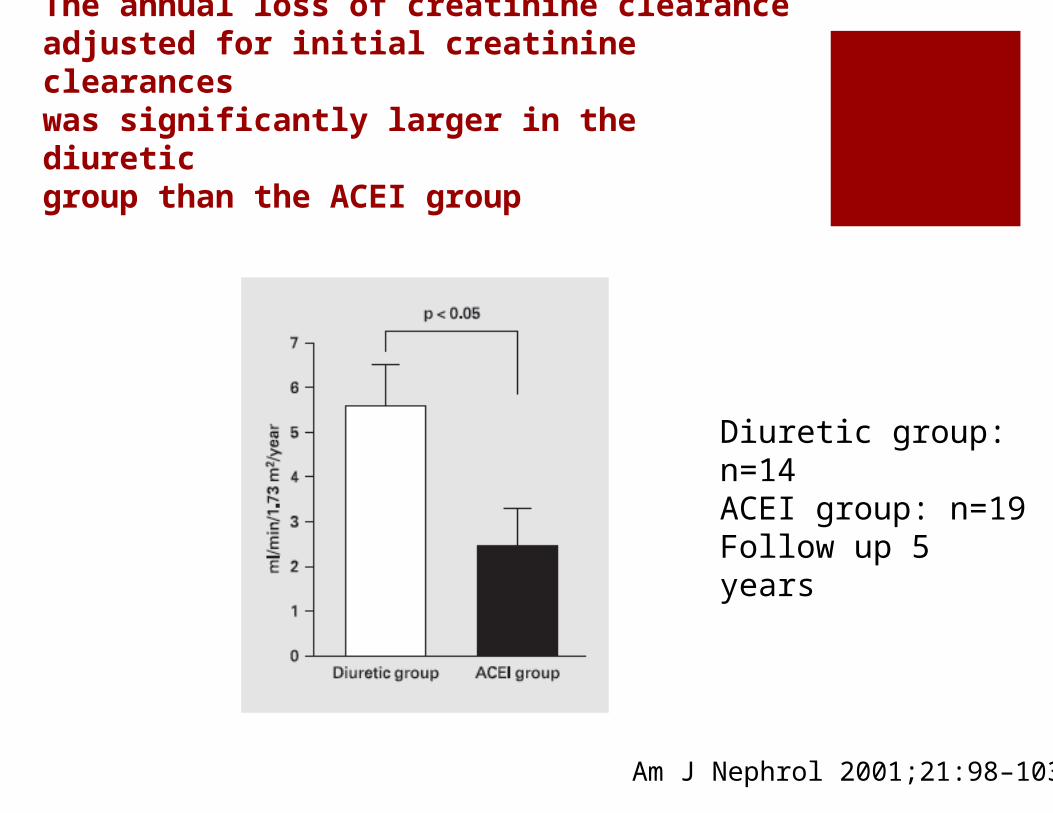
The annual loss of creatinine clearanceadjusted for initial creatinine clearanceswas significantly larger in the diureticgroup than the ACEI group
Am J Nephrol 2001;21:98–103
Diuretic group: n=14ACEI group: n=19Follow up 5 years
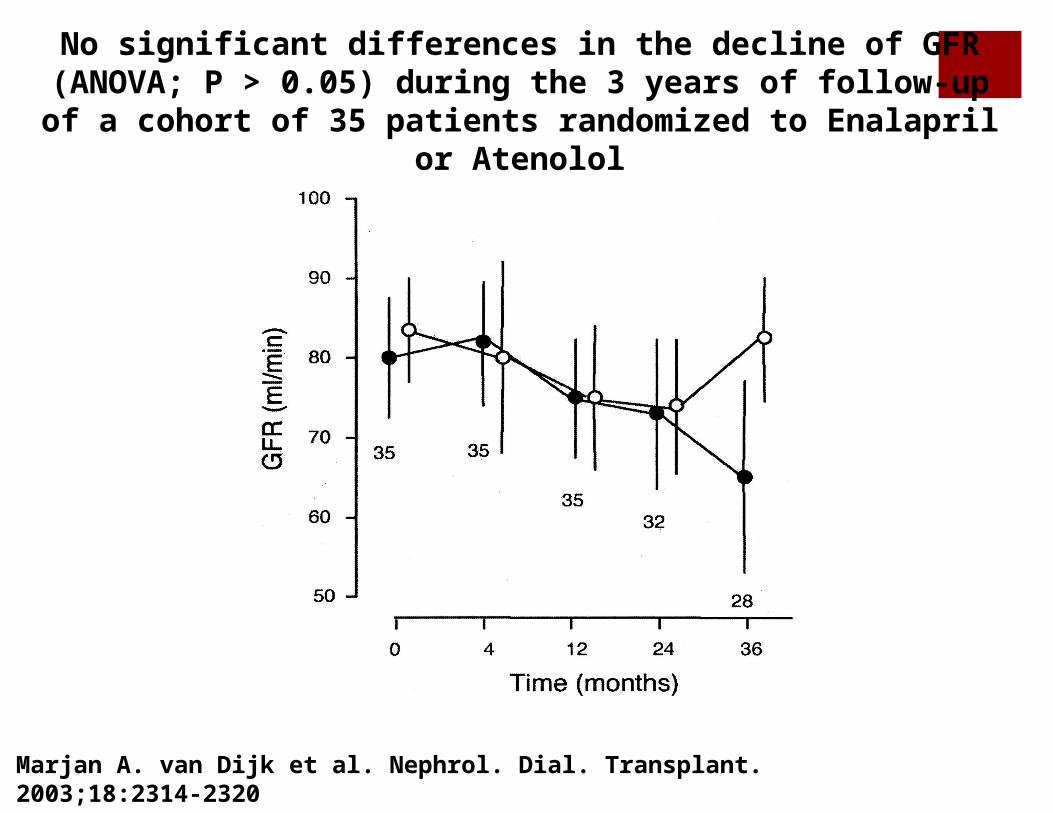
No significant differences in the decline of GFR (ANOVA; P > 0.05) during the 3 years of follow-up of a cohort of 35 patients
randomized to Enalapril or Atenolol
Marjan A. van Dijk et al. Nephrol. Dial. Transplant. 2003;18:2314-2320
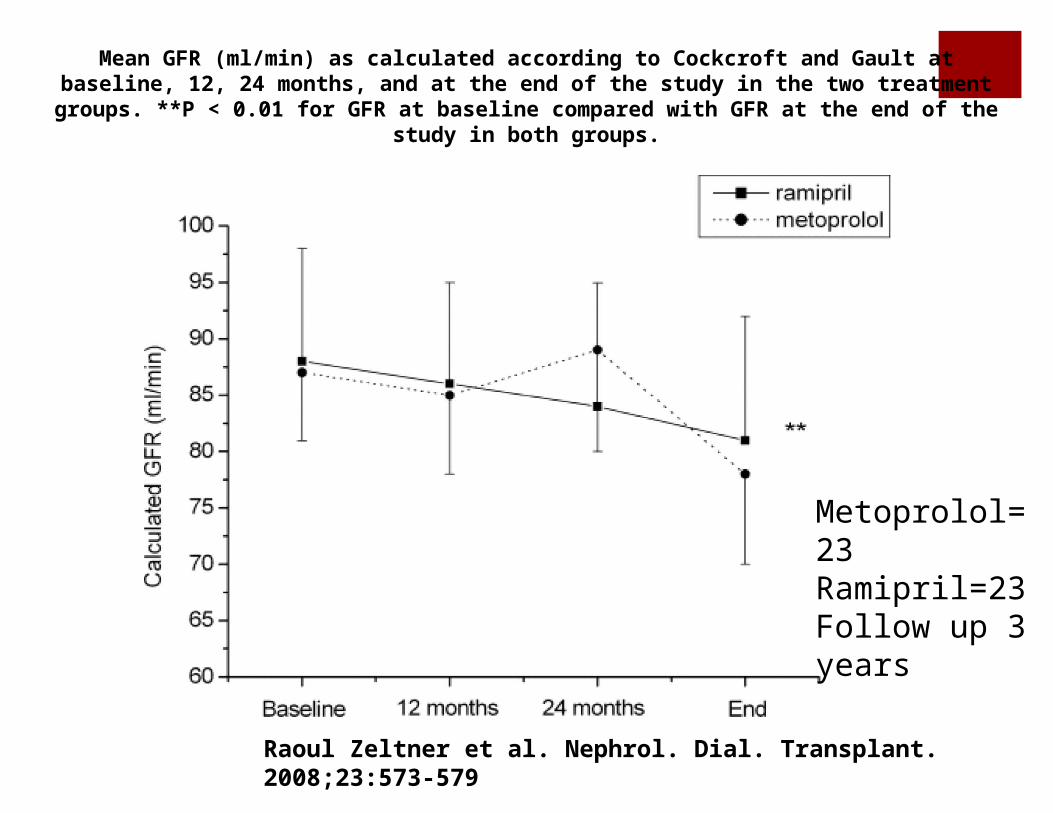
Mean GFR (ml/min) as calculated according to Cockcroft and Gault at baseline, 12, 24 months, and at the end of the study in the two treatment groups. **P < 0.01 for GFR at baseline compared
with GFR at the end of the study in both groups.
Raoul Zeltner et al. Nephrol. Dial. Transplant. 2008;23:573-579
Metoprolol=23 Ramipril=23 Follow up 3 years
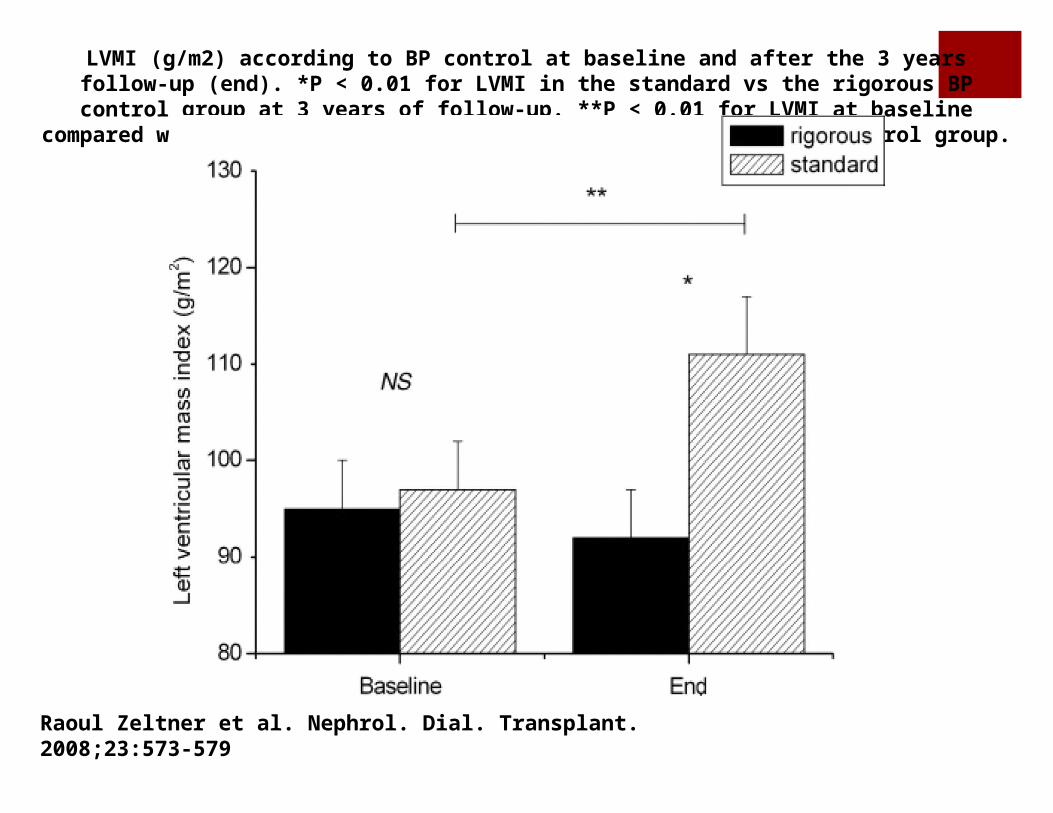
LVMI (g/m2) according to BP control at baseline and after the 3 years follow-up (end). *P < 0.01 for LVMI in the standard vs the rigorous BP control group at 3 years of follow-up. **P < 0.01 for LVMI at baseline compared with LVMI at the end of the study in the standard BP control group.
Raoul Zeltner et al. Nephrol. Dial. Transplant. 2008;23:573-579


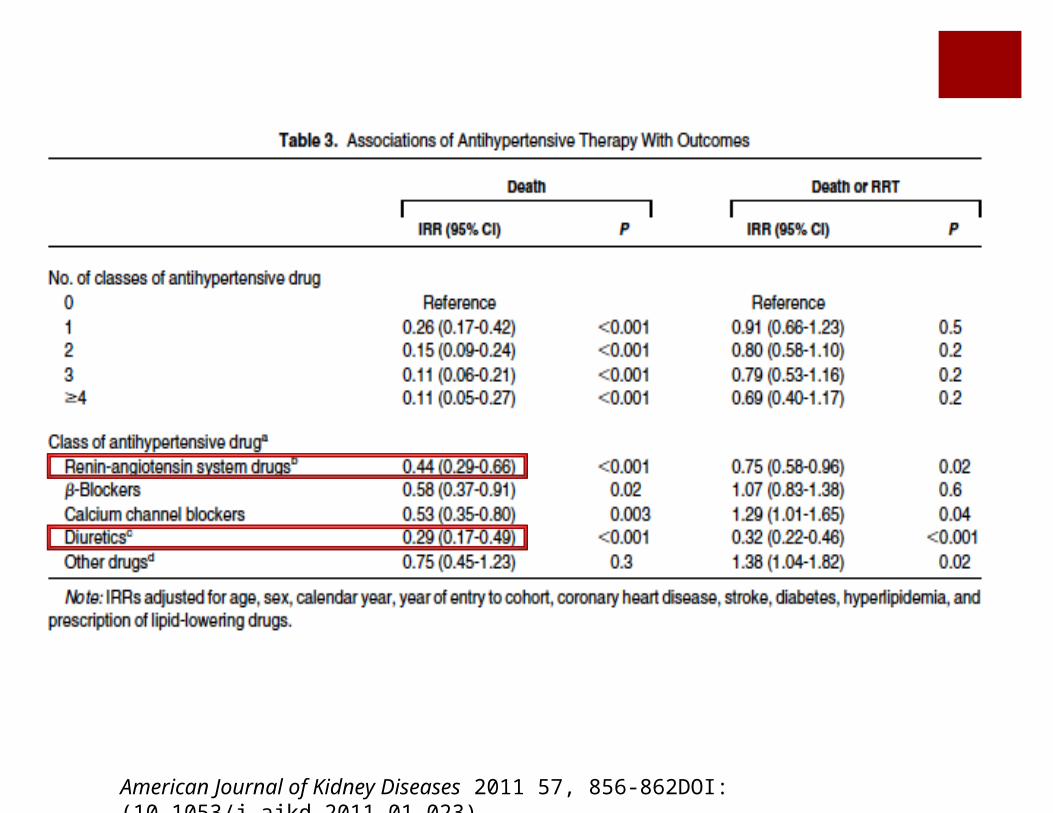
Figure 1
American Journal of Kidney Diseases 2011 57, 856-862DOI: (10.1053/j.ajkd.2011.01.023)
American Journal of Kidney Diseases 2011 57, 856-862DOI: (10.1053/j.ajkd.2011.01.023)

Is there an Ideal Target?
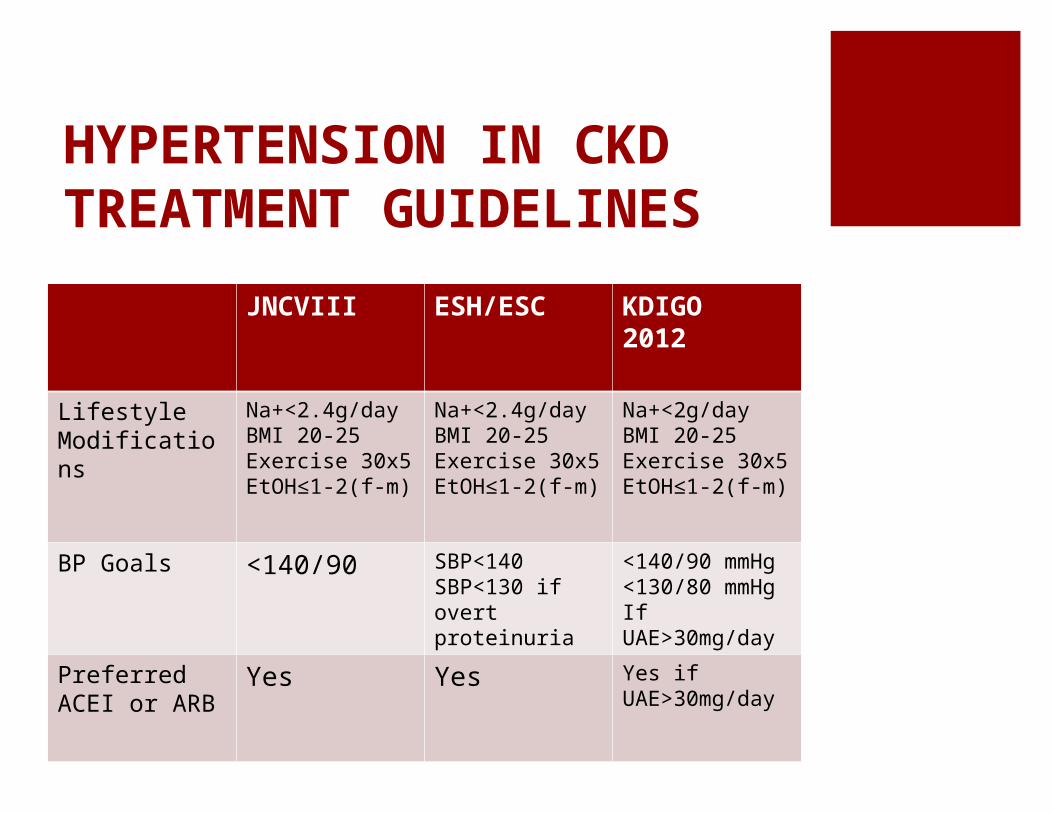
HYPERTENSION IN CKDTREATMENT GUIDELINES
JNCVIII ESH/ESC KDIGO2012
Lifestyle Modifications
Na+<2.4g/dayBMI 20-25Exercise 30x5EtOH≤1-2(f-m)
Na+<2.4g/dayBMI 20-25Exercise 30x5EtOH≤1-2(f-m)
Na+<2g/dayBMI 20-25Exercise 30x5EtOH≤1-2(f-m)
BP Goals <140/90 SBP<140SBP<130 if overt proteinuria
<140/90 mmHg<130/80 mmHgIf UAE>30mg/day
Preferred ACEI or ARB
Yes Yes Yes if UAE>30mg/day
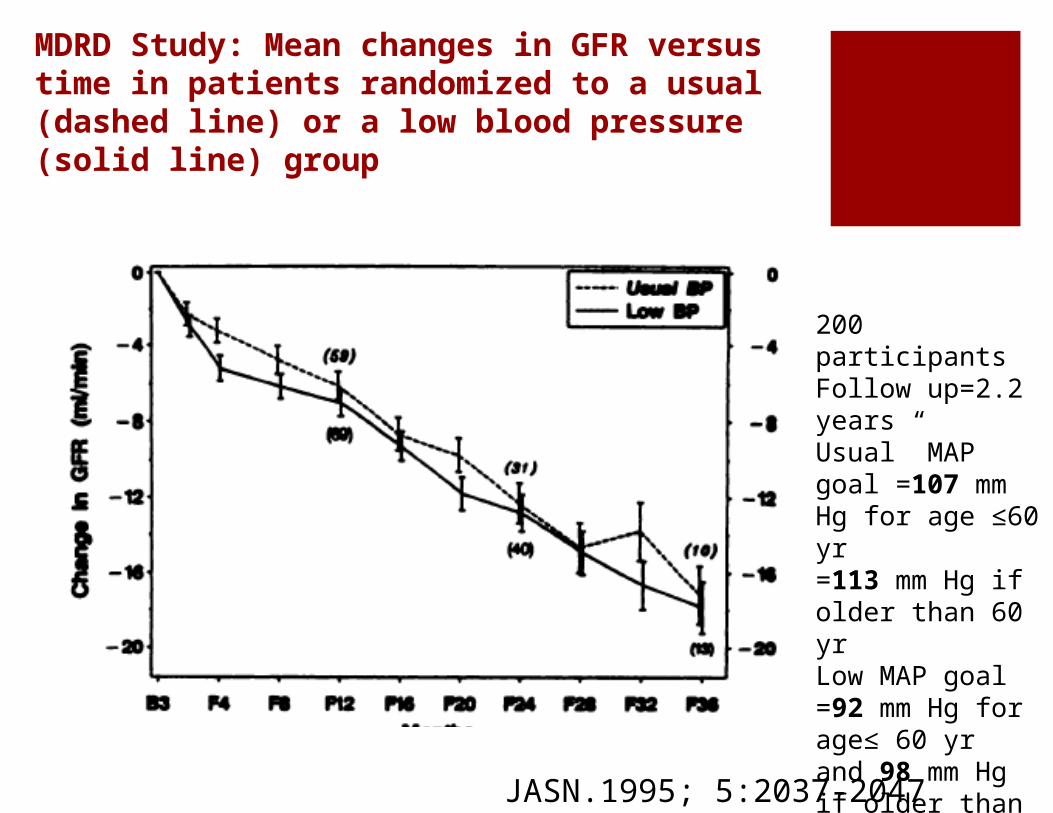
MDRD Study: Mean changes in GFR versus time in patients randomized to a usual (dashed line) or a low blood pressure (solid line) group
JASN.1995; 5:2037-2047
200 participantsFollow up=2.2 yearsUsual” MAP goal =107 mm Hg for age ≤60 yr =113 mm Hg if older than 60 yrLow MAP goal =92 mm Hg for age≤ 60 yr and 98 mm Hg if older than 60 yr.
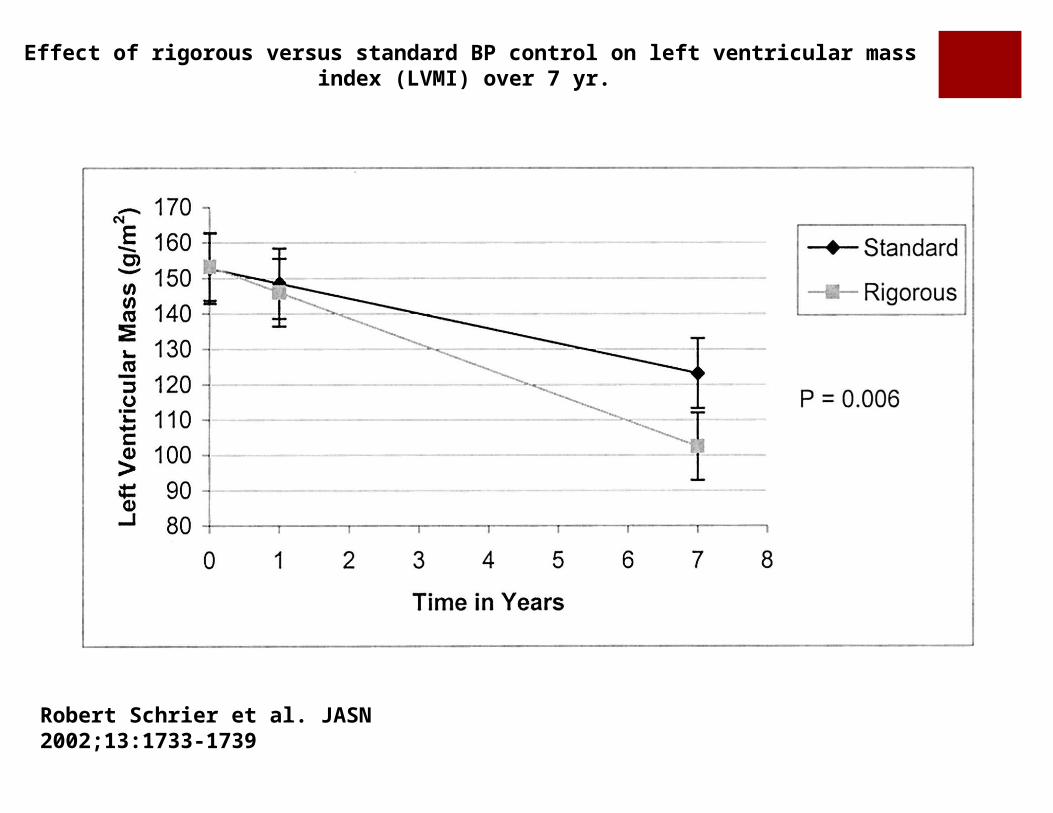
Effect of rigorous versus standard BP control on left ventricular mass index (LVMI) over 7 yr.
Robert Schrier et al. JASN 2002;13:1733-1739
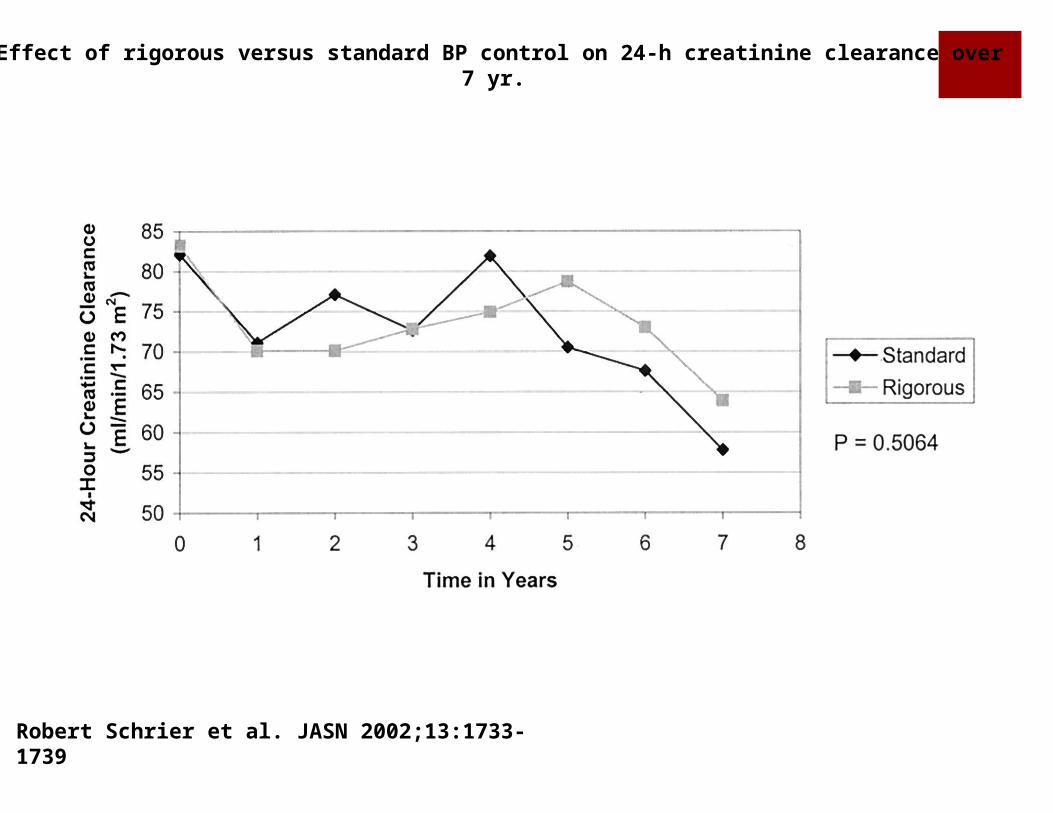
Effect of rigorous versus standard BP control on 24-h creatinine clearance over 7 yr.
Robert Schrier et al. JASN 2002;13:1733-1739

HALT-PKD TRIAL: Goals and Design
Intervention BP Target(mmHg)
PrimaryOutcome
Study A(CKD1-2)N=558
1.ACE+ARB2.ACE3.ACE+ARB4.ACE
120-130/70-80120-130/70-8095-110/60-7595-110/60-75
Change in renal volume by MRI
Study B(CKD 3)N=470
1.ACE+ARB2.ACE
110-130/70-80110-130/70-80
Doubling in serum creatinineESRD/Death
Goals: 1)ACEI+ARB> ACEI alone (CKD 1-3) 2)Low>standard BP target (CKD1-2)

HALT-PKD TRIAL: Protocol for addition of antihypertensive agents
Step Treatment Control
1-4 Combination ACE-ARB:ACELisinopril 5 mgLisinopril 10 mgLisinopril 20 mgLisinopril 40 mg
Combination ACE-ARB:ARBTelmisartan 40 mgTelmisartan 40 mgTelmisartan 80 mgTelmisartan 80 mg
ACE-I
Lisinopril 5 mgLisinopril 10 mgLisinopril 20 mgLisinopril 40 mg
Placebo
5 Hydrochlorothiazide 12.5 mg Hydrochlorothiazide 12.5 mg
6-8 Metoprolol 50 mg BIDMetoprolol 100 mg BIDMetoprolol 200 mg BID
Metoprolol 50 mg BIDMetoprolol 100 mg BIDMetoprolol 200 mg BID
9 onwards Non dihydropyridine calcium channel blocker (diltiazem), clonidine, minoxidil, hydralazine at discretion of investigator
Non dihydropyridine calcium channel blocker (diltiazem), clonidine, minoxidil, hydralazine at discretion of investigator

Total Kidney Volume and Estimated Glomerular Filtration Rate (eGFR) during Follow-up and Subgroup Analyses, According to Blood-Pressure
Group.
Schrier RW et al. N Engl J Med 2014;371:2255-2266.

Changes in Total Kidney Volume and eGFR during Follow-up, and Subgroup Analyses, According to Treatment Group.
Schrier RW et al. N Engl J Med 2014;371:2255-2266.
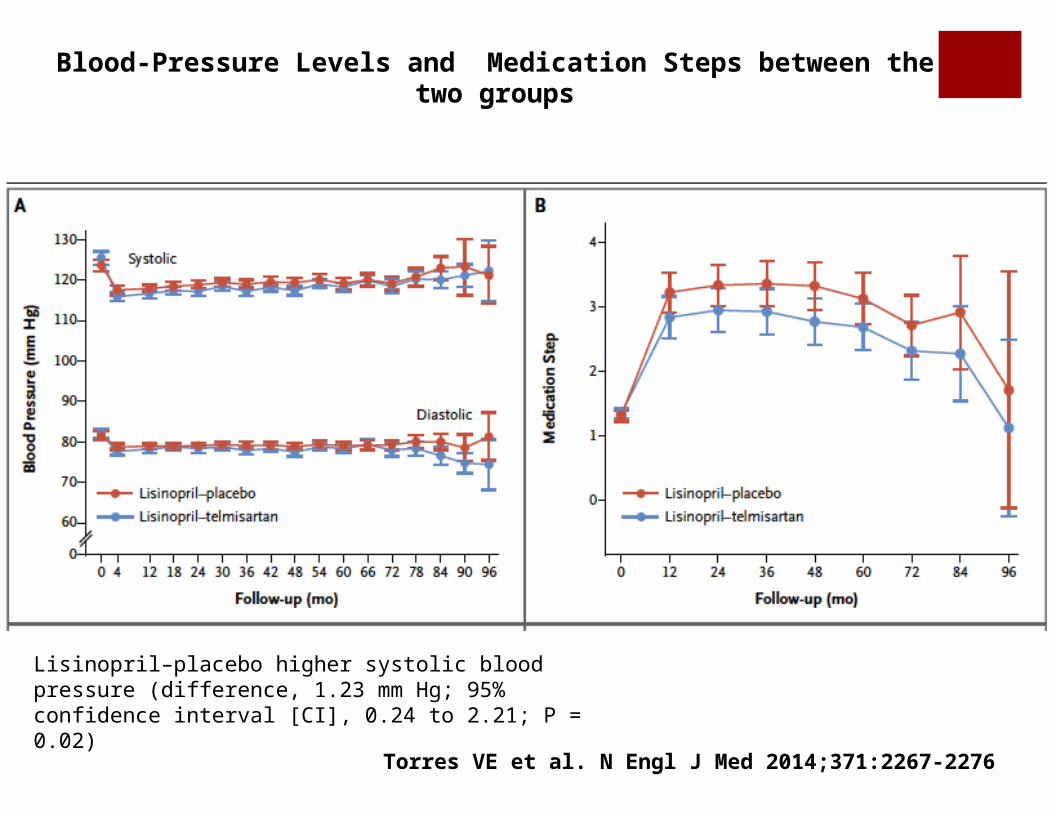
Blood-Pressure Levels and Medication Steps between the two groups
Torres VE et al. N Engl J Med 2014;371:2267-2276
Lisinopril–placebo higher systolic blood pressure (difference, 1.23 mm Hg; 95% confidence interval [CI], 0.24 to 2.21; P = 0.02)

Urinary Aldosterone and Albumin Excretion in both groups
Torres VE et al. N Engl J Med 2014;371:2267-2276
P=0.08
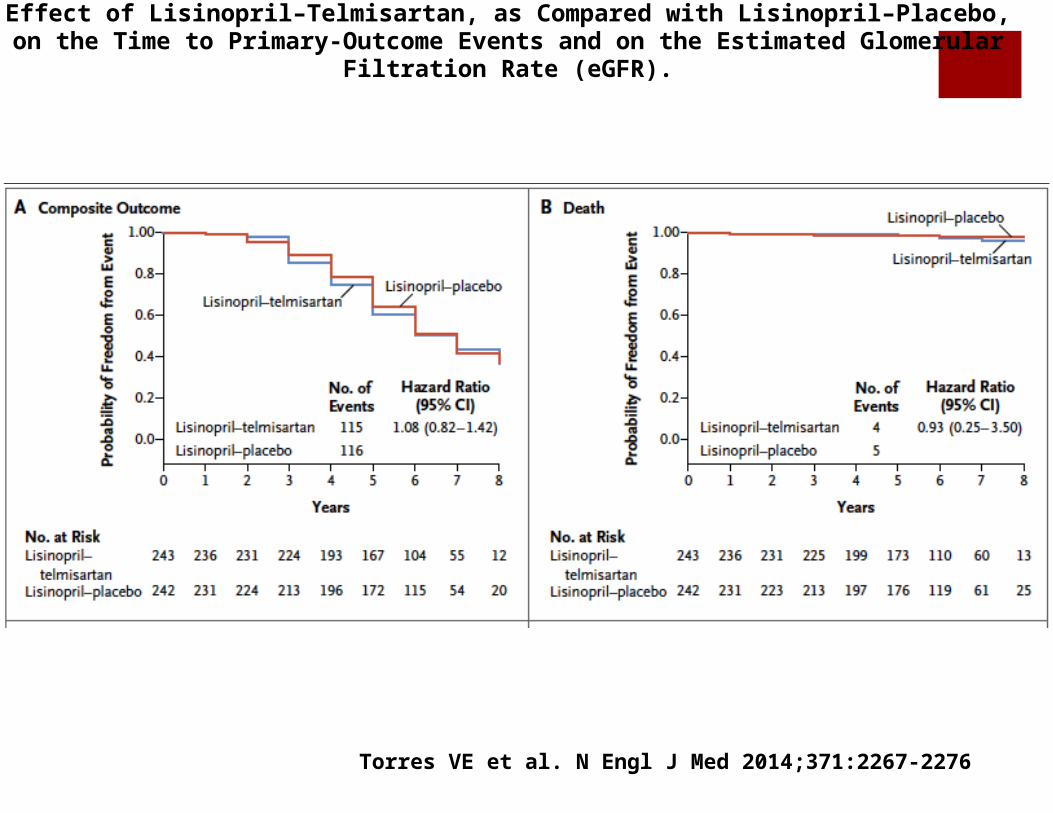
Effect of Lisinopril–Telmisartan, as Compared with Lisinopril–Placebo, on the Time to Primary-Outcome Events and on the Estimated Glomerular Filtration Rate (eGFR).
Torres VE et al. N Engl J Med 2014;371:2267-2276

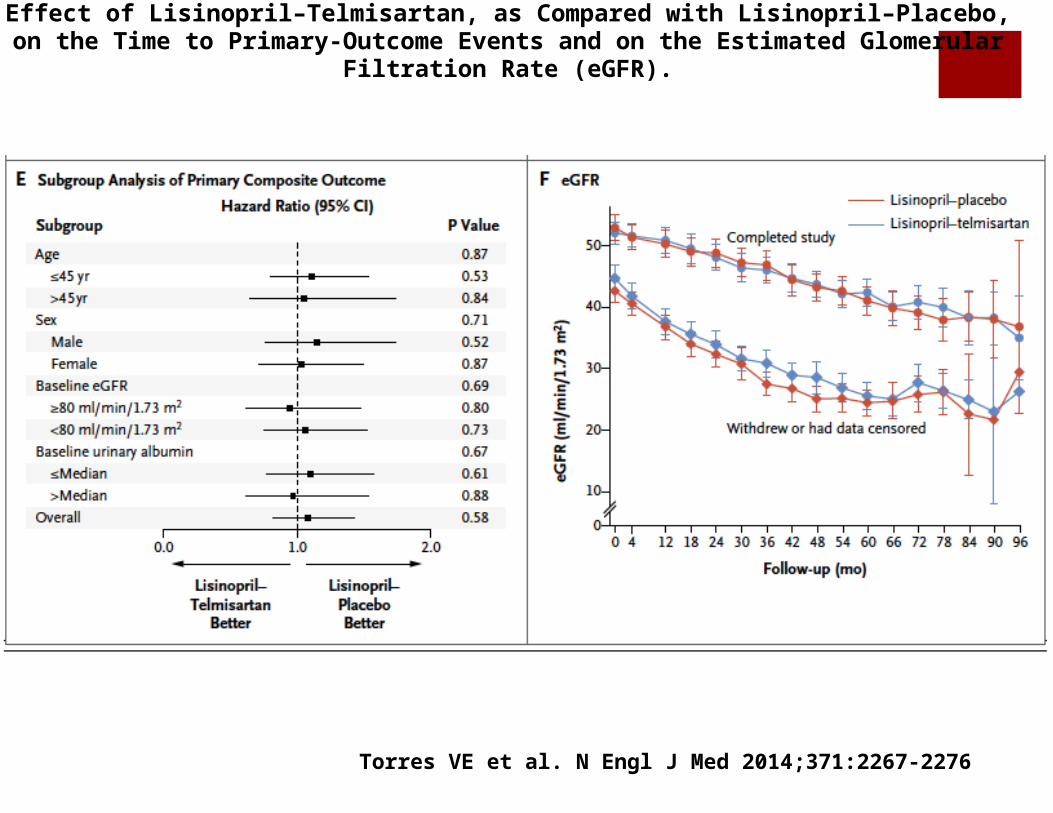
Effect of Lisinopril–Telmisartan, as Compared with Lisinopril–Placebo, on the Time to Primary-Outcome Events and on the Estimated Glomerular Filtration Rate (eGFR).
Torres VE et al. N Engl J Med 2014;371:2267-2276
Effect of Lisinopril–Telmisartan, as Compared with Lisinopril–Placebo, on the Time to Primary-Outcome Events and on the Estimated Glomerular Filtration Rate (eGFR).
Torres VE et al. N Engl J Med 2014;371:2267-2276

Treatment of hypertension in the adult ADPKD population BP target ⩽ 140/90mmHg
Agents that interfere with the renin-angiotensin-aldosterone system (RAAS) are first-line BP-lowering agents
Sodium-restricted diet
Calcium channel blockers and diuretics may be preferred over beta-blockers for cardiovascular protection

THANK YOU!


















