Hyperspectral Imaging for Resection Margin Assessment ...hyperspectral imaging for margin assessment...
10
Precision Medicine and Imaging Hyperspectral Imaging for Resection Margin Assessment during Cancer Surgery Esther Kho 1 , Lisanne L. de Boer 1 , Koen K. Van de Vijver 2,3 , Frederieke van Duijnhoven 1 , Marie-Jeanne T.F.D.Vrancken Peeters 1 , Henricus J.C.M. Sterenborg 1,4 , and Theo J.M. Ruers 1,5 Abstract Purpose: Complete tumor removal during cancer surgery remains challenging due to the lack of accurate techniques for intraoperative margin assessment. This study evaluates the use of hyperspectral imaging for margin assessment by reporting its use in fresh human breast specimens. Experimental Design: Hyperspectral data were first acquired on tissue slices from 18 patients after gross sectioning of the resected breast specimen. This dataset, which contained over 22,000 spectra, was well correlated with histopathology and was used to develop a support vector machine classifica- tion algorithm and test the classification performance. In addition, we evaluated hyperspectral imaging in clinical prac- tice by imaging the resection surface of six lumpectomy speci- mens. With the developed classification algorithm, we deter- mined if hyperspectral imaging could detect malignancies in the resection surface. Results: The diagnostic performance of hyperspectral imaging on the tissue slices was high; invasive carcinoma, ductal carcinoma in situ, connective tissue, and adipose tissue were correctly classified as tumor or healthy tissue with accuracies of 93%, 84%, 70%, and 99%, respectively. These accuracies increased with the size of the area, con- sisting of one tissue type. The entire resection surface was imaged within 10 minutes, and data analysis was performed fast, without the need of an experienced operator. On the resection surface, hyperspectral imaging detected 19 of 20 malignancies that, according to the available histopathology information, were located within 2 mm of the resection surface. Conclusions: These findings show the potential of using hyperspectral imaging for margin assessment during breast- conserving surgery to improve surgical outcome. Introduction One of the major challenges of cancer surgery remains the complete removal of the tumor. Therefore, positive resection margins, which indicate that tumor resection is incomplete, are frequently found after various kinds of cancer surgery (1). Spe- cifically for breast cancer, in up to 37% of the 500,000 women undergoing breast-conserving surgery in the United States and Europe each year, resection margins are tumor positive (2–6). For these patients, additional surgery or a radiotherapy boost of the resection area is needed, which has a major impact on the cosmetic outcome, patients' quality of life, and health care costs (7, 8). Currently, evaluation of positive resection margins is per- formed by histopathologic evaluation of the margins under the microscope and typically requires several days. The number of tumor-positive resection margins could be reduced by assessing resection margins during surgery. Methods currently available in the clinic for intraoperative resection margin assessment are frozen section analysis, touch preparation cytology, intraopera- tive ultrasound, and specimen radiography (9–12). However, because these methods are either time-consuming or exhibit a low accuracy, there is still a clear unmet need for a more effective intraoperative margin assessment technique. Therefore, several other techniques have been proposed for margin assessment during breast-conserving surgery (9–25). Among these techniques are the use of various fluorescent imaging probes (13, 14), optical coherence tomography (15), photoacoustic tomography (17), and optical spectroscopic methods like Raman spectroscopy (18, 19) and diffuse reflec- tance spectroscopy (22–25). Despite the potential of these techniques, they have various drawbacks, like the need for exogenous contrast agents, excessive time to assess the entire resection surface, or a low diagnostic performance in detecting ductal carcinoma in situ (DCIS), a potential precursor of inva- sive carcinoma (IC). A promising new approach for intraoperative margin assess- ment that eliminates these drawbacks is hyperspectral (HS) imag- ing. HS imaging offers great potential for noninvasive tissue diagnosis because diffuse reflectance measurements can be per- formed fast, over a wide field of view, without tissue contact and without the need for exogenous contrast agents (26). Here, we report for the first time on margin assessment with HS imaging, specifically for breast-conserving surgery. With an HS 1 Department of Surgery, The Netherlands Cancer Institute, Amsterdam, the Netherlands. 2 Department of Pathology, The Netherlands Cancer Institute, Amsterdam, the Netherlands. 3 Department of Pathology, Ghent University Hospital, Ghent, Belgium. 4 Department of Biomedical Engineering and Physics, Amsterdam University Medical Center, Amsterdam, the Netherlands. 5 Faculty of Science and Technology, University of Twente, Enschede, the Netherlands. Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). Corresponding Author: Esther Kho, Netherlands Cancer Institute, Plesmanlaan 121, 1066 CX Amsterdam, the Netherlands. Phone: 31-20-512-7816; E-mail: [email protected] Clin Cancer Res 2019;25:3572–80 doi: 10.1158/1078-0432.CCR-18-2089 Ó2019 American Association for Cancer Research. Clinical Cancer Research Clin Cancer Res; 25(12) June 15, 2019 3572 on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089
Transcript of Hyperspectral Imaging for Resection Margin Assessment ...hyperspectral imaging for margin assessment...

Precision Medicine and Imaging
Hyperspectral Imaging for Resection MarginAssessment during Cancer SurgeryEsther Kho1, Lisanne L. de Boer1, Koen K. Van de Vijver2,3,Frederieke van Duijnhoven1, Marie-Jeanne T.F.D. Vrancken Peeters1,Henricus J.C.M. Sterenborg1,4, and Theo J.M. Ruers1,5
Abstract
Purpose: Complete tumor removal during cancer surgeryremains challenging due to the lack of accurate techniques forintraoperativemargin assessment. This study evaluates the useof hyperspectral imaging for margin assessment by reportingits use in fresh human breast specimens.
Experimental Design: Hyperspectral data were firstacquired on tissue slices from18patients after gross sectioningof the resected breast specimen. This dataset, which containedover 22,000 spectra, was well correlated with histopathologyand was used to develop a support vector machine classifica-tion algorithm and test the classification performance. Inaddition, we evaluated hyperspectral imaging in clinical prac-tice by imaging the resection surface of six lumpectomy speci-mens. With the developed classification algorithm, we deter-mined if hyperspectral imaging could detect malignancies inthe resection surface.
Results: The diagnostic performance of hyperspectralimaging on the tissue slices was high; invasive carcinoma,ductal carcinoma in situ, connective tissue, and adiposetissue were correctly classified as tumor or healthy tissuewith accuracies of 93%, 84%, 70%, and 99%, respectively.These accuracies increased with the size of the area, con-sisting of one tissue type. The entire resection surface wasimaged within 10 minutes, and data analysis was performedfast, without the need of an experienced operator. On theresection surface, hyperspectral imaging detected 19 of 20malignancies that, according to the available histopathologyinformation, were located within 2 mm of the resectionsurface.
Conclusions: These findings show the potential of usinghyperspectral imaging for margin assessment during breast-conserving surgery to improve surgical outcome.
IntroductionOne of the major challenges of cancer surgery remains the
complete removal of the tumor. Therefore, positive resectionmargins, which indicate that tumor resection is incomplete, arefrequently found after various kinds of cancer surgery (1). Spe-cifically for breast cancer, in up to 37% of the 500,000 womenundergoing breast-conserving surgery in the United States andEurope each year, resectionmargins are tumor positive (2–6). Forthese patients, additional surgery or a radiotherapy boost of theresectionarea is needed,whichhas amajor impact on the cosmeticoutcome, patients' quality of life, and health care costs (7, 8).
Currently, evaluation of positive resection margins is per-formed by histopathologic evaluation of the margins under the
microscope and typically requires several days. The number oftumor-positive resection margins could be reduced by assessingresection margins during surgery. Methods currently available inthe clinic for intraoperative resection margin assessment arefrozen section analysis, touch preparation cytology, intraopera-tive ultrasound, and specimen radiography (9–12). However,because these methods are either time-consuming or exhibit alow accuracy, there is still a clear unmet need for a more effectiveintraoperative margin assessment technique.
Therefore, several other techniques have been proposed formargin assessment during breast-conserving surgery (9–25).Among these techniques are the use of various fluorescentimaging probes (13, 14), optical coherence tomography (15),photoacoustic tomography (17), and optical spectroscopicmethods like Raman spectroscopy (18, 19) and diffuse reflec-tance spectroscopy (22–25). Despite the potential of thesetechniques, they have various drawbacks, like the need forexogenous contrast agents, excessive time to assess the entireresection surface, or a low diagnostic performance in detectingductal carcinoma in situ (DCIS), a potential precursor of inva-sive carcinoma (IC).
A promising new approach for intraoperative margin assess-ment that eliminates these drawbacks is hyperspectral (HS) imag-ing. HS imaging offers great potential for noninvasive tissuediagnosis because diffuse reflectance measurements can be per-formed fast, over a wide field of view, without tissue contact andwithout the need for exogenous contrast agents (26).
Here, we report for the first time onmargin assessment withHSimaging, specifically for breast-conserving surgery. With an HS
1Department of Surgery, The Netherlands Cancer Institute, Amsterdam, theNetherlands. 2Department of Pathology, The Netherlands Cancer Institute,Amsterdam, the Netherlands. 3Department of Pathology, Ghent UniversityHospital, Ghent, Belgium. 4Department of Biomedical Engineering and Physics,AmsterdamUniversity Medical Center, Amsterdam, the Netherlands. 5Faculty ofScience and Technology, University of Twente, Enschede, the Netherlands.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Esther Kho, Netherlands Cancer Institute, Plesmanlaan121, 1066 CX Amsterdam, the Netherlands. Phone: 31-20-512-7816; E-mail:[email protected]
Clin Cancer Res 2019;25:3572–80
doi: 10.1158/1078-0432.CCR-18-2089
�2019 American Association for Cancer Research.
ClinicalCancerResearch
Clin Cancer Res; 25(12) June 15, 20193572
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089

camera, diffuse reflectance images were obtained of fresh breastspecimens. In these images, each pixel contained an entire spec-trum from approximately 900 to 1,700 nm, which reflects opticaldifferences in tissue composition andmorphology between tissuetypes. First, we acquired data from tissue slices that were obtainedafter gross sectioning of resected breast specimens. This datasetcontained spectra of all different tissue types with accurate his-topathologic annotations and was used to develop and test atissue classification algorithm. Next, we imaged the resectionsurface of lumpectomy specimens to evaluate HS imaging in away similar to the intended application in the clinical workflow.In addition, we applied the developed classification algorithm topredict malignancies in these resection surfaces.
Materials and MethodsHS imaging system
HS images were obtained using an HS imaging system (VLNIRCL-350-N17E, Specim, Spectral Imaging Ltd.) that captures lightin the near-infrared (�900–1,700 nm, 256 wavelength bands,5 nm increments) with an InGaAs sensor (320 � 256 pixels).Previous research showed that this wavelength range containsdistinctive information for a robust discrimination betweentumor and healthy breast tissue (27, 28). Figure 1 shows the HSimaging setup. The tissue was placed upon a translation stage andilluminated with three halogen light sources that excite light overthe full wavelength range of our camera, under an angle of 45degrees. After penetration into the tissue, the light underwentmultiple scattering and absorption events and was subsequentlycaptured by the camera. The imaged scene was captured line-by-line by moving the translation stage. Each imaged line contained320 pixels, and on average 200 lines were obtained per tissuespecimen. Thereby, a 3D hypercube was created, in which eachpixel in the 2D image contained one spectrum. The scanningspeed was adjusted to 50 lines per second to match the spatialresolution of the imaged line (�0.5 mm/pixel). Due to the lowsensitivity of the InGaAs sensor at the edges of the spectral range,
only wavelengths between 953.25 and 1645.62 nm (210 wave-length bands) were used.
Study designMeasurements were performed on ex vivo fresh breast tissue
from female patients that had primary breast surgery at the Antonivan Leeuwenhoek hospital and did not receive neoadjuvanttreatment. This study was performed in compliance with theDeclaration of Helsinki and approved by the Institutional ReviewBoard of The Netherlands Cancer Institute/Antoni van Leeuwen-hoek (Amsterdam, the Netherlands). According to Dutch law(WMO), no written-informed consent from patients wasrequired. The involved surgeons and pathologist were blindedto any HS information. In total, two datasets were obtained fromdifferent patients.
Data acquisition of tissue slicesIn the first dataset, HS data were acquired of tissue slices to
minimize spatial registration artifacts between HS images andhistopathology information. Fresh lumpectomy specimens weretransferred to the pathology department immediately after resec-tion, where they were colored and sliced according to standardprocedure. In consultation with the pathologist, one tissue sliceper patient that contained both healthy and tumor tissue wasselected. This slice was placed in a macrocassette, on top of blackrubber, where it remained during the optical measurements. Theblack rubber highly absorbs light over the whole wavelengthrange and prevented that the macrocassette under the tissue wasmeasured. In total, 18 tissue slices from different patients weremeasured. The age of these patients was 67 � 11 years (mean �SD), and their American College of Radiology (ACR) score, whichreflects thebreast density,was 2.18�0.95 (mean� SD). The slices
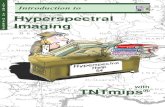
Figure 1.
HS data acquisition and HS data. A, The HSmeasurement setup. The breastspecimen was placed upon the translational stage and imaged line by line bymoving the translational stage. Thereby, an area of 20� 10 cm2 was scannedin 4 seconds, creating a 3D HS image (B), in which each pixel contains onespectrum (C).
Translational Relevance
Breast-conserving surgery in combination with adjuvanttreatment is the preferred treatment for women with breastcancer. These surgeries, however, remain challenging becausevisualization of the tumor is difficult, andnodirect feedback oftumor-positivemargins, which indicate that tumor resection isincomplete, is possible. Therefore, additional surgery or aradiotherapy boost is often required to clear tumor tissue thatis left behind during the initial operation. This study evaluatesthe use of hyperspectral imaging for tumor detection in freshhuman breast tissue specimens. Thereby, a high diagnosticperformance on sliced breast specimen was reported. In addi-tion, hyperspectral imaging was much faster compared withcurrently available margin assessment techniques. Becausedata acquisition and analysis can be performed in the oper-ation theater, it would be possible to provide near real-timefeedback to the surgeon. This offers potential for re-excisingsuspected tumor-positive margins during the initial operationin the future.
Hyperspectral Imaging for Resection Margin Assessment
www.aacrjournals.org Clin Cancer Res; 25(12) June 15, 2019 3573
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089

varied in size from2� 3.5 cm2 to 4.5� 6.3 cm2 andwere at least 2mm thick. In addition to the HS image, a white light (WL) imageof the tissue was taken from the same point of view. All opticalmeasurements tookplacewithin10minutes after collectionof thetissue slice at the pathology department. After the measurements,the slices were placed in formalin and further processed accordingto standard protocol.
After a few days, hematoxylin and eosin (H&E)–stained sec-tionsof themeasured surface of the tissue sliceswereobtained anddigitized (Aperio ScanScope, Leica Microsystems B.V.). To correctfor tissue deformations during histopathologic processing, theH&E sections were registered to the HS images using MATLAB2015a (The Math Works Inc.). Supplementary Fig. S1 shows thisregistration process. First, the whole H&E section was annotatedwith tissue classes aftermanually removing the background in theH&E section. These tissue classes were IC, its potential precursorDCIS, adipose tissue, connective tissue, and healthy glandularducts. IC, DCIS, and glandular ducts were annotated on the H&Esection using delineations drawn by the pathologist. The remain-ing tissue was annotated as connective or adipose tissue bythresholding all RGB channels of the H&E section in MATLABat 90%: adipose tissue was washed away in the histopathologicprocessing and was therefore white on the digitized H&E image,whereas connective tissue colored red/pink with the H&E stain.Second, a transformation matrix was obtained of the registrationof the nonannotated H&E section to the WL image. The H&Esection was resized to the size of the WL image and, based ondistinctive features both visible in the H&E section and the WLimage, control points weremanually selected in both images (theminimum pair used was 61). Therefore, each point in the H&Esection had a corresponding point in the WL image. Using anonrigid local weightedmeans transformation with 12 neighbor-ing control points, the H&E section was registered to the WLimage. With this transformation matrix, also the annotatedH&E section was registered to theWL image. Third, the annotatedH&E section was registered to the HS image. For this, we used thetransformation matrix that described the registration of the WLimage to the HS image. Because the WL image was taken simul-taneously to theHS image, the tissue did not deform and a simplerigid registration based on the edges of the tissue sufficed. Finally,with the H&E section, all pixels in the HS image were labeled asIC, DCIS, adipose tissue, or connective tissue. Because healthyglandular ducts were often smaller than the pixel size of our HScamera, they were included in the connective tissue class. Due tothe highly inhomogeneous character of connective tissue, con-nective tissue was often observed in an HS pixel along withanother tissue class. In the event that multiple tissue classes wereobserved in one HS pixel, this pixel was labeled as "unknown."
Data acquisition of resection surfaceThe second dataset was used to evaluate HS imaging of lump-
ectomy specimens in the current clinical workflow.Ourmain goalwas to evaluate the amount of time required to image the entireresection surface and to analyze the data. In addition, we evalu-ated whether HS imaging could detect malignancies within 2mmof the resection surface.
In total, six fresh lumpectomy specimens were imaged imme-diately after resection. To ensuremeasuring tumor at the resectionsurface, lumpectomy specimens were selected that, according tothe surgeon, were suspicious for tumor-positive resection mar-gins. The age of these patients was 61� 8 years (mean� SD), their
ACR score was 2.67 � 0.52 (mean � SD), and the size of thespecimens varied from 16 to 118 cm3. The resection surface of thespecimen was imaged from six sides by repositioning the spec-imen. As guidance for repositioning, we used sutures that wereplaced on the specimen during surgery, which allows for reori-entation by pathology. The resection specimen was placed onblack polyoxymethylene material that, like the black rubber,highly absorbs light over the whole wavelength range. After theoptical measurements, the specimens were brought to the pathol-ogy department. According to standard pathology protocol, theywere painted and sliced from nipple to peripheral side. Of allspecimens, 43 of 66 slices (�3 mm thick) were further processedin H&E-stained sections (�3 mm thick). Two sections per spec-imen, taken at the nipple- andperipheral side,were excluded fromfurther analysis because they were taken parallel to the resectionsurface and thus did not provide histopathology informationabout the resection margin width. On the remaining 31 H&Esections, the pathologist delineated IC and DCIS so that we couldcalculate the shortest distance between the inked resection edgeand the malignant tissue. Due to the limited number of H&Esections and the perpendicular orientation of the sections to theresection surface, it was not possible to verify the entire HS imageof a resection side with histopathology. Therefore, we limited theanalysis of HS margin assessment to verifying whether a malig-nant area, containing IC or DCIS, within 2 mm of the resectionsurface was detected with HS imaging. Two millimeter is therequired tumor-free margin width for DCIS according to guide-lines of the Society of Surgical Oncology (SSO)-American Societyfor Radiation Oncology (ASTRO)-American Society of ClinicalOncology (ASCO; ref. 29). We used the color of the histopathol-ogy paint at the edge near the malignant area to determine itslocationon the resection surface. Amalignant areawas consideredcorrectly detected with HS analysis if at least one pixel in thislocation was classified as IC or DCIS.
PreprocessingAll data analysis and tissue classification were performed
using MATLAB. Prior to spectral classification, HS data werepreprocessed.
First, raw tissue images were converted into normalized diffusereflectance to correct for spectral nonuniformity of the illumina-tion setup and the influence of the dark current using:
Rðx;lÞ ¼ 1Rref ðlÞ �
Imagetissueðx;lÞ � Imagedarkðx;lÞImagewhiteðx;lÞ � Imagedarkðx; lÞ � 100% ð1Þ
Where R(x,l) is the normalized diffuse reflectance (in percent-age), Rref(l) is the reference reflectance value of Spectralon (SRT-99-100, Lapsphere, Inc.), x is the location of the pixel in theimaged line, and l is the wavelength band. Imagewhite(l) andImagedark(l) are the reference images acquired in addition to thetissue image. The white reference image was acquired on Spec-tralon99%, and for thedark reference image,we closed the shutterof the camera. Prior to normalization of raw tissue images, weapplied a pixel-wise third-order correction model to the raw HSdata to correct for the slight nonlinearity of our InGaAs sensor.This model describes the sensors signal output with respect to theamount of light incident on the sensor.
Second, all spectra were preprocessed to eliminate spectralvariability due to tissue morphology effects. The oblique
Kho et al.
Clin Cancer Res; 25(12) June 15, 2019 Clinical Cancer Research3574
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089

illumination and nonflat surface of the tissue could cause unevenillumination of the tissue and nonspecific scatter. As shown inSupplementary Fig. S2, this could result in variations betweenspectra thatwere not related to the physiologic composition of thetissue. To correct for this, spectra were preprocessed using stan-dard normal variate (SNV; refs. 30, 31). SNV normalized eachindividual spectrum to a mean of zero and an SD of one andallowed for a robust and direct suppression of baseline drifts andmultiplicative scaling (31).
ClassificationClassification of tissue slices. The dataset acquired on the tissueslices contained approximately 51,000 spectra that were labeledwith one of the tissue classes. Spectra were excluded if they werecontaminated with pathology ink (�4,200 spectra), if the InGaAssensor saturated (112 spectra), or if spectra were located within0.5 mm of a tissue class border (�23,700 spectra). The lattercauses a larger amount of spectra from smaller tissue class pockets,like DCIS and connective tissue, to be excluded. In addition,spectral outliers were detected and eliminated per tissue class (IC¼ 370 of 5,193 spectra, DCIS¼ 7 of 613 spectra, connective¼ 37of 652 spectra, adipose¼ 563 of 16,948 spectra), using an outlierdetection method (32). This method calculated the SD of allEuclideandistances of a spectrum to the groupmeanand removeda spectrum when this distance was larger than three SDs.
A supervised classification model was developed using linearsupport vector machine (SVM). SVM is based on statistical learn-ing theory and separates two classes by determining an optimalhyperplane that maximizes the margin between two classes inmultidimensional space (33). With the one-against-one strategy,multiclass classification was realized so that each spectrum wasclassified into IC, DCIS, connective, or adipose tissue (34). Ofeach spectrum, both the intensity of all 210wavelength bands andthe pathology labels were used as input for the SVM classificationalgorithm. SVM was implemented using the software tool Per-Class (Academic version 5.0, PR Sys design). To develop thealgorithm with the largest amount of data, we first removed allspectra from one tissue slice from the dataset to use as test set.Second, with spectra from the remaining 17 slices, the algorithmwas developed using innercross validation: the 17 slices wererandomly split 5 times in a training set (2/3 of the slices) and avalidation set (1/3 of the slices) while keeping spectra from one
slice together. Finally, the trained SVM was applied on the test setfor evaluation of the classification performance. To account forvariability in the classification performance, this process wasrepeated until all tissue slices were used as test set. To correct forthe unbalancednumber of spectra per tissue class, each tissue classwas assigned a different weight, which is the inverse ratio of thetissue class sizes (35).
Classification of resection surface. HS images acquired on theresection surface were analyzed with a classification algorithmdeveloped with all tissue slices. The same linear, weighted SVMalgorithm as described above was used. However, instead oftraining the algorithm with 17 tissue slices, all 18 tissue sliceswere used. All the spectra in the HS image on the resection surfacewere SNV normalized and classified with the SVM algorithm aseither IC, DCIS, connective, or adipose tissue.
Classification performanceClassification performance of HS imaging on breast tissue was
evaluatedon the tissue slices thatwere used as test set. The numberof spectra per tissue class varied between tissue slices. Therefore,we calculated classification accuracies over all spectra instead ofaveraging accuracies over the tissue slices. Both the overall accu-racy to discriminate tissue classes and the accuracy per tissue classwere calculated. ROC curves and the area under the ROC curve(AUC), however, were calculated per tissue slice, and subsequent-ly averaged. Because classification with SVMwas performed usingthe one-against-one strategy, one ROC curve for each pair of tissueclasseswas obtained. For the resectionmargin dataset, no accuratecorrelationwithhistopathology could beobtainedwith thewholeHS image due to the limited number of H&E sections and theirperpendicular orientation to the resection surface. As a result, theclassification performance of resection margin assessment withHS imaging could not be evaluated. Nevertheless, we did assesswhether HS analysis confirms tumor-positive margins found onthe available H&E sections.
ResultsClassification results from tissue slices
The 18 tissue slices comprised an HS dataset of more than22,000 reliable spectra, which were classified as IC, DCIS,
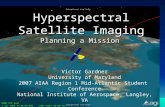
Figure 2.
Representative examples of two tissueslices. From left to right: WL image(A and E), histopathology H&E section(B and F), annotated H&E section(C and G), and HS classification resultusing the SVM algorithm (D and H). Themalignant tissue in the top row (A–D) ismainly IC, whereas the malignant tissuein the bottom row (E–H) consists ofmalignant pockets of DCIS. White pixelsin the classified HS image indicate pixelsthat could not be classified due to eitherhigh specular reflection or the presenceof pathology ink. Gray pixels are pixelsof which no histopathology wasavailable. The arrow (D) points out theincorrectly classified connective spectrathat are located near the border of thearea with IC.
Hyperspectral Imaging for Resection Margin Assessment
www.aacrjournals.org Clin Cancer Res; 25(12) June 15, 2019 3575
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089

connective, or adipose tissue using an SVM classification algo-rithm. Supplementary Fig. S3 shows an example of the tissueclasses and the average diffuse reflectance spectra per tissue classbefore and after SNV normalization. Based on the average SNVnormalized reflectance spectra, differences between tissue classeswere most noticeable around absorption bands of the dominantchromophores in the near-infrared region. For adipose tissue, thelarge amount of fat in the tissue was discriminating, whereasspectral differences between connective tissue and the malignantclasses weremainly related to the amount ofwater and collagen inthe tissue. Figure 2 shows the HS classification result of tworepresentative examples of tissue slices that contain IC (top) andDCIS (bottom). Table 1 shows the classification results of the HSanalysis of all spectra in the dataset. Overall, we could discrim-
inate the defined tissue classes with a diagnostic accuracy, aver-aged over all tissue slices, of 91%. Of these tissue classes, adiposetissue and IC were detected as, respectively, healthy and tumortissue in 99% and 93%. The more challenging tissue types wereDCIS and connective tissue, which were classified as, respectively,tumor and healthy tissue in 84% and 70%. These numbers are inaccordancewith the AUCs shown in Fig. 3. A high AUC is reportedfor both IC (0.90, 0.99, and 1.00) and adipose tissue (3 times1.00), and a lower AUC (0.78 � 0.12) is reported for the SVMclassifier that distinguishes DCIS and connective tissue. The latterindicates that DCIS and connective tissue were more likely to bemistaken for each other. These classification results were based onall individual 22,000 spectra, without considering the spatialinformation of the HS images. However, the surroundings of aspectrum might have a strong influence on the classificationaccuracy. For example, in the classified HS image in Fig. 2D, mostof the incorrectly classified connective spectra are located near theborder of the area with IC.
Smallest detectable size of tumor pocketsTo evaluate the influence of the surroundings of a spectrum to
its classification accuracy, we calculated for each pixel its distanceto the closest tissue transition, based on the histopathologicannotation of the slices. Figure 4A illustrates this by showing atissue slice that contains IC and adipose tissue. As can be seenin Fig. 4B, pixels near the IC–adipose tissue transition wereclassified with a lower accuracy. The inaccuracies that occuraround these tissue transitions affect the smallest size of a pocketthat can be detected. To assess this effect, the classificationaccuracy was calculated for each tissue class as a function of thesmallest pocket size in which a pixel was present (Fig. 4C). For
Table 1. Classification results of HS analysis compared with pathologyannotation
HS classificationTumor Healthy
IC DCIS Total Connective Adipose Total
Pathology annotationa
TumorIC 87% 6% 93% 7% 0% 7%DCIS 29% 56% 84%b 11% 4% 16%b
HealthyConnective 14% 16% 30% 66% 4% 70%Adipose 0% 1% 1% 1% 98% 99%
aIC (n ¼ 4,823, P ¼ 8), DCIS (n ¼ 606, P ¼ 9), connective (n ¼ 615, P ¼ 14), andadipose (n ¼ 16,385, P ¼ 18). n is the number of spectra, and P is the number ofpatients.bDue to rounding of percentages, the total percentage is not equal to the sum ofIC and DCIS or connective and adipose tissue.
Figure 3.
ROC curves of one-against-one SVM classification.ROC curves are calculated for IC (A), DCIS (B),connective tissue (C), and adipose tissue (D) againstthe other classes. ROC curves and the AUC arecalculated on the test set for each tissue slice andsubsequently averaged. The AUC is given as theaverage� SD.
Kho et al.
Clin Cancer Res; 25(12) June 15, 2019 Clinical Cancer Research3576
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089

each pixel, this smallest pocket size was estimated as twice theshortest distance to a tissue transition. The classification accuracywas determined for the ability of HS imaging to differentiate themalignant tissue types from the two healthy tissue types and viceversa. We found that for all tissue types, the classification accuracyper tissue class increased with an increase of the smallest pocketsize in which the pixel is located. Specifically, pixels in all tissuetypepockets larger than2�2mmwere correctly classified inmorethan 93% of cases (Fig. 4C). This also includes the two tissueclasses, DCIS and connective tissue, which exhibited the lowestclassification results in Table 1 and Fig. 3.
HS imaging of lumpectomy specimensTo assess the entire resection surface, we imaged each specimen
from six sides and applied the diagnostic classification algorithmthat we developed using the tissue slices, to predict malignancieswithin 2mmfrom the resection surface (Fig. 5). Each resection sidewas imaged in 20 seconds and could be analyzed in 40 seconds.Imaging of the entire resection surface, including takingWL imagesand repositioning the specimen, took on average 9minutes and 15seconds.
All six specimens had at least oneH&E sectionwith amalignantarea within 2 mm from the resection surface. In total, 31 H&Esections were available, of which 15 contained a malignant areawithin 2 mm from the resection surface. Supplementary Fig. S4shows three of these H&E sections and the corresponding HSanalysis of the resection side. Five sections contained two malig-
nant areas that corresponded to HS images taken at two differentresection sides. Of the 20malignant areas, 10 were IC (distance toresection surface: 0–1 mm) and 10 were DCIS (distance toresection surface: 0–1.5 mm). HS analysis confirmed all tumor-positive margins found on the available H&E sections, except forone IC spot that was smaller than 1 mm2. Further studies areneeded to evaluate the classification performance of resectionmargin assessment with HS imaging.
DiscussionTumor-positive resection margins are common after surgical
procedures for many types of cancer (1). Residual tumor cells atthe resection edgemay increase the chance of local recurrence andmay affect the ultimate patient outcome. Therefore, a techniquefor real-time intraoperative margin assessment is clearly needed.To comply with clinical needs during this type of surgery, asuccessful intraoperative margin assessment technique should beable to assess the entire resection surface almost real-time withhigh diagnostic performance, up to the required tumor-freemargin width (36). In this study, we used HS imaging for tumordetection after breast-conserving surgery. We report on a highdiagnostic performance of HS imaging on breast tissue slices andfast data acquisition and analysis of the entire resection surface oflumpectomy specimens. This approach couldmake near real-timeassessment of tumormargins during surgery feasible in the future.
We trained and evaluated the diagnostic performance on freshbreast slices so that HS images were well correlated with histo-pathology. We defined four tissue classes by distinguishing tissueclasses within the malignant and healthy classes. Specifically,within the malignant class, we made a distinction between ICand DCIS. Within the healthy class, we distinguished connectivetissue (which included benign glandular tissue) and adiposetissue. Clinically, differentiating these two healthy classes is notrelevant. However, due to their large spectral differences, thisimproved the classification algorithm. Both adipose tissue and ICwere detected as either healthy or tumorous tissue types with highaccuracies. More challenging was the differentiation betweenDCIS and connective tissue. Because IC is generally preceded byDCIS, which arises in benign glandular ducts embedded inconnective tissue, we would expect DCIS to be optically the mostsimilar to connective tissue. Nevertheless, DCIS and connectivetissuewere classified as tumor andhealthy tissue in 84%and70%,respectively. In this study, individual spectra were classified with-out taking into account their surroundings. Thereby, 30% of theconnective spectra were incorrectly classified as malignant. How-ever, when these connective spectra are located near or in a tumor,misclassifying them as malignant tissue would be clinically lessrelevant. In Fig. 4, we showed that classification inaccuracies aremost likely to occur around tissue transitions. This can beexplained by a difference in tissue information provided by thegold standard, theH&E sections, and the tissuemeasuredwith theHS camera. Based on diffusion theory, we image a volume up to afew millimeters in the tissue with our camera (37). However, theH&E sections reflect just a superficial portion of a few cell layers ofthe measured surface. As a result, HS data can be derived from amixture of different tissue classes instead of the single tissue classgiven by the superficial layer of histopathology. Because ourdeveloped classification algorithm classifies each spectrum intoone of the tissue classes, classification inaccuracies will be higherwhen HS imaging measures a mixture of tissue classes. This is
Figure 4.
Relation between classification accuracy and pocket size. A, Representativeexample of the histopathology annotation of one of the tissue slices thatcontains both IC and adipose tissue. For each pixel in the tissue slice, theshortest distance to the IC–adipose tissue transition is calculated. The scalebar indicates 4 mm. B, The graph shows the HS classification accuracy ofpixels in the white rectangle, which decreases toward the tissue transition.C, The relation between the classification accuracy and the smallest pocketsize in which a pixel was located for all pixels in the dataset per tissue class.
Hyperspectral Imaging for Resection Margin Assessment
www.aacrjournals.org Clin Cancer Res; 25(12) June 15, 2019 3577
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089

more likely in small tissue pockets (like DCIS and connectivetissue), or in tissue close to tissue transitions.
Nevertheless, pixels in tissue pockets larger than 2� 2mmwerecorrectly classified in more than 93%. Whether this is clinicallysufficient depends on the used definition of a positive resectionmargin. Over the last years, breast cancer guidelines have beenprogressing toward a more liberal attitude. For IC, the tumor-free
margin width changed from 2 mm to no tumor on the resectionedge, and for DCIS, a tumor-free margin width of 2 mm is nowaccepted (36). Even thoughwe can detect tumors larger than 2� 2mmat the resection surfacewith our currentHS setup,HS imaginghas the potential to detect even smaller pockets by sampling asmaller volume. This can be achieved by, for example, using amethod described by Jacques and colleagues (38) that uses
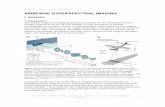
Figure 5.
Representative example of HS analysis on resection surface. BothWL (A) and HS images were taken from six sides so that the entire resection surface wasimaged. B, Classification result of the HS images using the SVM algorithm, developed with the tissue slices. The specimen was sliced according to standardpathology protocol, and 6 H&E sections were processed for further analysis. C, The orientation of these sections with respect to the 3D representation of the HSclassified specimen. H&E sections 1 and 6 were taken parallel to the resection surface and hence do not provide information on the margin width. Therefore,these sections were excluded from analysis. D, In H&E sections 2 to 5, an experienced pathologist annotated the tumor so that the resection margin widthcould be assessed.
Kho et al.
Clin Cancer Res; 25(12) June 15, 2019 Clinical Cancer Research3578
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089

polarization, or by developing classification algorithms usingselected wavelengths at which the penetration depth of light isonly superficial. Whether this is indeed necessary should beinvestigated in a larger prospective study of HS imaging onresection specimens.
In this study, we classified HS data with a linear, weighted SVMalgorithm. The usefulness of SVM for classifying HS data has beenreported by previous studies in other research areas as well (39).On the lumpectomy specimens, we showed that HS data could beanalyzed fast, without the need for an experienced operator. Toevaluate the amount of time required to image the entire resectionsurface, we imaged the lumpectomy specimens by taking siximages. However, a limiting factor in this approach was thecorrelation of HS analysis with histopathology due to the limitedavailable histopathologic information. Unlike HS imaging, resec-tion margin assessment with H&E sections covered only a smallfraction of the entire resection surface (Fig. 5C). Therefore, wewere not able to verify thewholemeasured surface, aswe could dowith the tissue slices dataset. In addition, the location of the H&Esections on the resection surface could not be precisely retrieved.We realize this is a limitation because this prevented us fromobtaining a classification accuracy of HS imaging on analyzingresectionmargins. As a result, the classification performance ofHSimaging on breast tissue was only calculated using the tissue slicesdataset. Nevertheless, in the lumpectomy dataset, HS analysisconfirmed 19 of 20 malignancies found within 2 mm of theresection surface on the available H&E sections. One IC spotsmaller than 1 mm2 was missed, which is in accordance with thedecrease in classification accuracy when tissue pockets get smaller(Fig. 4). In this study, we focused on detecting all malignancieswithin 2 mm of the resection surface, without differentiating ICandDCIS. In addition, we were not able to confirmHS analysis oftumor-negativemarginswithhistopathologic information. For anevaluation of the clinical sensitivity of HS imaging, a differenceshould be made between IC and DCIS in the resection margin.This, along with the specificity of HS imaging, needs to be furtherexplored in a clinical study that evaluates the benefit of HSimaging in routine breast-conserving surgery. By analyzing HSimages immediately after imaging, locations that are suspected tobe tumor positive as well as tumor-negative areas can be markedand retrieved after histopathologic processing. Thereby, a directcorrelation with histopathology can be obtained and the classi-fication performance of HS imaging for resection margin assess-ment can be evaluated.
With the classification algorithm developed in this study, ICand DCIS spectra from the tissue slices were classified with anaccuracy of 93% and 84%. This accuracy is much higher than canbe achieved with currently available imaging techniques formargin assessment such as ultrasound and specimen radiography,on which DCIS often remains invisible (10). In contrast, ourresults resemble pathologic margin detection techniques likefrozen section analysis (accuracy of 84%–98%; ref. 10) andtouch preparation cytology (accuracy of 78%–99%; ref. 10). HSimaging, however, has the advantage over these techniques that itcan scan an entire resection surface in a short amount of time. Weimaged lumpectomy specimens in a similar setup as the intendedfinal application in the clinical workflow. In this specific setting,each resection side was imaged in less than 20 seconds and couldbe analyzed in 40 seconds. Repositioning of the specimen toimage the next side required most of the time. Acquisition and
analysis time, however, could still significantly be improved byfurther development of the hardware and optimization of theclassification algorithm. Currently, we analyzed the whole resec-tion margin after surgery without providing feedback. Whenresection sides would be analyzed immediately after imaging,during repositioning of the specimen,HS analysis would bemuchfaster. In this way, it can easily outperform frozen section analysisand touch preparation cytology that require at least 15 to 30minutes (11). In addition, HS imaging can be performed in theoperating theatre, which could allow near real-time diagnosticfeedback of the resected specimen to the surgeon in the future.This would make a re-excision of a tumor-positive margin duringthe initial operation possible.
In summary, we showed the potential of HS imaging forintraoperative margin assessment by reporting on its first use inhuman breast tissue. The diagnostic performance of HS imagingon sliced breast specimen was high, and imaging of the entireresection surface was much faster in comparison with currentlyavailable margin assessment techniques. In addition, HS imagingin combination with SVM allowed for automated classification ofthe data, without the need for an experienced operator. Thesefindings support that HS imaging can become a powerful clinicaltool for real-time margin assessment during breast-conservingsurgery.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: E. Kho, L.L. de Boer, M.-J.T.F.D. Vrancken Peeters,H.J.C.M. Sterenborg, T.J.M. RuersDevelopment ofmethodology: E. Kho, K.K. Van de Vijver, H.J.C.M. Sterenborg,T.J.M. RuersAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): E. Kho, L.L. de Boer, F. van DuijnhovenAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): E. Kho, L.L. de Boer, K.K. Van de Vijver,H.J.C.M. Sterenborg, T.J.M. RuersWriting, review, and/or revision of the manuscript: E. Kho, L.L. de Boer,K.K. Van de Vijver, F. van Duijnhoven, M.-J.T.F.D. Vrancken Peeters,H.J.C.M. Sterenborg, T.J.M. RuersAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): E. Kho, K.K. Van de VijverStudy supervision: K.K. Van de Vijver, M.-J.T.F.D. Vrancken Peeters,H.J.C.M. Sterenborg, T.J.M. Ruers
AcknowledgmentsThe authors thank K. J�o�zwiak for help with statistical analyses, B. Dashtbo-
zorg andA.L. Post for attentive readingof the article, G.C. Langhout for graphicalassistance, and The Netherlands Cancer Institute/Antoni van Leeuwenhoek(NKI-AVL) Core Facility Molecular Pathology & Biobanking (CFMPB) forsupplying NKI-AVL biobank material. The authors also thank all surgeons andnurses from the Department of Surgery and all pathologists and pathologistassistants from the Department of Pathology for their assistance in collectingspecimens.
This work was partly supported by the Dutch Cancer Society (grant KWF10747).
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received July 4, 2018; revised October 24, 2018; accepted March 12, 2019;published first March 18, 2019.
Hyperspectral Imaging for Resection Margin Assessment
www.aacrjournals.org Clin Cancer Res; 25(12) June 15, 2019 3579
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089

References1. Orosco RK, Tapia VJ, Califano JA, Clary B, Cohen EE, Kane C, et al. Positive
surgical margins in the 10 most common solid cancers. Sci Rep 2018;8:5686.
2. Alrahbi S, Chan PM, Ho BC, Seah MD, Chen JJ, Tan EY. Extent of margininvolvement, lymphovascular invasion, and extensive intraductal compo-nent predict for residual disease after wide local excision for breast cancer.Clin Breast Cancer 2015;15:219–26.
3. Merrill AL, Coopey SB, Tang R, McEvoy MP, Specht MC, Hughes KS, et al.Implications of new lumpectomy margin guidelines for breast-conservingsurgery: changes in reexcision rates and predicted rates of residual tumor.Ann Surg Oncol 2016;23:729–34.
4. Merrill AL, Tang R, Plichta JK, Rai U, Coopey SB, McEvoy MP, et al. Shouldnew "no ink on tumor" lumpectomy margin guidelines be applied toductal carcinoma in situ (dcis)? A retrospective review using shaved cavitymargins. Ann Surg Oncol 2016;23:3453–8.
5. Langhans L, JensenM-B, TalmanM-LM, Vejborg I, KromanN, Tvedskov TF.Reoperation rates in ductal carcinoma in situ vs invasive breast cancer afterwire-guided breast-conserving surgery. JAMA Surg 2017;152:378–84.
6. Stewart BW, Wild CP. World cancer report 2014. Lyon: IARC Press; 2014.7. Munshi A, Kakkar S, Bhutani R, Jalali R, Budrukkar A, Dinshaw K. Factors
influencing cosmetic outcome in breast conservation. ClinicalOncol 2009;21:285–93.
8. Pleijhuis RG, Graafland M, de Vries J, Bart J, de Jong JS, van Dam GM.Obtaining adequate surgical margins in breast-conserving therapy forpatients with early-stage breast cancer: current modalities and futuredirections. Ann Surg Oncol 2009;16:2717–30.
9. Keating JJ, Fisher C, Batiste R, Singhal S. Advances in intraoperative marginassessment for breast cancer. Curr Surg Rep 2016;4:15.
10. St John ER, Al-Khudairi R, AshrafianH, Athanasiou T, Takats Z,HadjiminasDJ, et al. Diagnostic accuracy of intraoperative techniques for marginassessment in breast cancer surgery: a meta-analysis. Ann Surg 2017;265:300–10.
11. Esbona K, Li Z, Wilke LG. Intraoperative imprint cytology and frozensection pathology for margin assessment in breast conservation surgery: asystematic review. Ann Surg Oncol 2012;19:3236–45.
12. Versteegden D, Keizer L, Schlooz-Vries M, Duijm L, Wauters C, Strobbe L.Performance characteristics of specimen radiography for margin assess-ment for ductal carcinoma in situ: a systematic review. Breast Cancer ResTreat 2017:1–11.
13. Koch M, de Jong JS, Glatz J, Symvoulidis P, Lamberts LE, Adams AL, et al.Threshold analysis and biodistribution of fluorescently labeled bevacizu-mab in human breast cancer. Cancer Res 2017;77:623–31.
14. Tummers QRJG, Hoogstins CES, Gaarenstroom KN, de Kroon CD, vanPoelgeest MIE, Vuyk J, et al. Intraoperative imaging of folate receptor alphapositive ovarian and breast cancer using the tumor specific agent EC17.Oncotarget 2016;7:32144–55.
15. Nguyen FT, Zysk AM, Chaney EJ, Kotynek JG, Oliphant UJ, Bellafiore FJ,et al. Intraoperative evaluation of breast tumor margins with opticalcoherence tomography. Cancer Res 2009;69:8790–6.
16. Allen WM, Chin L, Wijesinghe P, Kirk RW, Latham B, Sampson DD, et al.Wide-field optical coherence micro-elastography for intraoperative assess-ment of human breast cancer margins. Biomed Opt Express 2016;7:4139–53.
17. Li R, Wang P, Lan L, Lloyd FP, Goergen CJ, Chen S, et al. Assessing breasttumor margin by multispectral photoacoustic tomography. Biomed OptExpress 2015;6:1273–81.
18. Haka AS, Volynskaya Z, Gardecki JA, Nazemi J, Lyons J, Hicks D, et al. Invivo margin assessment during partial mastectomy breast surgery usingRaman spectroscopy. Cancer Res 2006;66:3317–22.
19. KellerMD,Vargis E, deMatosGranjaN,WilsonRH,MycekM-A, KelleyMC,et al. Development of a spatially offset Raman spectroscopy probe forbreast tumor surgical margin evaluation. J Biomed Opt 2011;16:077006.
20. LaughneyAM,KrishnaswamyV, Rizzo EJ, SchwabMC, BarthRJ, Pogue BW,et al. Scatter spectroscopic imaging distinguishes between breast pathol-
ogies in tissues relevant to surgical margin assessment. Clin Cancer Res2012;18:6315–25.
21. Bigio IJ, Bown SG, Briggs G, Kelley C, Lakhani S, Pickard D, et al. Diagnosisof breast cancer using elastic-scattering spectroscopy: preliminary clinicalresults. J Biomed Opt 2000;5:221–8.
22. de Boer LL, Hendriks BHW, van Duijnhoven F, Vrancken Peeters-BaasMJTFD, VandeVijver KK, LooCE, et al. UsingDRSduring breast conservingsurgery: identifying robust optical parameters and dealing with inter-patient variation. Biomed Opt Express 2016;7:5188–200.
23. Nachab�e R, Evers DJ, Hendriks BH, Lucassen GW, van der Voort M, RutgersEJ, et al. Diagnosis of breast cancer using diffuse optical spectroscopy from500 to 1600 nm: comparison of classification methods. J Biomed Opt2011;16:087010.
24. Volynskaya Z, Haka AS, Bechtel KL, Fitzmaurice M, Shenk R, Wang N,et al. Diagnosing breast cancer using diffuse reflectance spectroscopyand intrinsic fluorescence spectroscopy. J Biomed Opt 2008;13:024012.
25. ZhuC, PalmerGM,Breslin TM,Harter J, RamanujamN.Diagnosis of breastcancer using fluorescence and diffuse reflectance spectroscopy: a Monte-Carlo-model-based approach. J Biomed Opt 2008;13:034015.
26. Lu G, Fei B. Medical hyperspectral imaging: a review. J Biomed Opt 2014;19:010901.
27. de Boer LL, Molenkamp B, Bydlon TM, Hendriks BHW, Wesseling J,Sterenborg HJ, et al. Fat/water ratios measured with diffuse reflectancespectroscopy to detect breast tumor boundaries. Breast Cancer Res Treat2015;152:509–18.
28. Taroni P, Paganoni AM, Ieva F, Pifferi A, Quarto G, Abbate F, et al.Non-invasive optical estimate of tissue composition to differentiatemalignant from benign breast lesions: a pilot study. Sci Rep 2017;7:40683.
29. Morrow M, Zee KJV, Solin LJ, Houssami N, Chavez-MacGregor M,Harris JR, et al. Society of Surgical Oncology–American Society forRadiation Oncology–American Society of Clinical Oncology consen-sus guideline on margins for breast-conserving surgery with whole-breast irradiation in ductal carcinoma in situ. J Clin Oncol 2016;34:4040–6.
30. Barnes R, Dhanoa MS, Lister SJ. Standard normal variate transformationand de-trending of near-infrared diffuse reflectance spectra. Appl Spectrosc1989;43:772–7.
31. Vidal M, Amigo JM.Pre-processing of hyperspectral images. Essential stepsbefore image analysis. Chemometr Intell Lab 2012;117:138–48.
32. Burger J, Geladi P. Hyperspectral NIR image regression part II: datasetpreprocessing diagnostics. J Chemometr 2006;20:106–19.
33. Vapnik VN. The nature of statistical learning theory. New York: SpringerScience & Business Media; 2013.
34. Hsu C-W, Lin C-J.A comparison of methods for multiclass support vectormachines. IEEE Transact Neural Net 2002;13:415–25.
35. Huang Y, Du S. Weighted support vector machine for classificationwith uneven training class sizes [abstract]. In: Proceedings of the2005 International Conference on Machine Learning and Cybernetics;2005 Aug 18–21; Guangzhou, China. Piscataway (NJ): IEEE; 2005.p. 4365–9.
36. Brouwer de Koning SG, Vrancken Peeters MTFD, J�o�zwiak K, Bhairosing PA,Ruers TJM. Tumor resection margin guidelines in breast cancer – a sys-tematic review and meta-analysis of current literature. Clin Breast Cancer2018;18:595–600.
37. Flock ST, Patterson MS, Wilson BC, Wyman DR. Monte Carlo modeling oflight propagation in highly scattering tissues. I. Model predictions andcomparison with diffusion theory. IEEE Trans Biomed Eng 1989;36:1162–8.
38. Jacques SL, Ramella-Roman JC, Lee K. Imaging skin pathology withpolarized light. J Biomed Opt 2002;7:329–40.
39. Mountrakis G, Im J, Ogole C. Support vectormachines in remote sensing: areview. ISPRS J Photogramm 2011;66:247–59.
Clin Cancer Res; 25(12) June 15, 2019 Clinical Cancer Research3580
Kho et al.
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089

2019;25:3572-3580. Published OnlineFirst March 18, 2019.Clin Cancer Res Esther Kho, Lisanne L. de Boer, Koen K. Van de Vijver, et al. Cancer SurgeryHyperspectral Imaging for Resection Margin Assessment during
Updated version
10.1158/1078-0432.CCR-18-2089doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2019/03/16/1078-0432.CCR-18-2089.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/25/12/3572.full#ref-list-1
This article cites 35 articles, 4 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/25/12/3572.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/25/12/3572To request permission to re-use all or part of this article, use this link
on August 27, 2020. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 18, 2019; DOI: 10.1158/1078-0432.CCR-18-2089