Hyperglycemia in inpatients: a call for intensive care Individualizing therapy for optimal results.
26
in inpatients: a call for intensive care Individualizing therapy for optimal results
-
Upload
deborah-riley -
Category
Documents
-
view
221 -
download
2
Transcript of Hyperglycemia in inpatients: a call for intensive care Individualizing therapy for optimal results.

Hyperglycemia in inpatients: a call for
intensive careIndividualizing therapy for optimal
results

Hyperglycemia-scope of the problem 5.7 million hosp annually, At least 1/4 have diabetes,
unknown more have hospital related hyperglycemia Diabetes now 8% of the population. 20 million! Hyperglycemia
common in acute illness (50% of ACS patients). Patients not known to be diabetic are hyperglycemic in
hospital undiagnosed, insulin-resistant population, hyperglycemia secondary to illness
Cost of inpatient diabetes care-$40 Bln DM pts $13,243 vs. $ 2,560 non-diabetics per admission“The most expensive chronic illness in the US”
Source: American Association of Endocrinologists

An evolving recognition of importance of glucose control.
Historically not an issue, no evidence for improved outcomes, even 1995 study no short term benefit.
Hyperglycemia expected, even good? “Stress hyperglycemia” 1997- Higher CABG wound infection rates with hyperglycemia 1999- Increased mortality and LOS in CABG patients with
hyperglycemia 2000- CVA; 2001: SICU; 2006: MICU 2003- AACE recommendations of hyperglycemia 2005- ADA guidelines 2006- AACE + ADA

The dangers of hyperglycemia Patients with AMI, elevated glucose correlates with increased
mortality and infarct size. Correlates with CHF 1
CVA patients: elevated glucose assoc with increased mortality 2
Increasing blood glucose concentrations are associated with adverse clinical outcomes in patients with AECOPD 3
Hyperglycemia on admission is independently associated with adverse outcomes in patients with CAP 4
Increased risk of wound infection post-CABG 5
1. Inpatient diabetes and glycemic control: A call to action. AACE, 20062. Parsons MW, et al. Acute hyperglycemia adversely affects stroke outcome: a magnetic resonance imaging and
spectroscopy study. Ann Neurol 2002;52:20-8.3. E H Baker, et al. Hyperglycaemia is associated with poor outcomes in patients admitted to hospital with acute
exacerbations of chronic obstructive pulmonary disease Thorax, April 1, 2006; 61(4): 284 - 289. 4. F. A. McAlister, et al. The Relation Between Hyperglycemia and Outcomes in 2,471 Patients Admitted to the Hospital
With Community-Acquired Pneumonia. Diabetes Care, April 1, 2005; 28(4): 810 - 815.5. SH Golden, et al. Perioperative glycemic control and the risk of infectious complications in a cohort of adults with
diabetes. Diabetes Care 22: 1408-1414.

Current regimensOral Hypoglycemics Sulfonylureas Metformin Alpha- Glycosidase
inhibitors Incretin mimetics TZDs Meglitinides Combination drugs
Insulins (IV, SQ, inhaled) Extended glargine, ultralente,
detemir Intermediate
NPH, lente Short
Regular Rapid aspart, lispro

Theory Why so common?
Counter regulatory hormones/ increased hepatic glucose prod/ reduced utilization/ decreased perfusion, FFA, cytokines?
Uncontrolled hyperglycemia causes:Infection: due to Immune dysfunction (leukocytes),
cytokines, superoxidesOrgan failure: due to Inflammation/ endothelial
damage/ neuronal damage/ increased thrombosis/ Mitochondrial dysfunction?

Definitions Diabetes: Fasting BS >126 mg/dL, random
>200 Hyperglycemia: >126 Intensive control: BS 80-110 Hypoglycemia: < 60

Normoglycemia proven benefits
2001 study NEJM, SICU patients with strict BS control 80-110
Reduced mortality by 34%Sepsis 46%Renal failure 41%Transfusion 41%Polyneuropathy 44%Van Den Berghe G, Wouters P, Weekers F, et al.
Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359-1367.

Normoglycemia proven benefits! Recent study in MICU
For patients who stayed >3 days, reduced mortality 18%, less renal dysfunction, prolonged mechanical ventilation.Patients < 3 days, increased mortality?? 1
Recent meta-analysis showed 15% decrease in mortality in a variety of settings. 2
1. Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU N Engl J Med. 2006; 354:449-61.
2. Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients:a meta-analysis of randomized, control trials. Arch Inter Med. 2004; 164:2005-2011.

Normoglycemia proven benefits DIGAMI- intensive insulin therapy 29% reduction
in mortality at 1 year. (Independent effect of insulin?)
CABG patients: Intensive therapy reduces sternal infections by 57%, 66% reduction in mortality 1
MICU patients: intensive therapy: catheter sepsis decrease 33.5%, LOS 0.25 days 2
1. Furnary AP, Zerr KJ, Grunkemeier GL, Starr A. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg 1999;67:352-62.

Normoglycemia : How to do it?Goal: physiologic mimicry OptionsOral meds ? Problems…Discontinue?
Oral+Insulins?Change to insulin for better control? SQ or IV?Sliding scale?Meal time insulins?Drip? Pumps?

Sliding scale insulin History and what’s wrong Abandoned! Retroactive not proactive Chasing our tail, esp. Type I Basal insulin Mealtimes/ eating Variation in disease state Dangers of hypoglycemia

It’s as easy as BBC FS Glucose qAC and qHS Check HbA1C
Then: BASAL: NPH/Glargine 0.2units/kg/day or drip BOLUS: Aspart/ Lispro 0.05units/kg meals CORRECTION: Both long acting and short acting

General recommendations for SQ insulin therapyTreatment goal for patient on SQ regimen is pre-prandial glucose level of 80-150
mg/dL, Insulin therapy should provide both basal and prandial insulin support when needed
Basal insulin:--Long-acting (glargine, detemir) - provides peakless insulin coverage for ~24
hours--Intermediate-acting (NPH): - Peak effect ~ 4-6 hours after administration with
about 12 hour duration of activity
Prandial and correction insulin:--Short-acting (Regular) - Peak effect ~ 2-3 hours after administration with about
6 hour duration of activity.--Rapid-acting (lispro, aspart, glulisine) - Peak effect ~ 1 hour after administration
with about 2 hour duration of activity.

Initiating SQ insulin therapy Already on Insulin * *All patients with type 1 diabetes and most patients with insulin-dependent type 2 diabetes require basal insulin, even when
NPO.
1. Estimate starting daily insulin doses:
For patients with insulin dependent diabetes
If good oral intake is expected, continue usual home insulin regimen If poor oral intake is expected or if NPO: o basal insulin: glargine, detemir at ~ 75% of home dose OR o intermediate-acting insulin: NPH at ~ 50% of home dose o short-acting insulin: hold rapid-acting (lispro, aspart, glulisine) and replace with Regular insulin sliding scale.

Considerations
Lower dose Higher dose
No previous DM Elevated HbA1C
Glucose sl elevated Glucose high
Poor PO good to excessive PO
Impaired renal function Metabolic stress
Corticosteroids
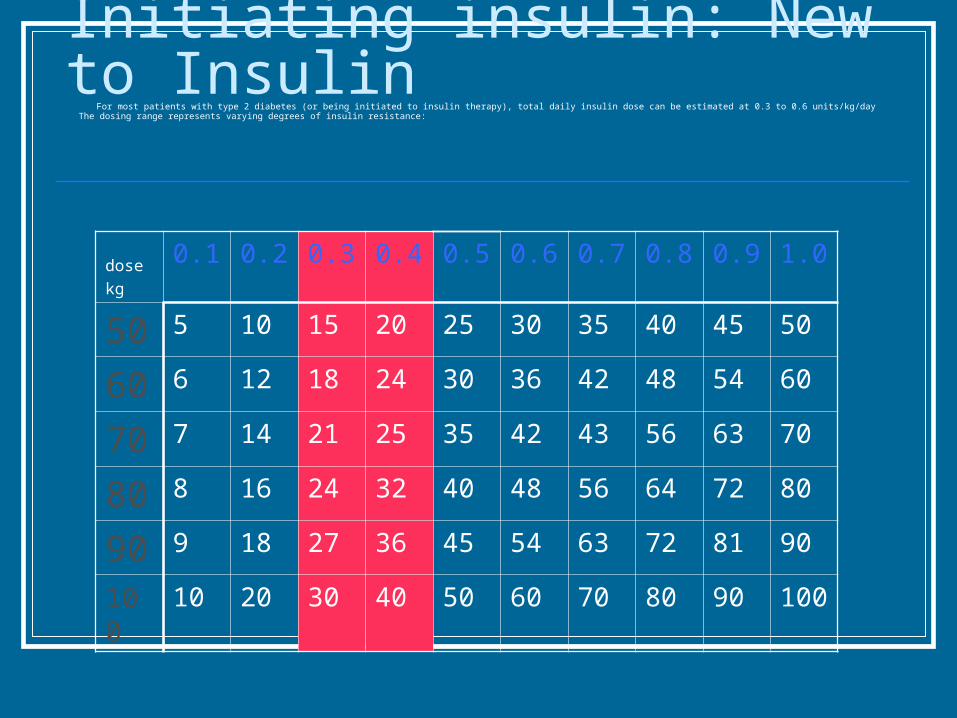
Initiating insulin: New to Insulin For most patients with type 2 diabetes (or being initiated to insulin therapy), total daily insulin dose can be estimated at 0.3 to 0.6 units/kg/day
The dosing range represents varying degrees of insulin resistance:
dose
kg
0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
50 5 10 15 20 25 30 35 40 45 50
60 6 12 18 24 30 36 42 48 54 60
70 7 14 21 25 35 42 43 56 63 70
80 8 16 24 32 40 48 56 64 72 80
90 9 18 27 36 45 54 63 72 81 90
100 10 20 30 40 50 60 70 80 90 100

2. Estimate scheduled doses.Glargine insulin - about 50% of total daily doseLispro insulin - about 50% of total daily dose
divided into the 3 meals Example: For an 80 kg patient who is new to insulin -
- glargine insulin 12 units SQ at hs - lispro insulin 4 units SQ before each meal
(hold if NPO or intake poor)
NPH insulin - about 44% of total daily dose before breakfast meal, and about 17% of total daily dose at hs
Regular insulin - about 22% of total daily dose before breakfast meal, and about 17% of total daily dose before supper meal
Example: For an 80 kg patient who is new to insulin - - NPH insulin 11 units SQ before breakfast
and 4 units SQ at hs - Regular insulin 5 units SQ before breakfast
and 4 units SQ before supper meal
Initiating SQ insulin therapy

3. Add correction insulin doses as desired
Monitoring of glucose levels and titration of insulin doses at least daily a. If blood glucose levels are consistently too high/low, the total daily insulin dose can be adjusted by shifting to a column to the right/left on the total daily dose table above
b. Insulin doses are adjusted based on subsequent glucose levels: i. glargine and evening NPH insulin doses based on glucose levels at 0200 and before breakfast ii. mealtime insulin doses based on glucose levels before the next
meal and at hs c. RN may administer as little as 50% of SCHEDULED insulin dose if: i. Patient has had change to NPO status and blood glucose is < 150 mg/dL. ii. Patient has had decline in PO intake to less than 33% from previous and blood glucose is < 150 mg/dL.
Initiating SQ insulin therapy

Insulin dripIndication for intravenous insulin infusion among nonpregnant adults
with established diabetes or hyperglycemia
Diabetic ketoacidosis and nonketotic hyperosmolar state A General preoperative, intraoperative, and postoperative care C
Postoperative period following heart surgery B Organ transplantation E MI or cardiogenic shock A Stroke E Exacerbated hyperglycemia during high-dose steroid therapy
E NPO status in type 1 diabetes E Critically ill surgical patient requiring mechanical ventilation A
Dose-finding strategy, anticipatory to initiation or reinitiating of subcutaneous insulin therapy in type 1 or type 2 diabetes C

Insulin dripAdvantages
Tightest control Good absorption Rapid adjustments Easy standardized
Disadvantages Frequent monitoring
(ICU/IMCU needed?)
Nursing time! Catheter complications Problems when switching
to SQ regimen Rapid Glucose shifts?

What about hypoglycemia ?BG level ≤40 mg/dL was 5.2% in intensive insulin-treated
patients versus 0.8% in conventionally treated patients.1
But… In a national survey, Cohen et al. found that 11% of serious medication errors resulted from insulin misadministration.2
Need for frequent monitoring Need for separate protocol, oral and IV D50 administration.
Prevents “overshooting”1. van den Berghe G, Wouters PJ, Bouillon R, Weekers F, Verwaest C, Schetz M, et al. Outcome
benefit of intensive insulin therapy in the critically ill: insulin dose versus glycemic control. Crit Care Med 2003;31:359-66.
2. Cohen MR, Proulx SM, Crawford SY. Survey of hospital system and common serious medication errors. J Healthc Risk Manag 1998;18:16-27.

Logistics Multidisciplinary steering committee Standardized order sets Glycemic management team. Monitoring results. Hypoglycemic protocol Nutrition Diabetes education

Cost vs. benefits Each increased 50 mg/dL of blood glucose
added 0.76 LOS in diabetic CABG patients.1
Use of diabetes team 56% reduction LOS $2353/patient.2
Intensive therapy in SICU saves $40K/year.Furnary AP, et al. Postoperative hyperglycemia prolongs length of stay in hospitalized
patients with diabetic CABG patients. Circulation. 2000; 102 (18) II-556.Koproski J et al. Effects of an intervention by a diabetes team in hospitalized patients
with diabetes. Diabetes Care. 1997; 20:1553-1555.

Barriers Fear of hypoglycemia Nursing time, data collection. Lack of standardization Changing insulin requirements Skepticism to benefits of good control. Multiple transfers of patients.

Further research Refinement of protocols Impact of hyperglycemia in development of
DM Non critically ill patients: goals? Continuous monitoring (pulse ox of the
future) Role of feedings