Hydraulic sinus lift technique: description of a clinical case maxillary sinus through a crestal ......
4
Case report Page 1 of 4 Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY) For citation purposes: Andreasi Bassi M, Lopez MA, Confalone L, Fanali S, Carinci F. Hydraulic sinus lift technique: description of a clinical case. Annals of Oral & Maxillofacial Surgery 2013 Jun 01;1(2):18. Compeng interests: none declared. Conflict of interests: none declared. All authors contributed to the concepon, design, and preparaon of the manuscript, as well as read and approved the final manuscript. All authors abide by the Associaon for Medical Ethics (AME) ethical rules of disclosure. Hydraulic sinus lift technique: description of a clinical case M Andreasi Bassi 1 *, MA Lopez 1 , L Confalone 1 , S Fanali 2 , F Carinci 3 approach, for implant purposes, today are widely used in ambula- tory clinical practice, for managing bone atrophy of the lateral–posterior sectors of the upper maxillary 1–4 . Their indication has progressively increased over the years also due to their lower morbidity compared with the techniques with a lateral approach 5–7 . The fracture or wear of the cortical sinus floor and the later displacement of the sinus membrane constitutes the crucial phases of all the crestal lifting techniques 1,8 not supported by direct visual monitoring. Detachment of the Schneiderian membrane can be performed directly with manual instruments 9 or indi- rectly through the graft material, most techniques use the latter 1,10–12 . The reason is found in the fact that the graft material is usually perme- ated with blood that, being a liq- uid, is not compressible. In 1994, Summers 10 stated that the pressure, exercised by the compactors on the graft material mixed with the blood, forced the indirect hydraulic detach- ment of the maxillary sinus mucosa 12 . Conversely it should be noted that the force transmitted by the compac- tors on graft material is not easily controlled to the point of sometimes being detrimental to the integrity of the sinus membrane 9 . Some authors have recently pro- posed crestal lifting techniques that use hydraulic pressure for the dis- placement of the sinus membrane with alternative methodologies to those currently in use 13,14 . The pro- posed methods provide a prelimi- nary detachment of the Schneiderian membrane through injection of a liquid followed by its spontaneous expulsion or aspiration, to then pass on at the insertion of the graft mate- rial in the sub-schneiderian space cre- ated this way. These methods, while effective, involve a prolongation of the operating procedure since it is con- ceptually simpler to use a graft mate- rial in a liquid state that when injected hydraulically raises the mucosa and fills the sub-schneiderian space at once. Furthermore, the method described above used conventional single-use syringes in which it is not possible to finely check on the pro- gression of the piston since this is connected with individual sensitivity. Other authors also have proposed, in the past, direct injection of fluid graft materials in the sub-antral space but always through conventional single- use syringes activated manually 15 . In 2010, Andreasi Bassi and Lopez 16 proposed a new method that takes advantage of the hydraulic pressure exercised on a graft material of a pasty consistency to detach the antral mucosa and simultaneously fill the sub-antral space created this way. The authors called the technique Hydraulic Sinus Lift (HySiLift) 16 . The instruments made for this pur- pose consist of three components: a titanium syringe (Hydromab, FMD, Rome, Italy) (Figure 1) equipped with a micrometric control piston on which it is possible to assemble single-use plastic syringes of various volumes, possibly equipped with a Luer-lock attachment; a dispenser in threaded surgical steel (ML Injec- tor, FMD, Rome, Italy) available in two forms (conical and cylindrical) and four measurements (two cylindrical of ø 3.2 and 4.0 mm and two conical of ø 2.8–4.0 and 3.5–4.6 mm) and a needle in surgical steel, also equipped Abstract Introduction In this work the authors describe a new method, indicating in the max- illary sinus lifting through a crestal approach, characterised by the hydraulic detachment of the mucosa and simultaneous filling of the sub- schneiderian space, with a graft material of a pasty consistency. Case report In a 56-year-old non-smoking patient, edentulous in area 1.6 (Figure 2), pre- sented to our observation for the need to reintegrate the missing element, we planned the implant placement and the later completion with an implant- supported metal-ceramic crown. The endoral x-ray exam of the edentulous site showed a reduced thickness of the residual bone which was confirmed by the Denta Scan CT exam (Figure 3.1); it was decided to make, along with the implant positioning, the maxillary sinus floor lifting, through the hydrau- lic sinus lift technique. Conclusion The hydraulic sinus lift technique allows the hydraulic detachment of the maxillary sinus mucosa and, at the same time, the filling of the sub-schneiderian space with the graft material. Introduction The techniques for lifting the floor of the maxillary sinus through a crestal *Corresponding author Email: [email protected] 1 Via Lucio Elio Seiano, 15, 00174-Rome, Italy 2 Dental Clinic, University of Chieti, Chieti, Italy 3 Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara, Italy Emerging Technologies
Transcript of Hydraulic sinus lift technique: description of a clinical case maxillary sinus through a crestal ......

Case report
Page 1 of 4
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Andreasi Bassi M, Lopez MA, Confalone L, Fanali S, Carinci F. Hydraulic sinus lift technique: description of a clinical case. Annals of Oral & Maxillofacial Surgery 2013 Jun 01;1(2):18.
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Hydraulic sinus lift technique: description of a clinical case
M Andreasi Bassi1*, MA Lopez1, L Confalone1, S Fanali2, F Carinci3
approach, for implant purposes, today are widely used in ambula-tory clinical practice, for managing bone atrophy of the lateral– posterior sectors of the upper maxillary1–4. Their indication has progressively increased over the years also due to their lower morbidity compared with the techniques with a lateral approach5–7.
The fracture or wear of the cortical sinus floor and the later displacement of the sinus membrane constitutes the crucial phases of all the crestal lifting techniques1,8 not supported by direct visual monitoring.
Detachment of the Schneiderian membrane can be performed directly with manual instruments9 or indi-rectly through the graft material, most techniques use the latter1,10–12. The reason is found in the fact that the graft material is usually perme-ated with blood that, being a liq-uid, is not compressible. In 1994, Summers10 stated that the pressure, exercised by the compactors on the graft material mixed with the blood, forced the indirect hydraulic detach-ment of the maxillary sinus mucosa12. Conversely it should be noted that the force transmitted by the compac-tors on graft material is not easily controlled to the point of sometimes being detrimental to the integrity of the sinus membrane9.
Some authors have recently pro-posed crestal lifting techniques that use hydraulic pressure for the dis-placement of the sinus membrane with alternative methodologies to those currently in use13,14. The pro-posed methods provide a prelimi-nary detachment of the Schneiderian membrane through injection of a liquid followed by its spontaneous
expulsion or aspiration, to then pass on at the insertion of the graft mate-rial in the sub-schneiderian space cre-ated this way. These methods, while effective, involve a prolongation of the operating procedure since it is con-ceptually simpler to use a graft mate-rial in a liquid state that when injected hydraulically raises the mucosa and fills the sub- schneiderian space at once. Furthermore, the method described above used conventional single-use syringes in which it is not possible to finely check on the pro-gression of the piston since this is connected with individual sensitivity. Other authors also have proposed, in the past, direct injection of fluid graft materials in the sub-antral space but always through conventional single-use syringes activated manually15.
In 2010, Andreasi Bassi and Lopez16 proposed a new method that takes advantage of the hydraulic pressure exercised on a graft material of a pasty consistency to detach the antral mucosa and simultaneously fill the sub-antral space created this way. The authors called the technique Hydraulic Sinus Lift (HySiLift)16. The instruments made for this pur-pose consist of three components: a titanium syringe (Hydromab, FMD, Rome, Italy) ( Figure 1) equipped with a micrometric control piston on which it is possible to assemble single-use plastic syringes of various volumes, possibly equipped with a Luer-lock attachment; a dispenser in threaded surgical steel (ML Injec-tor, FMD, Rome, Italy) available in two forms (conical and cylindrical) and four measurements (two cylindrical of ø 3.2 and 4.0 mm and two conical of ø 2.8–4.0 and 3.5–4.6 mm) and a needle in surgical steel, also equipped
AbstractIntroductionIn this work the authors describe a new method, indicating in the max-illary sinus lifting through a crestal approach, characterised by the hydraulic detachment of the mucosa and simultaneous filling of the sub-schneiderian space, with a graft material of a pasty consistency.Case reportIn a 56-year-old non-smoking patient, edentulous in area 1.6 (Figure 2), pre-sented to our observation for the need to reintegrate the missing element, we planned the implant placement and the later completion with an implant-supported metal-ceramic crown. The endoral x-ray exam of the edentulous site showed a reduced thickness of the residual bone which was confirmed by the Denta Scan CT exam (Figure 3.1); it was decided to make, along with the implant positioning, the maxillary sinus floor lifting, through the hydrau-lic sinus lift technique.ConclusionThe hydraulic sinus lift technique allows the hydraulic detachment of the maxillary sinus mucosa and, at the same time, the filling of the sub- schneiderian space with the graft material.
IntroductionThe techniques for lifting the floor of the maxillary sinus through a crestal
*Corresponding authorEmail: [email protected] Via Lucio Elio Seiano, 15, 00174-Rome, Italy2 Dental Clinic, University of Chieti, Chieti, Italy3 Department of Morphology, Surgery and
Experimental Medicine, University of Ferrara, Ferrara, Italy
Emer
ging
Tec
hnol
ogie
s

Case report
Page 2 of 4
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Andreasi Bassi M, Lopez MA, Confalone L, Fanali S, Carinci F. Hydraulic sinus lift technique: description of a clinical case. Annals of Oral & Maxillofacial Surgery 2013 Jun 01;1(2):18.
with a Luer-lock attachment, com-plementary to that of the single-use syringe, that allows connecting of the two instruments described above. The single-use syringes can be pre-loaded with a desired amount of graft material that, in our experi-ence, was represented by nanocrys-talline hydroxyapatite in an aqueous medium (Ostim, Heraeus-Kulzer, Hanau, Germany), or it is possible to directly use the syringe containing the graft material as provided by the manufacturer17–19. The semi-spherical tip of the ML Injector allows this instrument to penetrate barely 3 mm in the sub-schneiderian space without damaging the overlying mucosa while the lateral openings allow uniform distribution of the Ostim that, due to its paste-like consistency, forms a dome precisely in correspondence to the future implant site. The threaded portion of the dispenser extends for
a length of 6 mm thus making its use indicated for ridges of thickness between 3 and 6 mm to ensure suf-ficient stability of the tool during the injection manoeuvre.
The choice of the type of dispenser used is a function of the diameter and the shape of the implant that will be positioned at the end of the eleva-tion. The method cannot, however, be associated with the simultaneous insertion of the implant if the resid-ual ridge has a thickness less than 4 mm, such as not to allow its suf-ficient primary stability. In this case only the injection of the material will be performed and, after six months, after the consolidation of the graft, implant insertion will occur.
Generally the procedure takes 5 minutes to inject 1 ml of material, but in most operating situations that provide for the treatment of a single site, the volume injected is between
0.5 and 0.7 ml. The micrometric screw can be activated manually or, if desired, by contra angle hand piece geared down. In this last case, a speed of 20 rpm and a torque no greater than 45 Ncm is recommended. After com-pleting the injection, the Hydromab is disconnected from the dispenser and elevation obtained is checked through an x-ray prior to removing it. If the elevation is not considered sufficient it can be implemented by injecting other biomaterial with the same means already described.
After removing the ML Injector, if the remaining ridge has a height of more than 4 mm, the implant can be inserted and possibly should have a diameter of 0.4–0.5 mm wider than that of the dosing device used. Com-patibly, however, with the horizon-tal dimensions of the residual bony ridge the implant tunnel may, how-ever, be corrected, in the judgment of the operator, with osteotomy or with milling in order to make it more suit-able to accept the implant chosen. The aim of this report was to discuss a HySiLift technique.
Case reportIn a 56-year-old non-smoking patient, edentulous in area 1.6 ( Figure 2), presented to our observation for the need to reintegrate the missing ele-ment, we planned the implant place-ment and the later completion with an implant-supported metal-ceramic crown. The endoral x-ray exam of the edentulous site showed a reduced thickness of the residual bone which was confirmed by the Denta Scan CT
Figure 1: The Hydromab kit and the Hydromab system—biomaterial syringe, needle and ML Injector assembled.
Figure 2: Starting clinical condition.
Case report
Page 3 of 4
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Andreasi Bassi M, Lopez MA, Confalone L, Fanali S, Carinci F. Hydraulic sinus lift technique: description of a clinical case. Annals of Oral & Maxillofacial Surgery 2013 Jun 01;1(2):18.
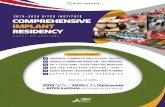
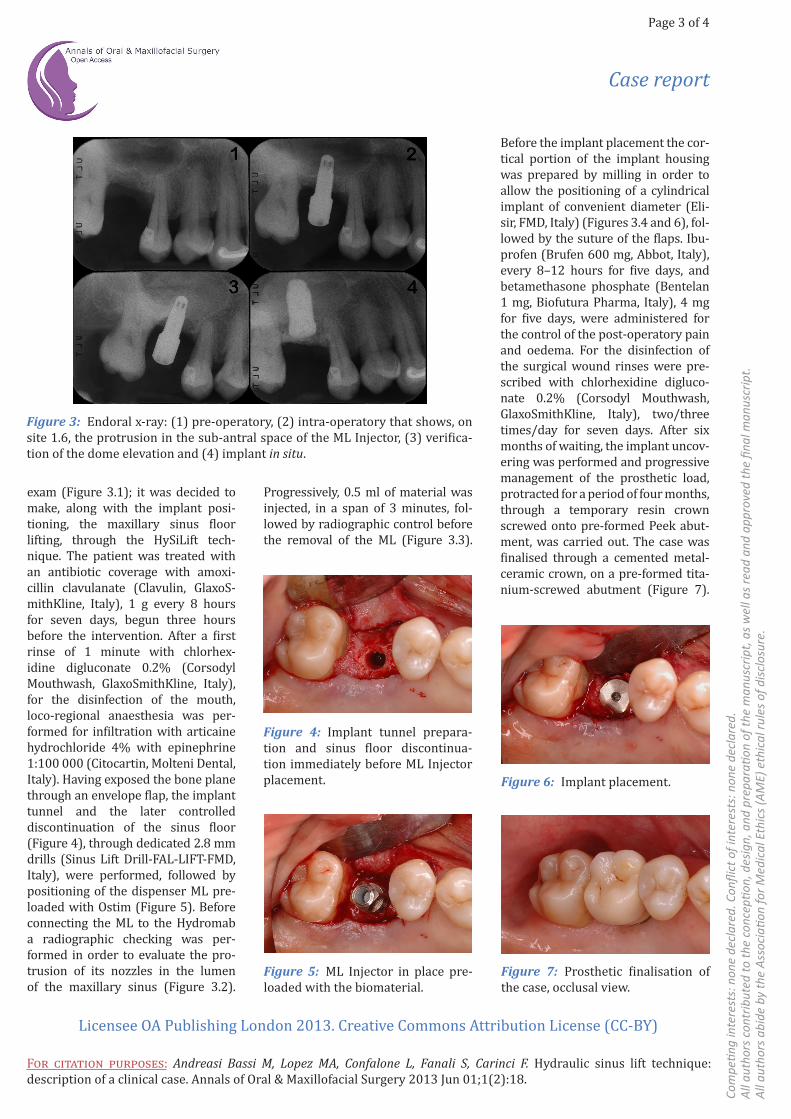
exam (Figure 3.1); it was decided to make, along with the implant posi-tioning, the maxillary sinus floor lifting, through the HySiLift tech-nique. The patient was treated with an antibiotic coverage with amoxi-cillin clavulanate (Clavulin, GlaxoS-mithKline, Italy), 1 g every 8 hours for seven days, begun three hours before the intervention. After a first rinse of 1 minute with chlorhex-idine digluconate 0.2% (Corsodyl Mouthwash, GlaxoSmithKline, Italy), for the disinfection of the mouth, loco-regional anaesthesia was per-formed for infiltration with articaine hydrochloride 4% with epinephrine 1:100 000 ( Citocartin, Molteni Dental, Italy). Having exposed the bone plane through an envelope flap, the implant tunnel and the later controlled discontinuation of the sinus floor (Figure 4), through dedicated 2.8 mm drills (Sinus Lift Drill-FAL-LIFT-FMD, Italy), were performed, followed by positioning of the dispenser ML pre-loaded with Ostim (Figure 5). Before connecting the ML to the Hydromab a radiographic checking was per-formed in order to evaluate the pro-trusion of its nozzles in the lumen of the maxillary sinus (Figure 3.2).
Before the implant placement the cor-tical portion of the implant housing was prepared by milling in order to allow the positioning of a cylindrical implant of convenient diameter (Eli-sir, FMD, Italy) ( Figures 3.4 and 6), fol-lowed by the suture of the flaps. Ibu-profen (Brufen 600 mg, Abbot, Italy), every 8–12 hours for five days, and betamethasone phosphate ( Bentelan 1 mg, Biofutura Pharma, Italy), 4 mg for five days, were administered for the control of the post-operatory pain and oedema. For the disinfection of the surgical wound rinses were pre-scribed with chlorhexidine digluco-nate 0.2% ( Corsodyl Mouthwash, GlaxoSmithKline, Italy), two/three times/day for seven days. After six months of waiting, the implant uncov-ering was performed and progressive management of the prosthetic load, protracted for a period of four months, through a temporary resin crown screwed onto pre-formed Peek abut-ment, was carried out. The case was finalised through a cemented metal-ceramic crown, on a pre-formed tita-nium-screwed abutment (Figure 7).
Figure 3: Endoral x-ray: (1) pre-operatory, (2) intra-operatory that shows, on site 1.6, the protrusion in the sub-antral space of the ML Injector, (3) verifica-tion of the dome elevation and (4) implant in situ.
Figure 4: Implant tunnel prepara-tion and sinus floor discontinua-tion immediately before ML Injector placement.
Figure 5: ML Injector in place pre-loaded with the biomaterial.
Figure 6: Implant placement.
Progressively, 0.5 ml of material was injected, in a span of 3 minutes, fol-lowed by radiographic control before the removal of the ML (Figure 3.3).
Figure 7: Prosthetic finalisation of the case, occlusal view.

Case report
Page 4 of 4
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Andreasi Bassi M, Lopez MA, Confalone L, Fanali S, Carinci F. Hydraulic sinus lift technique: description of a clinical case. Annals of Oral & Maxillofacial Surgery 2013 Jun 01;1(2):18.
A year, after prosthetic finalisation, a clinical and radiographic follow-up, of the case, was performed verifying proper condition of the soft and hard peri-implants tissues (Figure 8).
ConclusionThe HySiLift technique allows the hydraulic detachment of the maxillary sinus mucosa and, at the same time, the filling of the sub- schneiderian space with the graft material. This method, which can be used both with flap and flapless interventions, joins the most common techniques for preparation of the implant tunnel and discontinuation of the maxillary sinus floor, allowing conspicuous and harmonic increases in the three dimensions of the sub-antral space volume. The strong point of this method is researched in: a brief learn-ing curve, reduced invasiveness, reduc-tion of the operating times and greater precision, thanks to the micrometric control, on the progression of the pis-ton, that guarantees a precise and pro-gressive application of the biomaterial.
ConsentWritten informed consent was obtained from the patient for publi-cation of this case report and accom-panying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
References1. Deporter D, Todescan R, Caudry S. Simplifying management of the posterior
maxilla using short, porous-surfaced dental implants and simultaneous indi-rect sinus elevation. Int J Periodontics Restorative Dent. 2000 Oct;20:476–85.2. Fugazzotto PA. Sinus floor augmenta-tion at the time of maxillary molar extrac-tion: technique and report of preliminary results. Int J Oral Maxillofac Implants. 1999 Jul–Aug;14:536–42.3. Fugazzotto PA. The modified trephine/ osteotome sinus augmentation tech-nique: technical considerations and dis-cussion of indications. Implant Dent. 2001;10:259–64.4. Rosen PS, Summers R, Mellado JR, Salkin LM, Shanaman RH, Marks MH, et al. The bone-added osteotome sinus floor elevation technique: multicenter retro-spective report of consecutively treated patients. Int J Oral Maxillofac Implants. 1999 Nov–Dec;14(6):853–8.5. Del Fabbro M, Testori T, Francetti L, Weinstein R. Systematic review of survival rates for implants placed in the grafted maxillary sinus. Int J Peri-odontics Restorative Dent. 2004 Dec; 24(6):565–77.6. Zitzmann NU, Scharer P. Sinus eleva-tion procedures in the resorbed poste-rior maxilla. Comparison of the crestal and lateral approaches. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Jan;85(1):8–17.7. Ziccardi VB, Betts NJ. Complications of maxillary sinus augmentation. In: Jensen OT, editor. The sinus bone graft. Chicago: Quintessence Books;1999. p201–8.8. Cavicchia F, Bravi F, Petrelli G. Local-ized augmentation of the maxillary sinus floor through a coronal approach for the placement of implants. Int J Periodontics Restorative Dent. 2001 Oct;21(5):475–85.
9. Nkenke E, Schlegel A, Schultze- Mosgau S, Neukam FW, Wiltfang J. The endoscopically controlled osteotome sinus floor elevation: a preliminary prospective study. Int J Oral Maxillofac Implants. 2002 Jul–Aug;17(4):557–66.10. Summers RB. The osteotome tech-nique: Part 3—Less invasive methods of elevating the sinus floor. Compendium. 1994 Jun;15(6):698,700,702–4 passim; quiz 710.11. Summers RB. A new concept in max-illary implant surgery: the osteotome technique. Compendium. 1994 Feb; 15(2):152,154–6,158 passim; quiz 162.12. Summers RB. The osteotome tech-nique: Part 4—Future site develop-ment. Compend Contin Educ Dent. 1995 Nov;16(11):1090,1092 passim; 1094–6,1098, quiz 1099.13. Sotirakis EG, Gonshor A. Eleva-tion of the maxillary sinus floor with hydraulic pressure. J Oral Implantol. 2005;31(4):197–204.14. Kfir E, Kfir V, Mijiritsky E, Rafaeloff R, Kaluski E. Minimally invasive antral membrane balloon elevation followed by maxillary bone augmentation and implant fixation. J Oral Implantol. 2006;32(1):26–33.15. Bucci-Sabattini V, Salvatorelli G. New simplified technique for augmentation of the maxillary sinus. Montpellier ACTA; 1999.16. Andreasi Bassi M, Lopez MA. Hydrau-lic sinus lift: a new method proposal. J Osteol Biomater. 2010;1:93–101.17. Busenlechner D, Huber CD, Vasak C, Dobsak A, Gruber R, Watzek G. Sinus aug-mentation analysis revised: the gradient of graft consolidation. Clin Oral Implants Res. 2009 Oct;20(10):1078–83.18. Carmagnola D, Abati S, Celestino S, Chiapasco M, Bosshardt D, Lang NP. Oral implants placed in bone defects treated with Bio-Oss, Ostim-Paste or PerioGlas: an experimental study in the rabbit tibiae. Clin Oral Implants Res. 2008 Dec;19(12):1246–53.19. Smeets R, Grosjean MB, Jelitte G, Heiland M, Kasaj A, Riediger D, et al. [Hydroxyapatite bone substitute (Ostim) in sinus floor elevation. Maxillary sinus floor augmentation: bone regeneration by means of a nanocrystalline in-phase hydroxyapatite (Ostim)]. Schweiz Monatsschr Zahnmed. 2008;118(3):203–12.
Figure 8: Clinical condition and endoral x-ray of the follow-up, a year after the treatment.