huntington chorea for nursing
24
Khai Ho International University of Nursing Professor Geri Mitchell Huntington Running Head: Huntington Chorea
description
Published by kal_valentine, Nursing student at the International university of nursing.
Transcript of huntington chorea for nursing

Khai HoInternational University of Nursing
Professor Geri Mitchell
Huntington
Running Head: Huntington Chorea

Table of ContentsIntroduction of Huntington Chorea (HD)HistoryPrevalenceBiochemistry/PathophysiologyGenetic Association and TestingNursing dynamicEthical/legal/political issueReference

IntroductionHD is an inherited, degenerative brain disorder
which results in loss of both mental and physical control.
HD also known as Huntington Chorea (chorea mean to dance-like movement that is uncontrollable)
Onset before the age of 20y/o, the condition is call Juvenile HD

The Discovery of HDHD was first described by Dr. George
Huntington in 1872 as a chronic progressive neurodegenerative disorder affecting movement, cognitive function, and personality.
In 1983 scientists discovered the Huntington's gene was associated with chromosome 4 .
After 10 more years of research, scientists have pinpointed the exact location of Huntington gene to be at 4p16.3 gene site on chromosome 4. The gene was known as IT15 (HTT).

Prevalence
It is rare but deadly, common among white European 7/100,000
America: 30,000 people are affected and 200,000 are at risk of inheriting the disease
Onset usually occurs between the age of 30-50, death usually follow 12 years after onset

Biochemistry/PathophysiologyHD is a chromosome disorder that occurs on
4p16.3
At 4p16.3 juncture, the Huntington gene (HTT) contain a sequence of DNA bases (cytosine-adenine-guanine, CAG)
This sequence repeat many times (CAG-CAG-CAG-CAG-CAG-CAG-CAG-CAG)
Repeating of the CAG bases create a protein called huntingtin (Htt)
< 36 repeat is Htt but > 36 is mHtt

Biochemistry/Pathophysiology Continued
Repeated count Classification Disease Status
< 27 Normal Unaffected
27-35 intermediate unaffected
36-39 Reduce penetrance
+/- affected
>39 Full penetrance
affected
Number of CAG repeating determine onset

Pathophysiology ContinuedmHtt will cause decaying of neurons in
various regions of the brain such as the basal ganglia, frontal and temporal lobe
Basal ganglia is responsible for motor function control, cognition, emotion, and learning

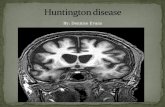
Huntington’s chorea
Note loss of caudate and putamen

SymptomsMotor
Cognitive
psychosocial
Chorea, muscle rigidity, unbalanced gait, tremor, dysphasia and choking
Difficulty processing information and concentration, loss of memory, poor judgment, aphasia
Aggressive antisocial behavior, outburst of yelling and aggression toward others, depression

Prognosis/Progression/Longevity
Once affected, disease will progressPrognosis, chronic disability and deathLife expectancy is 15-20 years after symptoms occurRate of progression depend on number of repeated
CAGProgression usually begins with lack of
concentration, short-term memory, uncontrollable muscular movements, depression, changes of mood (aggressive or antisocial behavior) and stumbling and clumsiness. It get more severe with times.

Genetic AssociationSingle gene &
chromosome related disorder
Is autosomal dominant disorder
HD is inheritance/ sporadic mutation due to (radiation, chemical, and viral infection)

Genetic TestingResearch is ongoing
Direct gene testing (predictive or pre-symptomatic testing)
Pre-implantation Genetic Diagnosis (PGD)
Confirmatory testing
Pre-natal testing
Testing can cost $600-$1500

Nursing DynamicNursing theory: Jean
Watson theory of caring
Nursing Diagnosis:Risk for injuryRisk for self-mutilation
(suicide)Risk for imbalance nutrition
less the body requirementMobility impairRisk for ineffective airwayChronic confusionPowerlessnessHopelessnessMemory impairment Impaired communication

Nursing Dynamic continuedExpected outcomeThe pt will:not injure himselfMaintain normal wtNot have skin break
downInteract socially with
othersMaintain independence
as possibleMaintain LOCAble to communicate
with care giver
Family DynamicPatience Assist in mealMonitor for self-
injurySupport/comfortAssist in legal issuesKnowledge deficitSelf-care deficit

Treatment & InterventionMonitor pt for self-harm (sleeping, home
safety)Keep pt away from sharp objectsFeed pt slowlyUse communication strategiesEncourage pt to be socially activeGroup homes or nursing homeOutpatient therapy (physical/speech)Educate familyRespite Care if at homeHospice/palliative care

Drugs Treatment1. Antipsychotics:
hallucinations, delusions, violent outbursts
2. Antidepressants: depression
3. Tranquilizers: anxiety, chorea
1. haloperidol, chlorpromazine, olanzapine (contraindicated if patient has dystonia)
2. fluoxetine, sertraline hydrochloride, nortriptyline
3. benzodiazepines, paroxetine, venlafaxin, beta-blockers
4. Tetrabenazine: chorea

Nutritional The pt requires more time to eat or be fed
Cut food in small pieces (choking)
Thick liquid in later stage (reduce aspiration)
Increased caloric intake
Insertion of PEG tube

Ethical/Legal/PoliticalEthical dilemmas Political issueIndividuals who are
carriers of HD want to have children
Psychological burden of genetic testing
Personal eugenic: abortion, Pre-implantation Genetic Diagnosis (PGD)
Stem cell Research

Legal IssueDraw up pt will during early stage of disease
Legal assistance may be necessary if the patient encounters discrimination over insurance or employment.
Insurance/employment can drop client if they found out the client is positive or carrier of HD
Abuse of the patient (sexual, physical, verbal. exploitation)

Future Research and TreatmentIntrabody therapy: genetically engineered
intracellular antibody: inhibit mHtt aggregation to delay neurodegeneration
Gene silencing: epigenetic process of switching off the mHTT gene
Stem cell implant: neural stem cells - a type of somatic (adult) stem cell or embryonic stem cell

Cost of CareDrugsCaregivers TherapyDr. visitGenetic testGenetic counselingHospital bill2.5 billion a year
Woody Guthrie

ReferenceFamiy Caregiver Alliance: Huntington Disease. Retrieved December 5, 2008 from FCA. Website:
http://www.caregiver.org/caregiver/jsp/content_node.jsp?nodeid=574
Huntington Disease Society of America. The High Cost of Care. Retrieved December 5, 2008 from HDSA. Website: http://www.lkwdpl.org/hdsa/dmb/
Millers Jean. The Physician Guide to Management of HD. Retrieved December 5, 2008 from HuntDiseaseFAQS. Website: http://endoflifecare.tripod.com/huntdiseasefaqs/id46.html
Neurology Channel. (January 15, 2008). Huntington Disease “Treatment and Prognosis”. Retrieved December 5, 2008 from Healthcommunities.com. Website: http://www.neurologychannel.com/huntingtons/treatment.shtml
Kansas Medical Center. (June 13, 2003). Caring for People with Huntington Disease. Retrieved December 5, 2008 from Kansas Medical Center. Website: http://www.kumc.edu/hospital/huntingtons/
Thulin, Perla Cassayre. (September 16, 2008). The Neurochemistry of Huntington Chorea. Retrieved December 5, 2008 from Docstoc. Website: http://www.docstoc.com/search/huntingtons-chorea/
University of Iowa. (2005). Huntington Chorea. Retrieved December 5, 2008 from University of Iowa Hospital and Clinic. Website: http://www.uihealthcare.com/topics/neurologicalhealth/neur3530.html

Questions/ QuizWhich type of Huntington
disease progresses faster and is more severe
A. Juvenile Huntington B. Adult Huntington
Nursing priority for a pt experiencing tremor during meal should be:
A. Do nothing, and wait for tremor stop
B. Remove sharp objects near ptC. Prevent pt from choking on foodD. Administer a dose of
Tetrabenazine to stop chorea












![ChoreaastheFirstandOnlyManifestationof … · 2019. 7. 31. · treat chorea in SLE patients with antiphospholipid antibod-ies [8, 13]. Considering her mild chorea, we did not start](https://static.fdocuments.in/doc/165x107/60ccda719ee066151f3b3d9b/choreaasthefirstandonlymanifestationof-2019-7-31-treat-chorea-in-sle-patients.jpg)