
A Neurologic Syndrome in Golden Retrievers Presenting as a Sensory Ataxic Neuropathy

IJCRI – International Journal of Case Reports and Images, Vol. 4 No. 6, June 201 3. ISSN – [0976-31 98]
IJCRI 201 3;4(6):321 –325.www.ijcasereportsandimages.com
Hunter syndrome presenting as heart failure: A case reportAsutosh Biswas, Prajowl Shrestha
ABSTRACTIntroduction: Hunter syndrome(Mucopolysaccharidosis type II, MPS II) is agenetic disorder associated with deficiency oflysosomal enzyme iduronate2sulfatase andimpairment of glycosaminoglycans (GAGs)metabolism. Hunter syndrome is well describedin medical literature but less is known aboutheart failure. We are presenting a rare case ofHuntersyndrome with heart failure. CaseReport: A 17yearold boy presented toemergency department with chief complaint ofdyspnea on exertion for last seven days. He alsohad history of progressive abdominal swellingsince five years of age. On examination, he wastachypneic with raised jugular venous pressureand bilateral pitting pedal edema. His head wasdolicocephalic in shape with coarse facialfeatures. His abdomen was distended withhepatosplenomegaly and an umbilical hernia.He has one younger brother with similar clinicalprofile and one normal younger sister.Suspecting mucopolysaccharidosis, weperformed a skeletal survey. A lateral Xray ofthe skull showed an enlarged and Jshaped sellaturcica. Patient’s and his brother’s enzymeassays for iduronate2sulfatase were markedly
low. Based on the clinicoradiological andenzyme assay diagnosis of Hunter syndrome(MPS II) was made. Conclusion: Various clinicaland radiological features are typical of MPS II. Adetailed clinical evaluation and radiologicalinvestigations help in diagnosis of MPS II. Theenzyme assay is required to confirm thediagnosis.Keywords: Mucopolysaccharidosis, Huntersyndrome, Iduronate2sulfatase
*********Biswas A, Shrestha P. Hunter’s syndrome presenting asheart failure: A case report. International Journal ofCase Reports and Images 2013;4(6):321–325.
*********doi:10.5348/ijcri201306322CR7
INTRODUCTIONMucopolysaccharidosis (MPS) is a group ofautosomal recessive metabolic disorders caused by theabsence or malfunctioning of the lysosomal enzymesneeded to break down the glycosaminoglycans (GAGs)[1]. GAGs are long chains of sugar carbohydrates in eachcell that help build bone, cartilage, tendons, corneas,skin and connective tissues. Hunter syndrome, a MPS IIis a rare, Xlinked disorder caused by a deficiency of thelysosomal enzyme iduronate2sulfatase, whichcatalyzes a step in the catabolism of glycosaminoglycans[1]. It is one of the most common MPS, with anestimated prevalence of 1 in 170,000 male live births[2–4]. In patients with Hunter syndrome,glycosaminoglycans accumulate within the tissues andorgans, contributing to the signs and symptoms of thedisease. Common clinical presentation includes facialdysmorphism, hepatosplenomegaly, joint stiffness and
CASE REPORT OPEN ACCESS
Asutosh Biswas1 , Prajowl Shrestha2
Affi l iations: 1 MD, Additional Professor, Department ofMedicine, All India Institute of Medical sciences, New Delhi,Delhi, India; 2MD, Resident, Department of Medicine, AllIndia Institute of Medical sciences, New Delhi, Delhi, IndiaCorresponding Author: Asutosh Biswas, AdditionalProfessor, Department of Medicine, Room No. : 4079, AllIndia institute of Medical Sciences, New Delhi, India11 0029; Phone: +91 9968304243; E-mail :asudelhi@gmail .com
Received: 27 August 201 2Accepted: 07 December 201 2Published: 01 June 201 3
Biswas et al. 321

IJCRI – International Journal of Case Reports and Images, Vol. 4 No. 6, June 201 3. ISSN – [0976-31 98]
IJCRI 201 3;4(6):321 –325.www.ijcasereportsandimages.com Biswas et al. 322
contractures, pulmonary dysfunction, myocardialenlargement and valvular dysfunction, neurologicalinvolvement and excess urinary GAGs excretion [5].Diagnosis of this disease is based on the compatibleclinico radiological profile with serum enzyme assay andurinary tests for excess GAGs. Enzyme replacementtherapy has emerged as a new treatment formucopolysaccharidosis disorders, including Huntersyndrome. We report this case of MPS type II because ofits rarity and features of acute decompensated heartfailure as a presenting feature. The purpose ofpresenting this case is to highlight the distinctiveclinical features of Hunter syndrome.
CASE REPORTA 17yearold boy from Madhya Pradesh (India)presented to emergency department with chiefcomplaints of dyspnea on exertion New York HeartAssociation (NYHA) class IV for last seven days. He hadhistory of progressive increase in shortness of breathsince last six months associated with swelling of boththe limbs. He also had a history of progressiveabdominal swelling since five years of age, excessivesnoring with disturbed sleep associated with excessiveday time sleepiness since nine years of age. There wasno history of chest pain, abdominal pain, fever,constipation, diarrhea, vomiting, bleeding, jaundice,seizure, weight loss or loss of appetite or ofconsciousness. His bowel and bladder habit was normal.He was deaf and dumb since childhood. He has oneyounger brother with similar clinical profile and onenormal younger sister. He was a product of nonconsanguineous marriage and was delivered after fullterm normal pregnancy. His perinatal period wasuneventful. Family pedigree chest of the patient isshown in Figure 1.On examination, the patient's head wasdolicocephalic in shape, with a circumference of 58 cm.He had a depressed and flat nasal bridge, flaringnostrils, large tongue, a short neck, coarse facialfeatures, small stubby fingers with flexion of the distalinterphalangeal joint (Figure 2A–2B). Anthropometricexamination showed him to be severely stunted (heightof 114 cm) without wasting. His fundus appearednormal. His abdomen was soft, distended with anumbilical hernia. His liver was 14 cm below the rightcostal margin in the midclavicular line, with a firm,sharp margin and a smooth surface with a span of 16cm. His spleen was 4 cm below the left costal margin inthe midclavicular line. There were diffuse inspiratorycrepitations all over the lung field. His heart had a grade3/6 nonradiating systolic murmur in the mitral andtricuspid area. Suspecting MPS, we performed a skeletalsurvey. Anteroposterior and lateral Xrays of the skullshowed an enlarged and Jshaped sella turcica (Figure3). The bones of the skull and sutures appeared normalfor his age. Anteroposterior and lateral Xrays of thedorsolumbar spine showed antero inferior beaking atL2. Xrays of both hands showed his phalanges and
metacarpals to be widened with proximal pointing(Figure 4). The remaining bones and joints under viewappeared normal. Xray of chest showed grosscardiomegaly with widened anterior end of ribs(Figure 5).Twodimensional ECHO showed thickened valveswith mild mitral, aortic and tricuspid regurgitation.Both the ventricles were hypertrophied. There was mildbiventricular dysfunction with left ventricular ejectionfraction of 45%.Otolaryngology (ENT) evaluation revealed adenoidhypertrophy and edematous arytenoids. Pure tone
Figure 1: Family pedigree chart of the patient, arrow showingthe patient.
Figure 2: (A) Patient with hunter’s syndrome with his brothershowing coarse facial features, flat nasal bridge and umbilicalhernia, (B) Patient’s hand with small stubby fingers withflexion deformity of the distal interphalangeal joint.
Figure 3: Lateral Xray of skull of patient showing prominentJshaped sella turcica.

IJCRI – International Journal of Case Reports and Images, Vol. 4 No. 6, June 201 3. ISSN – [0976-31 98]
IJCRI 201 3;4(6):321 –325.www.ijcasereportsandimages.com Biswas et al. 323
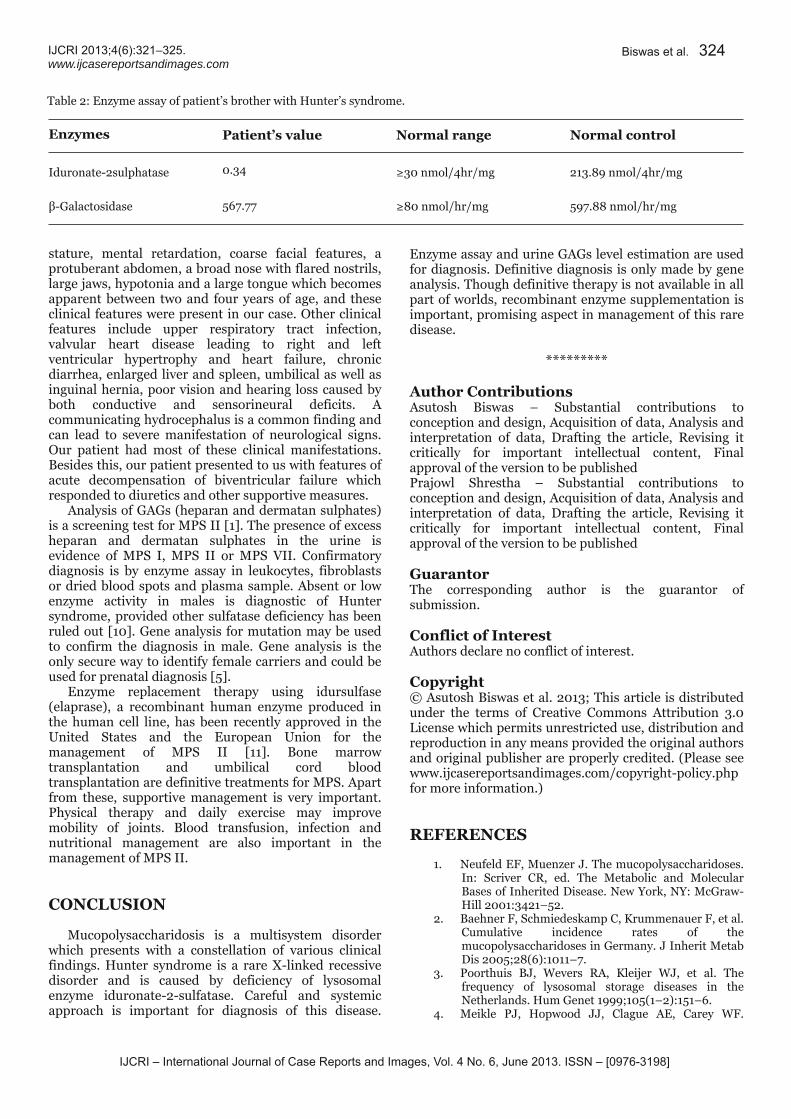
audiometry showed mixed conductive andsensorineural hearing deafness.Noncontrast computed tomography (NCCT) of headwas done which showed dolichocephalic head with mildventricular enlargement. Polysomnography was done inview of his excessive snoring and day time sleepiness.However, the polysomnography was normal withApneaHypopnea index of 4.7. Enzyme assay forIduronate2sulfatase was done for both the brothers.The Iduronate2 sulfatase levels were markedly low inboth the brothers, the levels were 0.19 nmol/4hr/mg inpatient and 0.34 nmol/4hr/mg in his brothers. Normalrange of this enzyme is > 30 nmol/4hr/mg (Table 1 andTable 2). The positive enzyme assay confirmed ourdiagnosis of Hunter syndrome (MPS II).
DISCUSSIONIn our case all the clinical features such as shortstature, a large head, organomegaly, a depressed nasalbridge, a short neck, coarse facial features, small stubbyfingers, mild mental retardation with normalintelligence; and radiological features such as a Jshaped sella turcica, beaking of vertebrae, proximaltapering of metacarpal bones and tapering of theposterior ends of ribs (paddle and/or spatulated ribs) aswell as his developmental history were all suggestive ofMPS II.Mucopolysaccharidosis was first described byCharles Hunter, a Canadian physician, who in 1917described a rare disease found in two brothers [6].Mucopolysaccharidosis is a group of inherited diseasescharacterized by defective lysosomal enzymesresponsible for the degradation of mucopolysaccharides,which are major components of intercellular connectivetissue. This leads to an accumulation of incompletelydegraded mucopolysaccharides in the lysosomes whichaffect various body systems through enzymatic activity[7].All MPS are autosomal recessive, except Huntersyndrome which is Xlinked recessive. In affectedindividuals, undegraded or partially degraded GAGaccumulates within the lysosomes and is excreted inexcess in the urine. The accumulation of GAG within thelysosomes is responsible for the clinical manifestation ofthis disorder [8]. Mucopolysaccharidosis type II orHunter syndrome is rare and is caused by a deficiency ofiduronate2sulfatase as described by Neufeld in 1987[9]. Hunter syndrome is one of the most common MPSwith a prevalence of one in 170,000 male live births[2–4]. Patients typically appear normal at birth. In thesevere form, clinical features appear between two andfour years of age while in the mild form the clinicalfeatures appear in the second decade of life. In thesevere form there is severe mental retardation and lossof skills. Death usually occurs in the first or seconddecade of life and the main cause of death is obstructiveairway disease or cardiac failure [1]. In the milder formthere is mild mental retardation but intelligence isnormal, stature is near normal and clinical features areless obvious and progress very slowly. Diagnosis isusually made in the second decade of life. Death usuallyoccurs in the fourth decade and the main cause of deathis cardiac failure.Diagnosis of the disease is usually made by clinicalpresentation and skeletal survey. The common clinicalpresentations are a large head (dolichocephalic), short
Figure 4: Xrays of both hands showing widened phalangesand metacarpals with proximal pointing.
Figure 5: Chest Xray showing the gross cardiomegaly withwidened anterior end of ribs.Table 1: Enzyme assays of patient with Hunter syndrome.Enzymes Patient’s value Normal range Normal controlIduronate2 sulphatase 0.19 ≥30 nmol/4hr/mg 213.89 nmol/4hr/mgβGalactosidase 547.09 ≥80 nmol/hr/mg 597.88 nmol/hr/mg
IJCRI – International Journal of Case Reports and Images, Vol. 4 No. 6, June 201 3. ISSN – [0976-31 98]
IJCRI 201 3;4(6):321 –325.www.ijcasereportsandimages.com
stature, mental retardation, coarse facial features, aprotuberant abdomen, a broad nose with flared nostrils,large jaws, hypotonia and a large tongue which becomesapparent between two and four years of age, and theseclinical features were present in our case. Other clinicalfeatures include upper respiratory tract infection,valvular heart disease leading to right and leftventricular hypertrophy and heart failure, chronicdiarrhea, enlarged liver and spleen, umbilical as well asinguinal hernia, poor vision and hearing loss caused byboth conductive and sensorineural deficits. Acommunicating hydrocephalus is a common finding andcan lead to severe manifestation of neurological signs.Our patient had most of these clinical manifestations.Besides this, our patient presented to us with features ofacute decompensation of biventricular failure whichresponded to diuretics and other supportive measures.Analysis of GAGs (heparan and dermatan sulphates)is a screening test for MPS II [1]. The presence of excessheparan and dermatan sulphates in the urine isevidence of MPS I, MPS II or MPS VII. Confirmatorydiagnosis is by enzyme assay in leukocytes, fibroblastsor dried blood spots and plasma sample. Absent or lowenzyme activity in males is diagnostic of Huntersyndrome, provided other sulfatase deficiency has beenruled out [10]. Gene analysis for mutation may be usedto confirm the diagnosis in male. Gene analysis is theonly secure way to identify female carriers and could beused for prenatal diagnosis [5].Enzyme replacement therapy using idursulfase(elaprase), a recombinant human enzyme produced inthe human cell line, has been recently approved in theUnited States and the European Union for themanagement of MPS II [11]. Bone marrowtransplantation and umbilical cord bloodtransplantation are definitive treatments for MPS. Apartfrom these, supportive management is very important.Physical therapy and daily exercise may improvemobility of joints. Blood transfusion, infection andnutritional management are also important in themanagement of MPS II.
CONCLUSIONMucopolysaccharidosis is a multisystem disorderwhich presents with a constellation of various clinicalfindings. Hunter syndrome is a rare Xlinked recessivedisorder and is caused by deficiency of lysosomalenzyme iduronate2sulfatase. Careful and systemicapproach is important for diagnosis of this disease.
Biswas et al. 324
Enzyme assay and urine GAGs level estimation are usedfor diagnosis. Definitive diagnosis is only made by geneanalysis. Though definitive therapy is not available in allpart of worlds, recombinant enzyme supplementation isimportant, promising aspect in management of this raredisease.*********
Author ContributionsAsutosh Biswas – Substantial contributions toconception and design, Acquisition of data, Analysis andinterpretation of data, Drafting the article, Revising itcritically for important intellectual content, Finalapproval of the version to be publishedPrajowl Shrestha – Substantial contributions toconception and design, Acquisition of data, Analysis andinterpretation of data, Drafting the article, Revising itcritically for important intellectual content, Finalapproval of the version to be publishedGuarantorThe corresponding author is the guarantor ofsubmission.Conflict of InterestAuthors declare no conflict of interest.Copyright© Asutosh Biswas et al. 2013; This article is distributedunder the terms of Creative Commons Attribution 3.0License which permits unrestricted use, distribution andreproduction in any means provided the original authorsand original publisher are properly credited. (Please seewww.ijcasereportsandimages.com/copyrightpolicy.phpfor more information.)
REFERENCES1. Neufeld EF, Muenzer J. The mucopolysaccharidoses.In: Scriver CR, ed. The Metabolic and MolecularBases of Inherited Disease. New York, NY: McGrawHill 2001:3421–52.2. Baehner F, Schmiedeskamp C, Krummenauer F, et al.Cumulative incidence rates of themucopolysaccharidoses in Germany. J Inherit MetabDis 2005;28(6):1011–7.3. Poorthuis BJ, Wevers RA, Kleijer WJ, et al. Thefrequency of lysosomal storage diseases in theNetherlands. Hum Genet 1999;105(1–2):151–6.4. Meikle PJ, Hopwood JJ, Clague AE, Carey WF.
Table 2: Enzyme assay of patient’s brother with Hunter’s syndrome.Enzymes Patient’s value Normal range Normal controlIduronate2sulphatase 0.34 ≥30 nmol/4hr/mg 213.89 nmol/4hr/mgβGalactosidase 567.77 ≥80 nmol/hr/mg 597.88 nmol/hr/mg

IJCRI – International Journal of Case Reports and Images, Vol. 4 No. 6, June 201 3. ISSN – [0976-31 98]
IJCRI 201 3;4(6):321 –325.www.ijcasereportsandimages.com
Prevalence of lysosomal storage disorders. JAMA1999;281(3):249–54.5. Martin R, Beck M, Eng C, et al. Recognition anddiagnosis of mucopolysaccharidosis II (Huntersyndrome). Pediatrics 2008;121(2):e377–86.6. Hunter C. A rare disease in two brothers. Proc R SocMed 1917;10:104–16.7. Kliegman RM, Behrman RE, Jenson HB, StantonFB. Nelson Textbook of Pediatrics. Volume 1. 18thedition. Philadel phia: Saunders 2007:620–6.8. Tuschl K, Gal A, Paschke E, Kircher S, Bodamer OA.Mucopolysaccharidosis Type II in females: casereport and review of literature. Pediatr Neurol2005;32(4):270–2.
Biswas et al. 325
9. Daniele A, Di Natale P. Hunter Syndrome: Presenceof material crossreacting with antibodies againstiduronate sulfatase. Human Genetics1987;75(3):234–8.10. Dean CJ, Bockmann MR, Hopwood JJ, Brooks DA,Meikle PJ. Detection of mucopolysaccharidosis typeII by measurement of iduronate2sulfatase in driedblood spots and plasma samples. Clin Chem2006;52(4):643–9.11. Muenzer J, Wraith JE, Beck M, et al. A phase II/IIIclinical study of enzyme replacement therapy withidursulfase in mucopolysaccharidosis II (Huntersyndrome). Genet Med 2006;8(8):465–73.
Access full text article onother devices Access PDF of article onother devices


















