
HUNGARIAN ENVIRONMENTAL HEALTH ACTION...
100
HUNGARIAN ENVIRONMENTAL HEALTH ACTION PROGRAMME Budapest 1997
Transcript of HUNGARIAN ENVIRONMENTAL HEALTH ACTION...

HUNGARIAN ENVIRONMENTAL HEALTH
ACTION PROGRAMME
Budapest1997
Ákoshegyi, GyörgyBenkő, GyöngyiBezegh, AndrásBíró, GyörgyBozó, PálBunyevácz, JózsefBuzásné, Harttyányi MariettaCsanády, MihályCsászár, GyörgydeBlasio, AntonioDura, GyulaFarkas, IldikóFodor, IstvánFórián, Szabó PéterGalgóczy, GáborGroszman, MáriaGyarmati, JánosHalasiné, Kőszegi ZsuzsannaHavas, PéterHibbeyné, Joó MártaHirka, FerencHorváth, AmandaHorváth, CsabaHorváth, MihályJózan, PéterKántor, MiklósKertész, MagdolnaKovács, SándorKőrösi, MáriaKöteles, György
Kvojka, FerencLantos, GézaLászló, FerencLászló, LászlóMáté, IstvánMolnár, JenőNemes, IstvánnéNikl, IstvánŐri, IstvánPintér, AlánRódler, ImreRózsahegyiné, Csapó OlgaRudnai, PéterSas, BarnabásSohár, PálnéSomfai, MagdolnaSóstói, PálnéSurján, JózsefSzerbin, PávelSzékely, KálmánTálas, ZsuzsannaTörök, EszterUngváry, GyörgyVarga, LászlóVári, AnnaVárkonyi, TiborVincze, IstvánWajand, JánosWittek, ErnőZoltai, Nándor
The Hungarian Environmental Health Action Programme
was developed by working groups consisting of the following experts:
The generous support of the Danish Government and especiallyJens Steensberg, Ph., D., Denmark is greatfully acknowledged
Responsible editor:Alán Pintér
Deputy Director General‘B. Johan’ National Institute of Public Health
1097 Budapest, Gyáli út 2-6.Tel/fax: (36 1) 215 21 46
Printed: Prospektus Nyomda, Veszprém
1997

Page
1. Background 4
2. Environment and Health in Hungary 6
3. Pilot Project and Pilot Countries 7
4. Goals of the HEHAP 8
5. National Environmental Programme 10
6. Health Status of the Population 12
7. Process of Prioritisation 20
8. Overview of the Most Important Areas of Environmental Health 23
8. 1 Air Quality 23
8. 2 Water Quality 33
8. 3 Noise 44
8. 4 Soil Quality and Wastes 48
8. 5 Work Environment 55
8. 6 Chemical Safety 59
8. 7 Road Traffic Safety 63
8. 8 Radiation Safety 68
8. 9 Food Safety 72
8. 10 Urban Environment 79
9. Areas and Instruments for Implementation of the HEHAP 84
9. 1 Environmental Health Information System 84
9. 2 Role of Local Authorities and Non-Governmental Organisations 86
9. 3 Environmental Health Institutions 89
9. 4 Environmental Health Research 92
9. 5 Education and Training in Environmental Health 94
10. International Relations 98
11. Abbreviations 99
3
Contents

Human health and life perspectives are greatlyinfluenced by many factors in the surroundingenvironment. At the same time, human activitieshave their impact on the environment, which isoften harmful for both the environment and health.The World Health Organisation (WHO) has clear-ly stated that human health is not only the absenceof disease, but physical, mental ad social well-being. Similarly, the environment cannot berestricted to the physical environment and envi-ronmental health in the broad sense incorporatesthe whole verticum of human beings and the envi-ronment.
“Environmental health comprises those aspectsof human health, including quality of life, that aredetermined by physical, biological, social andpsychosocial factors in the environment. It alsodeals with the theory and practice of assessing,correcting, controlling and preventing those fac-tors in the environment that can potentially affectadversely the health of the present and future gen-erations (WHO, 1993).”
In 1984 WHO launched an ambitious pro-gramme called “Health for All by the Year 2000(HFA)”. Out of its 36 goals, 9 are concerned withenvironmental health, namely:
11. Accidents;18. Shaping Environmental Health Policy;10. Environmental Health Service;20. Water;21. Air;22. Food;23. Waste, Soil;24. Human Settlements;25. Work Environment.
Although reducing communicable diseases is notpart of the target health environment, they cannotbe separated from the environmental factors andtheir importance is undeniable owing the thedeterioration in hygiene. The programme is stillbasically valid although changes have been intro-duced. An important milestone was the FrankfurtMeeting of countries from the WHO EuropeanRegion, in 1989, where ministers from environ-ment and health sectors first met. The ministersdeclared the decisive importance and role ofenvironmental health. The official document ofthe meeting, the “European Charter on Environ-ment and Health” summarized the environmental
health tasks and the role that WHO should play inmaintaining both the environment and health.
The relationship between the state of the envi-ronment and human health was at the centre of theUnited Nations’ Conference on Environment andDevelopment, held in Rio de Janeiro 1992.Programmes were prepared in the document called“Agenda 21” on how sustainable development canbe achieved.
Countries in Europe have also recognised thatdeterioration of the environment will lead todecline in human health. In this respect, especial-ly Central and Eastern European countries experi-enced deterioration of the environment, due tohigh emission of pollutants into air, water and soil.Ministers for Environment from European coun-tries, along with international organisations suchas EU, OECD, UN/ECE, met in Dobris Castle(Czechoslovakia) in 1991.
A programme was launched called “Environ-ment for Europe” which focused on improving thestate of the environment, with human health regar-ded as high priority.
The second conference, held in Luzern in 1993,and the recently held third conference in Sofia1995, gave a further boost to countries to developNational Environmental Action Plans (NEAP).
In keeping with the resolution of the FrankfurtConference on Environment and Health, the sec-ond interministerial conference was convened inHelsinki, in 1994, where the ministers of environ-ment and health evaluated the results of the past 5years, implementation of the decisions of theConference in Frankfurt and the situation analysison environmental health called Concern forEurope’s Tomorrow, CET.
Consequences due to the deteriorated environ-ment affecting the health status and welfare ofpeople living in the region were considered trou-bling. In the “Declaration” the ministers endorsedthat an “Environmental Health Action Plan forEurope” (EHAPE) should be developed. The basicprinciples of the Action Plan are the following:
maintenance of solidarity inside and amongnations;sustainable development concerning mea-sures to be taken by environmental andhealth agencies;
4
Background 1
1. Background

cooperation and partnership for the sake ofimproving environment and health status; the principle of subsidiarity has to betaken into account.
Member countries are to be supported in the elab-oration of action programmes resulting in devel-opment of an environmental health status of thepopulation.
5
1 Background

Hungary has been an active participant in the inter-national initiatives since the beginning and under-took an important role in the realization of the pro-grammes of the World Health Organisation. In1991 the WHO European Regional Committeestarted the programme EUROHEALTH supportingthe Central and Eastern European countries inimproving health status and reducing differencesbetween the East and West. Among the pro-grammes the following should be emphasised: pro-gramme for vaccination (EPI), national pro-grammes on noninfectious diseases like CINDI,etc. In 1992 the European Centre on Environmentand Health (ECEH) organised the NationalIntegrated Programme on Environment and Health(NIPEH) where Hungary actively participated.
In the framework of this programme, efforts weremade to develop an information system on envi-ronmental health, increasing the expertise in envi-ronmental epidemiology and environmental healthimpact assessment as tools for analysing healtheffects.
The Ministry of Welfare and the Ministry forEnvironment and Regional Policy did preparatorywork together for the second ministerial confer-ence held in Helsinki and declared that Hungarywished to play an active role in the implementa-tion of the Environment and Health Action Planfor Europe (EHAPE).
6
Environment and health in Hungary 2.
2. Environment and Health in Hungary

Ministers from several countries declared inHelsinki that they would closely collaborate withWHO in preparing their National EnviromentalHealth Action Plans, and based on their initiative,a Pilot Project was launched. Six countries wereselected as participants in the pilot project (Bul-garia, Hungary, Italy, Latvia, United Kingdom,Uzbekhistan). The pilot countries committedthemselves to develop their National Environ-mental Health Action Plans and ensure the neces-sary financial and personnel conditions. Thegained experiences will then be shared with othercountries, helping to establish their NEHAPs.
The governments of the pilot countries and interna-tional organisations (OECD, EU, UN/ECE) pledgedto support the pilot project by providing highlevelcommitment to elaborate national programmes andharmonise work among the countries.
In Hungary a Committee was formed in the frameof the National Public Health Committee supportedby the Ministry of Welfare and the Ministry forEnvironment and Regional Policy, to elaborate theNational Environmental Health Action Programme.The Danish Government, through the WHO-ECEH, generously provided support for developingthe pilot projects in Hungary and Latvia.
7
Pilot Project and Pilot Countries 3.
3. Pilot Project and Pilot Countries

Following the guidelines accepted by the confer-ence in Helsinki, the main goals and targets of theHEHAP are to provide a framework for improvingthe state of the environment and protecting andpromoting human health through environmentalimprovement.
Main aspects of the HEHAP are:
to promote an environment supportive tohuman health and improving the health sta-tus of the population;to overview the most important environmen-tal health issues and problems while settingpriorities for implementation;to develop scientifically sound projectsincluding technological, economic andadministrative details (“bankable projects”);to ensure close collaboration with respectiveministries, agencies and other parties, withthe health and environment sectors playing aleading role;to encourage local initiatives (local govern-ments, nongovernmental organisations) toimprove environmental health in local areas;to promote activities related to a healthy lifestyle;to improve the possibilities of research onenvironmental health problems; to encour-age international collaboration in the field ofenvironmental health; utilising availablefinancial tools to support priorities.
The National Environmental Health ActionProgramme will be successful if it gives supportfor setting up local programmes. Therefore it isvery important, that the regional institutionsbelonging to the Ministry of Welfare – first ofall the Regional Institutes of the NationalPublic Health and Medical Officers Service –use the Programme for elaborating their ownlocal plans.
In order to help attainment of these goals, toolsand strategic elements for the implementationshould be improved or established for:
establishment of new information systemsand further development of existing ones forthe systematic analysis of relationships bet-
ween environment and health, includingevaluation of changes and trends in time andspace;acquiring public support and cooperationamong the governmental organisations andNGOs;elaboration of a scientifically sound basis forpriority setting;improvement of the efficiency of environ-mental health services through an appropri-ate institutional infrastructure;promoting efficiency of environmental man-agement;improvement of professional and public edu-cation and training in environmental health;harmonisation of the existing and preparedprogramme such as governmental projects,National Environmental Programme, Pro-gramme of the Commission on SustainableDevelopment, etc.;publishing environmental health informationserving the prevention of environmental andhealth damage and the decisions of citizens;improvement of legal instruments.
DurationThe National Environmental Health Action Pro-gramme determines the tasks for a period of sixyears. Each second year, based on the experiencegained, the Programme should be reviewed andevaluated, priority determined, and correctionsmade.
Realisation of the Programme should be basedon wide social cooperation. Regional and localhealth and environmental institutions should playan outstanding role in the implementation. Thetasks described in the sections are to be performedwith the leadership of the specified responsibleorganisations.
Institutions responsible for implementing HEHAPImplementation of HEHAP is possible only withthe cooperation of the whole society.
Due to the leading role of health aspects, theNational Institute of Public Health and MedicalOfficers Service bears the highest responsibilityfor guiding cooperation among the other institu-
8
Scope and Purpose of the HEHAP 4.
4. Scope and Purpose of the Hungarian Environmental Health
Action Programme (HEHAP)
tions and organisations, such as competent author-ities, local governments, NGOs and local popula-tion. The role of the institutions is described insection 9. 3.
Controlling and monitoring the implementation of the Programme
After the Programme has been approved by theParliament, the Environmental Health SteeringCommittee of the National Public Health Com-mittee is to control and make proposals for amend-ment.
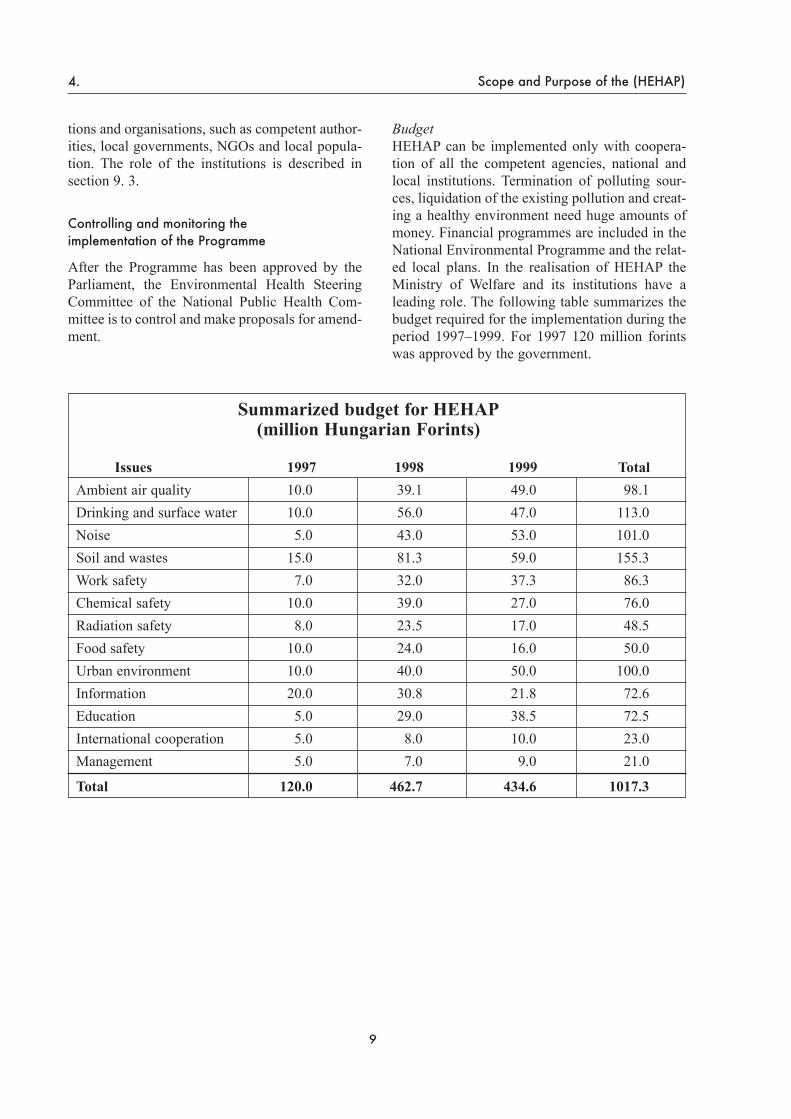
Budget HEHAP can be implemented only with coopera-tion of all the competent agencies, national andlocal institutions. Termination of polluting sour-ces, liquidation of the existing pollution and creat-ing a healthy environment need huge amounts ofmoney. Financial programmes are included in theNational Environmental Programme and the relat-ed local plans. In the realisation of HEHAP theMinistry of Welfare and its institutions have aleading role. The following table summarizes thebudget required for the implementation during theperiod 1997–1999. For 1997 120 million forintswas approved by the government.
9
4. Scope and Purpose of the (HEHAP)
Summarized budget for HEHAP(million Hungarian Forints)
Issues 1997 1998 1999 TotalAmbient air quality 10.0 39.1 49.0 98.1Drinking and surface water 10.0 56.0 47.0 113.0Noise 5.0 43.0 53.0 101.0Soil and wastes 15.0 81.3 59.0 155.3Work safety 7.0 32.0 37.3 86.3Chemical safety 10.0 39.0 27.0 76.0Radiation safety 8.0 23.5 17.0 48.5Food safety 10.0 24.0 16.0 50.0Urban environment 10.0 40.0 50.0 100.0Information 20.0 30.8 21.8 72.6Education 5.0 29.0 38.5 72.5International cooperation 5.0 8.0 10.0 23.0Management 5.0 7.0 9.0 21.0
Total 120.0 462.7 434.6 1017.3

Besides the initiative of the World Health Organi-zation, the ministers of environmental protectionof European countries decided to elaborate envi-ronmental programmes. The process “Environ-ment for Europe” is based on the environmentalprojects of the individual countries.
The Hungarian government passed the Act. LIII.of 1995 on the General Rules of Environmentalprotection, which provided for the elaboration of aNational Enviromental Programme. Taking intoaccount that the main goal of both HEHAP andNEP programmes sustain and protect humanhealth they should be harmonized.
Basic aims of the NEP are:to ensure the right to a healthy environment;conservation of nature and biodiversity;safe and protecting care for natural resour-ces, taking sustainable development intoconsideration;creating harmony between economy and en-vironment.
Defining priorities, elaborating plans and projectspreparation are included in both programmes,therefore the two programmes have to be done witha concerted approach. Cooperation to date appears toguarantee that unnecessary duplication will beavoided and that the two programmes determinetasks in a complementary way.
10
National Environmental Programme 5.
5. National Environmental Programme (NEP)
11
6. Health Status of the Population
Age distribution of the population by country

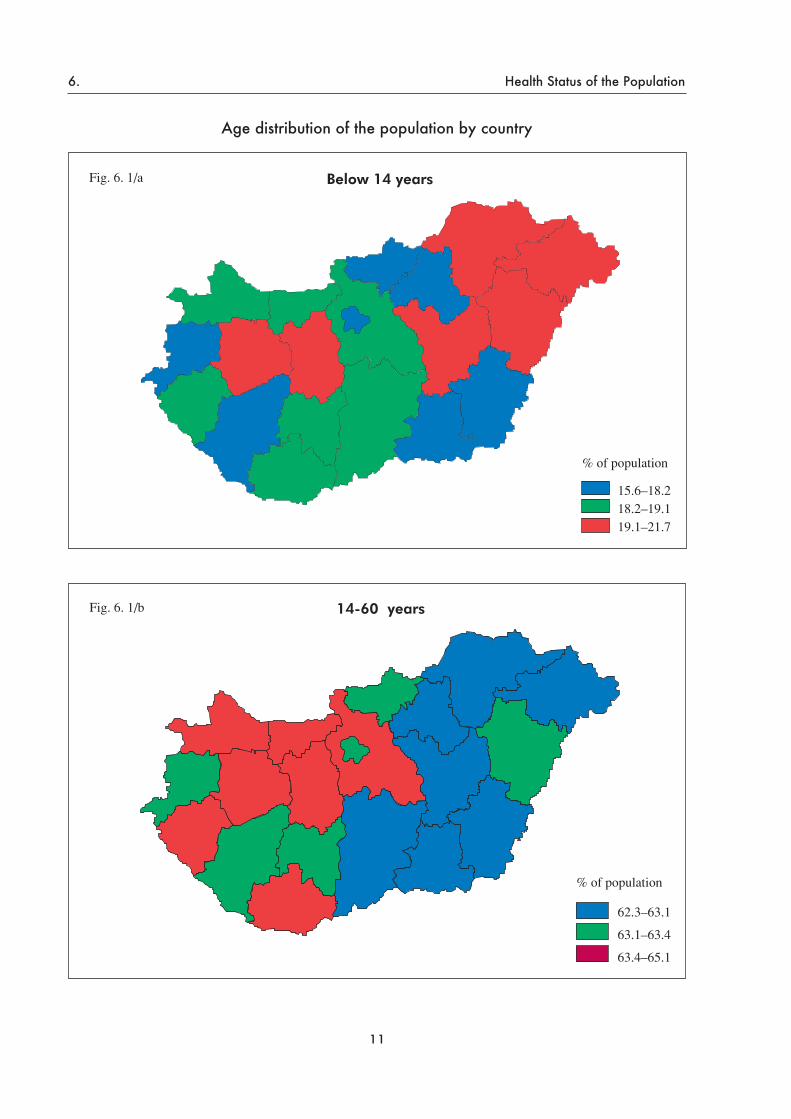
The health status of the Hungarian population isvery poor in absolute terms and in comparisonwith other European countries. The population isdecreasing due to the declining number of live-births and the increasing mortality. In recentdecades the proportion of middle aged and the agegroup above 60 grew significantly. Besides theageing of the population, the high mortality rate ofthe active, working population is a problem. Thereare big differences in the age distribution of thepopulation in the country – in the Eastern countiesthe rate of those aged 1–14 is high and the rate ofpeople above 60 is the lowest here. (Fig. 6. 1)
Reliable parameters characterising health statusare available only for mortality. To evaluate thereal situation and take proper measures, morbiditydata need to be known.
Infant mortality – although with declining ten-dency – is almost twice the average for Europe(11.5% versus 5.8%). Adult mortality is higherthan the European average in both men andwomen. (Fig. 6. 2 and 6. 3) The difference is hugefor middleaged men (40–60 years) where the mor-
tality is one of the highest in Europe. Life ex-pectancy at birth for males was 64.5 years in 1994,one of the lowest in Europe; that of females, 73.8years, was also lower than the European average.(Fig. 6. 4) In Europe the rate of avoidable deathsis the highest in Hungary after Bulgaria.
More than 90% of the mortality is due to fivegroups of diseases, namely cardiovascular dis-eases, cancer, violency, gastrointestinal and respi-ratory diseases. Mortality due to ischemic heartdiseases is higher than in most European countriesfor both men (Fig. 6. 5) and women. (Fig. 6. 6)Cardiovascular diseases show considerable regi-onal differences, of which causes need thoroughinvestigation. (Fig. 6. 7)
12
Health Status of the Population 6.
6. Health Status of the Population

13
6. Health Status of the Population

14
Health Status of the Population 6.

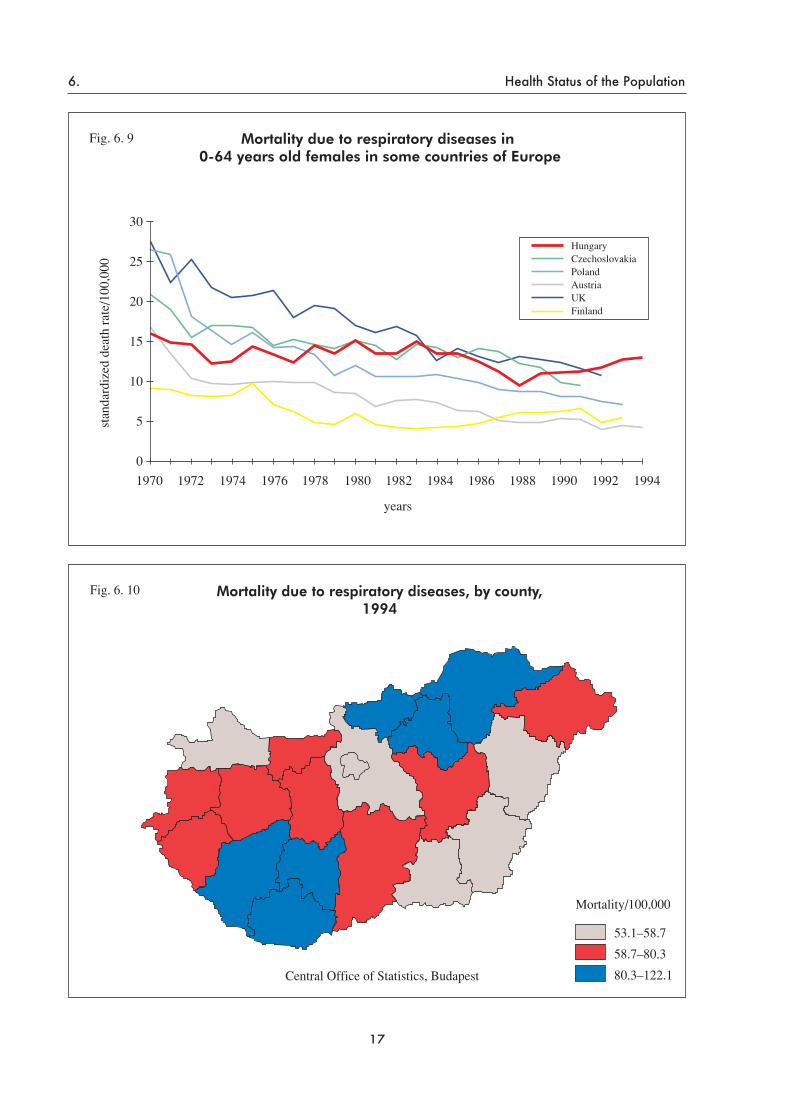
Mortality due to respiratory diseases – althoughwith declining tendency – is higher than the Euro-pean average. (Fig. 6. 8 and 6. 9)
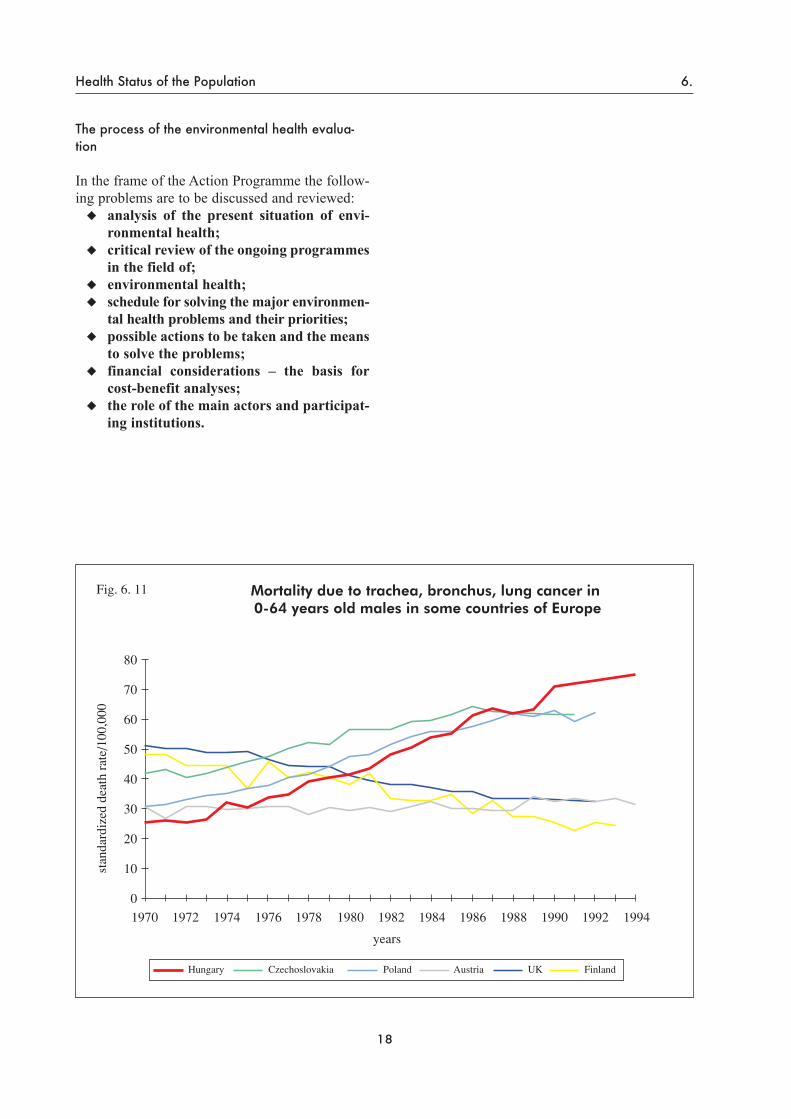
Outdoor and indoor air quality plays a consider-able role of in causing respiratory diseases andstatistics show regional differences within thecountry. (Fig. 6. 10) Cancer mortality is progres-sively growing, main causes being in men lung,liver, colon, pharynx/larynx, prostate cancer, inwomen the order is: breast, lung and cervical can-cer. The environment plays an outstanding role indevelopment of cancer. Smoking is the leadingcause of lung cancer but the role of environmentalfactors is also substantial. In European compari-son the increasing tendency is the greatest con-cern. (Fig. 6. 11 and 6. 12) There are regionalinequalities in the mortality of lung cancer inHungary (Fig. 6. 13) showing the importance ofsocial and economic factors. Among the causes ofviolent deaths, road accidents, murder and suicide,fatal accidents at work and home and poisoningsare the most important. The number of road acci-dents is very high, therefore this problem deservesspecial attention within the framework of the theAction Programme. Gastrointestinal diseases are
caused first of all by nutrition, life style factors,such as smoking, drinking, eating habits and thequality of food. The environment plays hardly anyrole but some elements of chemical and food safe-ty have a place in the Action Plan. Among theleading causes of mortality and morbidity arelifestyle (smoking, drinking) and nutrition, butenvironmental factors have a considerable role aswell. Besides harmful effects at work, urban envi-ronment and their mutual influence are significant.Mortality caused by environmental factors cannotbe easily determined; the estimated rate is about15–20%. The rate is different even within thecountry and the parameters show substantial dif-ferences. Analysis and assessment of the expo-sure-effectdiseaseprocess is complex. Lifestyle,smoking and nutrition have quite short-termimpacts, while impacts of environmental factorsmay appear as health damage only in the follow-ing generation. During the elaboration of theAction Programme the task is to discuss the prob-lems in details, set priorities, and evaluate possi-ble solutions. The following flowchart in chapter7 shows the steps of the process that are importantin assessing health consequences.
15
6. Health Status of the Population

16
Health Status of the Population 6.
17
6. Health Status of the Population
The process of the environmental health evalua-tion
In the frame of the Action Programme the follow-ing problems are to be discussed and reviewed:
analysis of the present situation of envi-ronmental health;critical review of the ongoing programmesin the field of; environmental health;schedule for solving the major environmen-tal health problems and their priorities;possible actions to be taken and the meansto solve the problems;financial considerations – the basis forcost-benefit analyses;the role of the main actors and participat-ing institutions.
18
Health Status of the Population 6.

19
6. Health Status of the Population

The Hungarian National Environmental HealthAction Programme should form the basis forachieving environmental protection with an envi-ronmental health perspective. Formulating thestrategic goals incorporates the main targets, themeans to achieve them, and the criteria for theirefficiency. The primary goal is to increase lifeexpectancy and the number of healthy life yearsby limiting the effects of harmful environmentalimpacts. One of the most important elements ofthe criteria is that the population should live alonger life in health and prosperity. The primaryrequisite for efficiency is an economic category.The category “efficiency” will determine alloptions for the highest benefit in a given econom-ic and financial circumstance. There are severaltechnical terms, which should be understood inorder to fully appreciate the whole context of pri-oritisation. To use costbenefit analysis is essentialto measure benefit. In some cases benefit appearsas reduced risk, and costbenefit analysis can becarried out with the unit of the reduced health risk.If benefit cannot be evaluated as reduced risk, orfinancial evaluation is not available, then the anal-ysis of costeffectiveness can be made.
It should also be pointed out that – concerningthe uncertainty of the present knowledge – sever-al principles should be fixed and applied, i.e:
environmental issues requiring immediateactions;issues requiring short-term action to preventor remedy environmental health problems orelaborating the mode for processing;medium-term issues in the study of factors,concerning the perception and recognitionof risk;long-term goals for securing sustainabledevelopment.
In the course of setting priorities, the goal is todecrease health risk coming from environmentalsources and jeopardising human health. In theseprocesses the following must be taken into consid-eration:
activities started earlier for improving envi-ronmental health targets;circumstances which may influence environ-mental health risks, such as the factors: mea-surability, data availability, their probabili-ties and uncertainties, etc.;
all resources (national, international andother data);options for achieving the targets, includingcost analysis.
1. Risk assessment
In order to be able to assess environmental healthrisk, a distinction must be made between the phas-es of risk estimation and risk management.
Risk assessment is a multistage process whichconsiders steps from hazard identification, throughrisk development, considering the scientificallysound evaluation of cause-effect relationships.
The essence of risk assessment is to collect andevaluate scientific knowledge and data on danger-ous processes and materials which in certain cir-cumstances are risk factors for human health andenvironment. Based on this, risk is quantifiable.
An indispensable part of the analysis is to des-cribe uncertainties.
Key elements of this process are:hazard identification, identification of thepollutant sources;prediction of environmental concentrationsin terms of processes (emission, deliberation,transmission, transformation);exposure assessment (monitoring the ambi-ent concentration, monitoring the exposurethrough biological monitoring);quantitative analysis of the effect as assessedon the basis of doseresponse;risk characterisation and perception.
2. Risk management
Risk management is an integrated part of the pro-cess, where risk assessment is considered as a gen-eral basis for action. Risk management is depen-dent on the political, social and economic contextof a given society, which means specific priorities,dependent on national, regional and local priori-ties. In the context of the HEHAP, attention will bepaid to justification of actions, for solving themost urgent environmental health problems.Problems as “hot spots” come up in the area of hu-man health (respiratory or cardiovascular diseases,cancer, toxicosis, etc.) or environmental damage
20
Process of Prioritization in Environmental Health 7.
7. Process of Prioritization in Environmental Health

(air pollutants from point sources, toxic pollutants,indoor air pollutants, ozone depleting substances,noise as nuisance, etc.). Both approaches are ade-quate and necessary for preparing evaluation,although they lead to considerably different inter-ventions.
At local, regional and national levels, possibili-ties of risk management differ, so local conditionsshould be taken into consideration, setting up per-haps different priorities. The method also differsfrom the processes discussed above. In the differ-ent institutional frames, actions and measures areto be carried out with special antecedents, meth-ods and limited financial resources.
Risk assessment and costbenefit analysis can con-tribute to the objective evaluation of the tasks basedon the requirements of cost efficiency. Priority set-ting is a dynamic process with the condition of con-tinuous planning, evaluation and review.
The approach described above can promote theelaboration of concrete projects, demands for leg-islation, determination of new research fields, me-thodological development and areas of monitoringrequired.
21
7. Process of Prioritization in Environmental Health

22
Process of Prioritization in Environmental Health 7.
1. Situation analysis
About 13% of the Hungarian territory, where 49%of the population lives – is regarded as “polluted”.Emission sources are the following:
traffic;industry;municipal heating and other sources.
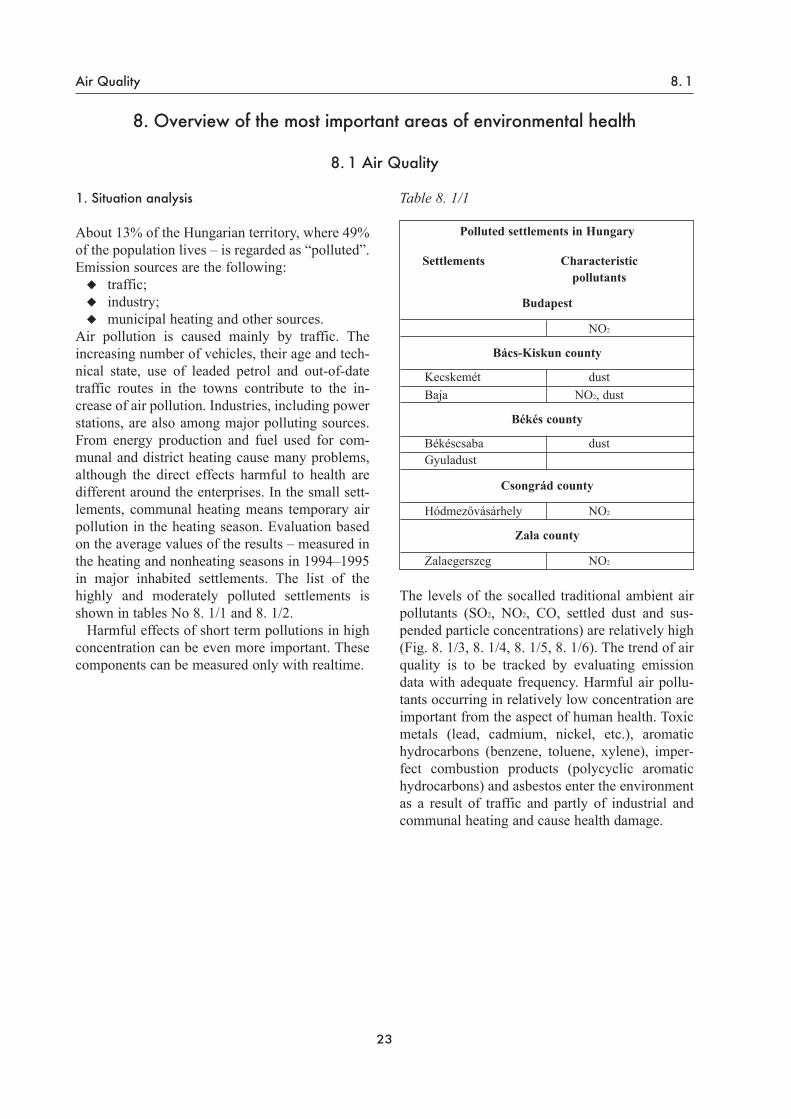
Air pollution is caused mainly by traffic. Theincreasing number of vehicles, their age and tech-nical state, use of leaded petrol and out-of-datetraffic routes in the towns contribute to the in-crease of air pollution. Industries, including powerstations, are also among major polluting sources.From energy production and fuel used for com-munal and district heating cause many problems,although the direct effects harmful to health aredifferent around the enterprises. In the small sett-lements, communal heating means temporary airpollution in the heating season. Evaluation basedon the average values of the results – measured inthe heating and nonheating seasons in 1994–1995in major inhabited settlements. The list of thehighly and moderately polluted settlements isshown in tables No 8. 1/1 and 8. 1/2.
Harmful effects of short term pollutions in highconcentration can be even more important. Thesecomponents can be measured only with realtime.
Table 8. 1/1
The levels of the socalled traditional ambient airpollutants (SO2, NO2, CO, settled dust and sus-pended particle concentrations) are relatively high(Fig. 8. 1/3, 8. 1/4, 8. 1/5, 8. 1/6). The trend of airquality is to be tracked by evaluating emissiondata with adequate frequency. Harmful air pollu-tants occurring in relatively low concentration areimportant from the aspect of human health. Toxicmetals (lead, cadmium, nickel, etc.), aromatichydrocarbons (benzene, toluene, xylene), imper-fect combustion products (polycyclic aromatichydrocarbons) and asbestos enter the environmentas a result of traffic and partly of industrial andcommunal heating and cause health damage.
23
Air Quality 8. 1
8. Overview of the most important areas of environmental health
8. 1 Air Quality
Polluted settlements in Hungary
Settlements Characteristic pollutants
Budapest
NO2
Bács-Kiskun county
Kecskemét dustBaja NO2, dust
Békés county
Békéscsaba dustGyuladust
Csongrád county
Hódmezővásárhely NO2
Zala county
Zalaegerszeg NO2

24
8. 1 Air Quality
Moderately polluted settlements
Settlements Characteristic pollutants
Baranya countyPécs SO2, NO2
Mohács NO2
Komló NO2
Siklós NO2
Sellye DUSTSzászvár SO2
Beremend NO2
Bács-Kiskun countyKiskőrös DUSTKiskunfélegyháza DUSTDunavecse DUSTKalocsa NO2, DUST
Borsod-Abaúj-Zemplén countyMiskolc SO2, NO2
Tiszaújváros SO2, NO2
Ózd SO2, NO2
Bükkszentkereszt SO2, NO2
Kazincbarcika SO2, NO2
Sajószentpéter SO2
Csongrád countySzeged NO2
Csongrád NO2
Makó NO2
Fejér countySzékesfehérvár NO2
Dunaújváros SO2, NO2, DUSTMór SO2, NO2, DUST
Győr-Moson-Sopron countyGyőr NO2
Sopron NO2
Hajdú-Bihar countyDebrecen SO2, NO2
Hajdúszoboszló SO2, NO2
Hajdúnánás NO2
Heves countyEger SO2, NO2
Gyöngyös NO2
Hatvan SO2, NO2
Moderately polluted settlements
Settlements Characteristic pollutants
Jász-Nagykun-Szolnok county
Szolnok SO2, NO2
Jászberény SO2
Karcag SO2, NO2
Kisujszállás SO2, NO2
Komárom-Esztergom county
Tatabánya SO2, NO2
Komárom DUSTEsztergom SO2, NO2
Oroszlány NO2, DUSTTata SO2, NO2
Dorog NO2, DUSTLábatlan NO2, DUSTAlmásfüzitő NO2, DUST
Nógrád county
Balassagyarmat DUST
Pest county
Vác NO2, DUSTBudaörs NO2
Cegléd NO2
Somogy county
Kaposvár NO2
Szabolcs-Szatmár-Bereg county
Nyíregyháza SO2, NO2
Rakamaz DUSTKisvárda DUST
Tolna county
Paks DUST
Vas county
Szombathely NO2
Veszprém county
Veszprém NO2, DUSTAjka SO2, NO2
Pápa NO2, DUSTVárpalota NO2
Zirc SO2
Zala county
Keszthely DUSTNagykanizsa NO2
Lenti NO2, DUST
Table 8. 1/2

2. Health effects
The bad health status of the population in Hungaryare – to a significant extent – related to the effectof air pollution.
2. 1 DiseasesPhysical, chemical and biological air pollutantsdamage almost the whole respiratory system anddecrease resistance against infections. They have arole in provoking and maintaining acute andchronic respiratory diseases. Acute respiratory dis-eases are the cause of 23–25% of all cases of sickleave. Connection between the prevalence of thedisease and the measured level of SO2 and sus-pended particles is justified by epidemiologicalstudies carried out among school children. Amongthe acute respiratory diseases, catarrh in the lowerrespiratory tract (e.g. bronchitis, pneumonia)should be given particular attention, because it candecisively influence the future health status.
The number of asthmatic cases is increasing allover world, first of all among children. (Fig. 8. 1/9)The causes are not very clear yet but environmen-tal factors have obviously quite an important role.To get to know the causes better, the prevalence ofthe diseases in Hungary should be better known.
A countrywide survey would be relevant besidesthe data from the pulmonology and allergologyoutpatient clinics.
The complexity of the problem can be seen inFig 8. 1/7, which shows the incidence of asthmaticpatients based on the turnover in hospitals. Severalair pollutants are recognised or suspected carcino-gens to human beings. In the occurrence of themore than eight thousand deaths from lung cancerper year – besides the obviously important smok-ing – certain polycyclic aromatic hydrocarbons andnitroso compounds, asbestos, and certain indoorpollutants (such as smoke, radon) play a major roleas well. The effects of short-term pollution in highconcentration are especially significant.
Among the health damaging factors carcinogensfrom traffic should be taken into account as well.The number of cancer cases is higher among urbandwellers.
Children are highly threatened by the lead con-tent of petrol. According to estimation based on astudy, the lead content of blood in 10% of childrenliving in towns is higher than the 10 mg/dl limitvalue, still not considered safe.
A very important element in prevention is to de-fine and track the indicators, accompanying harm-ful effects. Determination of pollutants or metabo-lites and biological materials (such as enzymes,pathological proteins) are important tools for pre-vention. Biological monitoring should be an out-standing activity in environmental health.
2. 2 MortalityMortality of patients with cardiac and vascular dis-eases rises suddenly in case of increased air pollu-tion (e.g. the smog in London), but the cause of thesocalled harvesting syndrome is not known yet. In1994 3.2% of the total mortality was traced back tochronic respiratory diseases. In recent years therewas no improvement. The rate is practically un-changed. The therapy and prognosis of the diseasesare quite good but the costs are high, which meansthat respiratory diseases have even a higher impor-tance from the economic point of view.
3. Goals to be achieved
Continuous evaluation of the impact of airquality on human health;Special attention to priority areas andprotection of human health by promotingpreventive measures;Prevention of aeroallergens and theirhealth impact;Improvement of indoor air quality;Preventive measures to limit trafficrelatedair pollution;Promotion of ongoing air quality prog-rammes;Increasing the efficiency of monitoring andof information dissemination.
25
Air Quality 8. 1

4. Ongoing programmes
National Environmental Protection andNature Conservation Policy;Implementation Programme for Air QualityImprovement. This programme is of thehighest importance for preventing furtherdeterioration and ensuring improvements.The elements of the programme are listedamong this programme’s objectives;Implementation of International Agreements(emissions of SO2, NO2, ozone-depletingsubstances, etc.);Research areas: within the framework of aPHARE/CESAR project, the effect of SO2
and suspended particles of less than 10 µmdiameter on the respiratory function of chil-dren is being studied.
The most important problems and issues are listedin the following table according to types and lev-els of action:
26
8. 1 Air Quality

27
Air Quality 8. 1Ta
sks l
iste
d ac
cord
ing
to le
vels
of a
ctio
n
Subj
ect a
rea/
Lev
el
Am
bien
t air
Loc
al
Bef
ore
ente
ring
scho
ol sc
reen
ing
pro-
gram
s fo
r le
ad c
onte
nt o
f bl
ood
inca
se o
f chi
ldre
n liv
ing
in to
wns
; In
form
ing
the
publ
ic o
n in
door
cle
an-
ing
to d
ecre
ase
alle
rgen
exp
osur
e;
Act
ions
aga
inst
sm
okin
g;Ex
stirp
atio
n of
wee
ds;
Pollu
tion
cont
rol a
t pow
er p
lant
s;
Loca
l scr
eeni
ng p
rogr
amm
es a
nd e
pi-
dem
iolo
gica
l sur
veys
;Lo
okin
g fo
r m
arke
rs t
o de
term
ine
early
hea
lth e
ffect
s;C
ompa
rison
bet
wee
n m
orta
lity
data
and
ambi
ent
air
qual
ity f
or p
lann
ing
inte
rven
tion;
Dec
reas
ing
indo
or
pollu
tion
inho
mes
, qua
lific
atio
n fo
r m
achi
nery
inbu
ildin
gs;
Smog
ala
rm sy
stem
in to
wns
equ
ip-
ped
with
am
bien
t air
mon
itorin
g st
a-tio
ns.
Reg
iona
l
Prev
entin
g tra
ffic
rela
ted
pollu
tion
(des
ign
of h
uman
set
tlem
ents
, tra
f-fic
lim
itatio
ns);
Reg
ular
mon
itorin
g of
acu
te r
espi
-ra
tory
dis
ease
s, m
orbi
dity
, ev
alua
-tio
n of
dat
a w
ith p
aedi
atric
ians
;A
pplic
atio
n of
bio
logi
cal m
arke
rs in
surv
eys a
nd e
pide
mio
logi
cal s
tudi
es;
Indo
or a
ir qu
ality
con
trol a
t wor
k;C
omm
unic
atio
n ca
mpa
igns
to
pre-
vent
env
ironm
enta
l hea
lth p
robl
ems
resu
lting
from
traf
fic.
Nat
iona
l
Furth
er d
evel
opm
ent o
f inf
orm
atio
nne
twor
ks s
uch
as a
mbi
ent a
ir m
oni-
torin
g sy
stem
for m
easu
ring:
– so
lidpa
rticu
late
s sm
alle
r th
an 2
.5 µ
m; –
BTX
, PA
H,
met
als,
asbe
stos
. Sp
e-ci
al n
etw
ork
for m
easu
ring
aero
bio-
logi
cal
com
pone
nts:
– da
ta c
olle
c-tio
n an
d ev
alua
tion;
Det
erm
inat
ion
(the
miss
ion
and
im-
miss
ion
leve
ls o
f pe
rsis
tent
org
anic
com
poun
ds);
Setti
ng u
p in
door
air
qual
ity li
mits
;Li
mit
valu
es f
or s
olid
par
ticul
ates
smal
ler t
han
10 a
nd 2
.5 µ
m;
Publ
ishin
g da
ta o
n re
latio
nshi
p be
t-w
een
heal
th st
atus
and
air
qual
ity;
Reg
ular
revi
ew o
f am
bien
t air
limit
valu
es.

28
8. 1 Air Quality
Act
ions
to d
ecre
ase
emis
sion
Red
ucin
g em
issi
on fr
ompo
wer
sta
tions
;R
educ
ing
traffi
c-bo
rnem
issi
ons;
Red
ucin
g ae
ro-a
llerg
ens.
Info
rmat
ion,
dat
a co
llect
ion,
mon
itori
ng
Mon
itorin
g of
resp
ira-
tory
dis
ease
s an
d m
or-
talit
y;
Mon
itorin
g of
em
is-si
ons;
Impr
ovin
g am
bien
t ai
r-qua
lity
mon
itorin
gne
twor
k;C
ontro
l of a
mbi
ent a
irpo
lluta
nts;
Parti
cipa
tion
in in
ter-
natio
nal i
nfor
mat
ion
netw
orks
;In
form
atio
n sy
stem
tofo
llow
tran
sbou
ndar
ypo
llutio
n.
zRes
earc
h
Stud
y on
rela
tions
hip
betw
een
air p
ollu
tant
san
d re
spira
tory
dis
ease
sam
ong
child
ren;
Mea
sure
men
t and
stud
yon
the
effe
cts a
nd im
pact
of o
rgan
ic c
ompo
unds
(VO
C, P
AH
, etc
.);St
udy
on a
mbi
ent t
oxic
met
al p
ollu
tant
s;M
onito
ring
expo
sure
, re
sear
ch o
n ch
arac
teris
-tic
mar
kers
.
Adm
inist
rativ
e m
easu
res,
legi
slat
ive
tool
s
Com
plia
nce
with
em
is-
sion
lim
it va
lues
;R
evie
w o
f am
bien
t air
qual
ity li
mit
valu
es;
Con
trol o
f tra
ffic
with
to re
gard
air
pollu
tion;
Intro
duct
ion
of th
e le
-gi
slat
ive
tool
s of
the
EU/O
ECD
;El
abor
atio
n of
indo
orlim
it va
lues
;Es
tabl
ishi
ng c
ondi
tions
for s
mog
ala
rm
syst
ems.
Trai
ning
, edu
catio
n
Publ
ic in
form
atio
n;Pr
even
tion
of e
xpos
ure
to le
ad;
Traf
fic-b
orn
pollu
tion;
Impr
ovin
g aw
aren
ess
in th
e fie
ld o
f ind
oor
air q
ualit
y;In
form
atio
n on
the
dang
er o
f ae
ro-a
llerg
ens.
Task
s lis
ted
acco
rdin
g to
type
s of a
ctio
n

29
Air Quality 8. 1

30
8. 1 Air Quality

31
Air Quality 8. 1

32
8. 1 Air Quality

1. Situation analysis
Drinking waterNearly 97 percent of the population is suppliedwith piped drinking water including public outlets.The quality of the water supplied is excellent intwo thirds of the settlements and the majority ofcomplaints is not directly related to health effects(e.g. iron, manganese, lower than ideal hardness,elevated total bacterial counts). The quality ofdrinking water in the larger towns is generallygood, so that the majority of the population is sup-plied with acceptable drinking water. Incidents ofcontamination with possible health risks (e.g.nitrate, arsenic, fecal-indicator bacteria) affect 3–4percent of consumers. The microbiological con-tamination is only transient, as the risk is reducedby urgent measures. Development and harmoniza-tion of the monitoring and data collection systemsis very important (e.g. frequency and parametersof the measurements of drinking water) to indicateacute hazard and unfavourable trends. Micro-pollutants are to be monitored regularly in thefuture. Collection and evaluation of data from thewaterworks is important as well. Table 8. 2/1shows the data on measurements carried out by theNational Public Health Service in the counties andthe rate of unacceptable results.
The number of settlements with waterworks,where a particular parameter of contaminationdoes not regularly meet the limit value can be seenin Fig. 8. 2/2.
Known and partly solved problemsA longstanding drinking water quality problemaffecting population of larger size is the presenceof nitrate in ground waters and shallow subsurfacewaters. The distribution by county of nitrate con-centrations in the drinking water supplied is illus-trated in Fig. 8. 2/3.
Arsenic occurrence of natural origin in theground water of the southern Great Plain hasaffected a population of almost half a million(according to data gained in 1981–82). As a resultof consecutive government subsidised pro-grammes, the affected settlements have by nowbeen supplied with drinking water with an arseniccontent satisfying the present Hungarian limitvalue of 50 mg/l. The problem, however, still exists
in case of some smaller remote settlements andindustrial and agricultural water supply plants.
In some parts of the country, the high ammoni-um concentration of drinking water represents anenvironmental health hazard.
Some chlorination by-products that are presentin some treated waters of surface water origin andchlorinated wellwaters with high humic contentare mutagenic with suspicion of carcinogenity. Awidespread and easily perceived water qualityproblem is caused by a high iron content, some-times together with manganese. Many – mostlyadequate – iron removal units are in operation butquite often the removal efficiency, especially ofmanganese, is not satisfactory. The drinking waterof large parts of the Great Plain and many adjoin-ing regions contains too much sodium and too lit-tle calcium and magnesium. Distribution of calci-um and manganese concentrations can be seen inFig. 8. 2/4.
Known problems, not yet solvedA drinking water quality problem in considerableparts of the Great Plain is the bacterial aftergrowthin deep well waters which may lead to very highbacterial densities.
The concentration of fluoride in most drinkingwater supplies (approx. 98%) is much lower thanoptimal from a dental health point of view.However, approximately 1% of the population issupplied with concentrations above the limit valueLow iodine intake – characteristic for 80% of thesupplies – is related to a higher frequency ofgoitre. Higher concentrations of iodine causeorganoleptic complaints in the south eastern partof the country (Fig. 8. 2/5).
33
Water Quality 8. 2
8. 2 Water Quality

Lesser known problemsNo data are available on the boron content of con-sumed waters. A more stringent limit value thanthe present Hungarian one has been proposed bythe WHO. Since high boron contents may befound in deep thermal or mineral waters, a surveyseems to be needed very soon.
High lead content in drinking water represents ahealth risk. Lead pollution may come from differ-ent sources, such as new PVC pipes, plumbingmaterials and hot water storage tanks. The signifi-cance of these sources should be elucidated.
Few data are available on the occurrence of pesti-cides. Waters originating from vulnerable sources,including bank filtration, is at potential risk.Especially in agricultural areas however, the dan-ger is possibly not very high because of the de-creasing use of pesticides in recent areas.
Little is known about the water polluting effectof known and unknown waste dumping sites. Thepresence of dichloroethylene as a decompositionproduct of tri- or tetrachloroethylene in the waterof a municipal waterworks is a warning sign.
34
8. 2 Water Quality
1995 All rejected% Rejected because of Rejected because of
bacterial contamination chemical contamination
CountiesWater
Wells TotalWater
Wells TotalWater
Wells Totalworks works works
Baranya 25.4 53.7 27.8 12.6 46.3 13.1 18.9 37.9 21.0
Bács-Kiskun 55.5 70.6 59.5 12.1 19.3 13.0 39.0 74.8 57.9
Békés 56.1 98.0 59.9 24.6 84.0 25.6 34.6 23.0 34.0
Borsod 25.0 75.6 36.7 16.2 61.2 21.0 12.1 15.4 12.9
Csongrád 59.8 100.0 60.1 54.5 68.8 54.6 64.9 88.0 66.0
Fejér 45.5 62.1 50.4 20.7 52.6 25.1 33.7 36.7 34.6
Győr-Sopron 19.8 41.2 23.8 12.2 29.0 13.2 11.7 25.4 14.6
Hajdú-Bihar 67.7 72.6 68.3 18.3 26.0 18.5 48.6 30.7 42.4
Heves 50.0 51.2 52.3 27.3 42.2 28.1 44.2 32.5 41.9
Jász-Nagykun 59.3 65.8 61.0 15.9 25.9 18.4 52.4 55.8 53.2
Komárom 30.9 78.4 32.8 11.9 46.0 12.7 26.4 56.0 27.8
Nógrád 55.3 79.2 58.4 12.1 28.7 12.6 43.7 73.0 47.6
Pest 37.0 56.0 42.7 15.3 34.4 17.7 30.6 46.0 35.2
Somogy 65.1 85.3 68.1 19.8 54.7 21.0 56.0 53.3 55.3
Szabolcs 64.7 89.7 66.5 26.4 29.2 26.5 35.1 60.3 36.8
Tolna 51.1 59.0 51.3 23.9 30.0 24.0 52.3 50.0 52.2
Vas 16.3 27.6 18.1 11.7 30.4 13.3 12.0 20.5 13.4
Veszprém 30.3 57.4 34.4 18.8 47.6 21.3 17.7 37.9 21.0
Zala 22.6 44.8 23.2 14.1 43.9 14.8 11.0 13.8 11.1
County average 44.2 63.9 47.1 18.7 38.2 19.9 32.5 48.1 35.7
Budapest 11.2 11.6 10.1 11.7 2.0 2.2
National average 40.0 64.0 43.2 18.3 38.9 19.6 27.8 48.2 31.5
Table. 8. 2/1National situation of drinking water quality characterized
by the rejected samples rate (%)

2. Bathing water
BeachesBathing and swimming in our largest streams isnot recommended because of the microbiologicalcontamination, except the lower reach of theRáckeve branch of the River Danube. The riverTisza has only few bacteriologically clean beach-es at the uppermost reach between Kisköre andSzolnok but it also has heavily polluted stretchessuch as downstream Szolnok and at Szeged. Someimpounded sections of smaller streams or backwa-ters may be used for bathing. The bacteriologicalcontaminations are caused first of all by the lowlevel of sewage treatment. In such a respect hard-ly 20 percent of the sewage of Budapest is biolog-ically treated; that of, for example Szolnok, Sze-ged and Dunaujváros is untreated.
The water quality of the Lake Balaton is threat-ened by end-of-summer algal blooms as a conse-quence of eutrophication. The lake is bacteriolog-ically clean, as a whole but the water closest to theshore may become contaminated by the bathersthemselves.
Also, the protection of many small lakes, pondsand sandpit excavations has not yet been solved.However, the water users, in general, are the mostsignificant polluters.
Public bathsOnly one third of public pools is equipped withwater treatmentrecirculation devices. Some ofthem, mostly smaller swimming pools, are notoperated correctly, making the water in peak-usage periods of inadequate quality. (Table 8. 2/7)The water in untreated (fill and drain type) poolsis extremely contaminated in peak use periods,such as weekends.
Quality of water used for irrigationIrrigation by polluted surface water is an indirectdanger to human health e.g. in case of wateringvegetables consumed without cooking with con-taminated water.
35
Water Quality 8. 2

36
8. 2 Water Quality

3. Health effects
As a result of upgrading some waterworks, thepopulation at risk of high nitrate levels has signif-icantly decreased. The reported number of methe-moglobinaemia cases dropped in 18 years fromabout 300 to less than 20 per year. In 1990 nitratewas still a problem for 34, mainly small commu-nal waterworks, amounting to 1.4 percent of thetotal of about 2,400 settlements then supplied. Interms of water quantity it represents proportion-ately much less.
As a result of the decreasing fertilizer use, therisk has been reduced but not yet eliminated. Sig-nificant sources of risk are settlements withoutproper sewage treatment. All cases of methe-moglobinaemia have been caused by the con-sumption of water from private wells and not fromcommunal supply. Occasionally, such cases maybe caused by a high nitrate content in vegetables.(Table 8. 2/6)
Epidemiological studies have revealed a signifi-cantly higher proportion of stillbirths and sponta-neous abortions in the region affected by theoccurrence of arsenic, first of all in Békés county,than in other region supplied with arsenicfreewater. Also symptoms of mild arsenic toxicosis –hyperkeratosis and hyperpigmentation – werediagnosed in children, and an elevated frequencyof skin and bladder cancer has been recorded.Prevalence of goitre is high in settlements sup-plied with water with low content of iodine. (Fig.8. 2/5)
37
Water Quality 8. 2

Table 8. 2/6Reported morbidity data on methemog-lobinaemia in Hungary:
Some chlorination byproducts are mutagenic. Therisk may not be very high as the concentrationsfound have been low but this cannot yet be esti-mated with certainty.
The rather poor hygienic situation of the publicbaths without water treatment has been shown byrepeated outbreaks of intestinal infections. Thenumber of outbreaks and registered cases duringthe last two decades is shown in Table 8. 2/7.
Most of these outbreaks were due to Shigellainfection, and the majority of cases were in children.
Table 8. 2/7Outbreaks associated with water of heatedswimming pools in Hungary:
* Includes three suspected outbreaks
4. Goals to be achieved
Overview of the possibility and probabilityof health consequences caused by drink-ing and bathing water pollution and inci-dental contamination;Evaluation of incidental contaminantsand their health effects;Setting priorities for interventions andrecommending measures to be taken;Proposals for the elaboration of projects.
5. Problems to be solved
As far as the arsenic content of drinking water isconcerned a revision is necessary as a conse-quence of the recent lowering of the WHO limitvalue to 10 µg/l. A part of the deep aquifers uti-lised by waterworks are suspected of having in-creasing arsenic concentrations over time. Nodata are available for half of the country as towhether arsenic concentrations exceed the newWHO limit value. The earlier survey was carriedout with a measurement method that is unable todetect concentrations in the range of the new limitvalue.
Passing the ownership of waterworks to mu-nicipalities has in many cases caused an increasedrisk (that is hard to estimate). This may be because– for economic reasons – they opt out of the regi-onal water supply system and start using the earli-er abandoned local water sources that were onlykept as reserves because of poor quality. The levelof operation has also in many cases decreased with
38
8. 2 Water Quality
Year Number Numberof cases of deaths
1976 207 41977 293 71978 239 31979 180 21980 172 31981 166 11982 91 11983 67 –1984 33 –1985 46 11986 41 –1987 30 –1988 31 21989 35 21990 22 –1991 19 21992 19 –1993 23 –1994 15 –1995 9 –Total: 1,738 2
Year Number Numberof outbreaks of cases
1975–1987 36 5,977*
1989 4 428*
1990 1 449+453*
1992 5 71*
1993 2 73*
Total: 48 7,451*

this change. This may have unpredictable conse-quences, including the risk of epidemics.
These may also be caused by the improper ter-mination of disinfection on the grounds of avoid-ing chlorination byproducts. The steep increase ofwaterrates is leading to the renewed use of privatewells that also adds to the risk of waterborn infec-tions.
Artificial waters supplied in containers and bot-tles are emerging on a commercial basis. They arehard to check and the effects of prolonged storage– most often in plastic containers – are not suffi-ciently known.
The above mentioned tasks are of nationwidenature.
Regional problems include the aftergrowth in thedistribution systems on the Great Plain and first ofall in the regions along the River Tisza, that areusing warmer wellwaters. Insufficient protectivezones lead to problems in regions supplied fromshallow aquifers such as bank filtration systems onthe upper reach of the Danube or in the capital andits surroundings, karstic zones in the Transdanu-bian and Northern mountain area (Eger, Miskolc)and in some local areas. The formation of chlorina-tion byproducts needs to be prevented, first of all inthe case of drinking water supplied from surfacewater resources, as in Szolnok and its surround-ings, the Balaton region, and in waterworks in theMátra mountains and north of Nógrád.
Regular control of quality in irrigation and ba-thing water is highly important especially in themain season and measures should be taken in caseof pollution above threshold limits.
Waste disposal sites and other sources of con-tamination occasionally endangering local sour-ces, will be mentioned in section 8. 4.
6. Earlier and recent water quality projects and related programmes
Only the most important projects of nationwidesignificance will be mentioned and summarized.
Drinking water quality upgrade project of theSouthern Great PlainThe project aiming at reduction of the arsenic con-tent of drinking water was initiated with govern-ment subsidy in 1983 and after gradually coveringwaterworks of 80 settlements was finally conclud-ed in 1995. The project brought about significant
improvements not only in the arsenic content butalso in other water quality related parameters,such as ammonium, iron and manganese. Sincethe project did not cover other than municipalwaterworks, the problem is still unsolved in indi-vidual water supply systems and systems operatedby industrial and agricultural plants, and institu-tions.
Protection of aquifersAn executive decree has been elaborated for theprotection of aquifers. This may significantly im-prove the situation if finally passed and implemen-ted. Another tool is the preferential subsidy systemfor sewage treatment projects of municipalities sit-uated upon a vulnerable aquifer. For water qualityprotection purposes the resources of the CentralEnvironmental Protection Fund (CEPF) are avail-able only for these local areas.
Improvement of drinking water supply in villagesThe “target support system” launched in 1991 forthe supply of villages with healthy drinking waterstipulates a 90 percent economic support to theimplementation of supplies with public outlets.The water supply of 247 settlements was ensuredin this way in 1990–92, lowering the number ofsettlements not yet supplied to 352. By the end of1995 only 14 settlements are left without even thisform of drinking water supply. However, about150,000–200,000 persons are living in the outskirtsof towns and villages or in the countryside where itis impossible to provide piped drinking water.
Protection of surface water used for recreationThe recreational district of utmost national impor-tance is the surroundings of Lake Balaton. Exten-sive protective measures with government supporthave been taken since 1983, first of all to halt theeutrophication of the lake. The governmental pro-gramme for Lake Balaton is being extended. Pre-parations are under way to launch a programmewith EU–PHARE support for the examination ofmicrobiological contamination of other surfaceand subsurface waters.
39
Water Quality 8. 2

7. Human health priority of factors impairing thequality of drinking water
In the following, the most significant factors thatimpair the quality of drinking water are listed inorder of priority.
ArsenicArsenic is the most dangerous factor, from ahealth perspective, having chronic effects at evenlow doses. This substance occurs in large areas ofthe country. Although a major part of the problemwas successfully solved (but at very high cost) itsoccurrence in significant concentrations is not rarein individual water supply systems.
Bacterial contaminationIn the districts of the Great Plain with a uniquewater quality, a significant proportion of drinkingwater samples are not yet acceptable because ofbacterial aftergrowth. The solution is not solely ofa financial nature, since no generally applicabletechnology is available. The reorganization of wa-terworks that is taking place may aggravate theproblem. The bacterial contamination may evenlead to disease outbreaks. To prevent this, protec-tion zones must be established to avoid waste wa-ter contamination.
NitrateThe situation is expected to deteriorate in somewater sources on vulnerable aquifers. The problemhas not been solved in some, mostly peripheric set-tlements that are not yet supplied from waterworks.The prevention applied earlier to protect the healthof babies, e.g. education and bottled water supply,is less organised in these areas. Another source ofrisk stems from the consumption of private wellwater that is being used increasingly as a conse-quence of the high waterrate.
Sodium (lack of calcium and magnesium)The problem exists in major parts of the GreatPlain. The excess of sodium may especially affectthe health of patients who are dependent on a lowsalt diet due to cardiovascular disease or renal fail-ure. An inadequate intake of calcium is a problemfor pregnant and elderly women. Also, the lack ofmagnesium may be of health importance.
NitriteAs a result of secondary pollution in the distribu-tion systems, nitrite occurs in bacteriologicallycontaminated pipelines. Nitrite is 10–15 timesmore toxic than nitrate. First of all babies are atrisk, but high concentrations are also of impor-tance to the health of adults.
Chlorination byproductsAs a result of earlier measures, chlorination by-products are not generally present in high concen-trations. Potential risk is related to the presence ofunknown, less volatile (and not yet measured) mu-tagenic compounds. Sometimes it is indispensableto chlorinate water with a high humic content whichmay also produce unknown substances.
Other micropollutantsAmong microcontaminants, boron, lead and pesti-cides may be mentioned, but no general knowl-edge is available about their occurrence, so thatthe possible risk cannot be estimated. Accordingto unrepresentative exploratory surveys, pesticidecontamination of drinking water does not at pre-sent seem to be a problem. The occurrence ofboron and lead is still to be estimated but the prob-ability is low that lead should be of concern.Barium may occur in mineral water, bottled forsale, where the concentration exceeds the limitvalue by one order of magnitude. No data areavailable for piped drinking water.
Geographical differencesThis priority list is not equally valid for all Hun-garian regions. Some differences exist as someconstituents represent a health risk in only someparts of the country.
According to existing knowledge, arsenic occur-rences are confined to the region beyond the riverTisza (with the exception of the northern andsouthernmost part), and to that between the Tiszaand the Danube. Bacterial aftergrowth is charac-teristic of the major part of the region beyond theTisza river, and the flat regions laying on the rightbank of the Tisza, but it also occurs in otherplaces. Nitrate is found in drinking water in dis-tricts that use groundwater, first of all in Borsod,Veszprém, and Pest counties, but it may be foundalmost everywhere, except in the region beyondthe Tisza. Sodium, i.e. soft water, is characteristicon the Great Plain.
40
8. 2 Water Quality

Nitrite is the result of aftergrowth in warmer wa-ters. Chlorination byproducts may occur in regionssupplied by surface water, such as Szolnok and itssurroundings, the regional distribution system ofthe Mátra mountains, around Lake Balaton, andoccasionally in Salgótarján and its surroundings.
8. Future tasks
The prevention of primary pollution, that is, pro-tection of the water sources, is the task of the envi-ronmental protection and water authorities. Themost important actions of human health impor-tance are summarized in the following two tables.
41
Water Quality 8. 2

42
8. 2 Water Quality
Drin
king
wat
er
Loc
al
Prev
entio
n of
har
mfu
l he
alth
effe
cts
of a
rsen
ic i
n re
gion
s w
ithou
t ce
ntra
lw
ater
sup
ply
(loca
l w
ater
tre
atm
ent,
bottl
ed w
ater
sup
ply,
joi
ning
wat
ersu
pply
net
wor
ks);
Prot
ectin
g in
fant
s ag
ains
t nitr
ate;
App
lyin
g ne
w
tech
nolo
gies
an
dm
etho
ds i
n ca
se o
f so
ft w
ater
with
high
sod
ium
con
tent
; di
sinf
ectio
n,ag
ains
t ni
trite
pro
duct
ion;
sec
onda
rypo
llutio
n. D
evel
opin
g ne
w w
ater
sup-
ply
netw
orks
.
Reg
iona
l
Mea
sure
s ta
ken
agai
nst
seco
ndar
ypo
llutio
n;
Mea
sure
s ta
ken
agai
nst e
utro
phic
a-tio
n at
wat
erw
orks
: act
ivat
ed c
arbo
nfil
ters
etc
; Tr
eatm
ent
met
hods
for
sof
t w
ater
with
hig
h so
dium
con
tent
: tre
atm
ent
to in
crea
se h
ardn
ess
in c
ase
of s
pe-
cial
wat
er q
ualit
y;
Prev
entio
n of
alg
atox
ins
ente
ring
drin
king
wat
er,
met
hods
for
det
er-
min
atio
n (H
PLC
). In
vest
igat
ing
pos-
sibi
litie
s fo
r re
mov
al o
f to
xins
and
deve
lopi
ng te
chno
logi
es;
Dat
a co
llect
ion
and
eval
uatio
n on
nitri
te c
onte
nt in
wat
er s
uppl
y ne
t-w
orks
; Su
rvey
on
boric
aci
d co
nten
t in
drin
king
wat
er a
nd ta
king
nec
essa
rym
easu
res.
Nat
iona
l
Proh
ibiti
ng
prod
uctio
n of
PV
Cpi
pes w
ith le
ad c
onte
nt o
r mod
ifica
-tio
n in
tech
nolo
gy;
Lead
as
seco
ndar
y po
lluta
nt: i
nfor
-m
atio
n ca
mpa
igns
to li
mit
cons
um-
ptio
n (te
a m
akin
g)
from
he
ater
tank
s;
Surv
ey o
n le
ad c
onte
nt i
n w
ater
from
PV
C p
ipes
and
hea
ter t
anks
;Li
miti
ng u
se o
f pes
ticid
es in
pro
tec-
tion
zone
s an
d vu
lner
able
cat
ch-
men
t ar
eas.
Suita
ble
met
hods
for
mea
surin
g us
e of
pe
stic
ides
at
hydr
ogeo
logi
cal p
rote
ctio
n zo
nes;
Su
rvey
on
harm
ful h
ealth
effe
cts
ofar
seni
c in
im
porta
nt w
ater
sup
ply
syst
ems.
Task
s lis
ted
acco
rdin
g to
leve
l of a
ctio
n

43
Water Quality 8. 2
Bot
tled
and
recr
eatio
nal w
ater
Loc
al
Dev
elop
ing
prot
ectio
n of
su
rfac
ew
ater
use
d fo
r rec
reat
ion:
dat
a co
llec-
tion
on w
ater
qua
lity
and
equi
pmen
tof
free
bea
ches
;Im
prov
ing
hygi
enic
qua
lity
of b
each
-es
: eq
uipm
ent
(num
ber
of s
how
ers,
toile
ts, p
otab
le w
ater
, gar
bage
col
lec-
tion,
etc
.); fi
nanc
ial a
nd le
gal s
uppo
rt.
Reg
iona
l
Prot
ectio
n of
sur
face
wat
er q
ualit
y:ne
w ru
les f
or se
wag
e di
sinf
ectio
n at
catc
hmen
t are
as;
Effe
ct o
f ha
rmfu
l to
xic
alga
e on
swim
mer
s: d
evel
opin
g fo
reca
stin
gm
etho
ds;
Mea
sure
s ta
ken
agai
nst e
utro
phic
a-tio
n an
d di
min
ishi
ng t
he h
arm
ful
effe
cts
on b
each
es (
show
ers,
med
i-ca
l ser
vice
etc
.).
Nat
iona
l
Info
rmat
ion
syst
em a
nd le
gal b
ack-
grou
nd f
or c
onsu
min
g bo
ttled
wa-
ter:
labe
ling
educ
atio
n an
d ad
vice
toco
nsum
ers
(adv
anta
ges
and
disa
d-va
ntag
es)
in c
ase
of m
iner
al w
ater
with
spe
cial
con
tent
;Su
rvey
on
bottl
ed p
otab
le a
nd m
in-
eral
wat
er o
n th
e m
arke
t;Pr
omot
ing
use
of re
cycl
ing
syst
ems
in s
wim
min
g po
ols;
Dev
elop
ing
met
hods
for
han
dlin
gan
d di
sinf
ectio
n of
bat
hing
wat
er in
case
of t
herm
al w
ater
(tria
l of c
hlo-
rine
diox
ide
or q
uate
rnar
y am
mon
i-um
or
ozon
e; f
iltra
tion
thro
ugh
diat
oma
earth
); po
ssib
ilitie
s an
dlim
its o
f use
.
Task
s lis
ted
acco
rdin
g to
leve
l of a
ctio
n

1. Situation analysis
Traffic and industrial activity are considered to bethe most significant noise sources, but many ofamusement places, building machinery, as well asmachines and devices used in the households andother – justified or unjustified – human activitiesare also important. The last three groups ofsources cause noise first of all in buildings and theliving environment.
Noise from road trafficToday about 50% of the population are disturbedby noise from road traffic. Especially along mainroads in the cities a significant number of inhabi-tants are exposed to noise exceeding limit values,thus being harmful to health. Few measurements,performed in a uniform way, are available on thenoise load from road traffic. However, the fewexisting data indicate an unfavourable situation allover the country. (Fig. 8. 3/1) The noise load onfacades of buildings along main public roads is70–83 dBA in daytime and 60–75 dBA at night,compared to the limit values of 65 dBA and 55 dBArespectively. When windows are kept shut thenoise is reduced by 20–25 dBA on the average.
Noise from railwaysNoise from railways has an impact on much small-er population groups but the character of the noisemay be more disturbing. There are no available
statistics on the extent of this noise problem. Thenoise level outside buildings – being 50 m away inthe protection zone – may be 70–85 dBA when atrain is passing. Sound signals from trains aremuch louder and give rise to complaints, first ofall at night.
Noise from air trafficNoise from air traffic has generally been limited tothe surroundings of the Budapest-Ferihegy inter-national civil airport. For decades this has been adominant problem around the airport. In the “innerzone” the noise load exceeds 75 dBA, in the mid-dle zone it is 70–75 dBA and in the outer zone thedaytime noise load is 65–70 dBA. The noise frommilitary air traffic is difficult to measure and sonicbooms frequently add to the noise nuisance.
Business activity with small aircraft has beenincreasing in parallel with the economic changes.This activity is taking place in the low airspaceclose to human settlements and resort areas.Hardly any measurements of the effect of thisactivity exist but it results in many complaints.The resumed use of the former Soviet military air-ports has also given rise to complaints.
Noise from industrial and service facilitiesIn Hungary the noise from industrial and serviceactivities disturbs about 5% of the inhabitants.According to present regulations only noise fromindustrial sources can be controlled. As a result of
44
Noise 8. 3
8. 3 Noise

the penalty system and the systematic inspectionscarried out by the authorities, the noise emissiondecreased to below limit values by 1991 in about40% of the industrial and service facilities in ques-tion. In recent years – due to the declining pro-
duction of large plants, the privatisation process,the growing number of small enterprises and thedelegation of power to local authorities – the situ-ation has been unclear. More and more smallenterprises are operating in buildings situated inhousing areas, where they cause noise problems.
Public complaints of the disturbing noise com-ing from cultural, sports and entertainment activi-ties are also increasing. These activities are typi-cally of a local character and their control is underthe jurisdiction of local authorities.
Noise from housing machinery and household equipmentAn increasing number of machines and equipmentare being used in housing estates and other pro-tected establishments.
There are no sufficient data available for theevaluation of the resulting noise problem.
Noise from in house human activitiesInsulation is an appropriate method for preventingnoise caused by common human activities insidebuildings. (Fig. 8. 3/2) Antisocial behaviour, wherethe person making noise does not take written and
unwritten rules into consideration, is a nuisancefor neighbours and gives rise to complaints. It isthe difficult task of the local authorities to try tosolve such problems.
2. Health effects
The effects of noise on human beings may be clas-sified as follows:
disturbance of sleep from around 20–30 dBA;psychological disturb and stress from around 25–40 dBA;disturbance of speech from around 40–50 dBA;impairment of hearing from around 85 dBA(long time exposure) and 120–130 dBA (sin-gle impulses);physiological effects.
In the case of environmental noise, the effects of thefirst three groups are relevant. Regular exposure tosuch noise levels may lead to neurological, circula-tory and digestive disorders, but the causal relation-ship cannot easily be recognised due to the effect ofmany other factors. Previously, hearing impairmentwas an occupational health problem. Nowadays itmay be caused by environmental noise as well, thatis, when young people regularly and for long peri-ods listen to loud music exceeding 85 dBA. Thismay affect 20–30% of young persons.
45
8. 3 Noise

3. Targets
As to noise load, the goal is to prevent further de-terioration, change the worsening trend and im-prove the situation.
These goals are listed below in detail:
Traffic born noise:Stop the continuous increase of excessivenoise and its spreading to protected zones;Start to decrease noise exposure in over-burdened places.
Noise from industrial and service facilities:Limit noise from new operations and stopnoise in protected areas; Start to decrease noise emissions from theexisting industrial sources.
Noise coming from sources within buildings:Establish general limits for emissionsfrom machinery;Begin sanctions against activities exceed-ing limit values.
Noise protection of buildings:Comply with requirements on insulationagainst noise in new buildings.
Noise coming from human behaviourEstablishing legislation and good practiceto reduce the problem;Process for immediate measures to betaken in case of disturbance.
4. Problems to be solved
National levelImprovement of economic, technical and legalregulations covering all fields of noise control inaccordance with regulations existing in theEuropean Union should be achieved. At the sametime, professional institutions and responsibleadministrative bodies must be strengthened so thatthe regulations can be enforced.
Regional levelNoise control along main traffic routes and rail-ways, and around airports close to human settle-ments should be organised. Sufficient expertise ofpublic health and environmental protectionauthorities should also be available to measure andevaluate noise related complaints.
Local levelThe control of small local point sources and theexpertise of local authorities should be improved.
5. Programmes in progress
Programmes directed at decreasing noise emissionCertain industrial products, according to specificregulations, should be tested for noise emission.However, such products are frequently sold with-out any prior testing. Limits exist on noise emis-sion from motor vehicles but compliance with reg-ulations is not checked.
Surveys and research on effectsSuch activities are, in principle, carried out by dif-ferent institutions. However, due to limited fundsduring the 1980s only “hot spot” problems have sofar been studied. Data are not being systematical-ly gathered and evaluated.
Programmes at international levelThere is a national obligation to harmonise theHungarian legal system with the EU regulations.Most directives fall under the jurisdiction of theMinistry for Industry, Trade and Tourism. Harmo-nisation of the relevant standards has recentlybeen slowed down because of the reorganisationof the National Office responsible for standardisa-tion and quality assurance.
6. Tasks to be performed
Practical operations, education, information, datacollection, necessary surveys and research, techni-cal and other types of regulation, are summarizedin the table below.
46
Noise 8. 3
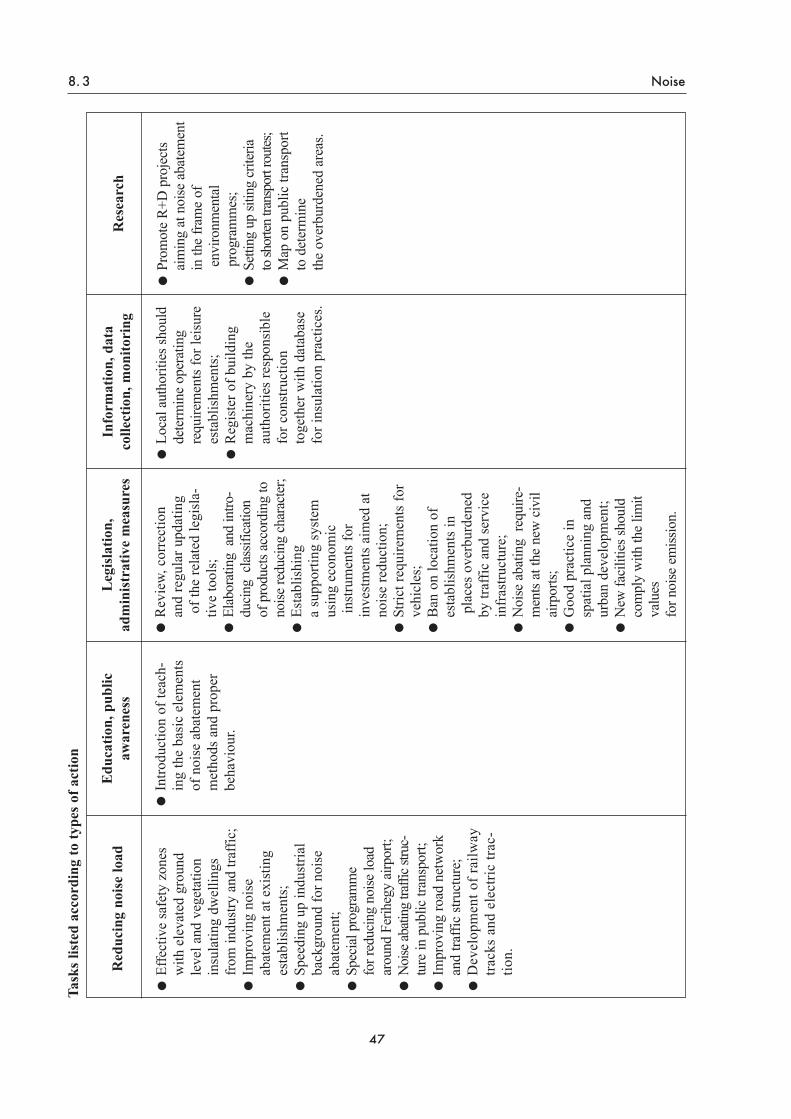
47
8. 3 Noise
Red
ucin
g no
ise
load
Effe
ctiv
e sa
fety
zon
esw
ith e
leva
ted
grou
nd
leve
l and
veg
etat
ion
insu
latin
g dw
ellin
gsfro
m in
dustr
y an
d tra
ffic;
Im
prov
ing
nois
e ab
atem
ent a
t exi
stin
g es
tabl
ishm
ents
; Sp
eedi
ng u
p in
dust
rial
back
grou
nd fo
r noi
seab
atem
ent;
Spec
ial p
rogr
amm
e fo
r red
ucin
g no
ise lo
adar
ound
Fer
iheg
y ai
rpor
t; N
oise
abati
ng tr
affic
stru
c-tu
re in
pub
lic tr
ansp
ort;
Impr
ovin
g ro
ad n
etw
ork
and
traffi
c str
uctu
re;
Dev
elop
men
t of r
ailw
aytra
cks
and
elec
tric
trac-
tion.
Info
rmat
ion,
dat
aco
llect
ion,
mon
itori
ng
Loca
l aut
horit
ies s
houl
dde
term
ine
oper
atin
g re
quire
men
ts fo
r lei
sure
esta
blis
hmen
ts;
Reg
iste
r of b
uild
ing
mac
hine
ry b
y th
e au
thor
ities
resp
onsi
ble
for c
onst
ruct
ion
toge
ther
with
dat
abas
efo
r ins
ulat
ion
prac
tices
.
Res
earc
h
Prom
ote
R+D
pro
ject
sai
min
g at
noi
se a
bate
men
tin
the
fram
e of
envi
ronm
enta
lpr
ogra
mm
es;
Setti
ng u
p sit
ing
crite
ria
to sh
orten
tran
spor
t rou
tes;
Map
on
publ
ic tr
ansp
ort
to d
eter
min
e th
e ov
erbu
rden
ed a
reas
.
Leg
isla
tion,
adm
inis
trat
ive
mea
sure
s
Rev
iew,
cor
rect
ion
and
regu
lar u
pdat
ing
of th
e re
late
d le
gisl
a-tiv
e to
ols;
El
abor
atin
g a
nd in
tro-
duci
ng c
lass
ifica
tion
of p
rodu
cts a
ccor
ding
tono
ise re
duci
ng c
hara
cter
; Es
tabl
ishi
ng
a su
ppor
ting
syst
emus
ing
econ
omic
inst
rum
ents
for
inve
stm
ents
aim
ed a
tno
ise
redu
ctio
n;St
rict r
equi
rem
ents
for
vehi
cles
; B
an o
n lo
catio
n of
esta
blis
hmen
ts in
plac
es o
verb
urde
ned
by tr
affic
and
ser
vice
infr
astru
ctur
e;N
oise
aba
ting
requ
ire-
men
ts at
the
new
civ
ilai
rpor
ts;
Goo
d pr
actic
e in
sp
atia
l pla
nnin
g an
dur
ban
deve
lopm
ent;
New
faci
litie
s sho
uld
com
ply
with
the
limit
valu
es
for n
oise
em
issio
n.
Edu
catio
n, p
ublic
awar
enes
s
Intro
duct
ion
of te
ach-
ing
the
basi
c el
emen
tsof
noi
se a
bate
men
t m
etho
ds a
nd p
rope
rbe
havi
our.
Task
s lis
ted
acco
rdin
g to
type
s of a
ctio
n

1. Situation analysis
Hungary’s territory is 93,030 sq km, 85.6% ofwhich is used for agriculture and the rest is occu-pied by settlements, industrial units, etc. It is ofutmost importance that the fertile soil be protectedfrom contamination.
Agricultural landsUntil 1988 fertility of soil and nutritive supplywere analyzed every third year by a unified labo-ratory network working under the direction of theMinistry of Agriculture. Metals were determinedonly as nutritive or essential microelements. Theresults cannot be compared to the limit values ontoxic metals used in other countries.
A monitoring system (Monitoring System of SoilProtection) was introduced in 1991 for regular assayof the most important toxicants at 1,236 locations.Toxic elements have been assayed and a completeinventory is being prepared. A similar activity is goingon for measurements of pesticide contamination on101 locations and the results will be available shortly.
Generally, the quality of soil is good and the pes-ticide content – due to decreasing use – can beconsidered low.
Point sources of contamination, such as pesti-cide depots and industrial pollution, should beassessed and evaluated. Toxic heavy metal con-centrations in soil are quite low as well.
Nonagricultural areasThese areas include industrial places, settlements,and road traffic surroundings.
Considerable contamination resulted from someprevious malpractice of waste disposal and theassessment of these areas is under way. The mostimportant contamination includes toxic metals(e.g. lead and cadmium), hydrocarbons (oil, tar,etc.) especially in military camps.
Abandoned industrial sites, inadequate wastedisposal, waste water treatment and storage of rawmaterials have caused soil contamination. Pollutedareas can be found inside and outside the settle-ments, where toxic metals and different organiccompounds – resulting from special technologies– constitute the highest danger.
Traffic is considered to be a significant source ofsoil pollution, mainly along the public roads and
the streets inside settlements. Lead and polycyclicaromatic hydrocarbons are the most importantpollutants. The disposal of solid and liquid house-hold wastes is not solved properly in many areas.
Overall assessment of contaminated areasA nationwide qualitative and quantitative surveyhas recently been launched by the Ministry for En-vironment and Regional Policy to assess the con-taminated areas; first of all the heavy metal contentof the soil is to be analyzed. A survey on the aban-doned military sites has been carried out and reme-diation plans elaborated. Based on the data of theNational Public Health Service and the Environ-mental Inspectorates, a joint database is to be set up.
2. Health effects
It is generally recognized that health effects of soilcontamination are very difficult to establish andascertain. So far, there is no indication that large-scale deleterious health effects have occurred inHungary due to soil contamination.
There are hardly any data on health damagecaused by point-, line- or patch-like soil pollutionsources. No quantitative analysis can be carriedout using the results of the available environmen-tal epidemiological studies. The available studieson soil pollution do not deal with the health statusof the population living in the area affected.
3. Goals to be achieved
Continuation of the assessment of pollutedareas and setting up a joint database;Identification of the endangered popula-tionin selected pilot areas by environmen-tal epidemiological methods;Further assessment of the already existingpriority areas;Proposal for actions to remedy areas withspecial health effects;Increase public awareness and encouragepublic participation in management of soilquality;Utilization of the experience gained at pilotsites for evaluating results in Hungary andother countries taking part in the WHOprogramme.
48
Soil Quality and Wastes 8. 4
8. 4 Soil Quality and Wastes

4. Problems to be solved
Comprehensive legislation relating to soil asan element of the environment and its pollu-tion;Establishment of a harmonized data base forassessing all contaminated areas, utilizationof advanced technology of the GeographicInformation System (GIS) for assessingcomplex health effects;Assessment of contamination in relation towater basins and raw water reservoirs;Extension of the existing studies on uptakeof toxic contaminants by edible plants andassessing their effects;Requirements for licensing and using chem-icals in agriculture are to be reviewed due tothe changes in ownership and the increasedknowledge in this field;Introduction of limitations on land use ofarable lands together with the compensationpaid to the owners.
5. Existing programmes
The Ministry for Environment and Regional Policystarted a long-term programme to study the aban-doned contaminated areas. In the frame of this pro-gramme a medium-term proposal for remediationof contaminated areas, determination of limit val-ues and legislation is to be elaborated. Limit valuesfor soil pollutants refer to ground water pollutionlevels until the special act on soil protection comesinto force. (Protection of arable land is providedfor by Act LV of 1994, and the limit values for uti-lization of waste water and sewage sludge are offi-cially used for soil pollution).
6. Further objectives and conditions for development
Based on a unified data base the particularlycontaminated areas should be determinedand the size of the affected population ana-lysed;Ensuring availability of data and sharing theinformation among relevant parties;Further development of human exposureassessment models, risk assessment andmanagement techniques;Ensuring active participation of health andenvironment authorities in assessing andsolving the problems;Cooperation among the competent authori-ties and institutions in the field of environ-mental monitoring, data collection and pro-cessing;Ensuring the financial background for thepoints mentioned above.
49
8. 4 Soil Quality and Wastes

1. Situation analysis
Management of the increasing amount of waste isa problem in Hungary, as in other countries. Thequantity of waste generated in Hungary amountedto 123 million tons in 1995. The amount of com-munal waste, hazardous waste and industrialwaste was 27.1, 4.9 and 91 million tons, respec-tively.
Government Decree No. 102 of 12.07.1995 ondisposal and utilization of hazardous waste regu-lates the transport, import and export of hazardouswastes. Measures to be taken to prevent environ-mental pollution and classification system are alsoincluded in the Decree.
Communal wasteRegular collection and disposal of municipal wasteis provided for about 75% of Hungarian house-holds. In towns this proportion exceeds 90%.However, less than 50% of the liquid waste is col-lected. More than 2,700 disposal sites are known.70% of these are not suitable, while only 10% canbe regarded as safe. Another serious problem is thenature of the disposed waste – some sites still con-tain previously deposited toxic materials.
The recultivation of the abandoned waste de-posits is not solved. There is only a single incinera-tor in the country for communal waste namely inBudapest, the capacity being 310,000 t/year, half ofthe total amount of the wastes from the capital city.
A major problem is the lack of treatment capac-ity for transported sewage water. Only 10% ofsewage is being treated, 20% is directed to com-munal drainage systems. The major part of thewaste water is drained directly into the soil with-out any treatment, causing serious contaminationto the soil and ground water.
Industrial wasteIndustrial processes generate large amounts ofwaste of potential environmental health concern.So far, about 50% has been recycled. The rest isstored in special depots.
Hazardous wasteThe quantity of hazardous waste was about 5 mil-lion tons in 1995, of which “red sludge” represents64%. Compared with other countries the amount
of hazardous waste is relatively high. There areregulations on the classification and characteriza-tion, further transport, disposal, etc. of hazardouswaste. Hungary has a low capacity for incinerationor other forms of disposal.
A special problem is the management of hospi-tal waste. The result of efforts to quantify andcharacterise the amount of waste generated in thehealth sector is shown in Fig. 8. 4/1.
For disposal of hazardous waste only one state-of-the-art incinerator in the town Dorog and oneadequate final storage facility in Aszód aera areavailable. At present six interim storage sites arebeing operated.
DatabasesIn order to deal with the mounting problems ofwaste management, it has to be ensured that all rel-evant information is available for the respective par-ties. This involves: inventory of communal wastedeposit sites, existing and old ones; the inventory ofhazardous wastes should be updated; hospital wastemanagement has recently been reviewed and will becorrected; questionnaires on industrial waste havebeen sent to more than 7,000 firms but the evalua-tion is still under way.
At the National Public Health Service the com-munal waste and waste water deposits, incinera-tors, storage sites for hazardous wastes and animalcarcasses, and other source of pollution are regis-tered.
Abandoned and operating waste landfills havebeen surveyed all over the country by the Hunga-rian Geological Service. Data on hazardous wastesare collected by the Ministry for Environment andRegional Policy.
Hospital wastes were surveyed twice but thedata are not suitable for evaluation and planning.Various ministries continue to collect data for spe-cial purposes according to different criteria.Therefore it is essential that a joint and unifieddatabase be established as soon as possible.
2. Health effects
The assessment of the immediate health conse-quences of the exposure to waste is as difficult asin the case of soil contamination. Long-term pros-pective and retrospective studies are needed to
50
Soil Quality and Wastes 8. 4
Wastes

substantiate any health effects. National and inter-national data suggest that an increased incidenceof allergic diseases, increased cancer mortalityand decreased birth weight may be found in settle-ments in the vicinity of waste dumping sites. InHungary no epidemiological survey on the impactof waste deposits has been carried out yet.
3. Goals to be achieved
Systematic analysis of health effectsaround waste dumping sites, establishmentof cause – effect relationships;Establishment of comprehensive databas-es and creation of a complete inventory;Promote environmental health policy withregard to decreasing the amount of waste;Better management of hospital wastes, i.e.selective collection, characterization, anddisposal;Elaboration of programmes to reduce soiland water contamination coming from un-controlled deposits.
4. Problems to be solved
A unified database should be set up. Theexisting data on waste disposal and landfills,taking into account the sites abandoned be-
fore 1982 as well, are to be processed, revie-wed and corrected. Waste load is to be identi-fied in the counties and regions;A classification system should also be estab-lished for correct prioritization, consideringthe affected populations, the endangered rawwaters and reservoirs;Proper risk assessment procedures should beimplemented for managing the potentialhealth effects and for remediation activities;Concerning the institutional background, therole of public health services and the envi-ronment protection inspectorates should bestrengthened in monitoring, regulating anddecisionmaking processes;As a specific problem, an effective hospitalwaste management system should be imple-mented, which would incorporate the selec-tive collection, storage and disposal of haz-ardous wastes from health institutions;Work environment conditions in relation tohandling waste should be studied and regu-lated;
The complex system of reducing the amountof waste, selective collection, storage, treat-ment and disposal of all wastes should beincorporated into national programmes;
51
8. 4 Soil Quality and Wastes

The industrial, institutional and financialbackground must be developed for wastecollection, disposal and utilization;Deposits of untreated waste water are to beliquidated and provision should be made forproper municipal waste water treatment.
5. Ongoing programmes
New legislation on hazardous wastes cameinto force and a new decree is being elabo-rated for the export and import of industrialwastes;An overall regulation on municipal solidwastes (under the PHARE programme) isbeing formulated;The Ministry of Industry, Trade and Tourismis carrying out a survey on utilization ofwastes;The regulation on environmental productcharges is to be continued, setting up a finan-cial fund for supporting waste disposal andutilization; Elaboration of a concept for treating hospitalwastes is under way in Budapest; Action programmes have been organised inseveral settlements for selective collection ofmunicipal waste.
Duties of the public health institutionsThe unified database is to be corrected;Identification of the potentially exposed pop-ulation in geographic and regional terms;Risk assessment using quantitative modelswith special consideration to the priority list;Model regions are to be selected for epide-miological studies;Close cooperation between the institutions ofthe National Public Health Service and theEnvironmental Inspectorates;Regular health control and exposure mea-surements have to be carried out amongworkers occupied in waste management.
The most important actions are listed in the fol-lowing tables.
52
Soil Quality and Wastes 8. 4

53
8. 4 Soil Quality and Wastes
Goa
ls
Was
te re
duct
ion;
M
oder
niza
tion
of w
aste
disp
osal
;R
emed
iatio
n of
co
ntam
inat
edar
eas;
Mod
erni
zatio
n of
leg
isla
tion
onpe
stic
ides
and
ferti
lizer
s;
Surv
ey o
n im
pact
s of
pol
lute
dso
il on
the
food
cha
in a
nd a
qui-
fers
;Sa
fety
mea
sure
s fo
r en
terp
rises
in t
he f
ield
of
was
te m
anag
e-m
ent;
Tech
nolo
gica
l an
d te
chni
cal
tool
s an
d de
vice
s fo
r re
duci
ngco
ntam
inat
ion
at d
ispo
sal s
ites;
Trea
tmen
t of
sec
onda
ry w
aste
sfr
om in
cine
rato
rs;
Prio
rity
list f
or so
il re
stor
atio
n at
natio
nal l
evel
;M
odel
regi
on fo
r rem
edia
tion
ofso
il an
d st
artin
g ep
idem
iolo
gica
lst
udy;
Red
ucin
g ris
k in
the
field
of
en-
viro
nmen
tal
heal
th r
elat
ing
toex
istin
g so
il co
ntam
inat
ion.
Info
rmat
ion,
res
earc
h
Usi
ng e
xper
ienc
e fr
om W
HO
surv
eys
in s
tudi
es,
eval
uatio
nan
d ris
k as
sess
men
t;A
sses
sing
hea
lth r
isk
rela
ted
toso
il an
d gr
ound
wat
er c
onta
mi-
natio
n an
d w
aste
dep
osits
;C
ontro
l of
hos
pita
l w
aste
ma-
nage
men
t to
red
uce
emis
sion
from
inci
nera
tors
and
pre
vent
or
redu
ce h
ealth
dam
age.
Adm
inis
trat
ive
mea
sure
s
Elab
orat
ion
of li
mit
valu
es f
orso
il po
lluta
nts;
Esta
blis
hing
inf
orm
atio
n ce
n-tre
s an
d ad
viso
ry b
oard
s.
Edu
catio
n
Educ
atio
n of
farm
ers t
o us
e fe
r-til
izer
s an
d pe
stic
ides
in
a
way
that
pro
tect
s th
e en
viro
n-m
ent;
Usi
ng e
xper
ienc
e fr
om m
odel
actio
ns,
elab
orat
ion
of m
eth-
ods,
guid
elin
es a
nd m
odel
s.
Task
s lis
ted
acco
rdin
g to
type
s of a
ctio
n

54
Soil Quality and Wastes 8. 4
Nat
iona
l
Envi
ronm
enta
l cl
assi
ficat
ion
of p
rodu
cts
mad
e of
dan
gero
us m
ater
ials
; Pr
even
tive
mea
sure
s fo
r w
aste
dep
osits
and
inci
nera
tors
to p
rote
ct w
orke
rs;
Tech
nolo
gies
and
met
hods
for
dim
inis
hing
pollu
tion
from
was
te d
ispo
sal;
Rev
iew
of h
ygie
nic
limit
valu
es fo
r soi
l pol
-lu
tant
s;
Mod
erni
zatio
n of
rule
s fo
r usi
ng s
oil f
ertil
iz-
ers
and
pest
icid
es;
Educ
atio
n of
farm
ers o
n en
viro
nmen
t-frie
nd-
ly u
se o
f fer
tiliz
ers
and
pest
icid
es;
Dra
win
g up
a n
atio
nal
prio
rity
list
on s
oil
reha
bilit
atio
n;
Pilo
t pro
ject
s on
dim
inis
hing
soil
pollu
tion
atsp
ecia
l pla
ces;
R
epre
sent
ativ
e he
alth
sur
vey
in a
reas
pol
lut-
ed w
ith to
xic
mat
eria
ls;
App
licat
ion
of W
HO
exp
erie
nce
for
surv
ey,
eval
uatio
n an
d ris
k as
sess
men
t;Ex
ploi
ting
succ
essf
ul a
ctio
ns,
wor
king
out
guid
elin
es, m
etho
ds a
nd m
odel
s;
Esta
blis
hing
cen
tres
for
info
rmat
ion
and
advi
sory
inst
itutio
ns.
Loc
al
Trea
tmen
t of s
econ
dary
was
tes f
rom
diff
eren
tw
aste
dis
posa
l fac
ilitie
s;D
ecre
asin
g ex
posu
re o
f wor
kers
at w
aste
dis
-po
sal f
acili
ties;
Hea
lth r
isks
com
ing
from
em
issi
ons
of in
ci-
nera
tors
bur
ning
med
ical
was
tes.
Reg
iona
l
Hea
lth r
isk
com
ing
from
soi
l an
d gr
ound
wat
er p
ollu
tion
rela
ting
to w
aste
dep
osits
; En
viro
nmen
tal
heal
th r
isks
com
ing
from
prev
ious
soi
l pol
lutio
n;Ef
fect
of
pollu
ted
soil
on f
ood
chai
n an
dw
ater
reso
urce
s;Es
tabl
ishi
ng r
egio
nal
land
fills
for
sol
idw
aste
s an
d de
posi
ts f
or w
aste
wat
er d
is-
char
ges
com
ing
from
hum
an s
ettle
men
ts.
Task
s lis
ted
acco
rdin
g to
leve
ls o
f act
ion

1. Situation analysis
The working environment is the most dangeroussubenvironment. The health risk is higher by 1–3orders of magnitude than in the case of all otherkinds of subenvironments.
In Hungary a characteristic change has occurredin the number of enterprises due to the privatisa-tion. The number increased dramatically: therewere 45,000 registered enterprises in 1989 and900,000 in 1994. Besides the increased number ofenterprises, the number of employees working atorganised companies decreased.
The possible reasons for that are the large num-ber of firms with one person or a family and thehigh rate of unemployment.
As always, work still means a hazard endanger-ing the health and safety of employees. In Hun-gary there are 150–200 deaths per year owing toaccidents and 40,000–50,000 injuries at work andabout 1,000 people contract occupational diseasedue to harmful effects. The number of registeredaccidents is considered a low estimate since bothemployers and employees are interested to concealthe truth. Eliminating or reducing work riskrequire special knowledge (technical, medical,legal) helping to recognise the risk factors and toimprove the methods for averting them.
Background data All over the world about 120 million work acci-dents and 60–120 million new cases of occupa-tional diseases are registered per year. The numberof deaths owing to accidents at work is 200,000per year worldwide, meaning that – calculatingwith 230 working days – 800–900 people die atwork each day (ILO, 1994). In addition, properstatistics on death cases caused by occupationaldiseases are not available.
The number of such cancers may be high.According to the most moderate estimates (Dolland Peto, 1981) 4% of fatal cancer cases are ofoccupational origin. This means the death of tensof thousands of employees per year worldwide.
Besides accidents and occupational diseases,there are so called workrelated diseases as well.These are of multicausal character, caused – alongwith several others – by the working environ-ment, meaning that certain elements of the work-
ing environment increase the risk of some di-sease.
The effect of the working environment as a fac-tor increasing the risk of certain diseases or harm-ful to certain populations has already been studied,but the data on incidence and prevalence are ques-tionable in the case of diseases occurring at work.
Sources and hazards of pollutantsAll technologies can be considered polluting in awider sense. Parameters of work environment aremainly unfavourably influenced but in somecases the effects can impact on the home environ-ment as well.
Work load, pathological and stress factorsWorkers are affected in one respect by physical,psychological and mental burdens and in otherrespects by numerous pathological factors (physi-cal, chemical, biological, ergonomical, psychoso-cial) coming from these work environment. Theinteraction between the two kinds of effects andthe genetically and anthropometrically determinedindividual is called stress. The basic task is to keepstress at an optimal level which is also very impor-tant in preventing harmful effects at work.
2. Health effects
DiseasesIn Hungary the number of work accidents andoccupational diseases are decreasing year by year.In 1989 the registered number of accidents (workand road together) was 81,310, and occupationaldiseases 1,424, in 1994 the number of accidentswas 35,919 and occupational diseases 531. In1995 there were 33,491 accidents and 829 occu-pational diseases.
The cause of the decreasing trend is unfortunate-ly not due to improvement of the working environ-ment. Since 1989, the beginning of the economic,social and political changes, the structure, produc-tivity and number of employees have drasticallychanged owing to privatisation and the transition toa market economy. The incidence of accidents andreported illnesses is mainly associated with theoperation of the Hungarian economy.
In 1994 42 cases of occupational toxicosis, a spe-cial form of occupational disease, were registered.
55
Work Environment 8. 5
8. 5 Work Environment

The number of deaths due to occupational accidents The number of fatal accidents was 324 in 1994and 176 in 1995.
Deaths due to occupational diseases are sporad-ically registered in Hungary and the number ofrecognised cases – even in case of lung cancercaused by radiation – cannot be considered as thetotal.
3. Goals to be achieved
The basic task is to regulate the domain ofthe work environment and harmonisewith the legislation of the EU. The key ele-ment in prevention of occupational dis-eases and health promotion is to ensurework safety and an occupational healthservice for all employees. The goal is toensure all the requirements for effectiveoperation thereof. About 80% of the casesof occupational diseases are recognizedand reported by doctors working in occu-pational health services;The second important task is to improvethe quality of the work environment andachieve the optimal level of work load andstress. This problem has got priority in thelegislation as well as all the other tasksmentioned above. From a practical pointof view these two problems should be equal-ly and simultaneously prioritised;It is also necessary, that administrativemeasures be unified and strict;To ban or restrict substances harmful tohealth in Hungary in accordance with thepractice in the European Union and inharmony with the decisions of OECD.
4. Harmonisation of legislation,regulation and supervision
Amendment of the Act on work safety and relatedlegislationThe decree of the Minister of Labour No 4 of26.12.1993 for implementation of the Act XCIII of1993 on work safety should be amended to deter-mine the obligations of the enterprises to carry outrisk assessment and on the other hand, to approachthe legislative system existing in the EuropeanUnion. The Act should be amended to set up a uni-
fied organisation in the field of occupationalhealth and safety.
Harmonisation of legislative tools with the EUdirectivesThe acceptance of the following EU directivesshould be promoted:
In the frame of responsibility of the Ministry ofWelfare:
Council Directive 90/679 EEC on protectionof workers against biological substances;Council Directive 90/394 EEC on hazard ofcarcinogens.
In the frame of responsibility of the Ministry ofLabour
Council Directive 89/654 EEC on the mini-mum occupational health and safety require-ments at work;Council Directive 89/655 EEC on the mini-mum occupational health and safety require-ments of tools at work;Council Directive 92/57 EEC on require-ments at temporary working places of con-struction work;Council Directive 92/58 EEC on occupation-al health and safety notifications used atwork places.
In the frame of the joint responsibility of theMinistries of Labour and Welfare
Council Directive 89/391 EEC on introduc-tion of rules for ensuring occupational healthand safety;Council Directive 89/656 EEC on occupa-tional health and safety requirements of per-sonal safety devices;Council Directive 89/686 EEC on approxi-mation of legislation on personal safetydevices;Council Directive 90/269 EEC on the mini-mum requirements of manual materials han-dling.
In the frame of the joint responsibility of theMinistries of Labour, Welfare, and Industry, Tradeand Tourism
Council Directive 90/270 ECC on the mini-mum occupational health and safety require-ments at work in front of a screen.
56
8. 5 Work Environment

Ratification of ILO conventionsand recommendations
ILO 170 “Convention on work with chemi-cal substances”;ILO 174 “Convention on the prevention ofindustrial catastrophes”;National occupational health and safety leg-islation on work with chemical substances;National legislation of work with hazardoussubstances.
Establishing a uniform control system for occupa-tional health and safetyAn organisation of inspectorates should be estab-lished with up-to-date knowledge of legislationand available inventory of all work-places andworking conditions. The occupational health andsafety inspectorates should know all the activities,hazards, exposures, work loads, and risks. Thesedata form the basis for prevention and intervention.
The task is to elaborate, model and establish anintegrated practice for the occupational health andsafety control system. The following aspects andmethods should be taken into consideration:
The strategy of supervision depends onthe methods for exploring the sources of haz-ard and forecasting risks; and elaboration of sampling methods for allworking processes and areas, taking intoaccount the total working time and the work-ers exposed.
The supervising process consists of three phases:preparation (data collection, information), inspec-tion at the site, and evaluation and recommenda-tions.
In all three phases records and reports are essential.
Different modules are to be worked out:Aspects of the general supervision of the en-terprise and requirements relating to tech-nologies;Health and safety facilities (facilities, protec-tive devices);Submodules of the pathological factors char-acteristic to a certain technology (sourcesand intensity of exposure, workers exposed,preventive measures).
5. Improvement of occupational health service
The task is composed of three parts:quality assurance;education;information system.
Quality assuranceIn Hungary the new system of occupational healthstarted in 1995, based on the Act on labour safetyof 1994. The act makes it obligatory for all enter-prises to ensure occupational health service forworkers in employment. A Government decreeand a decree of the Minister of Welfare regulatesthe organisation and operation of this service.
Before the Act came into force, the basic occu-pational health activities ceased to be financed bythe Health Insurance Fund; the expenses are to becovered by the employers who are responsible forensuring safe work conditions. This means ineffect the privatisation of occupational health ser-vices, which are employed directly or hired by theenterprise.
Quality assurance has high priority in this situa-tion to determine minimum standards and set up acontrol system.
EducationAt the beginning of 1995 about 60% of employeeswere provided with an occupational health service.
Due to the shortage of doctors specialised inoccupational health, other experts (such as inter-nists, oxyologists, general practitioners) have beenlicensed to provide the service with the conditionthat they pass a special exam by 31.12.1998. Forthem and the specialised doctors – and even occu-pational nurses –, education and postgraduatetraining are highly important.
In order to carry out the task, accredited centresare to be set up to teach occupational health – in-cluding toxicology, ergonomy, psychology, etc. –to meet the needs of the different branches of theeconomy.
Information system and service To facilitate access to information on occupation-al health, utilisation of the possibilities of the In-ternet is highly desirable.
57
Work Environment 8. 5

6. Scientific research
Epidemiology and prevention of cancer of occupational originStudies of cancer of occupational origin should begiven high priority in scientific research.
On the one hand cancer stands in second place onthe list of causes of death in Hungary, and on theother hand according to international data 80–90%of all malignant tumours are caused by environ-mental factors. Even by moderate estimates, 4% ofcancers are of occupational origin. In spite of thisfact, in Hungary no more than 50 cases are consid-ered to be of occupational origin among the 30,000cancers deaths per year compared to the minimumof 1,200 cases, that could be expected.
Research work should concentrate on the following:How much higher is the risk of canceramong workers than the population livingnear or further from the factory?How does the risk of cancer change with thedecrease of exposure and what is the expect-ed risk of the present exposure among work-ers and the population living nearby?Are the workers and the nearby populationaware of the danger arising from the activity?
In the first two years of investigation, asbestos andvinyl chloride are the centre of the research work andtherefore the sites of the survey are the following:
a factory producing asbestos slate;a factory producing polyvinyl chloride (PVC);dwellings within 2 km of the factories;settlements at least 20 km away from the fac-tories as control areas.
Development of samplers suitable for measuringexposure of certain groups of workers or certainbranches of industryThere is no appliance capable of providing a largevolume of data at low cost in a short time. There isonly an experimental appliance suitable for serialproduction if financed. The samplers should com-ply with both the technical and occupationalhealth requirements, so the experiments have toconcentrate on the following:
to produce a mixture of air pollutants withregulated temperature, composition, storage,humidity and space, and connected to an ap-pliance extracting and analysing the sub-stances collected;to define the criteria for selection of thematerial of the sampler with regard to theactive component and the substance exam-ined; sampling speed; storage time; and effi-ciency of extraction.
The experimental appliance should be tested inoperation in situ and modified according to theresults before serial production.
Elaboration of personal samplersThe appliance should be suitable for both indoorand outdoor measurements. Measurement of sus-pended fibres should include MMMF as well andan evaluation system complying with the interna-tional standards.
58
8. 5 Work Environment

1. Situation analysis
Chemical safety comprises all aspects of produc-tion, use and elimination of harmful and danger-ous chemicals which might cause deleterious ef-fects on human health or the environment.
Human beings are exposed to hazardous chemi-cals during production, packaging, transport, mar-keting, use and elimination (disposal) of harmfulchemicals. Also, the environment might be con-taminated during all these processes which in turnmight lead to deterioration of the ecosystem, andagain secondarily, affect human health.
Chemical safety received much attention duringthe UNCED Conference in Rio de Janeiro, in 1992.The decision of the conference outlines the mostimportant requirements for chemical safety andtraces guidelines for developing programmes toachieve specific targets and goals:
The document suggests actions in six areas:Extension and acceleration of an internation-ally harmonised assessment of chemical risks;Harmonisation of classification and labellingof hazardous chemicals;Exchange of information on hazardous che-micals and risks;Initiation of risk reduction programmes;Development of national capacities for man-agement of chemicals;Improvement of control measures for stop-ping illegal international marketing.
As a member of the OECD, the Hungarian gov-ernment is involved in an ongoing process to har-monise the present legislation with OECD requir-ements. The present Hungarian legislation alreadycontains many important elements of the OECDinstruments, and envisaged new regulations willbe harmonised with those instruments.
National perspectiveChemical industry is an important part of theeconomy, most prominent the production of petro-chemicals, synthetic materials, basic chemicalsand pharmaceutical products. Centers of chemicalindustries are located in densely populated areas(cities) which underlines the risk of considerableemissions and accidents during production ortransport (Fig. 8. 6/1).
Important condition for chemical safety is the safehandling, packaging, transport and disposal ofchemicals. Legal instruments are needed to meetthese conditions.
For effective prevention of environmental con-tamination, inventories of pollution sources, emis-sions and transport should be established. Also,surveys of already polluted areas are needed inorder to initiate risk reduction programmes. Che-mical safety is of relevance to the whole popula-tion but with considerable differences in exposure.Especially workers in industry and agriculture areat risk. Consumers are voluntarily or involuntarilyexposed to chemicals that may involve health risks.
2. Health effects
The major determinants of the effects of chemicalson the health (and well being) of the individual are:
the nature of the chemical per se; the duration of time over which the chemicalinteracts with the individual; the quality of the chemical present;the possibility of chemicals acting togetherto cause effects that may be additive, syner-gistic, antagonistic, or independent is alwayspresent.
Acute poisoningThe traditional scope of the regulations of poisonsand hazardous substances has been the prevention ofpoisoning in human beings. Acute poisoning maynot today be a problem of great health significancebut serious problems may still persist in subgroupsof the population, for example small children.
The risk of acute poisoning is particularly highfor workers in the chemical industry and in agri-culture due to exposure to pesticides and otherchemicals. Due to insufficient reporting the exactnumber of acute poisonings is not known. Fortu-nately, cases of fatal poisoning in the chemical in-dustry are rare. In 1994, the number of deaths inchemical industry from poisoning were 3.3 per100,000 workers.
The risk of acute poisoning, however, also existsin households. Routine statistics on morbidity arenot available. Household gas presents a risk inmany homes and deficient storing of chemicalproducts frequently exposes small children to the
59
Chemical Safety 8. 6
8. 6 Chemical Safety

risk of poisoning. A recent large scale intoxicationcaused by contamination of red pepper with leadand chromium underlines the importance of chem-ical safety to the general population.
Chronic health effectsAllergic reactions represent a difficult field in thecontrol of chemicals. The morbidity scene is con-stantly changing as even less sensitising compoundswhen used by a sizeable population may eventual-ly lead to reactions such as contact dermatitis. It isnot possible to protect all allergic individualsagainst any specific chemicals to which they havebecome sensitised.
Especially the risk of cancer development fol-lowing exposure to chemicals has been a drivingforce behind the strengthening of regulations inindustrialised countries. The enormous increase inthe production and use of chemicals comparedwith the steadily rising cancer mortality is thebackground for the concern of some scientists thatthe majority of cancers might be due to chemicalcarcinogens in the environment.
In estimating the risk attributable to differentclasses of environmental agents, the firmest esti-mates relate to the effects of tobacco, alcohol andgeographical factors, while by far the largest esti-mates relate to tobacco and diet. Earlier estimatesby more conservative scientists have reckonedthat not more than 2–8% of all cancer deaths maybe attributed to occupational exposure. Even if theproportion of cancers that may be attributed tospecific hazards of occupation, pollution, the useof chemical products, medicines and medical pro-ducts are individually small, some of these haz-ards may be of great importance to sections of thepopulation on whom the risks are concentrated.
The chronic effects of chemicals occur first ofall in industrial settings. Special attention shouldbe paid not only to cancer but also the effects onreproductive organs. In Hungary, only 40–50 casesof cancer related to occupational exposure havebeen reported yearly. However, this figure doesnot reflect the actual situation, and a special sur-vey of cancers related to occupational exposureshould be initiated.
60
8. 6 Chemical Safety

3. Goals to be achieved
Protection of human health and environ-ment from deleterious effects of hazard-ous chemicals;Establishing legal, technical and other na-tional circumstances for prevention;Continuous control and survey of the po-tential effects of exposure to chemicals;Establishing programmes for remedyinghighly contaminated areas.
4. Problems to be solved
Establishment of an institutional frameworkfor chemical safety;Coordination of the highly complex issuesrelated to chemical safety is of utmost im-portance. A commission for chemical safety,comprising high level representation of allrelevant ministries could be operational in allissues related to production, marketing, useand disposal of chemicals. This forum coulddeal with risk reduction programmes etc;International requirements for harmonisationof legislation have high priority, especiallyconcerning OECD and EU regulations;An optimal solution would be the establish-ment of an authority for all aspects of chem-ical safety (“Chemical Inspectorate”). Thisbody should deal with theoretical, legal andpractical aspects of regulating hazardouschemicals;A new Act on Chemicals should be created,which would cover all aspects of production,packaging, labelling, transport, use and dis-posal of hazardous chemicals. The followingtable lists a number of activities relating tochemical safety.
61
Chemical Safety 8. 6

62
8. 6 Chemical Safety
Loc
al
Acc
redi
ting
labo
rato
ries
mak
ing
mea
sure
-m
ents
, com
plyi
ng w
ith G
LPre
quire
men
ts;
Star
t an
d co
ntin
uatio
n of
pro
gram
s on
ris
kab
atem
ent,
dete
rmin
atio
n an
d co
ntro
l of
harm
ful c
hem
ical
s:
*Se
t up
lis
t of
che
mic
als
prod
uced
in
high
volu
me;
*In
form
atio
n ex
chan
ge o
n ba
nned
or l
imite
dch
emic
als;
*Ef
fect
s of
mer
cury
and
its
com
poun
dsbe
ing
harm
ful
to e
nviro
nmen
t an
d hu
man
bein
gs;
*D
imin
ishi
ng e
xpos
ition
of
lead
and
its
com
poun
ds;
*M
oder
atin
g ha
rmfu
l ef
fect
s of
cad
miu
man
d its
com
poun
ds t
o en
viro
nmen
t an
dhu
man
s;*
Prev
entin
g po
lych
lorin
ated
bip
heny
ls t
oge
t int
o th
e en
viro
nmen
t; *
Dim
inis
hing
eff
ects
of
poly
brom
inat
edfla
me
reta
rdan
ts;
*C
lass
ifica
tion
of c
ance
roge
n m
ater
ials
.
Reg
iona
l
Dev
elop
men
t of
educ
atio
n an
d re
sear
ch in
toxi
colo
gy a
nd e
coto
xico
logy
; Su
rvey
on
the
mos
t dan
gero
us m
ater
ials
tom
ake
up in
vent
ory
for c
ompo
unds
har
mfu
lto
env
ironm
ent a
nd h
uman
bei
ngs;
In
vest
igat
ing
effe
cts
on e
nviro
nmen
t, ris
kas
sess
men
t;Ec
otox
icol
ogic
al m
easu
rem
ents
and
eva
-lu
atio
n;
Setti
ng u
p su
itabl
e la
bora
torie
s;
Educ
atio
n of
exp
erts
; In
form
atio
n ex
chan
ge o
n ha
rmfu
l ch
emi-
cals
and
risk
s.
Nat
iona
l
Inte
rmin
iste
rial
Com
mitt
ee f
or d
ealin
g w
ithth
e co
mpl
ex p
robl
em o
f ch
emic
al s
afet
y.D
eter
min
atio
n of
task
s fo
r com
pete
nt a
utho
-rit
ies
wor
king
in th
is fi
eld;
Exte
nsio
n of
mea
sure
men
ts in
env
ironm
enta
lto
xico
logy
and
saf
ety;
Non
-clin
ical
mea
sure
men
ts i
n to
xico
logy
plan
ned
acco
rdin
g to
the
OEC
D g
uide
lines
and
Goo
d La
bora
tory
Pra
ctic
e fo
r m
utua
lac
cept
ance
of
data
in
gene
ral-
and
ecot
oxi-
colo
gy;
Prio
r In
form
ed C
onse
nt (
PIC
): ev
alua
tion
and
mut
ual n
otifi
catio
n on
ban
ned
or li
mite
dch
emic
als
in c
ase
of e
xpor
t: se
tting
up
PIC
Com
mitt
ee in
Hun
gary
; Se
tting
up
prop
er l
ist
on p
rodu
cts
of h
igh
prod
uctio
n vo
lum
e;
Ris
k de
crea
sing
pro
gram
s on
pest
icid
es: n
ewre
gist
ry s
yste
m, s
afe
usin
g, d
ispo
sal o
f pac
k-ag
es,
surv
ey o
n po
llutio
n of
gro
und
wat
er,
educ
atio
n of
use
rs,
mea
surin
g po
llutio
n of
food
stuf
fs;
Take
-ove
r an
d de
velo
pmen
t of
new
met
hods
in t
oxic
olog
y, e
duca
tion
and
postg
radu
atio
nof
exp
erts
, inf
orm
atio
n to
rise
pub
lic a
war
e-ne
ss, s
uppo
rting
rese
arch
in to
xico
logy
.
Task
s lis
ted
acco
rdin
g to
leve
ls o
f act
ion

1. Situation analysis
Although the road vehicle fleet grew continuouslyin the 80s, the number of road accidents involvinginjury more or less stabilised. The balance reachedcannot, however, be considered satisfactory. Yet itmay be considered as a certain achievement thatthe significant increase in the number of vehicles(and of the kilometres travelled) has not beenaccompanied by a growth in the accident rate. Thisrate, of course, must be evaluated in comparisonwith the change of traffic volume.
From 1988 the number of accidents involvinginjury and fatalities started to increase abruptly,and road accident deaths in 1990 exceeded all pre-vious levels. From 1990, both the number of roadaccidents and of persons injured or killed began todecrease. (Fig. 8. 7/1)
In 1991, the 12–13% decrease in road accidentsinvolving injuries and fatalities was accompaniedby a 5% lower road traffic volume. Consequently,the decrease in the number of accidents to someextent may be explained by the decline in traffic.
In 1992, a 3% traffic increase was registeredwhich partly may explain why accident figures didnot decrease that year.
In 1993, both accidents involving injury and thenumber of fatalities decreased markedly (by20–21%), although the volume of road traffic re-mained practically unchanged. Thus, this consid-erable improvement must be related to the consis-tently implemented road safety provisions andseries of measures taken in 1993.
Because of their impressive results the followingmeasures are worth mentioning:
introduction of the 50 km/h speed limit in-side builtup areas;mandatory use in daytime of headlights bymotor vehicles on motorways and mainroads outside builtup areas;mandatory use of installed seat belts in therear seats of passenger cars outside builtupareas;increased traffic control activity of the police.
In 1994, compared with the previous year, a smallincrease of the accident rate (6%) was experi-enced. It is estimated that a similar growth occur-red in the volume of traffic. In 1994, a total of1,562 persons died in road accidents (6.9% lowerthan the previous year).
In 1995, preliminary data show a discontinuityof the former favourable trend: the number of per-
63
Road Traffic Safety 8. 7
8. 7 Road Traffic Safety
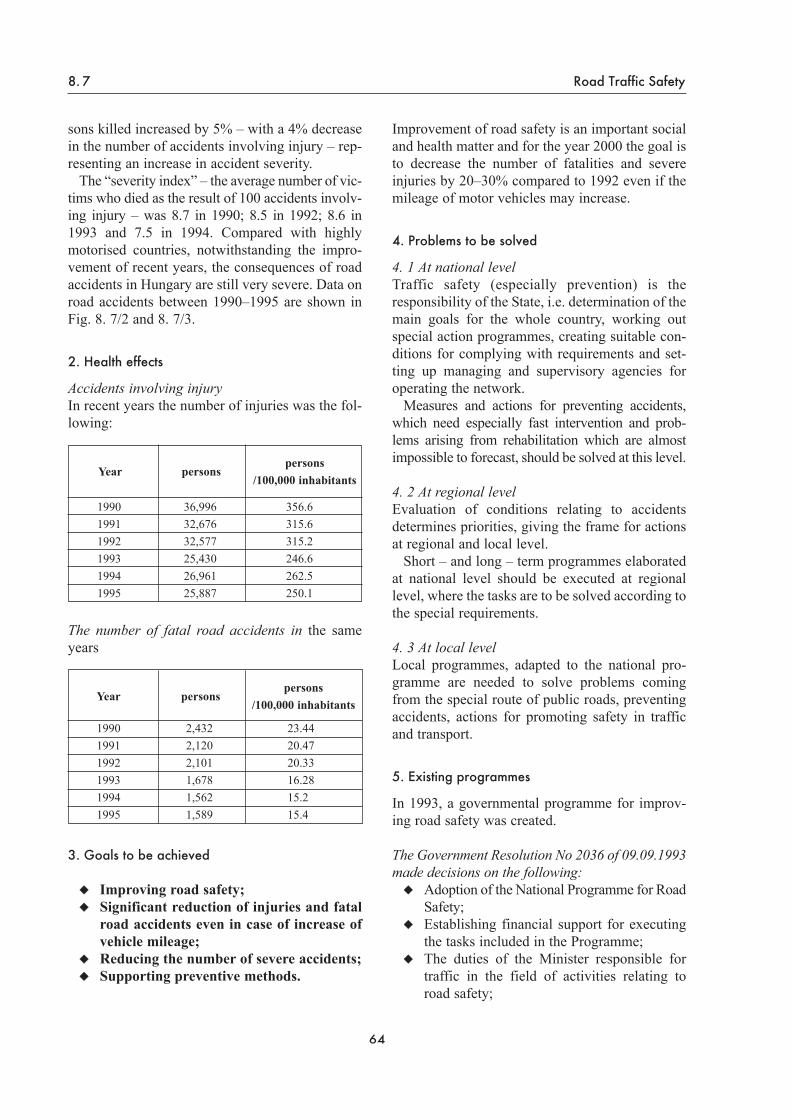
sons killed increased by 5% – with a 4% decreasein the number of accidents involving injury – rep-resenting an increase in accident severity.
The “severity index” – the average number of vic-tims who died as the result of 100 accidents involv-ing injury – was 8.7 in 1990; 8.5 in 1992; 8.6 in1993 and 7.5 in 1994. Compared with highlymotorised countries, notwithstanding the impro-vement of recent years, the consequences of roadaccidents in Hungary are still very severe. Data onroad accidents between 1990–1995 are shown inFig. 8. 7/2 and 8. 7/3.
2. Health effects
Accidents involving injuryIn recent years the number of injuries was the fol-lowing:
The number of fatal road accidents in the sameyears
3. Goals to be achieved
Improving road safety;Significant reduction of injuries and fatalroad accidents even in case of increase ofvehicle mileage;Reducing the number of severe accidents;Supporting preventive methods.
Improvement of road safety is an important socialand health matter and for the year 2000 the goal isto decrease the number of fatalities and severeinjuries by 20–30% compared to 1992 even if themileage of motor vehicles may increase.
4. Problems to be solved
4. 1 At national levelTraffic safety (especially prevention) is theresponsibility of the State, i.e. determination of themain goals for the whole country, working outspecial action programmes, creating suitable con-ditions for complying with requirements and set-ting up managing and supervisory agencies foroperating the network.
Measures and actions for preventing accidents,which need especially fast intervention and prob-lems arising from rehabilitation which are almostimpossible to forecast, should be solved at this level.
4. 2 At regional levelEvaluation of conditions relating to accidentsdetermines priorities, giving the frame for actionsat regional and local level.
Short – and long – term programmes elaboratedat national level should be executed at regionallevel, where the tasks are to be solved according tothe special requirements.
4. 3 At local levelLocal programmes, adapted to the national pro-gramme are needed to solve problems comingfrom the special route of public roads, preventingaccidents, actions for promoting safety in trafficand transport.
5. Existing programmes
In 1993, a governmental programme for improv-ing road safety was created.
The Government Resolution No 2036 of 09.09.1993made decisions on the following:
Adoption of the National Programme for RoadSafety;Establishing financial support for executingthe tasks included in the Programme;The duties of the Minister responsible fortraffic in the field of activities relating toroad safety;
64
8. 7 Road Traffic Safety
Year personspersons
/100,000 inhabitants
1990 36,996 356.61991 32,676 315.61992 32,577 315.21993 25,430 246.61994 26,961 262.51995 25,887 250.1
Year personspersons
/100,000 inhabitants
1990 2,432 23.441991 2,120 20.471992 2,101 20.331993 1,678 16.281994 1,562 15.21995 1,589 15.4

Setting up a Committee for the competent mi-nistries;Elaborating yearly action programmes adjus-ted to the financial possibilities.
In Hungary, passenger car drivers, first of allyoung males, are considered the principal targetgroup for road safety activities, due to their con-siderable role both in causing accidents and as theirvictims. Hence, the programme lists among themost urgent tasks the introduction of the penaltypoint system, and for young/novice drivers the useof the probation driving license period. (Fig. 8. 7/4)Since the main objective is decreasing the severi-ty of accidents, education and enforcement shouldalso concentrate on:
respect of the prescribed and safe speed limits;prevention of drinking and driving;a significant increase in the use of safety belts.
Road accidents – especially those caused by speed– have severe consequences, notably outside built-up areas. In 1994, 58% of road accident victims losttheir life outside builtup areas. In consequence, inthe future, speed control must be increased princi-pally on roads outside builtup areas. In the Govern-ment Programme’s implementation process, the de-velopment of the financing system has so far failed.Notwithstanding the weak financial background,annual action programmes were elaborated for1994 and 1995.
6. Future tasks
Tasks included in the National Road SafetyProgramme are to be regularly reviewed, takinginto consideration the situation of road safety.(This is reflected in the tasks set out in the yearlyaction programmes.) Measures taken for preventionare to be emphasised. This is a natural demand,because prevention is cheaper also in the field ofroad safety than the restoration of damage.
Human responsibilities are emphasised in thismatter, as they can have a substantial influence onroad safety even without major technical invest-ment. The following table lists tasks relating toroad traffic safety.
65
Road Traffic Safety 8. 7

66
8. 7 Road Traffic Safety

67
Road Traffic Safety 8. 7
Prac
tical
task
s (or
gani
zatio
n, c
ontr
ol)
Act
ivity
of t
he a
mbu
lanc
e se
rvic
e; im
prov
ing
spec
ial m
edic
al c
are
on th
e sp
ot b
y sh
orte
ning
arriv
al ti
me
incr
easin
g th
e nu
mbe
r of
am
bu-
lanc
e ca
rs a
nd d
evel
opin
g th
e ne
twor
k of
spe-
cial
, mob
ile e
mer
genc
y ca
re u
nits;
Impr
ovem
ent
of t
he a
mbu
lanc
e se
rvic
e to
trans
port
mor
e pa
tient
s by
hel
icop
ter;
Impr
ovin
g te
chni
cal p
ossi
bilit
ies a
nd st
aff f
orem
erge
ncy
resc
ue;
Cam
paig
ns to
forc
e re
spec
t of t
he s
afet
y re
g-ul
atio
ns o
n ro
ads,
regu
lar c
heck
ing
base
d on
loca
l pro
blem
s and
cau
ses o
f acc
iden
ts;El
abor
atin
g an
d in
trodu
cing
a “
poin
t sys
tem
”to
pen
alise
beh
avio
ur e
ndan
gerin
g ro
ad sa
fety
.
Info
rmat
ion
(edu
catio
n. tr
aini
ng, c
omm
unic
atio
n)
Reg
ular
info
rmat
ion
syst
ems s
houl
d be
wid
e-ly
int
rodu
ced
with
the
hel
p of
pub
lic a
ndco
mm
erci
al T
Vne
twor
ks;
Non
-pro
fess
iona
l firs
t aid
and
res
cue
shou
ldbe
im
prov
ed w
ith e
xper
t ed
ucat
ion
unde
rco
ntro
l and
org
aniz
ing
“ref
resh
er”
cour
ses.
Mea
sure
s tak
en b
y au
thor
ities
(te
chni
cal,
legi
slat
ive)
Intro
duci
ng d
rivin
g lic
ence
for
pro
batio
ntim
e fo
r yo
ung,
nov
ice
driv
ers
in c
onne
c-tio
n w
ith re
gist
erin
g fu
nctio
n of
the
pena
ltypo
int s
yste
m;
Poss
ibili
ties
for
repo
rting
acc
iden
ts a
re t
obe
dev
elop
ed,
such
as
tele
phon
e ne
twor
kal
ong
road
s w
ith h
igh
traffi
c de
nsity
(be
-si
des m
otor
way
s), C
B ra
dios
and
mob
ile te
-le
phon
es.
Task
s lis
ted
acco
rdin
g to
type
s of a
ctio
n

1. Situation analysis
Radiation dose from natural sourcesA thorough investigation was begun in the lateseventies for the assessment of the radiation doseof the population from various sources. Data ob-tained so far indicate an average of 0.34 mSv fromthe cosmic and 0.48 mSv from the terrestrial com-ponent of natural radiation. The average radiationdose is the same as all over the world, namely0.82 mSv/year, in the same way as the internal ra-diation dose from 40K assessed to be 0.18 mSvannually.
Among the manmade sources, the Paks NuclearPower Plant contributes only one thousandth(1/1,000) of the natural level.
Occupational and environmental exposureA well organized personal dosimetry system is inoperation covering 1,200 working places, approx.1.5 per thousand population. Based on the findingsobtained, the exposure did not exceed 10–15 percent of the occupational dose limit.
Despite this favourable situation, several problemshave still to be solved:
In the surrounding countries more and morenuclear establishments are operating quitenear the borders. Although in the opinion ofexperts the nuclear power plants are amongthe safest industrial establishments, the oc-currence of serious accidents at reactors cannot be excluded. Institutions monitoringradioactivity in the environment should mo-nitor for the background radiation, forecastcontamination and handle the consequences;Restoration of the environment contaminat-ed with radioactive substances due to urani-um mining is to be solved;Radioactive wastes of different activity lev-els, originating from the nuclear cycle andduring operation of industrial, health care,educational and other institutions should besafely deposited;A nationwide survey on indoor radon con-centrations from natural sources – causingsignificant radiation dose to the population –has been carried out only in dwellings. Thepreliminary survey of indoor radon concen-
trations must be continued and extended.The average value of 55 Bq per m3, however,might result in an annual dose of 2,5 mSv,approx. twice the world average value.
Radiation dose of the population from medicalapplications of ionizing radiationA project was started and has to be continued forthe assessment of the population dose from medi-cal applications of ionizing radiation. It is sup-posed that the resulting value may be higher thanthe European average and it is considered to be themost significant factor of the radiation dose fromartificial sources, among them medical X-rays anddiagnostic processes carried out with isotopes.More than 10 million X-ray and about 3 millionlung screening examinations are carried out in thecountry per year. It can be determined during theproject how much of the radiation burden is unjus-tified and should be reduced. The project cancooperate with experts in this field and also fulfillobligations to harmonize with the legislation ofthe EU relating to the reduction of radiation dosefrom medical sources. Based on the project, levelsrecommended by the National Regulation for Pro-tection from Radiation are to be introduced as aguide for radiologists.
The measurement of occupational exposures hasto be extended to include the excess dose fromnatural sources and to control nonhomogenous,irregular doses of radiation. A survey on equip-ment emitting nonionizing radiation should alsobe initiated.
2. Goals to be achieved
To maintain and extend radiation safety;To coordinate monitoring activitiesamong the different branches in the frameof OKSER;To monitor the radiation dose of the pop-ulation, environmental elements and foodand to achieve a suitable level of prepa-redness in case of nuclear emergency;To carry out a survey on the radiation doseof the population from X-ray and isotopediagnostic sources, to study the feasibilityof possible reduction and to serve as a basisfor the determination of acceptable levels;
68
Radiation Safety 8. 8
8. 8 Radiation Safety

To decrease the radiation dose of the pop-ulation from both manmade and naturalsources;To arrange and solve disposal of wastefrom uranium mining and the use of nucle-ar energy;To reveal and decrease the dose and possi-ble health effects of nonionizing radiation.
3. Main current programmes
Environmental Monitoring Programme of JointAuthorities for Radiological Protection around thePaks Nuclear Power PlantThe monitoring system is focused on the radioac-tive emission from the Paks Nuclear Power Plantand has been operating since 1983. The followinginstitutions participate in the programme:
Centre for collecting, processing andevaluating data;
Ministry of Agriculture;Ministry of Welfare;Ministry for Environment and RegionalPolicy;Paks Nuclear Power Plant.
The annual report of the Data Processing andEvaluation Centre (at the National Institute of Ra-diation Hygiene) contains detailed measurementdata on the excess radiation dose of the populationliving near the Nuclear Power Plant. This radia-tion dose is in the order of one tenth microsievertper year, according to the calculations made on thebasis of the distribution model of emitted radioac-tive substances.
Monitoring Network for Medical RadiationSince 1978 this network has been operated by theMinistry of Welfare and its institutions: RegionalInstitutes of the National Public Health Serviceare taking part in it with the guidance of theNational Institute for Radiation Hygiene. Themonitoring network controls the level of radioac-tivity of the environmental elements and food.The goal is to give information on and forecastcontamination (in air, food, water, etc.) and theradiation dose affecting the population. The net-work cooperates with international networks suchas GERMON operated by the WHO by exchang-ing data. Results of measurements are regularlypublished.
National Radiation Control System (OKSER)Based on the favourable experience of interminis-terial cooperation in the field of operating thenationwide monitoring system mentioned above,the control system has been created for ministriesand other national institutions, establishmentsusing nuclear technology, and several laboratories.
Nationwide survey of the environmental radiationlevelThe Nuclear Plant monitoring programme wasexpanded to survey the environmental radiationlevel all over the country. Systematic control ofthe radiation level takes place at 123 measuringpoints in the country using thermoluminescentdosimeters. This method is combined with highpressure ionizing chambers and in situ gamma-spectrometric measurements in some places. Thismonitoring system was able to assess changes inradioactive pollution in Hungary after the Cherno-byl accident.
Centralized personal dosimetry service for alloccupationally exposed personsThe National Personal Dosimetry Service routine-ly sends filmdosimeters to employees at variousworkplaces where it is considered justified and re-quested by the Radiation Protection Service or thelocal management. If the Dosimetry Service findslevels that give rise to concern, the local RadiationProtection Service and local authorities areinformed.
Cytogenetic monitoring of occupationally exposedmembers of high risk groupsThe human lymphocyte micronucleus test wasintroduced to detect genotoxic effects in exposedworkers or population groups. The test is suitableto detect overexposure to ionizing radiation and forprediction of the radiation dose. This method mayalso be applied for in vitro assessment of adversehealth effects caused by chemicals (metals, organicsolvents, antioxidants, radioprotective agents).This test seems to be more suitable than investiga-tion of chromosome aberration in metaphase.International cooperation is therefore proposed tostudy the possibilities of introduction/applicationof this screening method.
69
8. 8 Radiation Safety

Preparatory Program for the survey on radiation burden from medical sourcesThe NEXT (Nationwide Evaluation of X-rayTrends) was adapted to the Hungarian conditionsin 1990. The National Institute for RadiationHygiene elaborated a project applied to the prac-tice carried out in Hungary. A survey has beenstarted on the screening tests and examinationsconsidered to lead to the highest exposure to radi-ation like mammography CT, etc.
4. Problems to be solved
Monitoring networksTwo different monitoring networks are operated,One of them belongs to the Ministry of Welfareand the other to the Ministry of Agriculture. Thetask is to monitor the level of radioactivity in theenvironment and food consumed by the popula-tion and also to estimate the radiation dose fromradionuclides. The duties of the two networksoverlap in many cases so the sharing of the workand good cooperation should be established.
For the nationwide network, the most importantrequirement is regular monitoring besides enablingpreparedness for emergency. A project should beelaborated for a new – perhaps joint – institution.
Radiation dose from radonA representative survey on radiation exposure ofthe population caused by radon has been carriedout in dwellings, but there are many problems tobe solved. The survey has found the radiation dosefrom radon to be about twice as much as theworldwide average, but before taking any mea-sures these data should be reviewed. For calcula-tion of the acceptable doses, the rate of balanceamong radon and its several elements, and thetime spent in the premises has to be known, andthe level of radon should be studied at work, edu-cational institutions, etc. Legislation and determi-nation of threshold limits can follow the accom-plishment of these tasks.
Restoration of damage caused by uranium miningRestoration of damaged environments caused bythe activity of uranium mining is an importantregional problem. For the purpose of elaboratingrequirements and technology of restoration, differ-ent institutions collaborate, such as the institutesof National Public Health Service, the NationalInstitute for Radiation Hygiene, and a PHARECentre is to be set up to support the work.
Disposal of radioactive wastesDisposal of radioactive wastes is a regional and atthe same time a nationwide problem.
Taking the international tendencies into account,transmission and transport to other countries can-not be expected in the long run, and a solution hasto be provided inside the country. The selection ofsites for deposits of wastes with low and mediumactivity is under way and a deposit site for wastesof high activity is available in Paks. Russia is stillwilling to accept the spent fuel cassettes, but anational project has been started to find an under-ground deposit site as a final solution.
The National Institute for Radiation Hygiene istaking part in the preliminary study, and elabora-tion of the requirements is an important task forthe future.
Radiation dose of the population from medicaldiagnostic processesA survey is under way with international supportto measure the dose of the population, howeverthe staff and technical equipment are to be en-larged for accomplishing the task. An intersectoralcooperation is needed among radiologists, scien-tific experts and associations for this purpose, andmethods for data collection, processing and evalu-ation are to be elaborated as well.
5. Future tasks
The following table gives a summary of the futuretasks.
70
Radiation Safety 8. 8

71
8. 8 Radiation Safety
Edu
catio
n
Bas
ic a
nd p
ostg
radu
ate
educ
a-tio
n of
the
wor
kers
at a
n ap
pro-
pria
te le
vel;
Educ
atio
n of
the
staf
f wor
king
inth
e na
tiona
l mon
itorin
g ne
twor
k;G
ener
al e
duca
tion
of th
e po
pula
-tio
n w
ith th
e he
lp o
f mas
s med
ia;
Publ
ishi
ng
the
Inte
rnat
iona
lB
asic
Leg
isla
tion
for
Prot
ectio
nA
gain
st R
adia
tion
in H
unga
rian
new
spap
ers a
nd m
agaz
ines
.
Res
earc
h an
d de
velo
pmen
t
Expa
ndin
g te
sts
for
dete
ctin
gge
noto
xic
effe
cts;
Nat
ionw
ide
surv
ey o
n ra
dioa
c-tiv
ity o
f ind
ustri
al b
y-pr
oduc
ts;
Stud
y on
beh
avio
r of
rad
ionu
-cl
ides
in
the
envi
ronm
ent,
ex-
amin
ing
poss
ibili
ties
for
rest
o-ra
tion
of c
onta
min
ated
ara
ble
land
;Im
prov
ing
met
hods
of
mea
sur-
ing
radi
oact
ive
dose
s.
Adm
inis
trat
ive
mea
sure
s
Det
erm
inat
ion
of l
imit
valu
esfo
r ra
dion
uclid
es
cons
umed
with
food
and
drin
king
wat
er;
Legi
slat
ion
on i
ndoo
r ra
don
conc
entra
tion;
Legi
slat
ion
on w
aste
dis
posa
lan
d de
term
inat
ion
of li
mit
val-
ues
for e
mis
sion
;El
abor
atio
n of
requ
irem
ents
and
basic
met
hods
for r
esto
ratio
n;Le
gisl
atio
n on
no
n-io
nizi
ngra
diat
ion;
Intro
duct
ion
of i
nter
natio
nal
reco
mm
enda
tions
for t
he ra
dia-
tion
dose
from
med
ical
sour
ces
into
the
Hun
garia
n le
gisl
atio
n.
Info
rmat
ion,
dat
a co
llect
ion
Impr
ovin
g da
ta c
olle
ctio
n in
the
mon
itorin
g ne
twor
k;Es
tabl
ishin
g in
form
atio
n ce
ntre
;N
atio
nwid
e su
rvey
on
rado
nco
ncen
tratio
n in
side
pre
mis
es;
Stud
y on
rad
iatio
n do
ses
from
med
ical
exa
min
atio
ns;
Surv
ey o
n do
se f
rom
iso
tope
diag
nost
ic m
etho
ds.
Task
s lis
ted
acco
rdin
g to
type
s of a
ctio
n

Situation analysis, legislative background
The existing laws and/or decrees, aimed at pre-venting health against hazardous chemical andmicrobiological contamination of food, provide anadequate regulatory basis for creating food safetyin Hungary. The majority of Hungarian foodhygiene regulations are already in agreement withdirectives of the European Union. Priority foodhygiene problems, relating partly or totally toenvironmental contaminations, are mentioned inthe following.
Chemical contamination
1. Lead
The major part of lead exposure of the populationcomes from foods. The lead concentration in foodhas been controlled for 40 years in Hungary. Leadcontamination of food may occur during techno-logical processes but, today, it mainly comes fromenvironmental sources. Significant differences inthe lead level of food of plant origin have beenfound in different regions of the country. The leadcontent in vegetables has been decreasing. Resultsof the surveys are shown in Table 8. 9/1.
The result of meat tests carried out by the Na-tional Institute for Testing Meat shows a decreas-ing trend in the lead content of food. The reductionis due to the stricter limit values in fodder intro-duced in 1990 (see Table 8. 9/2). There is a nation-wide decreasing trend in lead content of differentfoods.
In 1995 the highest level of lead was 408 mg/kgin cereals, 234 mg/kg in vegetables, 320 mg/kg infruits measured by the Regional Laboratories ofthe Food Control Stations. However the situationis not as good as that, because the most contami-nated types of food and vegetables were not anal-ysed in 1995.
Tasks:Quality assurance/control/management;Clarification of sampling problems;Monitoring the lead content in food prod-ucts; evaluation of contamination of smallergroups of food products; analysis of differ-ences between regions;
Survey of food contamination in pollutedareas;Studying lead intake in daily diets;Elimination of contamination sources; Minimisation of emissions.
2. Cadmium
A considerable part of human cadmium exposurecomes from foods. According to food examinationdata, Hungary belongs to the moderately contami-nated countries. Cadmium levels in food show aslightly increasing tendency all over the world.Different foods contain cadmium in the followingorder: milk, eggs, fruit, vegetables, cereals, meat,fish and internal organs. The cadmium uptake ofplants depends on the type and species of soil andplant. The highest level of cadmium occurs inbran. Cadmium levels in Hungarian foods havenot changed considerably over recent years.The following median values were reported in 1995:in cereals 15–18 g/kg, in vegetables 4–150 g/kg, infruits 1–7 g/kg. Results are shown in Fig. 8. 9/3and 8. 9/4.
Cadmium levels above the limit value werefound in 10 of the sampled potatoes and Hunga-rian red pepper. The average cadmium content ofpig kidneys has not changed since 1992, but thatof cattle kidneys shows a continuous increase:357, 485 and 375 mg/kg, in the years 1992, 1993and 1994 respectively.
Tasks:Quality assurance/quality control of testinglaboratories;Clarification of sampling problems;Monitoring the cadmium level in food prod-ucts; evaluation of contamination of smallergroups of food products; analysis of differ-ences between regions;Investigation of the cadmium content in foodin polluted areas;Studying cadmium uptake by plants;Elimination of emission sources and min-imising emissions.
72
Food Safety 8. 9
8. 9 Food Safety

Contamination of vegetables with leadTable 8. 9/1
Contamination of meat with leadTable 8. 9/2
Contamination of vegetables with cadmiumTable 8. 9/3
*Note: one or two extreme values in bran
Contamination of meat with cadmiumTable 8. 9/4
73
8. 9 Food Safety
Food Number of samples Lead content (µµg/kg)median maximum
Cereals 8 50–600 110–2100Vegetables 22 3–308 90–6400
Fruit 9 3–190 40–750
YearAverage content of lead (µµg/kg)
Pork Beef Poultry Game 1989 430 500 310 3601990 210 250 240 4001991 190 190 200 4601992 150 140 130 3701993 70 70 60 111994 40 40 40 50
Food Number of samplesCadmium content (µµg/kg)
median maximumCereals 9 5–62 200–800*
Vegetables 8 5–30 20–461*
Fruit 7 1–16 5–90
YearAverage content of cadmium (µµg/kg)
Pork Beef Poultry Game 1989 41 144 15 151990 42 57 27 751991 32 31 17 551992 23 22 19 271993 13 16 10 141994 11 12 9 13

Average benzo(a)pyrene concentration of some vegetables (µµg/kg)Table 8. 9/5
Average benzo(a)pyrene and total PAH content in cereals (µµg/kg)Table 8. 9/6
Content of chlorinated hydrocarbon pesticides in meat (µµg/kg)Table 8. 9/7
nd = not detectable = 0.5 mg/kg
Weekly intake in 1995 of PCB from foodstuffsTable 8. 9/8
74
Food Safety 8. 9
In the vicinity of
Food Produced in clean air areaOil refinery Oil refinery
with old technology with modern technology
Carrots 0.37 8.5 3.5Lettuce 0.42 3.8 3.4
Produced in clean air area Polluted area (traffic)benzo(a)pyrene 0.2 2.1
total PAH 1.40 4.52
HCB HCH isomers Total DDTPork 1–2 1–2 20Beef 2 1–3 60
Poultry nd–2 nd–4 6–7Game 1–6 nd–10 10–400
Sampling place Number Total content of PCB (µµg/kg)of sample of samples median 90-percentile rangePécs 30 < 0.01 47.2 < 0.01–112.4Budapest 30 < 0.01 24.0 < 0.01–118.0Szolnok 30 < 0.01 14.4 < 0.01–22.5
3. Mercury
Foods of plant origin contain mercury in negligi-ble quantities. Fish are the best indicators of envi-ronmental mercury contamination. The mercurycontent of fish from fish ponds and Lake Balatonhas never reached the limit value. Higher concen-tration levels were detected in some cases in fishcaught from the rivers Danube and Tisza. Mercury,as an environmental contaminant, has no priorityfrom a food hygiene perspective in Hungary.
4. Nitrate
The increasing nitrate content of vegetables may bepartly due to the excessive use of artificial fertiliserscontaining nitrogen. The content of nitrate in veg-etables strongly depends on the plant species, agri-cultural methods and climate. Characteristic valuesare similar to those measured in Western Europe.
The nitrate content in fruit is considerablylower than in vegetables. The natural nitratecontent of foods of animal origin is insignif-icant; The high nitrate content of vegetables haspriority from a food hygiene perspective, es-pecially in the fields of targeted plant im-provement and good agricultural practice.
5. Radionuclides
In Hungary the regular monitoring of food is car-ried out by the Ministry of Agriculture. Since 1978the National Network for Measuring Radiationhas been working as well under the Ministry ofWelfare, monitoring and controlling radioactivityof the consumed food and water. The radiationdose from food in Hungary is the same as thatfrom the background level. Concentrations ofradionuclides in plants near the Paks NuclearPower Station have never reached the level of con-cern. They have been monitored systematicallysince the beginning of the plant’s activity. Thisproblem has no priority at present in Hungary, butmonitoring and controlling have to be continued.Control of imported food is not properly solvedyet, the monitoring laboratories sampled and ana-lysed imported food (such as milk powder, cannedfish) where the concentration of radioactivity wasseveral tenths or thousandths higher than theallowed value.
In addition, greater preparedness for emergency isvery important due to the increasing number ofnuclear establishments around the border in theneighbouring countries. (The problem is describedin detail in the section 8.8 on Radiation Safety).
6. Polycyclic aromatic hydrocarbons (PAHs)
PAHs may enter foods as technological contami-nation and as environmental pollution. Contami-nation can be minimized with appropriate techno-logical measures. Studies on environmental PAHsand their adverse effect through the food chainhave priority. PAH contamination might be con-siderable in soil and vegetation around busy roads,aluminium smelters, oil refineries, airports etc.Unprocessed, raw foods of animal origin do notcontain PAHs. (see Fig. 8. 9/5 and 8. 9/6)
Tasks:Collection of data;Measurements of PAHs in indicator foods;Elimination of sources.
7. Polychlorinated compounds
Hundreds of environmental pollutants of differenttoxicity belong to this group. Due to their fat sol-ubility, persistency and biomagnification in thefood chain, the highest concentrations areobserved in human adipose tissue. Human expo-sure comes almost only from food. Reduction ofemissions is the only effective preventive mea-sure, because the rate of elimination of polychlori-nated compounds from the environment is a verylong process.
8. Chlorinated pesticides
Even after more than 25 years of ban on their useas pesticides, they can be detected, first of all, indomestic foods of animal origin. Concentrationsof DDT, HCB and HCH isomers are presented inTable 8. 9/7. The monitoring of chlorinated hydro-carbon pesticides has no priority in Hungary.
9. Polychlorinated biphenyls (PCBs)
PCBs are typical industrial contaminants and canbe found everywhere in the environment. In the air0.002–15 ng/m3, around industrial plants in rain-
75
8. 9 Food Safety

fall 1–250 ng/l, in the ocean 0.05–06 ng/l.Vegetables contain about an average of 10 mg/kg,milk 5–200 mg/kg, butter 30–80 mg/kg, animal fats20–240 mg/kg. In the nutrition chain there is a sig-nificant cumulation and in breast milk 0.5–1 mg/kg,in human fat 1–5 mg/kg can be found.
Production of PCBs has been limited all over theworld. There has never been any production inHungary and the application has also been restrict-ed. The presence of PCBs has to be reckoned within food of plant origin in our industrial regions, inthe environment of big industrial plants, wasteincinerators and waste deposits. Examination ofdomestic meat samples has shown no PCB con-tamination with a method of 1 mg/kg sensitivity.
According to WHO/EURO the acceptable week-ly intake is 100 mg. From a food hygiene perspec-tives this topic has high priority in Hungary.
The results of dietary analyses carried out by theNational Institute for Nutrition Hygiene in 1995are shown in Table 8. 9/8.
Tasks:Monitoring the PCBs in food, breast milkand daily diet;Banning the use of materials containing PCBs;Control of industrial PCB emissions (includ-ing incinerators).
10. Polychlorinated dibenzo-dioxins and poly-chlorinated dibenzo-furans
There are no national data on the occurrence andlevel of dibenzo-dioxins and polychlorinateddibenzo-furans in food. As part of an internationalcooperation, two human milk samples were exam-ined abroad and proved to be less contaminatedthan samples from other European countries. Thetopic can be regarded as of high priority.
Tasks:Creating testing capacity;Monitoring of indicator foods, breast milk anddaily diet.
11. Pesticides
The registration of pesticides takes place understrict conditions in Hungary. Respect of instruc-tions of use and waiting times ensure the degrada-tion of residues before harvesting. Examinationsin recent years found that about 1% of the samplestested exceeded the maximum limits.
Microbiological contaminationHistorically, infections acquired through theintake of food have been of great public healthimportance. For example, the centralization ofmilk processing in dairies and the wide distribu-tion of milk in urban areas led to epidemics untilheat treatment was made obligatory, and hygienicinspection of the food production chain was estab-lished. Food control aiming at the prevention offoodborne infections is, therefore, still of greatimportance for the health of the population. Thereported food infections and food poisonings areshown in Fig. 8. 9/9, 8. 9/10 and 8. 9/11.
The infection of animals occurs in the environ-ment of animal husbandry partly due to hygienicdeficiencies and partly to the infectivity of import-ed fodder. In food-borne epidemics and diseases,Salmonellae bacteria of animal origin play thedecisive role. Therefore, the environmental hygieneof animal husbandry and of food processing ofanimal origin must be prioritized.
The following table lists some main tasks to besolved.
76
Food Safety 8. 9
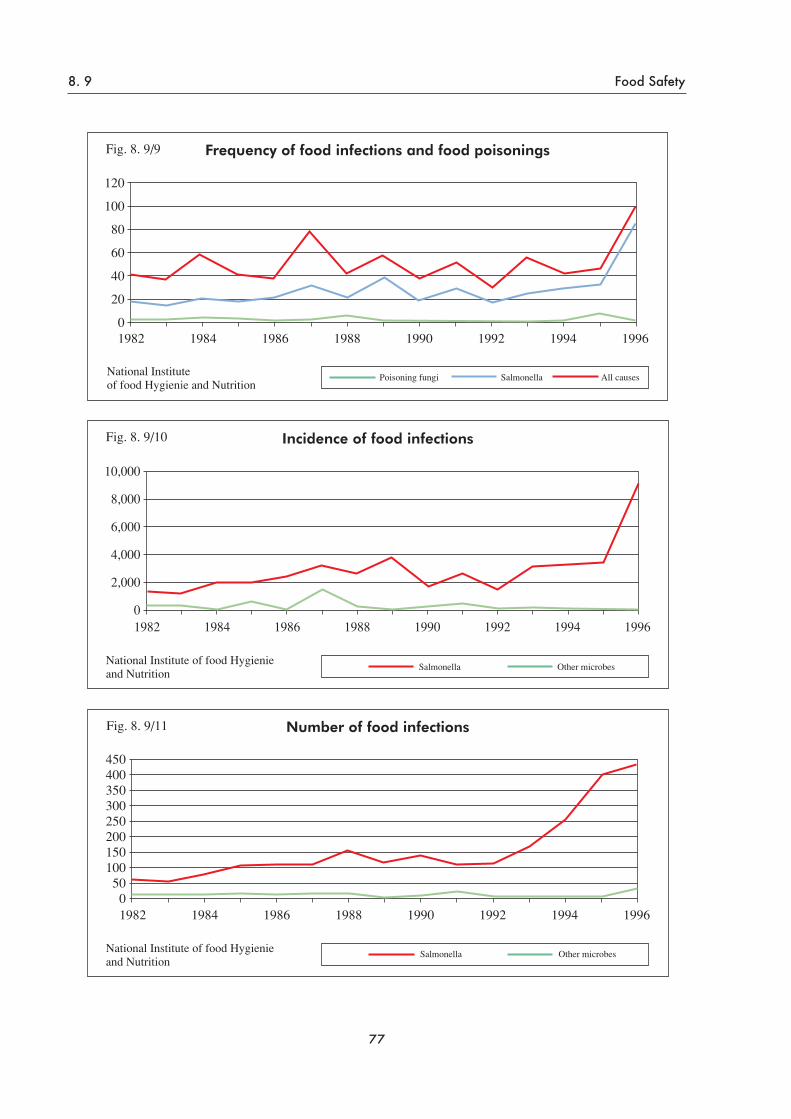
77
8. 9 Food Safety

78
Food Safety 8. 9
Prev
entio
n of
food
cont
amin
atio
n
Prev
entio
n of
food
co
ntam
inat
ion
with
lead
; B
anni
ng p
rodu
ctio
n on
soil
cont
amin
ated
with
cadm
ium
; R
educ
ing
nitra
te c
onte
ntin
food
; El
imin
atin
g po
llutio
nso
urce
s an
d re
duci
ngem
issi
on;
Prev
entin
g us
e of
su
bsta
nces
with
PC
B;
Prev
entio
n of
mic
robi
olog
ical
co
ntam
inat
ion
of fo
od.
Dat
a co
llect
ion,
su
rvey
and
stud
y
Syst
emat
ic a
naly
sis
ofco
ntam
inat
ed s
oil (
for
lead
, cad
miu
m, P
CB
,et
c.);
Impr
ovem
ent
of c
apac
ityan
d m
etho
ds o
f lab
orat
orie
s.
Res
earc
h, d
evel
opm
ent
Con
tinuo
us m
onito
ring
of fo
od;
In c
onta
min
ated
regi
ons,
com
plex
sur
vey
(soi
l and
pop
ulat
ion)
;M
onito
ring
PCB
con
tent
of b
reas
t milk
and
dai
lydi
etar
y in
take
.
Leg
isla
tion,
adm
inis
trat
ive
mea
sure
s
Ada
ptat
ion
to th
e EU
legi
slat
ion;
Am
endi
ng n
atio
nal
legi
slat
ion.
Edu
catio
n, in
form
atio
n
Educ
atio
n fo
r pro
per
nutri
tion;
Reg
ular
info
rmat
ion
ofth
e po
pula
tion.
Task
s lis
ted
acco
rdin
g to
type
s of a
ctio
n

1. Analysis of the situation
Housing situationAccording to the statistics 62.7% of the populationlives in towns in Hungary. This is due to migrationand an increasing number of settlements beinggiven the status of “town”. The concentrated de-velopment of industry resulted in migration andshortage of housing and the only solution was tobuild large housing estates. Between 1961 and1990 more than 2 million flats were built, includ-ing a 15-year period of the socalled “housing pro-gramme”.
Not only the number of home units but also thenumber of rooms and the average area of flats hasincreased. The proportion of one-room flats hasdecreased while the number of flats with two orthree rooms has increased. The number of roomsper flat increased by 50% between 1970 and 1990(Table 8. 10/1). The geographical situation, how-ever, differs, as in Budapest the proportion of flatswith 3 or more rooms is only 25% against 38.5%in the rest of the country. (Table 8. 10/2)
The increasing number of apartments has resultedin a favourable development of the density of occu-pants. In 1960 their number per 100 rooms was245, decreasing over 35 years to 108. However,this improvement hides the fact that the larger flatswere built by smaller and, therefore, better-offfamilies. By the end of the 1990s, in about 22% ofthe flats there were 1.5 persons per room.
Unfortunately not enough green areas were laidout for the large housing estates. In 1994 the aver-age area of green public sites in towns was 35.2 m2
per inhabitant (13.3–76.4 m2; Budapest: 38.6m2). While the new housing estates were followed by
a reasonable development of the basic infrastruc-ture, the density of dwellers was intolerable. Alsothe industrialised construction process broughtmany problems resulting from new materials,equipment and technology.
Factors like low ceilings, low permeability ofconcrete walls and improved insulation for energysaving reasons since the second half of the 1980shave caused emission of pollutants in apartmentsin harmful concentrations.
New equipment, coating and covering materialsdischarge several pollutants, including formalde-hyde emanating from chipboard (glued wood-
fibres), insulating and adhesive materials, wallpa-pers, carpets, etc. Hardly any information exists inHungary about the concentration of organic com-pounds used in paints, lacquers, building and cov-ering materials used in homes.
In villages, homes are usually heated with solidfuel. In towns, gas heating is quite frequent butmodern housing estates are supplied with districtheating (Table 8. 10/3). The negative side of theimprovement brought by district heating is that thehumidity is low and the temperature cannot beadjusted to individual needs.
Gas heating may be considered an advantage ifthe flue gas is conducted away through a chimney.In many cases so-called “parapet” appliances areused where the exhaust gas is emitted from theroom directly under the windows. Around largebuildings with several storeys heated by this sys-tem, the nitrogen oxide and carbon monoxide con-centrations may become so high in the heating sea-son that the apartments cannot be effectively aired.
Even in one-storey buildings the exhaust gasmay enter rooms through the windows.
Radon is a special pollutant in the indoor atmo-sphere of apartments. Radon emanates from thesoil with large geographical variations. In Mátra-derecske in the Mátra mountains extremely highconcentrations have recently been measured. Theconcentration of radon is much lower in buildingsconstructed with a cellar but building materialsmay discharge radon as well, or it may be foundalong the water supply system. Improved insula-tion and a low rate of ventilation can result inhigher concentrations. Besides the natural contentof radioactivity in building materials some addi-tives such as slag and ash from power stations mayshow high activity.
Among building materials, products made ofconcrete with asbestos should be specifically men-tioned because they are used for roofs, coveringsheets and pipes.
From the 1980s the growth of mould in apart-ments is an increasing problem due to insufficientventilation and heating and the construction prin-ciples used. Table 8. 10/4 showes the utilities ofhome units.
79
Urban Environment 8. 10
8. 10 Urban Environment

2. Health impacts
The relationship between urban conditions and thehealth status of the population is generally quitecomplex.
According to Hungarian studies, a high densityof dwellings, heavy traffic, noise and polluted aircontribute to the high incidence of neurosis andother pshychosomatic diseases such as high bloodpressure and gastric ulcers.
In housing estates conditions are not generallysuitable for the kind of physical exercise thatwould promote a healthy life style. Among chil-dren living in housing estates the prevalence ofvegetative instability is quite high due to lack ofphysical exercise and staying too little outdoors.According to the results of a survey covering morethan 2,700 apartments in Budapest, the signs of“sick building syndrome” were significantly morefrequent in modern housing estates than in tradi-tionally built buildings.
The unfavourable conditions of housing estates– besides the density of dwellers – originate fromthe ground-plan of the flats which is not adoptableto individual needs. Owing to plastic materials,formaldehyde emission and mites in the dust,allergic respiratory diseases (such as asthma) aremuch more frequent in modern buildings made ofconcreteelements than in traditional brick build-ings. Mould also seems to be one of the main caus-es of asthmatic disease.
In crowded flats the incidence of respiratory dis-eases – spread by droplet infection – is increased.The social conditions and resistance to disease ofpeople living in crowded apartments are generallypoorer than where fewer people live together, con-tributing to a higher frequency of diseases.
Many studies have found a relationship betweenthe high nitrogen oxide concentrations caused bygas appliances and acute respiratory diseases inchildren.
Radon is a well-known carcinogen. Calculatedon the basis of the WHO Guideline (1987), inHungary, 100–400 lung cancer cases annually areestimated to be due to the effect of radon and itscomponents. The estimated figure is ten timeshigher among uranium miners. In several countriesthe proportional mortality of lung cancer caused byradon and its components is 5–15%. The popula-tion risk estimated for Hungary on the base of thecancer cases referred to above, seems reasonable
because the main cause of the 7,500 annual casesof primary lung cancer would be smoking.
Asbestos is another carcinogen – inducing mainlymesotheliomas by inhalation. The number ofmesothelioma cases per year (among these all pri-mary and secondary cancers of the pleura) is about100, registered by the National PulmonologicalInstitute.
3. Goals to be achieved
The conditions of the urban environment with itsbuildings and apartments should satisfy the fol-lowing demands:
ensure adequate protection against theunfavourable effects of the outdoor envi-ronment;ensure the necessary circumstances forthe regeneration of the organism;ensure the necessary conditions for thedwellers to wash, cook, learn, run culturalactivities and live a healthy family andsocial life.
If these requirements are realised, the urban sur-roundings can contribute to the health status envis-aged by the broad WHO definition.
Besides the long-term optimal goals, it shouldbe ensured as a short-term minimum requirement,that housing does not damage the health status ofinhabitants.
4. Problems to be solved
One basic problem is the contradictory and imper-fect legislation. The “Act No. III 1964 on BuildingAffairs” is under review but not yet approved. The“National Building Rules” has been amended sev-eral times but is not longer up-to-date.
Several new types of buildings, constructionforms and specifications have appeared in recentyears along with new enterprises, but without anyappropriate legal background. The national stan-dards are no longer valid and the former technicalguidelines are not obligatory.
According to the law on local authorities, specialbuilding regulations may be issued locally but theymust not contradict the provisions of the NationalRules. This creates many practical difficulties.During the industrialised building era, the tradition-al building culture could not be maintained. Theemerging problems were solved in a practical way
80
8. 10 Urban Environment

with little attention being paid to the principle ofprevention. Thus, hardly any experience has beengained in how to plan buildings, and which materi-als to use to prevent harmful health effects.
In Hungary no rules are in force to regulate theclassification of building materials from a healthperspective and to determine requirements forchemical and microbiological discharges into theindoor atmosphere.
There is no limit value for acceptable radioac-tive concentrations (the standard No. 62 does notcontain any regulation). Based on research, twodecrees are presently in force (26/1960 ÉM and46/1969 ÉVM) banning the use of certain slagsfrom power stations to construct dwellings anddetermining the types of storage buildings wherethis material may be used.
The insufficient areas of parks and green areasmean that important functions of dwellings (likerecreation and sport) are missing and also that thebuilt-up area is crowded with urban traffic, caus-ing air pollution and noise.
In big towns the air and soil of playgrounds isoften so polluted that they are unsuitable for theirintended functions.
In urban areas rules for dog-keeping are non-existentcausing health risks first of all for small children.
Another serious public health problem is the fre-quent presence of Ambrosia weed on neglectedsites in towns causing allergic and asthmatic dis-ease. (As shown in Fig. 8. 1/8)
5. Programmes in progress
Efforts to implement the WHO “Health for All”programme target No. 24: “by the year 2000 townsand rural settlements should ensure for the inhabi-tants a physical and social environment promotinghealth conservation”.
Amendment of the Law On Construction WorkManagement and development of the newNational Building Rules.
6. Tasks to be performed
Tasks are summarized in the following table.
81
Urban Environment 8. 10
Total population, number of home units, average number of rooms per unit and the number of dwellers per room
Table 8. 10/1
Distribution of the number of rooms per occupied home units (196–90)Table 8. 10/2
1960 1970 1980 1990 1995Population (thousands) 9961 10322 10709 10375 10246Number of home units
2758 3122 3542 3853 3971(thousands)Average number of rooms per flat 1.5 1.6 2.0 2.4 2.4Number of dwellers per room 245 202 152 114 108
Number1960 1970 1980 1990 Of which
of rooms
Budapest Other
Villagestowns
1 room 62.5 45.7 27.7 17.5 52.2 14.5 16.52 rooms 32.8 43.8 52.2 50.6 49.7 55.2 44.83 rooms 4.7 10.4 20.1 32.2 25.0 30.3 38.5

Distribution of occupied home units by heating formTable 8. 10/3
Utilis in the occupied home units, 1990Table 8. 10/3
82
8. 10 Urban Environment
As a percentage (%) of the occupied flatsEquipment National total Budapest Other towns VillagesPiped water 84.5 98.7 89.8 70.6Of which: Water network 79.1 98.4 87.7 58.8Gas mains 40.9 78.7 50.4 8.7Bottled gas 45.8 5.7 35.8 79.7Flush toilets 75.3 90.7 83.0 57.9Local sewage Of which: Sewage network
85–44.3 98.8–86.9 90.3–58.9 71.3–3.8
National total Budapest Other towns VillagesNumber of occupied
3637 765 1518 1354home units (thousands)
Heating form As a percentage (%) of the occupied flats
Central heating 42.6 51.8 49.5 29.8Of which:
District heating16.9 31.6 24.2 0.4
Central heating in the building 2.9 5.8 3.4 0.7Central heating in the flat 22.8 14.4 21.9 28.7
Individual heating in the rooms 57.4 48.2 50.5 70.2Of which:
Electricity3.4 6.4 2.5 26.0
Gas 18.1 32.4 22.5 5.0Oil 4.5 2.6 4.3 5.8Wood 7.8 1.0 3.6 16.4Coal 23.4 5.4 17.5 40.3Other 0.2 0.4 0.1 0.1

83
Urban Environment 8. 10
Prac
tical
task
s
Intro
duci
ng
clas
sific
atio
n of
equi
pmen
t, bu
ildin
g an
d co
ver-
ing
mat
eria
ls u
sed
indo
ors
indw
ellin
gs, a
nd a
n ap
prov
al s
ys-
tem
for
thei
r ap
plic
atio
n fr
om a
heal
th p
oint
of v
iew
; H
eatin
g an
d co
okin
g m
etho
dsan
d ap
plia
nces
tha
t po
llute
the
indo
or a
ir sh
ould
be
avoi
ded;
D
urin
g th
e pl
anni
ng,
cons
truc-
tion
and
oper
atio
n of
new
hou
s-es
, he
alth
as
pect
s sh
ould
be
take
n in
to c
onsi
dera
tion;
Furth
er d
evel
opm
ent o
f par
ks an
dgr
een
area
s sh
ould
be
a fu
n-da
men
tal g
oal o
f urb
an-p
lann
ing.
All
negl
ecte
d ar
eas s
houl
d be
sur-
veye
d w
ith th
e ai
m o
f es
tabl
ish-
ing
park
s or
at
leas
t er
adic
atin
gA
mbr
osia
wee
ds;
In s
ettle
men
ts,
spec
ial
plac
essh
ould
be
desi
gnat
ed f
or d
ogex
erci
sing
in th
e ne
ighb
ourh
ood,
and
dogs
sho
uld
not b
e al
low
edac
cess
to p
layg
roun
ds.
Surv
ery,
mon
itori
ng
Asu
rvey
sho
uld
be i
nitia
ted
tom
easu
re th
e ex
posu
re o
f the
pop
-ul
atio
n to
ra
don
in
diff
eren
tty
pes o
f bui
ldin
gs a
lso
dete
rmin
-in
g th
e ra
dioa
ctiv
ity o
f bu
ildin
gm
ater
ials
an
d na
tura
l w
ater
sour
ces;
Furth
er re
sear
ch is
nee
ded
on th
ehe
alth
effe
cts
of r
adon
con
cen-
tratio
ns i
n dw
ellin
gs a
nd w
ork-
plac
es. F
urth
er re
sear
ch is
nee
d-ed
on
the
rela
tions
hip
betw
een
life
cond
ition
s res
ultin
g fr
om th
eus
e of
bui
ldin
g an
d ot
her m
ater
i-al
s an
d eq
uipm
ent,
and
the
heal
th st
atus
of d
wel
lers
to d
eter
-m
ine
requ
irem
ents
.
Offi
cial
mea
sure
s, le
gisl
atio
n
Rev
isin
g th
e N
atio
nal B
uild
ing
Rul
es;
App
roxi
mat
ing
to
and
har-
mon
isin
g w
ith t
he l
egis
latio
nof
the
EU.
Edu
catio
n, in
form
atio
n
Engi
neer
s, fa
mily
doc
tors
and
the
popu
latio
n sh
ould
be
in-
form
ed o
n th
e he
alth
asp
ects
of
hous
ing;
Reg
ular
pub
licat
ion
of i
nfor
-m
atio
n ab
out h
ousi
ng;
Educ
atin
g pr
oper
beh
avio
ur.
Tank
s lis
ted
acco
rdin
d to
type
s of a
ctio
n

1. Situation analysis
The health status of the population is influencedby environmental factors – in many cases to a con-siderable extent. In order to analyse and evaluatethese factors and their impact, reliable informa-tion, based on solid data should be available.There is a continuous need for registering andanalysing relevant data on the environment andfactors characterising health status to evaluaterelationships. This can be carried out only withharmonised work.
2. Goals to be achieved
Establishment of harmonised databaseson the status of human health and theenvironment;Establishment and development of corre-sponding infrastructure (like GIS);Development of an evaluation and report-ing system for decision makers on theinteraction of environment and health;Public information and ensuring avail-ability of data are basic requirements.
3. Problems to be solved
Since establishing a complex system includes thelong-term operation as well, it is important to en-sure an adequate budget for operation and mainte-nance. The legal and financial background are alsoessential. Data concerning the environment andhealth are collected, stored and evaluated in anumber of institutes, belonging to different min-istries. Quite understandably, the aspects of datacollection, the method of verification and valida-tion is different in various institutes. It is desirableto achieve a system in which data could be mutu-ally beneficially used.
It is necessary to establish an up-to-date infra-structure to deal with all informationrelated issues.
There are administrative, legal and very oftenfinancial obstacles which prevent further develop-ment of the existing system.
4. General tasks and basic principles
The complex relationship between environment andhealth can only be understood and dealt with, if thechanges and their results can be followed in timeand space. In order to achieve this, a well organisedstructure should be established for data collection,storage, elaboration, evaluation and reporting.
Data collection, structure of data basesWhen collecting data, the smallest possible aggre-gation level should be the aim. By utilising geo-graphic presentation and evaluation, an effortshould be made to attain the highest possible reso-lution. Individual data should be collected at thelowest level (district, city, county).
Analysis and mode of evaluationRoutine and ad hoc analyses are required. For con-tinuous, routine analysis, a comprehensive systemshould be established with relevant experts.Changes and tendencies should be evaluated atintervals. Ad hoc evaluation is also needed forspecific purposes. Validity and fidelity of the eval-uation should always be ensured. Tools for betterunderstanding are statistical methods.
Selection of indicators for environmental healthProper assessment and evaluation of tendencies ofenvironmental health require indicators that arecharacteristic for the given changes. Despite seve-ral international conferences and workshops, noestablished system yet exists. It is highly desirablethat in collaboration with international institutesand agencies, a system of indicators for environ-mental health be established.
MandateIt is essential to understand that a system of suchcomplexity can only be achieved if the necessarymandate for collecting, storing, evaluating anddisseminating information is ensured and secured.
5. Tasks for achieving goals
The tasks are summarized in the table below.
84
Environmental Health Information System 9. 1
9. Implementation of the Hungarian Environmental Health Action Programme
9. 1 Environmental Health Information System (EHIS)

85
9. 1 Environmental Health Information System
Prac
tical
task
s(o
rgan
izat
ion,
con
trol
)
Det
erm
inat
ion
of th
e lis
t of
rou-
tine
anal
yses
and
of
the
user
sre
ques
ting
the
resu
lts;
Dat
a pr
oces
sing
and
det
erm
inin
gpr
oble
ms f
rom
the
prev
ious
per
i-od
s;D
efin
ing
prob
lem
s us
ing
heal
thin
dica
tors
;D
etai
led
anal
ysis
for
ide
ntifi
ca-
tion
of e
nviro
nmen
tal
fact
ors
influ
enci
ng h
ealth
sta
tus;
Ana
lytic
al m
etho
ds f
or e
valu
a-tio
n of
the
effe
cts;
Stud
y fo
r id
entif
icat
ion
of a
llco
ncer
ned
grou
ps.
Info
rmat
ion,
edu
catio
n,
publ
ic a
war
enes
s
Elab
orat
ion
of t
he s
yste
ms
with
activ
e pa
rtici
pant
s fro
m th
e pr
o-je
ct f
or r
eque
st of
inf
orm
atio
n,an
d fo
r use
of d
ata
and
resu
lts;
Publ
ishin
g re
sults
of
anal
ysis
onhe
alth
and
env
ironm
enta
l iss
ues;
Det
erm
inat
ion
of d
ata
publ
ishe
dfo
r the
pub
lic th
roug
h th
e m
edia
.
Adm
inis
trat
ive
mea
sure
s(te
chni
cal,
legi
slat
ive)
Cho
osin
g in
dica
tor p
aram
eter
s;M
arki
ng o
f pr
oble
mat
ic a
reas
by u
sing
sele
cted
hea
lth in
dica
-to
rs a
nd d
ata
with
the
hel
p of
expe
rts,
star
ting
eval
uatio
n,te
stin
g in
dica
tors
;Ta
sks
for c
ompl
etin
g da
taba
se:
– de
term
inin
g th
e ex
istin
g an
dco
mpl
emen
tary
dat
a –
dete
r-m
inin
g so
urce
s and
ava
ilabi
lity
of d
ata
– en
surin
g le
gal
and
finan
cial
bac
kgro
und
– de
ve-
lopm
ent
and
amen
dmen
t of
prog
ram
mes
for
mai
nten
ance
and
regi
stra
tion
of d
atab
ase.
Stud
y, su
rvey
, dat
a co
llect
ion
Iden
tifyi
ng in
dica
tors
;D
ata
proc
essi
ng;
Cho
osin
g pr
oper
in
dica
tors
,an
alys
ing
thei
r effe
ctiv
enes
s;Pr
ogra
mm
e fo
r eva
luat
ion;
St
atis
tical
pr
ogra
mm
es
and
elab
orat
ion
of d
ata
prep
arat
ion
syst
ems
for s
patia
l ana
lyse
s;D
evel
opm
ent
of p
rogr
amm
esan
d te
chni
cal
cond
ition
s fo
rst
orag
e an
d ac
cess
of r
esul
ts.
Task
s lis
ted
acco
rdin
g to
type
s of a
ctio
n

1. Analysis of the present situation
The development of a health promoting environ-ment is one of the legal obligations of local aut-horities. However each local authority has to de-termine how this should be provided, dependingon local demands and financial conditions.
The basic health requirements of Hungarian laware the protection of healthy water supply, mainte-nance of public roads and cemeteries, lighting andprimary health and social care. The local authori-ties, of course, strive to comply with the require-ments but financial conditions make it difficult tolive up to the intentions of legislators.
The situation is complicated by the fact thatlocal authorities have limited powers in issuesrelating to the health status of inhabitants. ThisHungarian Environmental Health Action Prog-ramme cannot be implemented without the parti-cipation of local authorities but in many areas theyhave not been empowered to make decisions.
The implementation of the Action Programme isvery much dependent on central governmentaction as well. This means that all competent mini-stries must cooperate in solving the many environ-mental, regional planning and management prob-lems.
The public has become more and more aware ofits own responsibility for the environment andhealth. Hundreds of organizations, foundationsand associations have been set up and are operat-ing for different environment and health goals.Some county administrations have registeredthese non-governmental organizations (NGOs)and try to assist as coordinators, while others payless attention.
It should however be pointed out that whenreferring to NGOs, also the local professional/sci-entific and the business players (that is the localcommunities) are ment as well, all belonging tothe NGOs sector.
To solve special problems, cooperation betweenseveral local authorities may be necessary. Thismay facilitate the solution of problems and lead toa more uniform environmental health standard.Local authorities are not generally collecting envi-ronment and health data that allow comparison of
results with established limit values. Such collec-tion and evaluation of epidemiological data is newto these authorities and can only be performedwith the help of local Public Health Institutes.
Local authorities play an important role in limit-ing the harmful effects of pollution from localsources, such as industrial plants, traffic, energyand heat production and supply, and in securingwaste disposal and environment oriented regionalplanning.
2. Goals to be achieved
Helping local authorities to develop a spe-cial environmental health strategy basedon sufficient expertise;Elaboration of guidelines for setting uplocal programmes;Ensuring availability of environmentalhealth data;Facilitating the opportunity for the publicand different economic and interestpro-tecting organizations to cooperate in theevaluation and solution of environmentalhealth problems.
3. Problems to be solved
National levelWithout the active involvement of the populationthe environmental health targets cannot be reached.
The principle of sustainability should be builtinto the strategies of all sectors. The conservationand safe exploitation of natural resources shouldbe taken into consideration to ensure – from anecological point of view – long-term improve-ments in the quality of life of the population andthe preservation of diversity in nature.
Regional levelLocal authorities (municipalities) should cooper-ate in the organization and evaluation of environ-mental health studies.
The environmental health status for an extendedarea with similar conditions should be charac-terised as this would lead to a more reliable ap-praisal of the situation.
86
Role of Local Government and NGOs 9. 2
9. 2 Role of Local authorities and NGOs in the implementation
of the Environment and Health Action Programme

Local levelPriority should be given to the approval and con-trol of industrial activities taking into account theprinciple of limiting any harmful impacts on healthor the environment.
In environmental health decision-making, atten-tion should be paid to the different effects of envi-ronmental pollutants.
Local authorities are obliged to monitor the localenvironmental conditions and the impacts on thehealth status of the population, to register relevantdata and to make these available to the public (inaccordance with existing legislation).
4. Programmes in progress
Most local authorities have plans and activities forthe management of parks and green areas andwaste collection and disposal.
As an indication of interest shown by the publicmany organizations have been established in re-cent years with the aim of improving health andpreserving the environment. The appearance ofthese NGOs is favourable and local authoritiesshould pay attention to their views. However, theyshould not depart too much from the necessarybasic environmental health activities.
Local authorities should be willing to coordinatethe work of the different NGOs. Their targets andmethods should be reviewed so that their re-sources could be used to facilitate the implemen-tation of the Action Programme.
5. Tasks to be performed
The following table contains future tasks.
87
9. 2 Role of Local Government and NGOs
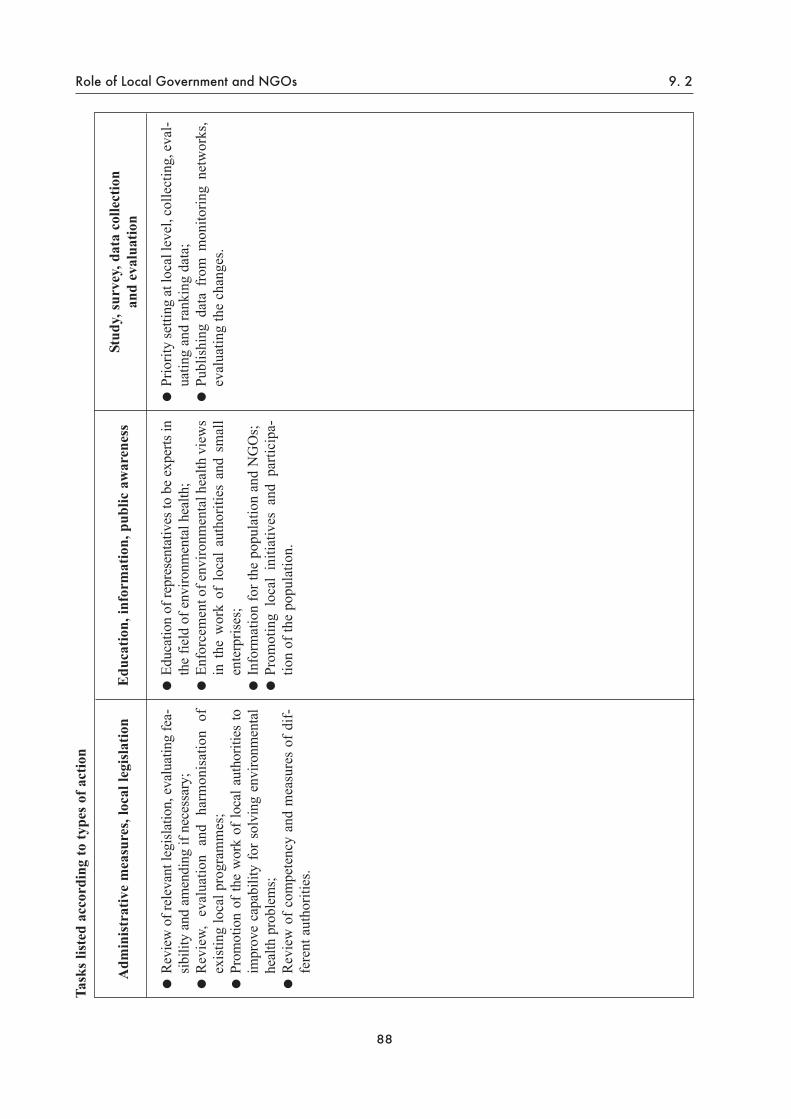
88
Role of Local Government and NGOs 9. 2
Adm
inis
trat
ive
mea
sure
s, lo
cal l
egis
latio
n
Revi
ew o
f rel
evan
t leg
islat
ion,
eva
luat
ing
fea-
sibili
ty a
nd a
men
ding
if n
eces
sary
; R
evie
w,
eval
uatio
n an
d ha
rmon
isat
ion
ofex
istin
g lo
cal p
rogr
amm
es;
Prom
otio
n of
the
wor
k of
loca
l aut
horit
ies
toim
prov
e ca
pabi
lity
for s
olvi
ng e
nviro
nmen
tal
heal
th p
robl
ems;
Rev
iew
of c
ompe
tenc
y an
d m
easu
res
of d
if-fe
rent
aut
horit
ies.
Stud
y, su
rvey
, dat
a co
llect
ion
and
eval
uatio
n
Prio
rity
setti
ng a
t loc
al le
vel,
colle
ctin
g, e
val-
uatin
g an
d ra
nkin
g da
ta;
Publ
ishi
ng d
ata
from
mon
itorin
g ne
twor
ks,
eval
uatin
g th
e ch
ange
s.
Edu
catio
n, in
form
atio
n, p
ublic
aw
aren
ess
Educ
atio
n of
repr
esen
tativ
es to
be
expe
rts in
the
field
of e
nviro
nmen
tal h
ealth
;En
forc
emen
t of e
nviro
nmen
tal h
ealth
vie
ws
in t
he w
ork
of l
ocal
aut
horit
ies
and
smal
len
terp
rises
;In
form
atio
n fo
r the
pop
ulat
ion
and
NG
Os;
Prom
otin
g lo
cal
initi
ativ
es a
nd p
artic
ipa-
tion
of th
e po
pula
tion.
Task
s lis
ted
acco
rdin
g to
type
s of a
ctio
n

1. Environmental health institutions
The network of different institutions all have toanalyse the interrelations between human beingsand the environment, prevent harmful effects andrestore existing damage. These tasks are part ofthe social responsibility of the State.
Because of its special role, the “EnvironmentalHealth Service” should act independently and pur-posefully, being sufficiently sensitive to recognisethe needs and demands of the population, while per-forming its the authoritative duties and activities.
The activity is based on cooperation betweenseveral ministries. The most important ministriesand other bodies are the following:
2. Responsibilities of institutions
In Hungary environmental health issues tradition-ally belong to several ministries. However, in sev-eral respects, the existing system in not sufficient-ly efficient and effective due to fragmentation andoverlapping of responsibilities.
In the following, environmental health functionsare listed with an indication of the responsible mi-nistries and institutions:
89
Environment Health Institutions 9. 3
9. 3 Institutions Responsible for Environmental Health Issues
Ministry of Welfare (NM)National Public Health Service (ÁNTSZ)Ministry for Environment and Regional Policy (KTM)Environmental Inspectorates (KÖFE)Ministry for Traffic, Communication and Water Management (KHVM)Water Management Directorates (VIZIG)Ministry of Agriculture (FM)Agrochemical and Plant Protection Stations (NAK)Veterinary and Food Control Stations (VA)Ministry of Labour (MüM)Ministry of Internal Affairs (BM)Local governmentsMinistry of Defence (HM)Ministry of Industry, Trade and Tourism (IKIM)
Discharges (emissions)Registering and controlling emissions to the environment (air, water, soil) KTM, KHVM, NMRegistering and controlling waste collection and disposal KTM, NMProduction, transport and trading of chemicals IKIM, NMRadiation IKIM, NMMicrobiological factors and vectors FM, NMWork environment MüM, NM

Ambient concentrations (immissons)Air: ambient air quality NM
background concentration KTMtransmission KTM
Water: Surface water KTM, KHVM, NMGroundwater KTM, KHVMDrinking water, recreational water NMMineral water, bottled water NM, FMSewage KHVM, KTM, NM
Soil: Quality, pollution FM, KTMDwellings: Quality, pollutants, urban environment KTM, NMCustomer products, household chemicals NM, IKIM, KTM
Quality assurance and control of food stuff FM, NMMonitoring of health status NM
Revealing harmful impacts NMAnalysis of factors relating to health NMPreventive measures and evaluation NM
Monitoring environmental status KTM
The role of the National Public Health ServiceAnalysis and monitoring with laboratory methods:
Ambient air quality in urban areasIndoor air qualityDrinking water qualityQuality of bathing and surface waterWork environmentDisposal of household wastes (interministerial task)Qualification and disposal of hazardous wastes (interministerial task)Nuisance caused by noise in settlements
Inspection and survey:Health status of population with epidemiological methodsActivities (places of work, settlements, institutions, enterprises)
Control, approval:Work with dangerous materialsUsage of buildings and other establishments
Research:In the field of preventionCauses of infectious and other diseasesImpacts of pollutants on health (air, water, waste, chemicals, physical agents, etc.)
90
9. 3 Environment Health Institutions

Assistance from other organizationsAt university departments of public health, epi-demiology, hygiene and social medicine researchin the different fields of environmental health, epi-demiological studies and provisions for regionalduties are undertaken besides education.
The activity of representatives from NGOs andlocal governments is very useful. For examplethey are actively participating in the WHOHealthy Cities Movement which also involvessome rural settlements and regions
2. Future tasks of the institutions
The future tasks of the environmental health ser-vice should be redefined as part of the healthreform, bearing in mind the results of previousnational and international analyses.
The basic elements should be the following:determination of the duties of the State;improvement of effectiveness;closer cooperation among the competentagencies.
It is essential that the different institutions andagencies performing similar activities coordinatetheir work to avoid unnecessary duplication. Themost important requirement is to clarify the res-ponsibilities of the state.
91
Environment Health Institutions 9. 3
The Ministerial Conference in Helsinki confirmedand declared the need to improve and extendresearch on environmental health issues.
Identification of the possibilities of preventioncannot be achieved without recognising the rela-tionship between causes and effects. Besides themany well-known pollution impacts, new factorshave appeared whose effects are not yet known.The early recognition of damages and monitoringof the exposed population – especially sensitivesubpopulations – are activities of great signifi-cance. The improvement of methodology shouldbe emphasised as well because of the unbelievablyfast technological development.
Analysis of solutions and technical means ori-ented towards improving the present status of theenvironment may also be an important area for theAction Programme.
Research of relevance to environmental healthcannot be separated from other environmental andhealth research activities and it is impossible tomake an exhaustive list.
Research in this field may be divided into fivemain groups:
Identification, qualitative and quantitative de-termination of environmental impacts (physi-cal, chemical, biological) and experimentalstudies of the mechanisms of health effects;Qualitative and quantitative identification ofexpected and real exposure. Methodology ofhow to estimate exposure;Studying the relationship between exposuredose and health effect; qualiative and quanti-tative doseresponse analyses, experimentallyand in human populations;Based on the above work, risk estimation ofthe damage to health and risk analysis;Different forms of risk control and practicalrealization.
1. Ongoing and future epidemiological researchin the field of environmental health
Air pollution and respiratory diseases:Acute and chronic respiratory diseases (asth-ma, allergic syndromes). There is an ongoingepidemiological study – in international co-operation – on the effects of sulphur dioxideand suspended particulates on the occurrenceof respiratory diseases;Measuring indoor air quality; monitoring theeffects of passive smoking; studying the roleof indoor allergens, radon and other physicalfactors; Monitoring some components of air pollu-tants coming from traffic; identification andtesting biological effects of indicator com-pounds (toxicity, genotoxicity, etc.) (lead,benzene, PAH, ect.);Testing and monitoring of carcinogenic airpollutants at molecular level (identificationand methodological development of carcino-genic adducts);Research on the relationship between air pol-lution and the frequency of congenital disor-ders.
Pollution of drinking water, analysis of the appear-ance and biological effects of harmful factors withspecial regard to carcinogenic compounds:
Chlorination by-products (trihalomethanes,MX-type compounds);Epidemiological study in populations con-suming water containing arsenic to revealhealth damages;Analysing microcomponents of naturalwater (mineral and medicinal water);Microbiological pollutants of surface andbathing water – methodological develop-ment (virus diagnostics, using molecularmethods).
Research on the toxic, mutagenic and carcinogeniceffects of chemical factors in the environment:
Study of mutagenic and carcinogenic effectsof pesticides;Analysis of xenobiotics with oestrogeniceffects; prevention of harmful effects.
Improvement of methods for classifying wastes:
92
Environmental Health Research 9. 4
9. 4 Improvement and Support of Environmental Health Research

Introduction of micromethods for identifyingand characterising chemical and microbio-logical pollutants;Development of methods for determinationand analysis of environmental hazards; im-proving ecotoxicological methods.
2. Institutions taking part in environmental research
The national institutes and the relevant faculties ofthe different universities take part in the researchwork. Possibilities should be given to the regionalorganizations and institutions to become involvedinto the elaboration of research programmes,evaluation of results and accomplishing the tasks.
93
9. 4 Environmental Health Research

Today environmental health forms a new branchof science dealing with the single or combinedimpacts and consequences of physical, chemical,microbiological, toxicological, psychological andbiological factors – existing in the natural, socialand urban environments – on individual humanbeings and the whole population. Environmentalhealth practice applies the results of scientificstudies and laboratory activities. Environmentalhealth interventions are preventive in character.The aim is to ensure harmony between the indi-vidual (or the whole population) and the envi-ronment for the benefit of society, bearing in mindthe concept of sustainable development. Educa-tion and training in the field of environmentalhealth can be divided into two main areas:
Specialised training is needed for profes-sionals who are working in this field and,therefore, must acquire a sufficient level ofexpertise;A culture of environmental health should bepart of our life style. It should be an impor-tant element in human behaviour and cus-toms. This cultural side should be recognisedin the everyday life of people. It should berooted in the family and later on formed byschools and other educational institutions.
The culture of environmental health is based onprevention and its goal is to achieve harmonybetween people and the environment in the inter-est of sustainable development.
1. Situation of environmental health education and training
The formation of habits starts in the family andcontinues in kindergarten, then by the institutionaleducational system, to influence future life styleand value systems.
KindergartensKindergartens, as institutions, function accordingto the Law on Public Education teaching childrenbetween 3 and 7 years until they enter school.Education takes the form of special lessons butmost important is the whole way of life in thekindergarten. In the educational programme, envi-ronmental health should be a pedagogical ideawhich inspires the whole lifestyle in the kinder-
garten. The development of children is continu-ously monitored with screening for growth prob-lems and any need for medical and psychologicalhelp so that any deviations can be corrected orcompensated. There are many differences amongkindergartens depending on regional conditions,size, staff and equipment, and consequently, on theeducational programmes. There are hardly anykindergartens where only the minimal require-ments are ensured. In recent years more and morekindergartens have achieved excellent results inthe field of environmental health education.
Primary schoolsThe practice of enrolling pupils in primary schoolsmay be considered exemplary compared withstandards in other European countries. By laweach child should go to a type of school which issuited to its maturity. All children have the right toan education that “corresponds to their interest,maturity and ability”. This requirement, however,does not always meet the ambition, interest andfinancial resources of the parents. Many factors ofthe schooling system jeopardise the health statusof children. Due to the high number of lessons, thelack of physical exercise and hardly any time tostay outdoors, the living conditions of school chil-dren cannot be said to be satisfactory.
Secondary schools and vocational schoolsAt most of the secondary schools and vocationalschools environmental and health education takesplace during the lessons of the principal form teach-er. In other subjects this education depends on thementality and expertise of the particular teacher.
Higher educationAt the institutions of higher education environ-mental health is not properly and satisfactorilytaught.
Postgraduate educationEducation at the postgraduate level is mainlyaimed at training experts who are already workingin the environmental health field.
Education outside the school system, further trainingSpecialised training is most important in this fieldof education.
94
Education and Training 9. 5
9. 5 Education and training in environmental health

2. Health impact
Environmental health education, generally, canonly be expected to have long term and indirectresults. This education, if properly performed, canprevent the effect of existing harmful factors in theenvironment. If this subject is not treated properlyby teaching institutions it can be expected to havea negative effect on the health of the population.
3. Goals to be achieved
The goal of improving environmental healtheducation is to introduce this form of know-ledge – necessary for a healthy everyday life –into all types of teaching institutions, fromkindergartens to universities. Besides this, spe-cial training is needed at expert institutions toteach health workers and other professionalswho will work in this field.
4. Ongoing programmes
KindergartensIn recent years several kindergartens joined thenetwork of the Environmental Educational Centreor are members of KÖRLÁNC (Chain circle).Further training of teachers is a regular activityand information about their experience has beenwidely spread to colleagues.
Primary schoolsThe idea of primary prevention appears in the cur-ricula. The main goal is to instruct and informchildren about a healthy lifestyle.
In practice, the lessons of the principal formteacher (in classes 3–8), biology lessons (in class-es 6–8), “residential schools” (in classes 1–8) and“daycare centres” give an opportunity for this kindof education. In the practice of teachers the appli-cation of new pedagogical methods like those ofWaldorf, Freinet and Rogers, Montessori and“Gesamtschule” has meant a positive change.These methods represent new directions in peda-gogical practice emphasising the relationshipbetween environment and human beings, theirlifestyle and basic values. In the school system thefollowing alternative methods have been intro-duced since 1986:
Programme of “transmitting values anddeveloping skills” led by Dr J. Zsolnai where
children gain basic knowledge of environ-ment and health issues in the frame of thesubject “Human nature”. The programmehas been developed for 8 class levels, andteachers are assisted by special teaching ma-terial;The plan of teaching called “Fifty-fifty” hasbeen available since 1990. In the frame of“nature” and “social issues” important ex-amples of the damage done by human beingsare analysed; An alternative curriculum for biology waspublished in 1991. Lessons on physiology andevolution – containing environment and healthtopics as well – are included for the 8 class lev-els of primary school; “Forest schools” were started in 1986, mean-ing that lessons are held in the “classroom ofnature”. Students make observations, study-ing the characteristics of the given naturalenvironment. The value of this form is tolearn to work together and it may have animpact on the future lifestyle of the childrenas well.
Secondary schoolsIn the 1980s a new programme called “Mankind andNature” was started. It was elaborated for schoolswhere the curriculum does not include biology as anindependent subject. The programme has been fur-ther developed by the schools and also serves asbasic material for the “special schools” that giveparticular emphasis to biology or other subjects. In“vocational schools” the subject is taught in theframe of occupational health and safety.
The tuition is not comprehensive, consistingonly of special and firstaid issues relating to thegiven trade. In secondary schools for health work-ers (nurses, laboratory assistants, emergency staff,etc.) environmental health is an independent sub-ject. This is to supplement traditional subjects likehygiene and epidemiology.
Higher educationAt the universities and special colleges medicaldoctors, dentists, pharmacists, hygienists, ambu-lance officers, nurses, etc. are trained, but envi-ronmental health is not included as a special sub-ject. This topic is taught in the frame of other sub-jects and the emphasis given depends on the atti-tude of the lecturers and the number of lessons.
95
9. 5 Education and Training

To improve the general understanding of environ-mental health problems, the education of teachers isvery important. The main goal of the education ofteachers is to prepare them for improving the wholepersonality of the child. Forming behaviour andcustoms in childhood is a part of the tuition. In theframe of other topics such as training for familylife, home economics, nature and health education,environment and health are given considerableemphasis. In pedagogy and psychology, studentslearn about developmental disorders, the causes andmethods for correction and compensation.
The effect of this education depends on the atti-tude of the teachers, their personal beliefs andconvictions. As the teachers are generally over-burdened the results do not always live up to theaims.
Post-graduate and extracurricular educationIn this field the following forms of education areavailable:
Education of medical doctors specialising inpublic health and hygiene (including envi-ronmental health), epidemiology, occupa-tional health, etc;Special courses for health managers, publichealth medical officers, infectious diseaseepidemiologists, etc. It is planned to be estab-lish in the near future a public health school.
Project activitiesEnvironmental health education and training issupported by special projects frequently in co-operation with international organizations or indi-vidual countries.
In 1992 Hungary joined a programmeoffered by the UN. By 1996 2,000 teacherswere to be trained. Each school gets theprogramme, adapted to Hungarian condi-tions, free. This programme can be used bothin primary and secondary schools for teach-ing health issues; Among the environmental projects support-ed by PHARE is a postgraduate programmefor teachers, including environmental healthissues;A programme supported by the Swiss gov-ernment to make the school curriculum“green”. Special courses are organized andsuggestions given as to how to the topic canbe integrated into other subjects;
The DADA programme developed in theUSA, against smoking, drug use and the pre-vention of AIDS. This programme is beingused by many schools in Budapest withpolice assistance;A European measuring programme for theimpact of ozone and acid rain, initiated byNorway. About 1,000 Hungarian schools areparticipating in the programme;Movements and campaigns for selectivewaste collection; applications for grants andcompetitions; celebration of environmentallyimportant occasions; and the “cleaning up”movement, are all significant activities;The KÖRLÁNC (Chain circle) projectinvolves hundreds of schools, kindergartensand teacher training institutions. Its maintask is to inform and help with organizingconferences and publishing literature;The Soros Foundation, Tempus Programme,Fact Foundation and other similar sourceshelp with environment and health educationby giving possibilities for financial support.
The work of the Environment and Nature ProtectionCentre is important as well. For more than twentyyears this centre has been organizing programmes atdifferent schools on environment topics.
Several NGOs deal with education and informa-tion. The task of these organizations is first of allpractical activities in the field of environment andhealth.
The media have an important role in informingand educating the public about positive attitudesand behaviour. Radio and television have broad-cast many programmes of this kind in recent yearswhich seems to have a positive impact on publicopinion.
In the environmental health education pro-gramme, journals and books play an importantrole as well. Ministries and different organizationssupport such publications but the choice of teach-ing material is not yet satisfactory.
5. Tasks to be performed
Education is one of the preventive tools showingresults only in a long term perspective. Changingpublic attitudes, customs and behaviour in a positivedirection is the ultimate aim of health promotion.
The following table outlines future tasks.
96
Education and Training 9. 5
97
9. 5 Education and Training
Prac
tical
task
s(o
rgan
izat
ion,
con
trol
)
Spec
ial f
urth
er tr
aini
ng fo
r sch
ool
and
kind
erga
rten
teac
hers
;Sp
read
ing
info
rmat
ion
in s
peci
aljo
urna
ls,
info
rmin
g as
soci
atio
nsan
d ex
pert
grou
ps;
Impr
ovem
ent
of
info
rmat
ion
syst
em a
nd m
etho
ds o
n to
pics
rela
ting
to e
nviro
nmen
tal h
ealth
;D
eman
d fo
r th
e m
edia
to ta
ke a
grea
ter
part
in i
nfor
min
g th
epu
blic
to im
prov
e pu
blic
aw
are-
ness
;A
genc
ies f
or re
gula
r inf
orm
atio
nof
the
publ
ic;
Proj
ects
invo
lvin
g lo
cal p
opul
a-tio
n, N
GO
s, sc
hool
s an
d lo
cal
auth
oriti
es;
Invo
lvem
ent
of f
amily
doc
tors
,pr
ovid
ing
them
with
lite
ratu
re.
Info
rmat
ion,
edu
catio
n,
publ
ic a
war
enes
s
Educ
atio
n sh
ould
inc
lude
soc
ial
fact
ors
as w
ell p
layi
ng a
sig
nifi-
cant
role
in e
nviro
nmen
tal h
ealth
issu
es;
Educ
atio
n is
one
of
the
long
-te
rm m
etho
ds. P
ublic
aw
aren
ess
is
impo
rtant
to
fo
rm
prop
erbe
havi
our a
s the
bas
ic e
lem
ent i
nth
e pr
even
tion
of d
isea
ses;
Task
s of
ed
ucat
ion
can
beac
com
plis
hed
only
with
wid
e-sp
read
coo
pera
tion.
Adm
inis
trat
ive
mea
sure
s(te
chni
cal,
legi
slat
ive)
Clo
se c
oope
ratio
n am
ong
go-
vern
men
tal
agen
cies
an
dN
GO
s,
educ
atio
nal
and
rese
arch
ins
titut
ions
and
the
med
ia in
volv
ing
the
publ
ic;
Wid
espr
ead
info
rmat
ion
for t
hepu
blic
abo
ut t
he r
esul
ts o
f th
esu
cces
sful
loca
l ini
tiativ
es;
Educ
atio
n on
env
ironm
enta
lhe
alth
topi
cs s
houl
d be
incl
ud-
ed i
n th
e ed
ucat
iona
l pr
og-
ram
mes
at a
ll le
vels
;A
dvis
ory
syst
em
is
need
edin
volv
ing
the
loca
l Pu
blic
Hea
lth S
ervi
ces
for
info
rmin
gth
e pu
blic
;Su
ppor
t of
dis
able
d pe
ople
is
spec
ially
impo
rtant
bas
ed o
n th
etra
ditio
nally
goo
d pr
actic
e in
Hun
gary
(e.g
. Pet
ô In
stitu
te).
Inth
e sa
me
time
the
who
le p
opu-
latio
n is
to b
e ed
ucat
ed fo
r tol
-er
ance
.
Stud
y, su
rvey
, dat
a co
llect
ion
Prom
otio
n of
loca
l edu
catio
nal
sche
mes
com
plyi
ng w
ith t
hena
tiona
l sc
hedu
le.
Expe
rtssh
ould
take
par
t in
the
elab
ora-
tion
of to
pics
on
envi
ronm
enta
lhe
alth
.
Task
s lis
ted
acco
rdin
g to
type
s of a
ctio
n

The occurrence and negative effects of environ-ment problems frequently extend across nationalborders so that countries are not able to find solu-tions in isolation.
The Helsinki Conference stated, that the Euro-pean Environmental Health Action Programmeshould be established as a result of a widespreadinternational cooperative effort. This process hasbeen confirmed by the initiation of the “PilotProject Programme” in which Hungary is one ofthe participants.
1. Present cooperation
Hungary is actively engaged in international coop-eration is several environmental health field.Among the many different forms of cooperation,participation in several WHO programmes – relat-ed to environmental hazards with an impact onhealth – should particularly be mentioned.
WHO
EUROHEALTH. Extensive research hasbeen going on in the frame of WHO pro-grammes, not only in the field of environ-mental health, but also prevention in generaland primary health care;National Integrated Programme on En-vironment and Health (NIPEH) has been themost important programme during the pastthree years. Although it has been terminated,some of its subprograms – like improvementof information systems – will be continued inthe coming years;Environmental health education – coopera-tion to set up a programme for a school ofpublic health;Extending the Basic Environmental HealthTraining course.
98
International Relations 10.
10. International Relations

Hungarian Environmental Health Action Programme (NEHAP)
Abbreviations
NPHS National Public Health Service (Hun.)MoIA Ministry of Internal Affairs (Hun.)BTX Benzene, Toluene, XyleneCET Concern for Europe’s Tomorrow.
(Health and the Environment in the WHO European Region, 1995)CINDI Countrywide Integrated Noncommunicable Disease InterventionDADA Programme agaist tobacco, drog, alcohol and AIDSDDT Dichlor-diphenyl-trichloroethaneECEH European Centre on Environment and HealthEEC European Economic CommunityEHAPE Environmental Health Action Plan for EuropeEHIS Environmental Health Information SystemÉM or ÉVM Ministry responsible for constructions work (Hun.)EPI Extended Programme of ImmunizationEU European UnionEUROHEALTH WHO Regional committee programme supporting Central-Eastern European CountriesMoA Ministry of Agriculture (Hun.)GERMON Network operated by the WHO for exchanging dataGIS Geographic Information SystemGLP Good Laboratory PracticeHCB HexachlorobenzeneHCH Hexachloro-cyclohexaneHEHAP Hungarian Environmental Health Action ProgrammeHFA Health for All by the Year 2000HM Ministry of Defence (Hun.) HPLC High Pressure Liquid ChromatographyIKIM Ministry of Industry, Trade and Tourism (Hun.)ILO International Labour OfficeKHVM Ministry for Transport, Communication and Water Management (Hun.)KKA Central Environmental Protection Fund (Hun.)KÖFE: Environmental Inspectorates (Hun.)KÖRLÁNC “Chain circle” project (Hun.)KTM Ministry for Environment and Regional Policy (Hun.)MM Ministry of Labour (Hun.)MMMF Manmade Mineral FibresNAK Agrochemical and Plant Protection Stations (Hun.)NEP National Environmental Programme (Hun.)NEXT Nationwide Evaluation of X-ray TrendsNGO Non-Governmental OrganizationNIPEH National Integrated Programme of Environment and HealthMÜM Ministry of Welfare (Hun.)OECD Organization of Economic Cooperation and DevelopmentOKSER National Radiation Control System (Hun.)PAHs Polycyclic aromatic hydrocarbonsPCBs Polychlorinated biphenylsPHARE Polish and Hungarian Assistance for the Reconstruction of EconomyPIC Prior Informed Consent
99

PVC Polyvinyl chlorideSPLUS Statistical Programme for Spatial AnalysisUN/ECE United Nations Economic Commission for EuropeUNCED United Nations Conference on Environment and DevelopmentVIZIG Water management Directorates (Hun.)VOC Volatile Organic CompoundsWHO World Health Organization
100

















