Human Factors in Medical Devices ● Alan Coulson ● Software Engineer ● LifeScan Scotland Ltd.
32
Human Factors in Medical Devices Alan Coulson Software Engineer LifeScan Scotland Ltd
-
Upload
emery-gerald-jefferson -
Category
Documents
-
view
218 -
download
0
Transcript of Human Factors in Medical Devices ● Alan Coulson ● Software Engineer ● LifeScan Scotland Ltd.

Human Factors in Medical Devices
Alan Coulson Software Engineer LifeScan Scotland Ltd

Usability
Design Examples Tools Summary
Toyota Prius gear stick

Design
• Objects and machines we use in everyday life must all be designed.
• Adding features often gives competitive edge in the marketplace, often at the expense of simplicity and usability.An office water dispenser

Design

Design

Design

Human Error?
• People tend to blame others (or themselves) when things go wrong
• Hence the term ‘human error’
• Often, its bad design that leads people to make errors.
“The following factors contributed to the incorrect response of the flight crew:
[…]
3. They did not assimilate the indications on the engine instrument display before they throttled back the No. 2 engine”
AAIB report into Kegworth Air Disaster Jan 1989

Human Error?
“Although there seems to be no question that the EIS display on the Boeing 737 provides accurate and reliable information to the crew, the overall layout of the displays, […] do appear to require further consideration.
These factors should not be ignored and the suitability of such new displays for use by airline pilots should be evaluated before they are brought into use”.
AAIB report into Kegworth Air Disaster Jan 1989

Medical example
• Therac 25• Contributory factors:
• Removal of ‘redundancy’ on the user interface
• Poor software design and testing
• Poor error messages
http://neptune.netcomp.monash.edu.au/cpe9001/assets/readings/Therac-3.GIF
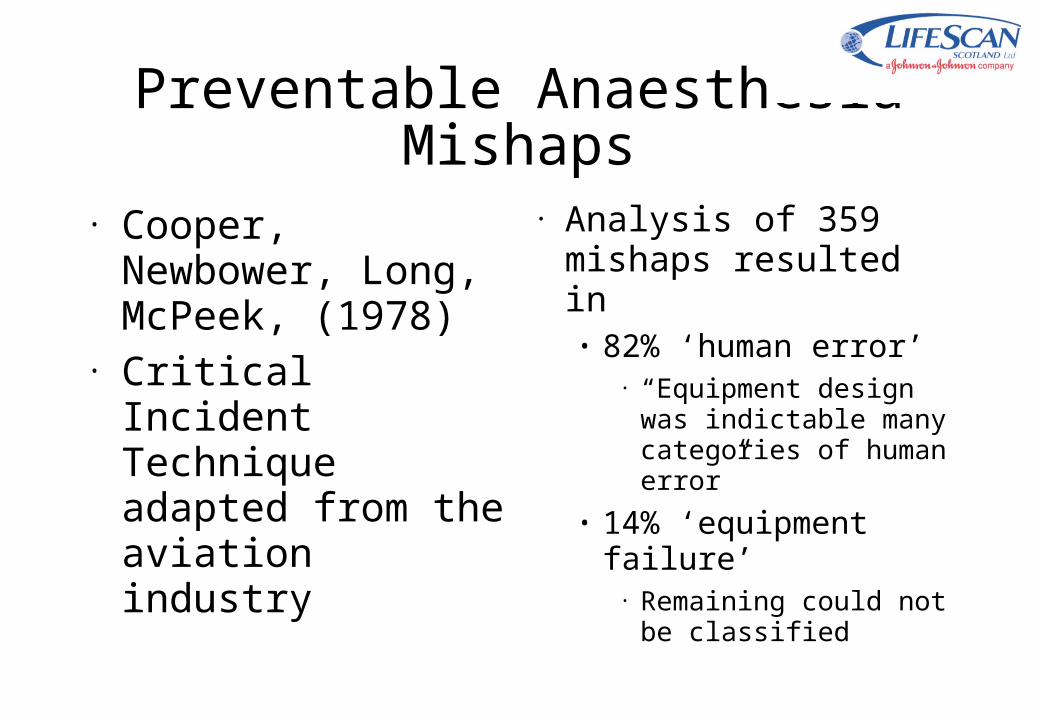
Preventable Anaesthesia Mishaps
• Analysis of 359 mishaps resulted in
• 82% ‘human error’• “Equipment design was
indictable many categories of human error”
• 14% ‘equipment failure’
• Remaining could not be classified
• Cooper, Newbower, Long, McPeek, (1978)
• Critical Incident Technique adapted from the aviation industry

Design

Design
• “Human errors in medical device use account for a large portion of medical errors
• Most of these errors are due to inappropriate designs for user interactions, rather than mechanical failures”
• Zhang J., Patel, V. L., Johnson, T.R., Chung, P., Turley, J.P 2005

FDA
• FDA actively promote and require “Human Factors” in design of medical devices– “Do it by Design” 1996– “Medical Device Use-safety:
Incorporating Human Factors Engineering into Risk Management”, 2000
– Manufacturer and User Facility Device Experience Database - (MAUDE)
• (amazing how similar these reports are to AAIB reports!)
From: http://www.fda.gov/cdrh/annual/fy2000/ohip/reduseerror.html

Patient-use Medical Device

Risk Management
• In the context of medical devices, FDA define a hazard as a potential source of harm arising from
• Medical treatment
• Device failure
• Device use

Design and Evaluation Tools
• Fortunately there are some tools available to help

Design and Evaluation Tools
• Fortunately there are some tools available to help

Design and Evaluation Tools
• How can these tools be used?
– In gathering requirements
– By designers and engineers
– By prospective purchasers

Design and Evaluation Tools
• Heuristic Evaluation• Cognitive Walkthrough• Design Principles
Tool #1: Heuristics
• Visibility of system status • Match between system and the real world • User control and freedom • Consistency and standards • Error prevention • Recognition rather than recall • Flexibility and efficiency of use • Aesthetic and minimalist design • Help users recognize, diagnose, and recover from errors • Help and documentation
Nielsen: http://www.useit.com/papers/heuristic/heuristic_list.html

Heuristic Evaluation
• Rate the usability of an object according to the heuristics

Heuristic Evaluation
• Rate the usability of an object according to the heuristics
• E.g. This example fails heuristic #2 (match between system and real world)
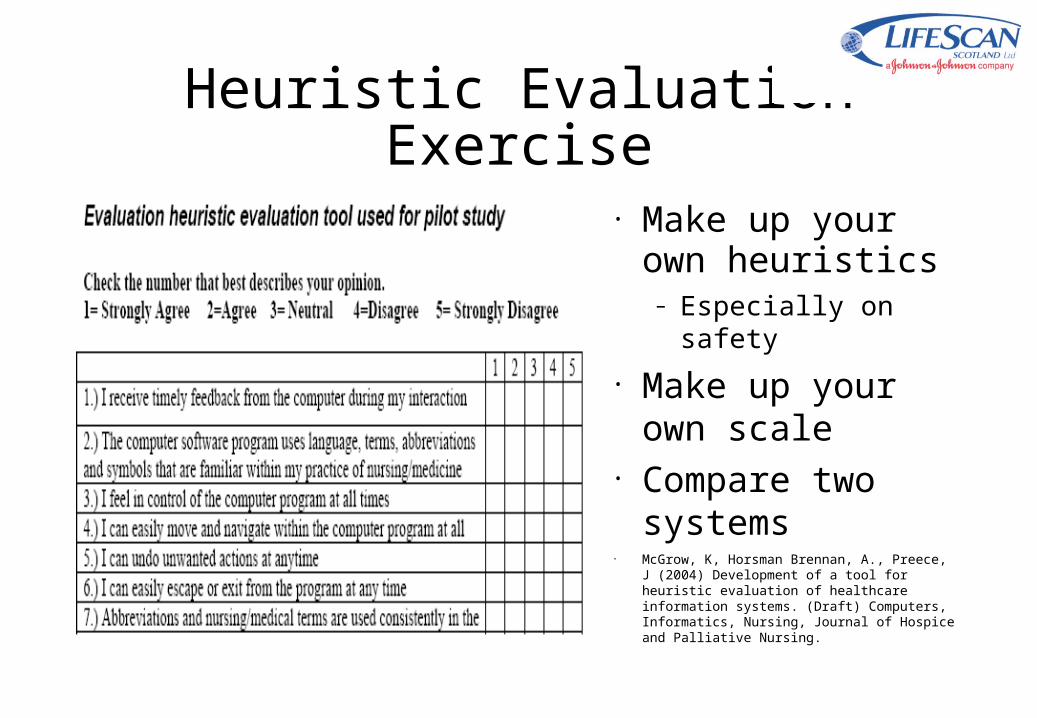
Heuristic Evaluation Exercise
• Make up your own heuristics
– Especially on safety
• Make up your own scale
• Compare two systems
• McGrow, K, Horsman Brennan, A., Preece, J (2004) Development of a tool for heuristic evaluation of healthcare information systems. (Draft) Computers, Informatics, Nursing, Journal of Hospice and Palliative Nursing.

Heuristic Evaluation Exercise

Tool #2: Cognitive Walkthrough
• Wharton, et al, 1993.• Evaluates the steps required to carry out a task• Attempts to uncover mismatches between how a
user and how a designer thinks about a task.• You need
• System (actual, simulated, or prototype)• Task scenario.• To know who the intended user is

Cognitive Walkthrough
• Step 0 – select task to be performed and list all actions to be performed
• For each action…• Step 1 – explore system
looking for action• Step 2 – select most
appropriate action• Step 3 – interpret system’s
response

Cognitive walkthrough
• At each step ask• Does the user know
what to do next• Is there a connection
between the correct action and what the user is trying to do?
• Will the user know they have made the right (or wrong) choice?
Task/Goal: Measure Blood Glucose Level
User Action System Response
Is the action correct evident?
Is there a connection between the action and the task?
Will the user know if the have made the correct choice?
... ... ... ... ...
Insert strip System turns on
No. There is no ‘on’ button so the user may not realize that the way to turn the thing on is by inserting a strip
Possibly. The user will know that the strip has something to do with the Task and there is only one obvious place to insert the strip
Yes – the meter powers on and the LCD ‘lights up’
...

Tool #3: Design Principles
• These principles are at a higher level than heuristics
• Affordance
• Visibility
• Feedback
• Simplicity
• Structure
• Consistency
• Tolerance

Example
Affords turning, but feedback was poor

Summary
Usability of medical devices is significant in minimising risk to patients
Usability has to be designed in – it’s not sufficient to say ‘it was human error’ after the fact
Use simple tools to evaluate usability of medical devices and systems.
The system with the most “utility” is not necessarily the most “usable”

However… In “Making Medical
devices more User-Friendly”, Wiklund states “Experienced designers [of medical devices] suggest limiting the colour palette of a user interface”
However…

However... A hospital chain in the
US is taping over patients' LiveStrong wristbands because they are yellow - the same colour as the "do not resuscitate" bands it puts on patients who do not want to be saved if their heart stops.
![[Noel James Coulson] a History of Islamic Law](https://static.fdocuments.in/doc/165x107/545f7647b1af9f16598b4c47/noel-james-coulson-a-history-of-islamic-law.jpg)