Human Factors and Ergonomics in Health Care and Patient … · Human Factors and Ergonomics in...
35
1 of 35 Human Factors and Ergonomics in Health Care and Patient Safety Pascale Carayon, Ph.D. Procter & Gamble Bascom Professor in Total Quality Department of Industrial and Systems Engineering Director of the Center for Quality and Productivity Improvement University of Wisconsin-Madison - USA IX International Ergonomics Congress of SEMAC – April 2007 – Mexico City, Mexico
Transcript of Human Factors and Ergonomics in Health Care and Patient … · Human Factors and Ergonomics in...

1 of 35
Human Factors and Ergonomics in Health Care and Patient Safety
Pascale Carayon, Ph.D.Procter & Gamble Bascom Professor in Total Quality
Department of Industrial and Systems EngineeringDirector of the Center for Quality and Productivity Improvement
University of Wisconsin-Madison - USA
IX International Ergonomics Congress of SEMAC – April 2007 – Mexico City, Mexico

2 of 35
What’s the problem?US – health care expenditures = 13% GNPInstitute of Medicine – 1999 – Report on medical errors and patient safety:
44,000 to 98,000 Americans die in hospitals each year as a result of medical errors.
Canada:about 185,000 of the 2.5 million annual hospital admissions associated with an adverse event

3 of 35
Mexico?

4 of 35
WHO World Alliance for Patient Safety
http://www.who.int/patientsafety/en/

5 of 35
Institute of Medicine-2001Crossing the Quality Chasm
“Health care has safety and quality problems because it relies on outmoded systems of work. If we want safer, higher-quality care, we will need to have redesigned systems of care, including the use of information technology to support clinical and administrative processes.”(p. 4)

6 of 35
Progress toward understanding patient safety
IOM’2000 Report – To Err is HumanIOM’2001 Report – Crossing the Quality ChasmIOM’2003 Report – Patient Safety – Achieving a New Standard for CareIOM’2003 Report – Keeping Patients SafeIOM’2006 Report – Preventing Medication Errors
Human error / System approachesDesign of information technologyImportance of human factors

7 of 35
HFE expertise in healthcare organizations
Employee health:occupational safety & health, ergonomics
Quality improvement:
process analysisPurchasing of equipment:
usability
Risk management:incident reporting, event
analysis
OR and critical care:teamwork,
communication

8 of 35
51 chapters:•Human error•Sociotechnical systems and macroergonomics•Technology, medical devices•Physical ergonomics•Methods and tools•Various care settings•…

9 of 35
Take-home messages
1. A human factors perspective can provide useful, important information on systemicfactors that contribute to patient safety.
2. Need to integrate human factors in the design of healthcare technologies, systems and processes.

10 of 35
Based on research on human factors in…
… health care and patient safety
Funding from the Agency for Healthcare Research and Quality
http://www2.fpm.wisc.edu/seips/

11 of 35

12 of 35
Leape et al. (1995) “Systems analysis of adverse drug events” JAMA
Causes of medication errors:•lack of knowledge of drug•faulty dose checking•setting up of infusion pump

13 of 35
Medication administration technologies

14 of 35
Safe Medication Administration through Technologies and Human Factors –SMArTHF
Aims of the project:1. To determine the effect of Smart IV Pump technology
implementation and integration with BCMA technology on medication errors.
2. To determine the impact of Smart IV pumps and the integration with BCMA technology on end users.
3. To describe a human factors prospective error analysis and to qualitatively evaluate its effectiveness on the implementation success of technology in an acute care hospital setting.
http://cqpi2.engr.wisc.edu/smarthf/index.html

15 of 35
Multidisciplinary research team
Pascale Carayon (PI)Tosha Wetterneck (co-PI)Roger BrownJoshua De SilveyMyra EnloeAnn Schoofs HundtQian LiMark LinzerTracy Love
Brad LudwigSusan KleppinMustafa OzkaynakPrashant RamSteve RoughTanita RobertsMark SchroederSade Sobande
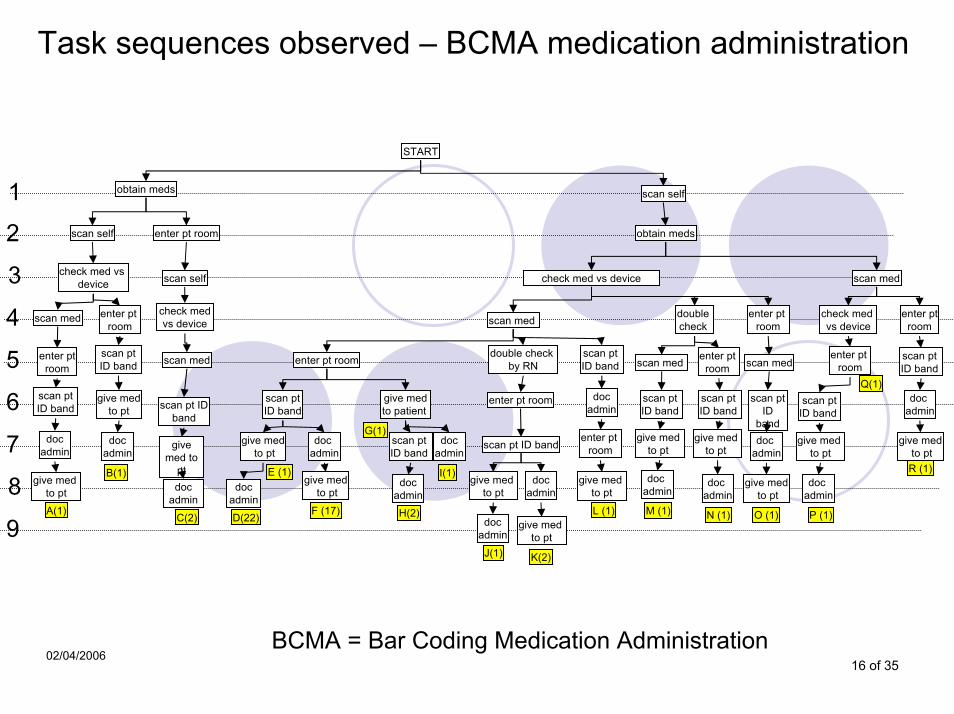
16 of 35
Task sequences observed – BCMA medication administration
scan self
obtain meds
check med vs device
enter pt room
scan med
scan med
doc admin
double check
enter pt room
M (1)
give med to pt
scan pt ID band
doc admin
N (1)
give med to pt
scan pt ID band
enter pt room
scan med
scan pt ID
banddoc
admin
give medto pt
O (1)
scan med
check med vs device
enter pt room
scan ptID band
Q(1)
give med to pt
doc admin
P (1)
scan ptID band
D(22)
E (1)doc
admin
doc admin
give medto pt
give medto pt
F (17)
give medto patient
G(1)scan pt ID band
docadmin
I(1)doc
admin
H(2)
double check by RN
scan pt ID band
give med to pt
docadmin
J(1)
enter pt room
docadmin
give med to pt
K(2)
START
obtain meds
scan pt ID band
A(1)
give med to pt
docadmin
scan self enter pt room
check med vsdevice
scan med enter pt room
enter ptroom
scan ptID band
give medto pt
docadmin
B(1)
scan self
check medvs device
scan med
scan pt ID band
give med to
ptdoc
admin
C(2)
scan pt ID band
docadmin
enter pt room
L (1)
give med to pt
enter ptroom
scan pt ID band
doc admin
R (1)
give medto pt
1
9
3
2
5
4
7
6
8
BCMA = Bar Coding Medication Administration02/04/2006

17 of 35
Work system factors observed in BCMA medication administration
Tasks:Potentially unsafe med. admin.
Person:Patient in isolation
Environment:Messy, insufficient light
Technology:Automation surprises, malfunctions
Organization:interruptions
Technologyand Tools
Organization
EnvironmentTasks
Person
Technologyand Tools
Organization
EnvironmentTasks
Person
18 of 35
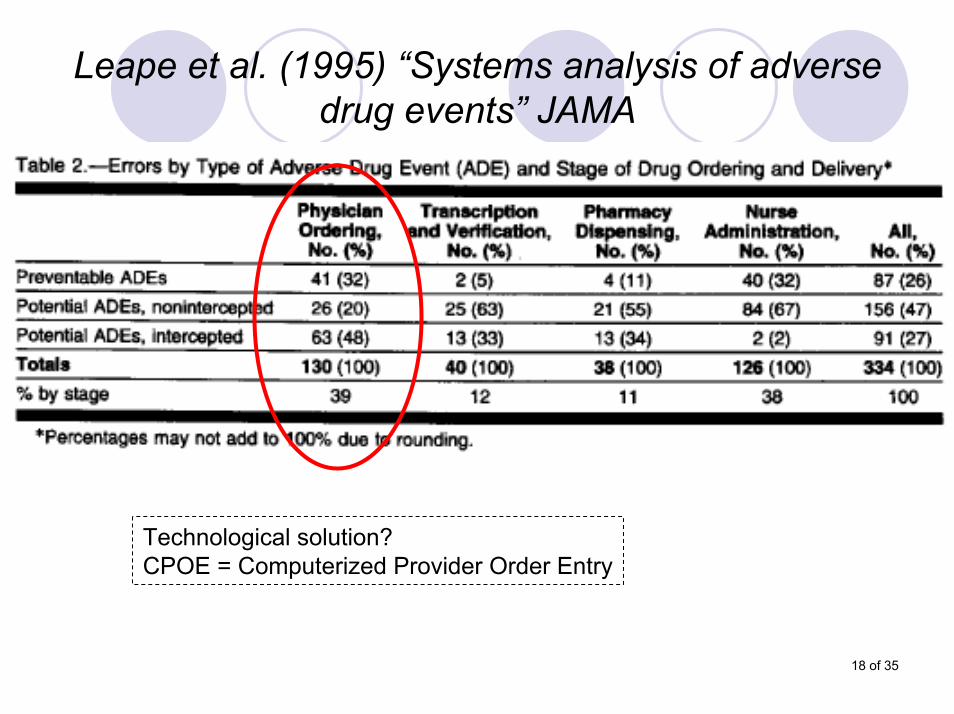
Leape et al. (1995) “Systems analysis of adverse drug events” JAMA
Technological solution?CPOE = Computerized Provider Order Entry

19 of 35
CPOE Implementation in ICUs

20 of 35

21 of 35
Intensive Care Unit (ICU)

22 of 35
How does a medication order look like?

23 of 35

24 of 35
CPOE Implementation in ICUs
Aims of the project:1. To determine the effect of CPOE on safety and
quality of care in ICUs.2. To determine the impact of CPOE on end users
(physicians, pharmacists, nurses, respiratory therapists) in ICUs.
3. To determine the financial value of CPOE implementation.
4. To examine the impact of prospective human factors error analysis in CPOE implementation.
http://cqpi2.engr.wisc.edu/cpoe/index.htm

25 of 35
Usability training at Geisinger
September 20-21’2006

26 of 35

27 of 35
178 medication incidents in 7 months

28 of 35
Probably the first (modern) study on medication errors…
… was conducted by Alphonse Chapanis (1960).

29 of 35
What can we do today so that 40 years from now human factors concepts and methods will have made a difference in
the safety of patient care?
30 of 35
Understanding the characteristics of health care:Complexity‘People’ industryTechnologyCriticalityVariety of care settings: hospital, outpatient, home,…
Partnership with health careSystemic effects or ‘unintended consequences’Impact

31 of 35
Need for HFE (intervention) research…
…that will contribute to care that is:safeeffectivepatient-centeredtimelyefficientequitable

32 of 35
HFE in Healthcare DeliveryResearch needs
Major issues facing health care and patient safety:
Workload of healthcare providersMedical errors and adverse events: identification, management, review, recoveryReliability of systems, processes and technologiesPatient safety in a variety of settingsTransitions of careMedical devices and healthcare information technology

33 of 35
Take-home messages
1. A human factors perspective can provide useful, important information on systemicfactors that contribute to patient safety.
2. Need to integrate human factors in the design of healthcare technologies, systems and processes.

34 of 35
Lucian Leape in Ergonomics in Design – Summer’2004
“Given the complexity of health care and the formidable obstacles it presents to change, to overcome those barriers and create a safe culture does indeed seem to
be the ultimate challenge for those who specialize in human factors.”

35 of 35