Human Epidermal Growth Factor Receptor 2 Testing in Gastroesophageal Cancer: Correlation Between...
6
Human Epidermal Growth Factor Receptor 2 Testing in Gastroesophageal Cancer Correlation Between Immunohistochemistry and Fluorescence In Situ Hybridization Laura J. Tafe, MD; Yelena Y. Janjigian, MD; Michael Zaidinski, MT; Cyrus V. Hedvat, MD, PhD; Meera R. Hameed, MD; Laura H. Tang, MD, PhD; James B. Hicks, PhD; Manish A. Shah, MD; Violetta Barbashina, MD N Context.—Patients with advanced gastroesophageal can- cer have poor survival with current therapy. Human epidermal growth factor receptor 2 (HER2) represents a promising therapeutic target, but the optimal HER2 testing strategy is not yet defined. Objectives.—To evaluate the concordance between immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH) and to determine if the American Society of Clinical Oncology/College of American Pathol- ogists HER2 scoring system is applicable to gastroesoph- ageal carcinomas. Design.—Formalin-fixed paraffin-embedded tumor sam- ples from patients with advanced stage gastroesophageal cancer were tested by IHC and FISH and scored according to the American Society of Clinical Oncology/College of American Pathologists criteria for breast cancer. Concor- dance between IHC and FISH was evaluated. A subset of cases was subjected to array comparative genomic hybrid- ization to verify the positive and negative HER2 results. Results.—A total of 135 cases with paired IHC and FISH results were evaluated. The majority of samples (84%) were biopsies. HER2 amplification was detected in 20 tumors (15%). Using the American Society of Clinical Oncology/College of American Pathologists scoring sys- tem, IHC-FISH concordance was 97% for IHC 0, 93% for IHC 1+, and 100% for IHC 3+. Human epidermal growth factor receptor 2 positivity was strongly associated with tumor grade (moderately differentiated . poorly differen- tiated, P , .001) and histologic subtype (intestinal . diffuse, P = .007). Array comparative genomic hybridiza- tion analysis was successful in 31 tumors (14 FISH+ and 17 FISH2). Fluorescence in situ hybridization and array comparative genomic hybridization results were highly concordant in both HER2-positive and HER2-negative groups (93% and 100% concordance, respectively). Conclusions.—Human epidermal growth factor receptor 2 testing in gastroesophageal cancer can be performed using standard breast cancer procedures and the American Society of Clinical Oncology/College of American Pathol- ogists scoring criteria. Although IHC 0 and IHC 3+ provide clear stratification, reliable separation of IHC 1+ and IHC 2+ may be difficult, especially in biopsy samples. The latter 2 groups are best referred to FISH for definitive classifi- cation. (Arch Pathol Lab Med. 2011;135:1460–1465; doi: 10.5858/arpa.2010-0541-OA) G astroesophageal cancer is a global health problem with approximately 800 000 deaths reported annu- ally. 1 Because the tumor produces no specific symptoms in its early stages, patients commonly present with advanced or metastatic disease where current therapies can offer only marginal benefit. 2 It is hoped that optimization of chemotherapy regimens and the addition of targeted agents directed at specific molecular pathways will result in better patient outcomes. Human epidermal growth factor receptor 2 (HER2) represents a promising therapeutic target. The HER2 gene is a proto-oncogene located on chromosome 17q11–12. It encodes a transmembrane receptor tyrosine kinase, a member of the epidermal growth factor receptor family known to play an important role in cell proliferation and survival. Oncogenic activation of HER2 commonly occurs through gene amplification, which results in protein overexpression on the cell membrane, leading to abnormal cell signaling and cell growth. The importance of HER2 is well established in breast cancer, where HER2 testing has become a standard approach to select appropriate systemic therapy and identify patients who may benefit from the HER2-targeted agents, such as trastuzumab and lapatinib. Accepted for publication January 31, 2011. From the Departments of Pathology (Drs Tafe, Hedvat, Hameed, Tang, and Barbashina and Mr Zaidinski) and Medicine (Drs Janjigian and Shah), Memorial Sloan-Kettering Cancer Center, New York, New York; and Cancer Genetics, Cold Spring Harbor Laboratory, Cold Spring Harbor, New York (Dr Hicks). Dr Tafe is currently affiliated with the Department of Pathology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire. Dr Barbashina is currently affiliated with the Breakthrough Breast Cancer Research Centre, Institute of Cancer Research, London, United Kingdom. The authors have no relevant financial interest in the products or companies described in this article. Presented in part at the annual meeting of the United States and Canadian Academy of Pathology, Washington, DC, March 22, 2010. Reprints: Violetta Barbashina, MD, The Breakthrough Breast Cancer Research Centre, Institute of Cancer Research, 237 Fulham Rd, London SW3 6JB, United Kingdom (e-mail: [email protected]). Original Articles 1460 Arch Pathol Lab Med—Vol 135, November 2011 HER2 Testing in Gastroesophageal Cancer—Tafe et al
Transcript of Human Epidermal Growth Factor Receptor 2 Testing in Gastroesophageal Cancer: Correlation Between...

Human Epidermal Growth Factor Receptor 2 Testing inGastroesophageal Cancer
Correlation Between Immunohistochemistry and Fluorescence InSitu Hybridization
Laura J. Tafe, MD; Yelena Y. Janjigian, MD; Michael Zaidinski, MT; Cyrus V. Hedvat, MD, PhD; Meera R. Hameed, MD;Laura H. Tang, MD, PhD; James B. Hicks, PhD; Manish A. Shah, MD; Violetta Barbashina, MD
N Context.—Patients with advanced gastroesophageal can-cer have poor survival with current therapy. Humanepidermal growth factor receptor 2 (HER2) represents apromising therapeutic target, but the optimal HER2 testingstrategy is not yet defined.
Objectives.—To evaluate the concordance betweenimmunohistochemistry (IHC) and fluorescence in situhybridization (FISH) and to determine if the AmericanSociety of Clinical Oncology/College of American Pathol-ogists HER2 scoring system is applicable to gastroesoph-ageal carcinomas.
Design.—Formalin-fixed paraffin-embedded tumor sam-ples from patients with advanced stage gastroesophagealcancer were tested by IHC and FISH and scored accordingto the American Society of Clinical Oncology/College ofAmerican Pathologists criteria for breast cancer. Concor-dance between IHC and FISH was evaluated. A subset ofcases was subjected to array comparative genomic hybrid-ization to verify the positive and negative HER2 results.
Results.—A total of 135 cases with paired IHC and FISHresults were evaluated. The majority of samples (84%)were biopsies. HER2 amplification was detected in 20tumors (15%). Using the American Society of Clinical
Oncology/College of American Pathologists scoring sys-tem, IHC-FISH concordance was 97% for IHC 0, 93% forIHC 1+, and 100% for IHC 3+. Human epidermal growthfactor receptor 2 positivity was strongly associated withtumor grade (moderately differentiated . poorly differen-tiated, P , .001) and histologic subtype (intestinal .diffuse, P = .007). Array comparative genomic hybridiza-tion analysis was successful in 31 tumors (14 FISH+ and 17FISH2). Fluorescence in situ hybridization and arraycomparative genomic hybridization results were highlyconcordant in both HER2-positive and HER2-negativegroups (93% and 100% concordance, respectively).
Conclusions.—Human epidermal growth factor receptor2 testing in gastroesophageal cancer can be performedusing standard breast cancer procedures and the AmericanSociety of Clinical Oncology/College of American Pathol-ogists scoring criteria. Although IHC 0 and IHC 3+ provideclear stratification, reliable separation of IHC 1+ and IHC2+ may be difficult, especially in biopsy samples. The latter2 groups are best referred to FISH for definitive classifi-cation.
(Arch Pathol Lab Med. 2011;135:1460–1465; doi:10.5858/arpa.2010-0541-OA)
Gastroesophageal cancer is a global health problemwith approximately 800 000 deaths reported annu-
ally.1 Because the tumor produces no specific symptoms inits early stages, patients commonly present with advanced
or metastatic disease where current therapies can offeronly marginal benefit.2 It is hoped that optimization ofchemotherapy regimens and the addition of targetedagents directed at specific molecular pathways will resultin better patient outcomes.
Human epidermal growth factor receptor 2 (HER2)represents a promising therapeutic target. The HER2 geneis a proto-oncogene located on chromosome 17q11–12. Itencodes a transmembrane receptor tyrosine kinase, amember of the epidermal growth factor receptor familyknown to play an important role in cell proliferation andsurvival. Oncogenic activation of HER2 commonly occursthrough gene amplification, which results in proteinoverexpression on the cell membrane, leading to abnormalcell signaling and cell growth. The importance of HER2 iswell established in breast cancer, where HER2 testing hasbecome a standard approach to select appropriate systemictherapy and identify patients who may benefit from theHER2-targeted agents, such as trastuzumab and lapatinib.
Accepted for publication January 31, 2011.From the Departments of Pathology (Drs Tafe, Hedvat, Hameed,
Tang, and Barbashina and Mr Zaidinski) and Medicine (Drs Janjigianand Shah), Memorial Sloan-Kettering Cancer Center, New York, NewYork; and Cancer Genetics, Cold Spring Harbor Laboratory, ColdSpring Harbor, New York (Dr Hicks). Dr Tafe is currently affiliated withthe Department of Pathology, Dartmouth-Hitchcock Medical Center,Lebanon, New Hampshire. Dr Barbashina is currently affiliated with theBreakthrough Breast Cancer Research Centre, Institute of CancerResearch, London, United Kingdom.
The authors have no relevant financial interest in the products orcompanies described in this article.
Presented in part at the annual meeting of the United States andCanadian Academy of Pathology, Washington, DC, March 22, 2010.
Reprints: Violetta Barbashina, MD, The Breakthrough Breast CancerResearch Centre, Institute of Cancer Research, 237 Fulham Rd, LondonSW3 6JB, United Kingdom (e-mail: [email protected]).
Original Articles
1460 Arch Pathol Lab Med—Vol 135, November 2011 HER2 Testing in Gastroesophageal Cancer—Tafe et al

HER2 positivity (defined as 3+ protein overexpressionor gene amplification) characterizes approximately 15% to20% of gastroesophageal tumors with adenocarcinomamorphology, which is similar to rates seen in breastcancer.3–6 Tumor heterogeneity can be observed in somecases, but its frequency and clinical significance are notwell documented. Most tumors, however, demonstrateconsistent HER2 patterns. Marx et al7 examined 62different tumor blocks from 8 HER2-amplified gastriccancers and found that HER2 amplification by fluores-cence in situ hybridization (FISH) was highly homoge-neous within the tumor and between primary tumor andlymph node metastases. These findings are corroboratedby the results of 2 additional studies on 248 and 168samples, which found relatively low rates of tumorheterogeneity by FISH (4.4%–4.8%).4,8
Recently published data6,9 from the randomized, pro-spective phase III clinical trial ToGA provided firstdocumentation of the clinical benefit of trastuzumabwhen used in combination with chemotherapy in thesetting of advanced gastric and gastroesophageal junction(GEJ) cancer. As a result of the survival benefit,laboratories are facing increasing demand for HER2 teststo determine patient eligibility for targeted therapy. Butbefore routine testing can be implemented, several pointsmust be clarified. The HER2 positivity rate needs to beconfirmed across different populations, including theUnited States patients who were not part of the ToGAstudy. The optimal testing strategy is not yet defined, andthe concordance between protein expression and geneamplification has been controversial. Another majorhindrance is the lack of formal guidelines or agreementon which HER2 scoring system should be applied togastric samples. Prior studies have used the HercepTestcriteria (Dako, Glostrup, Denmark) and different modifi-cations thereof, which accounts for some variability ininterpretation.4,6–8,10–14
Standardization of HER2 testing procedures and inter-pretations will be an essential step to ensure accurate andreproducible results. The aims of our study were (1) todetermine the concordance between immunohistochem-istry (IHC) and FISH in routinely processed gastroesoph-ageal samples and (2) to evaluate if the Food and DrugAdministration–approved breast cancer methods and theAmerican Society of Clinical Oncology/College of Amer-ican Pathologists (ASCO/CAP) scoring criteria can pro-vide accurate determination of HER2 status in gastriccancer.
MATERIALS AND METHODS
This study was approved by the institutional review commit-tee of Memorial Sloan-Kettering Cancer Center (New York, NewYork). Testing was performed on archival tissue from patientswith advanced stage gastroesophageal cancer who were consid-ered potential candidates for trastuzumab-based therapy. For-malin-fixed, paraffin-embedded tumor samples from 146 pa-tients were evaluated for HER2 protein expression and geneamplification using IHC and FISH. For each case, a correspond-ing H&E section was reviewed to assess the sample adequacy.All poorly and moderately to poorly differentiated tumors werereexamined by the gastrointestinal pathologist (L.H.T.) toconfirm the grade and histologic subtype (diffuse versusintestinal versus mixed).
Immunohistochemistry was performed with the VentanaPATHWAY rabbit monoclonal antibody (clone 4B5; prediluted)on a BenchMark series automated stainer (Ventana, Tucson,
Arizona), following the manufacturer’s protocol. The 4B5antibody is Food and Drug Administration approved for clinicalHER2 testing in breast cancer. Antigen retrieval was performedusing Cell Conditioning 1 citrate buffer (pH 6.0; Ventana) for30 minutes. The IHC results were interpreted using the 2007ASCO/CAP scoring method recommended for breast cancer(www.cap.org; accessed June 20, 2010), as follows: score 0(negative) 5 no membrane staining is observed; score 1+(negative) 5 weak, incomplete membrane staining in anyproportion of invasive tumor cells, or weak complete membranestaining in less than 10% of cells; score 2+ (equivocal) 5 completemembrane staining that is nonuniform or weak but with obviouscircumferential distribution in more than 10% of invasive tumorcells, or strong complete membrane staining in no more than 30%of cells; score 3+ (positive) 5 complete and uniform strongmembrane staining in more than 30% of invasive tumor cells.
Fluorescence in situ hybridization was carried out with thePathVysion HER2 DNA probe kit and procedure (Vysis/Abbott,Abbott Park, Illinois). The kit contains 2 fluorescently labeledDNA probes, HER2 (labeled with SpectrumOrange) and CEP17(chromosome 17 enumeration probe labeled with Spectrum-Green). The total numbers of HER2 and CEP17 signals werecounted in at least 20 tumor cell nuclei in 2 different areas. TheHER2/CEP17 ratios were interpreted in accordance with the 2007ASCO/CAP scoring criteria used in breast cancer: less than 1.8,HER2 gene not amplified; more than 2.2, HER2 gene amplified;1.8 to 2.2, equivocal.15 Before an equivocal result was recorded,the sample was subjected to additional counting (at least 20additional cells) or repeated as deemed necessary.
In all cases, FISH was performed first to exclude possibleinterpretation bias, followed by IHC. Immunohistochemistry wasindependently interpreted by 2 study pathologists (L.J.T., V.B.)who were blinded to FISH results. The concordance between the 2tests was then evaluated. Tumors showing 3+ protein expressionor gene amplification were considered HER2 positive.
A subset of 31 cases that had sufficient material for additionaltesting was subjected to array comparative genomic hybridiza-tion (aCGH; 244K platform, Agilent Technologies, Santa Clara,California) to verify the positive and negative HER2 results.
Fisher exact tests were performed using GraphPad software(http://www.graphpad.com/quickcalcs/; accessed June 10,2010). Statistical significance was defined as a P value less than.05.
RESULTS
Of the 146 patients, 11 had insufficient tumor tissue tocomplete IHC and FISH analyses, and therefore a total of135 cases with paired IHC and FISH results wereevaluated. Patient characteristics are listed in Table 1.There were 32 women and 103 men, with an age range
Table 1. Patient Characteristicsa
HER2Positive
(n = 21)b
HER2Equivocal(n = 5)
HER2Negative
(n = 107)c
Age at diagnosis, y
Median 60 56 59Range 22–88 50–78 31–90
Sex, No. (%)
F 4 (19) 1 (20) 26 (24)M 17 (81) 4 (80) 81 (76)
Abbreviations: FISH, fluorescence in situ hybridization; HER2, humanepidermal growth factor receptor 2; IHC, immunohistochemistry.a The 2 heterogeneous cases are not included (1 male and 1 female
patient, age 44 and 67, respectively).b IHC 3+/FISH failure included.c IHC 0–1+/FISH failure included.
Arch Pathol Lab Med—Vol 135, November 2011 HER2 Testing in Gastroesophageal Cancer—Tafe et al 1461

from 22 to 90 years. The median age for HER2-positiveand HER2-negative patients was equivalent (60 and59 years, respectively). The majority of patients hadmetastatic disease at the time of diagnosis. The tumorsample characteristics of the 135 cases are shown inTable 2. The majority of samples (84%) were biopsies and78% represented primary tumors. Approximately two-thirds of tumors were intestinal-type adenocarcinomas(65%) and one-third were diffuse type (27%). Poorlydifferentiated tumors comprised 55%, moderately differ-entiated 34%, and moderately to poorly differentiated11%. In terms of tumor location, there was approximatelyequal distribution between the stomach and GEJ/distalesophagus (46% versus 41%, respectively).
The IHC and FISH results for 133 tumors are shown inTable 3. Two cases, which demonstrated distinct patternsof HER2 heterogeneity by IHC and FISH, are not includedin the table and will be discussed separately. Humanepidermal growth factor receptor 2 amplification wasdetected in 20 tumors (15%) with HER2 to CEP17 ratiosfrom 2.6 to 12.1 (median 4.6). The majority of the FISH-positive cases (16 of 20; 80%) were also IHC 3+, with a100% concordance between IHC 3+ and FISH. None of the
IHC 0 tumors demonstrated FISH amplification above theASCO/CAP ratio criteria of 2.2, and only 1 tumor in theIHC 1+ group (1 of 44; 2%) was found to be FISH positive,with a ratio of 2.9. Using the 2007 ASCO/CAP scoringsystem, the IHC-FISH concordance rate was 97% for IHC0, 93% for IHC 1+, and 100% for IHC 3+. Equivocal HER2results, that is, IHC 2+ or FISH 1.8 to 2.2, were relativelyuncommon (6% by IHC and 4% by FISH). The 5 FISHequivocal cases were distributed in all IHC categoriesexcept for 3+.
Five cases failed FISH analysis. The failures were due topoor fluorescence signal (despite repeated attempts) in 4cases (4 of 135; 3%), and an inappropriate samplepreparation in 1 case (outside material received onnoncoated slides).
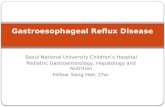
The majority of the HER2-positive tumors (19 of 20;95%) were Lauren intestinal type, comprising 22% of allintestinal-type cases. One tumor (1 of 20; 5%) was Laurendiffuse type, representing 3% of all diffuse-type tumors.Most HER2-positive tumors (85%) were moderatelydifferentiated. By location, 70% of the HER2-positivetumors originated in the proximal region encompassingthe gastric cardia/GEJ/distal esophagus (21% of alltumors at this location), and 25% in the gastric body andantrum (10% of tumors at this location; Figure 1). Amongstomach cancers, there was a slight trend for higherpositivity rate in the antral tumors, but the number ofcases was very small. Overall, HER2 positivity wasstrongly associated with tumor grade (moderately differ-entiated . poorly differentiated; P , .001) and histologicsubtype (intestinal . diffuse; P 5 .007), whereas theassociation with the anatomic location was not statisticallysignificant (P 5 .32).
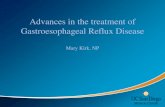
The 2 heterogeneous cases were biopsy specimens, andin both cases HER2 positivity was detected in a minorproportion of tumor cells. By IHC, one showed strongimmunoreactivity in approximately 15% to 20% ofinvasive tumor cells, and the other in 25% to 30% of cells.The first tumor was negative by FISH, but because theIHC-positive region was quite small it is likely that it wasnot represented in the tissue section evaluated by FISH. Inthe second case, FISH confirmed tumor heterogeneitywith distinct subpopulations of HER2-amplified andnonamplified cells. The amplified region comprisedapproximately 25% to 30% of the tumor and correspondedto the area of strong immunoreactivity (Figure 2, Athrough C). Overall, the rate of heterogeneity in this studywas 1.5%.
Array comparative genomic hybridization analysis wassuccessful in 31 tumors (14 FISH+ and 17 FISH2).Fluorescence in situ hybridization and aCGH results werehighly concordant in both HER-positive and HER2-
Table 2. Tumor Sample Characteristics (N = 135)
Samples, No. (%)
Sample type
Biopsy 114 (84)Resection 21 (16)
Specimen type
Primary tumor 106 (78)Recurrent tumor 5 (4)Metastasis 24 (18)
Tumor (adenocarcinoma) subtype(Lauren classification)
Intestinal 88 (65)Diffuse 36 (27)Mixed 9 (7)Undetermined 2 (1)
Tumor differentiation:
Moderate 46 (34)Moderate to poor 15 (11)Poor 74 (55)
Primary tumor location:
Stomach 62 (46)
Antrum 22 (36)Body 28 (45)Cardia 12 (19)
GEJ 33 (25)Distal esophagus 22 (16)Unknown 18 (13)
Abbreviation: GEJ, gastroesophageal junction.
Table 3. Immunochemistry (IHC)–Fluorescence In Situ Hybridization (FISH) Concordancea
FISH IHC 0 IHC 1+ IHC 2+ IHC 3+ Total, No. (%)
Positive (HER2/CEP17 . 2.2) 0 1 3 16 (100) 20 (15)Negative (HER2/CEP17 , 1.8) 60 (97) 39 (93) 4 0 103 (77)Equivocal (HER2/CEP17 1.8–2.2) 2 (1.9; 2.0)b 2 (2.1; 1.8)b 1 (2.1)b 0 5 (4)Failure 2 2 0 1 5 (4)
Total, No. (%) 64 (48) 44 (33) 8 (6) 17 (13) 133
Abbreviations: CEP17, chromosome 17 centromeric probe; HER2, human epidermal growth factor receptor 2.a The 2 IHC heterogeneous cases are not included.b Data in parentheses represent individual values rather than percentages.
1462 Arch Pathol Lab Med—Vol 135, November 2011 HER2 Testing in Gastroesophageal Cancer—Tafe et al

negative groups (93% and 100% concordance, respec-tively). We identified a single discrepant case (FISH+/aCGH2), where aCGH demonstrated the region ofgenomic gain immediately adjacent to the HER2 genebut not involving HER2.
COMMENT
Most of our knowledge about HER2 is derived from thestudies on breast cancer. Clinical HER2 testing of breastcarcinomas is carried out with IHC and in situ hybridiza-tion that are considered complementary techniques.Positive and negative results are expected to be 95%concordant by these methods, and it is recommended thatsuch concordance rates be periodically monitored.15
Correlation of IHC and FISH tends to be the best in theIHC 0 (no staining) and IHC 3+ groups. Any IHC categoryfailing the 95% mark should be considered potentiallyequivocal and undergo confirmatory FISH testing fordefinitive classification.16 Prior to 2007, as many as 20% ofbreast cancer HER2 results might have been inaccurate.15
Possible causes of variability included nonuniform tissuefixation, different sensitivity and specificity of the anti-bodies, and poor scoring reproducibility, attributed inpart to the specifics of the HercepTest interpretationmethod (Dako). The 2007 ASCO/CAP guidelines made asignificant contribution to standardization of the protocolsand introduced a revised scoring system aimed toimprove test specificity and IHC-FISH concordance.15 Arecent survey of 757 US laboratories conducted by theCollege of American Pathologists revealed that 84% of theresponders use the ASCO/CAP scoring method whereasonly 13% follow the interpretation guidelines included inthe test kit.17 We felt that having a simple and uniformscoring system would help to reduce testing variation, andwere interested to see if the ASCO/CAP method would beapplicable to gastroesophageal samples.
Prior retrospective studies on gastric cancer were donemainly on surgical resection specimens.4,7,8,10,12,14 Weexpect, however, that clinical testing will make extensiveuse of biopsy material, because many patients will not be
surgical candidates. Here we report on the HER2 IHC andFISH concordance in a large number of biopsies (84% of allsamples in this cohort). We found that in an unselectedpopulation the rate of FISH positivity is 15%, which issimilar to the 19% mean rate reported in the literature.3,4
We were able to classify most cases as either positive ornegative, whereas equivocal results were relativelyuncommon (6% by IHC and 4% by FISH). Using theASCO/CAP scoring criteria, we found excellent IHC-FISH concordance (.95%) in IHC 0 and IHC 3+ groups,suggesting that these IHC scores may not require routineFISH confirmation.
We noted a couple of possible IHC pitfalls whenevaluating these samples. In some cases, the normalgastric foveolar epithelium showed nonspecific cytoplas-mic staining, thought to be due to high mucin content ofthese cells. However, there was a clear distinction betweenthe normal epithelium and the tumor cells, so this stainingpattern did not interfere with interpretation. In addition,we observed that a minority of cases (6%) had intensecytoplasmic positivity in the tumor cells, considerednonspecific and probably related to cytoplasmic mucin.None of these cases were found to be positive by FISH.However, FISH confirmation may be appropriate in suchcases because strong cytoplasmic staining can mask themembranous positivity and cause difficulty in interpreta-tion of the IHC results.
Array comparative genomic hybridization and FISHresults were highly concordant in both HER2-positive andHER2-negative groups, but our single discrepant case(FISH+/aCGH2) highlighted possible limitations of theHER2 testing methods. As the HER2 FISH probes arelarger than the gene, they may on rare occasion producefalse positive results by detecting amplification of anearby region that does not involve the HER2 locus.
Gastroesophageal cancer is a heterogeneous group oftumors with differences in pathogenesis, epidemiology,and distribution. The predominant histologic subtype isadenocarcinoma, subdivided by the Lauren classificationinto intestinal, diffuse, and mixed subtypes. Epidemiologic
Figure 1. The association between humanepidermal growth factor receptor 2 (HER2)positivity and anatomic location was notstatistically significant ( P 5 .32). Positivityfor HER2 was strongly associated with tumorgrade (moderately differentiated . poorlydifferentiated; P , .001) and histologicsubtype (intestinal . diffuse; P 5 .007). Asingle HER2 amplified tumor with diffuse-type histology was located in the gastricbody. FISH indicates fluorescence in situhybridization; GEJ, gastroesophageal junction.
Arch Pathol Lab Med—Vol 135, November 2011 HER2 Testing in Gastroesophageal Cancer—Tafe et al 1463

studies have identified an additional distinct biologicgroup, so-called proximal gastric cancer, which combinestumors of gastric cardia, GEJ, and distal esophagusbased on their biologic similarities.18 Prior studies have
discovered more frequent HER2 positivity in intestinal-type carcinomas and GEJ location, compared to diffuse-type cancers and gastric origin. Our results confirm theseobservations and show strong association between HER2positivity, Lauren intestinal subtype, and moderate tumordifferentiation. Although we did notice a trend forincreased HER2 positivity in tumors originating in theproximal region (cardia/GEJ/distal esophagus), this didnot reach statistical significance in our study.
In 2008, Hofmann et al4 published results of a validationstudy of HER2 scoring in 168 gastric cancer resectionspecimens. The authors used the HercepTest (Dako) withmanufacturer-recommended interpretation method andfound an IHC-FISH discrepancy in 11 cases (7%). Therewere 2 major causes for this discrepancy, the first of whichwas tumor heterogeneity. In 3 cases, the tumors showedsmall foci of intense immunoreactivity (‘‘small, cohesiveIHC 3+ clones’’) comprising less than 10% of the totaltumor area, whereas the remaining cells were completelynegative, so these cases were initially scored as IHC 0according to the HercepTest scoring criteria. However,these same areas were found to be FISH amplified. Thesecond reason for the discrepancy was the observation ofincomplete membranous (basolateral only) immunoreac-tivity in gastric cancer cells. The authors believe that thispattern may be unique to gastric epithelium because of itssecretory nature, and may indicate how these tumors canbe underscored with the HercepTest method when in factthey may be FISH+, as was true in 2 of 7 of their cases.Based on these findings, Hofmann et al4 proposed amodified HER2 scoring system, which was later used inthe ToGA trial.
Some of the concerns raised by Hofmann et al4 areaddressed by the ASCO/CAP scoring system. The ASCO/CAP guidelines specify that IHC score 0 should bereserved for tumors with no staining at all (www.cap.org, accessed June 20, 2010), which would avoid some ofthe problems described above. In addition, a recentpublication by the CAP panel has provided guidelineson reporting genetic HER2 heterogeneity in breast cancersamples.19 Heterogeneity is detected when the tumorcontains 2 distinct subpopulations of HER2 amplified andnonamplified cells identified by FISH, and the amplifiedclone is minor (,50% of the tumor). Because the biologicsignificance of this rare phenomenon and its clinicalrelevance in terms of response to trastuzumab is currentlyunknown, it is recommended that heterogeneity bespecifically described in the report and the percentagesof the amplified and nonamplified cells indicated.19 Forstandardization purposes, it may be reasonable to applythe same definitions and reporting format to gastroesoph-ageal cancer until more data become available. For anyheterogeneous case, retesting of additional tissue blocks ormetastatic sites may help to better estimate the proportionof amplified cells and, thus, assist in selection ofappropriate therapy.
We recognize that the basolateral pattern of immuno-reactivity in some gastroesophageal cancers can result indifficulty assigning a definitive IHC score. Reliableseparation of IHC 1+ and IHC 2+ patterns can beparticularly challenging in small biopsy specimens, whichfrequently show crush and edge artifacts. Although IHC 0(no staining) and IHC 3+ (strong staining in more than30% of cells) provide clear stratification, we feel that IHC
Figure 2. Tumor heterogeneity. A, Immunohistochemical staining(IHC) for human epidermal growth factor receptor 2 (HER2) in the firstcase showing strong immunoreactivity in 15% to 20% of invasivetumor cells. B, HER2 IHC in the second case showing strongimmunoreactivity in 25% to 30% of invasive tumor cells. C, HER2heterogeneity in the second case confirmed by fluorescence in situhybridization (original magnifications 310 [A and B] and 3100 [C]).
1464 Arch Pathol Lab Med—Vol 135, November 2011 HER2 Testing in Gastroesophageal Cancer—Tafe et al

1+ and IHC 2+ scores should be referred to FISH fordefinitive classification.
To compare the ASCO/CAP and ToGA scoringmethods, we reexamined our data using the modifiedcriteria proposed by Hofmann et al4 (Table 4). Thisincluded separating the FISH results into positive andnegative categories using a HER2 to CEP17 ratio of 2.0 asthe cutoff point, and eliminating the equivocal category. Inorder to achieve this, our 5 FISH-equivocal cases werereclassified as positive in 3 instances (including 1 IHC 0case), and negative in 2. We also reevaluated all of our IHC1+ and 2+ cases and reclassified 3; all 3 were downgradedfrom 1+ to 0 based on the system proposed by Hofmann etal.4 With the Hofmann et al4/ToGA method, our positiverate has increased from 15% to 17% because of theinclusion of the 3 equivocal cases, but otherwise, theresults were not significantly different. In particular, evenwhen using the Hofmann et al4/ToGA criteria, FISHwould be recommended for IHC 1+ and 2+ cases with asimilar likelihood of identification of FISH amplification.This suggests that the intended advantage of the Hofmannet al4/ToGA scoring method is maintained by the ASCO/CAP guidelines for HER2 IHC.
In conclusion, we found that HER2 testing in gastro-esophageal cancer can be performed using standardtechnical procedures without protocol modification, andthat the HER2 status of gastroesophageal carcinomas canbe accurately determined with the ASCO/CAP scoringcriteria. Having a simple and straightforward interpreta-tion method can significantly reduce testing variation.
The search for targeted therapies is likely to continue.The international phase III EXPAND trial for epidermalgrowth factor receptor inhibitors in gastric cancer mayprovide insight into additional treatment options. As thenumber of tests is likely to grow, standardization of allsteps of the testing process from tissue fixation to finalinterpretation would help to ensure accurate identificationof patients who may benefit from specific therapies.
References
1. World Health Organization. Cancer: fact sheet 297. Published 2009. http://www.who.int/mediacenter/factsheets/fs297. Accessed June 20, 2010.
2. Power DG, Kelsen DP, Shah MA. Advanced gastric cancer—slow butsteady progress. Cancer Treat Rev. 2010;36(5):384–392.
3. Jorgensen JT. Targeted HER2 treatment in advanced gastric cancer.Oncology. 2010;78(1):26–33.
4. Hofmann M, Stoss O, Shi D, et al. Assessment of a HER2 scoring system forgastric cancer: results from a validation study. Histopathology. 2008;52(7):797–805.
5. Gravalos C, Jimeno A. HER2 in gastric cancer: a new prognostic factor anda novel therapeutic target. Ann Oncol. 2008;19(9):1523–1529.
6. Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combinationwith chemotherapy versus chemotherapy alone for treatment of HER2-positiveadvanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687–697.
7. Marx AH, Tharun L, Muth J, et al. HER-2 amplification is highlyhomogenous in gastric cancer. Hum Pathol. 2009;40(6):769–777.
8. Kim MA, Jung EJ, Lee HS, et al. Evaluation of HER-2 gene status in gastriccarcinoma using immunohistochemistry, fluorescence in situ hybridization, andreal-time quantitative polymerase chain reaction. Hum Pathol. 2007;38(9):1386–1393.
9. Van Cutsem E, Kang Y, Chung H, et al. Efficacy results from the ToGA trial:a phase III study of trastuzumab added to standard chemotherapy in first-lineHER2-positive advanced gastric cancer [abstract]. J Clin Oncol. 2009;27(18)(suppl):LBA4509.
10. Zhang XL, Yang YS, Xu DP, et al. Comparative study on overexpression ofHER2/neu and HER3 in gastric cancer. World J Surg. 2009;33(10):2112–2118.
11. Yano T, Doi T, Ohtsu A, et al. Comparison of HER2 gene amplificationassessed by fluorescence in situ hybridization and HER2 protein expressionassessed by immunohistochemistry in gastric cancer. Oncol Rep. 2006;15(1):65–71.
12. Takehana T, Kunitomo K, Kono K, et al. Status of c-erbB-2 in gastricadenocarcinoma: a comparative study of immunohistochemistry, fluorescence insitu hybridization and enzyme-linked immuno-sorbent assay. Int J Cancer. 2002;98(6):833–837.
13. Ruschoff J, Dietel M, Baretton G, et al. HER2 diagnostics in gastriccancer—guideline validation and development of standardized immunohisto-chemical testing. Virchows Arch. 2010;457(3):299–307.
14. Barros-Silva JD, Leitao D, Afonso L, et al. Association of ERBB2 gene statuswith histopathological parameters and disease-specific survival in gastriccarcinoma patients. Br J Cancer. 2009;100(3):487–493.
15. Wolff AC, Hammond ME, Schwartz JN, et al. American Society of ClinicalOncology/College of American Pathologists guideline recommendations forhuman epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol.2007;25(1):118–145.
16. Hammond EH, Wolff AC, Hayes DF, Schwartz JN. Reply to G. Sauter et al.J Clin Oncol. 2009;27(30):e153–e154; author reply e155–e157.
17. Nakhleh RE, Grimm EE, Idowu MO, Souers RJ, Fitzgibbons PL. Laboratorycompliance with the American Society of Clinical Oncology/College ofAmerican Pathologists guidelines for human epidermal growth factor receptor2 (HER2) testing: a College of American Pathologists survey of 757 laboratories.Arch Pathol Lab Med. 2010;134(5):728–734.
18. Shah MA, Kelsen DP. Gastric cancer: a primer on the epidemiology andbiology of the disease and an overview of the medical management of advanceddisease. J Natl Compr Canc Netw. 2010;8(4):437–447.
19. Vance GH, Barry TS, Bloom KJ, et al. Genetic heterogeneity in HER2testing in breast cancer: panel summary and guidelines. Arch Pathol Lab Med.2009;133(4):611–612.
Table 4. Our Data Reclassified According to the Criteria Used in the ToGA Trial4,6,a
FISH (ToGA) IHC 0 (ToGA) IHC 1+ (ToGA) IHC 2+ (ToGA) IHC 3+ (ToGA) Total, No. (%)
Positive (HER2/CEP17 . 2) 1 2 4 16 23 (17.2)Negative (HER2/CEP17 , 2) 64 37 4 0 105
Abbreviations: CEP17, chromosome 17 centromeric probe; FISH, fluorescence in situ hybridization; HER2, human epidermal growth factor receptor2; IHC, immunohistochemistry; ToGA, prospective, randomized, phase III multicenter study evaluating the efficacy of trastuzumab in combinationwith chemotherapy versus chemotherapy alone in patients with HER2-positive advanced gastric cancer (IHC and FISH scoring criteria used in theToGA trial are described by Hofmann et al4).a The 2 heterogeneous cases are not included. Five FISH-equivocal cases were reclassified as positive (3) or negative (2). Three IHC cases were
reclassified (all 3 downgraded from 1+ to 0).
Arch Pathol Lab Med—Vol 135, November 2011 HER2 Testing in Gastroesophageal Cancer—Tafe et al 1465