Huang 2014
42
Accepted Manuscript A systematic review and meta-analysis of psychotherapy for late-life depression Alice X. Huang, MD, MS Kevin Delucchi, PhD Laura B. Dunn, MD J. Craig Nelson, MD PII: S1064-7481(14)00121-3 DOI: 10.1016/j.jagp.2014.04.003 Reference: AMGP 367 To appear in: The American Journal of Geriatric Psychiatry Received Date: 10 January 2014 Revised Date: 27 March 2014 Accepted Date: 14 April 2014 Please cite this article as: A.X. Huang, K. Delucchi, L.B. Dunn, J.C. Nelson, A systematic review and meta-analysis of psychotherapy for late-life depression, The American Journal of Geriatric Psychiatry (2014), doi: 10.1016/j.jagp.2014.04.003. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
-
Upload
edhobiondi -
Category
Documents
-
view
220 -
download
0
description
somatoform
Transcript of Huang 2014

Accepted Manuscript
A systematic review and meta-analysis of psychotherapy for late-life depression
Alice X. Huang, MD, MS Kevin Delucchi, PhD Laura B. Dunn, MD J. Craig Nelson,MD
PII: S1064-7481(14)00121-3
DOI: 10.1016/j.jagp.2014.04.003
Reference: AMGP 367
To appear in: The American Journal of Geriatric Psychiatry
Received Date: 10 January 2014
Revised Date: 27 March 2014
Accepted Date: 14 April 2014
Please cite this article as: A.X. Huang, K. Delucchi, L.B. Dunn, J.C. Nelson, A systematic review andmeta-analysis of psychotherapy for late-life depression, The American Journal of Geriatric Psychiatry(2014), doi: 10.1016/j.jagp.2014.04.003.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT1
Manuscript 4210 words Title: A systematic review and meta-analysis of psychotherapy for late-life depression Byline: Alice X. Huang, MD, MS; Kevin Delucchi, PhD; Laura B. Dunn, MD; J. Craig Nelson, MD Authors: Alice X. Huang, MD, UCSF Department of Psychiatry and Langley Porter Psychiatric Institute; Kevin Delucchi, PhD, UCSF Department of Psychiatry and Langley Porter Psychiatric Institute; Laura B. Dunn, MD, UCSF Department of Psychiatry, Langley Porter Psychiatric Institute, and UCSF Helen Diller Family Comprehensive Cancer Center; J. Craig Nelson, MD, UCSF Department of Psychiatry and Langley Porter Psychiatric Institute Correspondence: J. Craig Nelson, MD 401 Parnassus Avenue, Box 0984 San Francisco CA 94143-0984 Phone: (415)-476-7405 Fax: Email: [email protected]
Previous Presentations: 1. American Psychiatric Association Annual Meeting 2013, San Francisco. May 20, 2013 2. American Association for Geriatric Psychiatry Annual Meeting 2013, Los Angeles. March
14, 2013
Disclosures and Acknowledgements: Alice X. Huang reports no competing interests. Kevin Delucchi reports no competing interests. Laura B. Dunn reports no competing interests. During the past 12 months J. Craig Nelson, M.D. has served as a consultant, adviser, or speaker for, received research support or travel support from, or participated in CME for Bristol-Myers Squibb, Cenestra Health, Corcept, Eli Lilly, Eli Lilly Global, Forest, Health Resources and Services Administration, , Lundbeck, Mylan/Dey Pharma, NIMH, Otsuka USA, Otsuka Asia, Pfizer, Shire, and Sunovion;, and he owns stock in Atossa. Grant Support: for this study was provided by the UCSF Epstein Endowment.
Keywords: geriatric, psychotherapy, late-life depression, meta-analysis

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT2
FINAL MANUSCRIPT WITH TRACKED CHANGES
Abstract
Objectives: To determine the efficacy of psychotherapy in late-life depression and to determine
the effect of the type of control group on the magnitude of psychotherapy effects
Design: A systematic review and meta-analysis of randomized controlled psychotherapy trials
for late-life depression
Setting: Outpatient clinics or in subjects’ home
Participants: Subjects ≥ 55 years of age with acute-phase depressive disorder
Measurements: Change in depressive symptoms was measured with validated scales.
Standardized mean differences (SMD) were calculated for each therapy-control contrast, as
meta-analytic summaries for contrasts using a similar control, and for all contrasts combined.
Results: The search identified 27 trials with 37 therapy-control contrasts and 2,245 subjects.
Trials utilized 5 types of control groups (waitlist, treatment-as-usual, attention, supportive
therapy, placebo). In the combined contrasts, psychotherapy was effective (SMD=0.73; 95% CI
0.51, 0.95; z=6.42, p<.00001). The SMD varied widely (from 0.05 to 1.36) and significantly
(χ2=35.67, df=4, p<.00001) between subgroups by type of control. In 5 trials that compared
psychotherapy with supportive therapy, the SMD was 0.39 (95% CI 0.16, 0.61; z=3.37,

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT3
p<0.0007; I2=0%). The SMD was 0.11 within the waitlist controls and 1.10 within the supportive
therapy subgroup.
Conclusions: Psychotherapy is effective for late-life depression, but the magnitude of the effect
varies widely with the type of control group. Supportive therapy appears to best control for the
non-specific elements of psychotherapy and is associated with considerable change itself, but
few trials have employed it as a control.
Keywords: geriatric, late-life depression, psychotherapy, meta-analysis

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT4
Objective
Depression is a common disorder in older adults that reduces quality of life and increases
disability, risk of suicide, morbidity, and mortality (1). Usual treatments include antidepressants,
psychotherapy, or a combination. Antidepressants are effective, but effects are modest (2) and
their use may be complicated by medical comorbidities, drug-drug interactions, and increased
vulnerability of elders to side effects. Finally, some patients prefer psychotherapy.
In the past decade, several reviews have examined the evidence for psychotherapies
targeting late-life depression (3-7) and have concluded that psychotherapy is effective (3-6) and
that it has “moderate to large effects” (3,5,6). Conclusions about the effectiveness of
psychotherapy may be premature, however, without adequate consideration of the type of
controls employed.
Unlike antidepressant trials, in which a placebo control remains the gold standard, types
of control groups utilized in psychotherapy trials vary widely. In psychotherapy trials for late-life
depression, examination of the effects of these controls on outcomes has been limited. Cuijpers
et al. (5) found no effect of the type of control condition on the magnitude of the treatment-
control difference; however, in that study, 11 of the 18 trials utilized a waitlist control, and the
study did not explicitly examine supportive therapy, attention, and placebo controls.
The effects of different types of control groups have been examined in mixed-age
samples (8,9). For example, Baskin et al. (8) demonstrated that smaller effect sizes result when
psychotherapy is compared to structurally equivalent controls (e.g. in number and duration of
sessions, format of therapeutic interaction) than when compared to structurally dissimilar
controls. Supportive therapy may best control for the non-specific factors common to all
psychotherapies (attention, education, reassurance, monitoring symptoms) (10). These factors

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT5
must be accounted for if trials are to provide strong evidence for the specific elements of
psychotherapies.
We performed a systematic search of randomized controlled trials (RCTs) of
psychotherapy in late life depression with the following goals: 1) to examine the effects of all
types of control groups employed in late-life depression trials on the magnitude of the therapy-
control differences; 2) to specifically determine the magnitude of treatment-control differences
when supportive therapy is the control and determine which psychotherapies have been
compared with supportive therapy; and 3) to systematically review all appropriate trials
published, including those published since the last review. We hypothesized that psychotherapy
would yield large effects when compared to waitlist, attention, or treatment-as-usual (TAU)
controls, but that the effects would be smaller when compared with supportive therapy. We
intentionally began our review with an inclusive approach and performed sensitivity analyses to
determine the effects of restrictive criteria. Finally, we were interested in the magnitude of
change that occurs within different controls, particularly waitlist controls and supportive
psychotherapy. As an exploratory analysis, we examined the effect size of change that occurred
within the different control groups.
Method
Search Strategy
We searched electronic databases PubMed (MESH and text), PsycInfo (title, keywords
and text), and Cochrane Central Register of Controlled Trials (MESH, keywords, title, abstract)
on May 11, 2012. We used terms the intervention (“psychotherapy,” “counseling,” “counseling,”

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT6
“therapy”), the older adult population (“aged,” “aging,” “elder,” “elderly,” “geriatric,” “late life,”
“later life,” “old,” “older”), and depression symptomatology (“depressed,” “depression,”
“depressive disorder”). We limited the search to published, English language, and randomized
controlled trials. We also examined recent reviews and a web database of psychotherapy trials
(11). Finally, we cross-referenced the search arms and removed duplicates.
Definition of Psychotherapy and Type of Control
We defined “psychotherapy” using a modification of a definition by Baskin et al (8).
Psychotherapy must have been delivered face-to-face by a trained therapist and the interaction
with the patient was the vehicle through which the therapeutic components were delivered. It
must have included two of the following: (a) treatment based on psychological principles, (b)
treatment offered to the psychological community (e.g. a manual was available), and (c)
treatment with specific components intended to be therapeutic. We excluded interventions
designed as adjuncts to pharmacotherapy or treatments that were not stand-alone treatments.
Because several bibliotherapy trials were performed in late-life depression, we included these
trials even though they were not administered face-to-face. We then performed a sensitivity
analysis to determine the effect of their inclusion.
Control groups described as “waitlist,” “delayed treatment,” or “no treatment” were
categorized as waitlist controls. “Treatment-as-usual” or “care-as-usual” controls were grouped
together. Control groups that controlled for time spent with the therapist while avoiding
therapeutic interventions were categorized as attention controls. Control groups that met
regularly and provided education and support were categorized as supportive therapy. In studies
comparing psychotherapy, antidepressants, and placebo, psychotherapy was contrasted with

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT7
placebo controls. Two authors (AXH, JCN) reached a consensus about the designation of the
control group.
Inclusion/Exclusion Criteria
We included acute-phase randomized controlled trials of psychotherapy published in
peer-reviewed journals from the inception of the PubMed, PsycInfo, and Cochrane Central
Register of Controlled Trials databases and that specified a minimum age of 55 years.
Depression was diagnosed using either DSM III or IV criteria or required a minimum score on a
depression rating scale. Included studies assessed outcomes with a validated symptom scale. We
excluded maintenance and prevention trials, interventions not meeting our psychotherapy
definition, trials with no depression criteria, trials that included patients with dementia, and trials
limited to one medical disease (e.g. Parkinson’s disease, stroke). We excluded trials using the
abstract when possible. When the abstract was insufficient, two authors (AXH, JCN) examined
the full article and reached consensus regarding inclusion.
Data Extraction
Data extracted included minimum and mean age of the subjects, sex, number of subjects
randomized, number of dropouts, number of subjects analyzed, number of treatment arms, type
of treatment and controls, duration of the trial, number of sessions, type of analysis (intention-to-
treat (ITT) versus completer) and whether clinician ratings were blind to treatment assignment. If
duration differed in the control and treatment arms, outcome was compared at the end of the
controlled period. If critical values for the analysis were not reported, we attempted to obtain

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT8
them from the authors. Data were extracted by one of the authors (JCN) and independently
checked by another author (LBD).
Quality Assessment
We used the 25-item psychotherapy quality rating scale (RCT-PQRS) developed by the
American Psychiatric Association’s Committee on Research on Psychiatric Treatments to assess
the quality of the trials (12).
Statistical Analyses
Because all trials reported change on depression scales while a minority reported
response and remission rates, change scores were employed to assess outcome using
standardized mean difference scores (SMDs) as a measure of effect size. The SMD is the
difference between the mean change scores of the treatment and control groups divided by the
standard deviation of the difference. SMDs are weighted by the sample size in the meta-analysis.
If change scores and their standard deviations (SDs) were not reported, we calculated change
scores subtracting the endpoint score from baseline score. We calculated the SD of the change
score using the following formula from the Cochrane Handbook (13) that accounts for the
correlation between baseline and endpoint ratings. We estimated this correlation (r=0.2,
df=4137) using individual patient data (N=4139) from a prior late-life depression study (14).
______________________________________________ SDchange = √ SD2
baseline + SD2endpoint - (2 x corr x SDbaseline x SDendpoint )
If endpoint scores from the last visit were not reported for the ITT sample, we used the observed
final visit score in completers. If SDs of mean values were not reported and could not be

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT9
calculated, we attempted to obtain them from the authors. If we were unable to obtain them, SD
values were imputed (for two contrasts) using other trials with that scale.
Because different rating scales were employed and several trials included more than one
scale, we used a fixed algorithm based on frequency to determine which scale to include
(Hamilton Rating Scale for Depression [HRSD] > Beck Depression Inventory [BDI] > Geriatric
Depression Scale [GDS] > other scale). The use of different scales to assess change was partially
mitigated by the use of standardized scores. A sensitivity analysis also was performed limiting
the trials to those using the HRSD.
Effects were expressed as SMDs with the 95% confidence intervals (CIs), z-score, and p-
values. Effects were calculated for each treatment-control contrast, for the trials grouped by type
of control condition, and as a meta-analytic summary for all treatments combined using a
random effects model. In studies with more than one active or control arm, we entered the full
sample for each treatment and control contrast. Heterogeneity was determined for each subset of
trials grouped by type of control and for the summary meta-analysis and expressed as χ2 and I2-
statistics. Review Manager version 5.25 (The Cochrane Collaboration, Oxford, England) was
used for statistical calculations.
Sensitivity analyses were performed to test if limiting trials to those that used the same
rating scale (the HRSD) differed from results using various scales and to determine if results
differed if we adjusted the size of the treatment or control group for those included in more than
one contrast. Because we used an inclusive approach, we examined if results differed had we
restricted trials to those with a minimum age of 60 years, to only subjects with MDD, to those
that performed only face-to-face psychotherapy or individual therapy. In an exploratory analysis,
we examined the correlations of the SMDs with mean age of the sample, duration of the trial,

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT10
number of sessions, baseline depression severity, sample size, publication year, and study
quality. To estimate severity, scale totals were converted to 17-item HRSD scores (see Text,
Supplement Digital Content 1, which describes the conversion). To assess publication bias, we
created a funnel plot, performed an Egger analysis (15), and determined the association of
sample size with the SMD. To assess recent trends in trial methodology we examined the
association of year of publication with the factors described above.
We examined the standardized mean difference (baseline-endpoint depression
scores/SDchange) within different control subgroups correcting for the association of repeated
measures.
Results
Characteristics of Included Studies
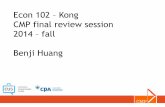
Our search yielded 2706 potential articles (Figure 1). Review of key articles, reviews, and
the online psychotherapy database produced another 64 articles. We excluded 2628 articles
based on abstract, and reviewed the remaining 142 full articles. There were 13 articles cited in
other reviews that were excluded because they did not meet our inclusion criteria (see Text,
Supplemental Digital Content 2, which describes these excluded trials ).
A total of 27 trials conducted between 1981 and 2011 were selected (Table 1) (16-42).
Four trials were included after authors supplied additional data (23,38,41,42). Since the last
meta-analysis of late-life depression (7), 8 trials were published (18,20,27,28,30,36,41,42).
Outcome data were reported for 2,245 subjects. The types of psychotherapy included were:
cognitive behavioral therapy, cognitive therapy, behavioral therapy, problem-solving therapy

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT11
(PST), interpersonal therapy, brief dynamic therapy, bibliotherapy, reminiscence therapy, and a
“Coping with Depression” course (26). Therapies were conducted in individual or group settings.
The types of control groups were: waitlist, TAU, attention, supportive therapy, and
placebo. Trial duration ranged from 4 to 26 weeks (median 7 weeks), with 4 to 12 psychotherapy
sessions (median 8 sessions). Reporting of treatment received in the TAU condition was variable
and ranged from no treatment to protocol-guided pharmacotherapy. Studies with supportive
therapy, attention, and placebo controls matched the number of sessions to the psychotherapy
intervention. Most samples were outpatient, though 4 trials involved home-based interventions
(24,25,27,28). Several trials had multiple treatment or control groups resulting in a total of 37
treatment-control contrasts. Trial characteristics are shown in Table 1.
Quality Assessment
Study quality was variable ranging from “exceptionally good” to “very poor” on the
RCT-PQRS. Numeric total scores ranged from 18 to 43 (mean 27.4; possible range 0-48). Total
quality scores, which were weighted for sample size, were highly correlated with year of
publication (r=0.68, df=25, p<.001). Of the 27 trials, 10 used an intention-to-treat analysis and 7
defined the primary outcome. All trials randomized subjects, but randomization was modified in
some, especially group treatment studies. In 11 trials, raters were blind to treatment assignment.
In 8 trials with clinician ratings, blinding of raters was not reported. In the 8 remaining trials, the
primary scale was a self-report.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT12
Meta-analysis Results
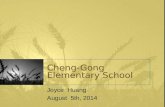
In all contrasts combined, treatment was more effective than control and the standardized
mean difference (SMD) for psychotherapy versus control was 0.73 (95% CI [0.51, 0.95], Z=6.42,
p<.00001) (Figure 2). There was significant heterogeneity for all contrasts combined (χ2=226.54,
df=36, p<.00001, I2=84%).
The test for subgroup differences, grouped by type of control, was significant (χ2=35.67,
df=4, p<.00001). The SMDs for the subgroups ranged from 0.05 to 1.36. Heterogeneity was
substantial in the subgroups using TAU and attention controls, moderate in the waitlist controls,
and not significant for supportive therapy and placebo controlled trials (Table 2).
Sensitivity Analyses
We corrected for duplicate entries by dividing the number of subjects by the number of
entries and found that the overall SMD was similar to the initial meta-analysis (SMD 0.69 vs.
0.73). If we restricted trials to those using the HRSD (20 of 37 contrasts), the overall SMD was
similar to that using other scales (0.72 vs. 0.72 respectively).
We then performed planned sensitivity analyses to assess the effects of more restrictive
trial selection (Table 2). Restricting trials to those with a minimum age of 60 years or to those
with face-to-face psychotherapy had no significant effect on the SMD. Limiting the sample to
trials that only included MDD lowered the SMD from 0.73 to 0.64. The SMD was similar in
face-to-face therapy and bibliotherapy but somewhat larger in trials using group therapy than
those with individual therapy. The magnitude of these differences appeared substantially smaller
than the differences in SMD obtained with different types of control groups. One exception was

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT13
therapy provided in the home, which appeared significantly more effective than therapy
administered in a clinic, although only 4 trials provided home care.
Exploratory analyses revealed that the SMD was modestly associated with trial duration;
strongly associated with study quality, sample size, and year of publication; and not significantly
associated with mean age, depression severity, or number of sessions (Table 2). Because some
factors were interrelated, we estimated and tested a regression model to assess their independent
contribution to the SMD, controlling for type of control group. While the overall model was
significant (p<.003) with R2=.56, no individual factor was significantly associated with the
SMD; however, we note that the power of this analysis to detect differences is limited by the
number of contrasts (N=37) (see Table, Supplemental Content 3, of the regression analysis). To
assess historical trends we examined the association of year of publication with the factors
detailed above weighting by sample size. Recent trials were of higher quality (r=0.68, df= 25;
p<.001), and mean age was greater (r=0.57, df=25; p=.002), but year of publication was not
associated with sample size, trial duration, depression severity, or number of sessions.
Publication bias
A funnel plot of the standard error of the SMD against the SMD indicated an excess of small
studies with large SMDs suggestive of bias (see Figure, Supplemental Digital Content 4, of the
funnel plot). The Egger test was significant (parameter estimate = 2.93, t = 3.77, df=1, p=.0006).
Sample size was inversely associated with the SMD, r = -0.46,, df = 35, p=.005). Exploratory
analysis of change in control groups
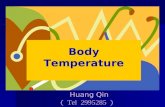
To explore differences in changes occurring within different types of control groups, we
calculated the within group standardized mean difference (SMD) for each of the control

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT14
subgroups (Figure 3). Change in waitlist controls was quite small (SMD=0.11, 95% CI -0.04,
0.27). Change was greatest in the supportive therapy controls (SMD=1.10, 95% CI 0.81, 1.40).
Change in the TAU, attention, and placebo control subgroups was intermediate (SMD ranged
from 0.37 to 0.9)
Conclusions
Our meta-analysis confirmed previous findings that psychotherapy is an effective
treatment for depression in late life (4-7). As hypothesized, the magnitude of the effect varied
significantly by the type of control group. Furthermore, the effect of type of control on the SMD
was relatively large compared to other factors (Table 2). Psychotherapy interventions yielded
large effects when compared to waitlist and attention controls but small to moderate effects when
compared to supportive therapy. Contrary to our hypothesis, the effect size of psychotherapy
versus TAU was small to moderate.
Previous authors have emphasized the importance of controlling for non-specific effects
during treatment such as attention, reassurance, education and monitoring symptoms (8,10).
Supportive therapy best controls for these elements (8,10,18,43) and our findings indicate that
supportive therapy itself is associated with substantial improvement. Although the effect size for
psychotherapy was modest when compared with supportive therapy, the effect size was notable
when compared with the effect size of drug-placebo differences in late-life depression (ES =
0.14) (2). Comparisons with antidepressant trials are complicated by recent findings of negative
expectation effects in placebo-controlled studies (44,45). Specifically, patients receiving
antidepressants in trials with a placebo have significantly lower response rates compared to

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT15
blinded trials without a placebo (52% vs. 65%) (45). Because patients cannot be blinded in
psychotherapy trials, rates of response may be higher than those usually encountered in placebo-
controlled drug trials. It remains unclear how expectation influences response in the control
condition in psychotherapy trials.
Five trials compared psychotherapy with supportive therapy. Four of these trials were
small pilot studies with N ≤ 25 subjects. Three of the five trials employed PST, including the
only large study in this group (N = 221). This was a high quality study (by RCT-PQRS rating)
for which the SMD was 0.33. Problem-solving therapy is the only psychotherapy in older adults
validated against a supportive therapy control (18). This finding underscores the paucity of
adequately powered psychotherapy trials with a supportive therapy control.
One purpose of the control condition is to account for spontaneous remission. Subjects
assigned to waitlist groups showed little change (SMD=0.11) suggesting low spontaneous
remission rates. This effect size is smaller than that reported by Rutherford et al. (46), who found
a within-group effect size of 0.5 for change in waitlist control subjects in 10 mixed-age trials. It
is possible the longer duration of treatment (10 vs. 7 weeks), greater depression severity (mean
HRSD 21 vs. 17), and younger mean age of patients in those trials resulted in greater change in
their waitlist controls than in ours.
Authors of a prior meta-analysis of psychotherapy trials in late-life depression found
significant heterogeneity in the included trials, which limited their conclusions (7). Our meta-
analysis addressed this limitation, in part, by examining treatment-control differences within
different types of control groups. The meta-analytic estimate of heterogeneity was <1% in
supportive therapy or placebo-controlled trials. Heterogeneity was greatest in the trials using

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT16
attention (I2=93%), TAU (I2=71%), and waitlist control trials (I2 = 34%). It seems possible that
the variability of treatments in the TAU controls contributed to heterogeneity.
In addition among the trials with a TAU control, one trial (24) had a much larger SMD
and appeared to be an outlier. If that trial was removed, heterogeneity (I2) in the TAU controlled
trials was reduced from 71% to 0%. The Gellis et al trial (24) provided PST in the home, and it is
possible that home care in home-bound subjects may show greater differences when compared
with usual care. In fact, the SMD in the 4 home care trials was larger than the 26 contrasts in
which therapy was provided in a clinic (SMD 1.20 vs. 0.66).
The nature of the attention controls varied and may have contributed to the heterogeneity
in those trials. It is possible that subjects perceived some attention activities (e.g watching TV or
discussing current events) as less credible therapies. It is unclear what accounted for the
heterogeneity in the waitlist controls, although limiting trials to those with subjects aged ≥60
years reduced heterogeneity. Finally, the presence of heterogeneity does not negate our findings,
but rather suggests that other unidentified factors contributed to differences in efficacy between
therapy and control in the waitlist, TAU, and attention control groups.
The funnel plot and Egger’s test of the combined trials suggested potential bias; however,
the funnel plots differed among the trials with different controls. Trials with supportive therapy
and trials with placebo controls had symmetrical funnel plots each anchored by one large study.
The funnel plot of the trials with TAU controls was asymmetric but asymmetry was reduced with
exclusion of the Gellis trial (24). The funnel plots of the waitlist and attention controlled trials
were relatively uninformative, yet the mean SMDs for these trials were considerably higher than
those of the other control subgroups. Eighteen of the 21 contrasts using waitlist or attention
controls were from small trials (< 30 subjects per arm). When the contrasts using WL or AC

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT17
were added to the combined group, they produced an apparent excess of small trials with large
SMDs. While we would be cautious about drawing conclusions given the small number of trials
in some subgroups, these data suggest the possibility that the asymmetry observed in the funnel
plot of the combined trials was the result of true differences in SMDs among the control
subgroups rather than publication bias.
In our meta-regression analyses, trial quality was inversely related to the SMD. Quality
and methodological rigor appeared to improve in recent studies resulting in more conservative
estimates of effects. Studies that were larger also tended to yield smaller effect sizes. Among
other factors examined, provision of therapy in the home stood out as having a relatively large
effect; however, this finding was based on just 4 trials.
Recent work by Rutherford and colleagues (47) suggests that other factors may influence
response in the control group, specifically in patients receiving placebo and clinical management.
They examined 11 placebo controlled antidepressant trials in older depressed adults. They found
that response rates in the control group increased with number of visits. The data in our
supportive therapy and placebo control samples were too limited to investigate this association.
We found no new comparison trials since Cuijpers’ 2006 review (5). Reminiscence
therapy was less effective than the other intervention in two trials (17,48). Most trials found no
significant difference between the psychotherapies, but caution is warranted before concluding
that these treatments were similarly efficacious. None of the comparison trials was adequately
powered to establish equivalence (see Text, Supplemental Digital Content 5, which describes the
comparison trials).
There are limitations to our study. First, we used an inclusive approach to trial selection;
however, our sensitivity analyses suggested this approach had little effect on the magnitude of

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT18
the therapy-control difference. Second, we found significant heterogeneity in the overall sample
and in the waitlist, TAU, and attention control groups; however, some of the heterogeneity in the
overall analysis was explained by the different control groups employed. Third, year of study
was highly correlated with study quality, and both were inversely related to the SMDs.
Combining studies over a period of 30 years likely diluted the results of recent, higher quality
studies. Fourth, the analysis of other factors (e.g. age, severity) was limited to mean values for
the trial. Different results might be obtained with an individual patient-level analysis. Lastly, we
performed a number of exploratory analyses without correcting for multiple comparisons.
Our results indicate that psychotherapy is effective in older depressed adults and that the
magnitude of the effect varies considerably with the type of control. The large within-group
effect that occurs with supportive psychotherapy underscores the importance of controlling for
the non-specific effects of all supportive interventions. Compared with supportive therapy,
psychotherapy has a moderate effect size of about 0.3 to 0.4, which appears to be a reasonable
current estimate of the efficacy in older adults. Although smaller than reported in prior reviews,
this is a meaningful effect. Problem-solving therapy has the strongest evidence base using
supportive therapy as a control, but only one of these trials was large. The superiority of one
therapy over another in depressed elders using direct comparisons has not been established.
The results of our study emphasize the importance of selecting appropriate control groups
in future psychotherapy trials. Our findings indicate that the magnitude of psychotherapy effects
will vary with the type of control employed. Although a waitlist condition may control for time,
these data suggest the change associated spontaneous improvement is slight. Alternatively
change associated with supportive therapy or placebo plus clinical management is considerable.
If the intent of a psychotherapy trial is to demonstrate that a specific form of psychotherapy is

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT19
superior to non-specific supportive effects of clinic visits, then a supportive therapy control is
required. If the intent is to determine effectiveness relative to current practice, then a treatment-
as-usual control is appropriate.
A TAU control might be especially appropriate if the intervention focuses on clinical
management. If a TAU control is employed, investigators should report what treatments were
actually received. A TAU control should not be employed when the research question is whether
a new therapy is as effective or superior to a common current treatment. In that case, the trial
should be designed as a comparison trial so that the “best practice” of each treatment is
compared. Given the effectiveness of supportive clinic visits, the role and value of the waitlist or
attention control conditions seem questionable. Finally, given the central role of non-specific
supportive elements in both psychotherapy and clinical management during antidepressant
treatment, investigation of the therapeutic effects of these elements is essential.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT20
References
1. Snowdon J, Almeida OP: The diagnosis and treatment of unipolar depression in late life, in
Late-life Mood Disorders. Edited by Lavretsky H, Sajatovic M, Reynolds CF, III. Oxford,
Oxford University Press, 2013, pp 79-103.
2. Nelson JC, Delucchi K, Schneider LS: Antidepressant in late-life depression: a meta-analysis
of the evidence. Am J Geriatr Psychiatry 2008;16:558-567.
3. Pinquart M, Sorensen S: How effective are psychotherapeutic and other psychosocial
interventions in older adults? A meta-analysis. J Ment Health Aging 2001;7:207-243.
4. Mackin RS, Areán PA: Evidence-based psychotherapeutic interventions for geriatric
depression. Psychiatr Clin North Am 2005; 28:805-820.
5. Cuijpers P, van Straten A, Smit F: Psychological treatment of late-life depression: a meta-
analysis of randomized controlled trials. Int J Geriatr Psychiatry 2006;21:1139-1149.
6. Pinquart M, Duberstein PR, Lyness JM: Treatments for later-life depressive conditions: a
meta-analytic comparison of pharmacotherapy and psychotherapy. Am J Psychiatry
2006;163(9):1493-1501.
7. Wilson K, Mottram PG, Vassilas C: Psychotherapeutic treatments for older depressed people.
Cochrane Database of Systematic Reviews 2008; Issue 1, Art. No.: CD004853.
8. Baskin TW, Tierney SC, Minami T, et al: Establishing specificity in psychotherapy: a meta-
analysis of structural equivalence of placebo controls. J Consult Clin Psychol 2003;71:973-
979.
9. Barth J, Munder T, Gerger H, et al: Comparative efficacy of seven psychotherapeutic
interventions for patients with depression: a network meta-analysis. PLOS Medicine [serial
online]. May 2013;10(5): e1001454. Available from: www.plosmedicine.org. Accessed
November 20, 2013.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT21
10. Wampold BE. The great psychotherapy debate: models, methods, and findings. Mahwah,
New Jersey: Erlbaum; 2001.
11. Psychotherapy: randomized controlled and comparative trials
(http://www.psychotherapyrcts.org) [database online]. Amsterdam: Vrije Universiteit
Amsterdam; 2013. Updated June 14, 2013.
12. Kocsis JH, Gerber AJ, Milrod B, et al. A new scale for assessing the quality of randomized
clinical trials of psychotherapy. Compr Psychiatry 2010;51:319-324.
13. Higgins JPT, Deeks JJ, Altman DG (editors). Chapter 16: Special topics in statistics. In:
Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions
Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from
www.cochrane-handbook.org
14. Nelson JC, Delucchi K, Schneider LS: Moderators of outcome in late-life depression: a
patient-level meta-analysis. Am J Psychiatry 2013; 170:651–659.
15. Egger M, Smith GD, Schneider M, et al. Bias in meta-analysis detected by a simple,
graphical test. BMJ 1997;315:629–34
16. Alexopoulos GS, Raue P, Arean P. Problem-solving therapy versus supportive therapy in
geriatric major depression with executive dysfunction. Am J Geriatr Psychiatry 2003;11:46-
52.
17. Arean PA, Perri MG, Nezu AM, et al. Comparative effectiveness of social problem-solving
therapy and reminiscence therapy as treatments for depression in older adults. J Consult Clin
Psychol 1993;61:1003-10.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT22
18. Arean, PA, Raue, P, Mackin RS, et al. Problem-solving therapy and supportive therapy in
older adults with major depression and executive dysfunction. Am J Psychiatry 2010;167:
1391-1398.
19. Beutler LE, Scogin F, Kirkish P, et al. Group cognitive therapy and alprazolam in the
treatment of depression in older adults. J Consult Clin Psychol 1987;55:550-556.
20. Ekkers W, Korrelboom K, Huijbrechts I, et al. Competitive Memory Training for treating
depression and rumination in depressed older adults: A randomized controlled trial.
Behaviour Research and Therapy 2011;49:588-96.
21. Floyd M, Scogin F, McKendree-Smith NL, et al. Cognitive therapy for depression: a
comparison of individual psychotherapy and bibliotherapy for depressed older adults. Behav
Modif 2004;28:297-318.
22. Fry PS. Structured and unstructured reminiscence training and depression among the elderly.
Clin Gerontol 1983;1:15-37.
23. Gallagher D. Behavioral group therapy with elderly depressives: An experimental study.
Upper D. & Ross S. (Eds). Behavioral group therapy. Champaign: Research Press. 1981;
187-224.
24. Gellis ZD, McGinty J, Horowitz A, et al. Problem-solving therapy for late-life depression in
home care: a randomized field trial. Am J Geriatr Psychiatry 2007;15:968-978.
25. Hanser SB, Thompson LW. Effects of a music therapy strategy on depressed older adults. J
Gerontol 1994;49:P265-269.
26. Haringsma R, Engels GI, Cuijpers P, et al. Effectiveness of the Coping With Depression
(CWD) course for older adults provided by the community-based mental heatlth care system
in the Netherlands: a randomized controlled field trial. Int Psychogeriatr 2006;18:307-325.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT23
27. Joling KJ, van Hout HP, van't Veer-Tazelaar PJ, et al. How effective is bibliotherapy for very
old adults with subthreshold depression? A randomized controlled trial. Am J Geriatr
Psychiatry 2011;19:256-65.
28. Kiosses DN, Arean PA, Teri L, et al. Home-delivered problem adaptation therapy (PATH)
for depressed, cognitively impaired, disabled elders: A preliminary study. Am J Geriatr
Psychiatry. 2010;18: 988-998.
29. Laidlaw K, Davidson K, Toner H, et al.. A randomised controlled trial of cognitive behaviour
therapy vs treatment as usual in the treatment of mild to moderate late life depression. Int J
Geriatr Psychiatry. 2008 ; 23:843–850.
30. Lamers F, Jonkers CC, Bosma H, et al. A minimal psychological intervention in chronically
ill elderly patients with depression: a randomized trial. Psychother Psychosom 2010;79:217-
226.
31. Landreville P, Bissonnette L. Effects of cognitive bibliotherapy for depressed older adults
with a disability. Clin Gerontol 1997;17:35-55.
32. Mossey JM, Knott KA, Higgins M, et al. Effectiveness of a psychosocial intervention,
interpersonal counseling, for subdysthymic depression in medically ill elderly. J Gerontol
Biol Sc Med Sc. 1996; 51:M172-M178.
33. Rokke PD, Tomhave AJ, Jocic Z. Self-management therapy and educational group therapy
for depressed elders. Cognit Ther Res 2000;24:99-119.
34. Scogin F, Hamblin D, Beutler L. Bibliotherapy for depressed older adults: A self-help
alternative. Gerontol 1987;27:383-7.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT24
35. Scogin F, Jamison C, Gochneaur K. Comparative efficacy of cognitive and behavioral
bibliotherapy for mildly and moderately depressed older adults. J Consult Clin Psychol
1989;57:403-7.
36. Serfaty MA, Haworth D, Blanchard M, et al. Clinical effectiveness of individual cognitive
behavioral therapy for depressed older people in primary care: A randomized controlled trial.
Arch Gen Psychiatry 2009;66:1332-1340.
37. Serrano JP, Latorre JM, Gatz M, et al. Life review therapy using autobiographical retrieval
practice for older adults with depressive symptomatology. Psychol Aging 2004;19:270-7.
38. Sloane RB, Staples FR, Schneider LS. Interpersonal therapy vs. nortriptyline for depression
in the elderly. Clinical and pharmacological studies in psychiatric disorders, Burrows GD,
Norman TR (eds). John Libby: London, 1985, pp. 344–346.
39. Thompson LW, Gallagher D, Breckenridge JS. Comparative effectiveness of psychotherapies
for depressed elders. J Consult Clin Psychol 1987;55:385-90
40. van Schaik A, van Marwijk H, Ader H, et al. Interpersonal psychotherapy for elderly patients
in primary care. Am J Geriatr Psychiatry 2006;14:777-86.
41. Watt LM, Cappeliez P. Integrative and instrumental reminiscence therapies for depression in
older adults: intervention strategies and treatment effectiveness. Aging Ment Health.
2000;4:166-77.
42. Williams JW, Barrett J, Oxman T, et al. Treatment of dysthymia and minor depression in
primary care: A randomized controlled trial in older adults. JAMA 2000; 284:1519-26.
43. Rosenthal D, Frank JD. Psychotherapy and the placebo effect. Psychol Bull 1956;53:294-302.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT25
44. Papakostas GI, Fava M. Does the probability of receiving placebo influence clinical trial
outcome? A meta-regression of double-blind, randomized clinical trials in MDD. Eur
Neuropsychopharmacol 2009;19:34–40.
45. Rutherford BR, Sneed JR, Roose SP. Does study design influence outcome? The effects of
placebo control and treatment duration in antidepressant trials. Psychother Psychosom
2009;78:172-81.
46. Rutherford BR, Mori S, Sneed JR, et al. Contribution of spontaneous improvement to
placebo response in depression: a meta-analytic review. J Psychiatr Res. 2012;46:697-702.
47. Rutherford BR, Tandler J, Brown PJ, et al. Clinic visits in late life depression trials: effects
on signal detection and therapeutic outcome. Am J Geriatr Psychiatry 2013 Nov 4 [Epub
ahead of print].
48. Gallagher DE, Thompson LW: Treatment of major depressive disorder in older adult
outpatients with brief psychotherapies. Psychotherapy 1982;19:482-490.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT26
Figure Legend
Figure 1. Search flow: trials identified and search process
Figure 2. Standardized mean differences for each treatment-control contrast, for each subgroup by type of control, and for all trials combined using a random effects meta-analysis Figure 3. Standardized Mean Difference and 95% confidence interval for change within each type of control group.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 1. Characteristics of Included Trials
Authors Year Definition of Depression Minimum Age
Na Treatment Conditions Trial Duration
# Sessions
Alexopolous et al. (16) 2003 MDD + HRSD≥18 65 12 PST 12 12 13 ST 12 Arean et al. (17) 1993 MDD + HRSD≥18 + BDI≥20 + GDS≥10 55 19 PST-GP 12 12 20 REM-GP 12 20 WL NA Arean et al. (18) 2010 MDD + HRSD≥20 60 110 PST 12 12 111 ST 12 Beutler et al. (19) 1987 MDD + HRSD≥18 65 16 CT-GP + PC 20 NR 15 PC NR Ekkers et al. (20) 2011 MDD with rumination + GDS≥11 65 53 Competitive Memory Training + TAU 7 7 38 TAU NR Floyd et al. (21) 2004 MDD or MinorD or DD + HRSD≥10 60 13 Biblio 4 NA 8 CT 8 14 Delayed treatment (WL) NA Fry (22) 1983 BDI ≥ 19 65 54 Structured REM 5 5
54 Unstructured REM 5 54 AC 5 Gallagher (23) 1981 MMPI D-scale 2 SDs above mean 65 10 BT-GP 5 10 10 ST-GP 10 Gellis et al. (24) 2007 CES-D≥22 65 20 PST 8 6
20 TAU NR Hanser and Thompson 1994 MDD or Minor D 61 10 Home-based music CBT 8 8 (25) 10 WL NA Haringsma et al. (26) 2006 MDD 55 21 Coping with Depression-GP 10 10
22 WL Joling et al. (27) 2011 CES-D >16; Not MDD 75 86 CBT-Biblio 9 3
84 TAU NR Kiosses et al. (28) 2010 MDD + HRSD≥17 65 13 PATH 12 NR
12 ST 12 Laidlaw et al. (29) 2008 MDD + HRSD 7-24 + BDI 13-28 60 20 CBT 8 8c
20 TAU NR Lamers et al. (30) 2010 DD or minorD or mild-mod 60 127 MPI 6 4c MDD + HRSD≤18 135 TAU NR Landreville and 1997 GDS ≥11 55 10 CT-Biblio 4 NA Bissonnette (31) 13 Delayed treatment (WL) NA Mossey et al. (32) 1996 GDS≥11 + no current MDD or DD 60 31 IPC 12 10 38 TAU 10

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Rokke (33) 2000 MDD 60 9 Self-management therapy-GP 10 10 9 Education and support GP (ST) 10 16 Treatment on Demand (WL) NA Scogin et al. (34) 1987 HRSD≥10 60 9 CT Biblio 4 NA 8 AC Biblio NA 8 Delayed treatment (WL) NA Scogin et al. (35) 1989 HRSD≥10 60 21 CT Biblio 4 NA 19 BT Biblio NA 21 Delayed treatment (WL) NA Serfaty et al. (36) 2009 depression + BDI≥14 65 59 CBT + TAU 16 7c 56 Talking control (AC) + TAU 8c 52 TAU NR Serrano et al. (37) 2004 CES-D≥16 65 20 Life review therapy 6 6 23 No treatment (WL) NA Sloane et al. (38) 1985 MDD + HDRS≥17 60 19 IPT 6 6 10 Nortriptyline 6 14 PC 6 Thompson et al. (39) 1987 MDD + HRSD≥14 + BDI ≥17 60 27 CT 6 16-20 25 BT 16-20 24 Brief Psychodynamic Therapy 16-20 19 Delayed treatment (WL) NA van Schaik et al. (40) 2006 Depression + GDS≥5 55 69 IPT 22 8c 74 TAU NR Watt and Cappeliez (41) 2000 GDS≥14 60 12 Integrative REM-GP 6 6 9 Instrumental REM-GP 6 5 Socialization GP (AC) 6 Williams et al. (42) 2000 DD or minorD + HRSD≥10 60 138 PST + PC 11 6 140 PC 6
AC=attention control, BDI=Beck Depression Inventory, Biblio=bibliotherapy, BT=behavioral therapy, CBT=cognitive-behavioral therapy, CES-D=Center for Epidemiological Studies-Depression Scale, COPD=chronic obstructive pulmonary disease, CT=cognitive therapy, DD=dysthymic disorder, DM=type II diabetes mellitus, GDS=Geriatric Depression Scale, GP=group treatment, Home=Home-based care setting, HRSD=Hamilton Rating Scale for Depression, IPC=interpersonal counseling, IPT=interpersonal therapy, MDD=major depressive disorder MinorD=minor depression, MMPI D-scale=Minnesota Multiphasic Personality Inventory depression scale, MOS=months, MPI=minimal psychological treatment (elements of CBT, PST, and self-management), NR=not reported, OUT=Outpatient setting, PATH=home-delivered problem adaptation therapy, PC=placebo control, PST=problem-solving therapy, REM=reminiscence therapy, ST=supportive therapy, TAU=treatment as usual, usual care, WK=weeks, WL=waitlist control a. total number analyzed and reported (ITT if available or completer sample) b. Table shows contrasts were included in our analysis. c. Mean number of sessions

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 2. Potential Moderators of Treatment-Control Differences
a. Test for differences between the categories defined b. Excluding bibliotherapy c. Correlation of the variable with the SMD weighted for sample size
(revised Jan 2014)
Dichotomous Variables Number
Contrasts SMD 95% CI I2 Testa, df, p
All Studies 37 0.73 0.51, 0.95 84% Type of Control Waitlist 15 0.94 0.71, 1.17 34% X2=35.67, df=4,
p<0.00001 TAU 8 0.28 0.02, 0.53 71% Attention Control 6 1.36 0.36, 2.37 93% Supportive Therapy 5 0.39 0.16, 0.61 0% Placebo Control 3 0.05 -0.16,0.26 0% Type Depression Major Depression only 15 0.64 0.42, 0.87 49% X2=2.79, df=1
p=0.09 Other Depression 22 0.79 0.46, 1.12 89% Minimum Age ≥ 55 years 5 0.77 0.04, 1.50 86% X2=0.02, df=1,
p=0.89 ≥ 60 years 32 00.88 0.62, 1.14 87% Face-to-Face Therapy Yes 30 0.73 0.48, 0.98 86% X2=0.31, df=1,
p=0.58 No 7 0.73 0.21, 1.26 75% Type of Therapy Individual 21 0.72 0.42, 1.02 89% X2=6.45, df=2,
p=0.04 Group 8 0.81 0.36, 1.27 60% Bibliotherapy 7 0.73 0.21, 1.26 75% Site of Careb Home Care 4 1.20 0.72,1.68 33% X2=14.14, df=1, Clinic 26 0.66 0.40, 0.93 86% p=0.0002
Continuous Variables Number
Contrasts rc p
Mean Age 37 -0.28 0.09 Trial Duration 37 -0.40 0.01 Number Sessions 30 0.03 0.84 Depression Severity 37 0.31 0.06 Study Quality 37 -0.58 0.0002 Sample Size 37 -0.46 0.005 Year publication 37 0.65 <0.0001

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT53
Supplemental Materials
1. Conversion of scales used to an equivalent 17-item HRSD score (.docx)
2. Description of trials excluded in this study but included in prior reviews (.docx)
3. Regression analysis of other factors on the standardized mean difference (SMD)
weighted for sample size and controlling for type of control group in 27 late-life
depression psychotherapy trials with 37 contrasts (.docx)
4. Funnel plot of psychotherapy trials (.tiff)
5. Comparison trials (.docx)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1. Conversion of scales used to estimate 17-item HDRS scores
In order to estimate baseline depression severity for the meta-regression of associated
factors, we converted all scales to an equivalent 17-item HDRS score. To convert different
versions of the HRSD to the HRSD17 we used a proportion based on the maximum possible value
in non-psychotic patients. To convert Beck and GDS scores we calculated an average conversion
factor using all studies in this sample that reported both the HRSD and the Beck or the HRSD
and the GDS. No trial in this sample used the CES-D with the HDRS. We calculated an average
conversion factor from two other trials that used both the CES-D and the HDRS in 231 depressed
patients (1, 2).
1. Kim JY, Park JH, Lee JJ, et al. Standardization of the Korean version of the geriatric
depression scale: reliability, validity, and factor structure. Psychiatry Investig
2008;5:232-238.
2. Vieta E, deArce R, Jimenez-Arriero MA et al. Detection of subclinical depression in
bipolar disorder: a cross sectional, 4-month prospective follow-up study at community
mental health services (SIN-DEPRES). J Clin Psychiatry 2010;71:1465-1474.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2. Description of trials excluded in this study but included in prior reviews
Thirteen articles cited in other reviews were not included. In two articles data was
insufficient and could not obtained (1,2) We also excluded three comparison trials with no
control group (3-5), duplicate reports of included trials (6-9), trials that did not assess stand-alone
psychotherapies (10-12), and a trial in which psychotherapy was one part of a collaborative care
program (13).
References
1. Campbell JM. Treating depression in well older adults: use of diaries in cognitive
therapy. J Consult Clin Psychol 1992;66:7-18.
2. Fry PS. Cognitive training and cognitive-behavioral variables in the treatment of
depression in the elderly. Clin Gerontol 1984;3:25-45.
3. Gallagher DE, Thompson LW. Treatment of major depressive disorder in older adult
outpatients with brief psychotherapies. Psychotherapy 1982;19:482-490.
4. Klausner EJ, Clarkin JF, Spielman L. Late-life depression and functional disability: the
role of goal-focused group psychotherapy. Int J Geriat Psychiatry 1998;13:707-716.
5. Thompson LW, Coon DW, Gallagher-Thompson D. Comparison of desipramine and
cognitive/behavioural therapy in the treatment of elderly outpatients with mild-to-
moderate depression. Am J Geriatr Psychiatry 2001;9:225-240.
6. Barrett JE, Williams JW, Oxman TE, et al. The Treatment Effectiveness Project. A
comparison of the effectiveness of paroxetine, problem-solving therapy, and placebo in

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
the treatment of minor depression and dysthymia in primary care patients: background
and research plan. General Hospital Psychiatry 1999;21:260–273.
7. Breckenridge JS, Zeiss AM, Breckenridge JN, et al. Solicitation of elderly depressives for
treatment outcome research: a comparison of referral sources. J Consult Clin Psychol
1985;53(4):552–4
8. Floyd M. Cognitive therapy for depression: a comparison of individual psychotherapy
and bibliotherapy for depressed older adults. Tuscaloosa: University of Alabama;
dissertation, 1998
9. Thompson LW, Gallagher D. Efficacy of psychotherapy in the treatment of late-life
depression. Adv Behav Res Ther 1984;6:127-139
10. Latour D, Cappeliez P. Pretherapy training for group cognitive therapy with depressed
older adults with a disability. Can J Aging 1994;13:221-235.
11. Lynch TR, Morse JQ, Mendelson T, et al. Dialectical behavior therapy for depressed
older adults: a randomized pilot study. Am J Geriatr Psychiatry 2003; 11:33-45.
12. Sirey JA, Bruce ML, Alexopoulos GS. The Treatment Initiation Program: An
intervention to improve depression outcomes in older adults. Am J Psychiatry 2005;
162(1):184-6.
13. Ciechanowski P, Wagner E, Schmaling K, et al. Community-integrated home-based
depression treatment in older adults; A randomized controlled trial. JAMA
2004;291:1569-1577.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3. Regression analysis of other factors on the standardized mean difference (SMD) weighted for
sample size and controlling for type of control group in 27 late-life depression psychotherapy
rrials with 37 contrasts
Parameter Estimate
df t-test p
Mean Age 0.024 1 0.87 0.39 Trial Duration 0.009 1 0.36 0.72 HDRS17 total 0.025 1 1.05 0.30 Study Quality -0.039 1 -1.40 0.17 Sample Size 0.001 1 0.83 0.41 Year of pub -0.029 1 -1.50 0.15
Although the overall model was significant (p < .003) with the adjusted r2 = .56, no individual
factor was significantly associated with the SMD; however, we note that the power of this
analysis to detect differences is limited by the number of contrasts (N=37).
Revised Feb 26, 2014

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5. Comparison trials
Our search identified 9 trials that compared active psychotherapies. Six of those trials (1-
6) were included in the preceding review of controlled trials. Three other comparison trials with
no control group were found (7-9). Our search did not identify any comparison trials published
since the Cuijpers review (10). Different from that review we did not include Gallagher 1981
(11) because we considered supportive therapy a type of control group. We did not include
Latour 1994 (12) because this was not a stand-alone treatment, and we did not include the
Thompson article from 1984 (13) which was an interim report published in final form in 1987
(5).
These 9 trials included 13 contrasts of which 10 were unique contrasts of different pairs,
e.g. PST vs. reminiscence, CT vs BT, CBT vs. dynamic, etc. The trials included 381 patients.
The largest had 54 in each arm, one other had an average of 25 per arm, and the other 7 trials had
less than 25 subjects per arm. Four of the trials were 4-6 weeks in length, four were 11-16 weeks,
and one was 36 weeks. Five of the trials were limited to subjects with MDD, the others included
other DSM depression diagnosis or defined depression with a scale threshold score. Only one of
the trials reported data from an intention-to-treat analysis, the others reported outcome in
completers.
Of the 13 contrasts of two psychotherapies, only 3 differed significantly. PST was more
effective than reminiscence therapy (1), structured reminiscence therapy was more effective than
unstructured reminiscence (3), and found goal-focused group therapy more effective than
reminiscence therapy (8). Because 10 contrasts were unique and 3 contrasts were only examined
twice, a meta-analysis did not appear indicated (i.e. there was no standard treatment with which
others could be compared).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Ten of the contrasts found no significant difference between therapies; however, we
would be cautious about concluding that they have similar efficacy. As noted above, only one of
the contrasts included more than 30 subjects per arm, the minimal number recommended for
treatment trials in depression (14). None of the comparisons were of sufficient size to establish
equivalence.
References
1. Arean PA, Perri MG, Nezu AM, Schein RL, Christopher F, Joseph TX. Comparative
effectiveness of social problem-solving therapy and reminiscence therapy as treatments
for depression in older adults. J Consult Clin Psychol 1993;61:1003-10.
2. Floyd M, Scogin F, McKendree-Smith NL, Floyd DL, Rokke PD. Cognitive therapy for
depression: a comparison of individual psychotherapy and bibliotherapy for depressed
older adults. Behav Modif 2004;28:297-318.
3. Fry PS. Structured and unstructured reminiscence training and depression among the
elderly. Clin Gerontol 1983;1:15-37.
4. Scogin F, Jamison C, Gochneaur K. Comparative efficacy of cognitive and behavioral
bibliotherapy for mildly and moderately depressed older adults. J Consult Clin Psychol
1989;57:403-7
5. Thompson LW, Gallagher D, Breckenridge JS. Comparative effectiveness of
psychotherapies for depressed elders. J Consult Clin Psychol 1987;55:385-90
6. Watt LM, Cappeliez P. Integrative and instrumental reminiscence therapies for
depression in older adults: intervention strategies and treatment effectiveness. Aging
Ment Health. 2000;4:166-77.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7. Gallagher DE, Thompson LW. Treatment of major depressive disorder in older adult
outpatients with brief psychotherapies. Psychotherapy 1982;19:482-490.
8. Klausner EJ, Clarkin JF, Spielman L. Late-life depression and functional disability: the
role of goal-focused group psychotherapy. Int J Geriat Psychiatry 1998;13:707-716.
9. Steuer JL, Mintz J, Hammen CL, Hill MA, Jarvik LF, McCarley T, Motoike P, Rosen R.
Cognitive-Behavioral and Psychodynamic Group Psychotherapy in Treatment of
Geriatric Depression. J Consult Clin Psych 1984;52(2):180-189
10. Cuijpers P, van Straten A, Smit F. Psychological treatment of late-life depression: a meta-
analysis of randomized controlled trials. Int J Geriatr Psychiatry 2006; 21(12):1139-49.
11. Gallagher D. Behavioral group therapy with elderly depressives: An experimental study.
Upper D. & Ross S. (Eds). Behavioral group therapy. Champaign: Research Press 1981;
187-224.
12. Latour D, Cappeliez P. Pretherapy training for group cognitive therapy with depressed
older adults with a disability. Can J Aging 1994; 13:221-235.
13. Thompson LW, Gallagher D. Efficacy of psychotherapy in the treatment of late-life
depression. Adv Behav Res Ther 1984; 6:127-139
14. Lieberman JA, Greenhouse J, Hamer RM, Krishnan KR, Nemeroff CB, Sheehan DV,
Thase ME, Keller MB. Comparing the effects of antidepressants: consensus guidelines
for evaluating quantitative reviews of antidepressant efficacy. Neuropsychopharmacology
2005;30(3):445-60.