
HSV-2 Meningitis Presenting with Acute Hydrocephalus ... · Central JSM Neurosurgery and Spine....
3
Central JSM Neurosurgery and Spine Cite this article: Infinger LK, Varma AK (2014) HSV-2 Meningitis Presenting with Acute Hydrocephalus Ultimately Requiring Long Term CSF Diversion. JSM Neurosurg Spine 2(1): 1012. *Corresponding author Libby Kosnik Infinger, 96 Jonathan Lucas St. Suite 301 CSB, Charleston, South Carolina 29425, USA, Tel: 843- 697-5056; Fax: 873-792-9279; Email: Submitted: 27 November 2013 Accepted: 12 January 2014 Published: 16 January 2014 Copyright © 2014 Infinger et al. OPEN ACCESS Keywords • Hydrocephalus • Meningitis • Herpes simplex virus • Aqueductal stenosis • Ventriculoperitoneal shunt Case Report HSV-2 Meningitis Presenting with Acute Hydrocephalus Ultimately Requiring Long Term CSF Diversion Libby Kosnik Infinger* and Abhay K. Varma Department of Neurosciences, Division of Neurosurgery, Medical University of South Carolina, USA Abstract Herpes simplex virus type 1 and 2 can infect the human nervous system causing meningitis and encephalitis. HSV meningitis tends to be benign, but HSF encephalitis can have a high morbidity and mortality despite treatment. We present a case of HSV meningitis leading to hydrocephalus without evidence of encephalitis. The patient had persistent hydrocephalus requiring long term CSF diversion despite successful treatment of the infection. A 57 year old African-American female presented with acute decline in sensorium secondary to hydrocephalus. HSV type 2 was isolated from the CSF by polymerase chain reaction (PCR). There was no evidence of infiltrative lesion in the brain parenchyma on MRI. She was treated with CSF diversion and antiviral therapy. The meningitis was successfully treated, but the patient required ventriculoperitoneal shunt placement due to persistent hydrocephalus. This is the second reported case of post HSV-2 meningitis presenting with acute hydrocephalus, and first reported case of persistent hydrocephalus following HSV-2 meningitis. Adult HSV-2 meningitis usually has a benign course. Hydrocephalus is rare sequelae of this condition. The patient in this case was treated for HSV meningitis, and the virus was cleared from the CSF upon repeat PCR testing. Aqueductal stenosis from ependymal inflammation may play a role in the pathophysiology of hydrocephalus. This is the first reported case of persistent hydrocephalus following HSV-2 meningitis that required a permanent CSF diversionary procedure. Viral etiology should be actively sought in a case of spontaneous and unexplained hydrocephalus, even in an adult. ABBREVIATIONS HSV: Herpes Simplex Virus; PCR: polymerase chain reaction; CSF: Cerebral Spinal Fluid; VPS: Ventricular Peritoneal Shunt INTRODUCTION Herpes simplex Virus (HSV) type 1 and type 2 can infect the human nervous system. HSV is the commonest cause of sporadic encephalitis [1]. HSV can also cause meningitis, myelitis and radiculitis [2]. HSV encephalitis carries a grave prognosis. Mortality reaches 70% in untreated patients and can be as high as 30% in treated patients with a high incidence of severe neurological deficit in survivors [2]. The clinical course of HSV meningitis tends to be benign. HSV associated aseptic meningitis occurs often after primary HSV-2 genital infection [3]. HSV-1 is more commonly associated with encephalitis [4]. We present a case of HSV-2 meningitis leading to hydrocephalus without evidence of intracranial lesion. This is the second case reported in the literature of post HSV-2 meningitis presenting with acute hydrocephalus. In the first case, the patient was not treated with anitvirals, and did not require long-term CSF diversion [16]. Our case is unique in that the patient had persistent hydrocephalus requiring ventricular peritoneal shunt placement despite successful treatment of the infection. Ependymal inflammation with aqueductal narrowing may be the cause of hydrocephalus. CASE PRESENTATION A 57 year old African American woman presented to an outside hospital with a three day history of lethargy, decreased oral intake, and decreased speaking. She was treated for dehydration and released. When her symptoms persisted she returned to the same facility and a computerized tomogram (CT) revealed acute hydrocephalus (Figure 1). She was transferred to our facility for neurosurgical care. She had a history of ovarian cancer at age 18 and was also successfully treated for lymphoma in the past per her family. On examination she had a GCS of 10. Fundoscopic exam revealed bilateral papilledema. An external ventricular drain (EVD) was placed revealing an opening pressure of 52 cm of H 2 O. Initial CSF analysis revealed: RBC 213cumm, WBC 52cumm, Neutrophils 11%, Lymphocytes 80%, Glucose 73 mg/dl, Protein 42 mg/dl, Gram stain was negative for bacteria. HSV polymerase chain reaction (PCR) was positive for HSV-2. Her mental status improved after placement of the EVD and GCS was then 13. Contrast enhanced magnetic resonance imaging (MRI) after EVD insertion showed diffuse
Transcript of HSV-2 Meningitis Presenting with Acute Hydrocephalus ... · Central JSM Neurosurgery and Spine....
Central JSM Neurosurgery and Spine
Cite this article: Infinger LK, Varma AK (2014) HSV-2 Meningitis Presenting with Acute Hydrocephalus Ultimately Requiring Long Term CSF Diversion. JSM Neurosurg Spine 2(1): 1012.
*Corresponding authorLibby Kosnik Infinger, 96 Jonathan Lucas St. Suite 301 CSB, Charleston, South Carolina 29425, USA, Tel: 843-697-5056; Fax: 873-792-9279; Email:
Submitted: 27 November 2013
Accepted: 12 January 2014
Published: 16 January 2014
Copyright© 2014 Infinger et al.
OPEN ACCESS
Keywords• Hydrocephalus• Meningitis• Herpes simplex virus• Aqueductal stenosis• Ventriculoperitoneal shunt
Case Report
HSV-2 Meningitis Presenting with Acute Hydrocephalus Ultimately Requiring Long Term CSF DiversionLibby Kosnik Infinger* and Abhay K. VarmaDepartment of Neurosciences, Division of Neurosurgery, Medical University of South Carolina, USA
Abstract
Herpes simplex virus type 1 and 2 can infect the human nervous system causing meningitis and encephalitis. HSV meningitis tends to be benign, but HSF encephalitis can have a high morbidity and mortality despite treatment. We present a case of HSV meningitis leading to hydrocephalus without evidence of encephalitis. The patient had persistent hydrocephalus requiring long term CSF diversion despite successful treatment of the infection.
A 57 year old African-American female presented with acute decline in sensorium secondary to hydrocephalus. HSV type 2 was isolated from the CSF by polymerase chain reaction (PCR). There was no evidence of infiltrative lesion in the brain parenchyma on MRI. She was treated with CSF diversion and antiviral therapy. The meningitis was successfully treated, but the patient required ventriculoperitoneal shunt placement due to persistent hydrocephalus. This is the second reported case of post HSV-2 meningitis presenting with acute hydrocephalus, and first reported case of persistent hydrocephalus following HSV-2 meningitis.
Adult HSV-2 meningitis usually has a benign course. Hydrocephalus is rare sequelae of this condition. The patient in this case was treated for HSV meningitis, and the virus was cleared from the CSF upon repeat PCR testing. Aqueductal stenosis from ependymal inflammation may play a role in the pathophysiology of hydrocephalus. This is the first reported case of persistent hydrocephalus following HSV-2 meningitis that required a permanent CSF diversionary procedure. Viral etiology should be actively sought in a case of spontaneous and unexplained hydrocephalus, even in an adult.
ABBREVIATIONSHSV: Herpes Simplex Virus; PCR: polymerase chain reaction;
CSF: Cerebral Spinal Fluid; VPS: Ventricular Peritoneal Shunt
INTRODUCTIONHerpes simplex Virus (HSV) type 1 and type 2 can infect
the human nervous system. HSV is the commonest cause of sporadic encephalitis [1]. HSV can also cause meningitis, myelitis and radiculitis [2]. HSV encephalitis carries a grave prognosis. Mortality reaches 70% in untreated patients and can be as high as 30% in treated patients with a high incidence of severe neurological deficit in survivors [2]. The clinical course of HSV meningitis tends to be benign. HSV associated aseptic meningitis occurs often after primary HSV-2 genital infection [3]. HSV-1 is more commonly associated with encephalitis [4]. We present a case of HSV-2 meningitis leading to hydrocephalus without evidence of intracranial lesion. This is the second case reported in the literature of post HSV-2 meningitis presenting with acute hydrocephalus. In the first case, the patient was not treated with anitvirals, and did not require long-term CSF diversion [16]. Our case is unique in that the patient had persistent hydrocephalus requiring ventricular peritoneal shunt placement despite
successful treatment of the infection. Ependymal inflammation with aqueductal narrowing may be the cause of hydrocephalus.
CASE PRESENTATIONA 57 year old African American woman presented to an
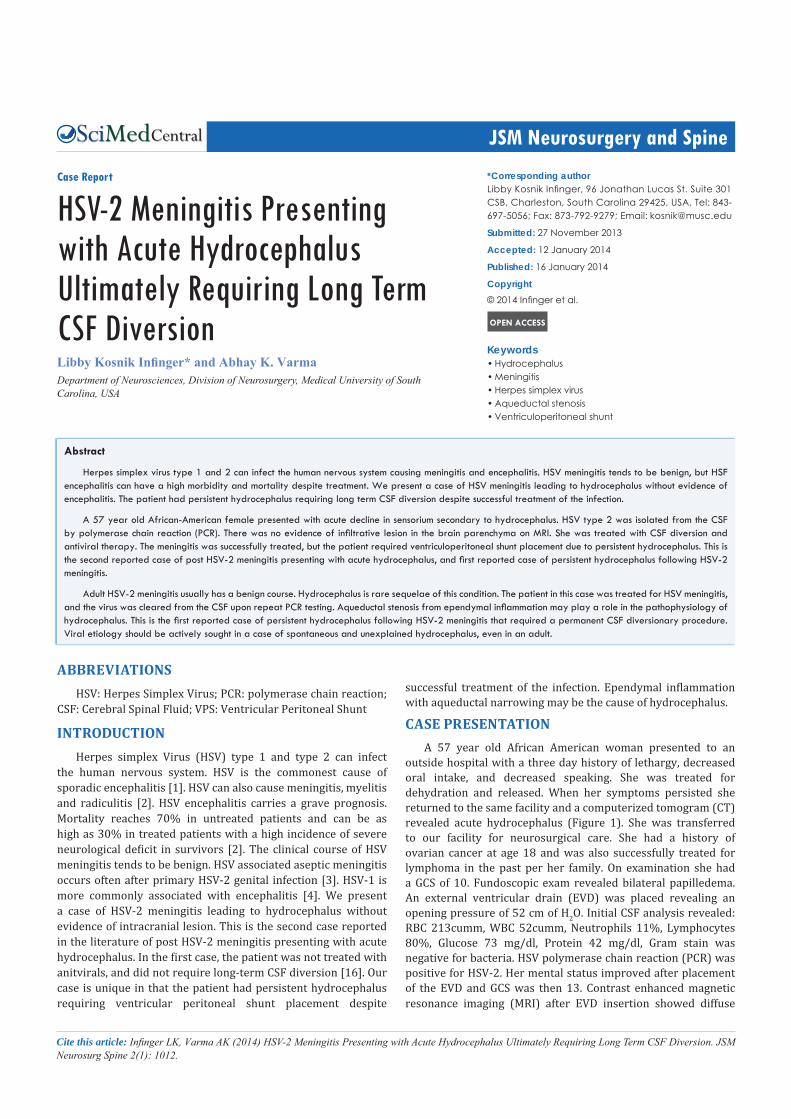
outside hospital with a three day history of lethargy, decreased oral intake, and decreased speaking. She was treated for dehydration and released. When her symptoms persisted she returned to the same facility and a computerized tomogram (CT) revealed acute hydrocephalus (Figure 1). She was transferred to our facility for neurosurgical care. She had a history of ovarian cancer at age 18 and was also successfully treated for lymphoma in the past per her family. On examination she had a GCS of 10. Fundoscopic exam revealed bilateral papilledema. An external ventricular drain (EVD) was placed revealing an opening pressure of 52 cm of H2O. Initial CSF analysis revealed: RBC 213cumm, WBC 52cumm, Neutrophils 11%, Lymphocytes 80%, Glucose 73 mg/dl, Protein 42 mg/dl, Gram stain was negative for bacteria. HSV polymerase chain reaction (PCR) was positive for HSV-2. Her mental status improved after placement of the EVD and GCS was then 13. Contrast enhanced magnetic resonance imaging (MRI) after EVD insertion showed diffuse
Central
Infinger et al. (2014)Email: [email protected]
JSM Neurosurg Spine 2(1): 1012 (2014) 2/3
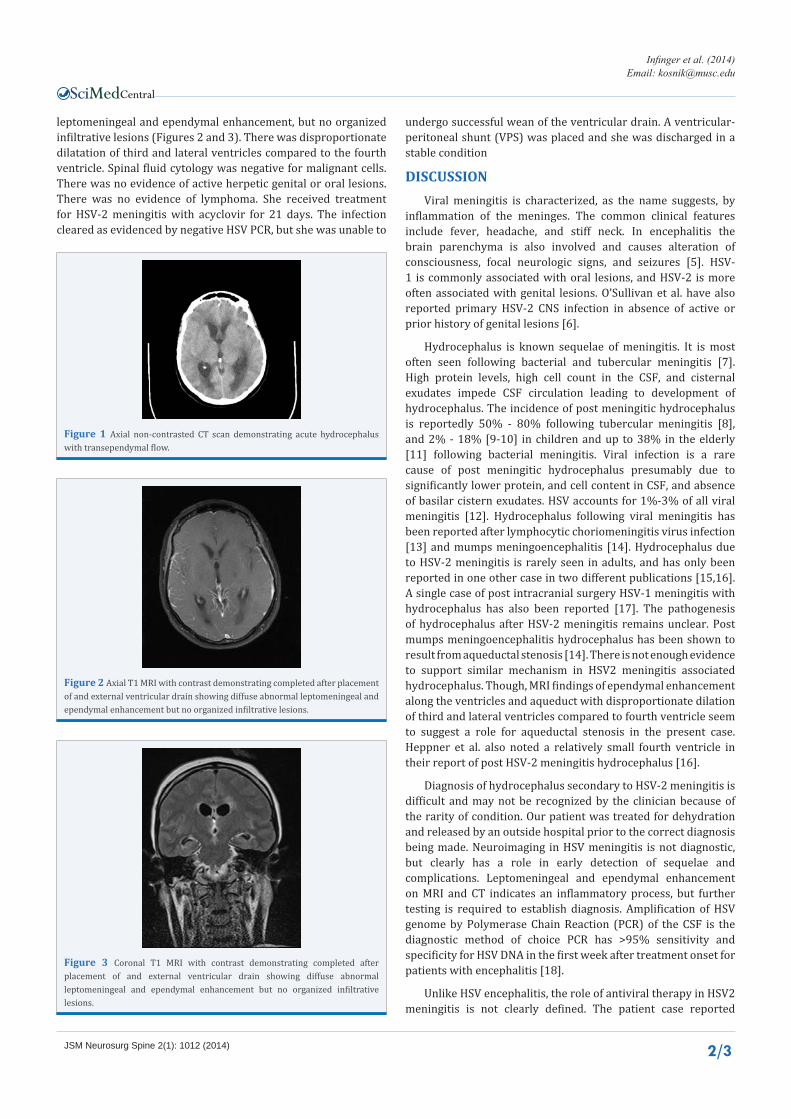
leptomeningeal and ependymal enhancement, but no organized infiltrative lesions (Figures 2 and 3). There was disproportionate dilatation of third and lateral ventricles compared to the fourth ventricle. Spinal fluid cytology was negative for malignant cells. There was no evidence of active herpetic genital or oral lesions. There was no evidence of lymphoma. She received treatment for HSV-2 meningitis with acyclovir for 21 days. The infection cleared as evidenced by negative HSV PCR, but she was unable to
undergo successful wean of the ventricular drain. A ventricular-peritoneal shunt (VPS) was placed and she was discharged in a stable condition
DISCUSSION Viral meningitis is characterized, as the name suggests, by
inflammation of the meninges. The common clinical features include fever, headache, and stiff neck. In encephalitis the brain parenchyma is also involved and causes alteration of consciousness, focal neurologic signs, and seizures [5]. HSV-1 is commonly associated with oral lesions, and HSV-2 is more often associated with genital lesions. O’Sullivan et al. have also reported primary HSV-2 CNS infection in absence of active or prior history of genital lesions [6].
Hydrocephalus is known sequelae of meningitis. It is most often seen following bacterial and tubercular meningitis [7]. High protein levels, high cell count in the CSF, and cisternal exudates impede CSF circulation leading to development of hydrocephalus. The incidence of post meningitic hydrocephalus is reportedly 50% - 80% following tubercular meningitis [8], and 2% - 18% [9-10] in children and up to 38% in the elderly [11] following bacterial meningitis. Viral infection is a rare cause of post meningitic hydrocephalus presumably due to significantly lower protein, and cell content in CSF, and absence of basilar cistern exudates. HSV accounts for 1%-3% of all viral meningitis [12]. Hydrocephalus following viral meningitis has been reported after lymphocytic choriomeningitis virus infection [13] and mumps meningoencephalitis [14]. Hydrocephalus due to HSV-2 meningitis is rarely seen in adults, and has only been reported in one other case in two different publications [15,16]. A single case of post intracranial surgery HSV-1 meningitis with hydrocephalus has also been reported [17]. The pathogenesis of hydrocephalus after HSV-2 meningitis remains unclear. Post mumps meningoencephalitis hydrocephalus has been shown to result from aqueductal stenosis [14]. There is not enough evidence to support similar mechanism in HSV2 meningitis associated hydrocephalus. Though, MRI findings of ependymal enhancement along the ventricles and aqueduct with disproportionate dilation of third and lateral ventricles compared to fourth ventricle seem to suggest a role for aqueductal stenosis in the present case. Heppner et al. also noted a relatively small fourth ventricle in their report of post HSV-2 meningitis hydrocephalus [16].
Diagnosis of hydrocephalus secondary to HSV-2 meningitis is difficult and may not be recognized by the clinician because of the rarity of condition. Our patient was treated for dehydration and released by an outside hospital prior to the correct diagnosis being made. Neuroimaging in HSV meningitis is not diagnostic, but clearly has a role in early detection of sequelae and complications. Leptomeningeal and ependymal enhancement on MRI and CT indicates an inflammatory process, but further testing is required to establish diagnosis. Amplification of HSV genome by Polymerase Chain Reaction (PCR) of the CSF is the diagnostic method of choice PCR has >95% sensitivity and specificity for HSV DNA in the first week after treatment onset for patients with encephalitis [18].
Unlike HSV encephalitis, the role of antiviral therapy in HSV2 meningitis is not clearly defined. The patient case reported
Figure 1 Axial non-contrasted CT scan demonstrating acute hydrocephalus with transependymal flow.
Figure 2 Axial T1 MRI with contrast demonstrating completed after placement of and external ventricular drain showing diffuse abnormal leptomeningeal and ependymal enhancement but no organized infiltrative lesions.
Figure 3 Coronal T1 MRI with contrast demonstrating completed after placement of and external ventricular drain showing diffuse abnormal leptomeningeal and ependymal enhancement but no organized infiltrative lesions.

Central
Infinger et al. (2014)Email: [email protected]
JSM Neurosurg Spine 2(1): 1012 (2014) 3/3
Infinger LK, Varma AK (2014) HSV-2 Meningitis Presenting with Acute Hydrocephalus Ultimately Requiring Long Term CSF Diversion. JSM Neurosurg Spine 2(1): 1012.
Cite this article
by Heppner et al. recovered without antiviral therapy. In the absence of clear guidelines, we would recommend managing these patients in close collaboration with infectious disease service. Our patient was treated with a 21 day course of acyclovir therapy.
CONCLUSIONCentral nervous system infection with herpes simplex
virus can have a significant amount of morbidity and mortality. Hydrocephalus is rare sequelae of this condition. This case is the second reported case of HSV-2 meningitis presenting with acute hydrocephalus, and the first reported case of persistent hydrocephalus following HSV-2 meningitis. This is important for neurosurgical clinicians to be aware of in caring for patients who present with acute hydrocephalus and no intracranial lesions. PCR for identification of herpes viruses should be included in the diagnostic testing completed on patients presenting with acute hydrocephalus. Swift identification of the pathogen should be completed to get treatment underway therefore allowing permanent CSF diversion with hardware, allowing the patient to progress to recovery.
REFERENCES1. Kennedy PG. Herpes simplex virus and the nervous system. Postgrad
Med J. 1984; 60: 253-259.
2. Whitley RJ, Miller RL. Immunologic approach to herpes simplex virus. Viral Immunol. 2001; 14: 111-118.
3. Olson LC, Buescher EL, Artenstein MS, Parkman PD. Herpesvirus infections of the human central nervous system. N Engl J Med. 1967; 277: 1271-1277.
4. Corey L, Adams HG, Brown ZA, Holmes KK. Genital herpes simplex virus infections: clinical manifestations, course, and complications. Ann Intern Med. 1983; 98: 958-972.
5. Najioullah F, Bosshard S, Thouvenot D, Boibieux A, Menager B, Biron F, et al. Diagnosis and surveillance of herpes simplex virus infection of the central nervous system. J Med Virol. 2000; 61: 468-473.
6. O’Sullivan CE, Aksamit AJ, Harrington JR, Harmsen WS, Mitchell PS,
Patel R. Clinical spectrum and laboratory characteristics associated with detection of herpes simplex virus DNA in cerebrospinal fluid. Mayo Clin Proc. 2003; 78: 1347-1352.
7. Chatterjee S, Chatterjee U. Overview of post-infective hydrocephalus. Childs Nerv Syst. 2011; 27: 1693-1698.
8. Tandon V, Mahapatra AK. Management of post-tubercular hydrocephalus. Childs Nerv Syst. 2011; 27: 1699-1707.
9. Singhi P, Bansal A, Geeta P, Singhi S. Predictors of long term neurological outcome in bacterial meningitis. Indian J Pediatr. 2007; 74: 369-374.
10. Jadavji T, Biggar WD, Gold R, Prober CG. Sequelae of acute bacterial meningitis in children treated for seven days. Pediatrics. 1986; 78: 21-25.
11. Lai WA, Chen SF, Tsai NW, Chang CC, Chang WN, Lu CH, et al. Clinical characteristics and prognosis of acute bacterial meningitis in elderly patients over 65: a hospital-based study. BMC Geriatr. 2011; 11: 91.
12. Rotbart HA. Viral meningitis. Semin Neurol. 2000; 20: 277-292.
13. Al-Zein N, Boyce TG, Correa AG, Rodriguez V. Meningitis caused by lymphocytic choriomeningitis virus in a patient with leukemia. J Pediatr Hematol Oncol. 2008; 30: 781-784.
14. Cinalli G, Spennato P, Ruggiero C, Aliberti F, Maggi G. Aqueductal stenosis 9 years after mumps meningoencephalitis: treatment by endoscopic third ventriculostomy. Childs Nerv Syst. 2004; 20: 61-64.
15. Yap E, Ellis-Pegler R. Hydrocephalus in herpes simplex type 2 meningitis. J Infect. 2006; 53: e75-77.
16. Heppner PA, Schweder PM, Monteith SJ, Law AJ. Acute hydrocephalus secondary to herpes simplex type II meningitis. J Clin Neurosci. 2008; 15: 1157-1159.
17. Mallory GW, Wilson JW, Castner ML, Driscoll CL, Link MJ. Herpes simplex meningitis after removal of a vestibular schwannoma: case report and review of the literature. Otol Neurotol. 2012; 33: 1422-1425.
18. Tyler KL. Herpes simplex virus infections of the central nervous system: encephalitis and meningitis, including Mollaret’s. Herpes. 2004; 11 Suppl 2: 57A-64A.

![Post-mortem detection of six human herpesviruses (HSV-1, HSV … · 2019. 1. 9. · The Seeplex Meningitis-V1 ACE Detection [V2.0] PCR kit (Seegene, Seoul, Korea) for in vitro diagnostic](https://static.fdocuments.in/doc/165x107/5fbc07d3eb846918dd3a8263/post-mortem-detection-of-six-human-herpesviruses-hsv-1-hsv-2019-1-9-the-seeplex.jpg)
















