HPV and Cervical Cancer, Screening and Prevention and Cervical Cancer, Screening and Prevention John...
60
HPV and Cervical Cancer, Screening and Prevention John Ragsdale, MD July 12, 2018 CME Lecture Series
Transcript of HPV and Cervical Cancer, Screening and Prevention and Cervical Cancer, Screening and Prevention John...

HPV and Cervical Cancer, Screening and Prevention
John Ragsdale, MDJuly 12, 2018
CME Lecture Series
Presenter
Presentation Notes
This is a topic of medicine which is continuing to evolve – we will look at the progresss we made around screening, vaccinations and look at cases

We have come a long Way…
Presenter
Presentation Notes
Rates of cervical cancer have dropped to roughly ½ of what they were in the seventies. In fact from the 1930’s we have seen an 80% decline in the morbidity associated with cervical cancer

Prevalence HPV in Young Adults in U.S
Presenter
Presentation Notes
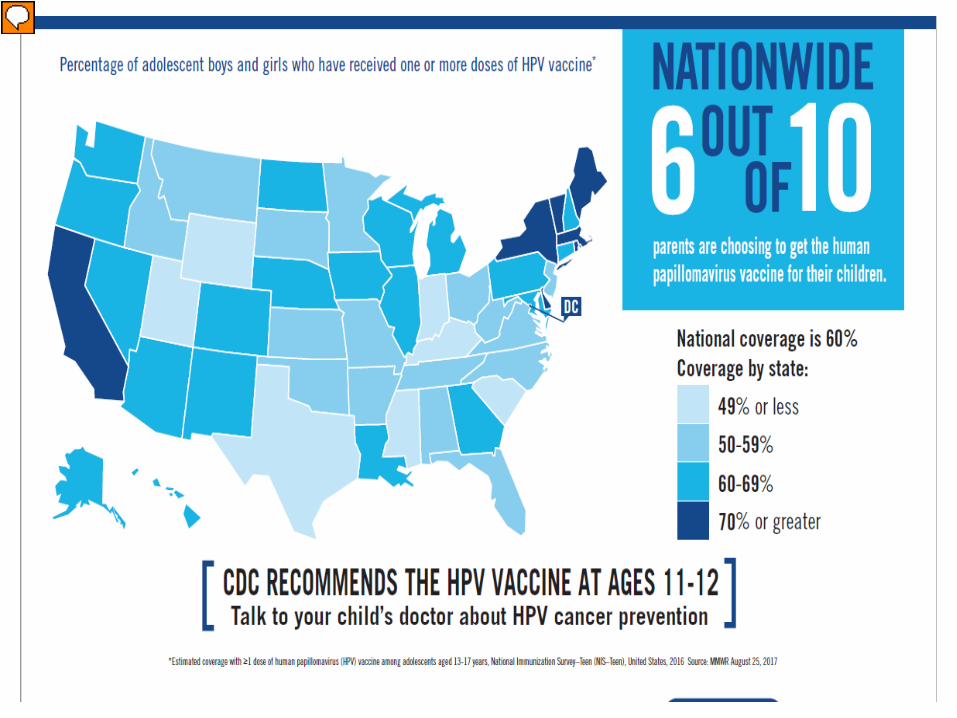
You will notice that happily, the rates are dropping due to increased rates of vaccination in the U.S. In fact you totaled the prevalence of all HPV serotypes from folks aged 18-59 – anyone want to hazard a guess as to that %?
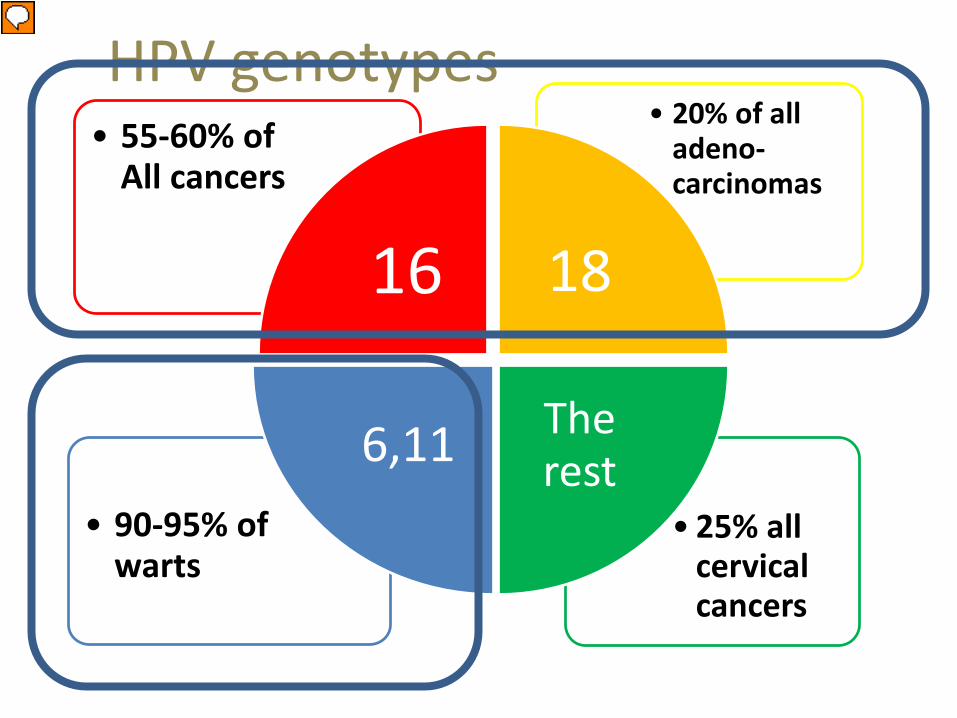
• 25% all cervical cancers
• 90-95% of warts
• 20% of all adeno-carcinomas
• 55-60% of All cancers
16 18
The rest6,11
HPV genotypes
Presenter
Presentation Notes
If you know these statistics then you know why HPV 16 and 18 were originally the focus of so much energy and research So not all HPV is created equal – most strains rarely if ever cause a problem And mostly they do not cause symptoms (hence the high prevalence)
Presenter
Presentation Notes
Do you know what your vaccination rates are? Do you have system of reminders? What strategies are you using to motivate parents and kids to get vaccinated? we are not doing a very good job at vaccinating in NC – we are below the national average Hep B discussion

HPV Vaccines • Gardisil 9:
– 6, 11, 16, 18, 31, 33, 45, 52, and 58
• Gardisil: – 6, 11, 16, and 18
• Cervarix:– 16 & 18 – For girls only
Presenter
Presentation Notes
16 & 18 cause 70 % of all HPV mediated cancers – do you know which you are offering in your clinic These vaccines as we will see are effective but you have to use them They will likely eventually cause a change in how we screen We do not know how long protection lasts – that is a very active field of study
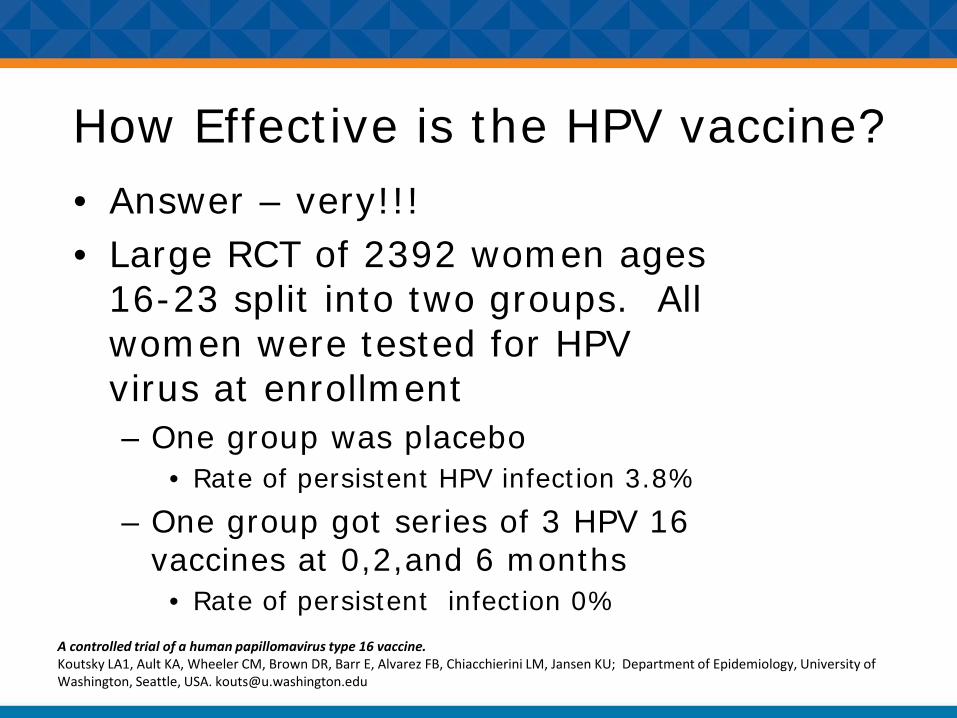
How Effective is the HPV vaccine? • Answer – very!!!• Large RCT of 2392 women ages
16-23 split into two groups. All women were tested for HPV virus at enrollment– One group was placebo
• Rate of persistent HPV infection 3.8%– One group got series of 3 HPV 16
vaccines at 0,2,and 6 months• Rate of persistent infection 0%
A controlled trial of a human papillomavirus type 16 vaccine.Koutsky LA1, Ault KA, Wheeler CM, Brown DR, Barr E, Alvarez FB, Chiacchierini LM, Jansen KU; Department of Epidemiology, University of Washington, Seattle, USA. [email protected]

HPV vaccine: efficacy • HPV Cancers U.S.
2008-12:– 38,793 HPV-associated
cancers (11.7 per 100,000 persons)
• 23,000 (13.5) among females
• 15,793 (9.7) among males.
– 30,700/38,793 = HPV attributed
– 28,500/38793 = Preventable
Human Papillomavirus–Associated Cancers —United States, 2008–2012 MMRW Weekly / July 8, 2016 / 65(26);661–666
23,000
15,793
HPV Cancers38,793
Women Men
74% Preventable
Presenter
Presentation Notes
Two things on this slide caught my attention – first – the high number of preventable cancers and secondly – the relatively high number of men that end up with HPV related cancers. What % of HPV is detected in all SCC and adenocarcs?: 99.7%

Risk Factors
Presenter
Presentation Notes
Smoking is assoc with SCC but NOT adenocarc Risk decreases by 50% after 10 yrs of quitting OCPs for 5-9 years assoc with hazard ratio of 2 – effect is hormonal – may be result of sex steroids on oncogenic expression – BUT CIN is not a contraindication to OCPs

Cervical Cancer Screening
Being rarely or never screened is THE major contributing factor to the MOST cervical cancer deaths today.
Presenter
Presentation Notes
According to the CDC Who is not screened? Minorities Low SES Foreign born and has lived in the U.S. less than 10 years No usual source of health care or fragmented healthcare –

Cervical Anatomy
s
Squamous epithelium
Transformation zone
Columnar epithelium
os
SC Junction
Presenter
Presentation Notes
So the cervix is a busy place cytologically -cells are changing from columnar to squamous (column to plate) It is forever transforming and remodeling which is required for it to function normally So this is just a reminder about what’s going on within the cervix anatomically and remember overtime the SC junction tends to migrate up into the OS making colposcopy more difficult

SETZ
SCJ
CE
TZ: transformation zone
SCJ: squamo-columnar junction
SE: squamous epithelium
CE: columnar epithelium
Presenter
Presentation Notes
Just as a quick reminder about anotomy From central to peripheral

Review of Pap Nomenclature & Results

A bit of Context…. • Bethesda system
– System for reporting cervical or vaginal cytologic diagnoses, used for reporting Pap smear results. It was introduced in 1988 and revised in 1991, 2001, and 2014.
• ASCCP: – Governing body – Devised rationale cytological definitions
then correlated with pathologic definitions– Established Guidelines:
• Based on data from 1.4 million women followed from Jan 2003 – December 31st 2010 at Kaiser
Presenter
Presentation Notes
Standardization began in the 80s when physicians began to realize there was no standard way of discussing pap abnormalities, and consequently, no standard parameters for treatment
Reflecting our evolving understanding HPV pathology
The ASCCP will no longer be referenced as the American Society for Colposcopy and Cervical Pathology – but rather now simply as the ASCCP, with a mission to improve lives through the prevention and treatment of ano-genital and other HPV-related diseases.
Presenter
Presentation Notes
From their webpage Mission for the ASCCP recently updated to reflect our increasing understanding of the role HPV plays in the development of cervical pathology and more importantly – and a rising emphasis on non cervical based HPV pathology – we will be looking at slides later on of the broader disease burden the HPV is responsible for – I think you will be surprised at the %s
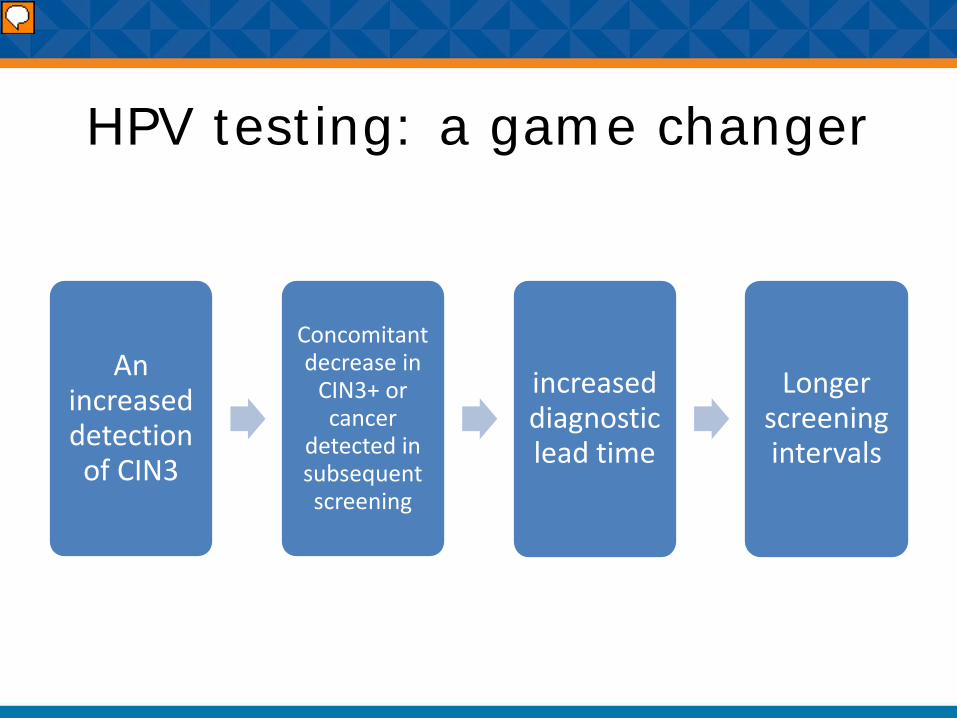
HPV testing: a game changer
An increased detection of CIN3
Concomitant decrease in
CIN3+ or cancer
detected in subsequent screening
increased diagnostic lead time
Longer screening intervals
Presenter
Presentation Notes
40% more sensitive at detecting CIN3+ however they have a lower specificity

HPV testing: a game changer
• Enhanced detection of women with adenocarcinoma of the cervix and its precursors
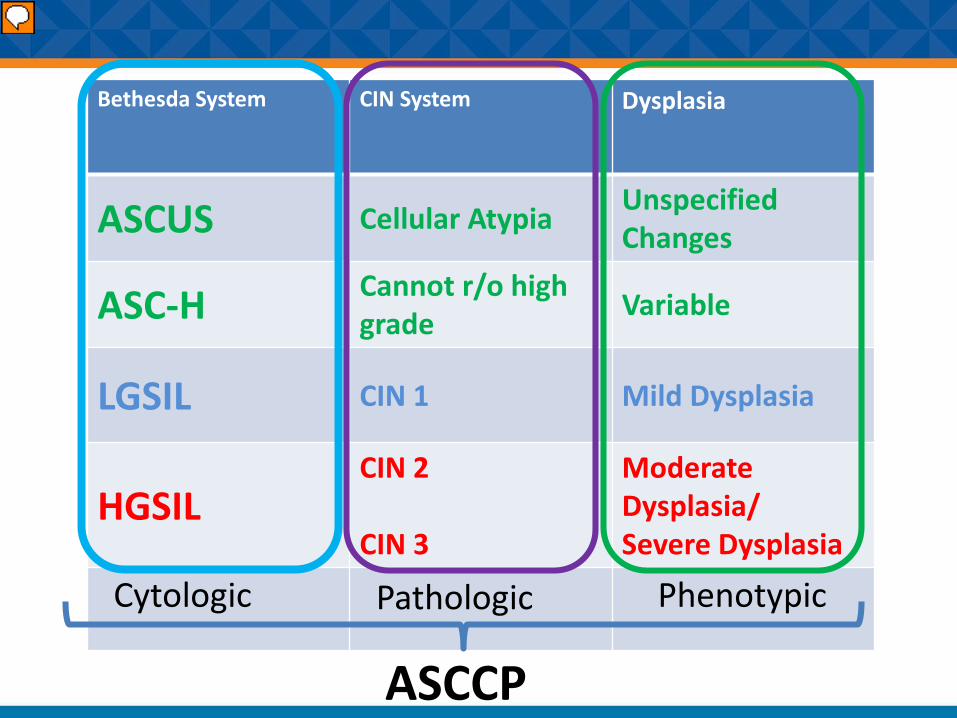
Bethesda System CIN System Dysplasia
ASCUS Cellular Atypia Unspecified Changes
ASC-H Cannot r/o high grade Variable
LGSIL CIN 1 Mild Dysplasia
HGSILCIN 2
CIN 3
Moderate Dysplasia/Severe Dysplasia
Cytologic Pathologic
ASCCP
Phenotypic
Presenter
Presentation Notes
The bottom two are cancer equivalents It was the conferences with the ASCCP with the foundational work by the Bethesda group that began to bring

ASCUS ASCUS – H
nuclear enlargement in Pap tests is due to reactive change
About 4% of total pap results
Not a cancer equivalent but evidence of infection
First exclude moderate/severe cervical intraepithelial neoplasia or carcinoma in-situ (CIN3/HSIL)
A rare but significant finding of a cancer equivalent
2% have cancer at time of pap
20% will go on to get cancer without proper care
Presenter
Presentation Notes
No cellular designation was originally more problematic than ASCUS during the first Bethesda meeting in 1988 Colposcopist don’t like ASCUS H

LGSIL / CIN 1 What % of low grade pap smears progress to CIN2 or greater?
A)12-16%B)Less than 3%C)18-22%
Mildly increase nuclear/cytoplasmic ratioMild/moderate staining
What happens to LGSIL?
• 60% of CIN 1 regresses
• 30% of CIN 1 persists
• 10% progress to CIN 3
• 1% may ultimately go on to invasive cancer
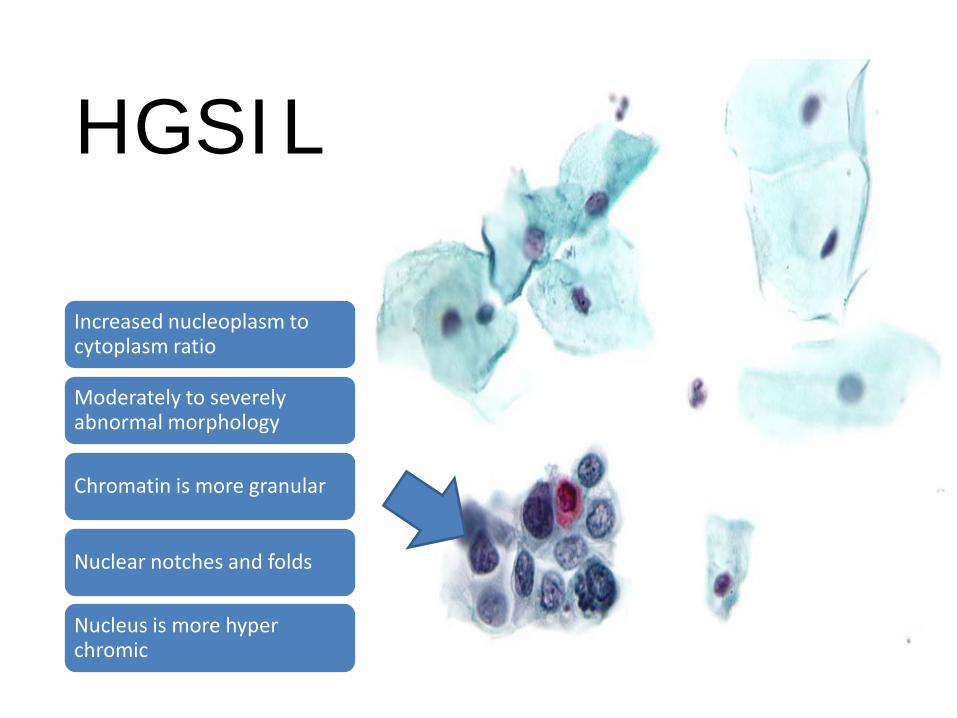
HGSIL
Increased nucleoplasm to cytoplasm ratio
Moderately to severely abnormal morphology
Chromatin is more granular
Nuclear notches and folds
Nucleus is more hyper chromic
Cervical cancer
Screening: Adolescents
• Care for contraception of STI screening / treatment is paramount
• NO pap test• NO speculum exam
for asymptomatic women
• STI screening can be done using urine
Treatment Saves Lives, but there is a cost….
• After LEEP women are more likely to have– Preterm birth (O.R 1.7– Low birth weight (O.R. 1..8)– PPROM (O.R. 2.7
• Increased risk (small) with perinatal death from incompetent cervix
• Risk rises with depth and number of LEEPs• Conization vs. laser treatment risks
essentially the same• Absolute risk is quite small
Case 1

CASE 1
A 21 year-old G0P0 presents to your office for her first gynecologic examination.
She has no symptoms or complaints and does not report chronic medical conditions.
She does not smoke or use illicit drugs.
She has had two male sexual partners in her lifetime and has been using combination oral contraceptive pills for the past 14 months.
She has completed her HPV immunization series

What is the screening interval for a 21 year old female?
• Pap and co-testing every three years
• Pap only every three years• Pap only every 5 years• Annual pap smear

Cervical Cancer Screening Women under 30
• HPV testing should not be used to screen
• NOT as a function of co-testing
• NOT as a primary stand alone screen
Cytology Aloneevery three years
• 20-30% prevalence of HPV in early 20s
• Vast majority cancer causing HPV infections resolve
• Call backs, anxiety, interventions
Why???

When is this ever going to clear????
• Most cervical HPV infections are transient
• Typically 12-24 months to clear most infections
• Who clears and why not fully understood
• 16-18 genotypes more likely to persist
• Younger women more likely to resolve

• A gynecologic exam is performed and cervical cytology is collected. Results of the cytology are as follows:
• Interpretation: Atypical squamous cells Cannot rule out high grade SIL (ASC-H)
• Adequacy: Satisfactory for evaluation.
• Transformation zone present.

What is the next step?
• Colposcopy• Repeat pap in 6 months• Repeat pap and co-testing in 6 months
• Diagnostic excisional procedure (LEEP)
Presenter
Presentation Notes
colposcopy is recommended. In this age group, triage to colposcopy is the same for ASC-H or HSIL. HPV testing is not recommended. A diagnostic excisional procedure (see and treat) is unacceptable. Although likely to have a higher HPV incidence, women aged 21-24 years have had on average, less time for a new HPV infection to produce treatable HSIL (CIN 2,3). However, if HSIL cytology is identified and in 0.6% of PAP results in the Katki study, the 5 year CIN 3+ risk is high and comparable to risks among women aged 25-29 years and 30-64 years. Importantly, the implicit 5.2% risk threshold for colposcopy is reached and colposcopy is recommended.

3-5% Acetic Acid has been applied. Which one of the following describes the colposcopic findings?
Squamocolumnar junction (SCJ) not fully visualized. Dense acetowhite epithelium with vessel changes.
SCJ not fully visualized. Dense acetowhite epithelium without vessel changes.
SCJ fully visualized. Dense acetowhite epithelium with vessel changes.
SCJ fully visualized. Dense acetowhite epithelium without vessel changes.

Management of women aged 21-24 years with biopsy confirmed HSIL
(CIN 2) and inadequate
colposcopy includes which one of the
following?
• Histology results– Cervix, 12:00 and
6:00, biopsy:(HSIL (CIN 2)
– A p16 immunostain is positive
– Endocervical curettage: Minute fragment of low-grade squamous intraepithelial lesion LSIL (CIN 1)
Diagnostic excisional procedure.
Ablative procedure. Cotesting in 1 year. Colposcopy and
cytology at 6 month intervals for the next 24 months
Presenter
Presentation Notes
The 2012 Consensus Guidelines state if a histological diagnosis of HSIL (CIN 2) is specified and the colposcopy is adequate (full visualization of the cervix and the SCJ), observation (colposcopy and cytology at 6 month intervals for 12 months) is preferred but treatment is acceptable. If the colposcopy is inadequate or there is CIN 2, CIN 3, CIN 2,3 or ungraded CIN on endocervical sampling, treatment is recommended. This patient should undergo a diagnostic excisional procedure because she has HSIL (CIN 2-specified) and the SCJ is not fully visualized. She tolerates the procedure well and continues with follow-up according to ASCCP guidelines for treated HSIL (CIN 2) in women aged 21-24 years. Ablation is not recommended if the SCJ is not fully visualized.

Pathology Results
What’s the follow up for CIN 2?Answer• Colposcopy and
cytology in 6 months.
• Cytology in 3 years.
• Cervical cotesting in 3 years.
• Cervical cotesting in 12 months.
Cervix, loop electrosurgical excision procedure (LEEP):• Transformation
zone with HSIL (CIN 2)
• Ectocervical surgical margin negative
• Endocervical margin negative
Presenter
Presentation Notes
For women in this age group, the 2012 Consensus Guidelines recommend follow-up according to ASCCP guidelines for treated CIN 2, CIN 3 or CIN 2,3 in this case, the surgical margins were clear. Cotesting is recommended at 12 and 24 months after a diagnostic excisional procedure. If both are negative, repeat cotesting can be performed in 3 years. Should any test be abnormal during the surveillance period, colposcopy with endocervical sampling should be pursued.

Case 2

32 year old woman has her first co-test which returns as cytology negative & HPV positive.
• She asks about her chances of testing HPV negative at her next visit and you respond
• About 25%• About 50%• About 75%• About 100%
Presenter
Presentation Notes
Studies have demonstrated that about 50% of HPV infections will clear within a year, including high risk type HPV 16. Since persistent infection is what is necessary for the development of cervical cancer, shortened intervals of surveillance are necessary in the woman who is HPV positive.
Follow Up pap in one year shows
• Persistent HPV infection with normal cytology
• Next Steps? • Colposcopy
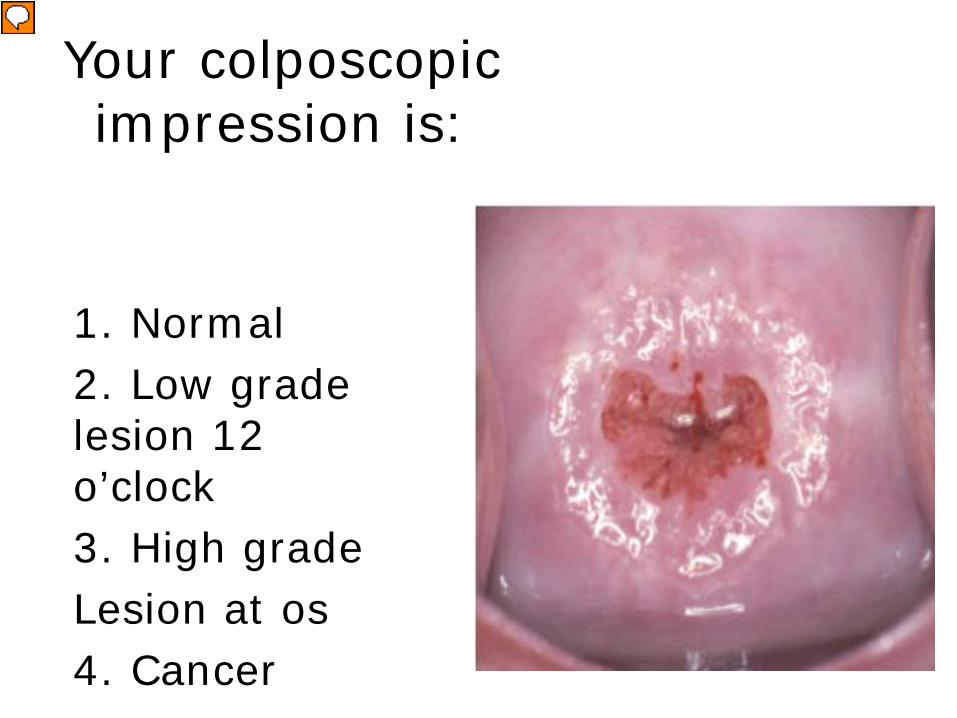
Your colposcopic impression is:
1. Normal 2. Low grade lesion 12 o’clock3. High gradeLesion at os 4. Cancer
Presenter
Presentation Notes
There are no lesions seen. Gland openings are noted in the transformation zone just outside the SCJ.

She is concerned and wants more information about possible outcomes.
You tell her:• 1. If cytology negative
/HPV positive next year, she will need LEEP
• 2. If cytology negative /HPV positive next year, you will repeat colposcopy
• 3. If cytology ASC-US /HPV negative next year, she may return to routine screening in 5 years
• 4. If cytology negative /HPV negative next year, she may return to routine screening in 5 years
Presenter
Presentation Notes
Treatment with excision (LEEP) or ablation (cryotherapy) is reserved for women with a diagnosis of CIN 2+, which has not been found in this patient. If the cytology is abnormal, even with a negative HPV test, colposcopy is recommended. Because she has had a high risk HPV type, lengthening the interval to 5 years at this point is not recommended. The correct answer is to repeat colposcopy with a persistent positive HPV test.

Case 3

A 58 year-old G0 postmenopausal woman comes to your office for follow-up. She had a first co-test two years ago showing negative cytology, but HR-HPV positive.
She was referred for colposcopy and had 2 cervical biopsies and ECC were all negative for dysplasia. Co-testing was be repeated in 12 months.
Due to her move, it was 18 months before she was seen by her new PCP, who performed cytology only.
The result returned as Atypical Squamous Cells, Cannot Exclude High-Grade Intraepithelial Lesion (ASC-H).
What is the appropriate next step?
Presenter
Presentation Notes
Colposcopy
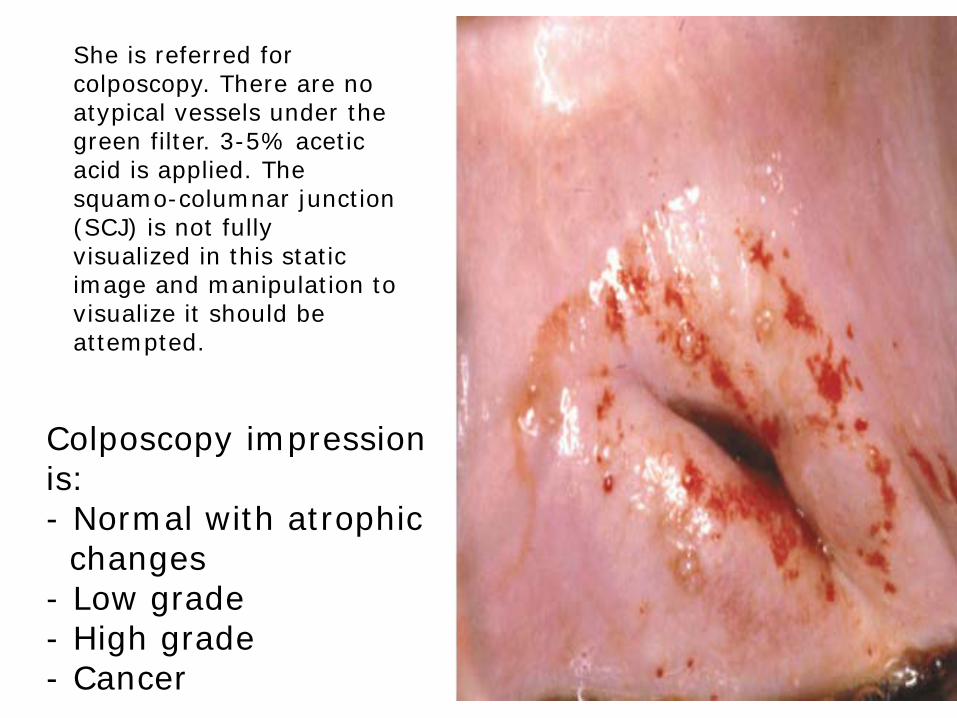
Colposcopy impression is: - Normal with atrophicchanges
- Low grade- High grade- Cancer
She is referred for colposcopy. There are no atypical vessels under the green filter. 3-5% acetic acid is applied. The squamo-columnar junction (SCJ) is not fully visualized in this static image and manipulation to visualize it should be attempted.

Biopsies are performed at 6:00 and 12:00 and an ECC is done. Biopsies
and ECC return as negative for dysplasia, with atrophic changes.
Which one of the following options is
recommended?
• Cotesting at 6 month intervals for 2 years
• Cotesting at 12and 24 months and if negative, cotesting in 3 years
• Diagnostic excisional procedure
• Hysterectomy
Presenter
Presentation Notes
Although a diagnostic excisional procedure can be offered, she could also be followed with cotesting at 12 and 24 months since the SCJ was visible with manipulation and ECC is negative. If there is any cytologic abnormality except HSIL or HPV positivity in subsequent follow up, she will require colposcopy again. If HSIL is present, a diagnostic excisional procedure is recommended. Hysterectomy is not recommended.

Case 4

A 54 yo G0P0 presents to your office to establish care because of an insurance change. She received care from her former gynecologist for the past 15 years. She received annual cervical cancer screening showing no history of cervical abnormalities or gynecologic procedures. She has never had an HPV test. Today, she expects her “annual exam” including a PAP test.

Pap test results: AGUSWhat are the next steps?
•Interpretation: Atypical glandular cells, not otherwise specified (AGC-NOS).Adequacy: Satisfactory for evaluation. Transformation zone present.HPV testing: Negative for high-risk HPV.
Presenter
Presentation Notes
These abnormal cells are found in a small number of Pap smears and may be a sign of more serious lesions or cancer

AGCUS
• Colposcopy • Endocervical
Curettage• Endometrial
biopsy
Presenter
Presentation Notes
Less than 1 % of all pap semar results An represent a wide range of pathology

Aggregate Result of AGUS colposcopy
• 8% of patients have: low-grade squamous intraepithelial lesions (LSIL).
• 11% of patients have: high-grade squamous intraepithelial lesions (HSIL).
• 3% of patients have: adenocarcinoma in situ..
• 1% of patients have endometrial hyperplasia.
• 5% of patients have cancer. • 72% of patients have no problem
Presenter
Presentation Notes
This has a very good chance of resolving without treatment. This is a precancerous spot that has a moderate to high chance of becoming cervical cancer. This is a precancerous spot that has a high chance of becoming cervical cancer This is a precancerous spot that has a low to moderate chance of becoming uterine cancer.

End of Cases

Cervical Cancer • Mostly no
symptoms• Bladder obstruction • Pelvic or back pain • Management
– Stage: size, depth of invasion, distant mets and Lymph node involvement
– Comorbidities– Risk factors for
recurrence • Prognosis
– IA : 93% at 5 years– IVB: 15% at 5
years
Presenter
Presentation Notes
May be some bleeding - post coital or UAB On exam : ulceration or exophytic lesion Management – often minimally invasive

Current Disease burden
•Approximately 12,000 new cases in 2017
•Approximately 4,200 deaths
Presenter
Presentation Notes
This disease is especially tough because it strikes young women and men often at child bearing age.

When to Stop Screening
Three consecutive
negative paps
Two consecutive
negative HPV tests
(Tests within 10 years of stopping; most recent within 5 years.)
OR
Presenter
Presentation Notes
Screening should not resume for any reason, even if she reports having a new sexual partner Why? CIN2 + is rare after 65 – most screens at this age are false positive HPV risk stays about 5-10% Colposcopy is more difficult so harms are magnified Indolent nature of HPV makes cancer much less likely

When to Stop Screening
After total hysterectomy
&No history of
CIN2+
Presenter
Presentation Notes
Screening should not resume for any reason, even if she reports having a new sexual partner Why? CIN2 + is rare after 65 – most screens at this age are false positive HPV risk stays about 5-10% Colposcopy is more difficult so harms are magnified Indolent nature of HPV makes cancer much less likely

When NOT to stop Screening
Who:
•History of CIN 2 or greater disease
For How Long?
• A) Until death• B) 10 years• C) 3 normal pap smears• D) 20 years
Presenter
Presentation Notes
Anyone here a member of the ASCCP

Screening After Vaccination : Looking to the Future…
• May lead to later screening and less frequent intervals of screening… but not there yet– Vaccinating until age 26– Vaccination rates still quite low in the
U.S. (32% vaccination rate in 2010 had received all three dosages)

Where the research is headed…
• Ways to increase vaccination rates• Moving towards HPV testing only• Determining duration of protection
from vaccination • Refining management of cytology
negative/HPV positive women
Presenter
Presentation Notes
HPV testing is more sensitive for detection of CIN2+ and CIN3+ than cytology alone and is almost as sensitive as cotesting (2Y5% additional CIN3+ are detected among women with HPV-negative, cytologypositive results,

Take home points • Our HPV vaccination rates are low –
thousands of cancers could be prevented if we improve
• The greatest risk factor for cervical cancer is lack of or insufficient screening
• HPV screening for those 30 and older• The algorithms are complex and
evolving – use ASSCP guidelines to direct screening and management

GET THE APP


Questions?