
How to Succeed in Alternative Payment Models -...
64
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution How to Succeed in Alternative Payment Models Shannon Calhoun Regional Vice President, Caravan Health
-
Upload
truongthuy -
Category
Documents
-
view
221 -
download
2
Transcript of How to Succeed in Alternative Payment Models -...
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution
How to Succeed in Alternative Payment Models
Shannon Calhoun
Regional Vice President, Caravan Health

Caravan Health
23 MSSP ACO’s
• 6,000 Clinicians
• 55 PPS Hospitals
• 92 Critical Access Hospitals
• 168 Rural Health Clinics
• 39 FQHC’s
• 500,000 Medicare lives
• 32 states
1 Practice Transformation Network
• 11,000 Clinicians
• 800 Independent Practices
2

Caravan Health Services and Programs
• Establish Care Coordination programs
• Establish Wellness and Prevention programs
• Population Health Management software and analysis
• Evidence-based medicine programs
• 24/7 Access program
• Patient Satisfaction program
• Clinically integrated networks
• Advocacy
• Legal and financial services
3
Overview and Learning Objectives
• Learn about MACRA and Alternative Payment Models
• Understand the implications for your organization
• Consider what changes you will need to make to be successful
• Hear about opportunities to engage in alternative payment models
• Learn about tools and resources funded by Medicare and available to you now!
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 4

MACRA: Engage Now for the Future of
Health Care
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution
The Big Picture-Results Matter
6
CMS uses cost and quality data to show results inPrograms.
• It matters that every beneficiary/patient has access to quality care.
• It matters that cost is controlled.
• It matters what your claims and quality submissions say about your practice.
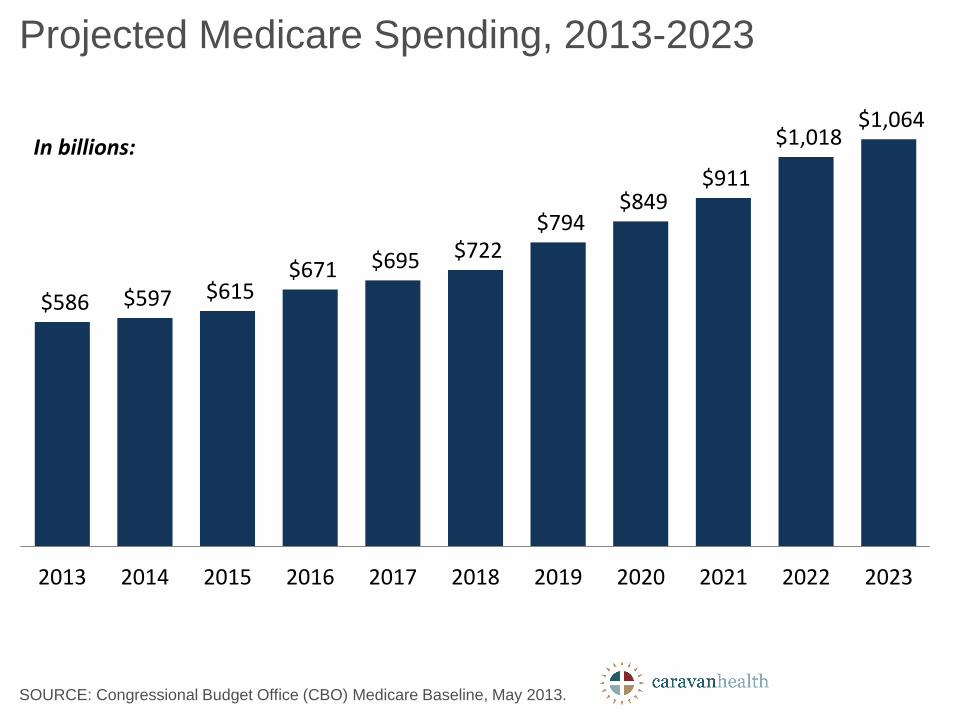
$586 $597 $615 $671 $695 $722
$794 $849
$911
$1,018 $1,064
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023
SOURCE: Congressional Budget Office (CBO) Medicare Baseline, May 2013.
Projected Medicare Spending, 2013-2023
In billions:
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
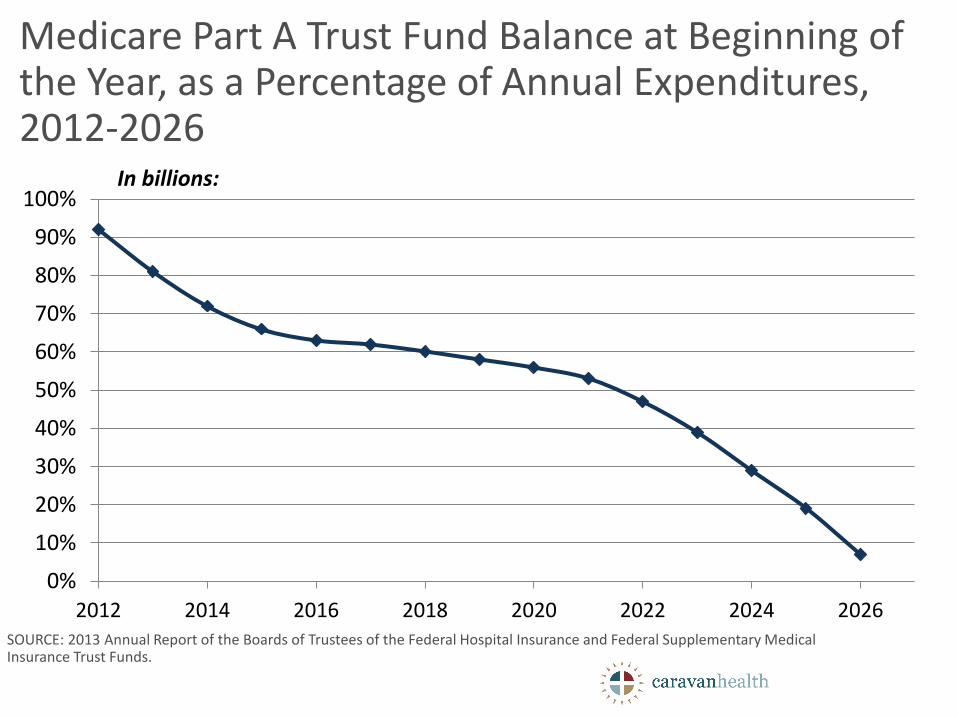
2012 2014 2016 2018 2020 2022 2024 2026SOURCE: 2013 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds.
Medicare Part A Trust Fund Balance at Beginning of the Year, as a Percentage of Annual Expenditures, 2012-2026
In billions:


Why Quality Matters: Disparities in Quality of Care Between Rural and Urban
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 10
2 2 1
13 14
25 15 16
42
17 11 9
0%
20%
40%
60%
80%
100%
Patient Safety(n=19)
Person-Centered Care
(n=16)
EffectiveTreatment
(n=44)
Healthy Living(n=27)
Access (n=25)
Better Same Worse

Disparities in Life Expectancy Between Rural and Urban are Wide and Growing
50,000,000 Rural Americans x 2.4 years lost = 120 million years lost by today’s rural residents.
11
Rural vs. Urban Death Rate per 100,000

Quality Payment Program:
Merit Based Incentive Payment System
andAlternative Payment
Models
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 12

Alphabet Soup: A Guide
www.CaravanHealth.com | Proprietary &
Confidential, Not for Distribution
1
3
• PFS: Physician Fee Schedule. Medicare payment program for clinician rates effective through CY2018.
• MACRA: Medicare Access and CHIP Reauthorization Act. Legislation passed in 2015 replacing the PFS with the QPP.
• QPP: Quality Payment Program. New Medicare payment program for clinician rates effective beginning CY2019.
• MIPS: Merit-based Incentive Payment System. One of two QPP tracks.
• A-APM: Advanced Alternative Payment Model. One of two QPP tracks.
The Speed of Change is Increasing
Secretary Burwell’s historic announcement:
“Our first goal is for 30% of all Medicare provider payments to be in alternative payment models that are tied to how well providers care for their patients, instead of how much care they provide – and to do it by 2016. Our goal would then be to get to 50% by 2018.
Our second goal is for virtually all Medicare fee-for-service payments to be tied to quality and value; at least 85% in 2016 and 90% in 2018.”
Only 36 percent of the 1,201,363 professionals who were eligible to participate in 2012 participated in PQRS, so how is that going to happen?
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 14

Payment Roadmap
Quality Payment ProgramProviders Choose Between Two Tracks
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 16
Merit Based Incentive
Payment System (MIPS)
Advanced Alternative
Payment Models (Advanced APM)
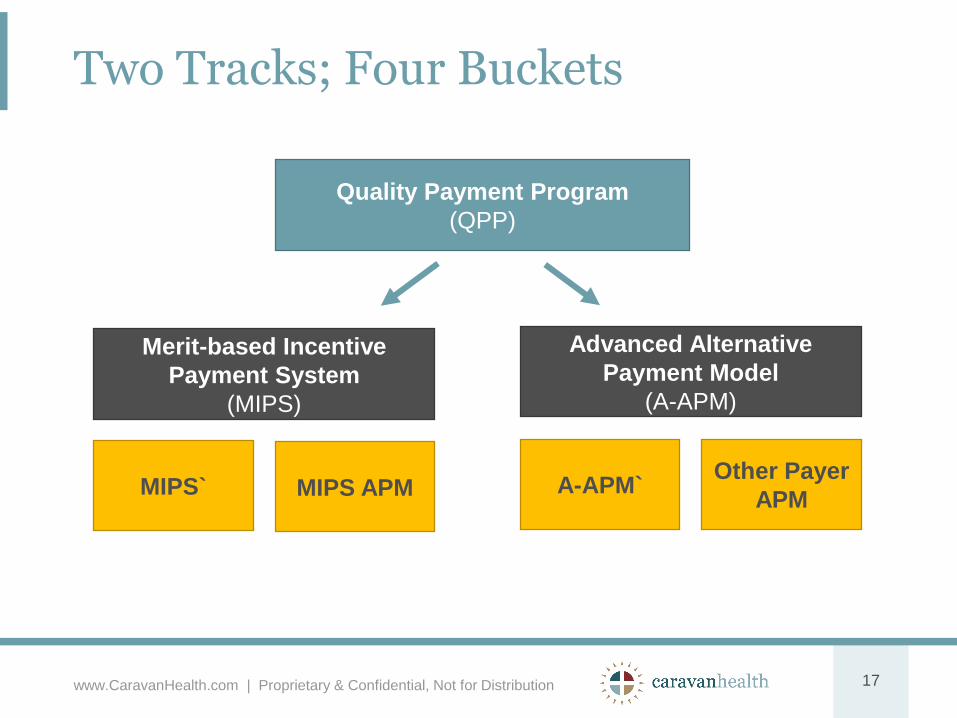
Two Tracks; Four Buckets
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 17
Quality Payment Program
(QPP)
Merit-based Incentive
Payment System
(MIPS)
Advanced Alternative
Payment Model
(A-APM)
Other Payer
APMA-APM`MIPS APMMIPS`

Who Is Included in the QPP?
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 18
Physician
Physician Assistant
Nurse Practitioner
Clinical Nurse Specialist
Certified Registered Nurse Anesthetist
Physical Therapist
Occupational Therapist
Clinical Social Workers
Speech-Language Pathologist
Others…To be considered2019+

Providers in first year of Medicare Part B participation
Providers below the low patient volume threshold
o Medicare charges less than $30k OR
o Fewer than 100 Medicare beneficiaries annually
Providers that bill through a Rural Health Clinic (RHC) or Federally Qualified Health Center (FQHC)
All eligible clinicians may voluntarily report
Who Is NOT in the QPP?
www.CaravanHealth.com | Proprietary &
Confidential, Not for Distribution
1
9
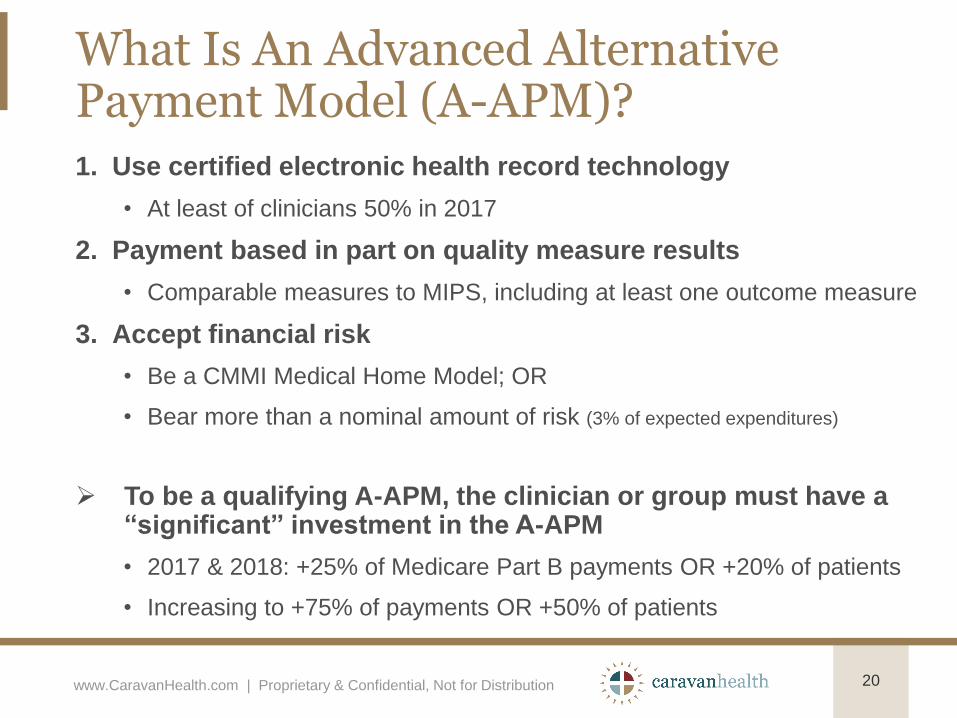
What Is An Advanced Alternative Payment Model (A-APM)?
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 20
1. Use certified electronic health record technology
• At least of clinicians 50% in 2017
2. Payment based in part on quality measure results
• Comparable measures to MIPS, including at least one outcome measure
3. Accept financial risk
• Be a CMMI Medical Home Model; OR
• Bear more than a nominal amount of risk (3% of expected expenditures)
To be a qualifying A-APM, the clinician or group must have a “significant” investment in the A-APM
• 2017 & 2018: +25% of Medicare Part B payments OR +20% of patients
• Increasing to +75% of payments OR +50% of patients
What It Means To Be A Qualifying A-APM
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 21
Exempt from MIPS (can opt in)
Receive a 5% lump sum incentive payment CY2019-2024
Beginning in CY2026, will receive higher annual updates on fee schedule rates

MIPS APMs
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 22
Shared Savings Program Track 1 Participants are considered “MIPS APMs”
Subject to MIPS performance categories and payment adjustment
Alternative scoring of performance categories
• No cost measure
Streamlined data submission
• ACO quality data automatically rolls over (no separate submission needed)
• Automatically receive credit for Improvement Activities that are part of the MSSP (full credit in 2017)
• ACO Participation Improves all MIPS performance
• All providers billing under ACO TIN’s will get the ACO quality score unless they choose to report both.
• All Participants must submit data individually for Practice Improvement and Advancing Healthcare Information.

Performance Year 2017 Data Submission
Test the Quality Payment Program. Submit a minimum amount of data to avoid a downward payment adjustment (one quality measure, one improvement activity, OR advancing care information)
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 23
Participate for the full calendar year. Report all of the required MIPS data
for the full year to be eligible for the maximum incentive adjustment
Participate for part of the calendar year. Report all of the required MIPS
data for a 90 day period to earn a neutral to small positive payment
adjustment
Do not participate. Submit no data for 2017; receive a negative 4% payment adjustment in 2019
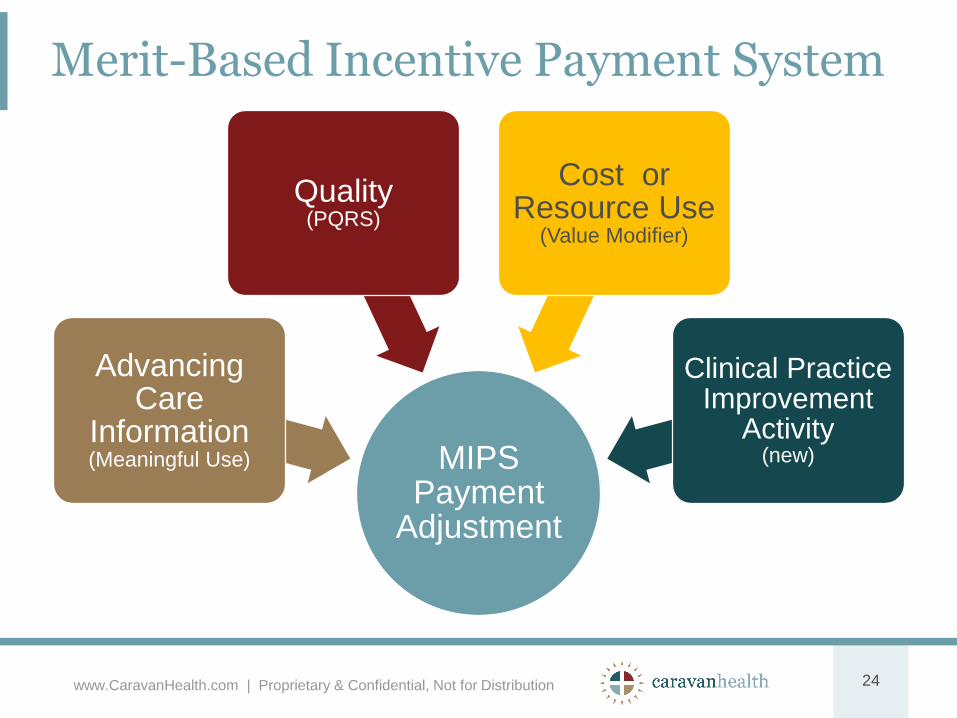
Merit-Based Incentive Payment System
MIPS Payment
Adjustment
Advancing Care
Information (Meaningful Use)
Quality (PQRS)
Cost or Resource Use
(Value Modifier)
Clinical Practice Improvement
Activity(new)
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 24
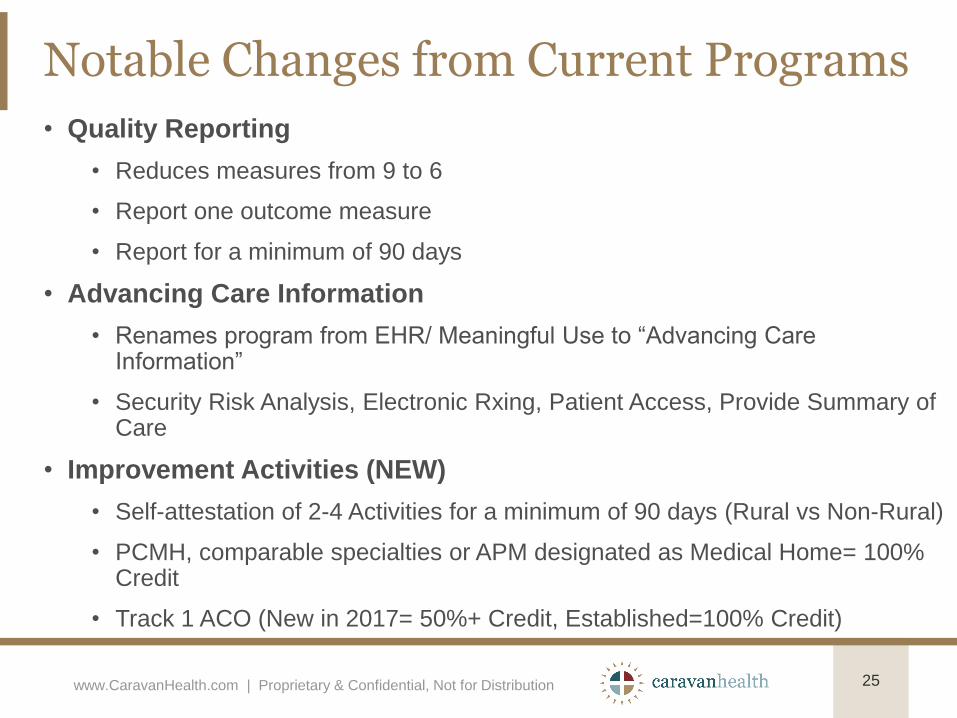
Notable Changes from Current Programs
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 25
• Quality Reporting
• Reduces measures from 9 to 6
• Report one outcome measure
• Report for a minimum of 90 days
• Advancing Care Information
• Renames program from EHR/ Meaningful Use to “Advancing Care Information”
• Security Risk Analysis, Electronic Rxing, Patient Access, Provide Summary of Care
• Improvement Activities (NEW)
• Self-attestation of 2-4 Activities for a minimum of 90 days (Rural vs Non-Rural)
• PCMH, comparable specialties or APM designated as Medical Home= 100% Credit
• Track 1 ACO (New in 2017= 50%+ Credit, Established=100% Credit)
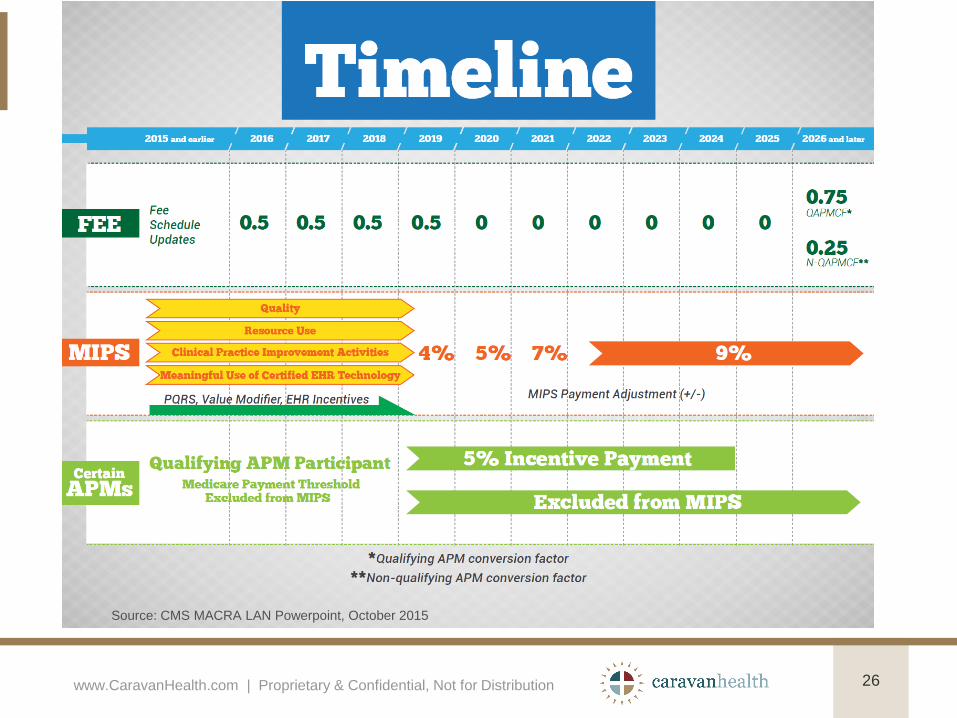
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 26
Source: CMS MACRA LAN Powerpoint, October 2015

Quality Payment Program Timeline
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 27

28
Key Considerations
• Final Rule announced Friday October 14, 2016
• CMS estimates more than 125,000 providers will participate in Advanced APMs and qualify for the 5% incentive payment.
• RHCs and FQHCs are exempt from reporting – can do so on a voluntary basis
• Solo practitioners and most small group practices are not exempt from reporting
• Performance periods start 2017 for payment adjustments in 2019
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution

Advanced APMs or MIPS APMs Which is Right for You?
Requires Risk
Up to 10% loss 5% Max Bonus
Does Not Require Risk
27% Max Bonus
4-9% Max Penalties
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 29
Advanced
APM
MIPS APM

Value-Based Payments• Medicare Incentive Payment System (Starts 2017)
• Up to 9% penalty or 27% bonus by 2022
• $3- $9 PMPM
• Medicare Shared Savings Program (Open)
• Average Payment = $7.34 PMPM
• AIM Funding = ~$7.50 PMPM
• Comprehensive Primary Care Plus (Regional-FFS only)
• Average Payment = $16.50-$32 PMPM
• NextGen ACO Shared Savings Program (Open)
• $8 PMPM
• Million Hearts (closed)
• $10 PMPM for 30% of Medicare patients
• Humana Medicare Advantage Shared Savings Program (New!)
CONFIDENTIAL | 30

MIPS Alternative Payment Models
• MIPS APMs: e.g., Track 1 Medicare Shared Savings Program
• ACO Participation Improves MIPS performance.
• All providers billing under ACO TIN’s will get the ACO quality score, which are generally higher than MACRA scores.
• MIPS APMs are exempt from the Resource Utilization metric.
• You automatically get 100% credit for Clinical Practice Improvement.
• All Participants must submit data individually for Advancing Healthcare Information, but ACO has one score.
• Most ACO Participants will not be penalized and can earn high bonuses if they pay attention to EHR issues.
• Most specialists in an ACO will not have to report quality.
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 31

MSSP Program Elements
• All reimbursement stays the same for all providers
• Quality reporting and care coordination is required
• If savings are realized, payor will share savings with the provider
• Bonus payments are adjusted downward based on quality scores
• All claims data is provided to participants
• Waivers of Stark, Anti-trust, Anti-Kickback and Patient Inducement regulations
• Patients have full choice on where to go for care.
• Cost: $5 PMPM + 10% SS (AIM funding may be available)
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution 32

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Practice Transformation
Network (PTN): Getting
Ready for Value-Based
Payments
The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the
U.S. Department of Health & Human Services, Centers for Medicare & Medicaid Services. Its
contents are solely the responsibility of the authors and do not necessarily represent the official
views of HHS or its agencies.

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
HOW DO WE TRANSITION FROM
VOLUME TO VALUE ?
E & M AWV
Procedures TCM - CCM
20192015
2016
2017
2018

Proprietary & Confidential, Not for Distribution
www.nationalruralaco.com
Common Elements of Success
Prevention: • Annual Wellness Visits
• Chronic Care Management
• Advanced Care Planning
• Behavioral Counseling
• Depression Screening
• Mental Health Support
• 24/7 Access
Coding:
• Complete and accurate
documentation of all chronic
conditions is key to correct
payment under value-based
models.
Quality: • Process
• Pre-visit Planning
• Patient Satisfaction
35

Proprietary & Confidential, Not for Distribution
www.nationalruralaco.com
Current Revenue Opportunities
Fee Schedule: • Annual Wellness Visits
• Chronic Care Management
• Advanced Care Planning
• Behavioral Counseling
• Depression Screening
Value-Based
Payments:• Medicare Incentive Payment
System
• Medicare Shared Savings Program
• NextGen ACO Shared Savings
Program
• Mandatory or Voluntary Bundled
Payments
• Comprehensive Primary Care Plus
• Million Hearts
36

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
What Are We Trying To Improve?• Quality
• Most practices do not have processes in place to promote wellness and
address gaps in care – which are key quality measures.
• We need to establish the processes and workflow to address these
issues.
• Cost
• Reduce unnecessary care
• In value-based payments, payments are multiplied times HCC scores.
• We need to improve our coding to get paid what we are worth.
• Practice Economics
• We need to spend an extra hour with each of our Medicare patients
each year to address prevention, care gaps and appropriate coding.
How do you pay for that?
• We will need to fund the staff to do this work in order to be sustainable.
37

Proprietary & Confidential, Not for Distribution
www.nationalruralaco.com
Two-Thirds of Medicare Spending Is for People With Five or More Chronic Conditions
Percentage of Medicare Expenditures• Ninety-nine percent of
Medicare expenditures are
for beneficiaries with at least
one chronic condition.
• Ninety-eight percent of
Medicare expenditures
involve individuals with
multiple chronic conditions.
Source: Medicare Standard Analytic File, 2007
Proprietary & Confidential, Not for Distribution
www.nationalruralaco.com
Chronic Care Management Reduces Cost• At risk patients with 2+ chronic conditions expecting to last
for the following 12 months or until death of the patient
• Explanation of CCM with written consent
• Incident to Primary Care providers
• General Supervision except RHC, FQHC
• 20 minutes per month
• 24/7 access to care team with access to electronic care
plan
• Shown to reduce cost by 20-60%
• Generates an average of $20,000/year in profit
39
Proprietary & Confidential, Not for Distribution
www.nationalruralaco.com
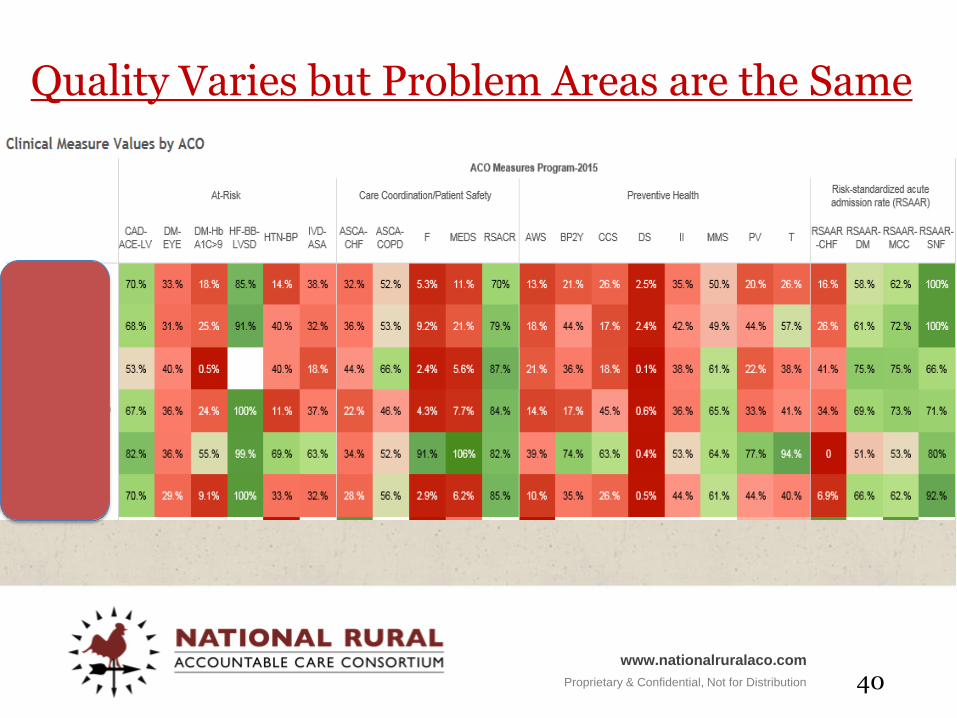
Quality Varies but Problem Areas are the Same
40

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
41
Value of Wellness Visit in Population HealthealthValue of Wellness Visit in
Population HealthGather as much data as possible
on lives
Find patients who are “at risk”
Refer for appropriate follow-
up services
Develop a consistent primary care relationship
Refer patients to Care Coordinator

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Our Version of the Wellness Visit
• Documentation of all drugs to support ongoing Medication Reconciliation.
• Documentation of all co-morbidities to support accurate risk coding.
• Perform PHQ-9 Depression Screen, Mini-COG, Fall Risk.
• Documentation of all interventions to support quality scores.
• Maximize number of patients who get the service.
• Maximize revenue to support staff needed for population health activities.
42
Proprietary & Confidential, Not for Distribution
www.nationalruralaco.com
Wellness Visit Risk Adjustment Impact
• Value-based payments are based on expected cost multiplied by
HCC risk scores. Providers will be penalized for falsely low
scores. For example:
• A hospital who has a joint replacement bundle expected cost of
$20,000 will get paid the following:
• $20,000 for a patient with an HCC score of 1.0
• $18,000 for a patient with an HCC score of 0.9
• $22,000 for a patient with an HCC score of 1.1
• HCC risk scores are calculated from all diagnoses listed on bills
sent to CMS in the prior calendar year – no institutional memory.
• DOCUMENT ALL SIGNIFICANT CHRONIC CONDITIONS ON
THE BILL FOR THIS VISIT. ASK PATIENT ABOUT EACH ONE
AND DOCUMENT IN SOAP NOTE. PRIORITIZE IF NECESSARY.
43

Proprietary & Confidential, Not for Distribution
www.nationalruralaco.com
Mandate to Improve Coding
• Value-based payments are based on allowed charges divided by
HCC risk scores.
• Cost/HCC score = adjusted cost
• E.g., a beneficiary who had $10K in claims last year and an
HCC score of 0.9 = $10,000 x .9 = $9,000 risk-adjusted cost
used for value-based payments.
• HCC risk scores are calculated from all diagnoses listed on bills
sent to CMS in the prior calendar year – no institutional memory.
• Rural typically under-codes because it does not generally affect
our payments.
• This makes our higher costs look even worse.
• Most providers can increase their risk scores by at least 10%.
44

Proprietary & Confidential, Not for Distribution
www.nationalruralaco.com
Mandate to Improve Coding
• Value-based payments are based on allowed charges divided by
HCC risk scores.
• Cost/HCC score = adjusted cost
• E.g., a beneficiary who had $10K in claims last year and an
HCC score of 0.9 = $10,000 x .9 = $9,000 risk-adjusted cost
used for value-based payments.
• HCC risk scores are calculated from all diagnoses listed on bills
sent to CMS in the prior calendar year – no institutional memory.
• Rural typically under-codes because it does not generally affect
our payments.
• This makes our higher costs look even worse.
• Most providers can increase their risk scores by at least 10%.
45

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
AWV as Key to Quality
46
Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
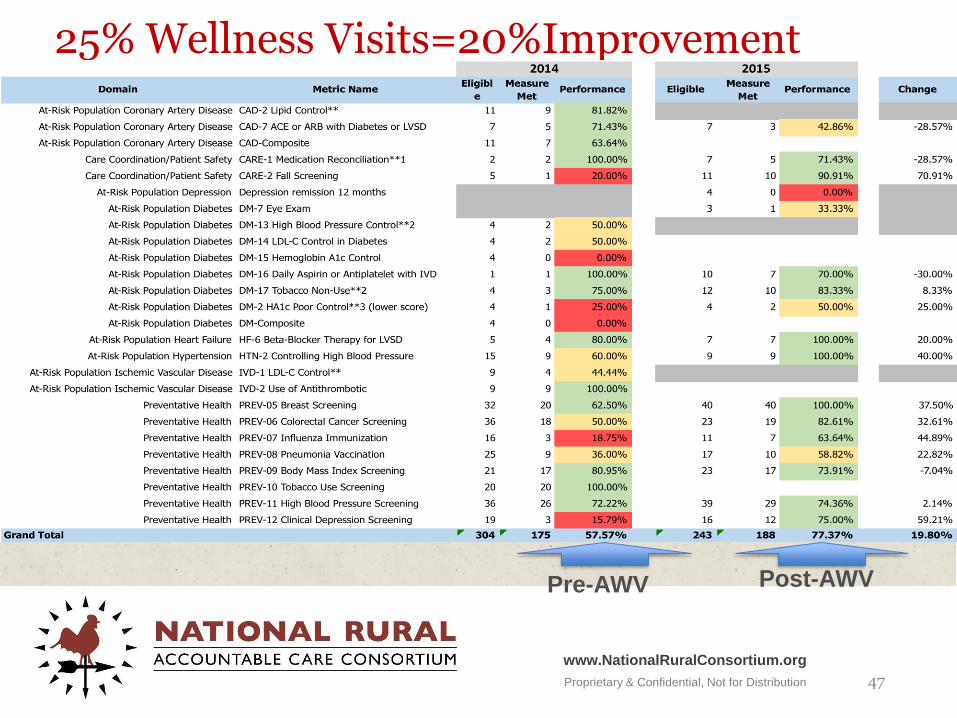
25% Wellness Visits=20%Improvement
47
Pre-AWV Post-AWV

Proprietary & Confidential, Not for Distribution
www.nationalruralaco.com
Wellness Visits Generate Income
48
Fee-for-Service(+$225-$300/visit)
• Wellness Visit
• Depression Screen
• Advanced Care Plan
• Smoking Cessation
• Obesity Counseling
• Substance Abuse Intervention
• Immunizations
• + E&M visit if needed
RHC (?)
• Can only bill All Inclusive Rate (AIR), but can add cost of staff to do work to cost report for reimbursement.
• Cannot bill for more than one visit.
FQHC (~+$60/visit)
• Can bill for the Wellness Visit (but not for the follow up or add-ons) for 1.3416 times FQHC PPS rate (including regular visit).
• Cannot bill for separate visit
What Should You Do Now?• Perform wellness visits on all of your patients.
• Embed a care coordinator in your practice.
• Start working on integrating behavioral health.
• Prepare to be flexible. This takes trial and error.
• Join a non-risk bearing Clinically Integrated Network.
• Keep up with your EHR.
• Code Baby Code! Get your HCC scores right.
• Join/Form an ACO.
• Get value-based payments from other payers.
• Keep up with announcements of new models.
• Get free training, software and support by joining National Rural Accountable Care Consortium Practice Transformation Network.
www.CaravanHealth.com | Proprietary &
Confidential, Not for Distribution
4
9

Join Our PTN:• Set up Care Coordination Services
• Maximize Wellness Visits
• Increase your Medicare revenue by $20 PMPM
• Increase your quality by 20% or more
• Provide 24 hour advice nurses for your patients
• Get help implementing new programs discussed today.
IT’S FREE• Go to www.nationalruralaco.com and click on “Apply Now”
• Or email [email protected]
Learn More

51
Questions?
www.CaravanHealth.com | Proprietary & Confidential, Not for Distribution
Thank You
Shannon Calhoun, Regional Vice President
916-542-4707
www.CaravanHealth.com
916.500.4777
Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
53
Practice Transformation Network
Establish Your Value-Based Infrastructure at No Cost.
Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Step One: Set up your Care Coordination Program
54
• Certify your coordinators with the Clinical Health
Coach (CHC) Training program offered by the Iowa
Chronic Care Consortium.
• A 26 hours on-line and self-paced program.
• Participate in hands-on Regional Workshops held
quarterly.
EDUCATION: Attend Care Coordination Webinar
ACTION: Designate a Care Coordinator

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Step Two: Develop Your Billable Chronic Care Management (CCM) Service
55
• Train and Certify your Care
Coordinators as Clinical Health
Coaches (CHC)
• Implement the necessary IT
infrastructure for access to Care
plans in Lightbeam
• Provide a federally-funded 24/7 nurse
advice hotline
• Bill Medicare $42 PMPM
EDUCATION: Attend Chronic Care Management Webinar
ACTION: Download Consent Form and Support Materials

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Lightbeam Data Support
56
Lightbeam Health Data Software
• for 24/7 access to your patient’s care plan
Action for Success: Designate a person as Super User for
Lightbeam – Webinar training instruction for Care Planning.

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Step Three: NurseWise/Evolve
57
• 24-hour telephonic access to
medical advice for Medicare
patients.
• Necessary for your billable care
coordination program’s after-
hours coverage.
EDUCATION: Attend 24hr Nurse Advice Hotline Webinar
ACTION: Complete Nursewise Survey on PTN website
Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Step 4: Point-of-Service Patient Satisfaction Survey Tool and Tablet
58
• Each practice is eligible to
receive single use tablet for
patients to complete satisfaction
survey & receive feedback.
• Tablets will be deployed within
60 days of enrollment.
EDUCATION: Attend webinar about survey tool and tablet.
ACTION: Complete Survey posted on PTN webpage.
Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Step 5: Preparing to become a Patient-Centered Medical Home (PCMH)
59
ACTION: Complete Practice Baseline Assessment
EDUCATION: Attend webinar about PCMH.
ACTION: Complete Plan-Do-Study-Act activities.
• Assessment is aligned with PCMH goals and
track’s your practice performance.
• Conducted by NRACC Quality Specialist or your
state’s QIO/QIN with your leadership.
• Lays the foundation to apply for certification as a
PCMH. PCMH elements are built into quarterly
training workshops in a Plan, Do, Study, Act
(PDSA) format.
Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Step 6: Practice Workflow Redesign
60
• Your practice will receive easy-to-
implement workflow tools.
• We will work together to create custom
implementation plan – tailored to your
practice’s needs and challenges
• Regional Workshop will be held in
Savannah on October 18th and in Atlanta
on October 21st.
EDUCATION / ACTION:
Schedule staff to attend one Regional Workshop per quarter.
Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
OUTCOMES: Redesign Your Practice to Better Manage Population Health
61
• Modify clinic workflow to address
care gaps
• Provide data to identify cost-savings
opportunities
• Report and improve ambulatory
quality scores
• Measure patient satisfaction at the
point of care (Tablet)
• Get paid quality bonuses

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
OUTCOMES: Improved Billing and New/Increased Revenue Streams
62
• Program activities designed to
reduce cost and improve quality.
• Maximize additional population
health payments
• Prevent value-based payment
penalties
• Improve financial stability of local
health systems.
Action for Success: Actively participate in program activities –
PDSAs, Workflows, Trainings, and Workshops.

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Eligibility
63
• PHYSICIANS, PA’s and NP’s
• Rural PPS Hospitals
• Critical Access Hospitals (CAHs)
• RHCs, FQHCs
• Rural Fee-for-Service Clinics
• Urban rural network providers
• Not already part of any Medicare Shared Savings
program (MSSP, CPCI, etc.)

Proprietary & Confidential, Not for Distribution
www.NationalRuralConsortium.org
Participation Requirements
64
• Participants must appoint or hire an in-house care
coordinator (will bill Medicare for new services)
• Active participation in the program, including attendance at:
• Training webinars
• Regional workshops
• Divisional workshops, and
(Travel for regional & divisional workshops is reimbursed through the grant)










![“It is the worst of our time”: Youth language, language ...salsa.ling.utexas.edu/proceedings/2015/Calhoun.pdf[Tumblr] (2) My life is literally a Lifetime movie right now & I cannot](https://static.fdocuments.in/doc/165x107/5f51ca6018aa995b423870c2/aoeit-is-the-worst-of-our-timea-youth-language-language-salsaling-tumblr.jpg)







