HOW TO RENOVATE YOUR DECISION SUPPORT … · Advanced cost accounting solutions, without being...
8
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19 SEPTEMBER/OCTOBER 2015 COST MANAGEMENT T his is proving to be a water- shed year in the transforma- tion of the U.S. health-care system from volume- to value-based care. The U.S. Department of Health and Human Ser- vices (HHS) has firmly planted a stake in the ground by pledging that 50 per- cent of Medicare payments must move to alternative payment agreements by 2018. 1 Accepting the thrown gauntlet, leading health systems and payers formed the Health Care Transformation Task Force (HCTTF) and pledged that 75 percent of their businesses will move to value-based payments by 2020. 2 With payment reform comes an increas- ing shift of care delivery from higher rev- enue and higher margin acute services to lower revenue and lower margin out- patient care, with a focus on a good patient experience tied to good clinical outcomes. Health systems will need to adopt a tech- nology-enabled delivery model across the continuum of care, including pre- operative, intra-operative, and post-oper- ative services, to manage cost and achieve the best financial and clinical outcomes across cases and episodes of care and attributed populations. Following are seven key elements to consider when renovating your decision support system to support health-care reform and our method for an effective action plan. Seven key elements Today’s health-care CFO is focused on developing and managing innovative reimbursement models and identifying new business models to generate new revenue growth amidst shrinking rev- enues from traditional revenue and reim- bursement models. Today’s CFO needs a new generation of decision support HOW TO RENOVATE YOUR DECISION SUPPORT SYSTEM FOR THE HEALTH CARE REFORM ERA PRASHANTH KINI AND WILLIAM BERCIK PRASHANTH KINI is senior director of health-care product strategy at Oracle with over 20 years of strategic technology and business leadership experience across multiple verticals. He was previously senior scientist at Procter & Gamble. Prashanth earned a Ph.D. in electrical and computer engineering from the University of Cincinnati with a focus in medical imaging. WILLIAM BERCIK is director of health care at Oracle. With over 25 years of experience in the health-care industry, he has specialized in enterprise applications and technology solutions since 1992. He provides specialist product expertise and devel- ops and executes solutions for the health-care market. Formerly, William was the CFO of a 350-bed acute care hospital. This article examines some key elements to consider when renovating your decision support system to facilitate health-care reform and presents a method for crafting an effective action plan.
Transcript of HOW TO RENOVATE YOUR DECISION SUPPORT … · Advanced cost accounting solutions, without being...

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19SEPTEMBER/OCTOBER 2015 COST MANAGEMENT
T his is proving to be a water-shed year in the transforma-t ion of the U.S. health-caresys tem f rom volume- tova lue-based care . The U.S .
Department of Health and Human Ser-vices (HHS) has firmly planted a stakein the ground by pledging that 50 per-cent of Medicare payments must move toa lternat ive payment agreements by2018. 1 Accept ing the thrown gauntlet ,leading hea lth sys tems and payersformed the Health Care TransformationTask Force (HCTTF) and pledged that 75percent of their businesses will move tovalue-based payments by 2020.2
With payment reform comes an increas-ing shift of care delivery from higher rev-enue and higher margin acute servicesto lower revenue and lower margin out-patient care, with a focus on a good patientexperience tied to good clinical outcomes.Health systems will need to adopt a tech-
nology-enabled deliver y model acrossthe cont inuum of care, including pre-operative, intra-operative, and post-oper-ative services, to manage cost and achievethe best financial and clinical outcomesacross cases and episodes of care andattributed populations.Following are seven key elements to
consider when renovating your decisionsupport system to support health-carereform and our method for an effect iveact ion plan.
Seven key elementsToday’s health-care CFO is focused ondeveloping and manag ing innovat ivereimbursement models and identify ingnew business models to generate newrevenue grow th amidst shrinking rev-enues from traditional revenue and reim-bursement models. Today’s CFO needsa new generat ion of decis ion suppor t
HOW TO RENOVATE YOUR DECISION SUPPORT SYSTEM
FOR THE HEALTH CARE REFORM ERA
PRASHANTH K IN I AND WILL IAM BERC IK
P R A S H A N T H K I N I is senior director of health-care product strategy at Oracle with over 20 years of strateg ic technologyand business leadership experience across multiple verticals. He was previously senior scientist at Procter & Gamble. Prashanthearned a Ph.D. in electr ical and computer engineering from the University of Cincinnati with a focus in medical imaging.
W I L L I A M B E RC I K is director of health care at Oracle. With over 25 years of experience in the health-care industry, he hasspecialized in enterprise applications and technology solutions since 1992. He provides specialist product expertise and devel-ops and executes solutions for the health-care market. Formerly, William was the CFO of a 350-bed acute care hospital.
This ar ticle examines some key elements to cons ider when renovating your decis ion suppor t system
to facilitate health-care reform and presents a method for crafting an ef fective action plan.
bstoehr
Typewritten Text
Cost Management, Volume 29, Number 5. Copyright 2015. Thomson Reuters/Tax & Accounting. Reprinted with permission.

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
tools, working in concert with the clin-ical and operational systems, to providepoint-of-decision insights to deliver themost clinically cost-effective care paths.The hard quest ions the CFO must
answer require insights across the continuumof care, bringing together clinical, oper-ational, and financial perspectives to drivecare-delivery decisions.The CFO, thinking also as the CMO,
COO, and CEO, must answer “hard” ques-t ions such as:• What are your biggest cost manage-ment strategies?• What data insights and analy t ics areyou using to drive down cost of careacross your system?• How are you using cost-of-careinsights in your populat ion healthstrategies?• What cost and revenue managementcapabilit ies do you need for shared-risk contract negotiat ions?• What methods are you employ ing toinfluence cost management beyondinpatient/acute care serv ices (i.e.,l inking costs across episode of care,ambulatory care sites, and contin-uum of care)?• How are you using workforce ana-ly t ics to respond to flex volumedemands?Once these ques t ions have been
answered, seven key elements of a deci-
sion support system must also be con-sidered. These elements include:1. shared cost and quality accountabil-ity ;
2. closed-loop strategic decision sup-port;
3. cost accounting al locat ion methods;4. value-based, labor productiv itycapabilit ies;
5. budgeting and flex variance analy-sis;
6. financial modeling and what-ifanalysis; and
7. cost insights in populat ion healthmanagement.Let’s examine each of these elements
in more detai l .
Shared cost and quality accountabilityAn effective cost management and value-based care delivery strategy requires coor-dinated buy-in and engagement f romstakeholders across the enterprise. This strat-egy should be driven by specific, action-able insights derived from a single sourceof truth: an enterprise-wide data repos-itory across the various functions. Rele-vant performance indicators and forecastedtrends must be delivered at the right time,in each manager’s specific decision-mak-ing workflow. Key performance indica-tors (KPIs) must be accompanied by thenecessary “drill-down” transparency and
20 COST MANAGEMENT SEPTEMBER/OCTOBER 2015 DECISION SUPPORT SYSTEMS
EXHIBIT 1 Stakeholder Value and Shared Accountability
bstoehr
Typewritten Text
Cost Management, Volume 29, Number 5. Copyright 2015. Thomson Reuters/Tax & Accounting. Reprinted with permission.

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
traceability to engender credibility and stake-holder buy-in.Exhibit 1 outlines a segmentat ion of
key stakeholders and influencers and therelevant insights necessary within eachrealm of the care delivery process.
Closed-loop strategic decision supportHealth systems, transforming to meet thedemands of value-based accountable carereimbursement models, must employ apor t fol io of next-generat ion strateg icdecision support tools that enable theirworkers to continuously, accurately, andtransparently engage stakeholders in thecommon mission to profitably evolve caredelivery models. Next-generation toolswill allow health systems to pragmaticallyand progressively adopt methodologiesthat effectively represent value-based con-structs, like total cost of care across acuteand ambulatory episodes of care, bun-dled service definitions, and populationhealth performance measures, while lever-aging today’s practices.“Traditional” decision support func-
tions of cost accounting, budgeting, plan-ning, forecasting, and workforce analyticsmust now be delivered as a single, inte-grated suite. This is necessary in order toharmonize data from clinical and opera-tional systems and provide multiple, seam-
less, real-time lenses on the health system’sshort- and long-term performance againstthe dr iv ing per formance measures ofvalue-based care. Stakeholders shouldalso be equipped with short- and long-termpredic t ive model ing ins ights into theimpact of changing pat ient volume oncosts and profitability. Such insights willsupport decisions on service-line growthand potential financial risk of multiple,simultaneously modeled contractual agree-ments across various payers.
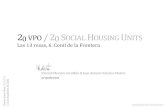
Cost accounting allocation methodsAdvanced cost account ing solut ions ,w ithout being prescr ipt ive or restr ic-t ive, give inst itut ions the capability todeploy and simultaneously compare avariety of costing methods ranging fromfundamental methods such as rat io ofcost to charge (RCC) through inst itu-t ion-specific or standard relat ive valueunits (RVUs) (see Exhibit 2). Inst itu-t ions can use mult iple methods to al lo-cate depar tmenta l cos t pool s to thecharge-master items (a chargeable pro-cedure) as an accurate proxy of act iv ityand service consumption.Often, the charge master is extended
to include non-chargeable act iv it ies tokeep the integrity of the same cost ingmethodology.
21DECISION SUPPORT SYSTEMS SEPTEMBER/OCTOBER 2015 COST MANAGEMENT
EXHIBIT 2 Advanced Cost Accounting Capabilities
bstoehr
Typewritten Text
Cost Management, Volume 29, Number 5. Copyright 2015. Thomson Reuters/Tax & Accounting. Reprinted with permission.

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Advanced decision support systems willprovide a rich set of pre-built and ad hocreporting capabilit ies to examine costsand revenues across clinical and operationaldimensions. Stakeholders would be ableto examine cost and profitability by ser-vice line, diagnosis-related group code(DRG), and costs from the physician leveldown to the patient level. They would alsobe able to quickly look at variability acrosseach dimension. Plotting profitability ona “whale” curve chart quickly enables theexamination of top- and bottom-tier per-formers in each category.Cost reports must provide traceability
to address any skepticism about accuracyof the numbers (this is crit ical) and togain stakeholder buy-in. Such traceabil-ity maps will provide drill-down visibil-ity into the step-down allocation and costdrivers used in cost allocation at the mostgranular level . Advanced t raceabi l i t yreports will also provide automatic visi-bility into unallocated costs and generalledger reconciliation. Traceability maps pro-vide transparency into revenue and costallocations. From any point in the modelyou can trace backward or forward, eas-ily visualizing the defined allocation flowfor validation and knowledge transfer.
Value-based, labor productivitycapabilitiesWith labor costs accounting for 60 per-cent or more of a hospital’s budget andwith hospitals already having reduced theworkforce down to the point of endan-ger ing quality, hospital f inance execu-
tives are now focused on managing laborcosts through other init iat ives. 3 Theseinclude effective application of the rightacuitybased staffing and scheduling toeliminate unnecessary payroll “leakage”from lost product iv ity and potent ial lyunnecessar y over t ime pay from subop-t imal sh i f t t rans i t ions and handof fs .Such labor product iv ity di l igence mustbe par t of an integrated decision sup-por t strategy informed by establishedoverr iding performance targets, as wel las cost and outcome r isk managementinsights. Nursing managers have l itt leor no insight into timekeeping data untilit appears in payrol l , and by then it istoo late to affect any staff a l locat ion orover t ime decisions.Kerri-Lynn Primmer Morris, executive
director of finance operations and strate-gic projects at the Oakland-based KaiserPermanente , emphas i ze s Ka i s e r ’sapproach to “give managers insight tomake decisions in the moment by imple-menting a new timekeeping ecosystem thatprovides real t ime, act ionable analy t icsand aler ts with consumer grade experi-ence with dashboards on mobile devices.”Value-based capabilities, such as those
shown in Exhibit 3, would provide someof the much-needed support for managersto make better decisions.
Budgeting and flex variance analysisFor most health-care organizations, bud-get ing and strategic planning are dis-connected, making it impossible to reportac tua l results against the budget and
22 COST MANAGEMENT SEPTEMBER/OCTOBER 2015 DECISION SUPPORT SYSTEMS
EXHIBIT 3 Labor Productivity Measurement Drives Staffing Optimization
bstoehr
Typewritten Text
Cost Management, Volume 29, Number 5. Copyright 2015. Thomson Reuters/Tax & Accounting). Reprinted with permission.

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23DECISION SUPPORT SYSTEMS SEPTEMBER/OCTOBER 2015 COST MANAGEMENT
EXHIBIT 4 Integrated Budgeting, Planning, and Forecasting Capabilities
strategic plan. Connecting disparate datain unconnected systems takes t ime andeffort, but this alone does not provide reli-able information for decision-making.Instead of isolating each functional area,it is important to connect them and lever-age the informat ion f rom a commonrepository.There are three key components of an
ef fec t ive f inancia l per formance solu-t ion:1. strategic planning;2. serv ice-line budgeting; and3. operat ional/capital budgeting.The goal is to develop a long-range
strateg ic plan; to create a ser v ice-l inebudget that prov ides bus iness de ta i land depicts volumes and revenues accu-rately whi le automat ica l ly generat ingoper at iona l budge t t a rge t s . How dorolling forecasts fit in? It is increasinglyimportant to align rolling forecasts withmult iyear plans and detai led budgets .Af ter c reat ing the operat ing budget ,analysis and report ing (e.g., actual ver-sus budget) cont inue on a go-forwardbasis . The net result is a real-t ime v iewof your strategic plan, market investments,variances, and actual performance downto the service-line level to promote mul-
t id i rec t iona l repor t ing and to re f ineyour project ions. Exhibit 4 l is ts someof t he v a lue -ba sed c apab i l i t i e s t hatwould make this long-range st rateg icplan a real it y.
Financial modeling and what-if analysisEquipped w ith high-qual it y, granular,h i s tor ica l data across the enterpr i sefunc t ions , hea l th-care organizat ionscan progress to the most advanced levelof analy t ics matur it y w ith predic t ivemodeling. Organizat ions need to assessfinancial models that reflect the impactof value-based payment arrangements,s ide by s ide w ith current f inancial pro-j e c t i ons b a s ed on vo lume . Wi t hadvanced planning and forecasting tools,f inance depar tments can examine mul-tiple financial scenarios simultaneously.Parameters such as var ious reimburse-ment rates by payer, average length ofstay (ALOS), and volume of admissionscan be adjusted to examine net revenueimpact .Advanced model ing tools enable
providers to organize services used acrossmultiple patient encounters into episodesof care or bundled service definit ions,
bstoehr
Typewritten Text
Cost Management, Volume 29, Number 5. Copyright 2015. Thomson Reuters/Tax & Accounting. Reprinted with permission.

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
and they also enable those providers to exam-ine care path and corresponding cost vari-ations. Such modeled service bundles canbe informative for contract negotiationsand can be exported into contract man-agement systems as a grouping of nego-tiated contractual service definitions.
Use cost insights in population healthmanagementThe abilities for health systems to createhierarchies of patient populations basedon clinical and financial risk will be piv-otal to their abi l it ies to manage thesepat ients under value-based payments.Managing them is, of course, hinging onthe savings and outcomes achieved acrosscohort (like cases) populations. The Cer-
tification Commission for Health Infor-mation Technology’s (CCHIT) 2013 frame-work for accountable care IT (see Exhibit5) outlines and describes the key functionsan IT infrastructure must deliver to sup-port the triple aim of accountable care:improving population health and deliver-ing the best patient experience, all at anaffordable level.4 A review of the detailedprocesses outlined in the framework revealsample and ubiquitous opportunities topropagate cost insights throughout vari-ous points of decision across the caredelivery path.
Action planHealth-care organizat ions can pursue apragmatic and progressive approach to
24 COST MANAGEMENT SEPTEMBER/OCTOBER 2015 DECISION SUPPORT SYSTEMS
EXHIBIT 5 CCHIT 2013 Framework Processes
bstoehr
Typewritten Text
Cost Management, Volume 29, Number 5. Copyright 2015. Thomson Reuters/Tax & Accounting. Reprinted with permission.

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
building out their portfolios of decisionsupport solut ions, but they first need tostar t w ith some fundamental buildingblocks to ensure v is ibi l i t y across theenterprise. It is important to be able toembark on phased, cross-organizationalinit iat ives with stakeholder engagementon each init iat ive, namely : 1. Establish an enterprise data ware-house (EDW) as a single source oftruth across clinical, f inancial, andoperat ional systems. • Adopt a unif y ing data model anddata governance inf rast ructureref lec t ing a health-care enterpr isew ith inpat ient , outpat ient , physi-cian pract ice, a l l ied health faci l i-t ies , and even home-based cares ites . Such a data model w i l l incor-porate health-care–specif ic cl ini-ca l , operat ional , and f inancia lsubject areas across the care con-t inuum.
2. Progressively integrate sources intothe EDW in the fol lowing order : • general ledger, pat ient accounting,and charge master : RCC- and RVU-based cost ing;
• electronic medical records(EMR)/admission discharge andtransfer (ADT) for encounter- andpatient-level act iv ity detai ls (t ime-based drivers): labor cost ing v iaact iv ity-based cost ing (ABC);• supply chain: Rx direct costs; and• enterprise resource planning (ERP). 3. Establish a portfolio of cost ingmethods and standardize withinact iv ity types (cost pools) acrossservice l ines and continuum of care.
4. Standardize stakeholder-specificdashboards and reports in enter-prise BI solut ion: Engage stakehold-ers in definit ion, traceability, andvalidat ion.
5. Provide ad hoc report ing and root-cause analysis dri l l-down capabili-t ies.
Case study: Providence Health &ServicesThe Seattle-based Providence Health &Services is committed to a system-wideconsolidated decis ion suppor t systemwhile adopting such a phased approach.
25DECISION SUPPORT SYSTEMS SEPTEMBER/OCTOBER 2015 COST MANAGEMENT
EXHIBIT 6 Providence Health & Services Costing Journey
bstoehr
Typewritten Text
Cost Management, Volume 29, Number 5. Copyright 2015. Thomson Reuters/Tax & Accounting. Reprinted with permission.

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
A key first step is driv ing standardizedapproaches across the continuum of carefor defining and providing comparableand reliable financial, operat ional, andclinical data as it relates to the report-ing and analy t ics of cost, profitability,and performance of business operationsand health-care services. Christ ine San-tos, chief of strategic business analy t icsat Providence, remarked that “as healthsystems embrace value-based purchas-ing , a key f irst step is to extend theircost-accounting capabilit ies beyond theacute-care sett ing to include ambula-tor y /c l in ic s and pos t -acute s e t t ings(home health, long-term care, and hos-pice) bui lding the cr it ical foundat ionfor understanding the cost of deliveringcare across the cont inuum.” Exhibit 6i l lustrates Providence’s phased imple-mentation approach toward unified costaccounting across the continuum, begin-n ing w i th s t andard iz ing dat a input sacross the organizat ion.
ConclusionAn effect ive populat ion health strategyin the era of health-care reform demandsa comprehensive, pervasive, and data-driven financial decision support port-fol io operat ing f rom a s ing le uni f iedsource of high quality: reliable data acrossclinical, financial, and operational func-t ions. Consider ing the seven key ele-
ments presented here and implement-ing the act ion plan are excel lent stepstoward renovat ing your decision sup-port system to support today’s health-care reform.Health-care organizat ions l ike Prov-
idence that deploy advanced, business-user–configurable and non-prescriptivedecis ion suppor t solut ions can avoidbig-bang investments and progressivelyharness targeted data sources to gaininsight across the care continuum whileleveraging current “best pract ices.”Health care is changing whether we
like it or not. Take up the chal lenge andrenovate your decision support systemto support it . n
NOTES1 Better care. Smarter spending. Healthier people: Pay-ing providers for value, not volume (press release),Centers for Medicare and Medicaid Services (Jan26, 2015). Avai lable at: http:/ /www.cms.gov/News-room/MediaRe leaseDatabase /Fact -sheets /2015-Fact-sheets- items/2015-01-26-3.html.
2 Major health care players unite to accelerate trans-formation of U.S. health care system, Health CareTransformation Task Force (Jan 28, 2015). Avai lableat: http:/ /www.hcttf.org/releases/2015/1/28/major-hea l th -care -p layers -un i te - to -acce lerate - t ransfor -mation-of-us-health-care-system.
3 Herman, B., “10 stat ist ics on hospital labor costsas a percentage of operat ing revenue,” Becker ’sHosp i t a l Rev i ew (Dec 10 , 2013 ) . Ava i l ab l e a t :http://www.beckershospitalreview.com/finance/10-statist ics-on-hospital - labor-costs-as-a-percentage-of-operat ing-revenue.html.
4 “A Health IT Framework for Accountable Care,” Cer-t i f icat ion Commission for Health Information Tech-no logy (CCHIT ) ( June 6 , 2013 ) . Ava i l ab l e a t :http://www.healthit.gov/FACAS/sites/faca/files/a_health_it_framework_for_accountable_care_0.pdf.
26 COST MANAGEMENT SEPTEMBER/OCTOBER 2015 DECISION SUPPORT SYSTEMS
bstoehr
Typewritten Text
Cost Management, Volume 29, Number 5. Copyright 2015. Thomson Reuters/Tax & Accounting. Reprinted with permission.