

How to maximize patient access Perspectives from The ... · Multi stake-holder approach Include all...
26
Vs18f13 How to maximize patient access Perspectives from The Netherlands Budapest, June 13, 2018 Arnold G. Vulto PharmD PhD FCP Professor Em. of Hospital Pharmacy & Practical Therapeutics Erasmus University Medical Center Rotterdam, The Netherlands Honorary Professor KU Leuven, Belgium [email protected]
Transcript of How to maximize patient access Perspectives from The ... · Multi stake-holder approach Include all...

Vs18f13
How to maximize patient access
Perspectives from The Netherlands
Budapest, June 13, 2018
Arnold G. Vulto PharmD PhD FCP
Professor Em. of Hospital Pharmacy & Practical Therapeutics
Erasmus University Medical Center Rotterdam, The Netherlands
Honorary Professor KU Leuven, Belgium

Conflict of Interest Statement
▪ I declare no personal financial interest in any pharmaceutical business.
▪ I entertain friendly relationschips with all innovative and generic / biosimilar companies
and I help them all where I can.
▪ Companies / Organisations involved are: AbbVie, Amgen, Biogen, EGA (Medicines for
Europe), Mundipharma, Pfizer/Hospira, Roche, Novartis/Sandoz
▪ I am the co-founder of the Generics & Biosimilars Initiative (GaBi), The Dutch Initiative
Group on Biosimilars (IBN) and the KULeuven – ErasmusMC MABEL Research Fund
2

For background
▪ www.gabionline.net
▪ www.gabi-journal.net
▪ www.biosimilars-nederland.nl
▪ www.pharm.kuleuven.be/clinpharmacotherapy/mabel
3

My personal motto as a hospital pharmacist
4
My drive is optimal treatment for all patients
at an affordable cost
Science gives us the best possible description of the world.
It is emotion that is distorting the view.

The Dutch Landscape
▪ Healthcare-coverage in The Netherlands is based on universal solidarity
▪ (although 3rd party payers are private companies)
▪ General principle is: every patient has access to treatment according to the current
scientific insights
▪ But: government is concerned about finacial sustainability of health care
▪ Continuous pressure on savings
▪ The choice of more cost-effective medicines is on every agenda of our Ministry of
Health
▪ The Dutch Ministry of Health strongly promotes competition in the drug market,
both at the top (innovative medicines) as at the bottom (generics, biosimilars).
5

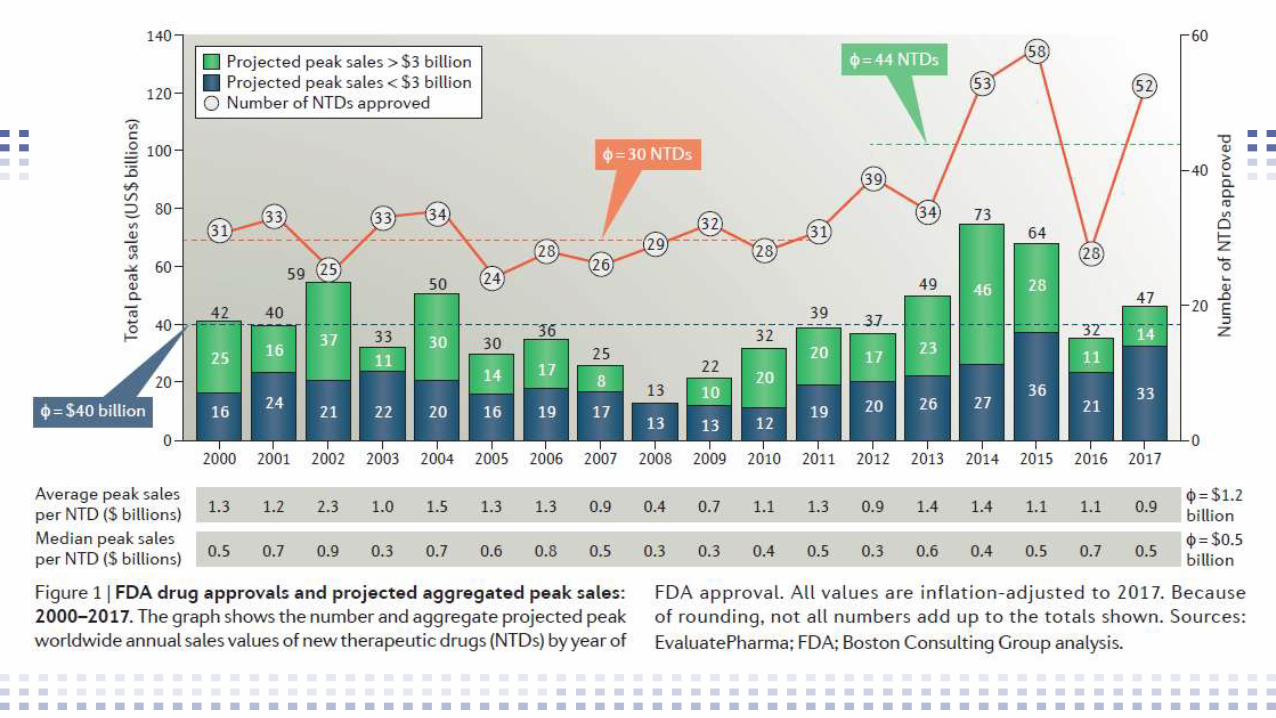
2017 approved blockbusters forecast 2023
40 billion dollars extra worldwide cost each year
Mullard A. Nat Rev Drug Discov 2018, January

How to maximize access to medicines?
▪ Biosimilars are cornerstone in 2 National policies:
▪Hoofdlijnenakkoord between Government and Healthcare-
sector
▪Cost-increase cost max 1% per year
▪ Improve efficiency: strengthen market-powers through
biosimilars
▪ Dutch Healthcare Institutes (NZI / NZA) carefully monitor both
policies and report to Minister / Parliament
8

The State of The
Netherlands 2016:
Medicines in
specialistic
medical care
9

▪ Total spending specialistic
medical care (2016):
23 miljard €
▪ From which expensive medicines:
2 miljard € (=8,4%)
▪ Annual increase in drug costs:
6,7% (mostly new, expensive
medicines)
10

11

NZA Monitor Expensive Medicines December 2017
Generic name Tradename Spending NL
2016 (M€)
Expiration
Exclusivity
adalimumab Humira 215 October 2018
etanerept Enbrel 142 free
Infliximab Remicade 139 free
trastuzumab Herceptin 77 free
Rituximab MabThera 63 free
Bevacizumab Avastin 58 2022 or earlier
total 69512

Potential effects expiring market exclusivities
▪ Imatinib (Glivec®, 2016 37 M€): ca. 90% reduction in acquisition costs
▪ Biological medicines spending in 2016 total ca. 700 M€
▪By competition in the market drop of 40 - 60% in costs
▪After 2018: ca. 1 million € savings EACH DAY!
▪ 3 Oncological drugs total in 2016 ca. 200 M€
▪Potential savings in due course 100 M€ of more per year
▪ However: savings can be less if volumes expand (see Norway)
13

Initiatives in Dutch Healthcare System
▪ Biosimilars Toolbox
▪ Joint initiative from Dutch Association of Hospital Pharmacists and
Federation of Medical Specialists
▪ BOM project
▪ Initiative from Biosimilars Nederland and Institute of Responsible
Medicines Use
▪ 3-year project, subsidised by Ministry of Health (800 k€E grant)
14

Dutch Hospital Pharmacists Association and
Dutch Federation of Medical Specialists
▪ Toolbox biosimilars (April 2017)
▪ A practical guide for succesful implementation
▪ Scientific background, definitions and
position papers (e.g. MEB)
▪ New patients, existing patients
▪ Implementation: task force and roadmap
▪ Policies for transitioning
▪ Information materials, letters
MEB, Medicines Evaluation Board

Successful biosimilar-policies follow the Rule of Four
1. Multi stake-holder approach
Include all that are involved: doctors, pharmacists, nurses, pharmacy-
technicians, patient(organisations), hospital management
2. Once voice principle
synchronise message from the healthcare-team; avoid nocebo-effects
3. Shared decision making
involve patient in decision-making process with positive attitude
4. Gain sharing
Create win-win for those who do the work (e.g. the medical department)

The confusing definition issue / words to avoid
▪ Switching is both:
▪ Change from one treatment / molecule to another
▪ Change from reference product to biosimilar
(also confusingly coined non-medical switching).
▪ Better word transitioning: only for biosimilars (FDA, Dörner, 2016)
▪ Interchangeability: EMA differs fundamentally from FDA
▪ Very confusing: population versus individual level
▪ Substitution:
▪ Why discuss? We don’t do it (with few exceptions).
▪ Using these words is framing the discussion (see: Lakoff/YouTube)
Weise et al. Nature Biotechnology 29, 690–693 (2011)
Dörner et al Ann Rheum Dis doi:10.1136/annrheumdis-2016-209166


BOM: Tailormade Education on
Biosimilars in Hospitals
National Educational Program for all
Hospitals
Sponsored by Ministry of Health (3 year,
800 k€)
19

BOM-project: on a voluntary basis (at no cost)
Objectives
▪ Increase knowledge about biosmilars among prescribers, hospital staff and patients
▪ Stimulate the prescribing of most cost-effective alternative when prescribing a
biological medicine
▪ Achieve maximal awareness of the potential offered by biosimilars to reduce
healthcare costs and increase access to medicines.
20

How the program is executed?
▪ Zero-measurement: inventory of todays situation in the hospital
▪ Acceptance of biosmilars; are there barriers?
▪ Local initiatives already started
▪ Efficiency of the drug-procurement process
▪ Initiation visit
▪ Tailormade educational program for all target-groups
▪ Lectures, classes, workshops, e-learning
▪ Monitoring developments (2 x per year)
▪ What works, what failed21

European Commission Q&A on biosimilars for patients
(available in almost all EU-languages)
http://ec.europa.eu/DocsRoom/documents/2664
3
▪ It contains questions and answers on
biosimilar medicines and is
now available in 23 languages,
serving as a reliable source of
information for patients.
▪ This consensus information on biosimilar medicinal products was
drafted by and for patients together with representatives of the
European Medicines Agency, the European Commission and
concerned stakeholders [the European Patients Forum (EPF), the
European Federation of Crohn’s & Ulcerative Colitis Associations
(EFCCA), the Standing Committee of European Doctors, European
Federation of Pharmaceutical Industries and Associations (EFPIA),
European Association for BioIndustries (EuropaBio) and Medicines
for Europe]. The Q&A was first launched in English in January 2017.

IAPO biosimilars toolkit (for patients) , update 2018 with 8 factsheets
https://www.iapo.org.uk/biosimilars-toolkit

IAPO biosimilars toolkit (for patients) update 2018 with 8 factsheets
https://www.iapo.org.uk/biosimilars-toolkit



















