How to Complete a Post Course Report
36
Military Training Network January 2015 Instructor Guide to Post Course Reports
Transcript of How to Complete a Post Course Report

Military Training Network
January 2015
Instructor Guide to Post Course
Reports

CONTENTS
IntroductionChecklistsPost Course Report (PCR)Grade ReportSummary of Course EvaluationsExample of a Completed PCRAdvanced Program PCR ChangesAgendasRemediation/FailuresMTN Wallet CardsConclusion

INTRODUCTION
MTN MissionThe mission of the Military Training Network
(MTN) is to develop and implement policy guidance and ensure compliance with curriculum
and administrative standards for resuscitative medicine programs.
Quality AssuranceStandardized Post Course Report Packages are an
integral part of quality assurance and program compliance.

INTRODUCTION
MTN Structure The MTN is the largest Regional Training Center aligned
under the American Heart Association.
Units that affiliate directly with the MTN are called Training Sites. A Training Site has assigned personnel to manage the
program for the unit including: the Program Director, Program Administrator, and Training Site Faculty (TSF).
Training Sites may have one or more satellites.
Instructors are aligned under the Training Site.

CHECKLISTS
MTN has developed a PCR Package for each discipline: BLS ACLS PALS/PEARS
The checklist page is the Instructor’s tool to make sure you have turned in everything needed to the Training Site. Instructors are responsible for completing the PCR and Grade Report correctly.

BLS CHECKLIST

ACLS CHECKLIST

PALS/PEARS CHECKLIST

Post Course Report Packages
MTN staff commonly refer to the Post Course Report Package as a PCR.
The PCR Package includes: Post Course Report page
Grade Report page Summary of all Course Evaluations
All PCRs must be typed. This will reduce clerical errors and increase efficiency of processing wallet cards by the Training Site staff.

PCRs
Training Sites are required to maintain a completed PCR Package for every course taught for three years.
Program Directors/Administrators are required to review PCRs for quality assurance.
If an error is made or documentation is missing, the Training Site Program Director/Administrator will ask the Instructor to correct the error.

Filling out a BLS PCR
Course Type, Location, Date and Number of Students
Lead Instructor’s Information
Program Director/Administrator Endorsement
Instructor List

Filling out a BLS PCR
POST COURSE REPORT
(Complete one PCR for each course)
Date:
Type of course conducted: Training Site Name Complete Course Location
Date Started
Date Completed # Enrolled
# Enrollees Retrained (those who completed course at
least once in their past)
# cards issued Provider / Instructor # of instructor reregistered
/
Lead Instructor’s Information
(Full Name, Rank, Corps)
(Work Phone No.) Comm DSN
(Work Email Address)
Infection Control Guidelines were adhered to during course and equipment was cleaned IAW Manufacturers instructions at the completion of the course:
_______________________________________________________ Signature and Title
Enter the type of course (e.g. HCP, HCP Refresher, HS – I, HS Refresher)
Enter the Training Site Name, avoid abbreviations.(e.g. 36th Medical Group, Martin Army Community Hospital)
Enter the date as DDMMMYY (e.g. 12Nov14)
Enter the location of the course. If the course is held at a satellite, list the satellite name here. (e.g. 123 A Street, Bldg 120, Rm 220 Fort Knox, KY)

Filling out a BLS PCR
POST COURSE REPORT
(Complete one PCR for each course)
Date:
Type of course conducted: Training Site Name Complete Course Location
Date Started
Date Completed # Enrolled
# Enrollees Retrained (those who completed course at
least once in their past)
# cards issued Provider / Instructor # of instructor reregistered
/
Lead Instructor’s Information
(Full Name, Rank, Corps)
(Work Phone No.) Comm DSN
(Work Email Address)
Infection Control Guidelines were adhered to during course and equipment was cleaned IAW Manufacturers instructions at the completion of the course:
_______________________________________________________ Signature and Title
Enter the date as DDMMMYY (e.g. 12Nov14)
Enter the date as DDMMMYY (e.g. 12Nov14)
Enter the number of students who have taken the course previously, as documented on the Grade Report (count only students who answer “No” in the First Time Student column).
Enter the number of students enrolled in the course.

Filling out a BLS PCR
POST COURSE REPORT
(Complete one PCR for each course)
Date:
Type of course conducted: Training Site Name Complete Course Location
Date Started
Date Completed # Enrolled
# Enrollees Retrained (those who completed course at
least once in their past)
# cards issued Provider / Instructor # of instructor reregistered
/
Lead Instructor’s Information
(Full Name, Rank, Corps)
(Work Phone No.) Comm DSN
(Work Email Address)
Infection Control Guidelines were adhered to during course and equipment was cleaned IAW Manufacturers instructions at the completion of the course:
_______________________________________________________ Signature and Title
Enter the Lead Instructor’s Contact Information to include telephone number and email.
Lead Instructor’s Signature Block. The Lead Instructor endorses that the infection control guidelines prescribed by the Training Site were adhered too.
***Note this is not an Infection Control Policy. The Training Site should provide the Instructor with infection control training specific to the equipment at the Training Site.

Filling out a BLS PCR
Program Administrator Information
(Full Name, Rank, Corps)
(Work Phone No.) Comm DSN
(Work Email Address)
I certify this course has been conducted under the standards and procedures established by the American Heart Association and the Military Training Network. ____________________________ ________________________________ Program Director Signature Program Administrator Signature
Enter the Program Administrator’s contact information.
When the Program Director receives a completed PCR, he/she will review and endorse the course. MTN wallet cards will be issued once the Program Director accepts the completed PCR.
The Program Administrator will review and endorse the course here. The Program Administrator will prepare the wallet cards for the Program Director.

BLS Grade Report
GRADE REPORT FOR BLS COURSE
COURSE DATE:
(Annotate with completed (C), with remediation (R), Instructor-Potential (IP), or unsuccessful (U) under appropriate column).
Minimum passing score on the written exam is 84%. (+) Indicates student has been remediated by Course Director or Instructor on missed items (i.e. using annotated answer key). Any Unsuccessful test score sheets and psychomotor skills must be maintained with the PCR.
Name (Last, First, MI) Rank, Branch of Service, Corps
Professional Licensure (MD, DO, CRNA, RN,
EMT, etc.)
Skills and evaluation
stations
First time student (Y or N)
Written Exam (84%)
Retest ( 84%) (+)
Performance Level
Date Monitored by TSF
(Instructor Courses only)
Enter the type of course (HCP-R, HS-Instructor, etc).
Enter the student’s information.
Enter the student’s professional licensure. (e.g. MD, DO, CRNA, RN, EMT, etc).
If no professional licensure, leave blank.
Enter the student’s completion of psychomotor skills stations as “C”, “R” or “U”.
Enter First time student “Y” or “N”.
Enter the course date as DDMMMYY.

BLS Grade Report
GRADE REPORT FOR BLS COURSE
COURSE DATE:
(Annotate with completed (C), with remediation (R), Instructor-Potential (IP), or unsuccessful (U) under appropriate column).
Minimum passing score on the written exam is 84%. (+) Indicates student has been remediated by Course Director or Instructor on missed items (i.e. using annotated answer key). Any Unsuccessful test score sheets and psychomotor skills must be maintained with the PCR.
Name (Last, First, MI) Rank, Branch of Service, Corps
Professional Licensure (MD, DO, CRNA, RN,
EMT, etc.)
Skills and evaluation
stations
First time student (Y or N)
Written Exam (84%)
Retest ( 84%) (+)
Performance Level
Date Monitored by TSF
(Instructor Courses only)
Enter the student’s written exam score. Minimum passing score is 84%.
Enter the student’s overall performance as “C”, “R”, “U” or “IP”. If student received remediation during either psychomotor skills or on the written exam, performance must be marked “R”.
Leave blank. For Instructor Courses only: PD/TSF will enter date.
Enter Retest score if applicable. Enter (+) to indicate remediation was completed.

Summary of Course Evaluations
Instructions: Please take a moment to complete this evaluation for the course in which you just participated. We want to provide excellent courses, and we value your opinion. Program Director:**Use shaded boxes after yes or no for total responses. Submit a summary of course evaluations with all suggestions or concerns to the MTN.
Which course did you complete: HS BLS ACLS PALS PEARS (check one)
Date (s) of Course: Name of Training Site:
Type of Course: Lead Instructor:
Course Content: 1. The course learning objectives were clear? Yes No
2. The overall level of difficulty of the course was? Easy Appropriate Difficult
3. The content was presented clearly? Yes No
4. The quality of videos and written materials was? Excellent Good Fair Poor
5. The equipment was clean and in good working condition? Yes No Skill Mastery:
1. The course prepared me to successfully pass the skills session? Yes No 2. I am confident I can use the skills the course taught me? Yes No Not Sure 3. I will respond in an emergency because of the skills I learned in this course? Yes No Not Sure 4. I took this course to obtain professional education credit or continuing
education credit? Yes No
My Instructor: 1. Provided instruction and help during my skills practice session? Yes No 2. Answered all of my questions before my skills test? Yes No 3. Was professional and courteous to the students? Yes No
6. Please rate the overall quality of the instructor (s): Excellent Good Fair Poor
Were there any strengths or weakness of the course that you would like to comment on? _______________________________________________________________________________________ ___________________________________________________________________________________________ Did this course meet your learning needs (visual, auditory, didactic, kinetic, etc)? How can we improve? _______________________________________________________________________________________ ___________________________________________________________________________________________ Do you have any recommendations to improve this course? ________________________________________________________________________________________________________
Student Name (Optional): Contact Information: Your comments will be used to make ongoing improvements in our program. Thank you for your participation.
Military Training Network Summary Course Evaluation
Instructors must also inform students that they can provide feedback directly to AHA. AHA contact information is found each Instructor Manual.
AHA and MTN requires a summary of all course evaluations to be maintained with the PCR.
Each student must be given an opportunity to provide feedback on AHA courses.

Summary of Course Evaluations
Instructions: Please take a moment to complete this evaluation for the course in which you just participated. We want to provide excellent courses, and we value your opinion. Program Director:**Use shaded boxes after yes or no for total responses. Submit a summary of course evaluations with all suggestions or concerns to the MTN.
Which course did you complete: HS BLS ACLS PALS PEARS (check one)
Date (s) of Course: Name of Training Site:
Type of Course: Lead Instructor:
Course Content: 1. The course learning objectives were clear? Yes No
2. The overall level of difficulty of the course was? Easy Appropriate Difficult
3. The content was presented clearly? Yes No
4. The quality of videos and written materials was? Excellent Good Fair Poor
5. The equipment was clean and in good working condition? Yes No Skill Mastery:
1. The course prepared me to successfully pass the skills session? Yes No 2. I am confident I can use the skills the course taught me? Yes No Not Sure 3. I will respond in an emergency because of the skills I learned in this course? Yes No Not Sure 4. I took this course to obtain professional education credit or continuing
education credit? Yes No
My Instructor: 1. Provided instruction and help during my skills practice session? Yes No 2. Answered all of my questions before my skills test? Yes No 3. Was professional and courteous to the students? Yes No
6. Please rate the overall quality of the instructor (s): Excellent Good Fair Poor
Were there any strengths or weakness of the course that you would like to comment on? _______________________________________________________________________________________ ___________________________________________________________________________________________ Did this course meet your learning needs (visual, auditory, didactic, kinetic, etc)? How can we improve? _______________________________________________________________________________________ ___________________________________________________________________________________________ Do you have any recommendations to improve this course? ________________________________________________________________________________________________________
Student Name (Optional): Contact Information: Your comments will be used to make ongoing improvements in our program. Thank you for your participation.
Military Training Network Summary Course Evaluation
The center section consists of rated questions, to include a section to allow students to rate the instructor(s).
The bottom section allows students to write in any additional comments. Contact information is optional for students who would like to be contacted regarding their comments.
The top section identifies the type of course, date, and location.

Course Content:
1. The course learning objectives were clear? Yes No
2. The overall level of difficulty of the course was? Easy Appropriate Difficult
3. The content was presented clearly? Yes No
4. The quality of videos and written materials was? Excellent Good Fair Poor
5. The equipment was clean and in good working condition? Yes No
Skill Mastery:
1. The course prepared me to successfully pass the skills session? Yes No
2. I am confident I can use the skills the course taught me? Yes No Not Sure
3. I will respond in an emergency because of the skills I learned in this course? Yes No Not Sure
4. I took this course to obtain professional education credit or continuing education credit? Yes No
My Instructor:
1. Provided instruction and help during my skills practice session? Yes No
2. Answered all of my questions before my skills test? Yes No
3. Was professional and courteous to the students? Yes No
6. Please rate the overall quality of the instructor (s): Excellent Good Fair Poor
Summary of Course Evaluations
In the fill-able box next to each question, enter the number of students that answered each question.
Gather all student course evaluations to summarize. Mark each rated box based on the students’ responses.

Were there any strengths or weakness of the course that you would like to comment on? _______________________________________________________________________________________ ___________________________________________________________________________________________ Did this course meet your learning needs (visual, auditory, didactic, kinetic, etc)? How can we improve? _______________________________________________________________________________________ ___________________________________________________________________________________________ Do you have any recommendations to improve this course? ________________________________________________________________________________________________________
Student Name (Optional): Contact Information: Your comments will be used to make ongoing improvements in our program. Thank you for your participation.
Summary of Course Evaluations
Summarize students’ written responses responses.
Student contact information is option. This information is used if a student requests feedback from the training site. The Program Director will contact the student.

Example of Completed BLS PCRPOST COURSE REPORT
(Complete one PCR for each course)
Date: 5 Jan 15
Type of course conducted: HCP Training Site Name 1234th Medical Group Complete Course Location Bldg 2 Rm 123
Date Started
Date Completed # Enrolled
# Enrollees Retrained (those who completed course at
least once in their past)
# cards issued Provider / Instructor # of instructor reregistered
5 Jan 15 5 Jan 15 6 3 /
Lead Instructor’s Information
(Full Name, Rank, Corps) John Doe, SSG, USA
(Work Phone No.) Comm 555-1234 DSN 555-1234
(Work Email Address) [email protected]
Infection Control Guidelines were adhered to during course and equipment was cleaned IAW Manufacturers instructions at the completion of the course:
_______________________________________________________ Signature and Title
Program Administrator Information
(Full Name, Rank, Corps) Wendy Marvin, MAJ
(Work Phone No.) Comm 555-4321 DSN 555-4321
(Work Email Address) [email protected]
I certify this course has been conducted under the standards and procedures established by the American Heart Association and the Military Training Network. ____________________________ ________________________________ Program Director Signature Program Administrator Signature
MILITARY TRAINING NETWORK INSTRUCTOR LIST
Instructor’s Full Name (Last, First, MI) Rank, Branch of Service, Corps
(Include Lead Instructor)
Professional Licensure (MD, DO, CRNA, RN,
EMT, etc.)
AHA Instructor Card Exp
Date
PD, TSF, or Inst
**Renewing Instructor
(yes/no)
John Doe, SSG, USA EMT Jan 15 Inst Y
Daisy Helper, LT, USN RN Jul 16 TSF N

Example of Completed BLS PCR
GRADE REPORT FOR BLS HCP COURSE
COURSE DATE: 5 Jan 15
Name (Last, First, MI) Rank, Branch of Service, Corps
Professional Licensure (MD, DO, CRNA, RN,
EMT, etc.)
Skills and evaluation
stations
First time student (Y or N)
Written Exam (84%)
Retest ( 84%) (+)
Performance Level
Date Monitored by TSF
(Instructor Courses only)
Mouse, Michael Capt, USAF
DO C N 96% IP
Ducky, David SFC, USA
EMT C N 88% C
Folgers, Kermit LT, USN
CRNA C N 96% C
Lion, Alexander PV1, USA
EMT C Y 76% 84% + R
Giraffe, Melanie SN, USN
C Y 76% 80% U
Vacation, Inda A1C, USAF
EMT C Y 88% C

Example of Completed PCR
Instructions: Please take a moment to complete this evaluation for the course in which you just participated. We want to provide excellent courses, and we value your opinion. Program Director:**Use shaded boxes after yes or no for total responses. Submit a summary of course evaluations with all suggestions or concerns to the MTN.
Which course did you complete: HS BLS ACLS PALS PEARS (check one)
Date (s) of Course: 5 Jan 15 Name of Training Site: 1234th Medical Group
Type of Course: Refresher Lead Instructor: John Doe
Course Content: 1. The course learning objectives were clear? Yes 6 No
2. The overall level of difficulty of the course was? Easy 4 Appropriate 1 Difficult 1
3. The content was presented clearly? Yes 6 No
4. The quality of videos and written materials was? Excellent 5 Good 1 Fair Poor
5. The equipment was clean and in good working condition? Yes 6 No Skill Mastery:
1. The course prepared me to successfully pass the skills session? Yes 6 No 2. I am confident I can use the skills the course taught me? Yes 5 No Not Sure 1 3. I will respond in an emergency because of the skills I learned in this course? Yes 5 No Not Sure 1 4. I took this course to obtain professional education credit or continuing
education credit? Yes No 6
My Instructor: 1. Provided instruction and help during my skills practice session? Yes 6 No 2. Answered all of my questions before my skills test? Yes 6 No 3. Was professional and courteous to the students? Yes 6 No 6. Please rate the overall quality of the instructor (s): John Doe – 5 Excellent, Lt
Helper – 1 Good
Excellent 5 Good 1 Fair Poor
Were there any strengths or weakness of the course that you would like to comment on? This was my first time taking this course/ videos were easy to follow _______________________________________________________________________________________ ___________________________________________________________________________________________ Did this course meet your learning needs (visual, auditory, didactic, kinetic, etc)? How can we improve? Yes x 6 _______________________________________________________________________________________ ___________________________________________________________________________________________ Do you have any recommendations to improve this course? More practice time ________________________________________________________________________________________________________
Military Training Network Summary Course Evaluation

Advanced Programs PCR Changes
POST COURSE REPORT
(Complete one PCR for each course)
Date: (DDMMMYY)
MTN Training Site Name: Training Site Address: Check type of course conducted: ACLS Initial ACLS Renewal ACLS Instructor
Date Started Date Completed # Enrolled # of Personnel Trained:
MD RN Other # cards issued
Provider / Instructor # of instructor reregistered
/
MILITARY TRAINING NETWORK INSTRUCTOR LIST
Lead Instructor’s Full Name (Last, First, MI) Rank, Branch of Service, Corps
Professional Licensure (MD, DO, CRNA, RN,
EMT, etc.)
AHA Instructor Card Exp
Date
PD, TSF, or Inst
**Renewing Instructor (yes/no)
NAME: Work Phone: Work Email:
Additional Instructor’s Full Name (Last, First, MI) Rank, Branch of Service, Corps
Lead Instructor Infection Control Affirmation Infection Control Guidelines were adhered to during course and equipment was cleaned IAW Manufacturers instructions at the completion of the course:
_____________________________________________________ Lead Instructor Signature
Program Administrator Information
(Full Name, Rank, Corps)
(Work Phone No.) Comm DSN
(Work Email Address)
I certify this course has been conducted under the standards and procedures established by the American Heart Association and the Military Training Network. ____________________________________ _____________________________________ Program Administrator Signature Program Director Signature
ACLS/PALS/PEARS PCRs need additional student information. Lead Instructor and Additional Instructor information has been streamlined together to reduce redundancy.

ACLS PCR
Check type of course conducted: ACLS Initial ACLS Renewal ACLS Instructor
Date Started Date Completed # Enrolled # of Personnel Trained:
MD RN Other # cards issued
Provider / Instructor # of instructor reregistered
/
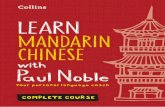
Mark the box that corresponds with the course type.
Enter the date the course started and was completed as DDMMMYY.
Enter the number of students enrolled in the course. Do not include instructors or evaluators.
This is a breakdown of personnel trained by category as follows: - MD: Enter the number of doctors (MDs, DOs, DDS’s, DMDs) - RN: Enter the number of Nurses (RNs, CNMs, CRNAs, FNPs, NPs) - Other: Enter all other personnel (PAs, LVNs, EMTs, etc)

Check type of course conducted: PALS Initial PALS Renewal PALS Instructor PEARS Provider PEARS Instructor
Date Started Date Completed # Enrolled # of Personnel Trained:
MD RN Other # cards issued
Provider / Instructor # of instructor reregistered
/
PALS/PEARS PCRMark the box that corresponds with the course type.
Enter the date the course started and was completed as DDMMMYY.
Enter the number of students enrolled in the course. Do not include instructors or evaluators
This is a breakdown of personnel trained by category as follows: - MD: Enter the number of doctors (MDs, DOs, DDS’s, DMDs) - RN: Enter the number of Nurses (RNs, CNMs, CRNAs, FNPs, NPs) - Other: Enter all other personnel (PAs, LVNs, EMTs, etc)

ACLS and PALS/PEARS Grade Report
GRADE REPORT FOR ACLS COURSE
Check type of course conducted: ACLS Initial ACLS Renewal ACLS Instructor
COURSE DATE:
Name (Last, First, MI) Rank, Branch of Service, Corps
Professional Licensure (MD, DO,
CRNA, RN, EMT, etc.)
BLS Exp. Date
First Time Student (Y or N)
Skills Stations Written
Test/Re-test ( 84%) (+)
Megacode Performance Level
Date Monitored by TSF
(Instructor Courses only)
GRADE REPORT FOR PALS/PEARS COURSE
Check type of course conducted: PALS Initial PALS Renewal PALS Instructor PEARS Provider PEARS Instructor
COURSE DATE:
Name (Last, First, MI) Rank, Branch of Service, Corps
Professional Licensure (MD, DO,
CRNA, RN, EMT, etc.)
BLS Exp. Date
First time student (Y or N)
Skills Stations
Written Test/Re-test ( 84%) (+)
Megacode Performance Level
Date Monitored by TSF
(Instructor Courses only)
Mark the box that corresponds with the course type.

Agendas
Whenever possible, a standard agenda should be followed. Training Sites will maintain copies of the agendas. Standardized agendas are available on the MTN website at: http://www.usuhs.edu/mtn/mtnprogramstools.html
Instructors should provide the course agenda to students two weeks in advance of the course whenever possible.
If a change is made to the agenda, you must submit the agenda change with the PCR package to your Training Site.

Remediation/Failures
If a student does not successfully complete the psychomotor skills evaluation or the written exam, the instructor should provide remediation in accordance with the AHA Instructor Course guidelines. After remediation, the student is re-tested.
If the student is successful on the second attempt, the student’s performance is marked as “R” for remediation.

Remediation/Failures
If the student fails to successfully complete the psychomotor skills evaluation and/or the written test again, the student’s performance is marked as “U” for unsuccessful.
Document remediation and failures on the Grade Report and turn in all unsuccessful psychomotor skills and test score sheets with the PCR.
GRADE REPORT FOR BLS HCP COURSE
COURSE DATE: 5 Jan 15
Name (Last, First, MI) Rank, Branch of Service, Corps
Professional Licensure (MD, DO, CRNA, RN,
EMT, etc.)
Skills and evaluation
stations
First time student (Y or N)
Written Exam (84%)
Retest ( 84%) (+)
Performance Level
Date Monitored by TSF
(Instructor Courses only)
Lion, Alexander PV1, USA
EMT C Y 76% 84% + R
Giraffe, Melanie SN, USN
C Y 76% 80% U

ACLS/PALS/PEARS Grade Report
GRADE REPORT FOR ACLS COURSE
Check type of course conducted: ACLS Initial ACLS Renewal ACLS Instructor
COURSE DATE:
Name (Last, First, MI) Rank, Branch of Service, Corps
Professional Licensure (MD, DO,
CRNA, RN, EMT, etc.)
BLS Exp. Date
First Time Student (Y or N)
Skills Stations Written
Test/Re-test ( 84%) (+)
Megacode Performance Level
Date Monitored by TSF
(Instructor Courses only)
Ducky, David 1Lt, USAF
Oct 2025 N C 76/84%+ C R
GRADE REPORT FOR PALS/PEARS COURSE
Check type of course conducted: PALS Initial PALS Renewal PALS Instructor PEARS Provider PEARS Instructor
COURSE DATE:
Name (Last, First, MI) Rank, Branch of Service, Corps
Professional Licensure (MD, DO,
CRNA, RN, EMT, etc.)
BLS Exp. Date
First time student (Y or N)
Skills Stations
Written Test/Re-test ( 84%) (+)
Megacode Performance Level
Date Monitored by TSF
(Instructor Courses only)
Ducky, David 1Lt, USAF
Oct 2025 Y C 76/84%+ C R
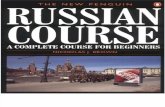
For advanced programs, document student completion of Skills Stations, Written test, Re-test and Megacode.
Documentation of Written Exam remediation will include the initial Written Test score and the Re-test score.

MTN Wallet Cards
MTN Wallet Cards are issued to the instructor for dispersal to students when the Program Director accepts a completed PCR package.
The MTN Wallet Cards should be stamped, typed, or computer printed.
Reference the Emergency Cardiovascular Care Course Card Reference Guide and the AHA Training Memo dated 29 May 2013 for further guidance.

Conclusion
If you have any questions, please contact the Training Site Program Director.

References
Military Training Network Administrative Handbook, 6th Edition, January 2014
The American Heart Association Program Administration (PAM) Manual, 5th Edition, February 1, 2013 (U.S. Version)
American Heart Association Training Memo dated 29 May 2013 The American Heart Association Advanced Cardiovascular Life
Support Instructor Course Faculty Guide May 2013 The American Heart Association Instructor Manual for Advanced
Cardiac Life Support (ACLS), 2011 The American Heart Association Basic Life Support Instructor
Course Faculty Guide May 28, 2013 The American Heart Association (AHA) Instructor Manual for
Basic Life Support (BLS), 2011

References
The American Heart Association Heartsaver Instructor Course Faculty Guide May 28, 2013
The American Heart Association Instructor Manual for Heartsaver First Aid CPR AED (HS CPR AED), 2011
The American Heart Association Pediatric Advanced Life Support Instructor Course Faculty Guide May 2013
The American Heart Association Instructor Manual for Pediatric Advanced Life Support (PALS), 2012
The American Heart Association Pediatric Emergency Assessment, Recognition, and Stabilization Instructor Course Faculty Guide May 2013
The American Heart Association Instructor Manual for Pediatric Emergency Assessment, Recognition, and Stabilization (PEARS), 2012
Emergency Cardiovascular Care Course Card Reference Guide June 2014