How Hypertrophic Cardiomyopathy Became a Contemporary ...
18
Barry J. Maron, MD Hypertrophic Cardiomyopathy Institute Tufts Medical Center Boston, MA Disclosures: Medtronic (Grantee) GeneDx (Consultant) How Hypertrophic Cardiomyopathy Became a Contemporary Treatable Genetic Disease With Low Mortality Shaped by 50 Years of Clinical Research and Practice
Transcript of How Hypertrophic Cardiomyopathy Became a Contemporary ...

Barry J. Maron, MDHypertrophic Card iomyopa thy Ins titu te
Tufts Medica l Cente rBos ton , MA
Dis c los ures :Medtronic (Grantee )GeneDx (Cons ultan t)
How Hypertrophic CardiomyopathyBecame a Contemporary TreatableGenetic Disease With Low Mortality
Shaped by 50 Years of Clinical Researchand Practice

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV mas sMas s ive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apica l aneurys mMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV mas sAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV mas sMassive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apica l aneurys mMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV mas sAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD
U.S./Canada: ACC/AHA: 2011


0
2
4
6
8
10
12
14
16
<15 16-19 20-24 25-29 30
Max. LV Wall Thicknes s (mm)
%P
ati
en
tsW
ith
SC
DRe la tio n Be twe e n LV Th ic kn e s s &
S CD in 482 HCM P a tie n ts

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV mas sMas s ive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apica l aneurys mMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV mas sAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD
U.S./Canada: ACC/AHA 2011

0
10
20
30
40
50
60
70
Alive Non-
Cardiac
De ath
Non-HCM
Cardiac
De ath
Embolic
S troke
He art
Failure
SCD
%o
fH
CM
Co
ho
rt
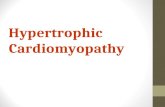
65%
13% 12%
2% 1%
0.2%/y
Outcome of HCM Patien ts Firs t Eva lua ted ≥ 60 Years
1%
HCM Death
Aging is Good in HCM
Maron BJ et. a l.Circ 2013; 127: 585

Intermediate
LowRisk
Risk Stratification for Sudden Death in HCM
Moderate
High
No risk factors
Family historyof suddendeath
NonsustainedVT
Unexplainedsyncope
ExtremeLVH
AbnormalBPresponsetoEx
0.5%/year

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV mas sMas s ive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apical aneurysmMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV mas sAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD
U.S./ Canada (ACC/AHA) 2011

C
D E F
D
P
VS
B
P
D
** *
**
*
Figure1.

1.0
0.8
0.6
0.4
0.0
0 5 1510 20
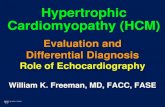
HCM pat ient s w i t hout LV apic a l aneur ysm sHCM pat ient s w i t h LV apic a l aneur ysm
Lo g-r ank t es t p<0 .00 1
Years f rom Fi rst Eva luat ion
Su
rviv
al
fre
efr
om
HC
Mre
late
dm
ort
ali
tya
nd
ad
ve
rse
ev
en
ts
0.2
H CM Re lat ed Deat h o r A dve r se Cl in ic a l Even t sin 93 Pat ien t s w i t h LV A p ic a l A neu r ysm s
8 .1% /yea r
1 .7% /yea r

LA
LA
V S
RV
LV VS
A B C
D E F
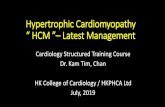
Pr eva lenc eo f LGE = 55 -70%

LGE
LGELGE
Extent of LGE vs. Sudden Death Risk in HCM
Follow-up (years )
Su
rviv
al
LGE (-)LGE < 10%
LGE 10-20%
LGE > 20%
Chan RH et. a l.Circ 2014; 130(6):484-95

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV massMas s ive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apica l aneurys mMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV massAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD

0
0.5
1
1.5
2
%H
CM
Mo
rta
lity
HCM-Re la te d Mo rta lity
0
0.5
1.5
1
6
Genera l U.S .Popula tion
0.8%/y
0.5%/y
1.5%/y
3-6%/y
Early HCMReferra l Cohorts
HCM Cohorts :P rior to u tiliza tion
of cu rren t trea tments tra teg ies /
in te rven tions
ICD inte rve ntionHeart trans p lant/myectomy
OHCA/d efib rilla tion/hypo thermia
Pres ent HCMCohort:
Contempora rytrea tment

ICD
S u d d e n
De a th
Progres s iveHeart
Fa ilure(obs tructive)
AdvancedHeart Fa ilure& End Stage
(non-obs tructive)
AF
&
S tro ke
Benign/S table(n o rm a l lo n g e vity)
DrugsSep ta l Myec tomy(Alcohol Abla tion)
Trans plant DrugsAnticoagulan ts
Abla tion
Profiles in Prognosis for HCM

(15%)
(15%)
(7%)
(7%)
(<1%)
(<1%)
(<1%)
(<1%)
(<1%)
(<1%)

25-Year Contemporary In itia tives inHypertrophic Card iomyopa thy
Genetic (molecu la r)S ingle s arcomere muta tion
hypothes is “ Clin ic ians ”
0 ThousandsLive s
S a ve d
0 Many thousandsIm p ro ve d
Qu a lity o f
Life