How can we reduce the mortality of ruptured aaa
20
Antalya, 27/30-10-2011 Medical School Twente How can we reduce the mortality of ruptured AAA? Pitfalls ! EVAR team Medisch Spectrum Twente Enschede, the Netherlands
-
Upload
uvcd -
Category
Presentations & Public Speaking
-
view
157 -
download
3
Transcript of How can we reduce the mortality of ruptured aaa

Antalya, 27/30-10-2011 Medical School Twente
How can we reduce the mortality of ruptured AAA?
Pitfalls!
EVAR team Medisch Spectrum Twente
Enschede, the Netherlands

Antalya, 27/30-10-2011 Medical School Twente
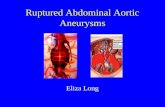
Ruptured AAA
• No surgical treatment
• Open approach
• EVAR

Antalya, 27/30-10-2011 Medical School Twente
Ruptured AAA
• No surgical treatment
• Non-responsive patient
- 2 year prospective study -> 100% mortality
• Very old patient?
- Do no harm
- Recent discussion: costs
- Older patients benefit more
Giles et al. J Endovasc Ther, 2009, 16, 365-372 and 554-564

Antalya, 27/30-10-2011 Medical School Twente
Ruptured AAA
• Open approach
- High mortality rate
- Little improvement over the last decades
- Little change of techniques

Antalya, 27/30-10-2011 Medical School Twente
Ruptured AAA
• rEVAR
- New technique
- New generations grafts
- Periscope and chimney grafts
- Less invasive
- Reduced ischemia and reperfusion injury
Fast ongoingdevelopment

Antalya, 27/30-10-2011 Medical School Twente
Ruptured AAA in reality• Call from ambulance, GP or other hospital
– “scoop and run”, where to? (high volume, transfer time)
– Permissive hypotension, reduce hypertension
– Inform team
• On arrival
– CTa, not ultrasound
- Extravasation of blood outside vessel wall: rupture
- Where is the rupture located
- Open repair: anatomic information (left renal vein, horseshoekidney, additional aneurysms, cross clamp site, Riolan collateral)
– Responsive?
– Last moment for family members (1 min)
OR

Antalya, 27/30-10-2011 Medical School Twente
Ruptured AAA in practiseEVAR team:
•Radiologist and surgeon– EVAR possible?
• Neck length
• Landing zone(s)
• Access
• Angulation
• Thrombus/calcification
•In the mean time– Patient is prepared in OR

Antalya, 27/30-10-2011 Medical School Twente
Ruptured AAA in practise
EVAR possible:
• AUI?
• Bifurcation graft?
• Tube?
• Femoral dissection

Antalya, 27/30-10-2011 Medical School Twente
When AUI?

Antalya, 27/30-10-2011 Medical School Twente
When AUI?

Antalya, 27/30-10-2011 Medical School Twente
Preserve side branches
X

Antalya, 27/30-10-2011 Medical School Twente
the bulge shaped neck
Type Ia endoleak

Antalya, 27/30-10-2011 Medical School Twente

Antalya, 27/30-10-2011 Medical School Twente
Type Ia endoleak75 year
contained RAAA
H1 45 mm; angulation 800
AUI; uneventful recovery
Plain abdominal 5th PO day
Plain abd 9th PO month
Progressive angulation
Migration
No endoleakage (CT)Conversion?
Suprarenal clampThrombus sealed
No endoleakage
Cut through the
exoskeleton with
orthopedic scissor
Infrarenal inlay anastomosisFollow up 4 years
No complicationsPlain abd. (discharge 8th po-day)

Antalya, 27/30-10-2011Medical School Twente
Type Ia endoleak
72 year, SAAA
AUI; perop DSA small endoleak (type ?)
3e po night; shock (systolic<50mmHg)
CT; contained RAAA
DSA; type 1 prox and type 3 connection

Antalya, 27/30-10-2011 Medical School Twente
Ruptured AAA in practise
Supra celiac balloon occlusion?
• Can render an unstable patient to steady state
• Wires?
• Emboli and thrombosis

Antalya, 27/30-10-2011 Medical School Twente
Ruptured AAA in practisepost-operative
•Abdominal compression syndrome
– Major killer
• Increases early mortality up to 5x
• Bladder pressure > 20 mmHg
• rEVAR 20% vs open 20-33%
•Intestinal injury
– Ischemia and reperfusion
– Motor inflammatory response -> MOF

Antalya, 27/30-10-2011 Medical School Twente
How can we reduce the mortality of ruptured AAA?
• Protocolise the complete route of the patient
₋ From the initial call until discharge
• Work with an experienced team
• Concentrate in high volume hospitals
• Keep it simple
• Be informed about the anatomical situation
• Use rEVAR when possible
– Local anaesthesia

Antalya, 27/30-10-2011 Medical School Twente
Pitfalls!
– Select patients
– Use CTa, not ultrasound
– Always the same experienced team and the same procedure
• Radiologist and vascular surgeon day and night
• Femoral dissection
• Do not stare to the neck
– Do not cover AII if not needed, spare branches (I/R)
– In case of a type Ia endoleak and conversion
• Just treat proximal, avoid cross clamping

Antalya, 27/30-10-2011 Medical School Twente
Pitfalls!• rEVAR
-Be sure you have the equipment
• Omniflush and snare
• Balloons, stents and coils
• Large (21-24 Fr) destination sheets
• Long wires (additional access via the arm)
• Post-operatively watch for
-Abdominal compartment syndrome
- Intestinal injury
• CA, SMA, IMA (pathological collateral – Riolan?)