How can we control VRE?
38
How can we control VRE? ACIPC plenary presentation November 2021 JOHN FERGUSON INFECTIOUS DISEASES PHYSICIAN & MICROBIOLOGIST MEDICAL DIRECTOR, INFECTION PREVENTION SERVICE HUNTER NEW ENGLAND HEALTH (NSW)
Transcript of How can we control VRE?
How can we control VRE? ACIPC plenary presentation November 2021
J O H N F E R G U S O N
I N F E C T I O U S D I S E A S E S P H Y S I C I A N & M I C R O B I O L O G I S T
M E D I C A L D I R E C T O R , I N F E C T I O N P R E V E N T I O N S E R V I C E
H U N T E R N E W E N G L A N D H E A LT H ( N S W )

Our IPC team

No disclosures
HNE LHD: 1 tertiary and 6 district hospitals, 40 smaller facilities; population circa 1 million; 130,000 km^2 = size of England

John Hunter Hospital (JHH)- Newcastle
800 bed adult and paediatric facility – opened 1991; 37 bed ICU, 42 bed neonatal ICU
3 x FTE Infection Prevention & Control Consultants until COVID-19 (currently 4)

HNE approach to MRO surveillance
Selective MRSA, VRE or CPE screening:◦ ICU – admission and discharge screening done since 2008◦ No general admission screening for VRE◦ Cohort screening performed – 4 bed bay exposure > 48 hrs
All new patient detections of are categorised by healthcare status: ◦ Hospital onset (48 hour rule) ◦ HACO (healthcare-associated community onset) ◦ Community-associated
Healthcare Epidemiologist on staff (S Munnoch and N Fraser)

HNE: VRE timeline
Mahony-AA et al. Vancomycin-resistant vanB Enterococcus faecium sequence type 796 - rapid international dissemination of a new epidemic clone. Antimicrobial Resistance and Infection Control (2018) 7:44 Van Hal- SJ et al. Relentless spread and adaptation of non-typeable vanA vancomycin-resistant Enterococcus faecium: a genome-wide investigation. J Antimicrobial Chemotherapy, 2018.

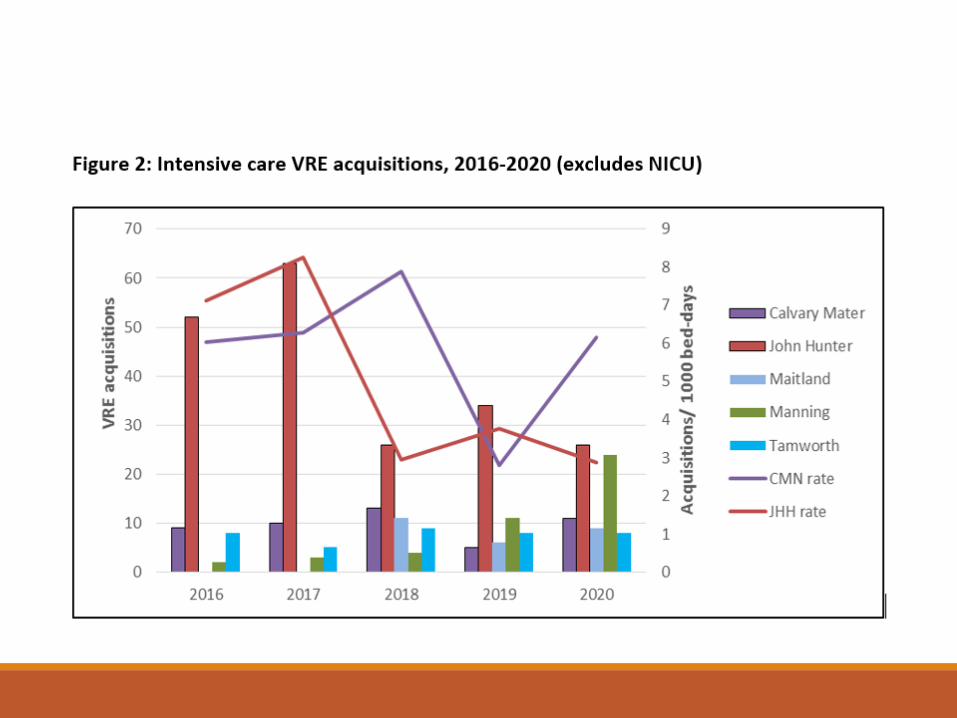
JHH: endemic VRE Situation 2016-2017
Genotypes:
VanA 301 (25% ICU)
VanB 151 (26% ICU)
Acquisition rate: 0.29% of separations
Clinical samples (morbidity):
Bloodstream 15 (vanA x 12)
= 0.28/10,000 patient-days
Other sterile site 31
Urine sample 77
Virtually all healthcare-associated events

Endemic VRE – control options 2017 (1)
A dearth of good quality evidence: 9 studies located; 7/9 were in ICU settings; one RCT
No interventional trial evidence supporting surveillance screening, environmental measures, isolation and cohorting (CP) or AMS interventions
Hand hygiene measures associated with significant decrease in VRE acquisition rate - 47% reduction (27-61% CI):
J Antimicrob Chemother 2014; 69: 1185–1192

JHH: Hand hygiene compliance vs SABSI
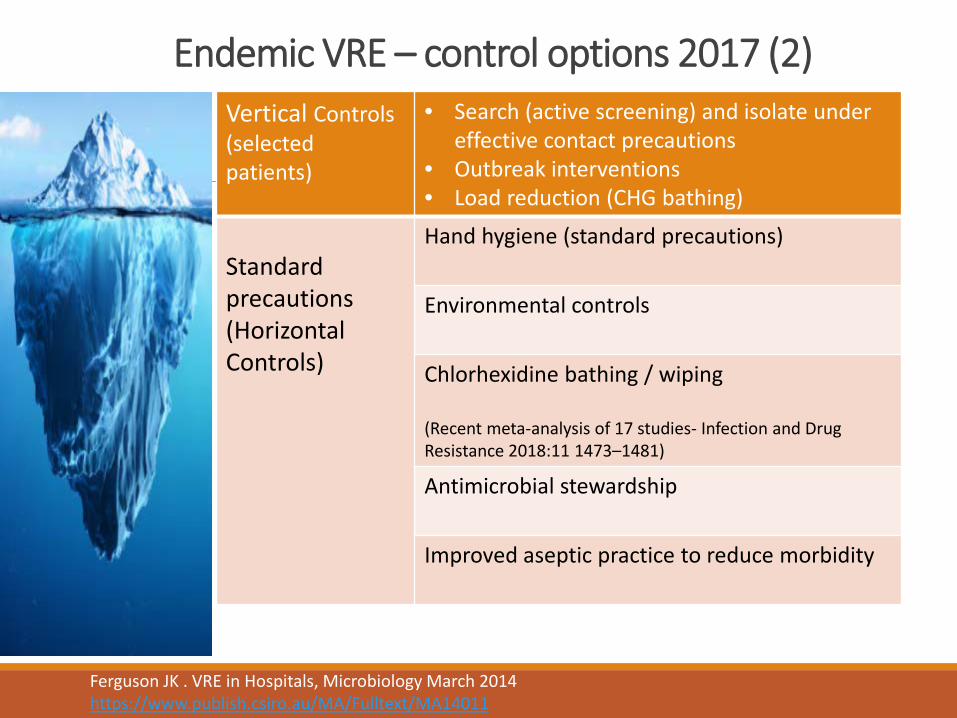
Endemic VRE – control options 2017 (2)Vertical Controls (selectedpatients)
• Search (active screening) and isolate under effective contact precautions
• Outbreak interventions • Load reduction (CHG bathing)
Standard precautions (Horizontal Controls)
Hand hygiene (standard precautions)
Environmental controls
Chlorhexidine bathing / wiping
(Recent meta-analysis of 17 studies- Infection and Drug Resistance 2018:11 1473–1481)
Antimicrobial stewardship
Improved aseptic practice to reduce morbidity
Ferguson JK . VRE in Hospitals, Microbiology March 2014 https://www.publish.csiro.au/MA/Fulltext/MA14011

d
Kleyman et al. AJIC, 2021 49: 784-791
Conclusions:
There was no significant difference in rates of hospital-associated MRSA infection before and after removing CPs.
Additionally, there were decreased rates of hospital-associated VRE infection following stoppage of CPs.

Why doesn’t MRO screening and isolation work in endemic situations?
Large reservoir of colonised patients; unknown environmental and staff reservoirs
In the absence of admission screening, undisclosed patient carriers predominate– e.g.
- John Hunter : percent of new detections that are clinical isolates 29% at JHH; c.f. Intensive care where 8% are clinical isolates (admission and discharge screening occurs)
- Alfred Hospital: VRE Point Prevalence study (Karki et al. 2012) 46 of 58 (79%) patients found to be VRE colonised were previously unknown
i.e. Majority of VRE colonised patients are being managed under standard precautions
MRSA, ESBL: similar situation- large admitted burden of colonised patients in many regions

The environment and MRO acquisition risk
1. Conventional cleaning and disinfection of MRO rooms does not eradicate the risk
2. Environmental disinfection – should it be part of standard precautions?
3. Is there a role for advanced methods (UVC, hydrogen peroxide vapour systems)?
Mitchell BG et al JHI 2015 Risk of organism acquisition from prior room occupants: a systematic review and meta-analysis

REACH: landmark study at 11 Australian hospitals
REACH cleaning bundle, a multimodal intervention, focusing on optimising product use, technique, staff training, auditing with feedback, and communication, for routine cleaning.
After the intervention, vancomycin-resistant enterococci infections reduced from 0·35 to 0·22 per 10,000 occupied bed-days (relative risk 0·63, 95% CI 0·41-0·97, p=0·034)
Farrington A, Mitchell BG et al 6 published papers to date! https://pubmed.ncbi.nlm.nih.gov/?term=reach+mitchell-bg+farrington&sort=date
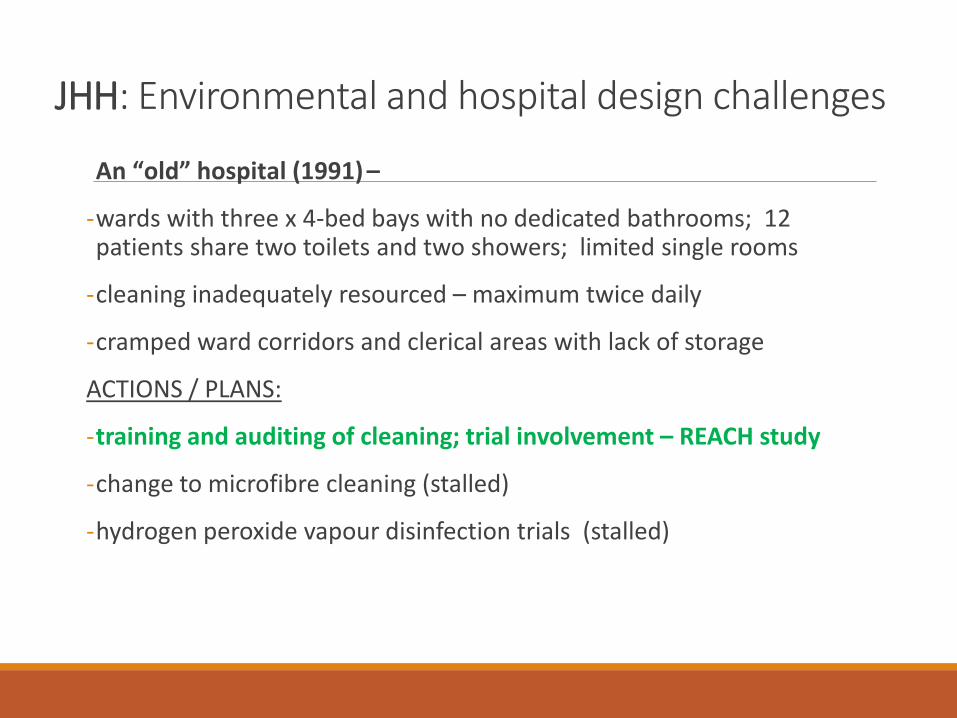
JHH: Environmental and hospital design challenges
An “old” hospital (1991) –
-wards with three x 4-bed bays with no dedicated bathrooms; 12 patients share two toilets and two showers; limited single rooms
-cleaning inadequately resourced – maximum twice daily
-cramped ward corridors and clerical areas with lack of storage
ACTIONS / PLANS:
-training and auditing of cleaning; trial involvement – REACH study
-change to microfibre cleaning (stalled)
-hydrogen peroxide vapour disinfection trials (stalled)
The role of antibiotic stewardship

Impact of integrated AMS program in Scotland
Mixed persuasive and restrictive approach
Aimed to reduce the ‘4C’ antibiotics associated with the emergence of virulent C. difficile in the UK Cephalosporins, “Coamoxyclav”, Ciprofloxacin and Clindamycin
Hospital usage – 47% reduction in target a/b
Community antibiotic use – 30% reduction
Prior infection control interventions documented
Lancet Infect Dis 2017; 17: 194–206
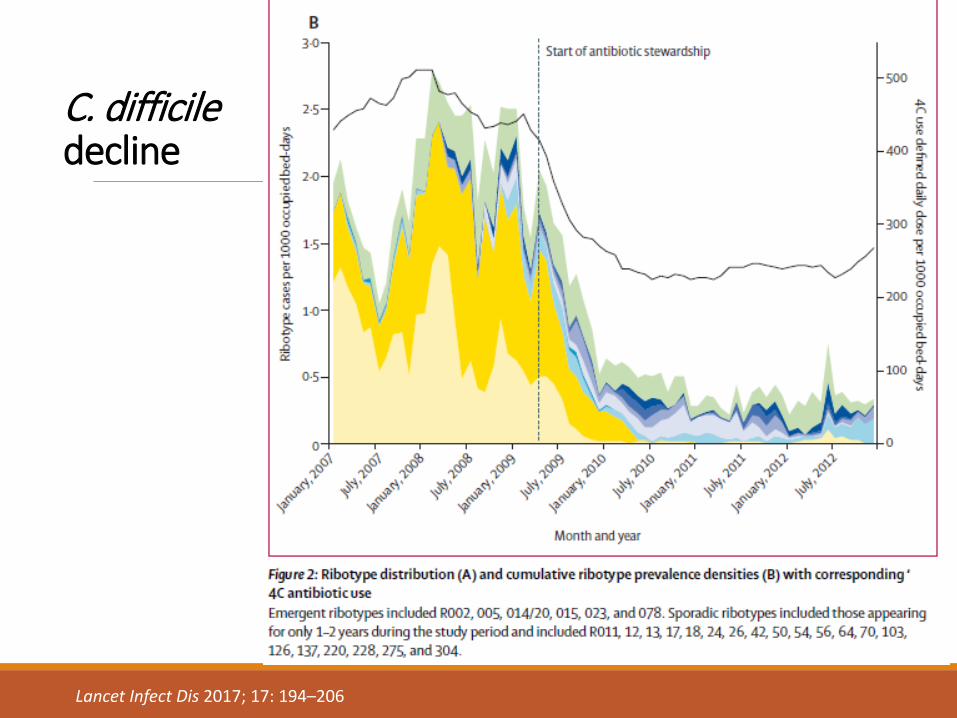
C. difficile decline
Lancet Infect Dis 2017; 17: 194–206
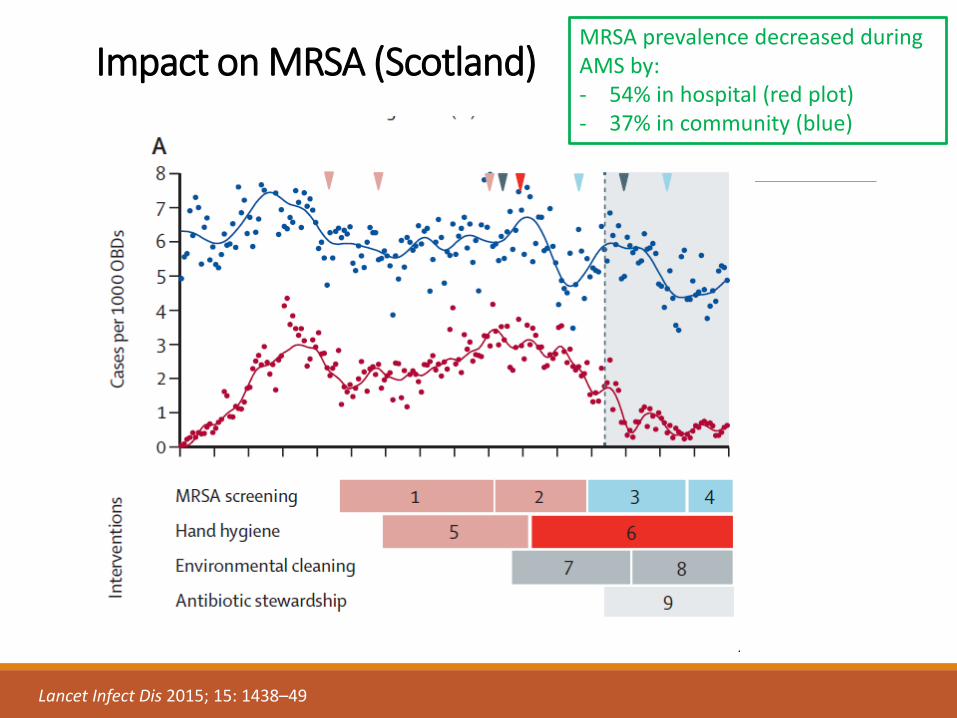
Impact on MRSA (Scotland)
Lancet Infect Dis 2015; 15: 1438–49
MRSA prevalence decreased during AMS by:- 54% in hospital (red plot) - 37% in community (blue)
JHH: a natural AMS experiment …
Explosion in Chinese factory in 2016 led to a global shortage of piperacillin+tazobactam (PT), affecting Australia from Sep 2017
John Hunter Hospital prepared for the PT shortage by:◦ Guidelines amended with inclusion of role for IV augmentin (available
from 2017); avoidance of ceftriaxone or meropenem alternatives◦ Short course intra-abdominal sepsis guideline ◦ Diabetic and vascular foot infection guideline
◦ Piperacillin+tazobactam access restricted◦ General advice sheet provided to clinicians
https://aimed.net.au/2017/06/09/piperacillintazobactam-shortage-recommended-alternatives-hnelhd/

JHH: Sept 2017 - falling off a cliff…
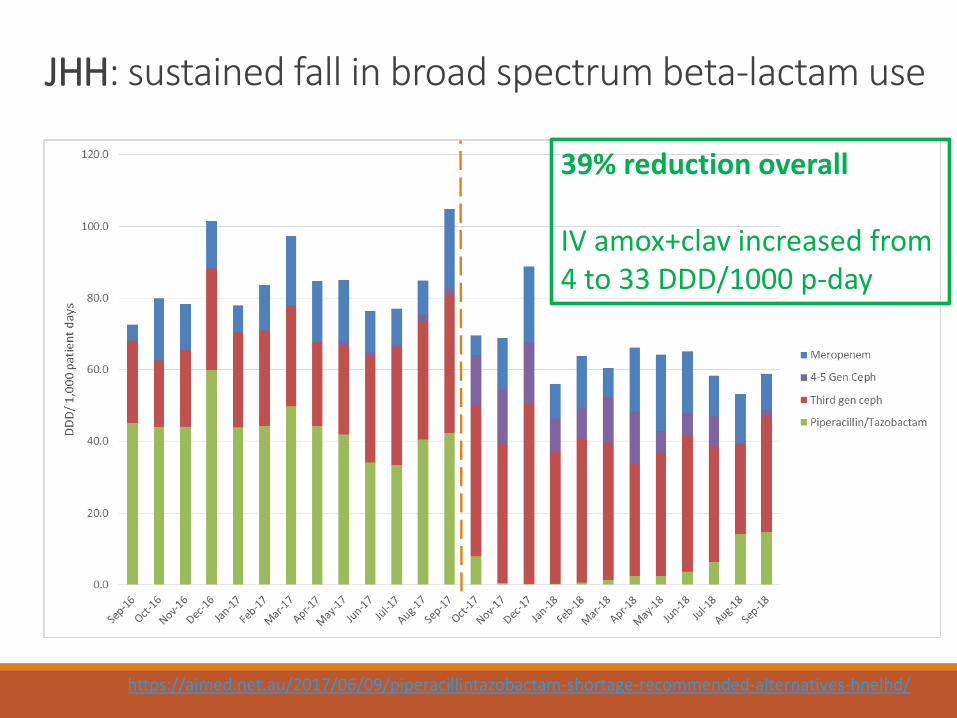
JHH: sustained fall in broad spectrum beta-lactam use
39% reduction overall
IV amox+clav increased from 4 to 33 DDD/1000 p-day
https://aimed.net.au/2017/06/09/piperacillintazobactam-shortage-recommended-alternatives-hnelhd/
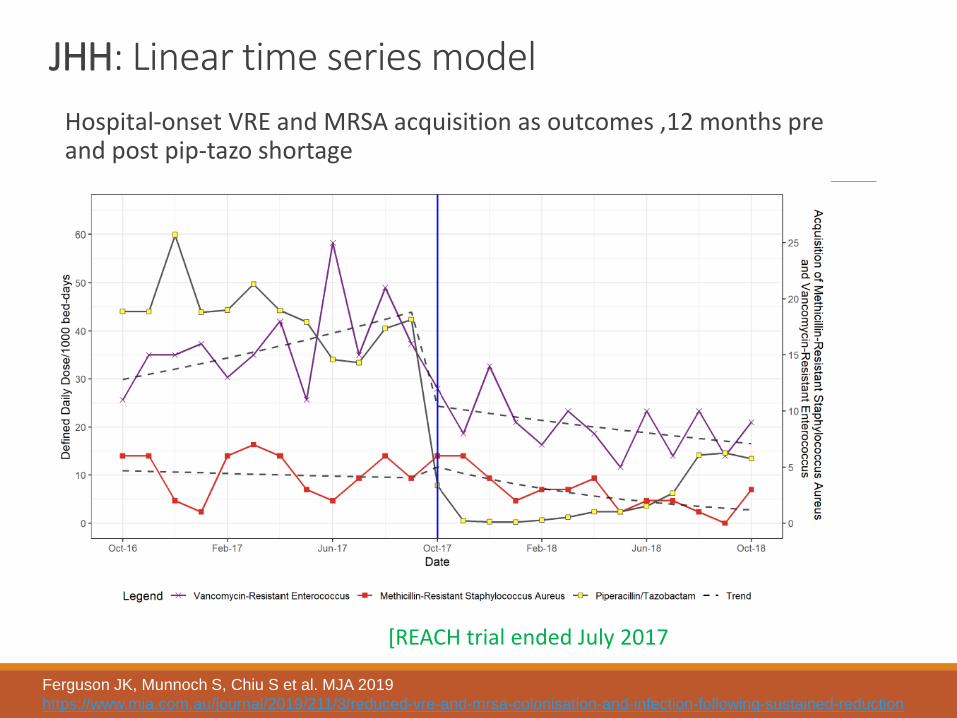
JHH: Linear time series model Hospital-onset VRE and MRSA acquisition as outcomes ,12 months pre and post pip-tazo shortage
Ferguson JK, Munnoch S, Chiu S et al. MJA 2019https://www.mja.com.au/journal/2019/211/3/reduced-vre-and-mrsa-colonisation-and-infection-following-sustained-reduction
[REACH trial ended July 2017

JHH results: MRO acquisitions and infectionsSignificant change in VRE level
(p=0.004) and trend (p=0.002) after October 2017
Ferguson JK, Munnoch S, Chiu S et al. MJA 2019https://www.mja.com.au/journal/2019/211/3/reduced-vre-and-mrsa-colonisation-and-infection-following-sustained-reduction

JHH experiment: Why was it so? Were there significant confounders?
New antiseptic wipe introduced sequentially to the hospital from February 2018
Hand hygiene rates remained above 90% across both periods
No change to hospital activity or test utilisation
Some return in VRE in December 2018 in the main ICU where pip/tazo usage increased to some extent

JHH experiment: Why was it so? Was it replacement with agents less likely to have a sustained impact on gut microbiota and colonization resistance?
◦ Ceftriaxone and pip/tazo have a sustained impacts on gut microbiota diversity ; both are heavily excreted to bile
◦ Le Guern et al: Exposure to agents with wide anaerobic spectrum is associated with high density MRO colonization and reduced microbiota resilience (murine models)
◦ Amoxycllin+clavulanate (augmentin): ◦ less impact on microbiota and colonization resistance◦ HOWEVER – has similar anaerobic action◦ BUT – low biliary excretion into gut
Le Guern et al. Colonization resistance to MDRO – narrative review JHI 2021 118: 48-58

Are there more instructive waysto examine AMU/AMR Data?
Yes! Non linear modelling can examine retrospective time series data
MARS (multivariate adaptive regression splines) regression technique models nonlinearities and interactions between variables. No pre-determined relationship between predictors and the dependent variable is assumed.
López-Lozano JM et al Nature Microbiology A nonlinear time-series analysis approach to identify thresholds in associations between population antibiotic use and rates of resistance https://en.wikipedia.org/wiki/Multivariate_adaptive_regression_spline

Scenario 1: NL-TSA Carbapenem-R Acinetobacter baumannii and antibiotic use (Spain)
López-Lozano JM et al Nature Microbiology
Model best-fit R2 = 0.86
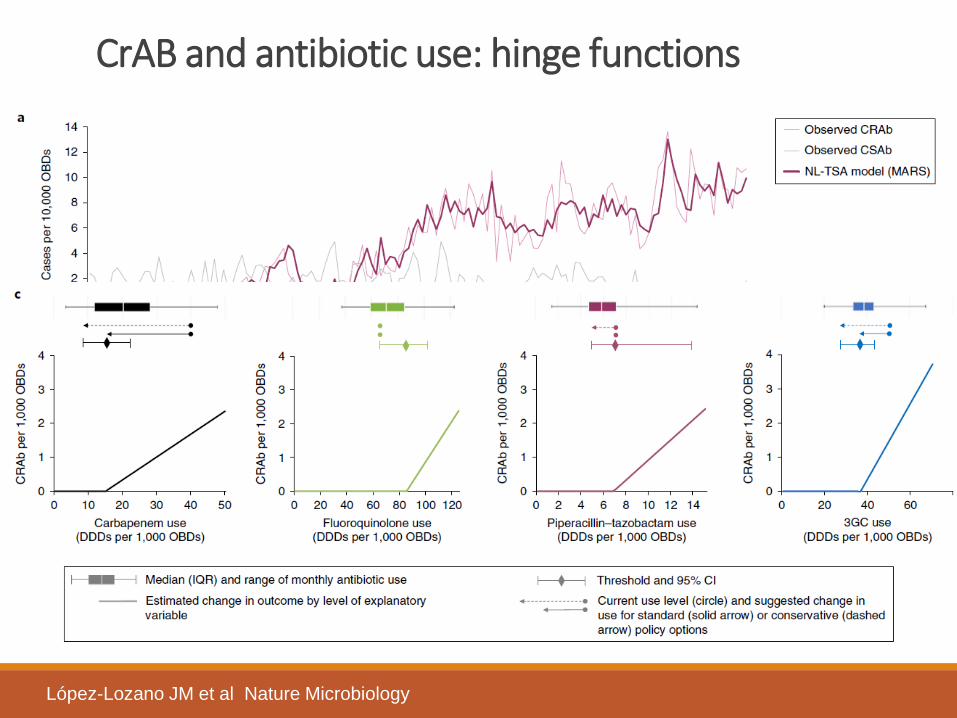
CrAB and antibiotic use: hinge functions
López-Lozano JM et al Nature Microbiology

Scenario 5: NL-TSA MRSA, hand hygiene and antibiotic use (N Ireland)
(Best fit model R2 = 0.56)
López-Lozano JM et al Nature Microbiology
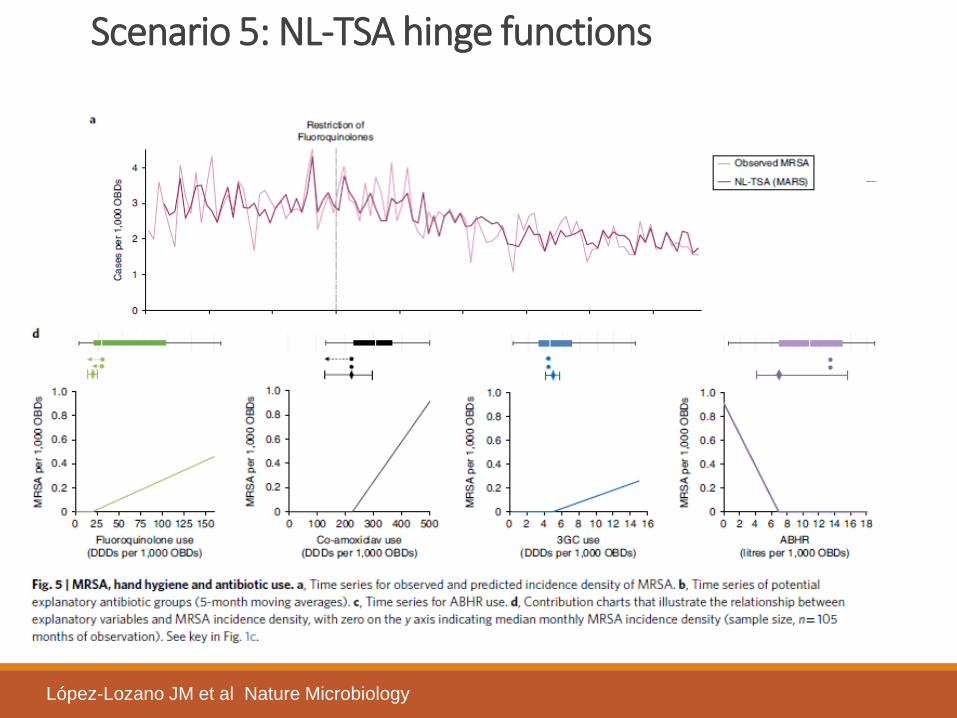
Scenario 5: NL-TSA hinge functions
López-Lozano JM et al Nature Microbiology
JHH: Applying non linear time series analysis
Longer time series: 2015-March 2020 (pre COVID19!)
Primary outcome: hospital-onset VRE acquisitions (vanA or vanB)
Independent variables:
- Total antibiotic use (DDD/1000 patient-days)◦ broad spectrum ◦ less broad spectrum (amox/clav, macrolides, metronidazole,
aminoglycosides and glycopeptides)◦ narrow spectrum
- Time lags for each variable to address potential autocorrelations
MARS models identified the most likely predictors and their lags (pre-specified to allow up to 3-way interactions and a maximum of 4 variables). Various diagnostic checks and validation completed.
Chiu S, Oldmeadow C , Hunter Medical Research Institute

JHH Model 1: Aggregate antibiotics
Broad spectrum antibiotic Threshold153 DDD/1000 patient-days per month (95%CI 113, 177)
EffectVRE is expected to increase onset by 1.0% for every DDD above threshold
Chiu S, Oldmeadow C , Hunter Medical Research Institute

JHH Model 2: Broad spectrum category
Piperacillin/tazobactam Threshold17.4 DDD-per-1000 patient-days (95%CI: 13.4, 20.5).
EffectVRE is expected to increase onset by 1.8% for every DDD above threshold
Chiu S, Oldmeadow C , Hunter Medical Research Institute

What happened elsewhere?
Diverse changes to pip/tazousage during and after shortage by State
All State averages well above JHH VRE harm threshold of 17.4 DDD/1000 patient-days
NAUSP Report March 2021 https://www.safetyandquality.gov.au/sites/default/files/2021-03/report_-_2019_nausp_-_key_findings_-_11_mar_2021.pdf

In summary: Where to with VRE IPC? Vertical Screening and
isolation under CPShould it be abandoned in most endemic settings?
Horizontal Hand hygiene Remains an essential control strategy
Environmental controls
Implement REACH bundle in standards and practiceFurther research: advanced techniques for disinfectionImprove hospital design
Chlorhexidine bathing
What is its role relative to other measures?
Antimicrobial stewardship
Analyses of thresholds and case control data can provide objective program goals
Research Quality studies that use reliable methods to factor together the impact of different control elements
http://aimed.net.au HNE AMS site

Thank you!
Acknowledgements :• HNE Infection Prevention Service colleagues, Geoff Deane, Nurse Manager• Hunter Medical Research Institute, Simon Chiu, Chris Oldmeadow, John
Attia• Pathology North, NSW Microbiology Service colleagues, Dr Hema
Varadhan, Director• John Hunter Immunology & Infectious Diseases Department colleagues,
Dr Rob Pickles, Director• European Thresholds Collaborative Group, Jose-Maria Lopez-Lozano,
Convenor