How can we commission alcohol pathways that are fit for purpose? Dr Carsten Grimm Bradford Districts...
31
How can we commission alcohol pathways that are fit for purpose? Dr Carsten Grimm Bradford Districts CCG Board Member
-
Upload
robin-mozley -
Category
Documents
-
view
215 -
download
1
Transcript of How can we commission alcohol pathways that are fit for purpose? Dr Carsten Grimm Bradford Districts...

How can we commission alcohol pathways that are fit for purpose?
Dr Carsten GrimmBradford Districts CCG Board Member

Declaration of Interest
Current roles and affiliations
• Clinical Lead Alcohol Services Locala (former Kirklees Community Health Services, NHS provider arm)
• Cluster Lead Alcohol Misuse and Gambling Certificates, RCGP England
• RCGP Clinical Commissioning Champion
• Associate IHWB UK
Honoraria
• Turning Point• Lundbeck• BayerSchering• KJ Physiotherapy & Medical Consultancy
Ltd• RCGP England• Doctors.net UK• Richmond Pharmacology• Pfizer• NHS via various primary and secondary
care trusts• LMC Bradford & Airedale Ltd


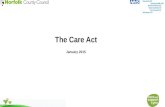
Gable, R. S. (2006). Acute toxicity of drugs versus regulatory status. In J. M. Fish (Ed.),Drugs and Society: U.S. Public Policy, pp.149-162, Lanham, MD: Rowman & Littlefield Publishers



“It is also very important that the recommendations are not just aimed at young binge drinkers, but at the silent majority of heavy drinkers whose drinking puts them at risk of serious damage to their health.”Ian Gilmore


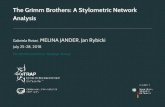
Alcohol consumption and liver disease in Europe 1970 - 2000
Adapted from Mayhew L & Lee B. ActivAge Project HPSE-CT-2002-00102. 2005; 77. http://www.iccr-international.org/activage/docs/ActivAge-WP4-SynthesisReport.pdf

Can we change society?

The Resource Legend of the NHS
• There is no money• There is no staff• Clinicians are expensive

The Bradford Model
- £1.2m pa- Four elements (PCAS, PCDS, polish drinkers,
top up of hospital liaison team)- In addition to Bradford CDAT- Lifeline and Project 6

The Kirklees Model
• £1m pa• Three partners• Lifeline, Locala, Community Links• Strong links into shared care• Locality model and remaining main service

How to commission the perfect pathway

You don’t!
• Pathways are operational• Need to be able to adjust to local need• Lead provider model or Accountable Care
Organisations must have flexibility to create their own
• Look at what works – smoking cessation!


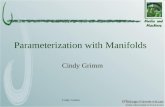
No intervention
Brief intervention
Treatment in primary c.
Disorder Severity
How to measure outcomes
• PbR• Audit-O• Reduction in hospital admissions• Reduction in liver disease

Public Health Tendering Model
• Part of Local Authority• Must retender every 5 years• Intrinsic preference to “lowest possible bidder”• Lack of clinical input

Translation into service model
• Downshift to minimum qualified staff• Abandonment of principle of Clinical
Leadership• Upshift of responsibilities

What is the problem?
A 2010 survey of GPs showed the following barriers to alcohol screening and intervention:• Lack of time• Inadequate training• No incentives in the current contract• Worries about cost and availability of alcohol services• The perceived normality of heavy drinking amongst health
professionals

What works• Primary care based services• Organic growth with long term commitment
(5-10 years)• Link to CVD risk• Shared care & clinically led service• Housing support• Peer led groups

• Link with liver (yet)• Link with dementia• PH commissioned clinical service• Link with illicit drugs agenda• Tiered (1-4) approach to diagnosis and service
commissioning• Piecemeal commissioning
What doesn’t work

Computers are rubbish…

…that’s why kids use them all the time.




Google “RCGP alcohol”Quarterly National Training Days in LondonLocal Training Days available

Summary• The majority of people with alcohol use
disorder can be treated in primary care• Primary care is arguably best placed to bridge
the gap between physical health need management, accessibility and specialist treatment options
• Look at the CCGs now – it is an issue for hospitals