Laurel K. Leslie, MD, MPH Thomas I. Mackie, MPH, MA Justeen Hyde, PhD Christopher Bellonci, MD
Upload
charla-kellyCategory
view
214download
3
1
Hot Topics in Health Care
Drew Alexander, MDJohn Kulig, MD, MPH
Sara Mackenzie, MD, MPHGary Strokosch, MD
November 18, 2010

2
Learning Objectives
As a result of this presentation, participants will:• Implement a comprehensive influenza immunization program
for all students and staff on center in accord with current CDC recommendations
• Obtain Pap testing only if indicated by current national guidelines
• Prescribe and monitor student medications for attention deficit hyperactivity disorder (ADHD)
• Counsel students regarding the risks associated with frequent use of “energy drinks”
• Offer optional human papillomavirus immunization for both female and male Job Corps students
• Recognize students with signs and symptoms of eating disorders

3
Influenza 2010-2011
John Kulig, MD, MPHLead Medical Specialist
Job Corps

4
Influenza
• 20% of US population infected with influenza virus annually
• 200,000 hospitalizations annually• 20,000 deaths annually• Mortality risk greatest among infants
and elderly• Large economic cost in work
absenteeism and productivity loss
5
6
Influenza Vaccine
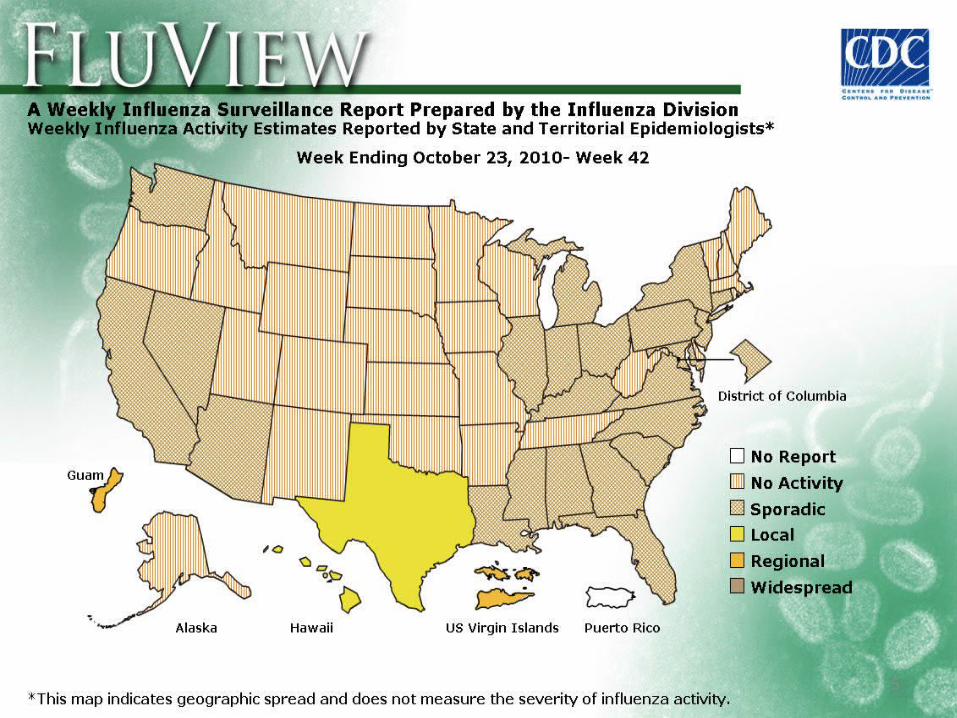
• The seasonal influenza vaccine protects against the three main flu strains that research indicates will cause the most illness during the flu season.
• Influenza vaccine for the 2010-2011 season contains three influenza virus strains: an A/California/7/09 (H1N1)-like virus; an A/Perth/16/2009 (H3N2)-like virus; and a B/Brisbane/60/2008-like virus.
7
Influenza Vaccine
• CDC recommendations for seasonal influenza vaccination during the 2010-11 season include “universal” annual vaccination for everyone age 6 months and older in the US.
• While everyone should get flu vaccine each flu season, it’s especially important that high risk groups get vaccinated.
8
High Risk Groups• Pregnant women • Children younger than 5, but especially children younger than 2
years old• People 50 years of age and older • People of any age with certain chronic medical conditions • People who live in nursing homes and other long-term care
facilities • People who live with or care for those at high risk for complications
from flu, including: – Health care workers – Household contacts of persons at high risk for complications
from the flu – Household contacts and out of home caregivers of children
less than 6 months of age (these children are too young to be vaccinated)
9
Job Corps Policy
Information Notice 10-28• Job Corps centers should offer seasonal influenza vaccine on a
voluntary basis to all students, not just to students with health conditions placing them at higher risk of medical complications.
• One dose of seasonal flu vaccine should be administered as early as September. Early administration of flu vaccine (September) is not associated with loss of protection, and late administration of flu vaccine (March) still affords protection as cases of seasonal flu often peak in late winter.
• Injectable vaccine (trivalent inactivated vaccine or TIV) or nasal spray vaccine (live attenuated influenza vaccine or LAIV) may be administered, but nasal spray vaccine should not be administered to pregnant or immunocompromised students.

10
Job Corps Policy
Information Notice 10-28• Centers may wish to offer influenza vaccine administration to
students in alternate locations, such as the cafeteria during the lunch break or the dormitories after hours, to increase voluntary participation.
• Influenza vaccine should remain available on center throughout the flu season for new students and for students who may initially decline to be immunized.
• Influenza vaccination is strongly encouraged for all center health staff members, who could potentially transmit infection to students. Increased absenteeism among health staff could also reduce the capacity of a center to respond to increased demand for care in the event of an influenza outbreak on center.

11
EducationJob Corps centers are encouraged to share with students and staff the following tips for controlling the spread ofinfluenza on center: • Cover your nose and mouth with a tissue when you cough or
sneeze. Throw the tissue in the trash after use. • Wash your hands often with soap and water, especially after
you cough or sneeze. Alcohol-based hand cleaners are also effective.
• Avoid touching your eyes, nose, or mouth. Germs spread that way.
• Try to avoid close contact with sick people. • Encourage residential students to report to the Wellness
Center if they become ill. Sick nonresidential students and staff should be encouraged to stay home and limit contact with others.
12
Testing and Treatment
• Centers should not stockpile diagnostic materials or antiviral medications for influenza, and should only conduct diagnostic testing and begin antiviral treatment or prophylaxis based upon specific recommendations from the state or local health department.

13
Reporting
• Centers should continue to use the Significant Incident Report (SIR) system to keep the National and Regional Offices of Job Corps informed about epidemic influenza on center.
• For the purpose of reporting, epidemic influenza will be defined by Job Corps as cases affecting 10% or more of on board strength (OBS).

14
CDC Resources
• http://www.cdc.gov/flu/ - influenza overview
• http://www.cdc.gov/flu/professionals/index.htm - information for health professionals
• http://www.cdc.gov/flu/freeresources/index.htm - free influenza resources to download

15
Pap Testing
Gary Strokosch, MDMedical Specialist
Job Corps

16
Pelvic Exams and Pap Smears
A. When to Perform a Pelvic Exam and PapB. Which Pap Technique to UseC. Reflex Testing for HPVD. How to Manage Abnormal Pap Smears
A. American Cancer SocietyCervical Cancer Screening
Recommendations
18
Cervical Cancer Screening Recommendations
• Pre-1980 American Cancer Society Cervical Cancer Screening Recommendation– no reference to age– as part of a regular check-up

19
Cervical Cancer Screening Recommendations
• 1980-1987 American Cancer Society Cervical Cancer Screening Recommendation– Over 20– But, under 20 if sexually active– Yearly, but after 2 negative exams 1 year
apart, at least every 3 years

20
Cervical Cancer Screening Recommendations
• 1987-2002 American Cancer Society Cervical Cancer Screening Recommendation– 18 and over– or sexually active– Yearly, but after 3 consecutive normal
exams, less frequently at the discretion of the doctor

21
Cervical Cancer Screening Recommendations
• 2003 – Present American Cancer Society Cervical Cancer Screening– Start 3 years after first vaginal intercourse
but no later than 21– Yearly with conventional Pap or every 2
years with liquid-based Pap

It is expected that the American Cancer Society
will soon change their recommendations for
cervical cancer screening

23
ACOG
The American College ofObstetricians and Gynecologists
24
ACOG Recommendations 2003-2009
• Practice Bulletin No. 45, August 2003
• Similar to 2003 ACS recommendations

25
ACOG Revised RecommendationsNovember 20, 2009
• Women should have their first cancer screening at age 21
• Women from 21 to 30 should be screened every two years instead of annually using either conventional Pap or liquid-based cytology

26
Basis of ACOG Revised Recommendations
• Although the rate of HPV infection is high among sexually active adolescents, invasive cervical cancer is very rare.
• The immune system clears the HPV infection within 1-2 years among most adolescent women.

27
Basis of ACOG Revised Recommendations
• The adolescent cervix is immature and there is a higher incidence of HPV-related precancerous lesions, but the large majority of cervical dysplasias in adolescents resolve on their own.
• A significant increase in premature births has recently been documented among women who have been treated with excisional procedures for dysplasia.
28
Basis of ACOG Revised Recommendations
• Adolescents have most of their childbearing years ahead of them and should avoid unnecessary procedures that negatively affect the cervix.
• Screening for cervical cancer in adolescents only services to increase their anxiety and has led to overuse of follow-up procedures for something that usually resolves on its own.

29
PRH Change Notice 09-20March 2, 2010
• Pap Smears obtained from all females ≥ 21 yrs (unless documented Pap smear results within 24 mos before arrival)
• Completed within 14 days after arrival
• Students < 21 yrs only require pelvic/speculum exam for clinical indications such as pelvic pain, vaginitis, menstrual disorders, pregnancy, etc.

B. LIQUID-BASEDCYTOLOGY REPLACINGCONVENTIONAL PAPS
Two FDA approved productsThinPrep since 1996SurePath since 1999

31
Techniques ofCervical Cytology
• Both liquid-based and conventional methods are acceptable for screening.
• The majority of screening in the U.S. is liquid-based (90% of OBGYNs in 2003).
• Lubricant will interfere with transfer of cells in both methods.
• Most contaminating blood and discharge are filtered out with liquid-based technique.

32
Techniques of Cervical Cytology
• There is conflicting evidence whether or not the two methods are comparable.
• Liquid-based is more expensive.
• Liquid-based allows for simpler reflex testing.

C. Reflex HPV TestingFDA approved in 2000
• Assesses exfoliated cervical cells for the presence of 1 or more of 13-14 of the 15-18 potentially cancer causing HPV types.
• There are two FDA approved products.• Most commonly performed on liquid-based
specimen.• Should not be used for females < 21 yrs.

34
Terminology2001 Bethesda System
• ASC-US: atypical squamous cells of undetermined significance reflex testing
• LSIL: low-grade squamous intraepithelial lesion (mild dysplasia / CIN 1)
• HSIL: high-grade squamous intraepithelial lesion (moderate & severe dysplasia / CIN 2 & 3)

35
Rx ofAbnormalPap SmearsIn Women≤ 20 yrs old
≤ 20 yrs
ASCUS/LSIL
12 mos retest:ASCUS/LSIL
12 mos retest:negative
Resumenormaltesting
12 mos retest:ASCUS/LSIL/HSIL
Culposcopy
12 mos retest:HSIL
Culposcopy
HSIL
Culposcopy
ASCCP 2006ConsensusGuidelines

36
≥ 21 yrs
ASCUS
6 mos retest:negative
6 mos retest:negative
Resumenormaltesting
6 mos retest:ASCUS/LSIL/HSIL
Culposcopy
6 mos retest:ASCUS/LSIL/HSIL
Culposcopy
LSIL/HSIL
Culposcopy
Rx ofAbnormalPap SmearsIn Women≥ 21 yrs old
ASCCP 2006ConsensusGuidelines

37
≥ 21 yrsASCUS
HPVnegative
Repeatin 12 mos
HPVpositive
Colposcopy
ASCCP 2006ConsensusGuidelines
ASCUS Reflex HPV Testing(Not Recommended for ≤ 20)
References
• Job Corps PRH-6: 6.10, R1• PRH Change Notice No. 09-20• American College of Obstetricians and
Gynecologists (www.acog.org) • American Society for Culposcopy and
Cervical Pathology (www.asccp.org)

39
Attention Deficit Disorder (ADD) and Attention Deficit Hyperactive Disorder
(ADHD)
Drew Alexander, MDMedical Specialist
Job Corps
40
Inheritance of ADD/ADHD:Is the Disorder Real?
• 25-35% if sibling has ADD
• 20-54% if parent has ADD
• 78-82% if identical twin has ADD
• Ongoing research attempts to isolate alleles
41
Conditions Potentially Leading to ADD
• Genetic variable penetrance
• Fetal Exposure to smoking, alcohol, trauma
• Prematurity
• Post natal head and other trauma
42
Core ADD Symptoms
• Inattention
• Lack of focus
• Easy distraction

43
Ancillary ADHD Symptoms
• Hyperactivity• Impulsivity• Disruption
• Altered judgment• Affect differences• Mood differences

44
Current Types of ADD/ADHD
• Inattentive (quiet/often noted in females)
• Impulsive (disruptive/often noted in males)
• Combined type
• Mood and affect disorders associated with attention are not clearly typed
45
Treatment Modalities
• Remediation of deficits
• Academic, vocational and life coaching (reconfiguring less effective coping styles)
• Pharmacology

46
Current Pharmacology
• Dopamine enhanced neuro-transmission
• Norepinephrine enhanced neuro-transmission
• Serotonin enhanced neuro-transmission

47
Dopamine
• Methlyphenidate and amphetamine salts (generic)
• Ritalin IR and Adderall IR (brand names)
• Once a day dosing preferred (multiple products)

48
Norepinephrine
• Generic
• Strattera and Intuniv (Brand Name)
• Once a day dosing preferred but twice daily an option for Strattera

49
Serotonin
• SSRI is the class of medication• FDA approves SSRIs for depression • SSRIs help some conditions of
inattention• 1986, Prozac is marketed as the first
SSRI• Many generics and brands are now
available

50
Medication Combinations• Given the specificity of targeting neuro-
transmiters combining these meds is effective
• Commonly for mood, affect and behavior, disorders serotonin enhancers are used first
• When inattention surfaces alone or persists after the serotonin enhancer dopamine is used
• Norepinephrine enhancers are added to either of the above meds when indicated

51
Summary• ADD/ADHD is a chemical/physiologic disorder
• Core symptoms include inattention, easy distraction and poor focus
• Ancillary symptoms include hyperactivity, impulsivity and behavior disorders
• Three treatment options are available
• Three class of medications are available for the treatment of attention disorders
• Mono or combined therapy may be effective

52
Energy Drinks: The Acceptable Stimulant?
Sara Mackenzie, MD, MPHMedical Specialist
Job Corps

53
How many of you had your cup of coffee this morning?

54
Energy Drinks
• Heavily promoted to adolescents and young adults
• 35 to 45 percent adolescents and young adults report drinking them
• Fastest growing sector of the beverage industry
• Red bull• Full throttle• Rock star• Vault• Jolt• Go Girl• Rip it chic• Sobe No Fear…

55
What Are They?
• No clear definition• Refers to beverage
designed to “boost” energy
• Main component- Caffeine 34 mg
75 mg
80 to >500 mg

56
Food and Drug Administration
• FDA recommends drinks contain no more than 65 mg per 12 ounces
• However, FDA does not have regulatory control over energy drinks
• Energy drinks = “dietary supplements”
• Cannot require disclosure of caffeine content

57
We All Drink It. What’s the Problem?
• Caffeine considered safe at low dose (<3mg per kg body weight) – alert, increase energy, increased sociability
• Risk at high dose (>3 mg per kg body weight)– anxiety, jittery, upset stomach, headaches,
flushed face, difficulty sleeping, dehydration, racing heart, increase BP, arrhythmia
• EVEN reports of seizure, stroke, heart attack, and death
58
Caffeine Risk
• Dose dependent
• Adolescent and young adults may have greater risk due to less tolerance
• Associated with other risk taking behaviors: tobacco, alcohol, non-medical prescription drugs, lack of seat belts, sexual risk taking… a gateway drug??

59
What Can You Do?
• Think about caffeine• Ask about caffeine intake (soda, energy
drinks, energy pills, coffee…)• Explore what they see as benefit• Assess for harmful effects (sleep,
anxiety, headaches, heart rate, blood pressure…)
• Encourage abstinence• REDUCE CAFFEINE ON CAMPUS

60

61
4 LOKO• 23.5 ounce can – fruit punch, orange blend,
grape, watermelon, lemonade…• Cost =$2.50• Ranks 4th leading sales growth for alcoholic
beverages at 7-11• 12% alcohol – each can is the equivalent to 4
beers• Caffeine• Guarana• Taurine
62
The Wide Awake Drunk!
• Caffeine = stimulant• Alcohol = depressant• Miss warning signs of alcohol-related
intoxication• Increased risk of alcohol-related harm• Consuming energy and alcohol associated
with:– Higher blood alcohol content– 4 fold increase in intent to drive upon leaving
bar
63
ReferencesPennington, N et al. Energy Drinks: A new health hazard for
adolescents. The Journal of School Nursing. 2010 June 10Arria, A.M. et al. Increased alcohol consumption, nonmedical
prescription drug use and illicit drug use are associated with energy drink consumption among college students
Kaminer, Y. et al. Problematic Use of Energy Drinks by Adolescents. Child and Adolescent Psychiatric Clinics. 19(3):643-650
Duchan, E. et al. Energy Drinks: a review of use and safety for athletes. The physician and sports medicine. June 38(2)171-9
Thombs et al. Event level analysis of energy drink consumption and alcohol intoxication in bar patrons. Addictive Behaviors 35 (2010) 325-330

64
Human Papillomavirus Vaccines
John Kulig, MD, MPHLead Medical Specialist
Job Corps

65
Human Papillomavirus (HPV)• The Centers for Disease Control and
Prevention (CDC) estimates that close to 5.5 million new genital HPV infections occur each year and that more than 24 million people in the US are infected with HPV at any given time.
• A recent study conducted by the Kaiser Family Foundation found that 70% of Americans knew nothing about the existence of HPV as a sexually transmitted infection.

66
Infection From Time of First Infection From Time of First Sexual IntercourseSexual Intercourse
From Winer RL, Lee S-K, Hughes JP, Adam DE, Kiviat NB, Koutsky LA. Genital human papillomavirus infection: incidence and risk factors in a cohort of female university students. Am J Epidemiol. 2003;157:218–226. Reprinted with the permission of Oxford University Press.
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56
0
0.2
0.4
0.6
0.8
1Study of female college students (N=603)
Months Since First Intercourse
Cu
mu
lati
ve I
nci
den
ce o
f H
PV
Infe
cti
on

68
HPV Disease Burden: Female
• Genital warts• Cervical cancer• Vulvar cancer• Vaginal cancer• Anal cancer• Head and neck cancers• Recurrent respiratory papillomatosis

69
1.4 million new cases of low-grade cervical dysplasia (CIN 1)2
3,700 estimated deaths1
Estimated Annual Burden of HPV-Related, Diagnoses in the United States, 2006
1 million new cases of genital warts3
330,000 new cases of high-grade cervical dysplasia2
9,710 new cases of cervical cancer1
1. American Cancer Society. Cancer Facts and Figures 2006. Atlanta, Ga: American Cancer Society; 2006:4. 2. Schiffman M et al. Arch Pathol Lab Med. 2003;127:946–949. 3. Fleischer AB et al. Sex Transm Dis. 2001;28:643–647.
CIN = cervical intraepithelial neoplasia.
70
HPV Disease Burden: Male
• Genital warts• Anal cancer• Penile cancer• Head and neck cancers• Recurrent respiratory papillomatosis

71
Genital Warts
Estimated number of new cases per year in the United States1:
1 million
Estimated number of sexually active adults with clinically visible genital warts2:
1 in 100
Estimated number of people who will develop genital warts in their lifetime3:
1 in 101. Fleischer AB et al. Sex Transm Dis. 2001;28:643–647. 2. Koutsky L. Am J Med. 1997;102:3–8. 3. Franco EL et al. In: Franco EL, Monsonego J, eds. New Developments in Cervical Screening and Prevention. Blackwell Science; 1997:14–22.
Estimates include both males and females.

72
Head and Neck Cancers
• Cancers of the head and neck are usually caused by tobacco and alcohol, but recent studies show that about 25% of mouth and 35% of throat cancers are caused by HPV.
• More than 1,700 new cases of HPV-associated head and neck cancers are diagnosed in women and nearly 5,700 are diagnosed in men each year in the US.
• Black people get these cancers more often than people of other races and ethnicities.

73
HPV Vaccines
• HPV L1 major capsid protein of the virus is antigen used for immunization
• Expression of L1 protein uses recombinant technology
• L1 proteins self-assemble into virus-like particles (VLP)
HPV VLP
74
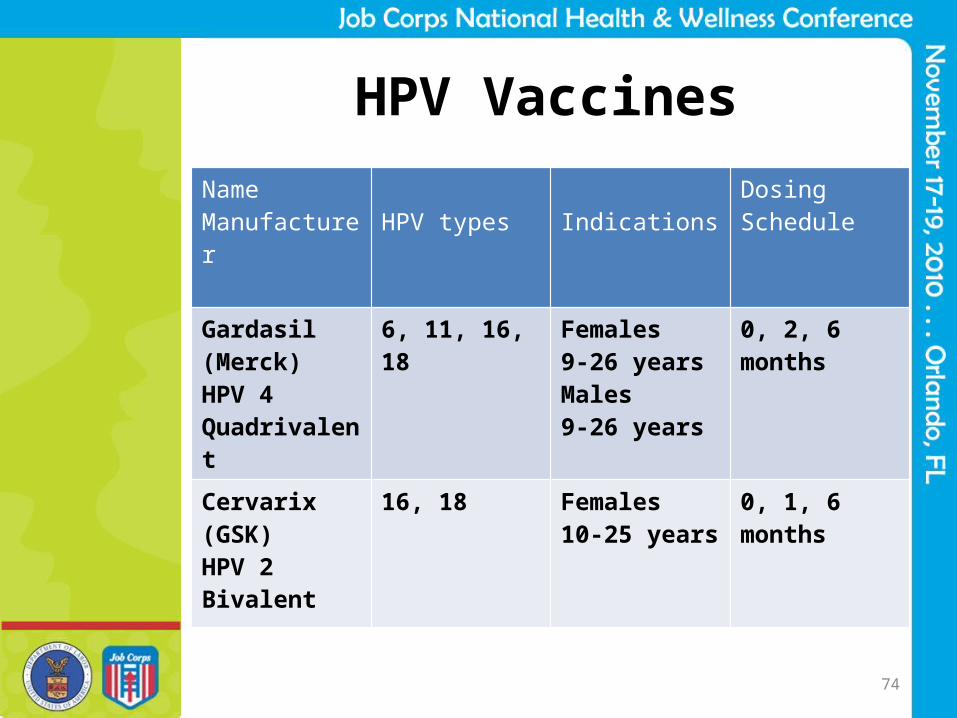
HPV VaccinesName Manufacturer HPV types Indications
DosingSchedule
Gardasil(Merck)HPV 4Quadrivalent
6, 11, 16, 18 Females9-26 yearsMales 9-26 years
0, 2, 6 months
Cervarix(GSK)HPV 2Bivalent
16, 18 Females 10-25 years
0, 1, 6 months

75
HPV Immunization Resources
• Vaccines for Children Program (VFC)http://www.cdc.gov/vaccines/programs/vfc/default.htm
• State and local health departments• Vaccine manufacturers: GlaxoSmithKline http://www.bridgestoaccess.com/
Merck http://www.merck.com/merckhelps/vaccines/home.html
• Partnership for Prescription Assistance http://www.pparx.org/en/prescription_assistance_programs

76
Should Patients be Observed After HPV Immunization?
• Syncopal events post-immunization– 63% occur < 5 min after immunization– 89% occur within 15 min
• “Vaccine providers should consider observing patients for 15 minutes after they receive HPV vaccine.”*
• Consider inquiring about previous syncope and whether patient ate/drank before visit
*ACIP: MMWR 2007; 56(RR-02):1-24

77
Recognize Students with Eating Disorders
Gary Strokosch, MDMedical Specialist
Job Corps
78
--1994-- --2000--
(The next edition to be published in May 2013)
Diagnostic andStatisticalManuel ofMentalDisorders

79
DSM Publication Dates
• History– DSM-I 1952– DSM-II 1968– DSM-III 1980– DSM-III-R 1987– DSM-IV 1994– DSM-IV-TR 2000

80
Eating Disorders in Job Corps

81
Conditions Often Confusedwith Eating Disorders
• Feeding and Eating Disorders of Infancy and Early Childhood–Feeding Disorders (307.59)
–Pica (307.52)
–Rumination Disorder (307.53)

82
Conditions Often Confusedwith Eating Disorders
• Other disorders– Obesity (278.00)
– Binge Eating Disorder (BED)• DSM-IV Appendix B
– Compulsive Overeating• AKA Food Addiction• Similar Definition as BED

83
Two Eating Disorders• Anorexia Nervosa (307.1)
– Restrictive Type (the majority)– Binge-Eating/Purging Type
• Bulimia Nervosa (307.51)– Purging Type (the majority)– Non-purging Type

84
Anorexia Nervosa
• ANOREXIA NERVOSA is characterized by a refusal to maintain a minimally normal body weight.

85
Bulimia Nervosa
• BULIMIA NERVOSA is characterized by repeated episodes of binge eating followed by inappropriate compensatory behaviors.

86
Anorexia Nervosa
Four Diagnostic Criteria• Refusal to maintain normal body
weight• Fear of gaining weight or becoming
fat• Disturbance in the way one’s body
weight or shape is experienced• Amenorrhea
What to watch for in Job Corps

87
Bulimia Nervosa
Five Diagnostic Criteria• Binge eating episodes • Compensatory purging • Bingeing/purging at least twice a
week for three months• Negative self-evaluation via body
weight and shape• Not during episodes of Anorexia
NervosaWhat to watch for in Job Corps
88
Bulimia Nervosa
Compensatory Behaviors
1. Self-induced vomiting * 2. Misuse of laxatives,* diuretics,
enemas, or other medications 3. Fasting4. Excessive exercise

89
Eating Disorders: Equal-Opportunity Diseases
• Mostly adolescent and young adult women.• 5-10% of patients are male.• Found in children as young as 5 years and people
well into their geriatric years.• Found in nearly all ethnic and racial groups when
exposed to Western culture.• Two peak ages of onset: 13 to 14 years and 17 to 18
years (developmental transitions). • Not associated with body weight at onset.Job
Corp
s

90
Making the Diagnosisin Job Corps
• Anorexia – the health & wellness staff should recognize symptoms
• Bulimia – fellow students tattle on their classmates

91
Eating Disorders Pose aMedical Dilemma
• Classified as a mental disorder.• Has the highest mortality rate of all
mental health conditions.• Over half of the deaths are due to medical
complications.• Unexplained weight loss is a sign of illness. • Effective management of an eating
disorder requires well informed multidisciplinary care.

92
Hurdles to Detection andEffective Treatment
• Patients hide the problem out of fear and embarrassment.
• Patients rarely seek help on their own.
• There is a mistaken notion that patients must want help to get help.

93
Two Key Concepts
• Eating disorders are more about body weight than eating!
• Body weight is the key to understanding and treating eating disorders.

For Example:Mary and the Amazing Muffins
Eatin
g D
isor
der
vs.
Wei
ght D
isor
der

The Muffins

Amazing Muffins!
0 calories0 gm fat
1 gm protein
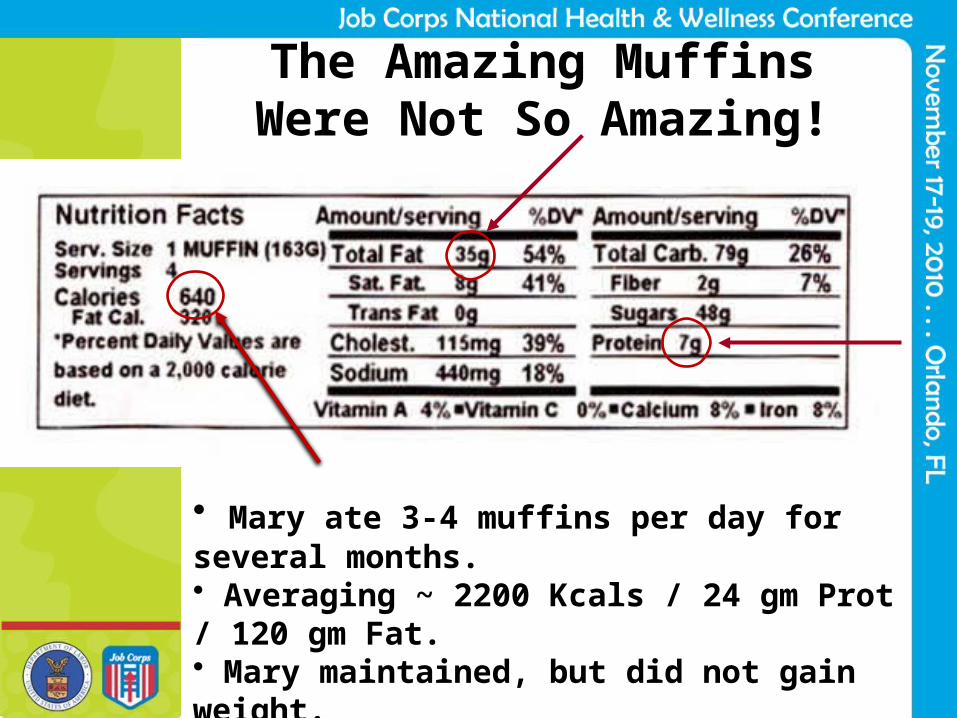
The Amazing MuffinsWere Not So Amazing!
• Mary ate 3-4 muffins per day for several months.• Averaging ~ 2200 Kcals / 24 gm Prot / 120 gm Fat.• Mary maintained, but did not gain weight.• Mary continued trying to lose weight.• Delayed hospitalization through the summer.

Body Weight(in eating disorders)
• Anorexia – failure to gain or maintain adequate body weight (usually low)
• Bulimia – extreme fluctuations in body weight (usually normal)

99Emaciation not necessary for anorexia

Some Signs and Symptoms
To Watch for in Job Corps

101
Severe Peripheral Vasoconstrictionand Hypothermia

102
Loss of Scalp Hair

103
Dizziness and Syncope

104
Arm Lanugo

105
Hypercarotenemia
106
Bulimia in the Dorms
• Empty food wrappers everywhere• Backed-up sink drains• Backed-up shower drains• Emesis around toilet• Sleep disturbances• Loss of motivation

107
Ankle and Foot Edema
Especially with laxative abuse

108
Severe Parotid Gland Swelling

109
Subconjuctival HemorrhagesDue To Purging
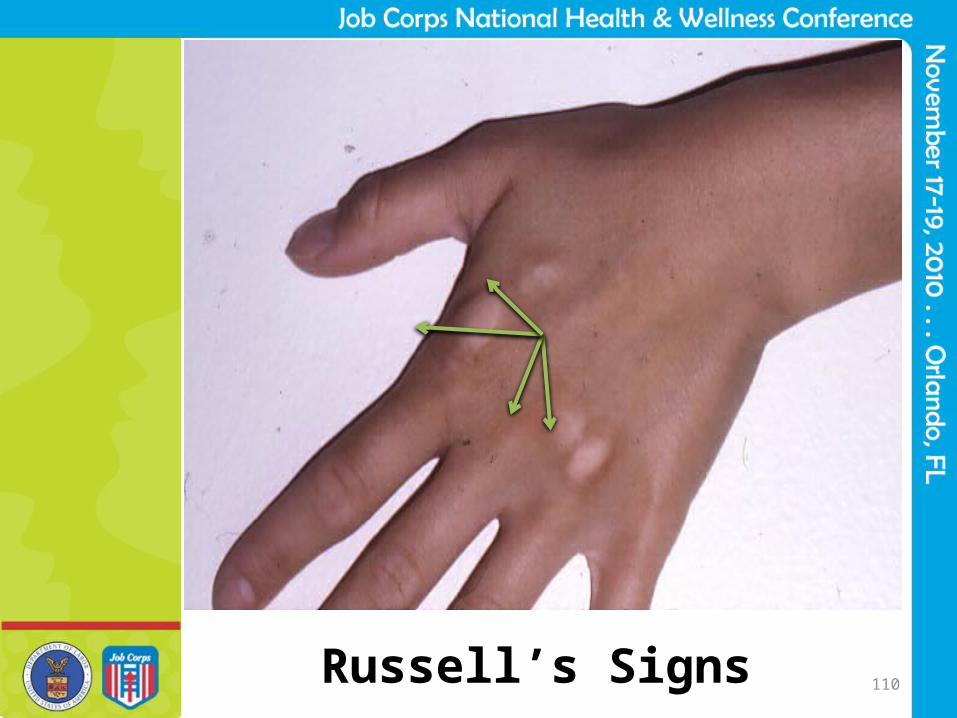
110Russell’s Signs

111
Drinking chocolate milk from a spoonU
nusu
al E
ating
Hab
its

112
Preoccupation with Food

113
Reading Food and Cooking Magazines

114
Hoarding Food
One Patient’s Saved Food – Just in Case!

115
Loss of Concentrationand Increased Distractibility
Cellist
Four auto accidents in six months

October ‘04 April ‘05
However, Treatment Can Be Successful

117
Risks to Keeping Studentson Center with Eating Disorders
• Missed classes from spending time in the health and wellness center
• Decreased motivation for training• Occasional trips to the ER for
dehydration and/or electrolyte imbalance
• Possible medical hospitalization for the sickest of them

118
Staff Education
• There should be an in-service to make staff aware of an eating disorder and what the approach should be in helping a student complete their training while struggling with this illness.
119
Managementon Center?
• Bulimia students are sometimes helped by treatment with SSRI’s
• Bulimia students must decrease their symptoms enough to live in the dorm, stay in class and minimize ER trips
• Anorexia students must be willing to increase their weight to a safe level (est. 17.5 BMI)
• Anorexia students must be able to fully participate in the training and minimize their need for ER trips
Chronic Health ProblemsPRH 6.10 R1.b.4
• Students identified as having chronic health problems…..shall be monitored as directed by the center physician or other appropriate center health care provider.

Medical SeparationPRH 6.12 R11.b
• Students are medically separated when they are determined to have a pre-existing or acquired health condition that: significantly interferes with or precludes
further training in Job Corps, or the health problem is complicated to
manage, or the necessary treatment will be unusually
costly.
LastResort
122
Questions?