
Hospitals and surface contamination - utoledo.edu · Hospitals and surface contamination, Summer...
21
Hospitals and surface contamination, Summer 2013 1 Hospitals and surface contamination Infections contracted during hospital visits remain the fourth largest killer in America (Klevens and Luman, 2001). This is not a problem limited to the United States, as hospitals throughout the world are aiming for the goal of zero healthcare-associated infections (HAIs). It is estimated that 1 in 10 people will acquire an infection during a hospital visit (Plowman et al., 1997). From: Fauci et al., 2005.
Transcript of Hospitals and surface contamination - utoledo.edu · Hospitals and surface contamination, Summer...

Hospitals and surface contamination, Summer 2013 1
Hospitals and surface contamination Infections contracted during hospital visits remain the fourth largest killer in America (Klevens and Luman, 2001). This is not a problem limited to the United States, as hospitals throughout the world are aiming for the goal of zero healthcare-associated infections (HAIs).
It is estimated that 1 in 10 people will acquire an infection during a hospital visit (Plowman et al., 1997).
From: Fauc i et al., 2005.

Hospitals and surface contamination, Summer 2013 2
Limiting the density of infectious agents in the patient's immediate environment can decrease the infectious risk and prevent further infection. Where do hospital infectious agents originate? Much attention has centered on the efficacy of terminal cleanings Extensive cleaning performed following the discharge of a patient.
Terminal cleaning is often suboptimal.
This has been documented in different types of hospitals and intensive care units as well as on general medical or surgical wards. Inadequate cleaning and disinfection is usually a result of suboptimal cleaning practices, and not problems with the detergent or disinfectant solution used.
~ 50% of the surfaces in patient rooms that should be cleaned are actually addressed by the staff. Use of incorrect concentration of disinfectant solution. Inadequate product contact time.

Hospitals and surface contamination, Summer 2013 3
Methods of terminal cleaning 1. Quaternary ammonium compounds
The most commonly used for terminal cleaning of patient rooms (“mop and bucket method”).
Disinfects by denaturing cellular proteins leading to the breakdown of the cell membrane.
Concentration and contact times are extremely important. Limited effectiveness when used with materials such as cotton and gauze pads.
Insoluble precipitates on cotton/gauze absorb the active ingredients.
~40%–50% decline of quaternaries released after one hour of contact with cotton rags or cellulose-based wipes.
From: G oldsmith et al., 1954.

Hospitals and surface contamination, Summer 2013 4
Gram-negative bacteria can survive or grow in quaternary compounds.
Limited effectiveness against Clostridium difficile (below).
2. Microcondensation hydrogen peroxide vapor (VHP)
VHP is a gaseous form of hydrogen peroxide (H2O2) used to decontaminate enclosed and sealed areas. VHP quickly breaks down into water, releasing free oxygen radicals.
Radicals effectively oxidize many compounds within living cells, killing them.
Highly effective against all forms of vegetative bacteria, bacterial spores, fungi, fungal spores, and viruses.
Norovirus, MRSA, VRE, Serratia, Acinetobacter, C. difficile.
VHP was one of the chemicals approved for decontamination of anthrax spores resulting from the 2001 anthrax attacks in the U.S.
It is also effective in removing exotic animal viruses, such as avian influenza and Newcastle disease from equipment and
From: Luc chesi et al., unpublished.

Hospitals and surface contamination, Summer 2013 5
surfaces.
VHP is produced from a solution of liquid H2O2 and water, and dispersed by special aerosolizers.
Vapor is circulated in the air, and contains an H2O2 concentration of 140 ppm to 1400 ppm depending on the infectious agent to be treated.
A concentration of 75 ppm is considered to be immediately dangerous to life by the EPA.
3. Ultraviolet (UV-C) light
Used historically to reduce microbial contamination of air-handling systems, but is gaining popularity for disinfecting hospital surfaces.
Preparing for VHP treatment of a hospital room. O ne unit produces the vapor, while the other unit removes the vapor from the air following treatment, and c onverts it to water.

Hospitals and surface contamination, Summer 2013 6
UV-C, particularly in the 254-nm range, destroys microorganisms by creating thymine dimers in nucleic acids, inhibiting DNA replication.
Can reduce bacteria contamination of surfaces by 2-3 logs (99% - 99.9%). Is that enough?
Effective on high-touch areas, including bed rails, remote controls and toilets following 45 minutes of exposure.
Why is it so effective on high touch areas?
Eradicates both vegetative bacteria and bacteria spores. Acinetobacter spp. and VRE - 98% decrease on surfaces following treatment.
UV light treatment of a hospital room. Shaded areas of the room the rec eive low exposure to the UV radiation usually require supplemental treatment.
Formation of a thymine dimer will impac t subsequent DN A replic ation and effec tively reduce of the mic robial population.

Hospitals and surface contamination, Summer 2013 7
Terminal cleaning techniques - not always effective
The case of Clostridium difficile. C. difficile is one of the leading causes of hospital-associated infections.
Gram positive, anaerobic, spore-forming rod that causes severe diarrhea and other intestinal disease when competing bacteria in the gut flora have been killed by antibiotics.
Hospitals and chronic care facilities are reservoirs for C. difficile because spores can survive on surfaces for long periods of time.
Transmission most often occurs via the hands of health care workers who have contacted contaminated surfaces.
Ingestion of spores often results in GI distress. The rate of C. difficile acquisition is estimated to be 13% in patients with hospital stays of up to two weeks, and 50% in those with hospital stays longer than four weeks.
The spore is made of a thick protein layer that renders it resistant to most chemicals including quaternary ammonium compounds and alcohol hand gel.
C . diffic ile G ram stain (left) and endospore stain (right).

Hospitals and surface contamination, Summer 2013 8
Decontamination of rooms with VHP significantly reduced the incidence of hospital-onset, hospital-associated C. difficile diarrhea.
T he rate o f no so c omia l C D A D ra te dropped signific antly fro m 0.88 c ases/1,000 pa tient-days to 0.55 c a ses/1,000 pa tient-days (rate ratio , 0.63; 95% c o nfidenc e interva l: 0 .50-0.79, P < .0001). F rom: M anian, et a l., 2013.
Hand washing with soap and water is signific antly more effec tive at removing C . diffic ile spores from the hands of volunteers than are alcohol based hand rubs. From: Jabbar et al., 2010.

Hospitals and surface contamination, Summer 2013 9
Sodium hypochlorite (bleach) is one chemical that can penetrate the spore’s thick protein coat and destroy the organism.
MRSA and other staphylococci in the hospital environment
MRSA is methicillin-resistant Staphylococcus aureus.
Gram positive, aerobic cocci that are resistant to many antibiotics (MSSA are susceptible to many antibiotics). Several MRSA clones have evolved and ensure that the organism has spread to almost every country.
Eight pulsed-field gel electrophoresis (PFGE) types exist (USA100 to USA800).
USA300 and USA400 have been associated with community-associated (CA)-MRSA infections.
USA300 is the most common clone in the United States.
The remaining types have been associated with hospital-associated (HA)-MRSA.
S witc hing from quaternary ammo nia -ba sed c leaning to a b lea c h interventio n (red line) in hosp ita ls resulted in a 48% reduc tio n in the preva lenc e density o f C . d iffic ile (95% c o nfidenc e interva l: 36% -58% , P , .0001). F ro m: H ac ek et a l. , 2010.

Hospitals and surface contamination, Summer 2013 10
Many strains are virulent and can cause aggressive infections, even in healthy young people.
Skin, bone, joint, surgical wound, bloodstream, heart valve and lung infections.
MRSA can spread in animals and be spread from animals.
The MRSA resistance spectrum includes virtually all commonly used antibiotics, leading to severe difficulties in selecting the appropriate treatment.
The impact of MRSA
HAIs caused by MRSA are responsible for approximately 280,000 hospitalizations and 19,000 deaths per year.
This significantly impacts health care (Filice et al., 2010).

Hospitals and surface contamination, Summer 2013 11
Median 6-month unadjusted costs for patients infected with MRSA were $34,657, compared with $15,923 for patients infected with MSSA. Patients with MRSA infection were also more likely to die than were patients with MSSA infection (23.6% vs 11.5%; P < 0.001).
Non-aureus staphylococci (sometimes called coagulase-negative staphylococci (CoNS)).
Can result in significant morbidity, as well as special control measures, expensive treatments, extensive surveillance, and longer hospital stays.
Among the most important pathogens involved in hospital-associated bloodstream infections and infections related to vascular catheters and prosthetic devices.
S. epidermidis Many CoNS are resistant to the majority of the available antibiotics.

Hospitals and surface contamination, Summer 2013 12
CoNS have been established as opportunistic pathogens in the healthcare settings.
Why the hospital environment?
Because of their illnesses, hospital inpatients are predisposed to contracting and spreading infections.
Staphylococci can survive for up to several months on items commonly contacted by healthcare personnel, and those in close proximity to the patient. Healthcare personnel readily transport and transmit pathogens between patients.
The high demand for ICU and step-down rooms necessitates rapid room turnover following patient discharge, making effective cleaning difficult.
This is why ~70% of MRSA isolates cultured from infected inpatients are acquired from within the healthcare environment.

Hospitals and surface contamination, Summer 2013 13
Case study: Prevalence and persistence of MRSA at the UT Medical Center
Two objectives:
(i) Determine the impact of a typical daily cleaning process on the prevalence of MRSA on room surfaces.
(ii) Determine the distribution of mixed staphylococci assemblages before and after daily cleanings of surfaces in isolation rooms housing inpatients infected with MRSA.
Site
Ten, single-patient isolation rooms in the UT medical Center (250 beds)
Rooms were selected if:
(i) the room was occupied by an inpatient infected with MRSA. (ii) the room had not yet been subjected to daily cleaning on
the day of the sampling.
Room cleaning was performed by environmental service staff according to established hospital protocol.
Fresh cleaning solution and a clean mop for each room.
All wet moppings were performed with a quaternary ammonia product decanted with tap water.
Dusting with a microfiber mop Wipe cleaning of room furnishings, bed and window components. Walls and doors were spot-cleaned, floors were dust- and wet-mopped.

Hospitals and surface contamination, Summer 2013 14
The patient bathroom was cleaned by dusting, wipe cleaning of fixtures and surfaces, and dust- and wet-mopping of the floors.
Each cleaning event was visually monitored to ensure that all surfaces were cleaned during each sampling event and that the staff washed their hands between each room.
Sampling
Sixteen surfaces were sampled in each room prior to and after daily cleaning activities by swabbing three 100 cm2 areas of each surface.
Laboratory analysis
1. Isolation of putative MRSA
Enrichment of MRSA from sampling swabs (presence/absence of MRSA on surfaces).
Swabs were added to Mueller-Hinton broth and incubated with shaking at 35o C for 16 h. Twenty ml of enriched culture was streaked onto oxacillin resisistance screening agar base (ORSAB) medium and incubated at 35o C for 48 hours.
The remaining enrichment was saved for DNA isolation and DGGE fingerprinting (described below).
2. Confirmation of bacteria identity.
3-4 well-isolated, blue-pigmented colonies (putative MRSA) representing each sampled surface and enrichment type (direct
plating vs. broth enrichment) were subcultured onto tryptic soy agar (TSA) medium and incubated at 35o C for 16 h.

Hospitals and surface contamination, Summer 2013 15
Colonies isolated from ORSAB were subjected to:
a. Coagulase test – coagulation of fibrin
b. Catalase test – degradation of H2O2
c. Multiplex PCR targeting the 16S rRNA gene of
staphylococci, femB (S. aureus) and mecA (methicillin resistance)
3. Genetic fingerprinting of the staphylococci community.
MRSA c olonies growing on O RS A B medium. O RSA B contains oxac illin, high salt and aniline blue (pH reac tion).

Hospitals and surface contamination, Summer 2013 16
Cultures were chosen for fingerprinting analysis if they were associated with a surface that was:
(i) a high-contact surface. (ii) contaminated with a high heterotrophic bacteria load,
relative to other sampled surfaces.
Results
1. Sampling effort
158 surfaces comprising 25 surface types were sampled
Five types of rooms were sampled throughout the campaign, including three MICU rooms, two SICU rooms, two rehab rooms, two step-down rooms and one orthopedic room.
2. MRSA prevalence prior to and following daily room cleaning.
Surface Sampling
effort (n)
# Positive surfaces (%) Direct culture Enriched culture Pre-cleaning Post-cleaning Pre-cleaning Post-cleaning
Floor 10 5 (50) 1 (10) 6 (60) 2 (20) Sink/fixtures 10 4 (40) 1 (10) 5 (50) 2 (20) Bed rails 10 4 (40) 4 (40) 5 (50) 4(40) Overbed table 10 3 (30) 2 (20) 3 (30) 1 (10) TV Panel 10 1 (10) 1 (10) 1 (10) 2 (20) Dry eraser 9 0 (0) 0 (0) 3 (33) 1 (11) IV Box 9 1 (11) 0 (0) 0 (0) 0 (0) Phone 9 4 (44) 1 (11) 5 (56) 3 (33) Chair 9 2 (22) 0 (0) 2 (22) 3 (33) Call light 8 3 (38) 3 (38) 5 (63) 3 (38) Light switch 8 0 (0) 1 (13) 0 (0) 1 (13) Bath door handle 7 1 (14) 0 (0) 1 (14) 0 (0) Bath rails 6 1 (17) 0 (0) 1 (17) 1 (17) Cabinet handles 6 2 (33) 2 (33) 2 (33) 0 (0) I&O record 6 0 (0) 0 (0) 1 (17) 0 (0) Soap dispenser 6 1 (17) 0 (0) 1 (17) 1 (17) Info. Binder 5 2 (40) 1 (20) 4 (80) 3 (60) BP cuff 4 0 (0) 0 (0) 0 (0) 0 (0) Linens 4 0 (0) 0 (0) 0 (0) 0 (0) Sink counter 3 1 (33) 0 (0) 1 (33) 0 (0) Biohaz. container 2 1 (50) 0 (0) 0 (0) 0 (0) Main door handle 2 0 (0) 0 (0) 2 (100) 0 (0) Linens bin 1 1 (100) 0 (0) 1 (100) 0 (0) Mobile cart 1 0 (0) 0 (0) 0 (0) 0 (0) Toilet handle 1 0 (0) 0 (0) 0 (0) 0 (0)

Hospitals and surface contamination, Summer 2013 17
Cleaning efforts decreased (not significantly, P=0.241) the percentage of surfaces harboring MRSA.
MRSA was detected on 29±7% of the sampled surfaces prior to daily cleaning and on 17±4% of the surfaces following cleaning. Surfaces most frequently harboring MRSA contamination prior to daily cleanings included: Floor (contaminated during 60% of the sampling events) Sink/fixtures (50%) Bed rails (50%) Telephone (56%) Call light (63%)
The floor, overbed table and dry-eraser experienced the greatest decrease in MRSA harborage following cleaning (67% each), while the bed rails experienced the least (20%).
Why?
O verall perc entage of surfac es c ontaminated with MRSA prior to (n) and following (☐) daily c leaning as determined by broth enric hment.

Hospitals and surface contamination, Summer 2013 18
Following daily cleaning, the bathroom rails, soap dispenser handle experienced no reduction in the frequency of MRSA occurrence. MRSA was successfully removed from the bathroom door handle, cabinet handles, I&O record, sink area counter, main room door handle, used linens bin. The frequency of MRSA occurrence increased on two surfaces following cleaning.
TV button panel (10% prior to cleaning and 20% following cleaning) Visitor's chair (22% to 33%).
Perc entage of spec ific surfaces c ontaminated with MRSA prior to (n) and following (n) daily c leaning. *, MRSA not detec ted.
Hospitals and surface contamination, Summer 2013 19
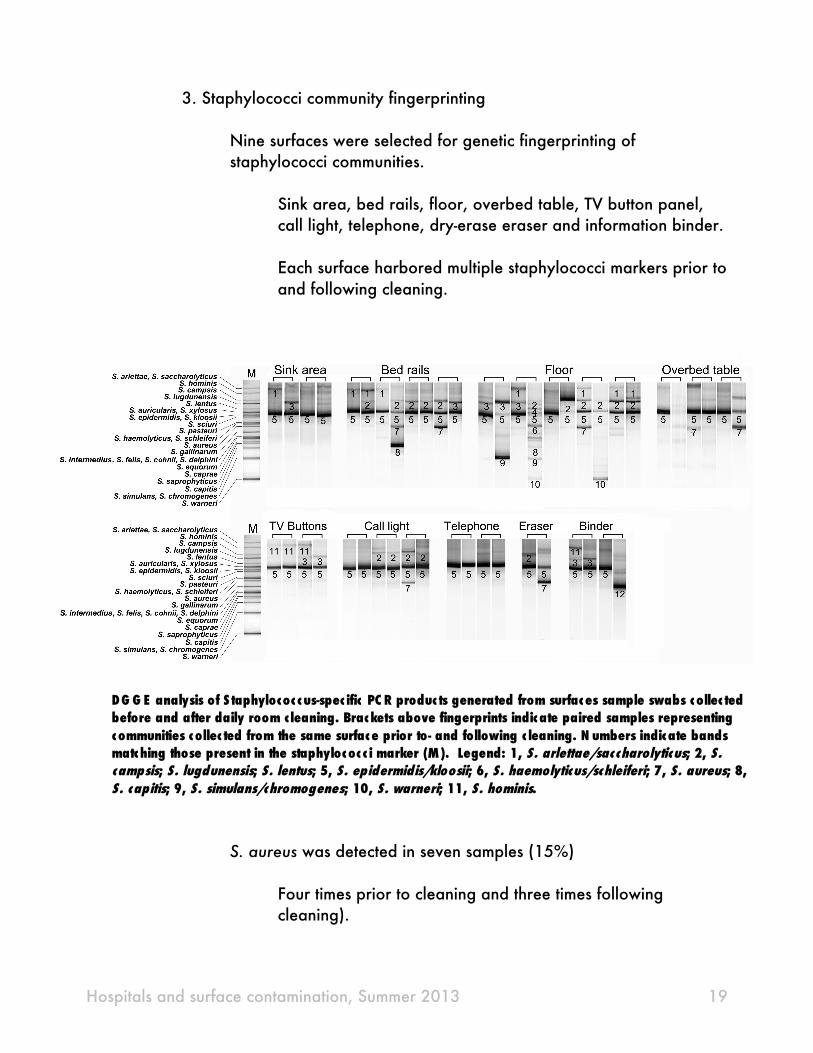
3. Staphylococci community fingerprinting
Nine surfaces were selected for genetic fingerprinting of staphylococci communities.
Sink area, bed rails, floor, overbed table, TV button panel, call light, telephone, dry-erase eraser and information binder.
Each surface harbored multiple staphylococci markers prior to and following cleaning.
S. aureus was detected in seven samples (15%)
Four times prior to cleaning and three times following cleaning).
DG G E analysis of S taphylococ c us-spec ific PC R produc ts generated from surfac es sample swabs c ollec ted before and after daily room c leaning. Brackets above fingerprints indic ate paired samples representing c ommunities c ollec ted from the same surfac e prior to- and following c leaning. N umbers indic ate bands matc hing those present in the staphyloc oc c i marker (M). Legend: 1, S. arlettae/sac charolyticus; 2, S. campsis; S. lugdunensis; S. lentus; 5, S. epidermidis/kloosii; 6, S. haemolyticus/schleiferi; 7, S. aureus; 8, S. capitis; 9, S. simulans/chromogenes; 10, S. warneri; 11, S. hominis.

Hospitals and surface contamination, Summer 2013 20
S. epidermidis/kloosii was detected on all nine assayed surfaces prior to and after cleaning, and in all but two (96%) of the 48 samples selected for fingerprinting.
S. epidermidis is the most frequently isolated Staphylococcus species in the clinical environment and is responsible for a significant number of infections among inpatients.
S. lugdunensis was detected in seven samples, twice prior to cleaning and five times following cleaning.
Although S. lugdunensis is a known skin commensal, we regard its persistence as an emerging threat, as it is responsible for a variety of nosocomial and community-associated infections that progress with similarity to those caused by S. aureus
Why are these bacteria so persistent?
Staphylococci attached to particulates in air can be a significant source of contamination.
CoNS and S. aureus were isolated from 86% and 64% of air samples, respectively, collected from hospital operating rooms. Aerosolization can result from daily maintenance activities including floor cleaning and bed making
Limitations in the cleaning process.
Variability in cleaning efficacy, untrained/unmotivated cleaning staff or unreasonable cleaning workload can contribute to persistent contamination. Detergent-based cleaning materials can remove microbes from common hospital surfaces, but might not consistently kill them.

Hospitals and surface contamination, Summer 2013 21
Microfiber and cotton/cellulose cleaning cloths can neutralize quaternary ammonia products and effectively spread microbes across surfaces rather than removing them.
Conclusions
Daily cleaning methods were largely ineffective at removing MRSA and other staphylococci on high touch surfaces, many of which are commonly in close proximity to the patient. The persistence of potentially pathogenic staphylococci on hospital surfaces represents a significant infection threat and should be addressed in future research efforts that examine the efficacy of cleaning materials and processes.


















