Hospitals. Introduction History of Hospitals Hospitals vs. Hospice.
Upload
jordi-varelaCategory
view
489download
0
The hospital necessary reforms
10Recommendations to improve hospitals efficiency, quality and
effectiveness
Jordi VarelaMarch 9, 2015

Hospitals are structures with a powerful influence on the overall health system. Its effectiveness in solving certain acute health problems, especially in the surgical area, gives them a major social prestige. However this fact should not undermine two structural problems that are weighing their image down:
• The first problem is internal. The own bureaucracies are showing signs of fatigue and this affects the service quality, especially when it comes to the safety of admitted patients.
• The second problem is relational. The hierarchical superiority of hospitals has placed them apart from the communitarian reality and the primary care, and causes now a serious difficulty in dealing, in an integrated manner, with the complex chronic disease care and with the geriatric frailty....
.
.
9/3/15 10 structurals reforms hospitals 3
The 10 recommendations are focused on providing
structural reforms proposals aimed at overcoming
hospitals’ internal problems
9/3/15 10 structurals reforms hospitals 4
Industrializing the processes that can be subjected to a protocol (1/3 of case mix)
1

9/3/15 10 structurals reforms hospitals 5
There is evidence showing that the carefully designed clinical trials, involving dedicated professionals and well-informed patients, give good outcomes, such as fast-track in colon surgery, for example (1). Following this track, the Department of Cardiac Surgery from Mayo Clinic
has gone further and has industrialized a good part of their surgical procedures using the following criteria (2): selection of patients according to risk; patient’s understanding and acceptance at being included in the process; industrial process mapping; competence redefinition; use of Lean or Six Sigma; comprehensive in-depth quality controls; specific facilities and fully committed professionals.
(1) Fast-track surgery. A new revolution after laparoscopy? Posted April 18, 2014 “Advances in Clinical Management”
(2) From ‘Solution Shop’ Model To ‘Focused Factory’ In Hospital Surgery: Increasing Care Value And Predictability Health Aff May 2014 33:5746-755
9/3/15 10 structurals reforms hospitals 6
Releasing coordinated clinical sessions and individualized care plans as a working methodology in hospital wards(2/3 of case mix)
2

9/3/15 10 structurals reforms hospitals 7
Patients admitted through a specialized process, but who do not meet factory criteria, patients with clinical complexity and chronically ill patients hospitalized for complications should be treated according to a new working model which we may call generalist hospital.
In the generalist wards, work will be performed by a multidisciplinary team. It will be drawn an individualized care plan for each patient admitted through the clinical coordination meetings and therefore the medical orders and interdisciplinary consultation will disappear. Hospitalists and nurses of reference to each patient must ensure the quality and continuity of care. Specialists will have to choose between working in the factory or contributing as consultants in the generalist hospital (1).
(1) The hospital of the future. New report (UK). Posted December 15, 2014 “Advances in Clincial Management”

Joint development of the individualized care plan (ICP)A patient with clinical complexity
RH
Reference professionals
ICP
RH: reference hospitalits/ RN: reference nurse / GP: general practitioner / PCN: primary care nurse/ SP 1...n: specialists that are necessaries for the clinical process / var SP : various specialists (according to the case): social worker, physioterapist,etc.
RN
GP
PCN
SP 1
SP n var SP
9/3/15 810 structurals reforms hospitals
A new model for the generalist hospital The clinical coordination meetings(2/3 of case mix)

9/3/15 10 structurals reforms hospitals 9
Adjusting the criteria for admission in the critical care units and deploying strategies for semi-critical patients
3

9/3/15 1010 structurals reforms hospitals
ICU: demands flexibility and semi-critical strategies
The number of Intensive Care Unit (ICU) beds in the US is 10 times higher than in the UK with no apparent impact on the life expectancy in the two countries and when the experts analyse the case mix, they have observed that the fundamental variability is due to improper use of the ICU (1).
The criteria for admission to ICU for patients with clinical complexity and chances of survival should be well established but, on the other hand, care strategies for semi-critical patients with less complexity (such as in the image) or for patients with low probability of survival, would have to be deployed (2).
(1) ICU Bed Supply, Utilization, and Health Care Spending. An Example of Demand Elasticity. Rebecca A. Gooch; Jeremy M. Kahn. JAMA. 2014;311(6):567-568
(2) Goal-Oriented Patient Care — An Alternative Health Outcomes Paradigm. David B. Reuben, Mary E. Tinetti. N Engl J Med 2012; 366:777-779. March 1, 2012

9/3/15 10 structurals reforms hospitals 11
Reorient the organization toward the geriatric frailty and deconstruct the care of chronic patients
4

9/3/15 1210 structurals reforms hospitals
Hospitals orientation towards geriatric fragility
The integration of social and health services within the community framework is the proposal best suited to the needs of the elderly frail patients, but this does not prevent that sometimes they need to be admitted to the hospital. A committee of British experts (1) indicates how the hospitals reorientation strategy towards this increasingly numerous group of patients should be: a) the emergency department should incorporate geriatric methodology and should be very clear about the admission criteria, b) geriatric assessment and individualized care plans
would be essential for patients hospital admission, c) the ward staff should develop specific communication skills, and d) defining plans to avoid the most common iatrogenic issues (ulcers, delirium, infections, falls, dehydration, undernourishment, thromboembolism, etc.) should be deployed.
(1) Comission on Hospital Care for Frail Older People. Main Report Comission HSJ. November 2014

9/3/15 1310 structurals reforms hospitals
Deconstruction of chronic patients care
Chronic patients require a model of integrated care (1) that allows tailoring the treatments to their real needs and to their ways of understanding their own diseases (2). For this reason, it is desirable to keep them away from the specialized medicine which, at least for this group, has a tendency to fragmentation and disproportionate performance.
Meanwhile, hospitals must know how to deal with disruptive reforms (3) that allow them to invest the resources coming from inappropriate performances aimed at enhancing the integration of services to maintain the chronic patients at the community level as far as possible (4).
(1) The Chronic Care Model. Improving Chronic Illness Care (web site)
(2) Minimally Disruptive Medicine. Posted August 18, 2014 “Advances in Clinical Management”
(3) The Innovator’s Prescription. A disruptive solution for Health Care. Clayton M. Christensen. Mc Graw Hill 2009
(4) Developing integrated care: what role do acute hospitals play? Posted by Chris Ham. January 14, 2014 “The King’s Fund Blog”

9/3/15 10 structurals reforms hospitals 14
Involve the doctors according to Max Weber’s principles (noble proposals, intrinsic motivation, respect and belonging)
5
9/3/15 1510 structurals reforms hospitals
Involvement of doctors in the transformations (1)
In its publication in Harvard Business Review, "Engaging Doctors in the Health Care Revolution", Thomas Lee and Toby Cosgrove, focus on the 4 fundamental Max Weber’s motivations towards social actions to make proposals aimed at achieving doctors’ involvement (1):
Motivation 1. Seek noble proposals. When managers and physicians meet up, they should do it with the purpose of discussing patients, quality and results. According to Mayo Clinic, the basic script is: a) at the time of sitting down, everyone should be clear that things can not continue as they are, b) the ideal transformative project must be clearly focused on the patient, and c) everyone involved must take the same path.
(1) Engaging Doctors in the Health Care Revolution. Posted by Thomas H. Lee and Toby Cosgrove. June 2014. “Harvard Business Review”

9/3/15 1610 structurals reforms hospitals
Involvement of doctors in the transformations (2)
Motivation 2. Find the intrinsic motivation of each individual. Doctors like to be valued if they perceive the set objectives as timely and consistent. The motivation is more about consistency than it is about money
Motivation 3. Promote respect. Respect must be based on the value that each doctor provides to his/her patients, colleagues and the organization, in that order.
Motivation 4. Promote a sense of belonging. Doctors must be able to proudly say: "Here we have a way of doing things”.

9/3/15 10 structurals reforms hospitals 17
Distribute the competencies between specialists and hospitalists
6

9/3/15 1810 structurals reforms hospitals
In the new bimodal hospital (1), the specialist will have two options: a) to work in the factory, and/or b) to become a consultant in the generalist hospital working in a multidisciplinary team who develops individualized care plans for each patient. On the other hand, the hospitalist
will be directly responsible for the admitted patients. The internists, geriatricians and other specialists who choose the generalist function will be the hospitalists, and they will be fully dedicated to the wards and will not make them compatible with any other clinical responsibility.
Specialists competencies versus hospitalists
(1) The hospital of the future. New report (UK). Posted December 15, 2014 “Advances in Clincial Management”

9/3/15 10 structurals reforms hospitals 19
Increase training, organizational quality and nurses’ competencies; and generate magnetism
7

9/3/15 2010 structurals reforms hospitals
Nurse responsibilities: more power, more organizational quality
a) Two different studies: the doctoral thesis of MireiaSubirana, Director of Care in Hospital de Vic and a European observational study developed with the input from more than 26,000 nurses from 9 different countries (1) demonstrate that both the nurse educational level as the nurse staffing in wards influence the rate of patients mortality.
b) The advanced nursing practice (ANP), a post-graduate training that provides an overview for the care of complex patients, are specially trained to lead many aspects of the clinical processes, according several sources (2).c) A systematic review and a meta-analysis (3) have shown that substitution of doctors with nurses (the study is framed in the field of primary care) improve patient satisfaction and reduce avoidable hospitalizations.
(1) Nurse staffing and education and hospital mortality in nine European countries: a retrospective observational study. Linda H Aiken, Douglas M Sloane, Luk Bruyneel, et al. The Lancet 383, 9331, 24 May 2014, 1824:30
(2) Scope on Nursing Practice Toolkit and Decision making Framework Toolkit. International Council of Nurses (web site)
(3) Substitution of physicians by nurses in primary care: a systematic review and meta-analysis. Martínez-González et al. BMC Health Services Research 2014, 14:214

9/3/15 2110 structurals reforms hospitals
What is a magnet hospital?
It’s a hospital that, in a context of lack of nurses, is able to retain and attract. They are centres that act as a magnet.
In a study of M. McLure (1) the magnetism has been characterized as a feature of certain hospitals where: a) nurses have a high level of autonomy, b) there is supervisory support and therefore the work load lacks fluctuations, c) there are well developed continuing education programs, d) the working model is geared towards the patient, e) there is good communication between doctors and nurses, and f) competence is a value for promotion.
(1) “Essentials of Magnetism,” in Magnet Hospitals Revisited: Attraction and Retention of Professional Nurses, M. McClure and A. Hinshaw (eds). Kansas City, Mo., American Nurses Publishing, 2002.

9/3/15 10 structurals reforms hospitals 22
Organizational stress to ensure care continuity and to improve patient safety
8
9/3/15 2310 structurals reforms hospitals
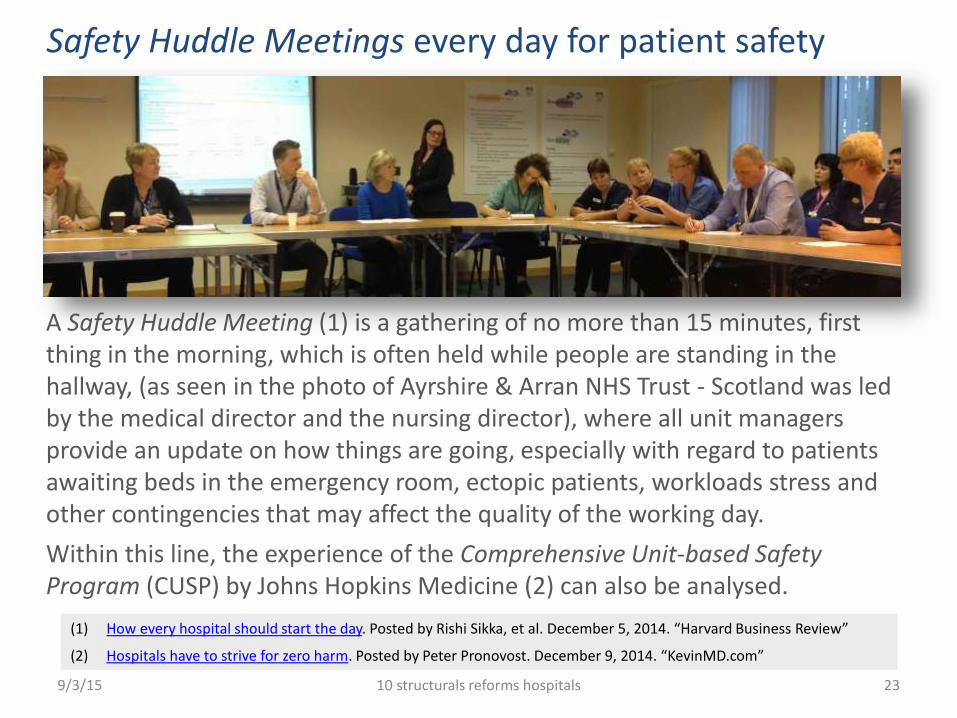
Safety Huddle Meetings every day for patient safety
A Safety Huddle Meeting (1) is a gathering of no more than 15 minutes, first thing in the morning, which is often held while people are standing in the hallway, (as seen in the photo of Ayrshire & Arran NHS Trust - Scotland was led by the medical director and the nursing director), where all unit managers provide an update on how things are going, especially with regard to patients awaiting beds in the emergency room, ectopic patients, workloads stress and other contingencies that may affect the quality of the working day.
Within this line, the experience of the Comprehensive Unit-based Safety Program (CUSP) by Johns Hopkins Medicine (2) can also be analysed.
(1) How every hospital should start the day. Posted by Rishi Sikka, et al. December 5, 2014. “Harvard Business Review”
(2) Hospitals have to strive for zero harm. Posted by Peter Pronovost. December 9, 2014. “KevinMD.com”

9/3/15 10 structurals reforms hospitals 24
Rethinking the organization to adapt it to patient-centred care
9

9/3/15 2510 structurals reforms hospitals
Patients induced reforms (1)
Clinical shared decision making is a third alternative after the authoritarian medicine and technocratic medicine. One must know how to lead the patients so that they can take their own decisions (3).
The new concept of patient experience (beyond the traditional "satisfaction") means involvement in organizational design and process redesign (1).
Patients can request an active rolein clinical documentation and can record the visits (in the UK they are already entitled by law to it) (2).
(1) The Optimal Practice of Evidence-Based Medicine. Incorporating Patient Preferences in Practice Guidelines. Victor Montori, et al. JAMA. 2013;310(23):2503-2504
(2) Should doctors encourage patients to record consultations? Glyn Elwyn and Laurence Buckman. BMJ 2015;350:g7645
(3) Critical Decisions. How you and your doctor can make the right medical choices togheter. Peter Ubel. HarperOne 2012
.
.
.

9/3/15 2610 structurals reforms hospitals
Patients induced reforms (2)
Knowing how to design decision aids for clinical shared decision making, materials that should be far more advanced than the traditional brochures (1).
Being more concentrated on reconciling medications and deprescribing whenever necessary, in coordination with the family physician (2).
Knowing how to activate the community volunteerism, beyond the traditional accompaniment during hospitalization (3).
(1) Mayo Clinic Shared Decision Making National Resource Center (web site)
(2) Garfinkel D, Mangin D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults. Adressing polipharmacy. JAMA Intern Med, Oct 11 2010;170(18):1648-54
(3) How time banking is making a difference to patients’ lives. Posted by David Boyle. February 6, 2015. “The Guardian Healthcare Network”
.
.
.

9/3/15 10 structurals reforms hospitals 27
Fostering leadership, learning from mistakes and promoting innovation
10

9/3/15 10 structurals reforms hospitals 28
the organization, leaders who should be present in all corners of all processes and, above all, leaders who know how to involve colleagues in the resource management and further promote the patients participation in clinical decisions.
Fostering leadership
(1) The future of leadership and management in the NHS. No more heroes. Report from the King’s Fund Commission on leadership and management in the NHS. The King’s Fund 2011
Managers are essential for the work quality of doctors, nurses and other professionals. But the new leadership should no longer be attributed to the heroic action of managers. Now there must be clinical leaders distributed throughout

9/3/15 10 structurals reforms hospitals 29
As defended by Richard Bohmer (1), hospitals must implement best practices rigorously, should address the complex processes with trial and error mechanisms and should have a strategy to improve things from on a daily basis.
(1) Fixing Health Care on the Front Lines. Posted by Richard Bohmer. April 2012. “Harvard Business Review”
Learning from mistakes

9/3/15 10 structurals reforms hospitals 30
Most health professionals have an innate innovative capacity, but then, why is it so hard to change things? Well, the answer sometimes is cultural or related to the work environment. How often a good idea is met with: "We already have been doing it for a long time”, or "We're too busy to think about
Promoting innovation
(1) Build an Innovation Engine in 90 days. Posted by Scott Anthony. December 2014. “Harvard Business Review”
innovation”, so it turns out being difficult to push a cart with square wheels.
Scott Anthony (1) has defined a minimum viable innovation system, based on projects that should not exceed three months in duration.

9/3/15 10 structurals reforms hospitals 31
When speaking of structural reforms, many think of labour rights, financing or investments. These and other aspects are important, not in vain hospitals deal with a reknowned complexity. But make no mistake: only from clinical management, its business core, one can start the imperative change towards improving process effectiveness and resources optimization.
...

9/3/15 10 structurals reforms hospitals 32