Neurological emergencies Mackay Memorial Hospital Department of Neurology Ju-Fen Yeh.
©2002 J Dietrick CRNA
Hospital Emergencies and
Anesthesia
Joe Dietrick, CRNA, M.A. Have A Nice Day Anesthesia Associates, LLC
Chillicothe, MO

©2002 J Dietrick CRNA ©2002 J Dietrick CRNA
Declarations No conflict or affiliation to report No discussion of off-label use of medications
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA
Objectives The participant will understand the four facets of emergency management personal, organizational, & anesthetic response to emergencies concepts of triage mechanisms of injury in terrorism anesthetic considerations in disasters
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Planning
What is a Disaster? Facility emergency Operations altered Most likely
Facility disaster Operations overwhelmed Most extreme
Both require adequate Emergency Plan Mandated by JCAHO E.C. 1.4, 2.4, & 2.9.1 Plan execution twice per year

©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Planning
Four Facets of Planning 1) Mitigation Threat risk assessment Strategy to minimize vulnerability
2) Preparedness Building organizational capacity
3) Response Implementation of some phase of plan Tracking & modifying activities
4) Recovery Restoration of essential service Restoration of normal service

©2002 J Dietrick CRNA Mitigation
Risk Assessment Hazard Vulnerability Analysis tool Likelihood of event occurring Anticipated severity if event occurs
Types of emergency categories Internal External
- Many emergencies result in a combination - All are Security events as well
Must develop plans to respond to each threat
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Mitigation
Types of Emergencies: Internal Safety Facility damage Inadvertent HazMat release
Operational Utility or Communication Disruption Impaired services
Security Fire/smoke Hostile party / disturbance Implied / explicit threats
©2002 J Dietrick CRNA Mitigation
Types of Emergencies: External Mass Casualty Incident (MCI) Types Natural or man-made cataclysmic event Weather, earthquake, nuclear or explosive event
Cyber Terrorism: CBRNE Chemical Biological Radiological Nuclear Explosive
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Mitigation
Terrorism Definition of terrorism (28 CFR Section 0.85) Terrorism is the unlawful use of force or violence against persons or property to intimidate or coerce a government, the civilian population, or any segment thereof, in furtherance of political or social objectives.
Goals of terrorists Mass casualty generation Lethality Disruption
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Preparedness - ICS
Building Organizational Capacity Ability to respond Expand resources Anesthesia normally 1:1 patient care Minimal primary responsibilities outside OR May be responsible for triage & immediate stabilization May have to care for multiple patients
Requires organized system
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Preparedness - ICS
Incident Command System (ICS) Designed to provide organized and flexible response Originated in the Fire Service Successfully used by most Public Safety agencies HEICS - Hospital Emergency ICS
ICS creates a dependable chain of command flexibility in activation & expansion of response prioritization of duties
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Preparedness - ICS
ICS Assigns roles rather than individuals Mission Duties Priorities
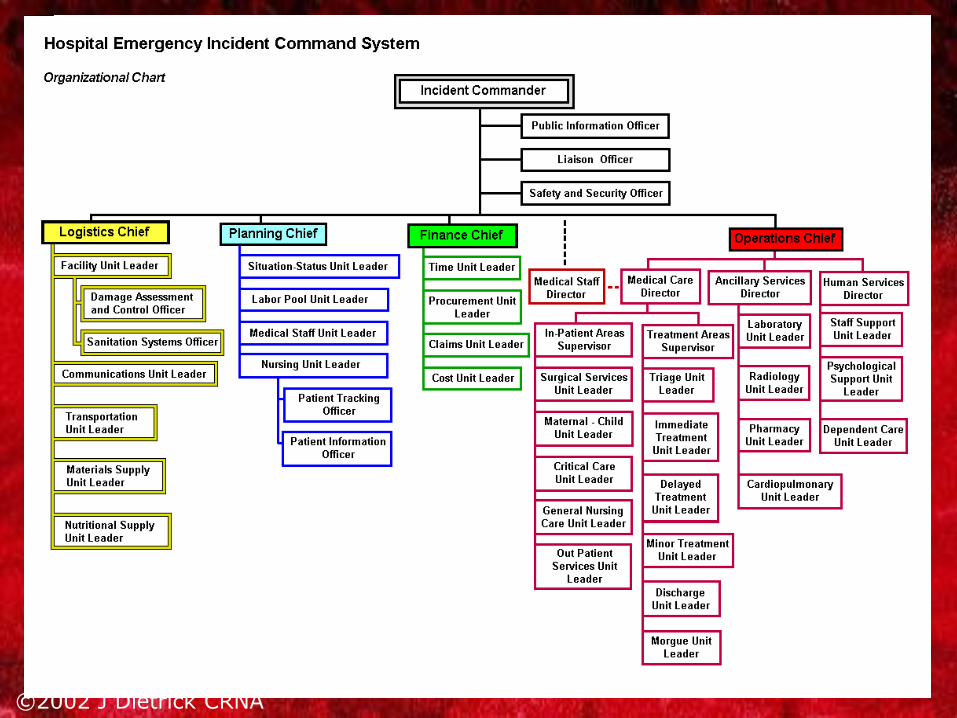
Incident Command Center
Purpose maintain optimal hospital operation during a threat (actual or perceived) by being a central point of coordination, contact, and resource management in support of other departments.
Bottom up structure All roles provide support to those below!
©2002 J Dietrick CRNA Preparedness - ICS

©2002 J Dietrick CRNA
Four Sections Logistics Things
Planning Foresight People
Finance/Admin Pay for it, or get paid
Operations Whoever has the expertise & capability to manage event and mitigate hazards
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - ICS
Operations Medical Operations primary design of HEICS Internal Emergencies Primary Operations Section branch: Facilities or Security
Medical Operations branch in addition
Divisions: Care & Support Care areas In-Patient: early discharge Out-patient: augmentation ED: triage, critical care
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - ICS
Incident Commander Overall responsibility Set objectives according to priorities
Obtain Incident Summary understand the situation Identify objectives & prioritize (life, then property)
Establish an Incident Action Plan (IAP) to accomplish objectives Communicate IAP Re-evaluate IAP frequently, and consider:
worst-case scenario secondary threat/consequences
Level of response Level of service
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response
Disaster Notification Obvious a disaster has occurred (earthquake) Patients start arriving at your facility Unusually similar illnesses appear Prehospital / Public Safety Telephone Radio Network
Number of casualties & resources required, almost always overestimated.
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response
Disaster Scene Operations Search Rescue Triage Initial Stabilization Transport

©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response
Your Response
Problems Not accountable to anyone Not accounted for by anyone Not trained in scene safety (safety over care) Secondary events are likely
Goal: Rapid removal to higher level of care
Victims often arrive at facility quickly
Consider searching all victims
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response
GO TEAM External response team Medical care above the level of prehospital / EMS providers Attributes Planned Organized Equipped Trained
May be useful in rural areas
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response
Internal Facility Damage Scene safety first observe for: Electrical hazards - Broken glass Fire danger - Jagged metal Unstable objects - Toxic substances Adverse environmental conditions
Do not enter until hazards are secured and scene is safe
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response
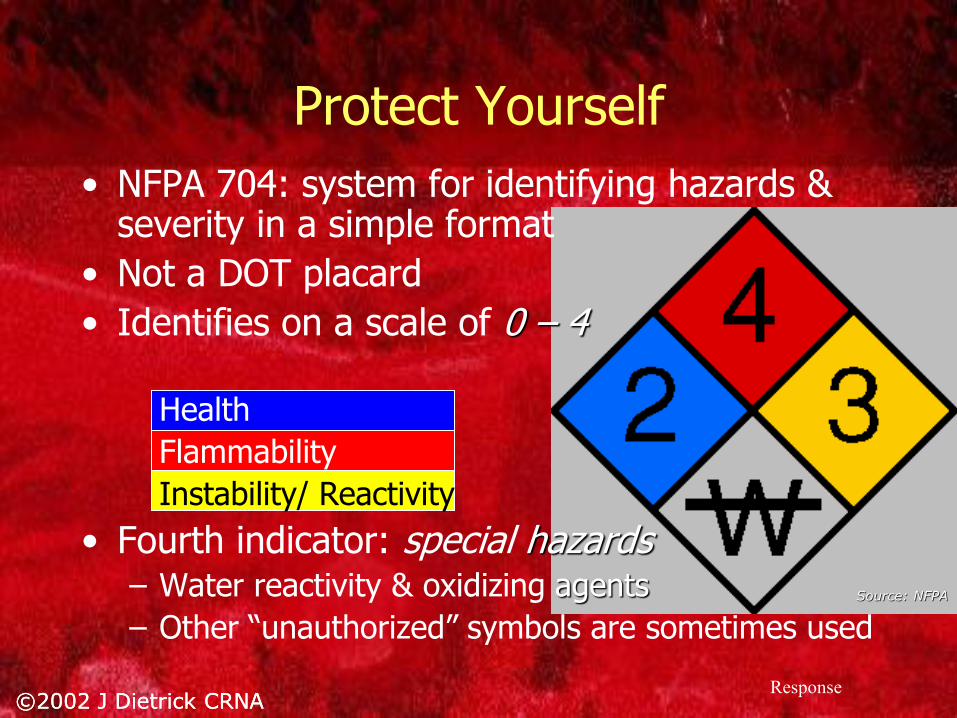
Protect Yourself NFPA 704: system for identifying hazards & severity in a simple format Not a DOT placard Identifies on a scale of 0 4 Health Flammability Instability/ Reactivity Fourth indicator: special hazards Water reactivity & oxidizing agents
Source: NFPA
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response
Mass Casualty Incidents (MCI) Three levels I: Local resources adequate II: Pooling of resources necessary III: State/ Federal assistance required
Level III resources include National Guard / Military FEMA Disaster Medical Assistance Teams (DMAT) Urban Search & Rescue (USAR)
Augmented medical sources Medical Reserve Corps Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VP)
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Triage
Triage MCI = [demand] > [resources] Everyone has to be on the same page Terminology Urgency those who need rapid medical attention to save life/limb those with minor injuries
Level of care to provide
Improve distribution of casualties among available hospitals Often keeps hospitals below MCI levels
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Triage
Triage Categories Immediate Require immediate treatment for life/limb for which survival likely with initial stabilization
Delayed Not likely to die if treatment delayed, but... Will require definitive treatment
Minimal Minor injuries requiring no or minimal treatment
Generally performed by most senior physician

©2002 J Dietrick CRNA
A MASS START to a good finish Quickly group large number of victims MASS Move Ambulate? Move an extremity? Nothing
Assess Individual START assessment
Sort Send
Simple Triage And Rapid Treatment Three assessments Respirations Pulse Mental Status
Immediate if any RPM abnormal Three treatments Open Airway (may insert OAW) Stop bleeding Elevate extremities
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Triage
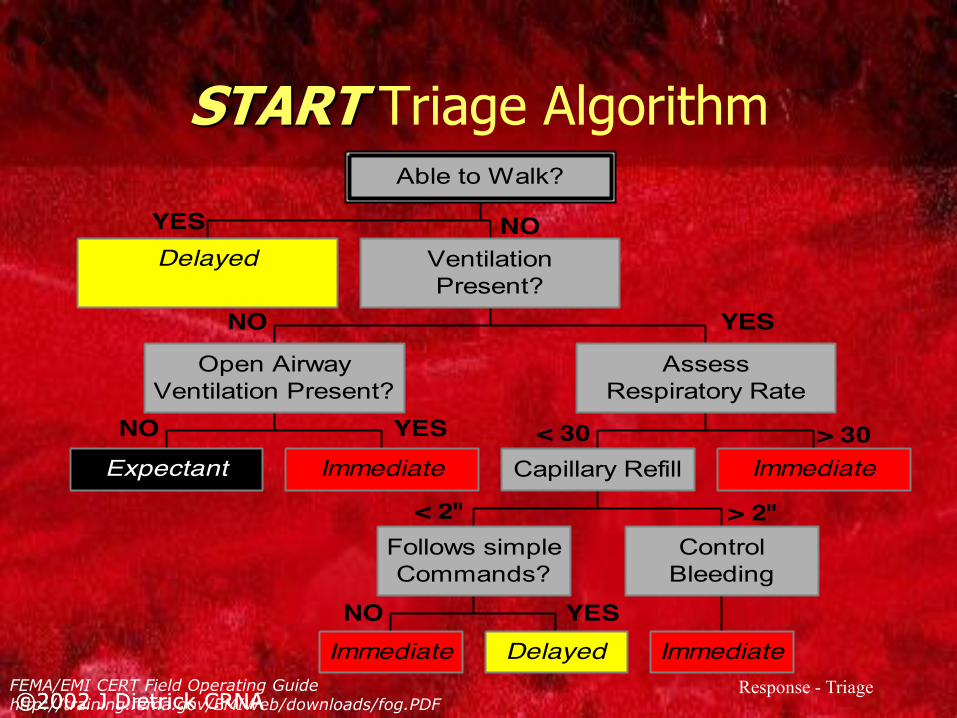
START Triage Algorithm
YES NO
NO YES
< 30 > 30
< 2" > 2"
NO YES
NO YES
Delayed
Expectant Immediate
Open AirwayVentilation Present?
Immediate Delayed
Follows simpleCommands?
Immediate
ControlBleeding
Capillary Refill Immediate
AssessRespiratory Rate
VentilationPresent?
Able to Walk?
FEMA/EMI CERT Field Operating Guide http://training.fema.gov/EMIWeb/downloads/fog.PDF

©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Triage
Triage error Under-triage Assignment of immediate victim to delayed Must be avoided
Over-triage Assignment of immediate care when not critically injured (delayed) Common
In true MCI, over-triage is directly proportional to mortality rate of critical injuries
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Injuries
Not all terrorism is BIOterrorism: CBRNE CDC has outstanding website Ideally, mass effect by delayed recognition of undetectable (to senses) agent Wisconsin Statewide Health Information Network (WISHIN)
ABSOLUTE RULES: Contaminated victims must be prevented from entering your facility Decontaminate outside to protect your facility, patients, & staff
©2002 J Dietrick CRNA
CBRNE Chemical Pulmonary / Choking agents: Pulmonary edema Phosgene
Blood agents Cyanide-based
Blister agents: Respiratory tract & skin Mustard, Lewisite, Phosgene Oxime
Nerve agents: Inhibit Ach-ase cholinergic activation Sarin, Tabun, Soman, VX
Decontaminate as for biological exposure
Biological More toxic by weight than chemicals Dissemination
Inhalational, ingestion, dermal contact
Category A agents: Anthrax (95% mortality inhaled Plague Smallpox (30% in unvaccinated) Tularemia Viral Hemorrhagic Fever Botulism
Decontamination (warm water!):
Wet victim, strip clothing, flush with water, cover Use soap/water &/or Bleach/Water (10:1)
©2002 J Dietrick CRNA
CBRNE Radiological Dirty Bomb Conventional explosive used to disseminate radiological agent Good news Limited exposure to care providers Do not delay critical care to decontaminate
Nuclear Good-bye
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Injuries
CBRNE: bombs/blasts Most common deliberate cause of mass disaster Primary: 2º shockwave Creates high: pressure, temperature, speed Air-tissue interfaces disrupted: Ears, Lung
After overpressure Negative pressure/implosion Then air movement: blast wind secondary/tertiary
Secondary Debris set in motion Blown or collapse
Tertiary Body set in motion Crashes into other objects
©2002 J Dietrick CRNA
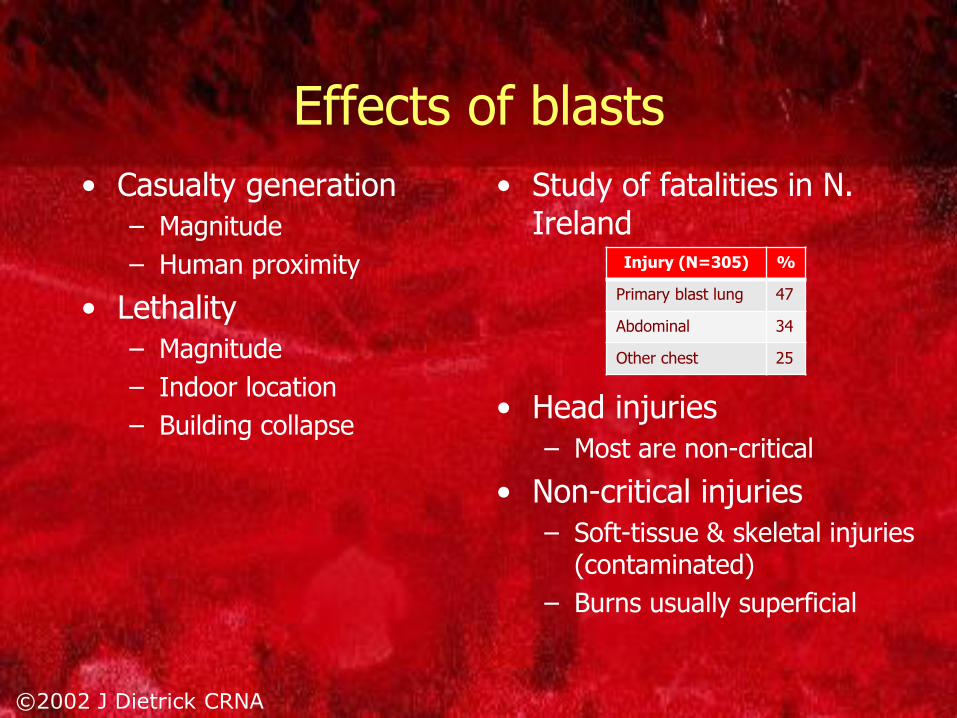
Effects of blasts Casualty generation Magnitude Human proximity
Lethality Magnitude Indoor location Building collapse
Study of fatalities in N. Ireland Head injuries Most are non-critical
Non-critical injuries Soft-tissue & skeletal injuries (contaminated) Burns usually superficial
Injury (N=305) %
Primary blast lung 47
Abdominal 34
Other chest 25
©2002 J Dietrick CRNA
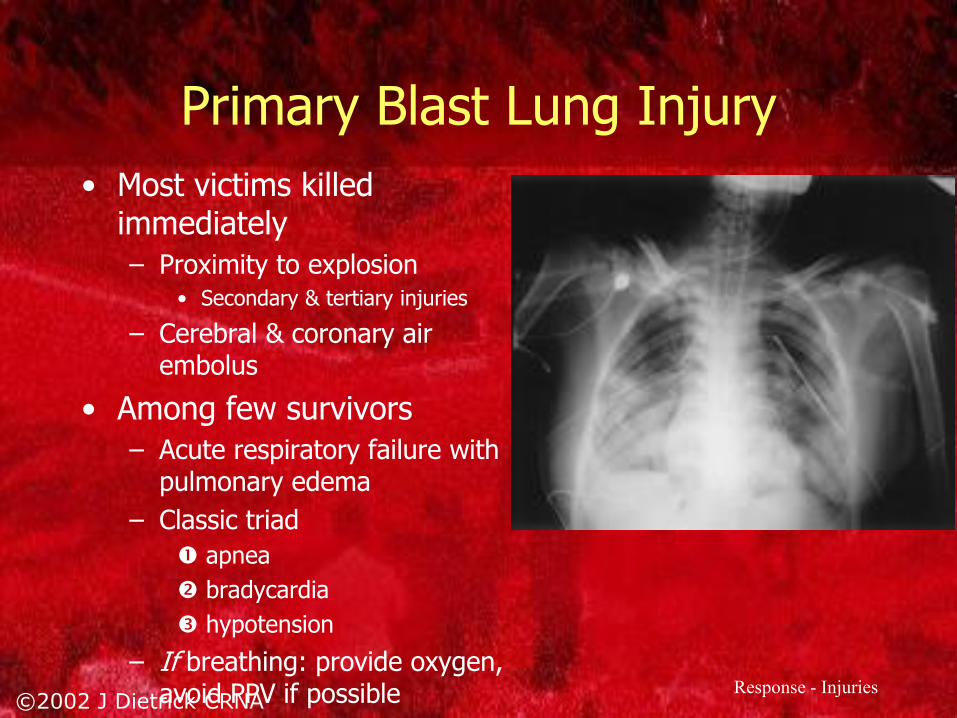
Primary Blast Lung Injury Most victims killed immediately Proximity to explosion Secondary & tertiary injuries
Cerebral & coronary air embolus
Among few survivors Acute respiratory failure with pulmonary edema Classic triad apnea bradycardia hypotension
If breathing: provide oxygen, avoid PPV if possible
Response - Injuries
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Injuries
Crush Syndrome Local & systemic injury Traumatic rhabdomyolysis Common in collapse with masonry Release of myoglobin, potassium, uric acid, and lactic acid Metabolic acidosis & renal impairment
Hypovolemia & coagulopathy

©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Anesthesia
Disaster Anesthesia Avoid contamination from CBR agents Prepare & have supplies for most likely critical injuries Hypovolemia Head injury Airway management Hypothermia Cervical spine injury Pneumothorax
During MCI, conventional level of care may not apply Pain control: a priority in all clinical situations
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Anesthesia
Disaster Anesthesia Options dependent on environmental situation Can you use the OR? Other locations?
Can you use your machine? Electricity Pipeline oxygen
Do you have adequate oxygen supply? Source: King Systems
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Anesthesia
Oxygen Supply Hospital liquid oxygen requires electricity Alternatives Cylinders: E 660 liters, H 6900 liters Concentrators Unlimited supply, reliable, economical Require electricity lpm, FiO2 = 0.85 - 0.95
Generally accepted as best disaster source
Portable liquid oxygen tanks No electricity, heat , or noise 20 - 60 liter liquid 17k - 50k liter gas 0-15 lpm
Source: CAIRE, Inc.
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Anesthesia
Monitors Pulse Oximeter Oxygenation Pulse rate & rhythm Peripheral perfusion
Blood Pressure Manual cuffs available?
Temperature Hypothermia is common
Capnometry? Relative cardiac output, RR, pulmonary dynamics
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Anesthesia
Anesthesia Techniques IV Sedation minimal anesthesia, monitoring necessary
Regional Anesthesia Once block established care may be reduced Good prolonged pain control Reduces systemic medications & side effects
General anesthesia (inhalation or TIVA) Maintain spontaneous ventilation Maintain CV stability
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Anesthesia
Intravenous Agents Long-acting rather than short Diazepam > Midazolam Morphine > Fentanyl
Minimize respiratory depression NSAIDs > Mixed Opioid Ag/Antag > Opioids
Cardiovascular stability Etomidate / Ketamine (±) > Thiopental / Propofol
Agent with multiple routes of administration Ketamine Fentanyl Midazolam
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response - Anesthesia
Blood Consider autotransfusion techniques In OKC bombing > 300 units blood administered Regional blood center had adequate supplies on the shelf
In OKC tornado < 100 units given Problem: distributing blood due to traffic
Decision to transfuse: demand vs. resources
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA
Altered Standards of Care? Standard of care
What a reasonable person would do in similar circumstances
Resource allocation does change
Schultz & Annas
allocate scarce resources maximizing patient outcomes is a necessary and appropriate goal for those engaged in disaster preparedness and
Altering the Standard of Care in Disasters Unnecessary and Dangerous. Ann Em Med 2012
©2002 J Dietrick CRNA ©2002 J Dietrick CRNA Response
Media: Releasing Information ICS always appoints Media role early Guidelines published by American Hospital Association: Any inquiry must contain name of the patient Unless patient has requested information withheld Location One-word description of condition
Conditions Undetermined Serious Good Critical Fair