Hong Kong Eye Hospital Biometry Audit 2012 SN60WF IOL Dr. Rose Chan Resident, Hong Kong Eye...
33
Hong Kong Eye Hospital Hong Kong Eye Hospital Biometry Audit 2012 SN60WF IOL Dr. Rose Chan Resident, Hong Kong Eye Hospital
-
Upload
lewis-haynes -
Category
Documents
-
view
220 -
download
0
Transcript of Hong Kong Eye Hospital Biometry Audit 2012 SN60WF IOL Dr. Rose Chan Resident, Hong Kong Eye...

Hong Kong Eye HospitalHong Kong Eye Hospital
Biometry Audit 2012
SN60WF IOL
Dr. Rose Chan
Resident, Hong Kong Eye Hospital
Acknowledgement
Pre-admission and post-discharge (PAPD) nursing staff
Medical Record Office (MRO) staff Ms Chiu Wai Yee Dr. Victoria Wong

Introduction Importance of auditing cataract
surgery outcomesMost commonly performed surgery Increased patient expectation
Adopt practices that promote the patient’s best interests and safety in performing cataract surgery

Possible complications in cataract surgery
Refractive surprise
Diminished quality of life Binocular diplopia Altered depth perception Lens exchange Medicolegal implications
Purpose of audit Royal College of Ophthalmologists Cataract
Surgery Guidelines 2010“The accuracy of the biometry should be
continuously audited by comparing the expected spherical equivalent with the achieved spherical equivalent.”
Refraction within 1 diopter of target is considered to be satisfactory
A benchmark standard of 85% is suggested
Summary of last year result
Mean difference between target and post-op SE: -0.58 D (range, -3.22D to +3.7D)
Within ± 1 D of target SE 64.6 % (177/274)
Biometry performance significantly better forPAPD nursing staff Nidek machine
Suggestions from last year To concentrate biometry service by
experienced staff
To aim emmetropia for SN60WF Choose target refraction between 0D and -0.5D
To repeat audit next year To refine A-constant if similar outcome

Methods July 2010– Oct 2011 Patients implanted with SN60WF (15-20% of IOL in 2011)
Biometry by PAPD NS, optometrists and orthoptists SRK/T formula regardless of axial length Uneventful phacoemulsification + IOL Major reasons for exclusion
○ Combined surgeries○ No refraction available○ Complicated surgery
Methods
Data CollectedDemographicsAxial length, keratometryBiometry machine and staffTarget and outcome refraction

Biometry staff and machineNursing Optometrist Orthoptist
Nidek Echoscan
n= 196/390 (50.3%)● ● ○
Quantel Medical Axis
n= 110 (28.2%)● ●
Canon KU-1
n= 40 (10.3%)●
Alcon Ocuscan
n= 22 (5.6%)●
Zeiss IOL Master
n= 22 (5.6%)●

Current A-constant
For USG biometry: 118.7 For Optical biometry: 119.1
Results 897 SN60WF IOL were implanted
~15% total IOL
390 eyes were included into audit Female : Male 225:135 Left : Right 189:201 Age 74.4 years (range, 38-93 years) Axial length 23.64 mm (range, 20.0 –
30.28mm)
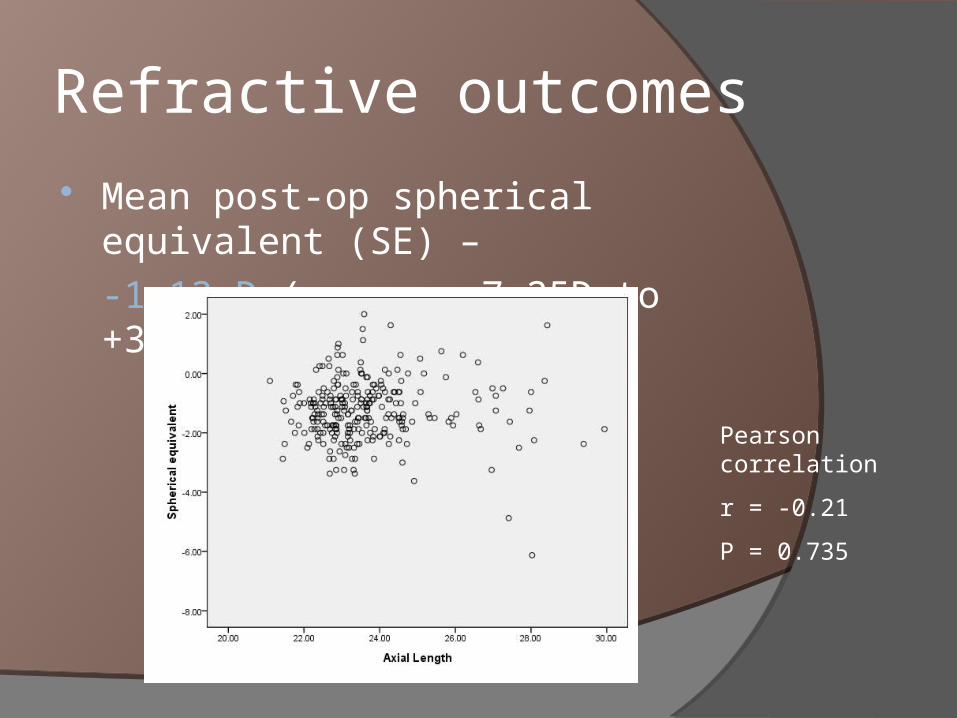
Refractive outcomes Mean post-op spherical equivalent (SE) –
-1.13 D (range, -7.25D to +3.125D)
Pearson correlation
r = -0.21
P = 0.735

Comparison of outcomes Mean target SE -0.61D (range, -4.66D to +0.44D) Mean post-op SE -1.13 D (range, -7.25D to +3.12D)
p<0.0001 (two-tailed t-test)
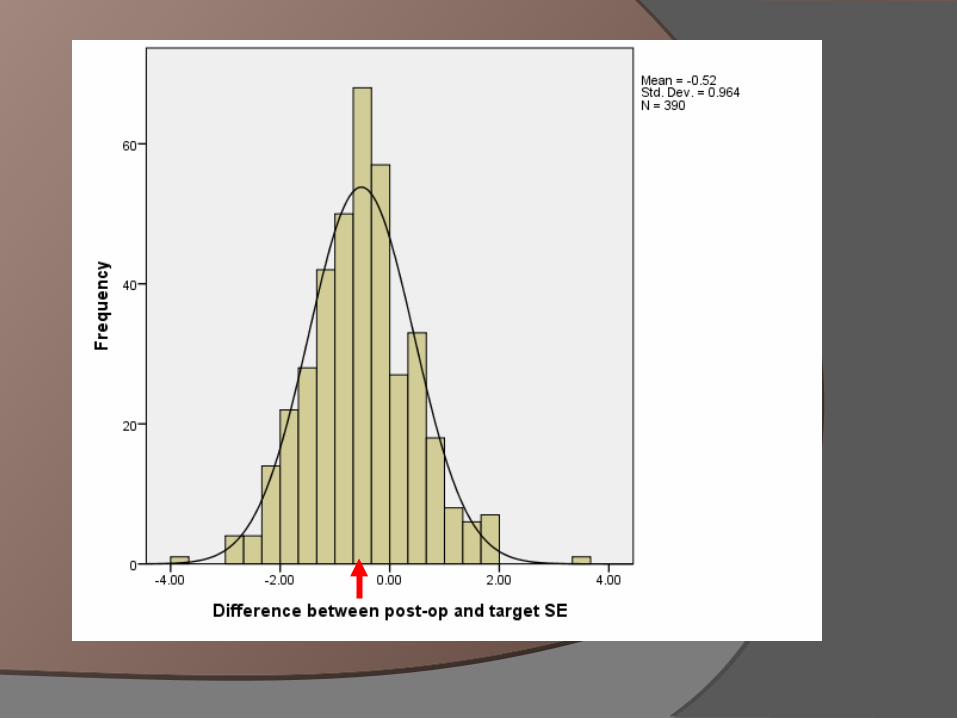
Mean difference between target and post-op SE: -0.52 D (-3.8D to +3.46D)
Calculation based on surgeon’s chosen target refraction
Within ± 1 D of target SE 64.9 % (253/390)
Factor analysis SRK/T formula used in all patients Calculation based on surgeon’s chosen target
refraction
Comparing proportion of patients within target refraction range (+/- 1D of target), and those not within target rangeChi-square test
Sex p=0.45
Age (<60, 60-80, >80 years old)p=0.83
Laterality of eyes p=0.733
Factor analysis
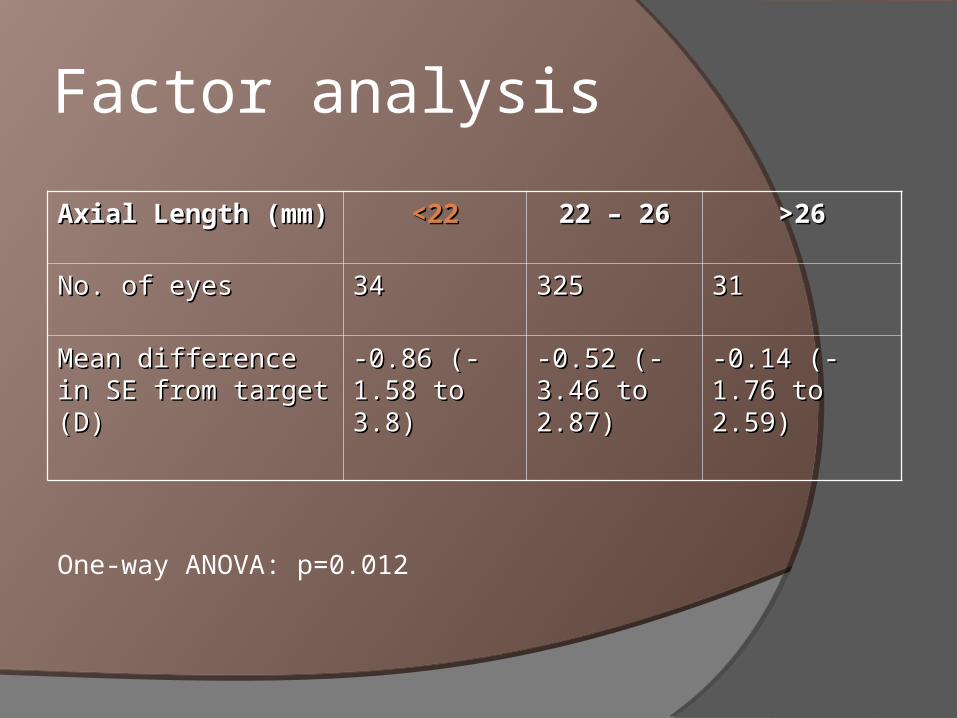
Axial Length (mm)Axial Length (mm) <22<22 22 – 2622 – 26 >26>26
No. of eyes No. of eyes 3434 325325 3131
Mean difference in SE Mean difference in SE from target (D)from target (D)
-0.86 (-1.58 -0.86 (-1.58 to 3.8)to 3.8)
-0.52 (-3.46 -0.52 (-3.46 to 2.87)to 2.87)
-0.14 (-1.76 to -0.14 (-1.76 to 2.59)2.59)
One-way ANOVA: p=0.012
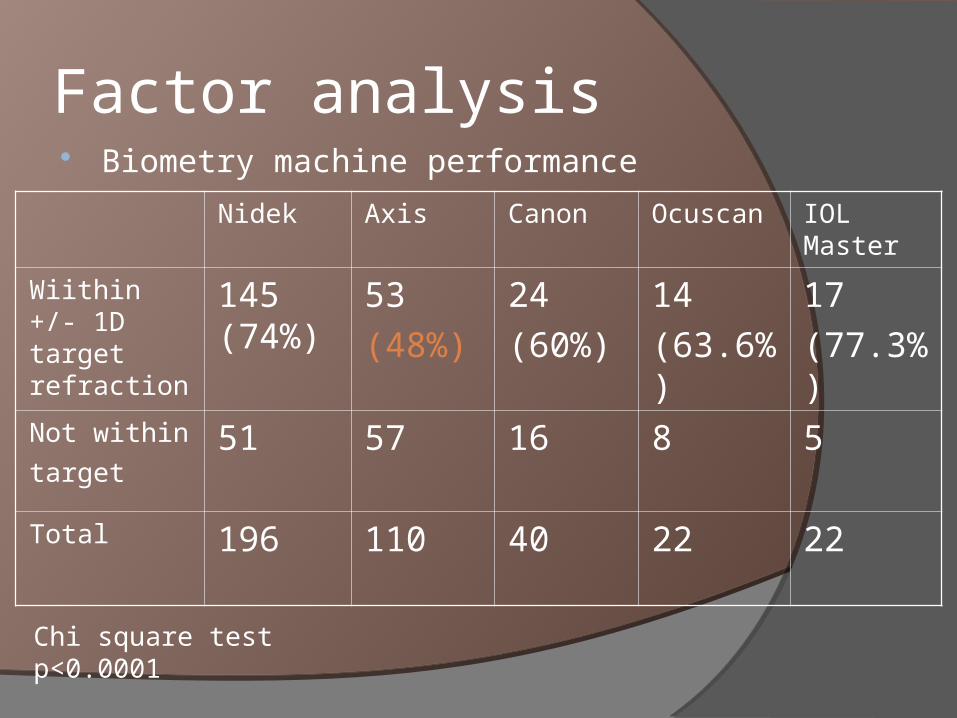
Factor analysis Biometry machine performance
Nidek Axis Canon Ocuscan IOL Master
Wiithin +/- 1D target refraction
145 (74%)
53
(48%)
24
(60%)
14
(63.6%)
17
(77.3%)
Not within
target 51 57 16 8 5
Total 196 110 40 22 22
Chi square test p<0.0001

Factor analysis Biometry staff performance by group
Chi-square test p<0.0001
Nursing Optometrist Orthoptist
Within +/- 1D of target refraction
103 (77.4%) 86 (51.8%) 64 (64.9%)
Out of target refraction range
30 80 27
Total 133 166 91

Factor analysis
Machine performance? Staff performance?
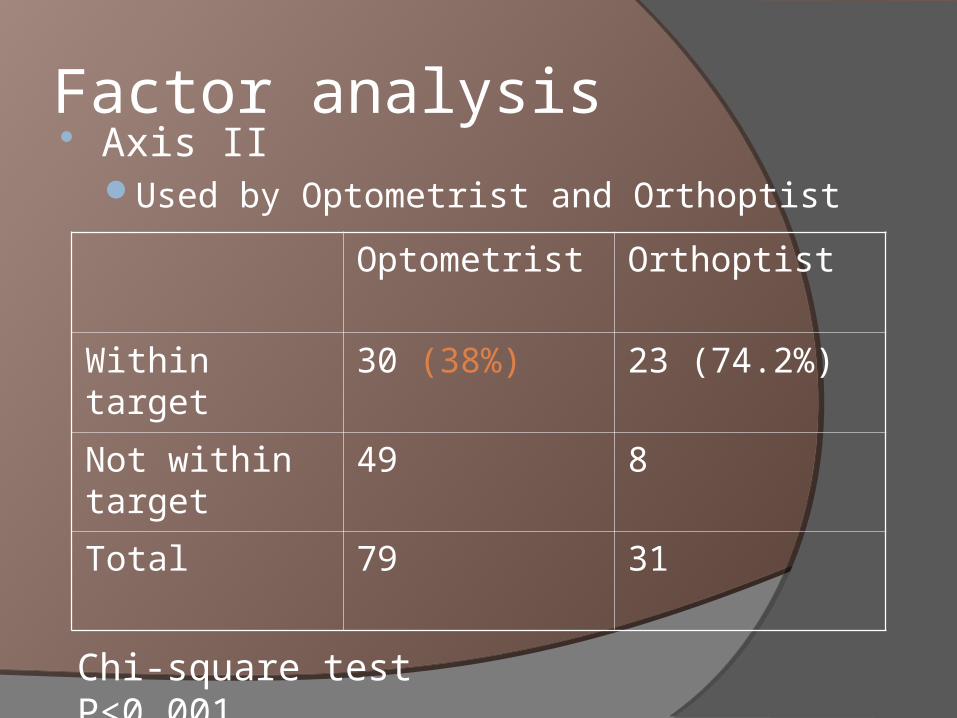
Factor analysis Axis II
Used by Optometrist and Orthoptist
Optometrist Orthoptist
Within target 30 (38%) 23 (74.2%)
Not within target
49 8
Total 79 31
Chi-square test P<0.001
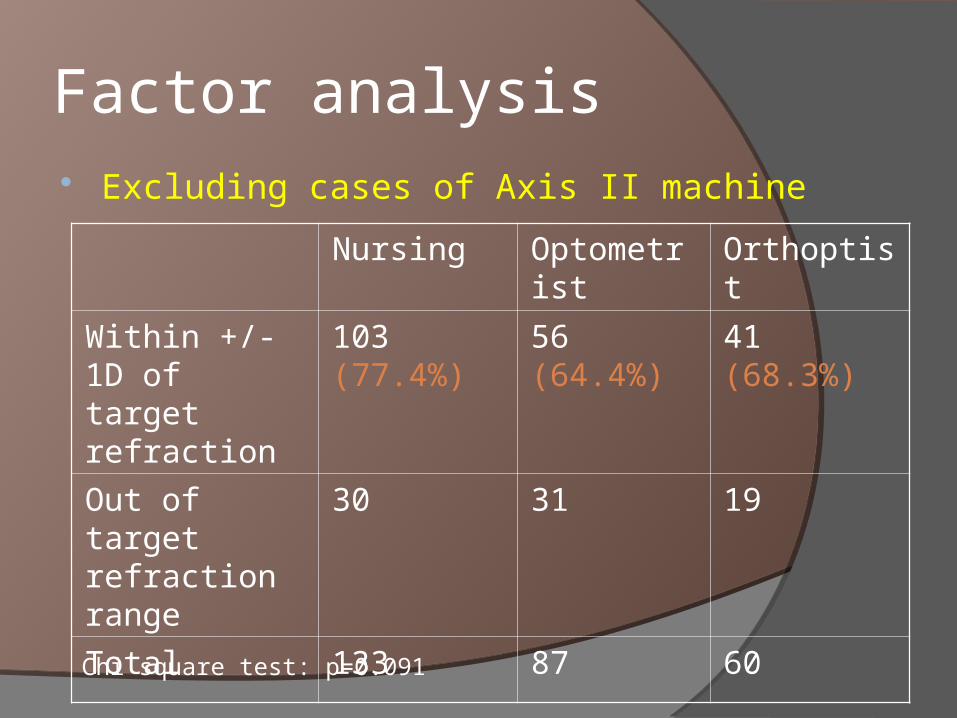
Factor analysis Excluding cases of Axis II machine
Nursing Optometrist Orthoptist
Within +/- 1D of target refraction
103 (77.4%) 56 (64.4%) 41 (68.3%)
Out of target refraction range
30 31 19
Total 133 87 60
Chi square test: p=0.091
Factor analysis
No significant difference of individual optometrist performance P=0.658 (Chi-square)
Discussion Suboptimal biometry outcomes not reaching 80% target
Overall biometry performance significantly better for PAPD nursing staff Nidek / IOL master machines
Previous years: most biometry performed by nursing staff But more biometry service to be taken up by optometrist
Need further enhancement of skills and technique
Discussion
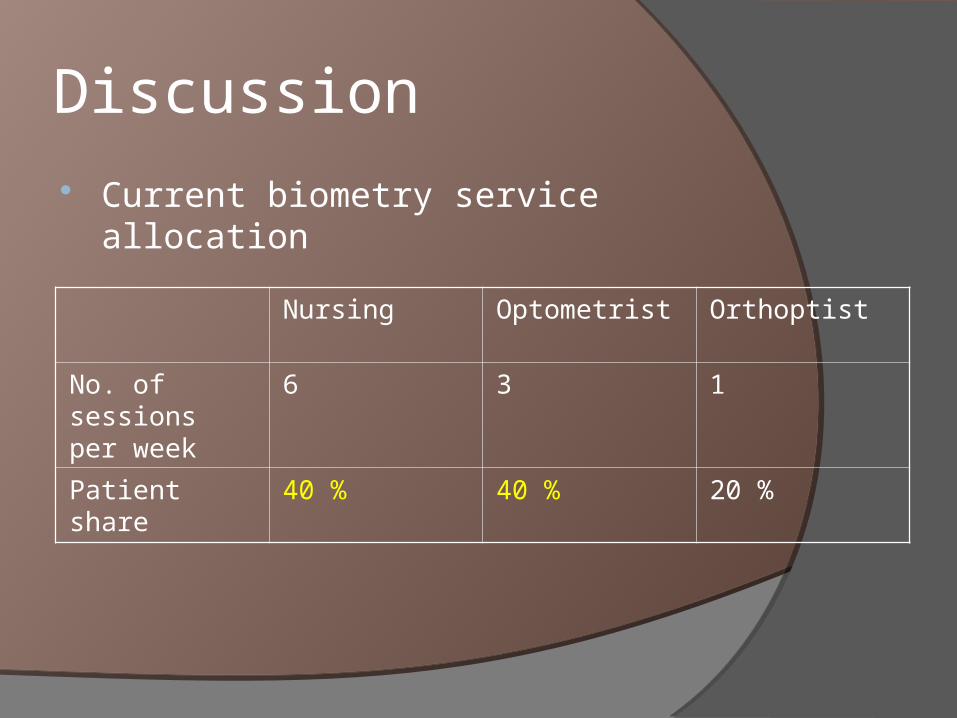
Current biometry service allocation
Nursing Optometrist Orthoptist
No. of sessions per week
6 3 1
Patient share 40 % 40 % 20 %

Discussion Mean target refraction of our surgeons:
-0.61D SN60WF
AsphericReduced spherical aberration best when
emmetropic
Myopic shift significantly more in short AL eyesAim emmetropia especially for short eyeball

Discussion
Poor results from Axis II machineNo longer in use
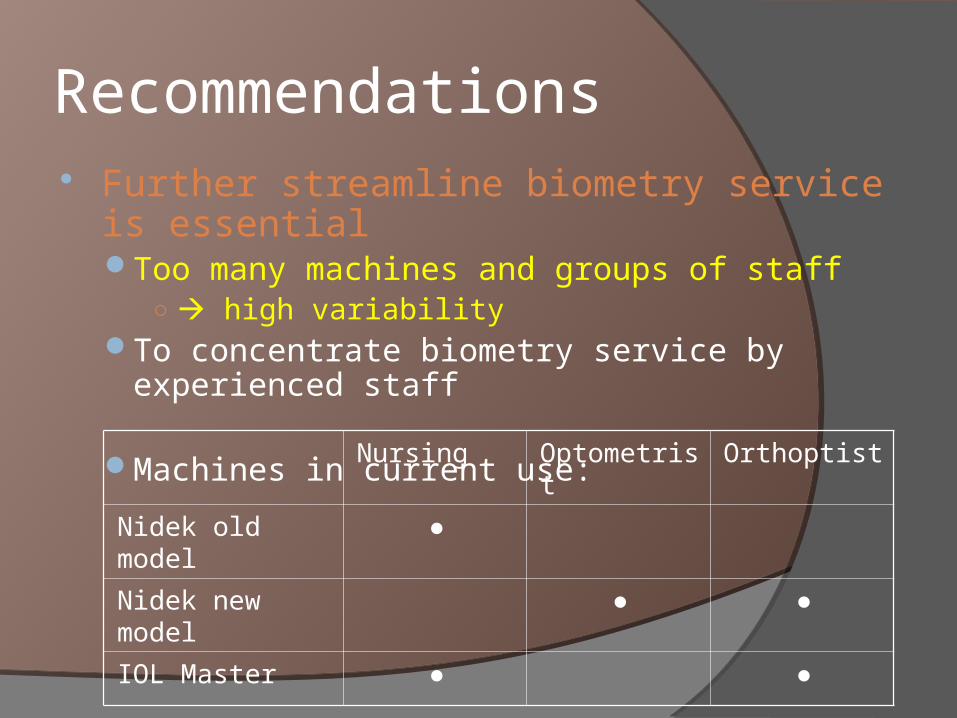
Recommendations Further streamline biometry service is essential
Too many machines and groups of staff○ high variability
To concentrate biometry service by experienced staff
Machines in current use:
Nursing Optometrist Orthoptist
Nidek old model ●
Nidek new model ● ●
IOL Master ● ●

Optometrist service improvementAudit for individual performanceEstablish protocol for double check mechanismImprove setting for biometry measurement
○ Head support, fixation targetUse of IOL master
○ Less technique demanding
To aim emmetropia for SN60WF Choose target refraction between 0 and -0.5D
○ Especially for short eyes

Recommendations
Re-calculation of optimized A-constant (excluding cases by Axis-II and IOL master)
Using Dr Warren Hill Constant Calculation spreadsheet
Modified optimized A-constant 118.2
Recommendations
Current optimization not applicable to IOL master (optical biometry)To review in coming yearMore cases anticipated coming year
○ 2/3 cases of nursing (VA better than 3/24)

Thank You