
Homograft replacement the pulmonary valve -...
6
Thorax (1966), 21, 337. Homograft replacement of the pulmonary valve DENIS N. FULLER, PAUL MARCHAND, MONTY M. ZION, AND SAUL ZWI From Johannesburg General Hospital and University of the Witwatersrand Pulmonary incompetence is a common sequel of pulmonary valvotomy, but many authors believe that the haemodynamic consequences of this regurgitation are well tolerated (Talbert, Morrow, Collins, and Gilbert, 1963). In this paper we report a patient who had severe pulmonary incom- petence after valvotomy and who failed to main- tain her initial clinical improvement. Because of the severe leak it was considered reasonable to correct the incompetence surgically. A homograft pulmonary valve was used, and we are unaware of any previous report of its use in man, though Ross, Cooper, and Brockenbrough (1961) de- scribed the experimental replacement of the pulmonary valve with a tricuspid semilunar prosthesis in dogs. CASE REPORT A 9-year-old white girl was seen in 1958. There was a history of sweating and listlessness during infancy. After the age of 1 year she began to tire easily, and at the age of 4 years cyanosis of the lips and nails was noted. She was breathless on moderate exertion. She was undersized for her age and weighed 53 lb. (24 kg.). Central and peripheral cyanosis was present. The pulse was regular and the blood-pressure was 104/70 mm. Hg. There was a left parasternal heave of right ventricular hypertrophy, but no thrill could be felt. On auscultation a loud coarse pulmonary ejection systolic murmur with a single second sound was heard. Femoral pulses were present. The liver was not palpable. Radiographs showed an increase in the transverse diameter of the heart with a cardiothoracic ratio of 55% and a prominent pulmonary artery segment. The right ventricle and right atrium were enlarged. The lung fields were under-vascularized (Fig. 1). The electrocardiogram (Fig. 2) showed right ven- tricular hypertrophy and strain. Cardiac catheterization was done under basal narcosis with rectal barbiturate and using local anaesthetic. The salient findings are listed in Table I. The diagnosis was 'valvular pulmonic stenosis with intact ventricular septum; small right-to-left shunt, probably via a patent foramen ovale'. In January 1959 open pulmonary valvotomy was performed under cardiopulmonary bypass using the disc oxygenator. The heart was arrested with potas- sium citrate. The pulmonary artery was opened and a cone-shaped pulmonary valve was encountered. No commissures were identifiable. The diaphragm was cut, converting it into a bicuspid valve with an esti- mated orifice diameter of 2-5 cm. A small patent foramen ovale was closed by direct suture. Convalescence was uneventful. Examination three weeks after operation revealed no cyanosis, and the systemic arterial pulse was col- lapsing in character. The blood-pressure was 120/60 mm. Hg. Jugular venous pressure was raised to the angle of the jaw due to tricuspid incompetence. The liver was not palpable. No adventitious sounds were audible in the lungs. On palpation of the precordium a systolic thrill under the left clavicle and a right ventricular left parasternal heave were felt. The first heart sound was loud. The pulmonary component of the second sound could not be heard. There was a coarse pulmonary ejection murmur (grade 4/6), stopping short of the second sound, and a rough pul- monary diastolic murmur. The patient was seen again at the age of 15 years in February 1964. She had remained well and been able to swim and play tennis until about a month previously, when she had begun to feel continually tired. She was now a well-developed adolescent. There was no cyanosis or respiratory distress. Prominent 'a' waves were noted in the jugular venous pulsa- tions. The marked left parasternal heave due to right ventricular enlargement persisted. There was a grade 2/6 pulmonary ejection systolic murmur and a grade 2/4 rough diastolic murmur of pulmonary incom- petence commencing 0-08 sec. after aortic valve closure (Fig. 3). TABLE I CARDIAC CATHETERIZATION 1958 Pressure 02 Site (mm. Hg) Saturation Systolic Diastolic (oximeter) Right pulmonary capillary| 5 3 96 Main pulmonary artery 15 8 35 Right ventricle 185 0-15 Right atrium a 11 (mean =6) Brachial artery 75 55 86 337 on 31 May 2018 by guest. Protected by copyright. http://thorax.bmj.com/ Thorax: first published as 10.1136/thx.21.4.337 on 1 July 1966. Downloaded from
Transcript of Homograft replacement the pulmonary valve -...

Thorax (1966), 21, 337.
Homograft replacement of the pulmonary valveDENIS N. FULLER, PAUL MARCHAND, MONTY M. ZION,
AND SAUL ZWI
From Johannesburg General Hospital and University of the Witwatersrand
Pulmonary incompetence is a common sequel ofpulmonary valvotomy, but many authors believethat the haemodynamic consequences of thisregurgitation are well tolerated (Talbert, Morrow,Collins, and Gilbert, 1963). In this paper wereport a patient who had severe pulmonary incom-petence after valvotomy and who failed to main-tain her initial clinical improvement. Because ofthe severe leak it was considered reasonable tocorrect the incompetence surgically. A homograftpulmonary valve was used, and we are unawareof any previous report of its use in man, thoughRoss, Cooper, and Brockenbrough (1961) de-scribed the experimental replacement of thepulmonary valve with a tricuspid semilunarprosthesis in dogs.
CASE REPORT
A 9-year-old white girl was seen in 1958. There wasa history of sweating and listlessness during infancy.After the age of 1 year she began to tire easily, andat the age of 4 years cyanosis of the lips and nailswas noted. She was breathless on moderate exertion.
She was undersized for her age and weighed 53 lb.(24 kg.). Central and peripheral cyanosis was present.The pulse was regular and the blood-pressure was104/70 mm. Hg. There was a left parasternal heaveof right ventricular hypertrophy, but no thrill could befelt. On auscultation a loud coarse pulmonary ejectionsystolic murmur with a single second sound washeard. Femoral pulses were present. The liver wasnot palpable.
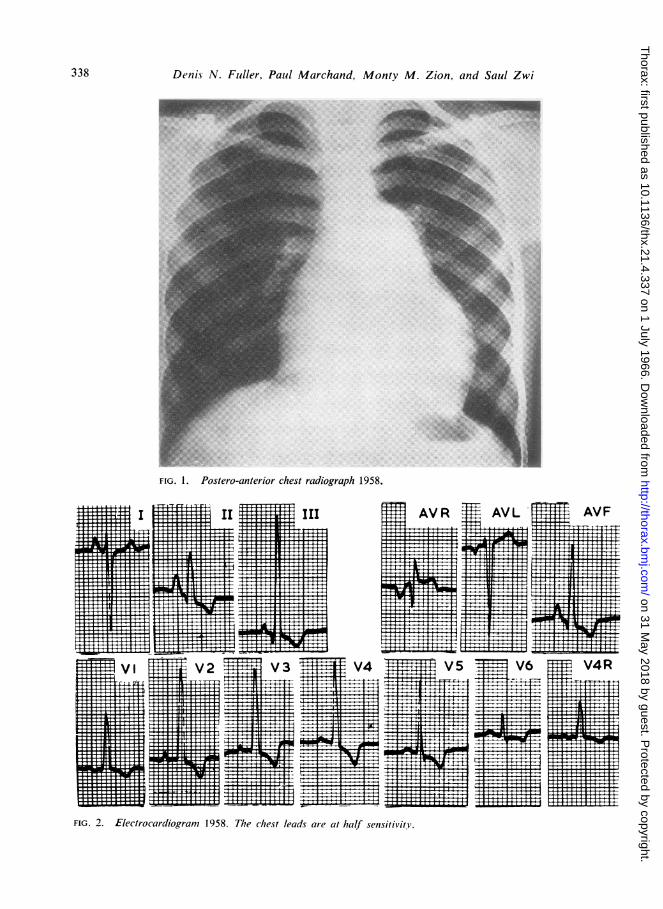
Radiographs showed an increase in the transversediameter of the heart with a cardiothoracic ratio of55% and a prominent pulmonary artery segment. Theright ventricle and right atrium were enlarged. Thelung fields were under-vascularized (Fig. 1).The electrocardiogram (Fig. 2) showed right ven-
tricular hypertrophy and strain.Cardiac catheterization was done under basal
narcosis with rectal barbiturate and using localanaesthetic. The salient findings are listed in Table I.The diagnosis was 'valvular pulmonic stenosis with
intact ventricular septum; small right-to-left shunt,probably via a patent foramen ovale'.
In January 1959 open pulmonary valvotomy wasperformed under cardiopulmonary bypass using thedisc oxygenator. The heart was arrested with potas-sium citrate. The pulmonary artery was opened anda cone-shaped pulmonary valve was encountered. Nocommissures were identifiable. The diaphragm wascut, converting it into a bicuspid valve with an esti-mated orifice diameter of 2-5 cm. A small patentforamen ovale was closed by direct suture.
Convalescence was uneventful.Examination three weeks after operation revealed
no cyanosis, and the systemic arterial pulse was col-lapsing in character. The blood-pressure was 120/60mm. Hg. Jugular venous pressure was raised to theangle of the jaw due to tricuspid incompetence. Theliver was not palpable. No adventitious sounds wereaudible in the lungs. On palpation of the precordiuma systolic thrill under the left clavicle and a rightventricular left parasternal heave were felt. The firstheart sound was loud. The pulmonary component ofthe second sound could not be heard. There was acoarse pulmonary ejection murmur (grade 4/6),stopping short of the second sound, and a rough pul-monary diastolic murmur.The patient was seen again at the age of 15 years
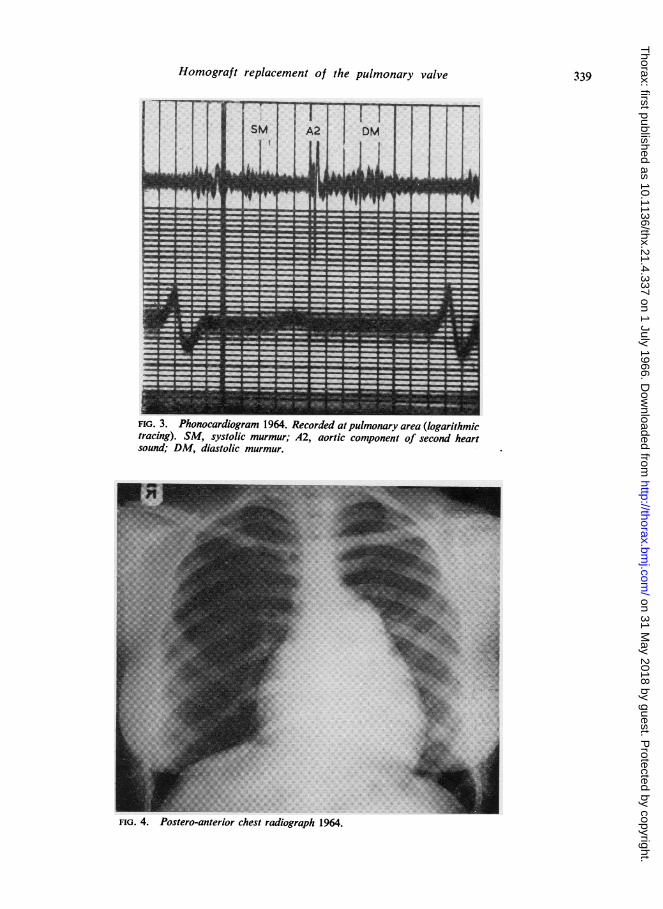
in February 1964. She had remained well and beenable to swim and play tennis until about a monthpreviously, when she had begun to feel continuallytired. She was now a well-developed adolescent. Therewas no cyanosis or respiratory distress. Prominent'a' waves were noted in the jugular venous pulsa-tions. The marked left parasternal heave due to rightventricular enlargement persisted. There was a grade2/6 pulmonary ejection systolic murmur and a grade2/4 rough diastolic murmur of pulmonary incom-petence commencing 0-08 sec. after aortic valveclosure (Fig. 3).
TABLE ICARDIAC CATHETERIZATION 1958
Pressure 02Site (mm. Hg) Saturation
Systolic Diastolic (oximeter)
Right pulmonary capillary| 5 3 96Main pulmonary artery 15 8 35Right ventricle 185 0-15Right atrium a 11 (mean =6)Brachial artery 75 55 86
337
on 31 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.4.337 on 1 July 1966. D
ownloaded from
Denis N. Fuller, Paul Marchand, Monty M. Zion, and Saul Zwi
FIG. 1. Postero-anterior chest radiograph 1958.
FIG. 2. Electrocardiogram 1958. The chest leads are at half sensitivity.
.+I
..
I
V6 XT tS V4RT x,XEL
- - r w T 1 r r tTTTT- o x r a
X _ __WT- ' . _ 1 . * _ _ : ^ S _ - 1l_.,, x _=1- x,
T-- T I_ _ _ w:xl _ - T I Tl!- - s TS - - _= y ' r T 14 1
tt .+ +^ _1ll ttT i w T r 1 - r z T T l T * *r I r * X r
T4t, ; 10t11t!111. ., I *T r r I s T XT T-TT I T X r r 1 T7 7 7 IT i i
338
on 31 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.4.337 on 1 July 1966. D
ownloaded from
Homograft replacement of the pulmonary valve
FIG. 3. Phonocardiogram 1964. Recorded atpulmonary area (logarithmictracing). SM, systolic murmur; A2, aortic component of second heartsound; DM, diastolic murmur.
FIG. 4. Postero-anterior chest radiograph 1964.
339
A A_
-.]L-- x
AL
Jr-------v
MIL I 9 XJL X -IL
__XMML_ -------- -Ar
--AL I-X IL --y
L7K X MEL-- -ILw N
JL___ N N ILJL X N JL-----AL
___JL_ X W Jr -X___X_ -X MK_ X X -AL -X __JF_
on 31 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.4.337 on 1 July 1966. D
ownloaded from
Denis N. Fuller, Paul Marchand, Monty M. Zion, and Saul Zwi
II III AVR AVL AVF
VI V2 V3 V4 Vs
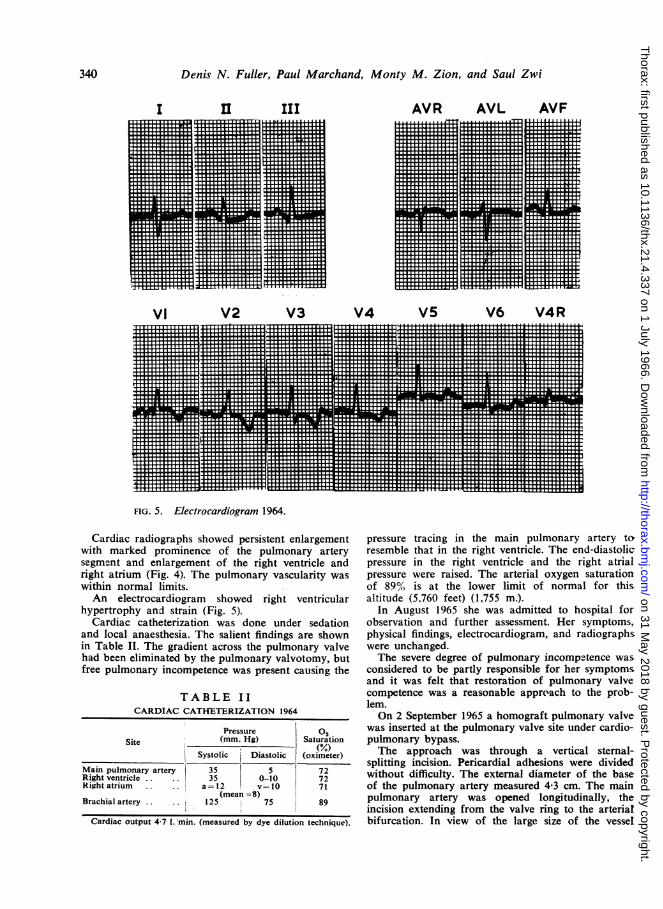
FIG. 5. Electrocardiogram 1964.
Cardiac radiographs showed persistent enlargementwith marked prominence of the pulmonary arterysegment and enlargement of the right ventricle andright atrium (Fig. 4). The pulmonary vascularity waswithin normal limits.An electrocardiogram showed right ventricular
hypertrophy and strain (Fig. 5).Cardiac catheterization was done under sedation
and local anaesthesia. The salient findings are shownin Table II. The gradient across the pulmonary valvehad been eliminated by the pulmonary valvotomy, butfree pulmonary incompetence was present causing the
TABLE IICARDIAC CATHETERIZATTON 1964
Pressure 02Site (mm. Hg) Saturation
Systolic Diastolic (oximeter)
Main pulmonary artery 35 5 72Right ventricle 35 0-10 72Right atrium a= 12 v= 10 71
-(mean-8)Brachial artery 125 75 89
Cardiac output 4-7 1. 'min. (measured by dye dilution technique).
pressure tracing in the main pulmonary artery topresemble that in the right ventricle. The end-diastolicpressure in the right ventricle and the right atrialpressure were raised. The arterial oxygen saturationof 89% is at the lower limit of normal for thisaltitude (5,760 feet) (1,755 m.).
In August 1965 she was admitted to hospital forobservation and further assessment. Her symptoms,physical findings, electrocardiogram, and radiographswere unchanged.The severe degree of pulmonary incompetence was
considered to be partly responsible for her symptomsand it was felt that restoration of pulmonary valvecompetence was a reasonable approach to the prob-lem.On 2 September 1965 a homograft pulmonary valve
was inserted at the pulmonary valve site under cardio-pulmonary bypass.The approach was through a vertical sternal-
splitting incision. Pericardial adhesions were dividedwithout difficulty. The external diameter of the baseof the pulmonary artery measured 4-3 cm. The mainpulmonary artery was opened longitudinally, theincision extending from the valve ring to the arterialbifurcation. In view of the large size of the vessel
I
V6 V4R.. I. 1.
... ....
.
im.WNWHERH. . . . .I . ti 1 1:1:i 1 n -t t m 1
.............................
340
on 31 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.4.337 on 1 July 1966. D
ownloaded from

Homograft replacement of the pulmonary valve
excellent exposure was provided. It was possible toidentify three blunt commissures, but the remnantsof the cusps were thickened and -retracted, formingnarrow ledges which could not possibly approximate.They were excised at their bases. A freeze-dried pul-monary valve homograft taken from a youth whohad been killed accidentally three months previouslywas rehydrated with a saline solution containingpenicillin and streptomycin. The stretched diameterof the reconstituted homograft, measured with aTubbs dilator, was 4-2 cm. and the internal stretcheddiameter of the host's pulmonary arterial ring usingthe same instrument was 3-8 cm. The arterial wall ofthe homograft had been cut about 2 mm. clear ofthe cusp bases and commissures, and below the cuspsas much muscle as possible had been removed up toand following the curve of the cusp bases.The insertion of the homograft in this position was
technically easier than the equivalent replacement ofan aortic valve because of the large size of both thehost's artery and the homograft. Three 4-0 silkanchoring sutures were placed precisely below thesite of the host's commissures. These were thenbrought through the base of the homograft in thesame relative positions and were tied. The commis-sural pillars of the homograft were then fixed withmattress sutures passed through the pulmonary arterywall at the precise situation of the commissural rem-nants and were tied externally over teflon pledgets.The fringes of pulmonary artery left attached to the
- - __ -4---;7 -q izF.' r ..5j ;.I
7 ._._...E_ss|j --~-I~z 111 ;A _ . ..
Eiell-7-f---,sm
1+:?~~~~@-.
nm.Hg
20
1I5
I0
5
0
homograft were then sewn to the remnants of thebases of the host's cusps with continuous 5-0 silksutures. These remnants were not always clearlyidentifiable, and in parts the suturing had to be madedirectly to the pulmonary artery endothelium alongan estimated curve. On completion the graft satsnugly in its bed and the cusps were free and mobile.The artery was then repaired.Throughout the 70 minutes' bypass the heart re-
mained in sinus rhythm and no difficulties wereexperienced when coming off the pump.
Pressures recorded by direct needle puncture of thepulmonary artery before bypass showed a closeresemblance to ventricular pressure curves (Fig. 6A).After replacement of the pulmonary valve the pul-monary artery pressure tracing (Fig. 6B) revealednormal features but with a Venturi effect in earlysystole. There was a peak systolic gradient of 10 mm.Hg across the homograft valve.
Convalescence was rapid and free of complica-tions.
Clinical examination three weeks after operationrevealed persistence of the prominent "a" waves inthe jugular venous pulsations and of the right ven-tricular enlargement. On auscultation (Fig. 7) therewas a grade 3/6 pulmonary ejection systolic murmur,and both aortic and pulmonary components of thesecond heart sound were clearly audible. Movementof the components of this sound with respirationwas normal.t ' f _ So_ { t-- tS . . 4 <. . t ; { _ 4_. ....4. i_... -_-4_ _ ' t: - @ @- t . - . ' t
*S 4 A__4 M-i-t_q _ - _ _ & ., .p_ .,. ,.d_ _ __4S_ 4* 4 5--+* + * i j X @ t -t.---B-9---b'* }-t -S x- 1 z-tv- IJ - R- | t > --t--- *-tt t>-m-j | {8-8 t4t}t.^ 1 .- _. 1 .. ___t ._°- . - 1 -' . i . | - A: . _ | t t_ _ . ... W . t - - - m4= .4 -* + ^ S 1 -- S _ 4 _ * _ - | A <- t ^, , W i ^ 2, , *, | W . 4 . | | , .e . + ,, t "- - t 9 i rr, § u t e s | "FFWEz 1 v -t 1 Z i 3 I 4tsetr*rne- ---1'-''''-'----!- i- --!----,-t-7,---1' ---!-----Tbtat--- !--u-tz ----t-- -+u-^- '---------+---l*i ----t-----;-----'! l. .-.-l t-t t | | t + o:ti ; * _ _ _4 te 6 - j - -------4- _I - 4|wi1 | ---. . * - - - i - - | j -**----*-n 1 1 I t W w | * . @ >S 3 i I I I -! i
1- l 8 -1 - ----F- - | 4 - t -i-> --- - ----i------ | C- -------tt - --- l"t HE----l------------*w------+-----|+|--^-^|-l---w-r--t.-*nt s ,.P ._ s ; s _ t t . :2 } \ . t jwEe7 *_._ .sl ..tDlI 1<Atlt 1--+4 b-- t'-- | t | a, V I I 1 :1;
-r-3i u wtn n t*l__t..tw-- t- _nnXm -u.w =|- -s z w t..sn
'.F wI t I i t ^4 1 -1- i i-:i 8 -s t:Xx 4i-m-'*' t5- - }- -l-----;-i--w->u-!--*---l----<'-i--'-i-7-9u l--n*-^^-w i--*t
z ---- - - - - a - -- ; - - - --- ---- - - t - -- w - - w -- ----- -4--- - - t; - --T | ;; - 8- - W4te-q--;;17L-..|...;.: - .1 1 >i 1 ..1 -.4.^tt -W^^ tS.f^+-L.S,.,:1--r.:aiP ;l;----t-,:.Imn
PAPER SPEED 50mm./sec.FIG. 6. Intra-operative pressure tracings by direct needle puncture ofpulmonary artery. (A) Pulmonary artery pres-sure before valve insertion; (B) pulmonary artery pressure after valve insertion.
341
on 31 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.4.337 on 1 July 1966. D
ownloaded from

Denis N. Fuller, Paul Marchand, Monty M. Zion, and Saul Zwi
FIG. 7. Phonocardiogram September 1965, three weeksafter surgery, recorded at pulmonary area (logarithmictracing). SM, systolic murmur; A, aortic, and P, pulmonarycomponent ofthe second heart sound.
The electrocardiogram and radiographs were un-changed.
SUMMARY AND CONCLUSIONS
A case of pulmonary incompetence followingpulmonary valvotomy with treatment by insertion
of a pulmonary valve homograft is reported. Thetechnique of the operation is described.The operation was not difficult, particularly as
coronary artery perfusion was not required. Thepulmonary valve homograft was not particularlyflimsy, and it held sutures without difficulty.
Clinical evidence to date suggests competenceof the pulmonary valve.The clinical and haemodynamic response will
be fully assessed one year after operation.
We wish to express our thanks to Dr. H. Pretoriusfor permission to reproduce the electrocardiogram inFig. 2, and to Mr. A. Shevitz for his assistance withall the reproductions.
REFERENCESRoss, J., Jr., Cooper, T., and Brockenbrough, E. C. (1961). Experi-
mental replacement of the pulmonic valve with a tricuspidsemilunar prosthesis. J. thorac. cardiovase. Surg., 42, 371.
Talbert, J. L., Morrow, A. G., Collins, N. P., and Gilbert, J. W. (1963).The incidence and significance of pulmonic regurgitation afterpulmonary valvulotomy. Anier. Heart J., 65, 590.
342
on 31 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.21.4.337 on 1 July 1966. D
ownloaded from


















