Homocystine-Induced Arteriosclerosis · 2014. 1. 30. · Fromthe DepartmentsofMedicine, Pathology,...
11
Homocystine-Induced Arteriosclerosis THE ROLE OF ENDOTHELIAL CELL INJURY AND PLATELET RESPONSE IN ITS GENESIS LAURENcE A. HABun, RussEu. Ross, SHiERILL J. SuaCfrx=, and C. RONALD Scowr From the Departments of Medicine, Pathology, Pediatrics, and the Regional Prinate Research Center, University of Washington School of Medicine, Harborview Medical Center and the Puget Sound Blood Center, Seattle, Washington 98104 A B S T R A C T The atherogenic mechanism of homo- cystinemia has been defined by measuring endothelial cell loss and regeneration, platelet consumption, and intimal lesion formation in a primate model. Three groups of baboons were studied: (a) 8 control animals; (b) 15 animals after 3 mo of continuous homocystin- emia; and (c) 11 animals after 3 mo of combined homocystinemia and oral treatment with dipyridamole. Experimental homocystinemia caused patchy endo- thelial desquamation comprising about 10% of the aortic surface despite a 25-fold increase in endothelial cell re- generation. Neither endothelial cell loss nor regenera- tion was changed significantly by dipyridamole. Homo- cystine-induced vascular deendothelialization produced a threefold increase in platelet consumption that was in- terrupted by dipyridamole inhibition of platelet function. All homocystinemic animals developed typical arterio- sclerotic or preatherosclerotic intimal lesions composed of proliferating smooth muscle cells averaging 10-15 cell layers surrounded by large amounts of collagen, elastic fibers, glycosaminoglycans, and -sometimes lipid. Intimal lesion formation was prevented by dipyridamole therapy. We conclude that homocystine-induced endo- thelial cell injury resulted in arteriosclerosis through platelet-mediated intimal proliferation of smooth muscle cells that can be prevented by drug-induced platelet dysfunction. INTRODUCTION Lesions of atherosclerosis, identical to those found in man, are readily produced in the subhuman primate Received for publication 18 December 1975 and in revised form 15 April 1976. (1-4). Intimal proliferative smooth muscle cell lesions, identical in appearance to the fibromusculoelastic lesion considered to be the precursor of atherosclerosis in man, are transiently produced in the arteries of nonhuman primates by a variety of methods including mechanical deendothelialization (5-8). Furthermore, the addition of a fatty diet, either alone or in combination with mechanical injury, can produce the classic lesions of atherosclerosis, the fatty streak and the fibrous plaque (9, 10). The genesis of these lesions may involve: (a) endothelial injury leading to focal desquamation of cells; (b) adherence and aggregation of platelets to exposed subendothelial connective tissue; (c) local release of platelet constituents, including a platelet mitogenic fac- tor (11), and passage of plasma constituents into the underlying artery wall; (d) migration of smooth muscle cells through fenestrae of the internal elastic lamina into the intima and platelet-mediated intimal prolifera- tion of smooth muscle cells; (e) formation of connective tissue matrix by the smooth muscle cells through syn- thesis and secretion of collagen, elastic fiber proteins, and glycosaminoglycans; and (f) intracellular and ex- tracellular lipid accumulation. Maximal lesion formation occurs within 3 mo after mechanical injury. The lesions appear to regress once the overlying endothelium has regenerated, and resolution is virtually complete 3 mo later in normocholesterolemic monkeys (6). This for- mulation suggests that repeated or chronic endothelial cell loss may be the first event leading to atherosclerosis. In this study we test the proposition that chronic, chemically induced endothelial cell injury produces ar- teriosclerosis through platelet-mediated intimal prolifera- tion of smooth muscle cells and that drug-induced plate- let dysfunction is capable of preventing the smooth muscle proliferative response. The Journal of Clinical Investigation Volume 58 September 1976 -731-741 731
Transcript of Homocystine-Induced Arteriosclerosis · 2014. 1. 30. · Fromthe DepartmentsofMedicine, Pathology,...

Homocystine-Induced Arteriosclerosis
THE ROLEOF ENDOTHELIALCELL INJURY AND
PLATELET RESPONSEIN ITS GENESIS
LAURENcEA. HABun, RussEu. Ross, SHiERILL J. SuaCfrx=, andC. RONALDScowr
From the Departments of Medicine, Pathology, Pediatrics, and the RegionalPrinate Research Center, University of Washington School of Medicine,Harborview Medical Center and the Puget Sound Blood Center,Seattle, Washington 98104
A B S T R A C T The atherogenic mechanism of homo-cystinemia has been defined by measuring endothelialcell loss and regeneration, platelet consumption, andintimal lesion formation in a primate model. Threegroups of baboons were studied: (a) 8 control animals;(b) 15 animals after 3 mo of continuous homocystin-emia; and (c) 11 animals after 3 mo of combinedhomocystinemia and oral treatment with dipyridamole.
Experimental homocystinemia caused patchy endo-thelial desquamation comprising about 10% of the aorticsurface despite a 25-fold increase in endothelial cell re-generation. Neither endothelial cell loss nor regenera-tion was changed significantly by dipyridamole. Homo-cystine-induced vascular deendothelialization produceda threefold increase in platelet consumption that was in-terrupted by dipyridamole inhibition of platelet function.
All homocystinemic animals developed typical arterio-sclerotic or preatherosclerotic intimal lesions composedof proliferating smooth muscle cells averaging 10-15cell layers surrounded by large amounts of collagen,elastic fibers, glycosaminoglycans, and -sometimes lipid.Intimal lesion formation was prevented by dipyridamoletherapy. We conclude that homocystine-induced endo-thelial cell injury resulted in arteriosclerosis throughplatelet-mediated intimal proliferation of smooth musclecells that can be prevented by drug-induced plateletdysfunction.
INTRODUCTION
Lesions of atherosclerosis, identical to those found inman, are readily produced in the subhuman primate
Received for publication 18 December 1975 and in revisedform 15 April 1976.
(1-4). Intimal proliferative smooth muscle cell lesions,identical in appearance to the fibromusculoelastic lesionconsidered to be the precursor of atherosclerosis in man,are transiently produced in the arteries of nonhumanprimates by a variety of methods including mechanicaldeendothelialization (5-8). Furthermore, the additionof a fatty diet, either alone or in combination withmechanical injury, can produce the classic lesions ofatherosclerosis, the fatty streak and the fibrous plaque(9, 10). The genesis of these lesions may involve: (a)endothelial injury leading to focal desquamation of cells;(b) adherence and aggregation of platelets to exposedsubendothelial connective tissue; (c) local release ofplatelet constituents, including a platelet mitogenic fac-tor (11), and passage of plasma constituents into theunderlying artery wall; (d) migration of smooth musclecells through fenestrae of the internal elastic laminainto the intima and platelet-mediated intimal prolifera-tion of smooth muscle cells; (e) formation of connectivetissue matrix by the smooth muscle cells through syn-thesis and secretion of collagen, elastic fiber proteins,and glycosaminoglycans; and (f) intracellular and ex-tracellular lipid accumulation. Maximal lesion formationoccurs within 3 mo after mechanical injury. The lesionsappear to regress once the overlying endothelium hasregenerated, and resolution is virtually complete 3 molater in normocholesterolemic monkeys (6). This for-mulation suggests that repeated or chronic endothelialcell loss may be the first event leading to atherosclerosis.
In this study we test the proposition that chronic,chemically induced endothelial cell injury produces ar-teriosclerosis through platelet-mediated intimal prolifera-tion of smooth muscle cells and that drug-induced plate-let dysfunction is capable of preventing the smoothmuscle proliferative response.
The Journal of Clinical Investigation Volume 58 September 1976 -731-741 731

METHODS
Baboon homocystine vascular model. 34 normal malebaboons (Papio cynocephalus) were studied: 8 controls, 15chronic homocysteine infusion animals, and 11 animals receiv-ing both chronic homocysteine infusions and dipyridamole. Theanimals weighed 10-12 kg and had hematocrits of 40±3%o,leukocyte counts of 5,000±1,200/,pl, and platelet counts of279,000+59,000/,l. They were free of tuberculosis, de-wormed, and observed to be disease-free for at least 6 wkbefore use. To facilitate continuous intravenous infusion andrepeated blood sampling, the animals were maintained inrestraining chairs during the period of observation. In addi-tion, a femoral arteriovenous Silastic shunt was used, 0.24cnm internal diameter and 25 cm in length, with Dacronsewing cuffs at skin exit sites (12-14).
A solution of l-homocysteine (Aldrich Chemical Co., Inc.,Milwaukee, Wis.) or a control solution alone was infusedcontinuously by femoral AV shunt throughout a 3-moperiod using a roller infusion pump (Holter pump, model921, Extracorporeal Medical Specialties, Inc., King ofPrussia, Pa.) and a T-tube connector. 0.3 g of homocys-teine per kg body weight was infused per day (3 g dis-solved in 100 ml 0.15 M NaCl solution at pH 7.4 andsterilized by filtration). The homocysteine infusion wasgiven at a rate of about 4 ml/h and produced plasma homo-cystine levels of 0.1-0.2 mMdue to the endogenous trans-formation of homocysteine to homocystine. Homocystineconcentrations were measured each week. Platelet andfibrinogen concentration, survival and turnover, were mea-sured before and at monthly intervals during the infusionperiod. Plasma cholesterol levels were obtained before theinfusion studies and before sacrifice.
Treatmentt. Dipyridamole was given orally to 11 animalsthroughout the 3-mo period of homocysteine infusion indoses of 30 mg/kg per day (in three divided doses). Thisdose, which is a threefold increase over that used in theacute studies (14), was required to normalize the plateletconsumption produced by the level of chronic homocystin-emia used in this study.
Laboratory studies. Platelet counts were measured withan electronic particle counter on peripheral blood collectedin EDTA by a previously described method (15, 16). Themean platelet count of 50 normal baboons was 279,000±59,000/pl (±1 SD). Platelet survival was determined fromthe disappearance of radioactivity from blood sampled 5-10times after injection of autologous 51Cr-labeled platelets(14, 16). In this procedure 100 ml autologous whole bloodwas collected directly into a plastic plasma pack (FenwallTA-6, Fenwall Laboratories, Inc., Morton Grove, Ill.) con-taining 20 ml ACD anticoagulant, and centrifuged at 200 gfor 10 min at room temperature. The supernatant, platelet-rich plasma was transferred to a second transfer bag bya plasma extractor, and the pH was adjusted to 6.5 with0.15 M citric acid (about 0.1 ml/10 ml plasma). Plateletswere then formed into a pellet by centrifuging at 3,000 9for 15 min. The supernatant plasma was removed exceptfor 2-3 ml residual plasma into which the platelets werecarefully resuspended. This platelet suspension was thenincubated with 50 /LCi of radiochromium (New EnglandNuclear, Boston, Mass.) for 20 min. About 40 ml nonradio-active platelet-poor plasma and about 50 ml sterile air werethen added, and the pellet reformed by centrifuging at 3,000g for 15 min. The residual radioactive platelet-poor plasmawas completely decanted without disturbing the pellet. 10 mlnonradioactive platelet-poor plasma was carefully layeredover the platelet pellet and then discarded by decantation.
This maneuver washed the bag of more than 95% of theresidual nonplatelet-bound 5"Cr. The presence of air in thebag facilitated this step by maintaining the overall con-figuration of the bag during decantation. The labeled plateletpellet was gently suspended in about 2 ml nonradioactiveplatelet-poor plasma. Contaminating erythrocytes werelargely removed by a final slow centrifugation of 100 gfor 5 min. A known amount of 51Cr-labeled platelet sus-pension was administered to the animal by intravenous in-jection after the preparation of a standard. 3-ml samples ofwhole blood, collected in EDTA twice daily for 3 days anddaily for an additional 3 days, were lysed with 0.1 mlsodium dodecyl sulfate and counted for radioactivity in agamma spectrometer (Nuclear-Chicago, Des Plaines, Ill.).Platelet survival time was determined by computer leastsquares fitting to a gamma function as described by Paulus(17) and Mlurphy et al. (18-20). The proportion of labeledplatelets remaining within the systemic circulation after in-fusion (i.e., "recovery") was calculated from the plateletactivity per milliliter extrapolated to zero time, multipliedby the estimated blood volume, and divided by the platelet51Cr activity injected. Platelet consumption, measured asplatelet turnover per microliter of blood per day, was calcu-lated from the peripheral platelet count divided by theplatelet survival time in days and corrected for recovery.In 24 normal male baboons, platelet survival was 5.5±0.3days. Platelet recovery averaged 85±5% and platelet turn-over was 59,000±7,000 platelets/pl per day.
For calculating fibrinogen turnover, the concentration offibrinogen was estimated by a spectrophotometric method inwhich the optical density of thrombin-clottable protein wasdetermined after collection on a glass rod and subsequentsolution in alkaline urea (21). The fibrinogen concentrationin 24 normal animals was 2.71±0.22 mg/ml. Labeling ofnormal fibrinogen with "2I was performed by the methodof Takeda (22). This technique involved repeated precipi-tation of fibrinogen with 257% ammonium sulfate saturationfollowed by dissolving the precipitate in 0.005 M sodiumcitrate, labeling with ['"I] Cl (monoiodochloride) and re-moval of unbound "I. The solution was maintained at 4°Cfor 1 h and then centrifuged at 20,000 g for 30 min at 4'Cto remove any cryoprecipitable material. It was sterilizedby filtration. In our preparations, the molar ratio of iodineto fibrinogen was always less than 0.25; the fibrinogen was95 % clottable (range, 92-98%). For survival measurementssufficient labeled fibrinogen was prepared for several monthsuse. Individual doses were flash frozen and stored at - 85°C.Survival did not change significantly during the time ofstorage. Fibrinogen survival, determined from the half-timedisappearance and divided by the natural logarithm of 2,averaged 2.6±0.2 days in 24 normal animals. Fibrinogenturnover, used as a measure of fibrinogen consumption, wascalculated from the concentration of plasma fibrinogendivided by its mean survival time. In 24 normal animalsfibrinogen turnover averaged 1.00±0.10 mg/ml per day.
Platelet function was measured by bleeding time, glass-bead retention test, and aggregation induced by ADP (0.5,1.0, 1.5, 2.0, and 10.0 ,uM final concentration), collagen (5,g/ml), and epinephrine (2.5 Ag/ml). The bleeding timewas measured by the standardized template technique (23),the mean value in 24 normal baboons was 4.0+1.2 min.Platelet retention by glass-bead columns was measured bythe Bowie modification of the Salzman method (24), bloodbeing drawn by a two-syringe technique without anticoagu-lant and immediately passed through the standard columnof beads by constant infusion at the rate of 2 ml/min. The
732 L. A. Harker, R. Ross, S. J. Slichter, and C. R. Scott

delay between drawing and initiation of flow through thebeads was less than 10 s. Platelet aggregation was esti-mated from changes in optical transmission of 0.02 Msodium citrated plasma at 37° C with a concentration of300,000 platelets/pul (14, 25, 26). Plastic equipment was usedthroughout, and plasma freshly drawn was kept at roomtemperature during the 30-70 min before testing.
Homocystine was quantified by column chromatographyusing a modified procedure of Spackman et al. (27).Plasma samples were deproteinized by addition of an equalvolume of 6%o sulfosalicyclic acid buffered to pH 2. Homo-cystine was separated on a 55-cm column of PA28 resin(Beckman Instruments, Inc., Palo Alto, Calif.) with useof 0.38 M sodium citrate buffer at pH 4.40. Temperaturewas maintained at 62°C with a buffer flow rate of 60 ml/hand the amino acid was eluted 62 min after addition ofbuffer. Homocystine is not detectable in the plasma ofncrmal animals.
Morphological procedures. Three types of vessel prepa-ration were obtained: (a) lower abdominal aorta, iliac andfemoral arteries for light and electron microscopic examina-tion of lesion formation; (b) carotid arteries for [3H]thy-midine incorporation by endothelial cells; (c) thoracic andupper abdominal aorta for silver stain quantitation of endo-thelial coverage. Specimens were obtained under general(halothane) anesthesia and assisted respiration in the fol-lowing way. After opening the abdomen, the aorta andinferior vena cava were carefully freed by sharp dissectionwithout affecting flow. The inferior vena cava was thencannulated to establish isolated venous drainage from thelower limbs and immediately thereafter the aorta was can-nulated, flushed free of blood elements with 5%o glucosesolution at 100 mmHg of hydrostatic pressure, and perfuse-fixed with buffered half-strength Karnovsky's fixative (28)under 100 mmHg pressure for 20 min in vivo. Once per-fusion fixation of the distal arteries was underway, thecarotid arteries were freed by sharp dissection, isolated, andcarefully removed. The artery segments were gently flushedfree of blood with saline, and excess adventitia removedfor [3H]thymidine studies. Immediately after removing thecarotid arteries, the chest was entered (thereby interruptingrespiration), the arch of the aorta quickly cannulated, anddrainage outflow was established above the renal arteries.The aorta was then cleared of blood using 5% glucosesolution at 100 mmHg pressure. In vivo fixation was thencarried out by perfusion-fixation of the thoracic and upperabdominal aorta with 0.3%o silver nitrate solution at apressure of 100 mmHg for 20 min (29). After perfusion-fixation, the vessels were removed by sharp dissection. Theforegoing- procedure ensured the procurement of three dif-ferent artery preparations from a single living animal whileusing isolated regional pressure-perfusion fixation.
Initimal lesion score. At the time of sacrifice the aortawas cannulated below the renal vessels, flushed free of bloodwith 5% glucose solution, and then perfuse-fixed withbuffered half-strength Karnovsky's fixative (28) under 100mmHg hydrostatic pressure for 20 min in vivo. Vesselswere subsequently removed by sharp dissection and placedin half-strength Karnovsky's fixative for 6 h at 4°C. Seg-ments from abdominal aorta, and each iliac artery wereremoved for scanning electron micrographs. The remainingvascular tissues were subsequently cut into approximately1-mm rings and returned to the fixative for another hourat 4°C. They were then washed in 0.1 M cacodylate buffercontaining 0.2 M sucrose (pH 7.3) and subsequently post-fixed in lgo osmium tetroxide buffered with s-collidine or
with phosphate buffer (pH 7.3) for 11 h, followed by enbloc staining with 2% uranyl acetate for i h. After em-bedding in epoxy resin, 1-,um thick sections were cut ascircles, and stained with a combination of basic fuchsinand azure II-methylene blue for light microscopy (30).Selected thin sections were cut at approximately 800 Athickness for transmission electron microscopy. These sec-tions were stained with lead citrate followed by uranylacetate. All of the sections for electron microscopy wereexamined in an AEI801 electron microscope (AEI Scien-tific Apparatus Inc., Elmsford, N. Y.).
Five random sections were prepared for each of fivevessels (abdominal aorta, right and left iliac arteries, rightand left femoral arteries) for light microscopic scoring ofintimal lesions. The lesions were graded by two observersin a 'blind' manner according to the cell layer depth of inti-mal smooth muscle cells: grade 0-only occasional intimalsmooth muscle cells; grade 1-1-5 cells deep; grade 2-6-10cells; grade 3-11-15 cells; grade 4-16-20 cells; grade5- > 20 cells deep. The overall score was calculated foreach animal by summing the scores of all 25 sections exam-ined (possible range of scores was 0-125).
[3H] Thymidine labelintg intdex. Both carotid arterieswere removed by sharp dissection, flushed with saline, andcut into 20-mm lengths. Whole segments were placed in 3-4ml medium TC 199 containing 1 /Ci ['H]thymidine/ml andincubated at 37°C for 4 h. The vessel segments were re-moved, trimmed, opened longitudinally, and mounted flat forfixing 24 h in 10%o neutral buffered formaldehyde (31). Theendothelium was prepared for autoradiography by the methodof Schwartz and Benditt (32) which involved the followingprocedures. The luminal surface of the specimen was em-bedded in collodion onto a slide leaving the adventitialsurface exposed. The adventitial surface was then embeddedin gelatin and bonded to a gelatin-coated slide by fixationwith formaldehyde while the specimen and the coated slidewere held together under pressure. Subsequently the col-lodion overlying the endothelial cells was removed withether and alcohol thereby exposing the luminal surface ofendothelial cells for coating with autoradiographic emulsion.Autoradiography was performed by hand dipping endothelialmounts in Kodak NTB-2 emulsion, 2-wk exposure, followedby Kodak D-19 developer and rapid fixer (Eastman KodakCo., Rochester, N. Y.). The preparations were stained withHarris' hematoxylin and mounted.
About 80%o of the mounts were complete, containing over90%o of the endothelial cells intact and countable. All ofthe endothelial cells from each mount, i.e., 15,000 cells each,were scored as labeled or unlabeled, and the [3H]thymidinelabeling index represented the ratio of these values ex-pressed as a percentage.
Entd othelial cell loss. Pressure-perfusion fixation wascarried out on the thoracic and upper abdominal aorta with0.3%o silver nitrate solution at the time of sacrifice in vivo.The entire endovascular surface of whole-aorta mounts wasthen examined morphometrically by means of a grid micro-meter, and the proportion of the surface not covered byendothelial cells was determined.
RESULTS
Endothelial cell inijury. Endothelial cell coverage wascompletely intact (Fig. la) in the eight control animalswhen the vessels were prepared by pressure-perfusionfixation in vivo using either 0.3% AgNO3 staining orscanning electron microscopy. Patchy endothelial cell
Homocystine-Induced Arteriosclerosis 733

'9~~~~~'-***
W~~ -
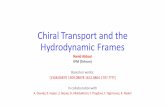
FIGURE 1 (a) Light micrograph demonstrating an en faceview of the aor.tic endothelium of a control baboon thatwas perfuse-fixed with 0.3% silver nitrate. The longitudinaldirection and the intact state of the endothelial cells can heclearly seen in this micrograph. The edges of the micro-graph are out of focus because of curvature of the vessel.Magnification X 220. (b) The aorta o)f a baboon that washomocystinemic for 3 mo. The patchy loss of the endothelium,and individual discrete areas of intense staining with silvernitrate demonstrate both focal desquamation of the endo-thelium, individual cell loss, and sites of alterations in thejunctions between the cells. Magnification X 200.
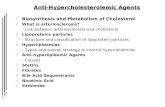
loss was observed in all animals made homocystinemicby continuous infusions of homocysteine (Fig. ib).When viewed by scanning electron microscopy, plateletswere found to accumulate at some sites of endothelialcell loss (Fig. 2), although platelets were not regularlyobserved on the chronically denuded areas when pre-pared by silv,er staining for direct microscopic examina-tion. The overall loss of aortic endothelium in the groupof 15 homocystinemic animals averaged 9.6±2.2% 1 ofthe aortic surface and corresponded with a mean plasmahomocystine concentration before sacrifice of 0.17±0.01mM(Table I). A linear relationship was observed be-
' In results variation about the mean is given at ±+1 SEM.
FIGuRE 2 Scanning electron micrograph of an area ofendothelial desquamation with adherent platelets and eryth-rocytes at these foci in an homocystinemic animal. The in-dividual platelets are obscured in the micrograph due to therelatively low magnification. However, their size can beestimated by comparing them with the erythrocytes whichare clearly visible. Magnification X 500.
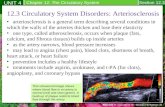
tween endothelial cell loss and homocystine concentra-tion (Fig. 3) with r =0.965. The regression line, repre-sented by y = 88.5x - 5.23, had an SD of 2.001, and
30-
20
a-
e 10
Q:
0
.
0
a
0
0.1 0.2 0.3
Plasma homocystine concentrotion (mM)
FIGURE 3 Correlation between homocystine level and endo-thelial cell loss. The desquamation of aortic endothelial cellswas directly related to the plasma concentration of homo-cystine (0) with r = 0.965 and P < 0.001. The computedregression line is shown (y = 88.5x - 5.23). Dipyridamoletreatment (A) did not alter the relationships between homo-cystine concentration and endothelial cell desquamation.
734 L. A. Harker, R. Ross, S. J. Slichter, and C. R. Scott
%,"W,4, ,
w --1s, I. I
'. U. '.'.YI . . ,

TABLE IHomocystine-Induced Endothelial Cell Desquamation, Platelet Consumption, and Endothelial Regeneration
Plasma Platelet [3H]thymidine-homocystine Endothelial labeling
Baboons concentration cell loss Survival Turnover index
mM % days plat/ld/day %Control (8) <0.001 0 5.4±0.1* 63,00044,000 0.001140.0001Homocystinemic (15) 0.170i0.019 9.6t42.2 2.8t40.3 183,000t±17,000 0.0296t±0.0087Dipyridamole-treated homocystinemic (11) 0.127 ±0.011 7.0-40.9 4.840.2 76,000±11,000 0.0162±-0.0051
* Variation about the mean given as ±1 SE.$ Significantly different from base line at P < 0.001.
an SD of slope and intercept of 7.205 and 1.359, re-spectively.
In the 11 homocystinemic animals treated with oraldipyridamole (30 mg/kg per day), 7.0+0.9% of theaortic endothelial cells was absent with a mean plasmahomocystine concentration before sacrifice of 0.13±0.01mM(Table I). The relationship between homocystinelevel and endothelial cell desquamation was not changedby dipyridamole treatment (P > 0.75).
Platelet consumption. Platelet survival in the homo-cystinemic animals was reduced to 2.8±0.3 days com-pared with 5.4±0.1 days in the control group (Table I).Reciprocally, platelet turnover was increased threefoldin the homocystinemic animals, i.e., 183,000+17,000platelets/isl per day compared with 63,000+4,000 plate-lets/,*l per day in the control group. Platelet survivaltimes were related to the logarithm of the homocystineconcentration (Fig. 4A). r = 0.965, P < 0.001, and theregression line was represented by y = 0.453e'-'.
Determinations of platelet survival also correlatedwith the logarithm of aortic endothelial cell loss (Fig.4B). r = 0.958, P < 0.001, and the regression line wasrepresented by y = 44.0ez'7.
Platelet survival times were significantly prolongedby dipyridamole treatment (4.8+0.2 days compared with2.8±0.3 days, P < 0.001) despite continued homocystin-emia (Fig. 4A and 4B). Platelet turnover was alsoreturned to near normal values (Table I, P < 0.001).
In homocystinemic animals fibrinogen survival andturnover were not changed significantly from controlvalues, i.e., 2.4±0.2 days and 1.2±0.2 mg/ml per day,respectively, compared with 2.5±0.2 days and 1.1 mg/ml per day in control animals. Fibrinogen kinetics werenot altered by dipyridamole treatment (2.4+0.2 daysand 1.3±0.3 mg/ml per day, respectively).
Platelet aggregation to ADP, epinephrine, and col-lagen was not significantly different in six dipyrida-mole-treated animals compared with six untreated homo-cystinemic animals. Similarly, the bleeding time wasnot significantly prolonged by dipyridamole therapy(4.8+2.5 min compared with 4.2±2.0 min). However,dipyridamole treatment reduced platelet retention by
glass-bead columns from 43±12% retained in homo-cystinemic animals to 26±9% in treated animals (P<0.05).
Endothelial cell regeneration. In control animals the['H]thymidine-labeling index of endothelial cells aver-aged 0.0011+0.0001%. Animals with induced homocys-tinemia showed a greater than 25-fold increase in theendothelial cells incorporating ['H]thymidine, i.e.,0.0296+0.0087%, P < 0.001. Dipyridamole-treated ani-mals had a 15-fold increase in [3H]thymidine-labelingindex (0.0162±0.0051%, P < 0.001).
Intimal lesion formation. For every animal studied,five random sections from each of five different arterieswere graded 0-5 (see Methods). Single intimal smoothmuscle cells were occasionally observed in control ani-mals (Fig. 5, scores averaged 4±1, range 1-9).
All of the homocystinemic animals developed eccentricfibromusculoelastic lesions (Fig. 6). 5-10% of the pro-liferation regions contained intracellular lipid or foamcells deep in the lesions. The intimal lesion scores for
A:;~ ~0A A
.0.
A i**a10I
B \ b
\ 'a
*\
2 4 66
Plotelet sur,,vol (doys)
FIGuRE 4 The relationships of platelet survival and plasmahomocystine level and endothelial cell loss. Platelet survivaltime correlated with the logarithm of the plasma homo-cystine concentration (0, Fig. 4A) with r = 0.965, P <0.001, and regression line represented by y = 0.453e' -.Measurements of platelet survival time also correlated withthe logarithm of endothelial cell loss (*, Fig. 4B) withr = 0.958, P < 0.001, and a regression line represented byy = 44.0e'"7X. Dipyridamole treatment (A) produced sig-nificant prolongation of platelet survival (P < 0.001).
Homocystine-Induced Arteriosclerosis 735
30
20-
2-oR

0~~~~~...m
,* I
FIGuRE 5 A light micrograph of a section of the iliac ar-tery of a control animal that was fixed and prepared forelectron microscopy, embedded in epoxy resin, and sectionedat 1 um thickness. The thin intima is demarcated by theinternal elastic lamina (arrow). The endothelial cells (e)are barely visible. The media (m) and adventia (a) areclearly visible in this micrograph. Magnification X 220.
the homocystinemic animals averaged 63+5, range 35-98 (Table II). The lesion score correlated directly withthe overall mean homocystine concentration (Fig. 8).r = 0.956, P < 0.001, and the regression line was y=0.375x - 12.7.
.-.--.-.--
FIGuRE 6 A light micrograph with magnification compar-able with that of Fig. 5 and demonstrating a characteristiclesion seen in the homocystinemic animals. The internalelastic lamina (arrow) is present at the bottom of thismicrograph, and the lumen of the vessel at the top. Incomparison with Fig. 5, it can be seen that the intimaoccupies essentially all of this micrograph demonstratingthe marked increase in thickness, smooth muscle prolifera-tion, and connective tissue formation that has occurred.Several lipid-laden cells (1) are present near the base of thislesion. A small portion of the media is present at thebottom of the micrograph. Magnification X 220.
TABLE I IPrevention of Intimal Smooth Muscle Proliferative Lesions
Aortic Intimalendothelial lesion
Baboons cell loss score
Control (8) 0 441*Homocystinemic (15) 9.6ti2.2 63t45Dipyridamole treated (11) 7.0t:0.9 1642
* Variance given as 4 1 SE.t Different from controls at P < 0.001.
The fine structure of the lesions (Fig. 9) was typicalof early lesion formation similar to the fibromusculo-elastic lesions in man (9). They demonstrated the pres-ence of numerous smooth muscle cells surrounded bylarge amounts of small collagen fibers and elastic fibersrich in microfibrils, suggesting that the elastic fiberswere relatively immature (33). In many regions theluminal surface of the lesions had no endothelial cellcover, while in other regions cells appeared to be in theprocess of attempting to cover the surface.
Effect of dipyridamole on intimal lesion formation.In the group of 11 animals receiving oral dipyridamolethroughout the 3-mo period of homocystinemia, themean intimal lesion score was 16±2 (range 7-25),compared with 4±1 in control animals and 63±5 inuntreated homocystinemic animals (Figs. 7 and 8, TableII). The difference in the intimal lesion scores betweenthe dipyridamole-treated and untreated homocystinemic
0
FIGURE 7 A light micrograph of a segment of the iliacartery of a homocystinemic-dipyridamole treated animal (cf.Figs. 5 and 6). It can be seen that the intima is nearlyas thin as that of the control animal, and that the mediaand adventia are both visible in this micrograph in com-
parison with the markedly thickened intima demonstratedin the homocystinemic animals in Fig. 6. Magnificationx 220.
736 L. A. Harker, R. Ross, S. 1. Slichter, and C. R. Scott

301
e20
10.-c
a)
0
q)
aa
aa
aa
/S
S
*
0/
20 40 60Intimol lesion score
FIGURE 8 The formation of intimal smootand endothelial cell desquamation. A linearobserved between the intimal proliferativethe loss of aortic endothelial cells (0).significance of P <0.001. The regressionsented by y = 0.375x - 12.7. Dipyridamolemarkedly reduced the intimal lesion score
animals was significant at P < 0.001. TIsponded with the dipyridamole interrupconsumption but was observed despiteaortic endothelial cells (Table I). Thescore in the dipyridamole-treated animahowever, also significantly greater thanmals (P < 0.01).
Serum cholesterol concentrations fohomocystinemic, and treated group wert96+6, respectively. No correlation was olanimals between cholesterol levels an(scores or the presence of lipid within tl
DISCUSSIONThe effects of homocystine. This stuc
to clarify the mechanism responsible foaccelerated atherosclerosis found in patieihomocystinemia. The clinical syndromeuria, an inborn deficiency of cystathioncharacterized by atherosclerotic occlusiorcerebral, renal, and pulmonary arteries,in fatal infarction before the 3rd decadeIt has been reported on the basis oftaneous injection of homocystine into ralcystine stimulates the synthesis of connements in the artery wall. These studies,been difficult, to reproduce presumablylack of continuous homocystinemia (40--
In an earlier acute study continuouscystinemia in primates was shown to incof arterial endothelium (14). The presetstrates that homocystinemia maintainedduces sustained endothelial cell loss in p:
level of plasma homocystine when the concentrationexceeds about 0.06 mM(Fig. 3). The inability to detectmeasurable deficiencies in endothelial cell coverage atlower homocystine concentrations may be explainedby compensatory coverage achieved by increased endo-thelial regeneration (Table I).
Although we find no evidence to implicate hypercho-lesterolemia or hypertriglyceridemia in homocystine-induced lesions, the importance of lipids in the genesisof atherosclerosis has long been emphasized (4) butpoorly understood. Clearly, lipid accumulation, bothwithin the smooth muscle cells and in the surroundingmatrix, is important in preventing lesion regression
80 160 (10). Both the smooth muscle cells and the matrix pro-teoglycans they form have a marked affinity for lipo-
:h niuscle lesions proteins (43). Of equal interest are observations sug-relationship was gesting that chronic (9 mo or longer) sustained hyper-lesion score and cholesterolemia will result in endothelial "injury" and
r = 0.956, with focal denudation similar to that observed in the homo-trne watm rent e
( cystinemic animals in the present study (44). Thus,(Pt<0.001). lipids may exert in part a similar effect to that seen in
homocystinemia.tis effect corre- The role of platelets in lesion formation. Plateletstino platseet ofaccumulate on exposed subendothelial connective tissue
.t .abse .o surface by adhesion and aggregation to form platelet1 (Finial 7e)sin thrombi (45-48). Adherent platelets undergo the re-
is (Fig .7) 'is lease reaction as evidenced morphologically by degranu-lation (6, 45-51). At least one constituent released from
r the control, platelets is a mitogenic factor that stimulates the pro-99±6, 106+7, liferation of smooth muscle cells (11). This plateletbseredi the factor was initially discovered from the observation that
dsterved intesen arterial smooth muscle cells in culture neither synthesizeetherlesions. DNA nor divide in medium containing serum made
hie lesions. from platelet-free plasma. In contrast, medium contain-
ing whole blood serum, or platelet-free plasma serumcontaining a supernate derived from exposure of a
ly was designed plasma-free preparation of platelets to purified throm-ry bin, are identical in their ability to elicit a mitogenic
its with chronicofs with chronic response from the cells ( 11 ).Of homocystin- The present studies provide in vivo evidence that
of myocardia platelets are important in the process of arteriosclerosisoft Yocaredial, by demonstrating that platelet consumption correlatesoftn rsulting with intimal lesion formation and that the interruptionof life (34-39). of platelet consumption using a known inhibitor of
repeated subcu- platelet function prevents lesion formation. Interestingly,)bits that homo- direct morphology evidences only minimal platelet ac-cumulation at sites of chronic endothelial loss which is
hbe e of the also in accord with the late findings after mechanical42). desquamation (46, 48).-infusion homo- The role of platelets in atherogenesis is further evi-luce patchy loss denced by several additional recent studies. Moore etat study demon- al. (52) were able to prevent arteriosclerotic lesionover 3 mo pro- formation induced by chronic indwelling arterial cathe-roportion to the ters in animals made severely thrombocytopenic with
Homocystine-Induced Arteriosclerosis 737

N'A:
el'-+:::~ ~~ <we a:- :--P~~~~ s) tj > io., ,rE 1s
V.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~N4 L~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~'
FIGURE 9 An electron micrograph of a portion of one of the lesions observed in the homo-cystinemic animals. The junction between the two lining cells which may be endothelium isincomplete (arrow). Beneath the linineg luminal cells can be seen numerous smooth muscle cellsthat have proliferated within the lesion. These are surrounded by large numbers of collagenfibrils (c) and newly formed elastic fibers (el). Magnification X 8,500.
antiplatelet serum. Similarly, Friedman and Stemmer- are secretory products of the proliferating smoothman (personal communication) prevented balloon cathe- muscle cells (55, 56). This lesion is characteristic ofter-induced lesion formation by severe thrombocyto- arteriosclerosis. The intra- and extracellular accumula-penia. And finally, a retrospective study in pigs affected tions of lipid by intimal smooth muscle cells and con-with von Willebrand's disease, a genetic defect in plate- comitant formation of connective tissue appear to belet-surface interaction (53), reported a reduced fre- facilitated by disruption of the endothelial cell barrierquency of atherosclerosis in the adult animals (54). and exposure of the artery wall to platelets and plasma
The intimal proliferative smooth muscle lesion con- factors.tains the connective tissue matrix components of elastic Role of antiplatelet agents. Inhibition of platelet ad-fibers, collagen, and glycosaminoglycanii, all of which hesion, aggregation, and release are variably produced
738 L. A. Harker, R. Ross, S. J. Slichter, and C. R. Scott

by a wide variety of pharmacologic agents (50, 51, 57-59). These include a group of nonsteroidal anti-inflam-matory drugs such as acetylsalicylic acid and sulfinpy-razone. Although their mode of action has not yet beenfully determined, these drugs characteristically inhibitthe platelet release reaction and the secondary phase ofADP or epinephrine-induced aggregation with little orno effect on primary ADP aggregation. These drugsappear to be less useful for interrupting adhesion-re-lated effects, e.g., acetylsalicylic acid fails to reduce theadhesion and degranulation of platelets to subendothel-ium (53). Correlation between in vitro effects on plate-let function tests and in vivo antithrombotic effects isvariable. For example, in man treatment with sulfinpy-razone normalizes platelet survival and reduces thrombusformation without showing any measurable effect on invitro tests of platelet function (60).
A second group of drugs, the pyrimido-pyrimidinecompounds, inhibits both primary and secondary ADP-or epinephrine-induced aggregation and platelet release,aggregation induced by thrombin or collagen, and plate-let retention by glass-bead columns. These drugs appearto affect platelet cAMPby enhancing adenylcyclase andinhibiting phosphodiesterase activity (50, 51, 57-59).Included in this class of agents is dipyridamole. Inter-estingly, dipyridamole interrupts platelet consumptionand thromboembolism in man at concentrations that donot effect platelet function tests in vitro (61, 62). Thisdiscrepancy between in vivo and in vitro effects isfurther evidenced by a recent comparison of in vivoand in vitro collagen-induced platelet aggregation thatshowed the inhibitory effect of dipyridamole in vivo tobe enhanced many times over that observed in vitro(63).
Consideration must be given to the possibility thatdipyridamole may have produced its beneficial effect onlesion formation by protecting the endothelium frominjury, by modifying the thrombogenicity of the sub-endothelium, or by inhibiting the proliferation of smoothmuscle cells. The data in Table I and Fig. 1 indicatethat homocystine-induced endothelial cell loss remainedquantitatively unchanged by dipyridamole therapy. Thedrug therefore appears to have no protective effect onthe endothelium. Furthermore, smooth muscle cell pro-liferation also appears to be unaffected because smoothmuscle cells proliferate normally in culture with dipyrid-amole concentrations as great as 10 M (unpublishedobservation). Since the only measurable effect of dipy-ridamole appears to be on platelet consumption, we con-clude that the drug effect is mediated through platelet-related mechanisms. Our observation that dipyridamole-treated animals show reduced platelet retention by glass-bead columns suggests that the effect involves pharma-cologic inhibition of platelet function rather than somealteration of the subendothelial surface.
On the basis of these studies we conclude that sus-tained chemically induced endothelial cell injury resultsin endothelial cell loss followed by platelet adherenceand release and the development of progressive intimalarteriosclerotic lesions. The fundamental role of plate-lets in the genesis of these lesions is demonstrated bythe capacity of an inhibitor of platelet function to pre-vent intimal smooth muscle proliferation, and conse-quent lesion formation. These observations imply po-tential therapeutic benefit of antiplatelet drugs in theprevention or interruption of atherogenesis in man.
ACKNOWLEDGMENTSWe are indebted to Tom Kirkman, Norma Joy, BeverlyKariya, and Cellini Chen for their technical assistance whichmade this study possible. We also wish to thank Drs. Haz-zard and Kushwaha of the Northwest Lipid Research Clinicfor performing the cholesterol determinations according tostandardized, equality-controlled Lipid Research Clinic pro-cedures (Lipid Research Clinics Program, Manual of Lab-oratory Operations. 1974. Volume 1).
Statistical analysis was carried out through the PROPHETSystem developed by the Chemical Biological InformationHandling Program of the Biotechnology branch of theDivision of Research Resources, National Institute of Health.
This work was supported by research grants (HL-11775,RR-00166 HL-14832, HL-14860, and HD-04665) from theU. S. Public Health Service.
REFERENCES1. Geer, J. C., C. Catsulis, H. C. McGill, Jr., and J. P.
Strong. 1968. Fine structure of the baboon aortic fattystreak. Am. J. Pathol. 52: 265-286.
2. Armstrong, M. L., E. D. Warner, and W. E. Connor.1970. Regression of coronary atheromatosis in rhesusmonkeys. Circ. Res. 27: 59-67.
3. Ross, R., and J. Glomset. 1973. Atherosclerosis and thearterial smooth muscle cell. Proliferation of smoothmuscle is a key event in the genesis of the lesions ofatherosclerosis. Science (Wash. D. C.). 180: 1332-1339.
4. Wissler, R. W. 1974. Development of the atheroscleroticplaque. In The Myocardium: Failure and Infarction.E. Braunwald, editor. New York, HP Publishing Co.,155-166.
5. Baumgartner, H-R., and A. Studer. 1966. Folgen desGefasskatheterismus an normo- und hypercholesterinae-mischen Kaninchen. Pathol. Microbiol. 29: 393-405.
6. Stemerman, M. B., and R. Ross. 1972. Experimentalarteriosclerosis. I. Fibrous plaque formation in primates:An electron microscope study. J. Exp. Med. 136: 769-789.
7. Bjorkerud, S., and G. Bondjers. 1971. Arterial repairand atherosclerosis after mechanical injury. Part I.Permeability and light microscopic characteristics ofendothelium in non-atherosclerotic and atheroscleroticlesions. Atherosclerosis. 13: 355-363.
8. Christensen, B. C., and C. Garbarsch. 1973. Repair inarterial tissue. A scanning electron microscopic (SEM)and light microscopic study on the endothelium of rab-bit thoracic aorta following a single dilatation injury.Virchows Arch. Pathol. Anat. Physiol. klin. Med.).360:A: 93-106.
9. National Heart and Lung Institute Task Force on Ar-teriosclerosis. Arteriosclerosis. June 1971. Department
Homocystine-Induced Arteriosclerosis 739

of Health, Education and Welfare Publ. No. 72-219.National Institutes of Health, Bethesda, Md. 2: 4-27.
10. Ross, R., and J. Glomset. 1974. Studies of primate ar-terial smooth muscle cells in relation to atherosclerosis.In Arterial Mesenchyme and Arteriosclerosis. W. D.Wagner and T. B. Clarkson, editors. Plenum Publish-ing Corp., New York. 265-279.
11. Ross, R., J. Glomset, B. Kariya, and L. Harker. 1974.A platelet-dependent serum factor that stimulates theproliferation of arterial smooth muscle cells in vitro.Proc. Natl. Acad. Sci. U. S. A. 71: 1207-1210.
12. Storb, R., H. Ragde, and E. D. Thomas. 1969. Extra-corporeal irradiation of the blood in baboons. Radiat.Res. 38: 43-54.
13. Slichter, S. J., and L. A. Harker. 1971. Studies ofplatelet destruction due to prosthetic arterio-venouscannulae. Clin. Res. 19: 135. (Abstr.)
14. Harker, L. A., S. J. Slichter, C. R. Scott, and R. Ross.1974. Homocystinemia. Vascular injury and arterialthrombosis. N. Engl. J. Med. 291: 537-543.
15. Bull, B. S., M. A. Schneiderman, and G. Brecher. 1965.Platelet counts with the Coulter counter. Ain. J. Clin.Pathol. 44: 678-688.
16. Harker, L. A., and C. A. Finch. 1969. Thrombo-kinetics in man. J. Clin. Invest. 48: 963-974.
17. Paulus, J. M., editor. 1971. Platelet Kinetics: Radioiso-topic, Cytological, Mathematical and Clinical Aspects.New York, American Elsevier Publishing Co., NewYork. 38-117.
18. Murphy, E. A., and M. E. Francis. 1971. The estimationof blood platelet survival. II. The multiple hit model.Thromizb. Diath. Haemnorrh. 25: 53-80.
19. Murphy, E. A. 1971. The estimation of blood plateletsurvival. III. The robustness of the basic models.Thromb. Diath. Haemorrh. 26: 431-448.
20. Murphy, E. A., M. E. Francis, and J. F. Mustard. 1972.The estimation of blood platelet survival. IV. Charac-teristics of the residual errors from regression. ThromDb.Diath. Haemitorrh. 28: 447-456.
21. Jacobsson, K. 1955. Studies on the determination offibrinogen in human blood plasma. Scanid. J. Clin. Lab.Invest. 7 (Suppl. 14): 3-54.
22. Takeda, Y. 1966. Studies of the metabolism and dis-tribution of fibrinogen in healthy men with autologous'I-labeled fibrinogen. J. Clin. Invest. 45: 103-111.
23. Harker, L. A., and S. J. Slichter. 1972. The bleedingtime as a screening test for evaluation of platelet func-tion. N. Engl. J. Med. 287: 155-159.
24. Bowie, E. J. W., C. A. Owen, Jr., J. H. Thompson,Jr., and P. Didisheim. 1969. A test of platelet adhesive-ness. Mayo Clin. Proc. 44: 306-308.
25. Born, G. V. R., and M. J. Cross. 1963. The aggregationof blood platelets. J. Physiol. (Lond.). 168: 178-195.
26. Mustard, J. F., B. Hegardt, H. C. Rowsell, and R. L.MacMillan. 1964. Effect of adenosine nucleotides onplatelet aggregation and clotting time. J. Lab. Clin. Med.64: 548-559.
27. Spackman, D. H., W. H. Stein, and S. Moore. 1958.Automatic recording apparatus for use in the chroma-tography of amino acids. Anal. Chem. 30: 1190-1206.
28. Haudenschild, C., H. R. Baumgartner, and A. Studer.1972. Significance of fixation procedure for preservationof arteries. Experienttia (Basel). 28: 828-831.
29. Poole, J. C. F., A. G. Saunders, and H. W. Florey.1958. The regeneration of aortic endothelium. J. Pathol.Bacteriol. 75: 133-143.
30. Huber, J. D., F. Parker, and G. F. Odland. 1968. Abasic fuchsin and alkalinized methylene blue rapid stainfor epoxy-embedded tissue. Stain Technol. 43: 83-87.
31. Sade, R. M., and J. Folkman. 1972. En face strippingof vascular endothelium. Microvasc. Res. 4: 77-80.
32. Schwartz, S. M., and E. P. Benditt. 1973. Cell replica-tion in the aortic endothelium: A new method forstudy of the problem. Lab. Invest. 28: 699-707.
33. Greenlee, T. K., Jr., R. Ross, and J. L. Hartman. 1966.The fine structure of elastic fibers. J. Cell. Biol. 30:59-71.
34. Carson, N. A. J., D. C. Cusworth, C. E. Dent, C. M.B. Field, D. W. Neill, and R. G. Westall. 1963. Homo-cystinuria: A new inborn error of metabolism asso-ciated with mental deficiency. Arch. Dis. Child. 38:425-436.
35. Gerritsen, T., and H. A. Waisman. 1964. Homocystin-uria: Absence of cystathionine in the brain. Scienice(Wash. D. C.). 145: 588.
36. Gibson, J. B., N. A. J. Carson, and D. W. Neill. 1964.Pathological findings in homocystinuria. J. Clint. Pathol.17: 427-437.
37. Carson, N. A. J., C. E. Dent, and C. M. B. Field, andG. E. Gaull. 1965. Homocystinuria: Clinical and patho-logical review of ten cases. J. Pediatr. 66: 565-583.
38. Schimke, R. N., V. A. McKusick, T. Huang, and A. D.Pollack. 1965. Homocystinuria. Studies of 20 familieswith 38 affected members. J. Am. Med. Assoc. 193:711-719.
39. Uhlendorf, B. W., and S. H. Mudd. 1968. Cystanthioninesynthase in tissue culture derived from human skin:Enzyme defect in homocystinuria. Science (Wash.D. C.). 160: 1007-1009.
40. McCully, K. S. 1969. Vascular pathology of homocys-teinemia: Implications for the pathogenesis of arterio-sclerosis. Am. J. Pathol. 56: 111-128.
41. McCully, K. S. 1972. Macromolecular basis for homo-cysteine-induced changes in proteoglycan structure ingrowth and arteriosclerosis. Amii. J. Pathol. 66: 83-95.
42.. Donahue, S., J. A. Sturman, and G. Gaull. 1974. Ar-teriosclerosis due to homocyst(e)inemia. Failure to re-produce the model in weanling rabbits. Am. J. Pathol.77: 167-174.
43. Iverius, P-H. 1972. The interaction between humanplasma lipoproteins and connective tissue glycosamino-glycans. J. Biol. Chewl. 247: 2607-2613.
44. Harker, L. A., S. J. Slichter, and L. R. Sauvage. 1976.Platelet consumption by arterial prostheses: The effectsof endothelialization and pharmacologic inhibition ofplatelet function. N. Entgl. J. Med. In press.
45. Mustard, J. F., R. L. Kinlough-Rathbone, and M. A.Packham. 1974. Recent status of research in the patho-genesis of thrombosis. Thromb. Diath. Haeniorrh. Suppl.59: 157-188.
46. Baumgartner, H. R., and C. Haudenschild. 1972. Ad-hesion of platelets to subendothelium. Ann. N. Y. Acad.Sci. 201: 22-36.
47. Stemerman, M. B. 1974. Vascular intimal components:Precursors of thrombosis. Int Progress in Hemostasisand Thrombosis. T. H. Spaet, editor. Vol. 2. Grune &Stratton, Inc., New York. 1-47.
48. Baumgartner, H. R. 1974. The subendothelial surfaceand thrombosis. In Thrombosis: Pathogenesis and Clini-cal Trials. E. Deutsch, K. M. Brinkhous, K. Lechner,and S. Hinnom, editors. F. K. Schattauer-Verlag, Stutt-gart. 91-105.
740 L. A. Harker, R. Ross, S. J. Slichter, and C. R. Scott

49. White, J. G. 1972. Platelet morphology and function.In Hematology. W. J. Williams, E. Beutler, A. J.Erslev, and R. W. Rundles, editors. McGraw-Hill BookCo., New York. 1023-1039.
50. Mustard, J. F., and M. A. Packham. 1970. Factors in-fluencing platelet function: Adhesion, release and aggre-gation. Pharmacol. Rev. 22: 97-187.
51. Weiss, H. 1975. Platelets: Physiology and abnormalitiesof platelet function (first of two parts). N. Engi. J.Med. 293: 531-541.
52. Moore, S., R. J. Friedman, D. P. Singal, J. Gauldie,and M. Blajchman. 1976. Inhibition of injury-inducedthromboatherosclerotic lesions by antiplatelet serum inrabbits. Thromb. Diath. Haemorrh. 35: 70-81.
53. Weiss, H. J., T. B. Tschopp, and H. R. Baumgartner.1975. Impaired interaction (adhesion-aggregation) ofplatelets with the subendothelium in storage-pool dis-ease and after aspirin ingestion. A comparison with VonWillebrand's disease. N. Engl. J. Med. 293: 619-623.
54. Bowie, E. J. W., V. Fuster, C. A. Owen, Jr., and A. L.Brown. 1975. Resistance to the development of spon-taneous atherosclerosis in pigs with von Willebrand'sdisease. 5th Congress of the International Society onThrombosis and Haemostasis, Paris.
55. Ross, R., and S. J. Klebanoff. 1971. The smooth musclecell. I. In vivo synthesis of connective tissue proteins.J. Cell. Biol. 50: 159-171.
56. Ross, R. 1973. The smooth muscle cell in connectivetissue metabolism and atherosclerosis. In Proceedingsof the Sigrid Juselius Foundation Symposium in Turku,
Finland. E. Kulonen, editor. Academic Press, London.627-636.
57. Weiss, H. J. 1972. The pharmacology of platelet inhibi-tion. In Progress in Hemostasis and Thrombosis. Vol. 1.T. H. Spaet, editor. Grune & Stratton, Inc., New York.199-231.
58. Didisheim, P. T., T. Shimamoto, and H. Yamazaki.1974. Platelets, thrombosis and inhibitors. Thromb. Di-ath. Haemorrh. Suppl. 60: 3-15.
59. Kinlough-Rathbone, R. L. 1975. The effects of someother drugs on platelet function. In Platelets, Drugsand Thrombosis. J. Hirsh, J. F. Cade, A. S. Gallus, andE. Schonbaum, editors. A. G. Karger, Basel, Switzer-land. 124-131.
60. Steele, P. P., H. S. Weily, H. Davies, and E. Genton.1973. Platelet function studies in coronary artery dis-ease. Circulation. 48: 1194-1200.
61. Harker, L. A., and S. J. Slichter. 1970. Studies ofplatelet and fibrinogen kinetics in patients with pros-thetic heart valves. N. Engl. J. Med. 283: 1302-1305.
62. Sullivan, J. M., D. E. Harken, and R Gorlin. 1971.Pharmacologic control of thromboembolic complicationsof cardiac-valve replacement. N. Engl. J. Med. 284:1391-1394.
63. Buchanan, M., and J. Hirsh. 1975. Comparison of invivo and in vitro effects of platelet function suppressingdrugs. In 5th Congress of the International Society onThrombosis and Haemostasis, Paris. p. 182. (Abstr. no.165)
Homocystine-Induced Arteriosclerosis 741