“Home is Where the Care is ” Annual Conference and Exhibition Glasgow Marriott Hotel Friday 31...
67
“Home is Where the Care is” Annual Conference and Exhibition Glasgow Marriott Hotel Friday 31 st May 2013
-
Upload
terence-jenkins -
Category
Documents
-
view
218 -
download
2
Transcript of “Home is Where the Care is ” Annual Conference and Exhibition Glasgow Marriott Hotel Friday 31...

“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013


“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013
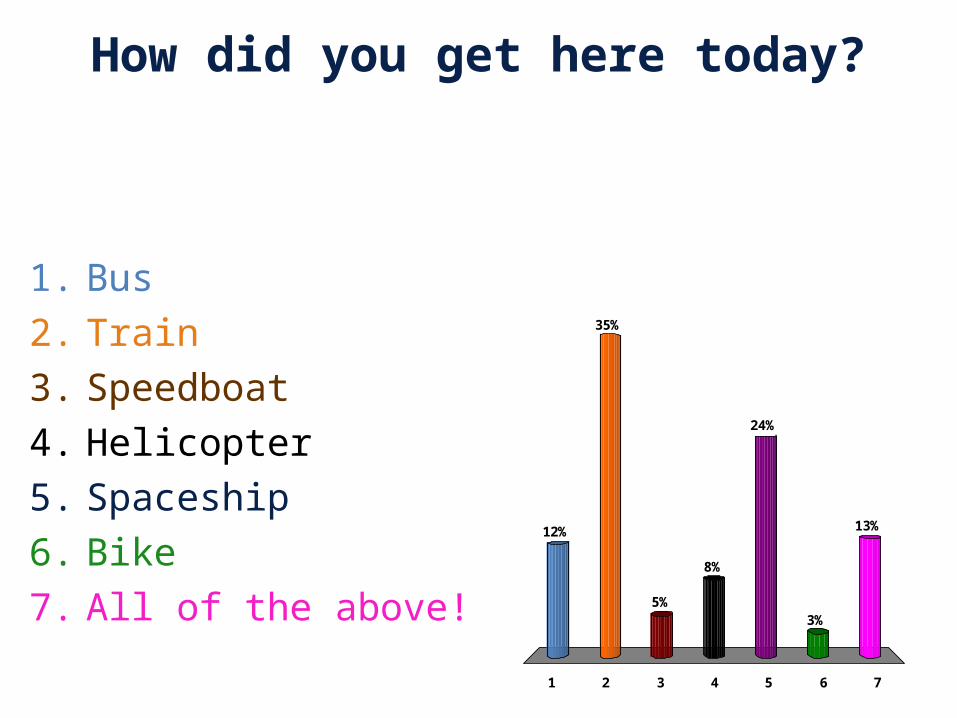
How did you get here today?
1 2 3 4 5 6 7
12%
35%
5%
13%
3%
24%
8%
1. Bus2. Train3. Speedboat4. Helicopter5. Spaceship6. Bike7. All of the above!
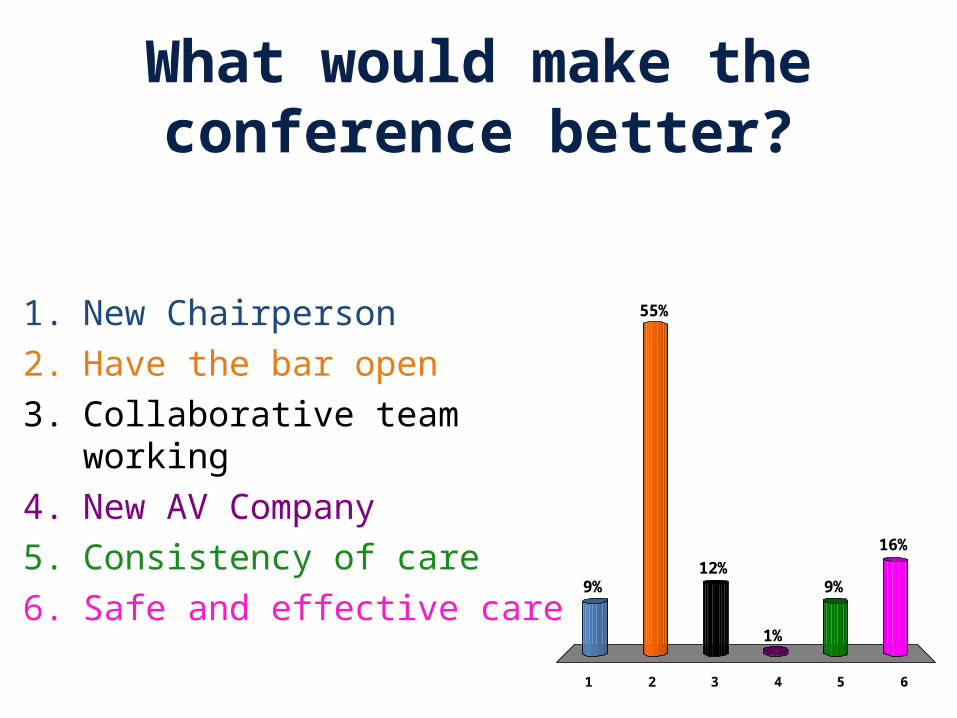
What would make the conference better?
1 2 3 4 5 6
9%
55%
16%
9%
1%
12%
1. New Chairperson2. Have the bar open 3. Collaborative team
working4. New AV Company5. Consistency of care6. Safe and effective care
“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013

Quality or Compromise
The reality of delivering Care at Home You decide…..

Shadowing our conference carer Mel in real time
• with a live broadcast through out the morning conference
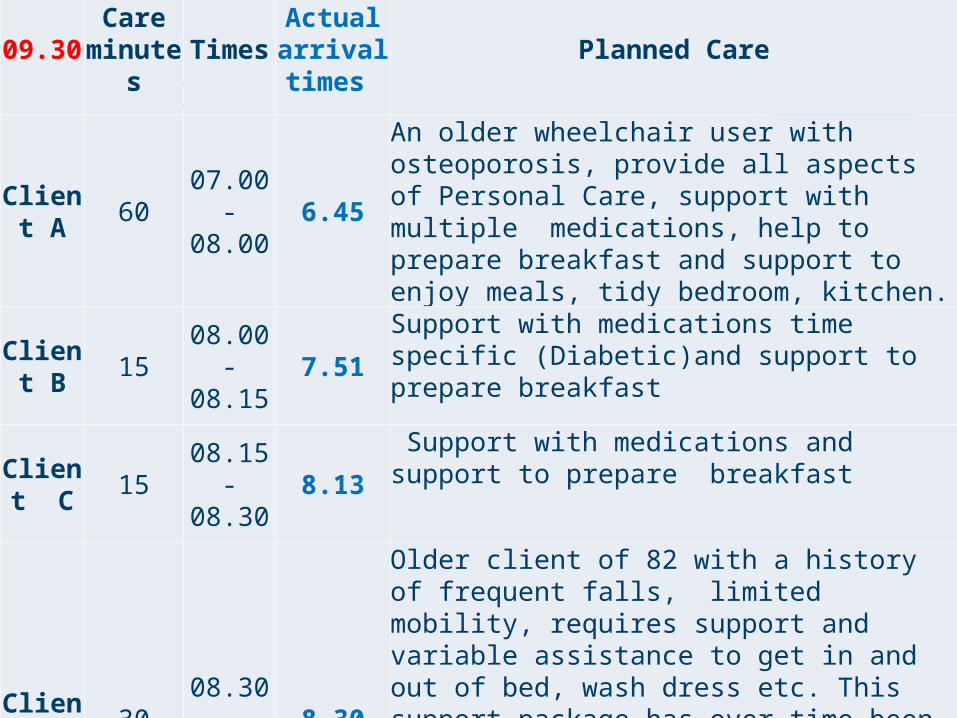
Session 109.30 Care
minutes TimesActual arrival times
Planned Care
Client A 60 07.00 -
08.00 6.45
An older wheelchair user with osteoporosis, provide all aspects of Personal Care, support with multiple medications, help to prepare breakfast and support to enjoy meals, tidy bedroom, kitchen.
Client B 15 08.00 -
08.15 7.51
Support with medications time specific (Diabetic)and support to prepare breakfast
Client C 15 08.15 -
08.30 8.13
Support with medications and support to prepare breakfast
Client D 30 08.30 -
09.00 8.30
Older client of 82 with a history of frequent falls, limited mobility, requires support and variable assistance to get in and out of bed, wash dress etc. This support package has over time been successfully reduced through an enablement approach. This client is also the main carer for her 60 year daughter with enduring Mental Health needs.
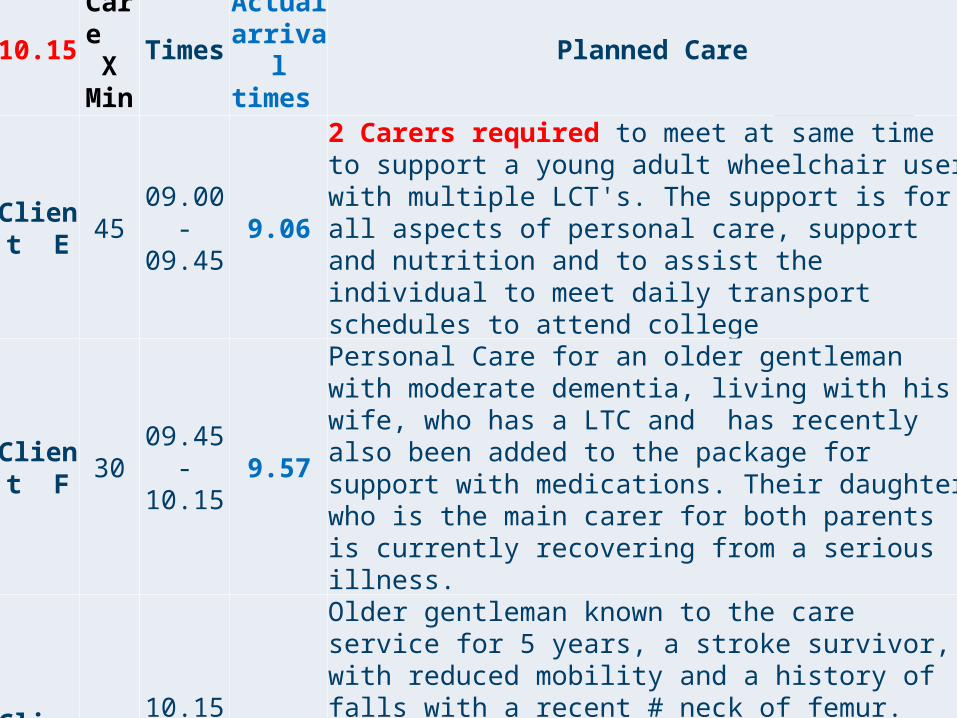
10.15Care
XMin
TimesActual arrival times
Planned Care
Client E 45 09.00 -
09.45 9.06
2 Carers required to meet at same time to support a young adult wheelchair user with multiple LCT's. The support is for all aspects of personal care, support and nutrition and to assist the individual to meet daily transport schedules to attend college
Client F 30 09.45 -
10.15 9.57
Personal Care for an older gentleman with moderate dementia, living with his wife, who has a LTC and has recently also been added to the package for support with medications. Their daughter who is the main carer for both parents is currently recovering from a serious illness.
Client G 60 10.15 -
11.15 10.29
Older gentleman known to the care service for 5 years, a stroke survivor, with reduced mobility and a history of falls with a recent # neck of femur. Staff have been integral to his return home and to his on-going rehabilitation. Following surgery the package of care has been slowly reduced in response to increasing independence.

12.15Care
x Mins
TimesActual
arrival times
Planned Care
Unpaid break 15 Client in
hospital Carer used own unpaid break to make up time and to avoid running late
Client H 30 11.30 -
12.00 11.34 Meal preparation for lunch, assist with continence management
Client A 30 12.00 -
12.3012.10 - 12.40
Meal preparation for lunch, assist with continence management
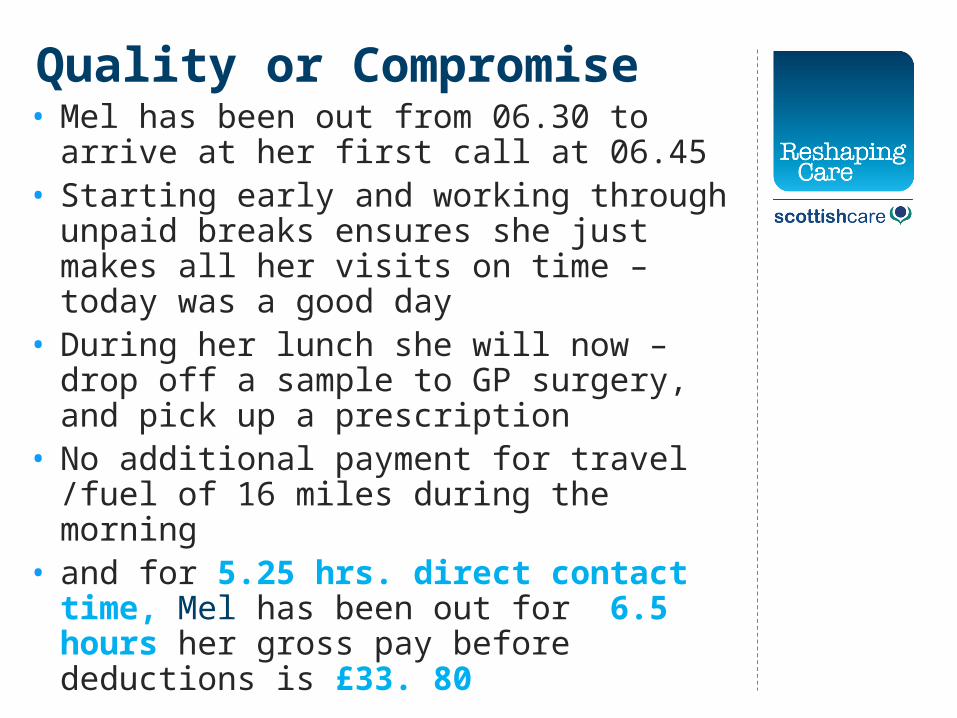
Quality or Compromise• Mel has been out from 06.30 to arrive at her
first call at 06.45• Starting early and working through unpaid
breaks ensures she just makes all her visits on time – today was a good day
• During her lunch she will now – drop off a sample to GP surgery, and pick up a prescription
• No additional payment for travel /fuel of 16 miles during the morning
• and for 5.25 hrs. direct contact time, Mel has been out for 6.5 hours her gross pay before deductions is £33. 80

Question

Should all care staff regardless of sector/ employer be paid the living wage of £7.45 then we can address time to care, time to
travel/fuel payments
1 2 3
0% 0%0%
1. Yes 2. No3. Don’t Know
“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013

Health & Social Care Integration
Professor Jim McGoldrickChair, Joint Improvement Partnership Board

JOINT IMPROVEMENT PARTNERSHIP BOARD
• Angela Leitch, Chief Executive, East Lothian Council;
• Angiolina Foster, Director, Health & Social Care Integration, Scottish Government;
• Annie Gunner-Logan, Director, Coalition of Care Providers Scotland (CCPS);
• Cathie Cowan, Chief Executive, NHS Orkney;
• Colin Mackenzie, Chief Executive, Aberdeenshire Council;
• Fiona Mackenzie, Chief Executive, NHS Forth Valley;
• Ian Welsh, Chief Executive, Health & Social Care Alliance Scotland;
• Kenneth Hogg, Director, Local Government & Communities, Scottish Government;
• Martin Sime, Chief Executive, Scottish Council for Voluntary Organisations (SCVO);
• Mary Taylor, Chief Executive, Scottish Federation of Housing Associations (SFHA);
• Ranald Mair, Chief Executive, Scottish Care; and
• Rory Mair, Chief Executive, CoSLA.
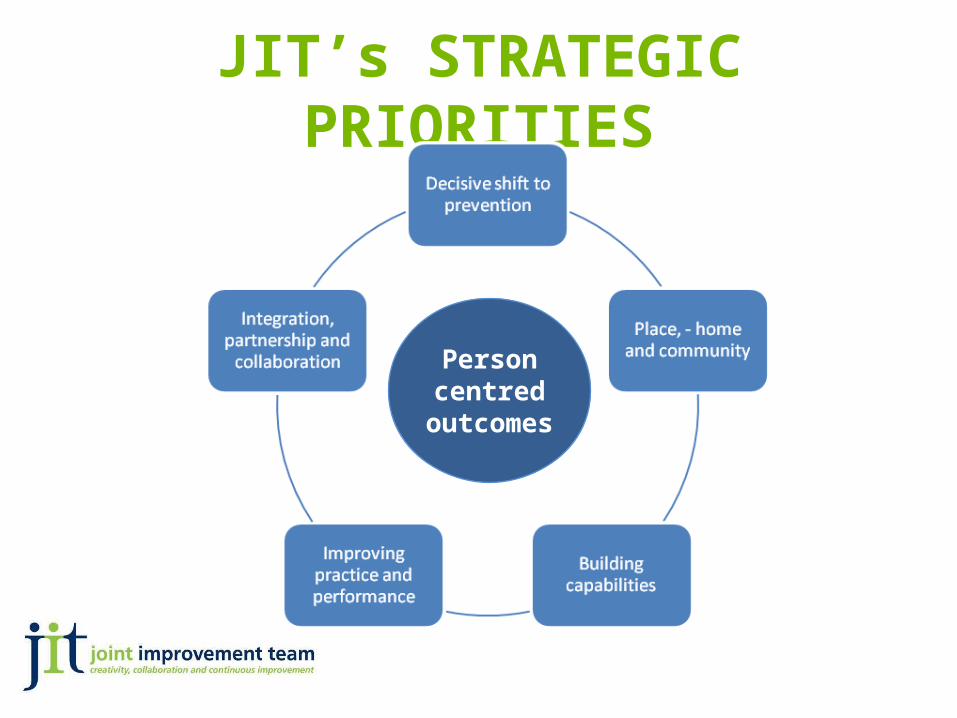
JIT’s STRATEGIC PRIORITIES
Person centred
outcomes

ROUTE MAP TO THE 20:20 VISION
20:20 Vision / Quality AmbitionsPerson Centred, Safe and Effective Care which supports people to live as
long as possible at home or in a homely setting.
Quality of CareHealth of the Population
Value & Financial
Sustainability
Independent livingServices are safe
Engaged workforcePositive experiences
Triple Aim
20:20 Vision
12 Priority Areas for Action
11/02/13
Quality Outcomes
Healthier living Effective resource use

Health & Social Care Integration
Underpinned by Legislation:• nationally agreed outcomes;
1.Healthier
2. Independent Living
3.Positive experiences and outcomes
4.Carers are supported
5.Services are safe
6.Engaged workforce
7.Effective resource use

Health & Social Care Integration
Policy Context SG Consultation• Improve Outcomes• Focus on Population• Address funding and demographic challenges• Variability in care by geography• The Accountability/Responsibility Paradox

Health & Social Care Integration
Key themes in the Consultation (the Bill)• Consistency of approach• Statutory underpinning• Integrated budget• Clear Accountability• Professional Leadership• Simplified structures and minimal disruption

Health & Social Care Integration
Workforce development issues
• Definition of Workforce – not just the paid employees of Health Boards and Councils
• “Professional leadership”• Definition of leadership – not a function of
hierarchy or job title. Leadership happens at all levels.
Health & Social Care Integration
Workforce development – strategic context• Ministerial Strategic Group• RCOP workforce work stream 2010- 2012• Change Plans and Change Fund• Position paper in response to SG Consultation
on what work has already been done• Development of a strategic narrative

Health & Social Care Integration
Strategic Narrative on workforce development
• Not about workforce planning• Not about terms and conditions• Not in isolation
Health & Social Care Integration
Workforce Development Strategic Group – WDSG
• “[SG] will work with NES and SSSC and other stakeholders to define priority training requirements within an integrated context; articulate what these mean for frontline staff and mobilise support through an education and training infrastructure”
• (Consultation doc p44)
Health & Social Care Integration
WDSG• Who are we and how do we work together?• Shared meaning and understanding for
“collaborative leadership• “Reference Groups” approach (not “Expert”
Group• WDSG as a portal to frontline staff

Health & Social Care Integration
Workforce Reference Groups – emerging themes• Don’t re-invent the wheel, use existing joint
working to observe the process of integration• Skills and training environment, better IT
support• Leadership and Clarity of communication
Health & Social Care Integration
Workforce Reference Groups – emerging themes• Understand what is already happening –
mapping existing work• Issues of Professional Identity• Need to define what’s national and what’s
local
Health & Social Care Integration
Workforce position paper – Scottish Care
• Follow-up to the reference group session• Strategic narrative • Well – defined priorities • Challenges and opportunity

“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013

Integrated Resource Integrated Resource Framework: Supporting Framework: Supporting Health and Social Care Health and Social Care Integration through Integration through Strategic Planning Strategic Planning Christine McGregor, Economic Adviser, Scottish Government, Health Analytical Services Division.
Scottish Care Annual Care at Home and Housing Support Conference.
Glasgow Marriot Hotel, Friday 31st May 2013.

OutlineOutlineIntegration and Strategic CommissioningWhat is the Integrated Resource
Framework?Two main aspects – “IRF mapping” and
“Patient (client) level analysis”Extensive examples of where IRF has
been used.Highlight where Scottish Care and
partners could input and benefit from IRF mapping.
Integration and Strategic Integration and Strategic CommissioningCommissioning
The Bill to integrate adult health and social care places a duty on Health and Social Care Partnerships to produce Strategic Commissioning Plans .
A multi-sectorial co-production approach to be used to develop the Strategic Plan.
Knowledge and expertise of independent and third sector will be critical for successful joint commissioning.
Build on change fund experience.
Strategic Commissioning Strategic Commissioning CycleCycle“Analysis is one of the most important
activities in the commissioning cycle. Poor analysis of post or future trends will result in flawed commissioning decisions and wasted resources” SWIA Guide to Strategic Commissioning
Critical for partnerships to understand current service provision, quality, costs of in house and procured services, and transparency of information for all partners.
Only then will decisions be based on robust evidence and result in positive outcomes for individuals.

Question 1Question 1
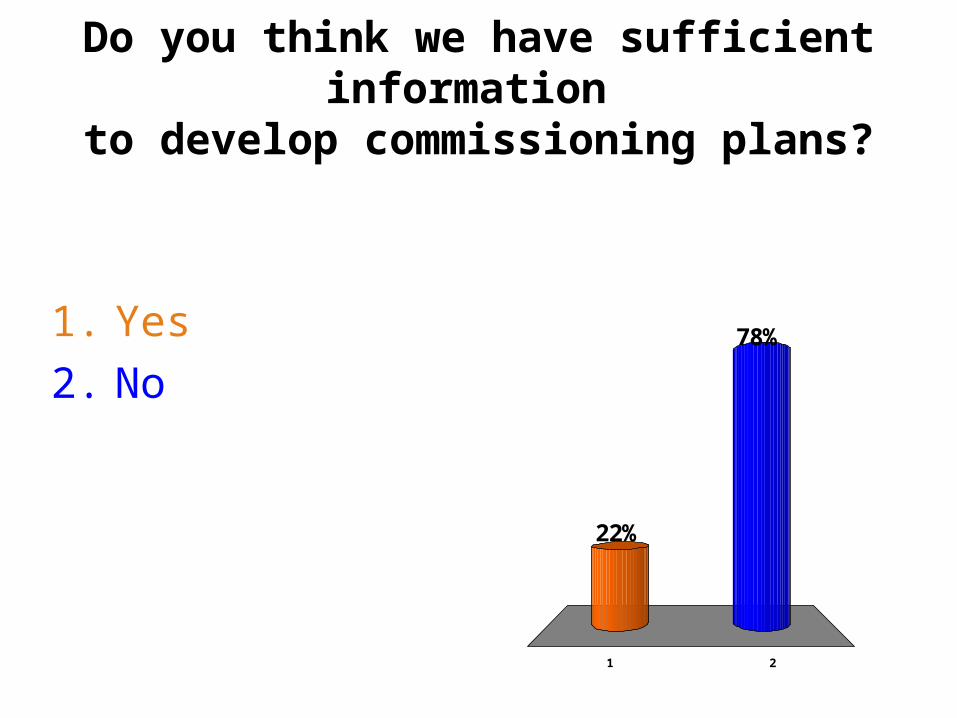
Do you think we have sufficient information to develop commissioning plans?
1 2
78%
22%
1. Yes2. No

National Support and National Support and Improvement Programme Improvement Programme AnalysisAnalysis
We will give you sufficient information!Quality of “analysis” in plans varied.Programme to support development of
commissioning abilities by extending what is already offered from IRF team.
Target for all partnerships to have patient (client level) data by April 2015 to inform decision making.
What is IRF - 1What is IRF - 1Development by SG, COSLA and NHS in
2008/09, with objective being to begin to understand joint resources (NHS and LA) across population they serve.
As it developed use by all sectors.
Focus on joint resources rather then more traditional budget lines such as acute budget, community budget, social work budget.
Provide a evidence base for shifts within and across health and social care.
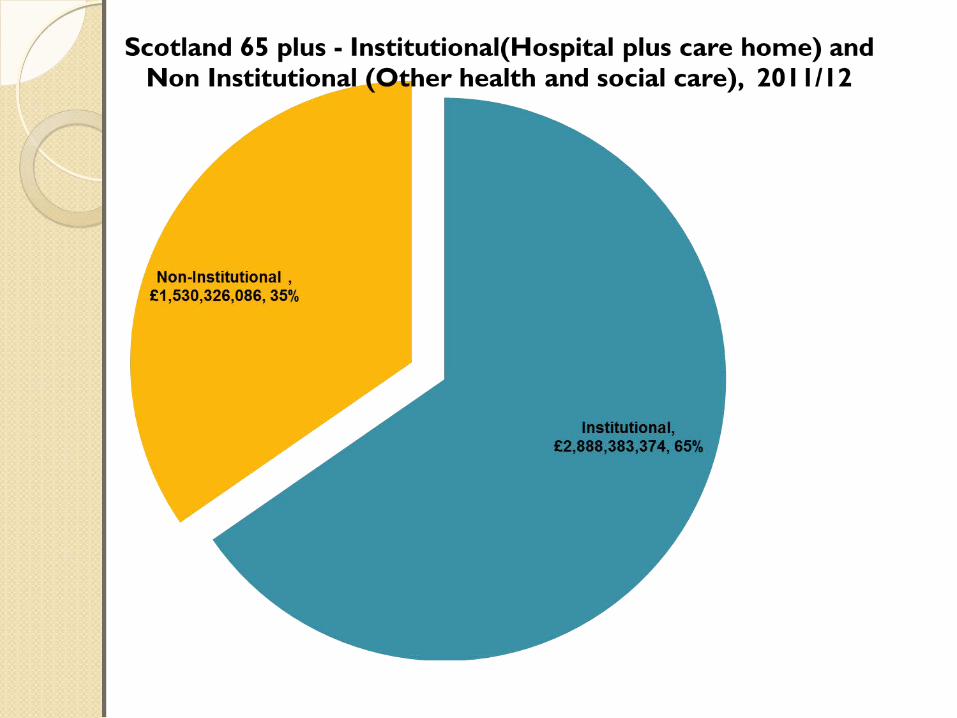
IRF mapping -1IRF mapping -1Every community health partnership in
Scotland is given mapped data for all ages 65 and 75 plus.
Mapping consists of:Hospital based services (£5.1bn, £2.2bn,
£1.4bn)Health community based services (£1.4bn,
£439m, £245m)GP and GP Prescribing (£1.7bn, £577m,
£297m)Local authority services (18 plus £2bn,
Older people £1.3bn)
Question 2Question 2

What percentage of hospital based resource is accounted for by
emergency (non elective) admissions?
1 2 3
12%
68%
21%
1. 25%2. 50%3. 60%


How has IRF mapping being How has IRF mapping being used?used?
Joint Commissioning – baseline for current resource adult/older people across sectors.
Key to the analysis part of cycle. Support change fund projects.Variation analysis emergency
admissions/prescribing by GP.Routine briefing/health and social
care bill. Basis of joint budgets.
Patient (client) level Patient (client) level analysis - 1analysis - 1
IRF mapping examines resource and activity to various geographical levels.
Doesn’t say WHO is using services, for example emergency admissions rates and costs may fall/rise but for certain cohorts they may be rising continually.
Patient (client) level health and social care allows various questions to be answered.

Patient (client) level Patient (client) level analysis - 2analysis - 2
Is it the same people who use both health and social care services?
Is it the same people that are always facing a delayed discharge?
Does level of home care make a difference to level of admissions?
Does prescribing have an effect on admissions?

Patient (client) level Patient (client) level analysis - 3analysis - 3ISD linked at patient level, hospital,
prescribing, social care activity and costs for all residents across Tayside.
Social care include care home, day care home care, meals, alarms, rehabilitation.
Other partnerships’ linked health only. Unit costing of social care will hopefully
simplify LFR return for social work. Area where we would welcome input from
independent and third sector providers.
Patient (client) level Patient (client) level analysis - 4analysis - 4Once data set linked at patient
(client level) it can be used for multiply needs.
What IRF team would like to offer each partnership.

Dementia - 1Dementia - 1Define dementia cohort - from GP
LTC register.What health and social resources
do dementia patients use?◦ Compared to non dementia population
Forecast future demand as a result of demographic pressure
Assist with planning and evaluating services redesign◦Key cohort for joint commissioning of
services.
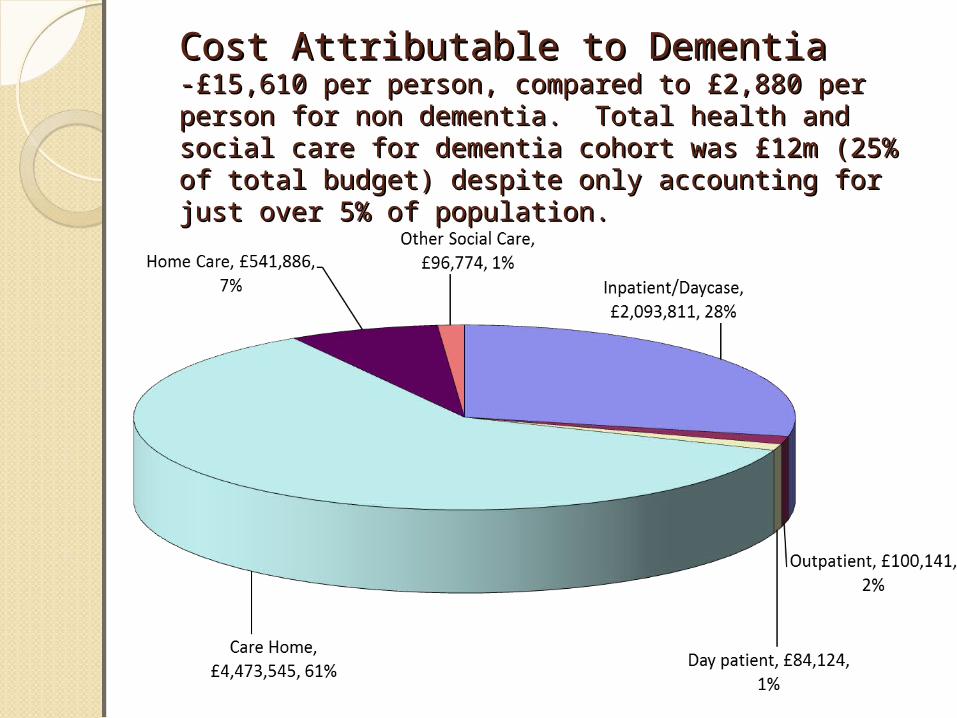
Cost Attributable to DementiaCost Attributable to Dementia-£15,610 per person, compared to £2,880 per person -£15,610 per person, compared to £2,880 per person for non dementia. Total health and social care for for non dementia. Total health and social care for dementia cohort was £12m (25% of total budget) dementia cohort was £12m (25% of total budget) despite only accounting for just over 5% of despite only accounting for just over 5% of population.population.
Substance MisuseSubstance Misuse
•Define substance misuse cohort.•Use data from criminal justice and ADP services to augment data•Prevalence and population characteristics
•Size and distribution of spend.
•Comparative to non substance misuse population.
•Follow as service is redesigned.

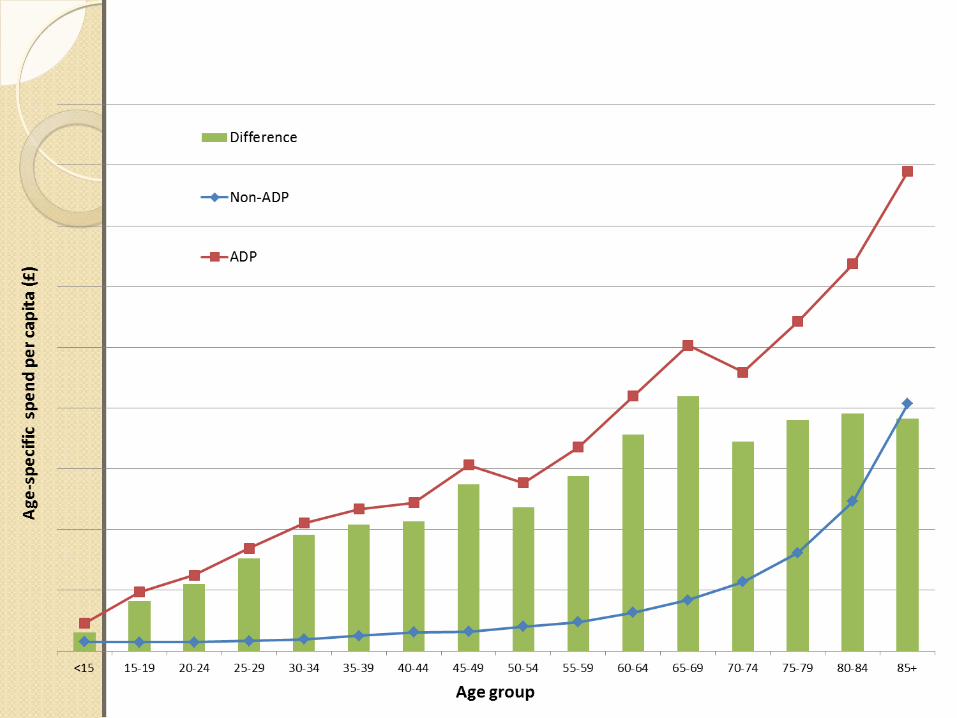
Breakdown of costs
Non-substance misuse:
Substance misuse:

Other examples of patient Other examples of patient (client level analysis(client level analysis
Anticipatory Care Plans.
Delayed Discharge.
High resource patient (clients).
Acute flow and capacity.

Question 3Question 3
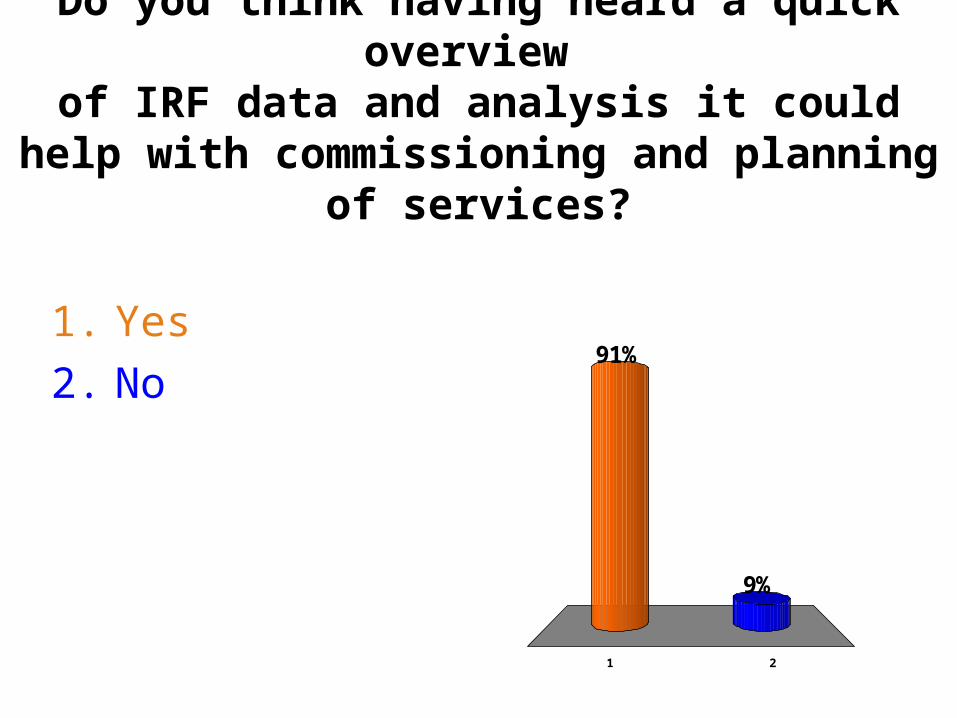
Do you think having heard a quick overview of IRF data and analysis it could help with commissioning and planning of services?
1 2
9%
91%1. Yes2. No

ConclusionsConclusionsDemonstrated the benefits of both
IRF mapping and patient level analysis for integration and planning services for future.
Happy to share IRF mapping data and patient level analysis.
Happy to answer questions/discuss how you could use analysis.
[email protected] 0131-244-3394
“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013

10.15Care
XMin
TimesActual arrival times
Planned Care
Client E 45 09.00 -
09.45 9.06
2 Carers required to meet at same time to support a young adult wheelchair user with multiple LCT's. The support is for all aspects of personal care, support and nutrition and to assist the individual to meet daily transport schedules to attend college
Client F 30 09.45 -
10.15 9.57
Personal Care for an older gentleman with moderate dementia, living with his wife, who has a LTC and has recently also been added to the package for support with medications. Their daughter who is the main carer for both parents is currently recovering from a serious illness.
Client G 60 10.15 -
11.15 10.29
Older gentleman known to the care service for 5 years, a stroke survivor, with reduced mobility and a history of falls with a recent # neck of femur. Staff have been integral to his return home and to his on-going rehabilitation. Following surgery the package of care has been slowly reduced in response to increasing independence.
“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013
Alex Neil MSPCabinet Secretary for Health and Wellbeing
“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013

“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013
“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013

“Home is Where the Care is”
Annual Conference and ExhibitionGlasgow Marriott Hotel
Friday 31st May 2013


















