Home Health Value Based Purchasing- 2016 and … B 115/Chris-Attaya... · • Massachusetts Eye &...
66
Home Health Value Based Purchasing – 2016 and Beyond Chris Attaya, VP Business Intelligence, SHP Rey Spadoni, President, Partners HealthCare at Home Sixth Annual New England Home Care & Hospice Conference and Trade Show May 17, 2016
Transcript of Home Health Value Based Purchasing- 2016 and … B 115/Chris-Attaya... · • Massachusetts Eye &...

Home Health Value Based Purchasing – 2016 and Beyond
Chris Attaya, VP Business Intelligence, SHP
Rey Spadoni, President, Partners HealthCare at Home
Sixth Annual New England Home Care & Hospice
Conference and Trade ShowMay 17, 2016

2
About the Partners HealthCare System
$11B health care system founded in 1994 by Brigham and Women's Hospital and Massachusetts General Hospital, Partners HealthCare System (PHS) includes community and specialty hospitals, a managed care organization, a physician network, community health centers, home care and other health-related entities.
• Per the US News 2015-16 Ranking:• Massachusetts General Hospital #1• Brigham & Woman’s Hospital #6• Spaulding Rehabilitation Hospital #6 Rehab• Massachusetts Eye & Ear #1 ENT• McLean Hospital #4 Psych
• A teaching affiliate of Harvard Medical School; national leader in biomedical research.
• Partners is the largest private employer in Massachusetts, with approximately 60,000 employees, including physicians, nurses, scientists, and caregivers.

About Partners HealthCare at Home
3
• $95m home health agency established in 2000 with the merger of 27 VNAs
• Certified home health care services, per year…• ADC 3,700• Admissions 27,000• Visits 470,000
• Private care services, per year• ADC 1,100• Hours 450,000
• Special programs
• Telemonitoring
• Mobile observation unit
• Wound care
• Infusion
• Pediatrics
• Enterprise technology platform: Epic (May 2015)

• Identify the components to Home Health Value Based Purchasing (HHVBP) defined in the Final Rule as well as lessons learned from the Hospital VBP program
• Illustrate the methodology for the calculating the Total Performance Score (TPS) and how to understand the current ratings and planning for improvement
• Identify the actions one agency addressed in operational and workflow considerations to be successful under HHVBP
Learning Objectives
4

Learning Objectives
5
• Identify the components to Home Health Value Based Purchasing (HHVBP) defined in the Final Rule as well as lessons learned from the Hospital VBP program
• Illustrate the methodology for the calculating the Total Performance Score (TPS) and how to understand the current ratings and planning for improvement
• Identify the actions one agency addressed in operational and workflow considerations to be successful under HHVBP

• CMS HHVBP Goals• OASIS, Claims and HHCAHPS Measures• New Measures• Piloted States Selection Criteria• Measure Points Scoring• Larger vs Small volume HHA Cohorts• Important Updates from CMS Q & A’s• HHVBP Connect Site
HHVBP Components
6

CMS is proposing the use of quarterly performance reports, annual payment adjustment reports, and annual publicly-available performance reports as a means of developing greater transparency of Medicare data on quality and aligning the competitive forces within the market to deliver care based on value over volume
CMS HHVP Goals
7

Measures by NQF Domain
DOMAINS
1) Patient and Caregiver centered experience 2) Clinical Quality of Care
3) Communication & Care Coordination 4) Population Health
5) Efficiency and cost reduction 6) Safety
8

9
• Each of these new measures will need to be reported by HHAs through a Web Portal starting with Q3 data
New Measures
Measure Measure Type Notes
Influenza Vaccination Coverage
for Home Health Care
Personnel
Process % HHA personnel received or documented not received – medical condition, received elsewhere, declined, unknown. Need to have worked 1 day Oct 1 to March 31st
Herpes zoster (Shingles)
vaccination: Has the patient
ever received the shingles
vaccination?
Process # of Medicare beneficiaries over 60 that ever received shingles vaccine
Advanced Care Plan Process Patients over 18 with plan or discussed with patient (no surrogate or plan made)

10
Review and understand the numerator and denominator values before starting data collection
New Measures for the Portal
• Do not wait to start collecting even though they are not due to be submitted until October 7th, 2016
• Centralize the collection and reporting within your organization
• Conduct your own dry run to ensure you have the data available and ready to enter into the Portal
• Plan to enter a least a week before they are due to make sure there are no glitches!

Example of Herpes Zoster
• 13 questions need to be collected in this example
11

• Domains into Classifications
Domains into Classifications
Classification IClinical Quality of
Care
Classification IIOutcome & Efficiency
Classification IIIPerson & Care-giver-Centered
Experience
Classification IVNew Measures
12

Randomly Selected States
Piloted State Selection Criteria
The 9 pilot states are: Massachusetts, Maryland, North Carolina, Florida, Washington, Arizona, Iowa, Nebraska, and Tennessee
Started with nine geographically-defined groupings of five or six states based on geographic, sample size and patient characteristics
13

14
Each Measure will have points scored based on the higher of an achievement score or improvement score
• Using the Base Year Period two calculations are set
• Threshold Value – 50th percentile (Median)
• Benchmark – Mean of the top decile (~95 percentile)
• Base Year (Calendar Year 2015) will not change
• Performance Years 2016 – 2020
• Each measure needs 20 or more episodes to be included in the total performance scores
• New Measures will be scored based on self reporting data only
Measure Points Scoring

• Measure Points Scoring (cont.)
Measure Points Scoring (cont.)
15

• Awarded by comparing an individual home health agency’s rates during the performance period with all home health agency’s rates from the baseline period
– Rate equal to or better than the benchmark: 10 points
– Rate less than the achievement threshold: 0 points
– Rate equal to or better than the achievement threshold and worse than the benchmark: 0 – 10 points
Measure Points Scoring (cont.)
Achievement Points – By Pilot State
16

• Awarded by comparing an individual home health agency’s (HHA’s) rates during the performance period with that same individual HHA’s rates from the baseline period.
– Rate equal to or better than the benchmark: 10 points
– Rate worse than the agency’s base year rate: 0 points
– Rate equal to or better than the agency’s base year rate and worse than the benchmark: 0 – 10 points
Measure Points Scoring (cont.)
Improvement Points – By Agency
17

• Measure Points Scoring (cont.)
Measure Points Scoring (cont.)
18

• Agencies reporting will be broken down in 2 Cohorts –Large: HHCAHPS Participant, and Small (Exempt from HHCAHPS due to <60 eligible patients in the calendar year)
• Intention to is group “like agencies” for performance reporting
Large vs. Small Agency Cohorts
19

• CMS quarterly will provide each agency with their scores• The first report will be available in July 2016 for the 2016 Q1 data
• Agencies will have the opportunity to contest their scores within 30 days of receiving
• Agencies will also have a chance to review their TPS and payment adjustments• August 1st first notification
• 30 days to request recalculation
• Final report no later than November 1, 2017
• Annual quality performance reports will be made publically available
Performance Reporting
20

21
Notable Answers:
• Information about the measures utilized in the first year of the HHVBP Model, including the measure specifications for the coordination of care and prior functioning measures will be presented during a webinar tentatively scheduled for January 2016.
• OASIS-based measures are calculated using assessments from the OASIS assessments from Medicare FFS, Medicare Advantage, Medicaid FFS, and Medicaid Managed care.
• All Medicare certified agencies in the 9 states are required to participate, even those with as few as 10 cases/year.
• CMS is compiling aggregate benchmark and achievement thresholds based on 2013 and 2014 data. Only the aggregate level Benchmarks and Achievement thresholds (by state and by cohort size) will be calculated using the 2013 and 2014 data.
CMS Q&A’s – Dec 2015
Source: https://innovation.cms.gov/initiatives/Home-Health-Value-Based-Purchasing-Model/faq.html

• HHVBP Connect: An interactive platform to learn more about the Model and collaborate with other HHAs• Find the latest updates for the HHVBP Model
• Download valuable resources to help you succeed in HHVBP
• View upcoming HHVBP events and key Model milestones
• Sole source for event registration
• Share best practices and “chat” with your colleagues in the nine Model states
• HHVBP Secure Portal• Where HHAs will submit data on new measures
• Where HHAs will retrieve quarterly and annual reports
HHVBP Connect Site
22

• HHVBP Connect Site – Landing Page
HHVBP Connect Site – Landing Page
23

HHVBP Base Line and Performance Periods
HHVBP Baseline and Performance Periods
24

25
What can we learn about this implementation?
• Has changed over time – The number of measures and domains have changed in each of the last 3 years since it’s inception, including Domain weighting
• HCAHPS also includes points for consistency if better than the 50th percentile in each of the Patient Experience dimensions
• The Bonus or Penalty is netted against the withholds in each year limiting the impacts on cash flow
• Unlike the Home Health Proposal, the Base year for Hospitals change every year by one year
Hospital Value Based Purchasing (HVBP)

• Measures and Domains
Hospital Value Based Purchasing (HVBP) (cont.)
26

• Identify the components to Home Health Value Based Purchasing (HHVBP) defined in the Final Rule as well as lessons learned from the Hospital VBP program
• Illustrate the methodology for the calculating the Total Performance Score (TPS) and how to understand the current ratings and planning for improvement
• Identify the actions one agency addressed in operational and workflow considerations to be successful under HHVBP
Learning Objectives
27

28
Total Performance Scoring
• CMS proposing that TPS and payment adjustments would be calculated based on an HHA’s CCN and therefore, based only on services provided in the selected states
• 21 OASIS/HHCAHPS/Claims based measures will be used in the TPS unless the an agency does not have 20 or more episodes per measure (Accounts for 90% of the score)
• Three New Measures will account for the 10% of the score
• If an HHA does not meet this threshold to generate scores on five or more of the Clinical Quality of Care, Outcome and Efficiency, and Person and Caregiver-Centered Experience measures, no payment adjustment will be made

• Total Performance Scoring (TPS) (cont.)
Total Performance Scoring (TPS) (cont.)
TPS Example (HHA 1)
29

Scores on 16 available OASIS/HHCAHPS measures = 88 Points
• HHA 1’s total possible points would be calculated by multiplying the total number of measures for which the HHA reported on least 20 (twenty) episodes by the maximum number of points for those measures ten (10), yielding a total of 160 possible points
• 88 points divided by the total 160 = .55
• .55 points X 90 = 49.5
• New Measures – all three entered equals 30 points out of a maximum of 30 = 1.0 X 10 points = 10 points
• Total Points = 59.5
30
Total Performance Scoring (TPS) (cont.)

• Each agency’s value-based incentive payment amount for a fiscal year will depend on:
• Range and distribution of agency total performance scores
• Amount of agency's base operating HHRG payment amount
• The value-based incentive payment amount for each agency will be applied as an adjustment to the base operating HHRG payment amount for each episode
Net Reimbursement Impacts
31

32
• CMS will use a linear exchange function (LEF) to distribute the available amount of value-based incentive payments to agencies, based on agency’s total performance scores on the HHVBP measures
Value-Based Purchasing (HHVBP)

CMS HHVBP Impact Reporting
CMS HHVBP Impact Reporting
• Distribution of the Payment Adjustments in the different model years
33

CMS HHVBP Impact Reporting (cont.)
CMS HHVBP Impact Reporting (cont.)
Example of HHA Large Cohort Payment Adjustments
34

LEF Distribution Examples
LEF Distribution Examples
35

• LEF Distribution Examples (cont.)
LEF Distribution Examples (cont.)
36

• LEF Distribution Examples (cont.)
LEF Distribution Examples (cont.)
37

LEF Distribution Examples (cont.)
38

LEF Distribution Examples (cont.)
39

40
Create Financial Baseline
• Meet with Operations and Quality to determine first pass at “what if” criteria for change on each measure.
• Using TPS computed, work through calculations in the Linear Exchange function to determine financial impact/risk for this first pass of assumptions.
• Create variation examples within each domain and across domains taking into consideration clinical team variation in scoring, resources needs ~ what’s a “heavy lift” and areas needing immediate or critical focus for the organization.
• Develop a table of each iteration recording results on assumptions on each measure, TPS and related financial impact. Share results with Operations and Quality team to help focus initiatives.

• Develop or obtain a tool to organize data for easy reference to domain, measure, data sources etc.
• Verify data from all sources
• Insert proxy data for any missing variables
• Achievement, Threshold and Benchmark will change as all agencies innovate for improvement
The Foundation of Analysis is Accurate Data
41
Measure Threshold Benchmark What ifAchv.
Pts.
Imprv.
Pts.Final Pts.
87.0 86.0 91.0 88.0 4.100 2.000 4.100
85.0 85.0 93.0 86.0 1.625 0.750 1.625
85.0 85.0 93.4 86.0 1.571 0.690 1.571
79.0 83.0 93.7 80.0 - 0.180 0.180

Financial Risk Estimates - PHH
42
AgencyMedicare
Budget
Payment Adjustment Distribution
Estimated Payment Adjustment
if TPS = 35 If TPS = 55 If TPS = 75
CY2016 $63,432,660 3% ($342,436) $190,298 $922,945
CY2017 $66,604,294 5% ($589,448) $329,691 $1,605,163
CY2018 $69,934,508 6% ($755,293) $419,607 $2,035,094
Estimated TPS Distribution for Agency Cohort
10 20 30 40 50 60 70 80 90 100
*actual adjustment % will change with cohort distribution and annual % distribution
*
*

• Identify the components to Home Health Value Based Purchasing (HHVBP) defined in the Final Rule as well as lessons learned from the Hospital VBP program
• Illustrate the methodology for the calculating the Total Performance Score (TPS) and how to understand the current ratings and planning for improvement
• Identify the actions one agency addressed in operational and workflow considerations to be successful under HHVBP
Learning Objectives
43

44
Government payers payment reform and quality timeline
10/1/2012: Value Based Purchasing (VBP) begins; Readmissions Penalty begins
10/1/2014: Hospital Acquired Conditions penalty begins 1/1/2015: Physician Value-Based Payment Modifier 3/2015: Next Generation ACO announced SGR repeal ties a greater share of physician payment to quality
10/1/2007: Pay for Performance begins
10/1/2011: Readmissions Penalty begins Health Policy Commission material changes/market reviews
• 1.0% VBP withhold
• 1.0% max readmission penalty
• 1.25% VBP withhold
• 2.0% max readmission penalty
• 1.5% VBP withhold
• Addition of VBP Efficiency Domain
• 3.0% max readmission penalty onwards
• Physician Value Based Payment Modifier in effect for some MDs
• 1.75% VBP withhold
• Medicaid F2F• HHVBP• IMPACT Act• Discharge COP
• 2.0% VBP withhold onwards
• Physician Value Based Payment Modifier in effect for all MDs
Goal of 50% of Medicare payments in alternative payment and/or population based payment by 2018
Site Neutral Payments (IP/OP; LTCH/IRF/SNF)
Short Stay payment reform Home Health Quality
Improvement Program Expansion of Shared Savings &
Bundled Payment Programs Expansion of quality measure
set for VBP, readmissions, HAC, inpatient psych, ESRD, condition specific Medicare Spending Per Beneficiary, etc
1/1/2012: Pioneer ACO and Medicare Shared Savings Programs begin; ESRD Quality Incentive Program begins; e-prescribing mandatory for MD’s
10/1/2013: Inpatient Psych Quality Reporting Program begins; Quality reporting for LTCHs and Inpatient Rehab Facilities begins
Phase I of Bundled Payments for Care Improvement Program begins July 2014: IOM Committee on GME Reform Report is published
10/1/2013: Primary Care Payment Reform Initiative (PCPRI) MassHealth ACO Request for Information Insurer calculation of enrollee out of pocket liability by provider
PCPRI: PMPM payment for PCP Services• Payment adjusted for quality • Shared Savings/Risk (optional) on total spend
Cost Trend Hearings TME / Relative Price Reporting
Increased oversight of insurance market
Continued expansion of quality measure set for P4P
Cap TME growth Medicaid inpatient psych bundled payment proposal MassHealth announced stakeholder sessions aimed at improvements /
new payment models; Downing Bill introduced
Federal FY09 FY10 FY11 FY12 FY13 FY14 FY15 FY16 FY17 [Future]
Care initiative for dual Medicare/Medicaid beneficiaries 1/1/2013: Mandate to increase penetration of alternate
payments from 25% to 80% by 1/1/15
1/1/2011: Center for Medicare & Medicaid Innovation (CMMI) established
State FY08 FY09 FY10 FY11 FY12 FY13 FY14 FY15 FY16 FY17 [Future]
3/2010: Passage of Affordable Care Act
Increasing Velocity of Change

Value-Based What? Our first reaction…
45
Please make it go away!

Value-Based What? Our second reaction…
46
What me worry?

Value-Based What? Our third reaction…
47

Goal is to synergize efforts
48
… while not muddling priorities and overcomplicating (e.g., case conferencing)

Action step sequence for PHH
49

• Where are our agency’s scores in relation to our stateaverages?
• Have we chosen the right comparison group?
• How have our quality and satisfaction scores improved over time?
• How does our Quality of Patient Care Star Rating compare to our state’s star ratings?
• Where do we have the best opportunity to improve our scores:– Process measures, Outcomes, HHCAHPs?
• Begin to drill down…
Take Stock of your Scores and PI Programs
50

How does Massachusetts compare to the Nation?
51
State
Nation
Outcomes Measures

• VBP Measures National vs. Massachusetts
VBP Measures National vs. Massachusetts
Source: HHC Scores Posted October 201552

Partners HealthCare at Home Outcomes 5 Star
53
Focus Areas
• Improvement in Pain
• Drug Education
• Flu Vaccine
• 60 Day Hospitalization

Partners HealthCare at Home HHCAHPs 5 Star
54

High Level Strategies
• ‘It takes a village’ – Improvement is everyone’s job
• Focus and data must be at the Team and Clinician Level
• Choose the highest bar (State, National, SHP) as your benchmark
• For Dashboards - Use ‘stoplight’ color coding with goal to ‘Get the Red Out’ – simplify reporting for impact
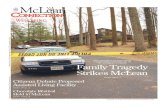
• Use Innovative Visuals like Tornado charts to drive home points like ‘Rate of Improvement’
55

Different Benchmarks for HHVBP and 5 STAR
Different benchmarks yield Different pictures
Compared to CMS National
Compared to SHP State
56

VBP/5-Star Rate of Improvement
Tornado Chart shows Rate of Improvement
57
-8.00 -6.00 -4.00 -2.00 0.00 2.00 4.00 6.00 8.00 10.00
Ambulation
Bed Transfer
Bathing
Pain Interfering w/ Activity
Dyspnea
Timely Initiation of Care
Drug Education All mEds in Short Tem EOC
Management of Oral Meds
Flu Vaccine Received - Current Season
PPV Received - Ever
Composite 1: Care of Patients
Composite 2: Comm Between Providers & Patients
Composite 3: Specific Care Issues
Universal 1: Gave the HHA a score of 9 or 10
Universal 2: Would recommend the HHA
0.20
0.40
-0.20
0.80
0.90
-1.70
0.90
0.70
-4.70
9.40
2.30
0.40
3.20
-0.20
0.50
0.30
0.60
0.30
0.30
0.30
0.10
0.30
0.50
-2.10
-0.80
0.00
0.00
1.00
1.00
0.00
2.10
3.90
2.20
2.00
2.20
0.50
1.20
4.00
-6.20
0.40
-0.40
-0.20
0.10
-0.40
-0.80
PHH Rate
StateCMS Rate
State SHPRate

• Clinical Managers, Quality, OASIS review and education staff all work together as a team• Identify team/clinician specific opportunities for improvement
• Education at the team and clinician level
• Monitor progress and provide ongoing ‘real time’ feedback• Re-educate as needed but not in perpetuity
• Performance management is critical
• Focus on entire spectrum from OASIS competency through to clinical practice – offer “Competency Days”
• Celebrate Improvements big and small
58
Education Strategies

59
Outcomes Improvement vs Stabilizationat Team and Clinician level
Education Strategies Using Data
Patient level detail
Room for improvement on one specific measure…
Room for improvement for one specific patient…

60
Education Strategies Using Data
HHCAHPs at Agency, Overall and Specific Question levelHH Provider
handled specific issues correctly
At SOC, did someone from agency talk with you about how to set up home?
About Rx and OTC?

Educational Approach
• OASIS Accuracy
• Skits/Videos demonstrating the ‘right’ and ‘wrong’ way to assess
• Home Care Institute ‘Room by Room’
• Fazzi ‘OASIS Walk’
• Improvement Concepts
• Improvement vs Stabilization
• Use of Dashboards and Tornado Graphs
61
• Care Planning and Goals
• InterprofessionalCollaboration
• Regular Case Conferencing
• Real Time Feedback from OASIS Reviewers
• Focus Topics

• Adding full-time resource to bridge between Quality/Education and Clinical Operations - based in Ops
• Help convert analysis, findings, strategies to action
• Help de-clutter multitude of priorities
• Support accountability orientation
Evaluating
62
ROI is compelling
Role tension

Re-assess as you go….
• Run quarterly sensitivity analysis and develop quarterly review sessions.
• As all HHA’s innovate to improve, the calculations remain dynamic.
• Check with corporate office concerning accounting ~ many hospital systems have experience and have developed standards for i.e. reserves for VBP and the associated timing. This could potentially play a role in future budget processes.
63

• Synergize efforts where possible (case conference should be targeted; multiple birds… one rock)• Culture change• Influence/change clinician
behavior; performance management
• Management discipline
• Convert analysis to action• Clinical managers need
specific strategies to work with individual staff
64
Lessons learned
• Reduce variation to allow for broader interventions
• Set it and forget it… NOT. Quarterly assessment meetings (iterative and learning process)
• Properly reserve so no P&L ‘surprises’
• Work with IT vendor (on new measures); start early as not all are preparing

Questions & Answers
65

66
Contact Information
Chris AttayaVP of Business IntelligenceStrategic Healthcare Programs (SHP)[email protected]: 805-963-9446Cell: 617-962-6950
Rey SpadoniPresidentPartners HealthCare at [email protected]: 781-290-4060