
HNHB LHIN Restorative Care Bed Review: Final Report and Recommendations
25
1 Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013 HNHB LHIN Restorative Care Bed Review: Final Report and Recommendations April 2013
Transcript of HNHB LHIN Restorative Care Bed Review: Final Report and Recommendations
1 Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
HNHB LHIN Restorative Care Bed Review: Final Report and Recommendations April 2013

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
2
Table of Contents
INTRODUCTION ...............................................................................................................................3
BACKGROUND ................................................................................................................................3
Project Scope and Objectives ........................................................................................................4
Process .............................................................................................................................................5
Rehabilitative Conceptual Framework .........................................................................................10
Applying the Methodology Phase 1 – Sizing of Restorative Beds ............................................12
RECOMMENDATIONS ...................................................................................................................17
APPENDICES
A. HNHB LHIN Alternate Level of Care (ALC) Steering Committee – Restorative Stream Working Group Terms of Reference
B. HNHB LHIN Restorative Stream Working Group Membership C. Restorative Bed Worksheet D. Restorative Data Review E. Complex Care Bed Numbers Post Implementation February 2013

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
3
INTRODUCTION
In November 2009, the Hamilton Niagara Haldimand Brant (HNHB) Local Health Integration Network (LHIN) completed an extensive population based planning study to develop a Clinical Service Plan (CSP) that would provide the foundation for strategies and activities to achieve improved outcomes and foster health system sustainability1. The CSP identified 18 clinical program areas where potential existed to develop LHIN-wide integrated programs2. Two areas for clinical program integration targeted in the first year of a three year plan were complex continuing care and rehabilitation. To complete this work two Task Groups were established; the Complex Care (CC) and the Rehabilitation Task Groups.
The HNHB LHIN Complex Care Task Group’s (Task Group) June 2009, final report proposed an integrated CC service model that included common definitions for CC and its sub streams and proposed a relatively new way of thinking about CC. In this model the CC bed was no longer intended as a “final destination” for the patient rather a plan of discharge was required on admission. Lengths of stay were targeted within a range of 45-90 days, with clear goals set, in order to enable appropriate care to be provided at home or at a different level (e.g., long-term care (LTC) or supportive housing). Key recommendations in the final report included an overall reduction of the HNHB LHIN’s CC bed capacity and recommended CC bed sizing by sub streams. To operationalize and implement the HNHB LHIN’s Integrated CC Program a Complex Care Implementation Steering Committee (SC) was established under the auspices of the HNHB LHIN Alternate Level of Care SC. It was expected that the CC program would be fully implemented by April 2012.
During the development and implementation of the Integrated Program for Complex Care in the HNHB LHIN a number of reports (Walker, Senior Friendly Hospitals) have been published on the readiness of the health care system to meet the needs of Ontario’s aging population. Current models of care were described as relying too heavily on the acute care hospital system that is designed for rapid diagnosis and management of serious illness. This system, for frail older seniors, can result in less than optimal outcomes and functional decline and a culture that emphasizes long term care placement rather than considering an older patients ability to recover sufficiently to return home3,4. Both reports recommend acute hospital care introduce strategies/care models that aim at preventing functional decline in older adults and supporting restorative programs that optimize their recovery.
BACKGROUND
During the implementation of the Integrated Program for Complex Care, the HNHB LHIN was also implementing a three year Action Plan to improve patient flow. The HNHB LHIN’s Action Plan (Action Plan) was based on the findings and recommendations of two patient flow reviews completed by PriceWaterHouseCoopers LLP and Dr. Walker’s ALC Action Team. A strong message resonated from both reports that a systematic change was needed in the planning and delivery of health care services to address the needs of an increasing aging population.
The HNHB LHIN’s Patient Flow Action Plan was developed to incorporate a culture that integrated a Home First philosophy and included initiatives that emphasized and promoted a culture where patients were always considered 1 HNHB LHIN Clinical Services Plan, November 2009 2 HNHB LHIN An Integrated Program for Complex Care, June 2010 3 Walker, Dr. David. Caring for Our Aging Population and Addressing Alternate Level of Care. June 30, 2011 4 Ontario LHINs. Senior Friendly Hospital Care Across Ontario Summary Report and Recommendations. September 2011

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
4
and assessed for programs that optimized their recovery allowing them to return home. The impact of the HNHB LHIN’s Action Plan was demonstrated in the reduction in number of individuals waiting in hospital for long term care (360 in 2010 to 135 in 2012), increased referrals to restorative programs (80% of 830 individuals were successfully discharged), discharged 1,350 individuals from hospital through Home First (341 received more than two hours of personal care per day), transitioned 129 individuals that accumulated 24,622 ALC days to the right level of care (LTC), and the Acute ALC rate reaching 12.94% - the lowest reported rate since 2007.
The HNHB LHIN was challenged with increased demand for restorative beds occurring in parallel to the implementation of the integrated complex care plan that recommended reduction of complex care beds. The change in how providers assess and determine care trajectories for our senior population following or prior to an acute care event in hospitals, has led to a fundamental change in our system. This recalibration has prompted the review of the Complex Care plan bed map of which was developed prior to the culture shift. A demand for restorative type programs, where seniors over a longer period of time than traditional rehabilitation programs, are given the opportunity to regain functional capacity to enable them to return home has risen.
Project Scope and Objectives In January 2012, the HNHB LHIN established the Restorative Stream Working Group to review the HNHB LHIN’s bedded restorative resources. The working group was comprised of individuals with expertise in restorative care, administration, planning, epidemiology and community care. The working group took into consideration the findings and recommendations from the Walker and Senior Friendly hospital reports; to reaffirm the number of inpatient restorative beds needed to meet the needs of individuals requiring restorative services prior to discharge from hospital now and in the next five years, and to provide clarity as to how the populations in the current restorative care beds differ. The HNHB LHIN Rehabilitation Task Group, in consideration of this review, put their work on hold pending the final report and key recommendations. The Restorative Stream Working Group was charged with the following goals, actions and deliverables:
Goals • To ensure individuals that require restorative care have timely access to these services, • To ensure bedded restorative resources are optimized by the appropriately streamed individuals, and • To have a clear understanding and ability to delineate between bedded restorative streams.
Actions
• Review population health data, Walker report, Senior Friendly Hospitals report and any other relevant reports,
• Determine the bedded restorative steams and needs for the HNHB LHIN population now and in the next five years (including sizing and siting) based on the population needs, best practices, and clinical outcomes.
Deliverables • Inventory of current and planned restorative beds in the HNHB LHIN. • Define and delineate bedded restorative streams. • Prepare a final report with recommendations for submission to the HNHB LHIN ALC Steering Committee.

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
5
For the Restorative Stream Working Group’s task, restorative beds were defined according to the following streams: • Restorative stream in Complex Care, • Debility, medically complex and geriatric stream(s) in Rehabilitation, • Convalescent care, • Assess and Restore, and • Slow Stream Rehab.
Terms of Reference and Membership are attached as Appendices A and B.
Process
Step 1 – Literature Review
The working group, as a starting point, reviewed relevant literature, which included Caring for Our Aging Population5, A Summary of Senior Friendly Hospital Care in the HNHB LHIN6, An Integrated Program for Complex Care in the HNHB LHIN7, and population health data. It was noted, in Caring for Our Aging Population report that an Assess and Restore philosophy and function must be central to health care delivery. Many frail seniors arrive at the ED could and should be directly transferred to the “Assess and Restore” programs delivered in either Complex Care or Rehab hospitals or in short-term/transitional programs in LTC. Similarly, patients designated ALC in acute care hospitals should have an opportunity to receive immediate “Assess & Restore” services in CC/Rehab or LTC settings, rather than waiting in hospital at risk of deterioration5.
Step 2 – Development of Methodology
The working group applied the methodological approach used in the Complex Care report to determine the LHIN’s restorative bed requirements. Adjustment factors incorporated into the methodology included existing information regarding best practices, advances in health care, care paths and clinical expertise. Refer to table 1 below.
5 Walker, D., (2011) Caring for Our Aging Population and addressing Alternate Level of Care, MOHLTC 6 Pizzacalla, A., Marr, S., (2011), A Summary of Senior Friendly Care in the HNHB LHIN. Regional Geriatric Program central 7 Pisko, L., et. all (2010) An Integrated Program for Complex Care in the HNHB LHIN

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
6
Table 1: Planning Methodology for Restorative Care Beds
Steps Adjustment Factors for Consideration
Description
Step 1 Determine current utilization
Outline current utilization of restorative beds.
Step 2
Adjust for changes in prevalence of health conditions
The purpose of including an adjustment changes in prevalence rates is to take into consideration significant changes that will impact demand for restorative services in the future.
Step 3 Address unmet need The purpose of including an unmet need adjustment is to take into consideration patients who are not currently receiving restorative services but meet the definitions and criteria.
Step 4
Address advances in health care
The purpose of including an adjustment for advances in health care is to take into consideration significant changes that will impact demand for restorative services.
Step 5 Address changes in scope of practice/delivery of health services
The purpose of including an adjustment for changes in the delivery of health services is to take into consideration significant changes that will impact demand for restorative services (e.g., shifts from inpatient to outpatient service).
Step 6 Adjust for population changes (growth and aging)
Adjust for population changes in the next 5 years by area of patient residence.
Step 7 Apply target length of stay
Apply target average length of stay.
Step 8
Apply target ALC (Alternate Level of Care) rate
Apply target ALC rate.
Step 9 Calculate bed equivalents Calculate bed equivalents by applying an occupancy rate. This calculation will provide bed numbers for restorative services in the HNHB LHIN based on population need by geographic area.
Step 3 – Snapshot and Data Analysis
To obtain a snapshot of the current state the Restorative Stream Working Group gathered information on restorative stream beds throughout the HNHB LHIN from a variety of settings to review the different programs according to bed type, staffing models, length of stay (LOS), admission/discharge criteria, discharge destination, percent of patients discharged home, and mean age of patients admitted into the program (Appendix C). A further review included an analysis of data from the National Rehabilitation Reporting System (NRS) for the debility / medically complex stream (Appendix D) and RAI (Resident Assessment Instrument) characteristics of the transitional care population which included: Assess and Restore, Assess, Restore and Reactivation, Slow Stream Rehab, Complex Care Restorative Stream, Convalescent Care, and Goldies2Home – an outpatient slow stream rehab program – refer to Table 2.
The Working Group’s reviewed the data on the characteristics of the populations that accessed the restorative programs and concluded that for the most part they were similar.
Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
7
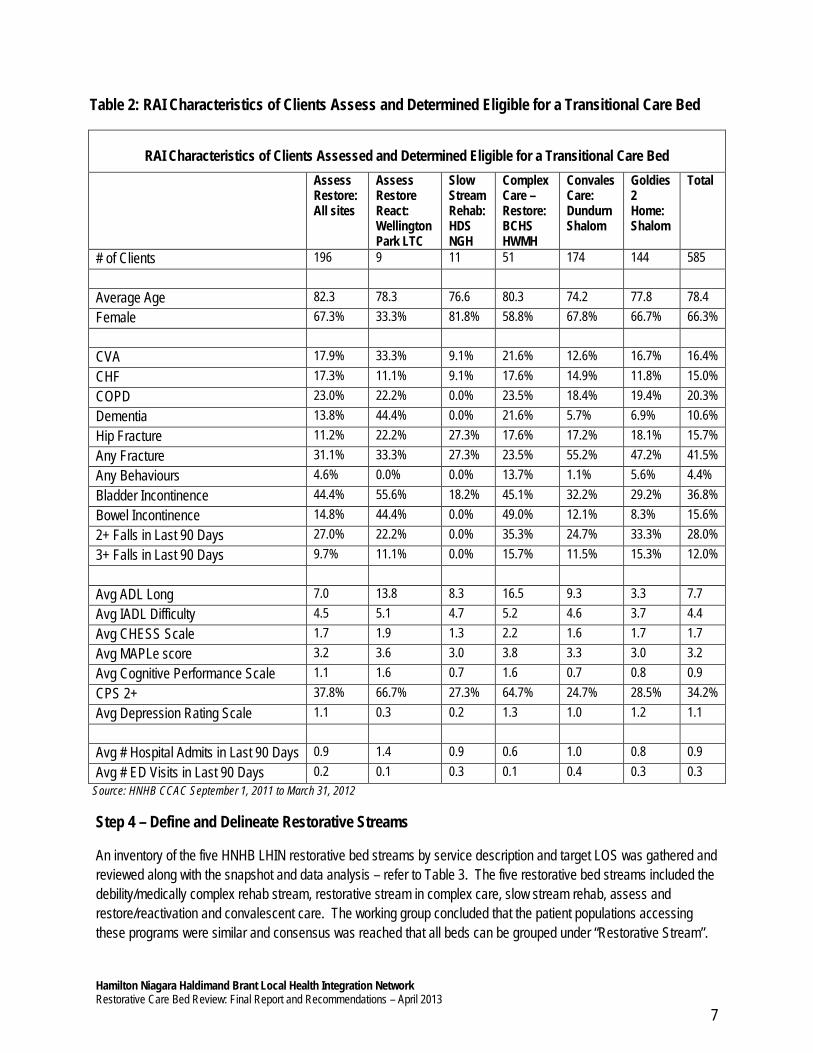
Table 2: RAI Characteristics of Clients Assess and Determined Eligible for a Transitional Care Bed
RAI Characteristics of Clients Assessed and Determined Eligible for a Transitional Care Bed
Assess Restore: All sites
Assess Restore React: Wellington Park LTC
Slow Stream Rehab: HDS NGH
Complex Care – Restore: BCHS HWMH
Convales Care: Dundurn Shalom
Goldies 2 Home: Shalom
Total
# of Clients 196 9 11 51 174 144 585 Average Age 82.3 78.3 76.6 80.3 74.2 77.8 78.4 Female 67.3% 33.3% 81.8% 58.8% 67.8% 66.7% 66.3% CVA 17.9% 33.3% 9.1% 21.6% 12.6% 16.7% 16.4% CHF 17.3% 11.1% 9.1% 17.6% 14.9% 11.8% 15.0% COPD 23.0% 22.2% 0.0% 23.5% 18.4% 19.4% 20.3% Dementia 13.8% 44.4% 0.0% 21.6% 5.7% 6.9% 10.6% Hip Fracture 11.2% 22.2% 27.3% 17.6% 17.2% 18.1% 15.7% Any Fracture 31.1% 33.3% 27.3% 23.5% 55.2% 47.2% 41.5% Any Behaviours 4.6% 0.0% 0.0% 13.7% 1.1% 5.6% 4.4% Bladder Incontinence 44.4% 55.6% 18.2% 45.1% 32.2% 29.2% 36.8% Bowel Incontinence 14.8% 44.4% 0.0% 49.0% 12.1% 8.3% 15.6% 2+ Falls in Last 90 Days 27.0% 22.2% 0.0% 35.3% 24.7% 33.3% 28.0% 3+ Falls in Last 90 Days 9.7% 11.1% 0.0% 15.7% 11.5% 15.3% 12.0% Avg ADL Long 7.0 13.8 8.3 16.5 9.3 3.3 7.7 Avg IADL Difficulty 4.5 5.1 4.7 5.2 4.6 3.7 4.4 Avg CHESS Scale 1.7 1.9 1.3 2.2 1.6 1.7 1.7 Avg MAPLe score 3.2 3.6 3.0 3.8 3.3 3.0 3.2 Avg Cognitive Performance Scale 1.1 1.6 0.7 1.6 0.7 0.8 0.9 CPS 2+ 37.8% 66.7% 27.3% 64.7% 24.7% 28.5% 34.2% Avg Depression Rating Scale 1.1 0.3 0.2 1.3 1.0 1.2 1.1 Avg # Hospital Admits in Last 90 Days 0.9 1.4 0.9 0.6 1.0 0.8 0.9 Avg # ED Visits in Last 90 Days 0.2 0.1 0.3 0.1 0.4 0.3 0.3
Source: HNHB CCAC September 1, 2011 to March 31, 2012
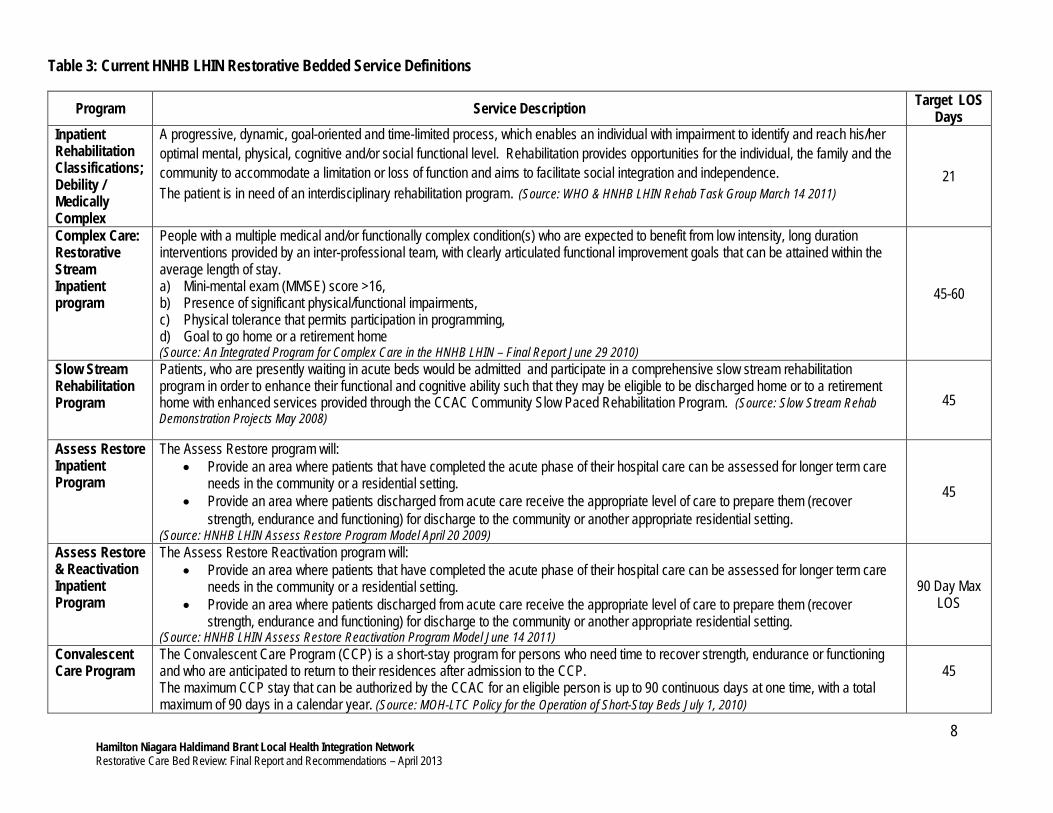
Step 4 – Define and Delineate Restorative Streams
An inventory of the five HNHB LHIN restorative bed streams by service description and target LOS was gathered and reviewed along with the snapshot and data analysis – refer to Table 3. The five restorative bed streams included the debility/medically complex rehab stream, restorative stream in complex care, slow stream rehab, assess and restore/reactivation and convalescent care. The working group concluded that the patient populations accessing these programs were similar and consensus was reached that all beds can be grouped under “Restorative Stream”.
8 Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
Table 3: Current HNHB LHIN Restorative Bedded Service Definitions
Program Service Description Target LOS Days
Inpatient Rehabilitation Classifications; Debility / Medically Complex
A progressive, dynamic, goal-oriented and time-limited process, which enables an individual with impairment to identify and reach his/her optimal mental, physical, cognitive and/or social functional level. Rehabilitation provides opportunities for the individual, the family and the community to accommodate a limitation or loss of function and aims to facilitate social integration and independence. The patient is in need of an interdisciplinary rehabilitation program. (Source: WHO & HNHB LHIN Rehab Task Group March 14 2011)
21
Complex Care: Restorative Stream Inpatient program
People with a multiple medical and/or functionally complex condition(s) who are expected to benefit from low intensity, long duration interventions provided by an inter-professional team, with clearly articulated functional improvement goals that can be attained within the average length of stay. a) Mini-mental exam (MMSE) score >16, b) Presence of significant physical/functional impairments, c) Physical tolerance that permits participation in programming, d) Goal to go home or a retirement home (Source: An Integrated Program for Complex Care in the HNHB LHIN – Final Report June 29 2010)
45-60
Slow Stream Rehabilitation Program
Patients, who are presently waiting in acute beds would be admitted and participate in a comprehensive slow stream rehabilitation program in order to enhance their functional and cognitive ability such that they may be eligible to be discharged home or to a retirement home with enhanced services provided through the CCAC Community Slow Paced Rehabilitation Program. (Source: Slow Stream Rehab Demonstration Projects May 2008)
45
Assess Restore Inpatient Program
The Assess Restore program will: • Provide an area where patients that have completed the acute phase of their hospital care can be assessed for longer term care
needs in the community or a residential setting. • Provide an area where patients discharged from acute care receive the appropriate level of care to prepare them (recover
strength, endurance and functioning) for discharge to the community or another appropriate residential setting. (Source: HNHB LHIN Assess Restore Program Model April 20 2009)
45
Assess Restore & Reactivation Inpatient Program
The Assess Restore Reactivation program will: • Provide an area where patients that have completed the acute phase of their hospital care can be assessed for longer term care
needs in the community or a residential setting. • Provide an area where patients discharged from acute care receive the appropriate level of care to prepare them (recover
strength, endurance and functioning) for discharge to the community or another appropriate residential setting. (Source: HNHB LHIN Assess Restore Reactivation Program Model June 14 2011)
90 Day Max LOS
Convalescent Care Program
The Convalescent Care Program (CCP) is a short-stay program for persons who need time to recover strength, endurance or functioning and who are anticipated to return to their residences after admission to the CCP. The maximum CCP stay that can be authorized by the CCAC for an eligible person is up to 90 continuous days at one time, with a total maximum of 90 days in a calendar year. (Source: MOH-LTC Policy for the Operation of Short-Stay Beds July 1, 2010)
45

9 Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
Step 5 – Inventory of Current Utilization of (February 2013) Restorative Programs by Geographical location and Bed numbers in comparison to the Identified Need of Restorative Stream beds in the 2010 Integrated Complex Care Program Report
A summary of the existing Assess Restore, Assess Restore Reactivation, Slow Stream Rehab, Convalescent Care and Complex Care Restorative beds as of February 2013 in comparison to the identified need of restorative stream beds in the 2010 HNHB LHIN Integrated Complex Care Program Report. See Table 4.
Table 4: Current Utilization of Restorative Beds as of February 2013 and the Identified Need for
Restorative Beds in the Complex Care Program Current Utilization of Restorative Beds in the HNHB LHIN – February 2013 Hamilton Burlington Brant Norfolk Haldimand Niagara Total Assess Restore 51 13 15 4 20 103
Assess Restore Reactivation
6 6
Slow Stream Rehab 10 15 25
Convalescent Care 35 35
Complex Care Restorative 44 30 19 * 6 121 220
Total 130 49 34 10 10 156 389 Identified Need for Restorative Beds – HNHB LHIN Complex Care Report 2010 Hamilton Burlington Brant Norfolk Haldimand Niagara Total
Total 80 28 19 9 6 79 221
Variance Between Current Utilization and Identified Need Hamilton Burlington Brant Norfolk Haldimand Niagara Total
Total 50 21 15 1 4 77 168 *Patients not admitted according to streams at the reporting time **Includes 13 restorative beds at the NHS- Niagara-on-the-Lake site for which implementation is on hold

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
10
Step 6 – Service Definition, Eligibility Criteria and Expectations of the Program
To bring clarity to the multiple programs that are currently classified as ‘restorative’ yet provide like services to similar populations the Restorative Stream Working Group developed a draft Service Definition, Eligibility Criteria and Expectations of the Program and chose to adopt the ‘Rehabilitative Conceptual Model’ presented by the Rehabilitation and CCC Expert Panel to frame detailed below. The application of the Framework to the LHIN’s restorative programs is shown in Table 5.
Rehabilitative Conceptual Framework8:
Foundational Principles • Early access to rehabilitative care should be equitable. • All patients should receive rehabilitation care to their level of tolerance with the goal of achieving maximum
functionality. • Every one of these services can be described or measured by data elements. • Every care service can be mapped to a CIHI NRS or CCRS category and to an OHRS category. • The care delivered to every category, cluster and in every location would be guided by best practices where
they exist. • All services would be delivered in an age appropriate manner (e.g. seniors focused, paediatric friendly). • Within each program or service there is flexibility to care for patients as their tolerance for treatment
changes to minimize transitions. • There is recognition that clustering patients with similar care needs leads to better outcomes.
Rehabilitative care is defined into four functional groupings. These categories are distinguished by the level of functioning of a patient combined with their capacity for restoring or maintaining function and their relative complexity. The determination of category is done at the time of transition from one destination to another using agreed-upon assessment tools. The four groupings are:
• Group 1: slow progress/low capacity for functional improvement • Group 2: slow to moderate progress/low to moderate capacity for functional improvement • Group 3: moderate to rapid progress/moderate to high capacity for functional improvement • Group 4: rapid progress/high capacity for functional improvement
8 Rehabilitation and Complex Care Expert Panel Update, December 9, 2011

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
11
Table 4: Application of the Rehabilitative Conceptual Framework to Current HNHB LHIN Restorative Programs
Group 1
Group 2 Group 3 Group 4
slow progress / low
capacity for functional improvement
slow to moderate progress / low to
moderate capacity for functional
improvement
moderate to rapid progress / moderate to high capacity for
functional improvement
rapid progress / high capacity for
functional improvement
Potential for Functional Improvement and/or attainable goals
LOW LOW / MOD MOD / HIGH HIGH
Risk of Deterioration HIGH HIGH HIGH LOW Complexity related to comorbidities HIGH LOW HIGH LOW
Complexity related to psychosocial factors LOW HIGH HIGH LOW
HNHB LHIN Programs Assess Restore Assess Restore
Reactivation
Assess Restore Slow Stream Rehab Convalescent Care
Complex Care – Restorative Stream
Inpatient Rehabilitation –
Deb/Med Complex Hospital Based Rehabilitation
Maximum LOS 90 days (Assess Restore, SSR)
90 days (Convalescent Care)
Target LOS 45 days 45 days 21 days Set by patients diagnosis and goal
Intensity of Therapy Minimum 1 – 3 hours per day
Minimum 1 – 3 hours per day
Minimum 3 hours / day
Greater than 3 hours / day
Level of Participation in Rehabilitation Therapies
Low 30 minutes to 1 hour
per day
Low to Moderate Typically 30 minutes to 2 hours per day
High Typically 3 hours per
day High
3 hours per day
Frequency of Physician Assessment
On admission and weekly follow up or as
clinically necessary
On admission and weekly follow up or as
clinically necessary Daily Daily

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
12
Recommendation #1 - The Restorative Stream Working Group recommends the following Definition, Eligibility and Expectations of the Program for groups 1 and 2 noted above. Definition Patients with multiple medical and/or functionally complex condition(s) who are expected to benefit from interventions provided by an inter-professional team, with clearly articulated functional improvement goals and/or, goals that address remediation of barriers to be discharged home Overall Eligibility Criteria
• 18 years of age or older • Needs daily skilled assessment by an inter-professional team • Requires 24/7 nursing care • Medically stable:
o The patient has completed the acute phase of illness o The major portion of diagnostic tests for the patient has been completed or the results of the
diagnostic tests will not affect participation in restorative program o Does not require daily physician visit
• Patients being considered for admission from an acute care hospital program have had their reason for their acute care visit defined, addressed and communicated to the patient.
• Presence of functional consequences of physical and/or cognitive impairment • Physical tolerance and cognitive ability that permits participation in programming • Clearly defined goals have been established (including a date of discharge). • Anticipated discharge to home or community setting (not including LTC)
Expectations of the Program
• Reasonable access to necessary consultations and appointments as required • Seen by most responsible health professional –physician, registered nurse extended class or physician
assistant - within accordance to the Public Hospitals Act and the Long Term Care Home Act. • Initial plan of care identified at time of admission • Access to full range of inter-professional team services (includes a core team and consulting services)
Applying the Methodology Phase 1 – Sizing of Restorative Beds
Step 1 – Determine Current Utilization of Restorative Care Beds
Incorporating the patient populations that utilize the Assess and Restore, Assess Restore Rehabilitation, Slow Stream Rehab, Convalescent Care, and Complex Care Restorative stream under one “Restorative” umbrella with a common new definition and eligibility criteria would facilitate the identification of individuals requiring restorative services and matching them with the appropriate resources in a timely manner. At this point the Restorative Stream Working Group noted that the population that accessed the debility/medically complex beds, while similar, experienced a shorted LOS. As such the Restorative Stream Working Group agreed to defer the sizing of these beds to the Rehab Task Group.

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
13
It is important to note that implementation of the Complex Care plan was not fully implemented at all sites which impacted the ability of some sites not being able to submit data. Based on the current bed map and utilization up to January 2013, an increased demand for Restorative streams has been noted, along with a decrease in demand for the Medically Complex Stream (Appendix E).
Step 2 – Adjust for Changes in Prevalence of Health Conditions
This methodology made the assumption that there would be no quantifiable change in the health status of the population over the next five years.
Step 3 – Address Unmet Need
The methodology includes an assumption that the unmet need is demonstrated by: • the continued demand and utilization of the assess restore, slow stream rehabilitation and convalescent care
capacity that were excluded from the complex care report; and • the average number of individuals ALC to restorative, convalescent care, LTLD (CC and Rehabilitation), AR and
SSR over a 24 month trend9. A review of data revealed approximately 48 patients per month across the HNHB LHIN were designated ALC to a restorative type program. A review of wait times for closed cases showed a median wait time for restorative type programs of approximately five days (January 16, 2013 data pull volume of closed cases 2054) Source WTIS ALC . This methodology did adjust for a wait time for the population waiting greater than the median wait time of five days. It is noted that ongoing monitoring will continue to be required due to the multiple changes occurring in the system.
Step 4 – Address Advances in Health Care
This methodology recognized a number of initiatives that are underway or being planned that are intended to have an impact on individuals preventing or reducing the degree of functional decline seniors experience during an admission to hospital. These include but are not limited to: falls prevention programs, senior friendly hospital initiatives, optimize use of ambulatory based or in home care over hospitalization e.g. hospital at home program, interRAI early intervention screener, and health promotion and wellness programs.
Step 5 – Address Changes in Scope of Practice/Delivery of Health Services
This methodology made the assumption that there will be a shift to move inpatient restorative programs to outpatient community based restorative programs and convalescent care resources in the community over the next five years. This shift together with the impact of initiatives to prevent or reduce the degree of functional decline the number of restorative inpatient beds will reduce the demand allowing for a reduction in restorative inpatient beds.
Step 6 – Adjust for Population Changes (Growth and Aging)
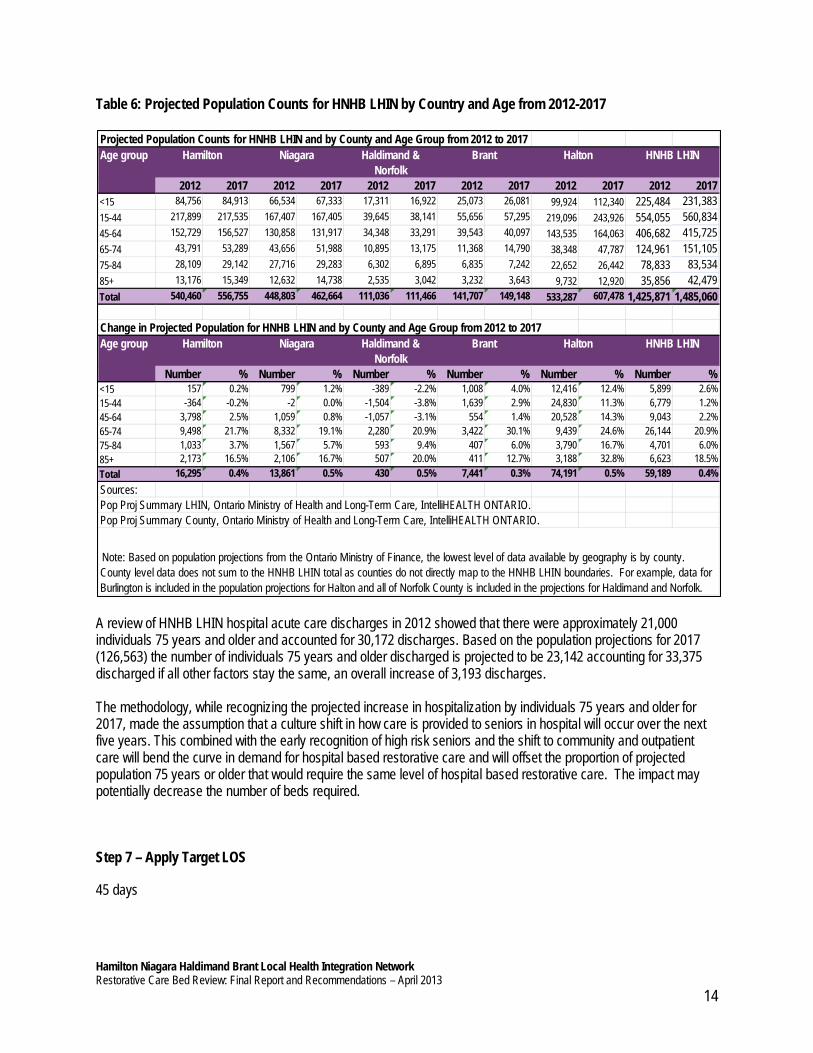
A review of population projections from 2012-2017 show that the overall HNHB LHIN population will increase by 59,189 - of which 11,324 will be 75 years or older (6,623 will be 85 years and older) – refer to Table 6. 9 HNHB LHIN ALCIS for Calendar years 2011 & 2012.
Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
14
Table 6: Projected Population Counts for HNHB LHIN by Country and Age from 2012-2017
A review of HNHB LHIN hospital acute care discharges in 2012 showed that there were approximately 21,000 individuals 75 years and older and accounted for 30,172 discharges. Based on the population projections for 2017 (126,563) the number of individuals 75 years and older discharged is projected to be 23,142 accounting for 33,375 discharged if all other factors stay the same, an overall increase of 3,193 discharges. The methodology, while recognizing the projected increase in hospitalization by individuals 75 years and older for 2017, made the assumption that a culture shift in how care is provided to seniors in hospital will occur over the next five years. This combined with the early recognition of high risk seniors and the shift to community and outpatient care will bend the curve in demand for hospital based restorative care and will offset the proportion of projected population 75 years or older that would require the same level of hospital based restorative care. The impact may potentially decrease the number of beds required.
Step 7 – Apply Target LOS
45 days
Projected Population Counts for HNHB LHIN and by County and Age Group from 2012 to 2017
2012 2017 2012 2017 2012 2017 2012 2017 2012 2017 2012 2017<15 84,756 84,913 66,534 67,333 17,311 16,922 25,073 26,081 99,924 112,340 225,484 231,38315-44 217,899 217,535 167,407 167,405 39,645 38,141 55,656 57,295 219,096 243,926 554,055 560,83445-64 152,729 156,527 130,858 131,917 34,348 33,291 39,543 40,097 143,535 164,063 406,682 415,72565-74 43,791 53,289 43,656 51,988 10,895 13,175 11,368 14,790 38,348 47,787 124,961 151,10575-84 28,109 29,142 27,716 29,283 6,302 6,895 6,835 7,242 22,652 26,442 78,833 83,53485+ 13,176 15,349 12,632 14,738 2,535 3,042 3,232 3,643 9,732 12,920 35,856 42,479Total 540,460 556,755 448,803 462,664 111,036 111,466 141,707 149,148 533,287 607,478 1,425,871 1,485,060
Change in Projected Population for HNHB LHIN and by County and Age Group from 2012 to 2017
Number % Number % Number % Number % Number % Number %<15 157 0.2% 799 1.2% -389 -2.2% 1,008 4.0% 12,416 12.4% 5,899 2.6%15-44 -364 -0.2% -2 0.0% -1,504 -3.8% 1,639 2.9% 24,830 11.3% 6,779 1.2%45-64 3,798 2.5% 1,059 0.8% -1,057 -3.1% 554 1.4% 20,528 14.3% 9,043 2.2%65-74 9,498 21.7% 8,332 19.1% 2,280 20.9% 3,422 30.1% 9,439 24.6% 26,144 20.9%75-84 1,033 3.7% 1,567 5.7% 593 9.4% 407 6.0% 3,790 16.7% 4,701 6.0%85+ 2,173 16.5% 2,106 16.7% 507 20.0% 411 12.7% 3,188 32.8% 6,623 18.5%Total 16,295 0.4% 13,861 0.5% 430 0.5% 7,441 0.3% 74,191 0.5% 59,189 0.4%Sources:Pop Proj Summary LHIN, Ontario Ministry of Health and Long-Term Care, IntelliHEALTH ONTARIO.Pop Proj Summary County, Ontario Ministry of Health and Long-Term Care, IntelliHEALTH ONTARIO.
HNHB LHIN
HNHB LHIN
Note: Based on population projections from the Ontario Ministry of Finance, the lowest level of data available by geography is by county. County level data does not sum to the HNHB LHIN total as counties do not directly map to the HNHB LHIN boundaries. For example, data for Burlington is included in the population projections for Halton and all of Norfolk County is included in the projections for Haldimand and Norfolk.
Age group Hamilton Niagara Haldimand & Norfolk
Brant Halton
Age group Hamilton Niagara Haldimand & Norfolk
Brant Halton

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
15
Step 8 – Apply Target ALC (Alternate Level of Care):
This methodology did not adjust of the ALC rate for acute and complex care. Acute 11% Complex Care ALC 17% It is important to note that the target ALC rates are overall HNHB LHIN rates and some sites have achieved an ALC rate below these, while others continue to be above the target rate. Recommendation #2: That LHIN hospitals continue to identify and implement strategies that will result in a sustainable ALC rate in Complex Care of 11% or lower.
Step 9 – Calculate Bed Equivalents
Target 95% occupancy Assumption – the unmet need is demonstrated by:
• Current restorative capacity located in Assess Restore and Slow Stream rehab programs located within permanent locations across the LHIN,
• Average number of individuals ALC to restorative programs that experience waits longer than five days, and • Assess Restore beds at St. Joseph’s Villa are located at a site that could not be considered permanent.

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
16
HNHB LHIN Restorative Bed Sizing
Steps Adjustment Factors for Consideration Description
Step 1 Determine current utilization
A review of existing restorative bed capacity and utilization identified: • 220 restorative beds in existing complex care beds at 90% occupancy • 134 AR/SSR beds at 91% occupancy • 35 Convalescent Care beds – assuming a 92% occupancy
Total = 389 Step 2
Adjust for changes in prevalence of health conditions
This methodology made the assumption that there would be no quantifiable change in the health status of the population over the next five years
Step 3 Address unmet need • 134 AR/SSR operational in 2012-2013. • 27 individuals waiting > five days for access to restorative beds for an
average LOS of 45 days10 equates to a 3.3 bed gap. Step 4
Address advances in health care
This methodology made the assumption that the impact of advances in health care would have a five year trajectory.
Step 5 Address changes in scope of practice/delivery of health services
This methodology did not adjust for the anticipated shift to community rehab.
Step 6 Adjust for population changes (growth and aging)
This methodology made the assumption that a culture shift in how care is provided to seniors in hospital will occur over the next five years. This combined with the early recognition of high risk seniors and the shift to community and outpatient care will bend the curve in demand for hospital based restorative care and will offset the proportion of projected population 75 years and older that would require the same level of bedded restorative care.
Step 7 Apply target length of stay Target average LOS is 45 days.
Step 8
Apply target ALC (Alternate Level of Care) rate
Apply target ALC rate - This methodology has not adjusted for the ALC target.
Step 9.
Calculate bed equivalents • 389 existing restorative capacity as noted in step 1 • + four beds to address wait list Total required restorative capacity = 393 (which is a gap of 14 beds) The 14 bed gap will be reduced by the following: • + 28 convalescent care beds approved in 2013-2014 • + five beds through adoption of a targeted occupancy rate of 92% • + nine based on the assumption that NGH’s restorative needs are being
currently in their SSR program Total required restorative capacity after adjustments = 351
As a result of the above adjustments, the system has excess capacity of 28 beds. Reducing the ALC rate in complex care to 11% will result in an additional 11 beds becoming available to the system for restorative care which will result in excess capacity of 39 beds.
10 Source: HNHB LHIN ALCIS & CCO WTIS Calendar Years 2011 & 2012

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
17
Assumptions:
• Occupancy of convalescent care beds is > 97%. • Occupancy rate reported by hospitals for their restorative beds reported on the CC implementation reports. • Restorative beds in CC are the beds hospitals have identified as restorative and are admitting by streams.
The HNHB LHINs Complex Care Report “An Integrated Program for Complex Care” released in June 2010, recommended the sizing of 221 restorative care beds and 141 medical complex beds.
Current utilization and demand for restorative care bedded programs demonstrate a need greater than that projected in the complex care report. Current restorative beds operating in complex care (393 vs. 220) demonstrate a gap of 173 beds. Assuming the continued operation of AR/SSR bed capacity of 124 beds and the 35 convalescent care beds, the gap is reduced to 14 beds. The 14 bed gap will be further reduced by the following:
• + 28 convalescent care bed s coming into the system in 2013-14 • + 5 beds through adoption of a targeted occupancy rate of 92% • + 9 based on the assumption that NGH’s restorative needs are being currently in their SSR program
As a result of the above adjustments the system has excess capacity of 28 beds. Note: these numbers have not been adjusted for the 13 beds at NHS – that are currently on hold. Reducing the ALC rate in complex care to 11% will result in an additional 11 beds available to the system for restorative care and will result in excess capacity of 39 beds.
RECOMMENDATIONS
Recommendation #1 - The Restorative Stream Working Group recommends the following Definition, Eligibility and Expectations of the Program for Groups 1 and 2. Patients with multiple medical and/or functionally complex condition(s) who are expected to benefit from interventions provided by an inter-professional team, with clearly articulated functional improvement goals and/or, goals that address remediation of barriers to be discharged home Overall Eligibility Criteria:
• 18 years of age or older • Needs daily skilled assessment by an inter-professional team • Requires 24/7 nursing care • Medically stable:
o The patient has completed the acute phase of illness o The major portion of diagnostic tests for the patient has been completed or the results of the
diagnostic tests will not affect participation in restorative program o Does not require daily physician visit
• Patients being considered for admission from an acute care hospital program have had their reason for their acute care visit defined, addressed and communicated to the patient.
• Presence of functional consequences of physical and/or cognitive impairment • Physical tolerance and cognitive ability that permits participation in programming • Clearly defined goals have been established (including a date of discharge). • Anticipated discharge to home or community setting (not including LTC)

Hamilton Niagara Haldimand Brant Local Health Integration Network Restorative Care Bed Review: Final Report and Recommendations – April 2013
18
Expectations of the Program:
• Reasonable access to necessary consultants and appointments as required • Seen by most responsible health professional –physician, advances practice nurse - within 24 hours of
admission to the program and in accordance to the Public Hospitals Act and the Long Term Care Home Act. • Initial plan of care identified at time of admission • Access to full range of inter-professional team services (includes a core team and consulting services)
Recommendation #2: That LHIN hospitals continue to identify and implement strategies that will result in a sustainable ALC rate in Complex Care of 11% or lower. Recommendation #3: That each individual LHIN restorative program aims for an occupancy target of 95%. Recommendation #4 That LHIN’s current restorative capacity be monitored for demand and utilization on a quarterly basis. Increases in demand must be evaluated against hospital’s performance on implementing strategies to reduce cognitive and functional decline.

Appendix A
Hamilton Niagara Haldimand Brant (HNHB) Local Health Integration Network (LHIN)
Alternate Level of Care (ALC) Steering Committee - Restorative Stream Working Group Terms of Reference - January 27 2012
Purpose: To review the LHIN’ s bedded restorative resources, taking into consideration the findings and recommendations from the Walker and Senior Friendly hospital reports; to reaffirm the number of inpatient restorative beds needed to meet the needs of individuals requiring restorative care services prior to discharge from hospital now, in the next 5 years and to provide clarity as to how the populations in the current restorative care services differ. For this working group restorative beds are defined in these streams: restorative stream in complex care, debility, medically complex and geriatric stream(s) in rehab, convalescent care, assess restore, and slow stream rehab. Goals:
To ensure individuals that require restorative care have timely access to these services.
To ensure bedded restorative resources are optimized by the appropriately streamed individuals.
To have a clear understanding and ability to delineate between bedded restorative streams.
Actions:
Review population health data, Walker report, Senior Friendly Hospitals report and any other relevant reports.
Determine the bedded restorative streams and needs for the HNHB LHIN population now and in the next 5 years (including sizing and siting) based on population needs, best practices, and clinical outcomes.
Deliverables:
Inventory of current and planned restorative beds.
Define and delineate bedded restorative streams.
Prepare a final report with recommendations for submission to the HNHB ALC Steering Committee. Membership: Working group membership is comprised of decision makers from a variety of post-acute restorative care settings, including: Assess & Restore, Slow Stream Rehab, Convalescent Care, Complex Care, Rehab and the HNHB LHIN. Members:
2 members from HNHB LHIN Assess/Restore SSR Committee
2 members from HNHB LHIN Complex Care task force
4 members from HNHB LHIN Rehab Task Group
1 member from Convalescent Care Program
1 member from CCAC if not already identified
Complex Care Coordinator
Geriatrician Ex officio:
Patricia Ciccarelli, Director, Finance, HNHB LHIN
Rosalind Tarrant, Director, Access to Care, HNHB LHIN

Kelly Cimek, Epidemiologist and Information Controller, HNHB LHIN
Shirley Stewart, Advisor, Health System Transformation, HNHB LHIN
Cheryl Cullimore, Advisor, Access to Care, HNHB LHIN Reporting Relationship and Membership Accountabilities:
Working group will be accountable to the ALC Steering Committee
Working group members represent their committee and their expertice with respect to decisions made by the group.
Members are responsible for attending meetings, advising on items presented for discussion, reviewing and providing feedback on materials as distributed.
The working group will be required to report back monthly to the ALC Steering Committee regarding their progress. Decision Making: The working-group decision will be based on consensus. If consensus is not possible, the chairperson may call a vote. Decisions arrived at by voting will be recorded with the percentage in favor of the decision and the content of any opposing positions. Decisions by consensus or vote require a quorum, set at 50% of working group members. Meetings:
Working-group meetings will be scheduled bi-weekly. Frequency may be changed by the chairperson to meet objectives set out in these terms of reference.
The meetings will continue for a period of two to three months, from January 2012 to February 2012, at which time the objectives set out are to be met.
February 2012
Appendix B
Hamiltion Niagara Halimand Brant (HNHB) Local Health Integration Network (LHIN)
Restorative Stream Bed Working Group
Membership list
Jennifer Kodis Rehab Task Group HHS
Lina Rinaldi Rehab Task Group BCHS
Jane Loncke - CHAIR CC Task Force SJHH
Jane Rufrano CC Task Force HDS
Kathryn Leatherland Assess Restore CCAC
Heather Patterson Assess Restore NHS
Michelle Draper Convalescent Care & LTC Shalom Village
Nesathurai Dr. Shanker Rehab Task Group Physiatrist
HHS
Ciccarelli, Patricia Finance HNHB LHIN
Cheryl Cullimore Access to Care HNHB LHIN
Shirley Stewart Health System Transformation HNHB LHIN
Kelly Cimek Epidemiologist/Information Controller HNHB LHIN
TBA Geriatrician
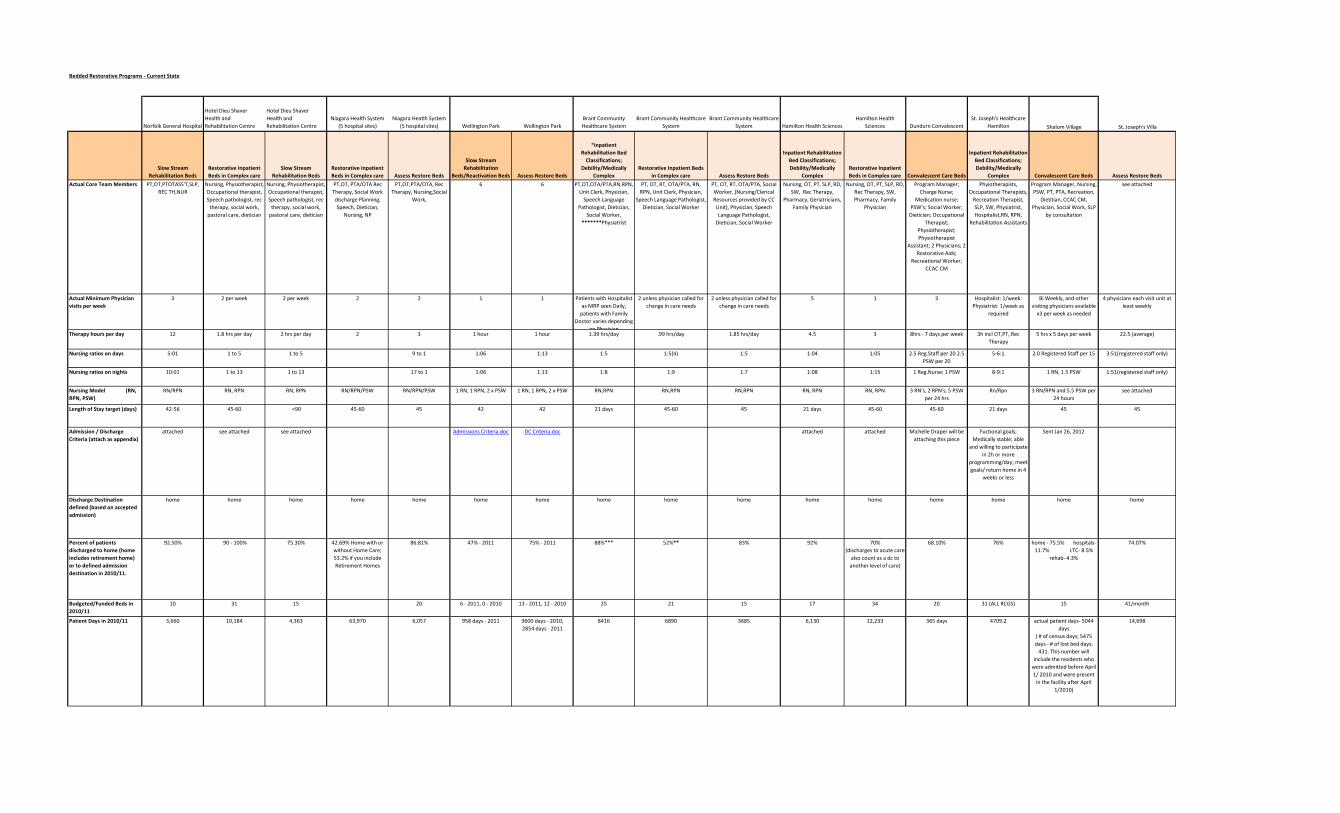
Bedded Restorative Programs - Current State
Norfolk General Hospital
Hotel Dieu Shaver
Health and
Rehabilitation Centre
Hotel Dieu Shaver
Health and
Rehabilitation Centre
Niagara Health System
(5 hospital sites)
Niagara Heatlh System
(5 hospital sites) Wellington Park Wellington Park
Brant Community
Healthcare System
Brant Community Healthcare
System
Brant Community Healthcare
System Hamilton Health Sciences
Hamilton Health
Sciences Dundurn Convalescent
St. Joseph's Healthcare
Hamilton Shalom Village St. Joseph's Villa
Slow Stream
Rehabilitation Beds
Restorative Inpatient
Beds in Complex care
Slow Stream
Rehabilitation Beds
Restorative Inpatient
Beds in Complex care Assess Restore Beds
Slow Stream
Rehabilitation
Beds/Reactivation Beds Assess Restore Beds
*Inpatient
Rehabilitation Bed
Classifications;
Debility/Medically
Complex
Restorative Inpatient Beds
in Complex care Assess Restore Beds
Inpatient Rehabilitation
Bed Classifications;
Debility/Medically
Complex
Restorative Inpatient
Beds in Complex care Convalescent Care Beds
Inpatient Rehabilitation
Bed Classifications;
Debility/Medically
Complex Convalescent Care Beds Assess Restore Beds
Actual Core Team Members PT,OT,PTOTASS'T,SLP,
REC TH,NUR
Nursing, Physiotherapist,
Occupational therapist,
Speech pathologist, rec
therapy, social work,
pastoral care, dietician
Nursing, Physiotherapist,
Occupational therapist,
Speech pathologist, rec
therapy, social work,
pastoral care, dietician
PT,OT, PTA/OTA Rec
Therapy, Social Work
discharge Planning,
Speech, Dietician,
Nursing, NP
PT,OT,PTA/OTA, Rec
Therapy, Nursing,Social
Work,
6 6 PT,OT,OTA/PTA,RN,RPN,
Unit Clerk, Physician,
Speech Language
Pathologist, Dietician,
Social Worker,
*******Physiatrist
PT, OT, RT, OTA/PTA, RN,
RPN, Unit Clerk, Physician,
Speech Language Pathologist,
Dietician, Social Worker
PT, OT, RT, OTA/PTA, Social
Worker, (Nursing/Clerical
Resources provided by CC
Unit), Physician, Speech
Language Pathologist,
Dietician, Social Worker
Nursing, OT, PT, SLP, RD,
SW, Rec Therapy,
Pharmacy, Geriatricians,
Family Physician
Nursing, OT, PT, SLP, RD,
Rec Therapy, SW,
Pharmacy, Family
Physician
Program Manager;
Charge Nurse;
Medication nurse;
PSW's; Social Worker;
Dietician; Occupational
Therapist;
Physiotherapist;
Physiotherapist
Assistant; 2 Physicians; 2
Restorative Aids;
Recreational Worker;
CCAC CM
Phyiotherapists,
Occupational Therapists,
Recreation Therapist,
SLP, SW, Physiatrist,
Hospitalist,RN, RPN,
Rehabilitation Assistants
Program Manager, Nursing,
PSW, PT, PTA, Recreation,
Dietitian, CCAC CM,
Physician, Social Work, SLP
by consultation
see attached
Actual Minimum Physician
visits per week
3 2 per week 2 per week 2 2 1 1 Patients with Hospitalist
as MRP seen Daily,
patients with Family
Doctor varies depending
on Physician
2 unless physician called for
change in care needs
2 unless physician called for
change in care needs
5 1 3 Hospitalist: 1/week:
Physiatrist: 1/week as
required
Bi Weekly, and other
visiting physicians available
x3 per week as needed
4 physicians each visit unit at
least weekly
Therapy hours per day 12 1.8 hrs per day 2 hrs per day 2 3 1 hour 1 hour 1.39 hrs/day .99 hrs/day 1.85 hrs/day 4.5 3 8hrs - 7 days per week 3h incl OT,PT, Rec
Therapy
5 hrs x 5 days per week 22.5 (average)
Nursing ratios on days 5:01 1 to 5 1 to 5 9 to 1 1:06 1:13 1:5 1:5(4) 1:5 1:04 1:05 2.5 Reg.Staff per 20 2.5
PSW per 20
5-6:1 2.0 Registered Staff per 15 3:51(registered staff only)
Nursing ratios on nights 10:01 1 to 13 1 to 13 17 to 1 1:06 1:13 1:8 1:9 1:7 1:08 1:15 1 Reg.Nurse; 1 PSW 8-9:1 1 RN, 1.5 PSW 1:51(registered staff only)
Nursing Model (RN,
RPN, PSW)
RN/RPN RN, RPN RN, RPN RN/RPN/PSW RN/RPN/PSW 1 RN, 1 RPN, 2 x PSW 1 RN, 1 RPN, 2 x PSW RN,RPN RN,RPN RN,RPN RN, RPN RN, RPN 3 RN's, 2 RPN's, 5 PSW
per 24 hrs
Rn/Rpn 3 RN/RPN and 5.5 PSW per
24 hours
see attached
Length of Stay target (days) 42-56 45-60 <90 45-60 45 42 42 21 days 45-60 45 21 days 45-60 45-60 21 days 45 45
Admission / Discharge
Criteria (attach as appendix)
attached see attached see attached Admissions Criteria.doc DC Criteria.doc attached attached Michelle Draper will be
attaching this piece
Fuctional goals;
Medically stable; able
and willing to participate
in 2h or more
programming/day; meet
goals/ return home in 4
weeks or less
Sent Jan 26, 2012
Discharge Destination
defined (based on accepted
admission)
home home home home home home home home home home home home home home home home
Percent of patients
discharged to home (home
includes retirement home)
or to defined admission
destination in 2010/11.
92.50% 90 - 100% 75.30% 42.69% Home with or
without Home Care;
53.2% if you include
Retirement Homes
86.81% 47% - 2011 75% - 2011 88%*** 52%** 83% 92% 70%
(discharges to acute care
also count as a dc to
another level of care)
68.10% 76% home - 75.5% hospitals-
11.7% LTC- 8.5%
rehab- 4.3%
74.07%
Budgeted/Funded Beds in
2010/11
10 31 15 20 6 - 2011, 0 - 2010 13 - 2011, 12 - 2010 25 21 15 17 34 20 31 (ALL RCGS) 15 41/month
Patient Days in 2010/11 3,660 10,184 4,363 63,970 6,057 958 days - 2011 3600 days - 2010,
2854 days - 2011
8416 6890 3685 6,130 12,233 365 days 4709.2 actual patient days- 5044
days
( # of census days; 5475
days - # of lost bed days;
431. This number will
include the residents who
were admitted before April
1/ 2010 and were present
in the facility after April
1/2010)
14,698

Norfolk General Hospital
Hotel Dieu Shaver
Health and
Rehabilitation Centre
Hotel Dieu Shaver
Health and
Rehabilitation Centre
Niagara Health System
(5 hospital sites)
Niagara Heatlh System
(5 hospital sites) Wellington Park Wellington Park
Brant Community
Healthcare System
Brant Community Healthcare
System
Brant Community Healthcare
System Hamilton Health Sciences
Hamilton Health
Sciences Dundurn Convalescent
St. Joseph's Healthcare
Hamilton Shalom Village St. Joseph's Villa
Slow Stream
Rehabilitation Beds
Restorative Inpatient
Beds in Complex care
Slow Stream
Rehabilitation Beds
Restorative Inpatient
Beds in Complex care Assess Restore Beds
Slow Stream
Rehabilitation
Beds/Reactivation Beds Assess Restore Beds
*Inpatient
Rehabilitation Bed
Classifications;
Debility/Medically
Complex
Restorative Inpatient Beds
in Complex care Assess Restore Beds
Inpatient Rehabilitation
Bed Classifications;
Debility/Medically
Complex
Restorative Inpatient
Beds in Complex care Convalescent Care Beds
Inpatient Rehabilitation
Bed Classifications;
Debility/Medically
Complex Convalescent Care Beds Assess Restore Beds
ALC Days in 2010/11 0 not available not available 36,802 0 195 39.3%***** 0 197 2,004
75.8 days; 6 Clients: 1-
78 days; 2- 54days; 3-84
days; 4- 85 days; 5- 84
days; 6-70 days
We had a total of 1289
ALC days in our internal
rehab program for
2010/11. However, this
is for all rehab patients.
This is not available by
RCG grouping
90 days - These days
accounted for by 5
residents as follows:
20 days
3 days
17 days
26 days
24 days
N/A
Mean Occupancy Rate in
2010/11
73% 90% 79.6 in 2010/11
96.1 2011/12 9
months
96.80% 83.60% 90% 90% 92%********* 90% 67% 98.8% 98.6% 90% 73.85% (By Service all
RCG groups Data
Source: Finance
Occupancy File)
92.13% 98.22%
Bed Equivalents based on
95% Occupancy
10 30 14 184.5 17.5 24 20 11********** 18 35.3 beds 19 out of 20 13.6 14
Mean LOS in 2010/11 31days 45 47.3 34 (median = 20) 23.4 (median = 19.9) 59 days - 2011 55 days - 2010, 51
days - 2011
27*** 36.1 21.9 27 days 174.8 days 59.2 days; this has
increased since we have
been getting more
acutely ill referrals
24.4 50 days
( The mean LOS covers
residents admitted during
the period Apri 1/2010-
March 31/2011.
46
Total Number of Admissions
in 2010/11
97 not available 104 1,297 251 16 in 2011 65 in 2010, 55
in 2011
325 129 175 225 80 114 199 ( 193 discharges) 94 331
Age Range of Admissions not available 44 - 97 30 - 99 23-103 yrs 43-96 yrs 67 - 92 in 2011 39 - 99 in 2010, 58 -
97 in 2011
17-96*** 35-98** 36-97 57-100 40-92 41-95 22 yrs - 99 years 0-30 1
31-40 0
41-50 5
51-60 8
61-65 8
66-70 8
71-80 18
81-90 36
91-100 9
101-106 1
19-101years
Mean Age of Admitted
patients
not available 79.94 76.28 79.94 yrs 79.71 yrs 80 in 2011 79 in 2010, 81
in 2011
74*** 77** 80 84 73 75 74.5 76 N/A
Percent of Patients > 65
years of age
not available 89.42% 80% 86.18% 90.84 100% in 2011 90% in 2010, 96% in
2011
75%*** 83%** 88% 3% 26% 76% 83% (Data Source: 3M) 76.60% N/A
Percent of patients outside
local catchment area (eg
City/Town)
0 not available not available 41.12% (based on
outiside the local
catchment of each NHS
site)
0.92% (If you consider
the catchment area to
be Niagara Region)
3.5% ****** not available not available 12.5% 12% 4.40% Approx 10% (Data
Source: 3M)
Berniece called CCAC to
provide this information-
waiting for their call back
N/A
Budgeted/Funded Beds in
2011/12 in Operation
10 31 15 20 6 13 25 21 15 17 34 20 31 (ALL RCGS) 15 April-Aug-41 Sept-Mar -
51
Note: Catchment area
can only be determined
on direct admits and not
on transfers in from
GNG CC to GNG Assess
Restore
40.28% (if you consider
the catchment area to
be Niagara
Falls/Chippawa)
Notes:*All data provided is for all Rehab Inpatients, not only for Medically Complex or
Debility. **2010/11 Data Unavailable. Data is for the period of April 1, 2011 to
December 31, 2011. ***Based on 2010/11 NRS Data. ****Therapy Hours/Pt Days
*****ALC Days for Restorative Care alone are not available. Number represents the
percentage of Patient Days that are ALC for all CC Beds in 2010/11.
**********Bed Equivalents calculated based on 2010/11 Data. 2011/12 Occupancy
currently 93% as of Q3
*********Rate is not 100% due to beds blocked to accommodate patients in need of
********Therapy Staff, RN,RPN and Unit Clerk are Staffing Resources directly assigned
*******Physiatrist is the Chief of the Inpatient Rehab Program******Percentage of Patients outside of HNHB LHIN

Appendix D
2010/11 data Bed Type Therapy
Hours/patient/day
# admits Total
patient
days
Average
LOS
Mean age % patients
>=65 years
% patients
>=55 years
Age range %
discharged
to
home/place
of
residence
% outside
area
FIM at
admission
(average)
FIM at
discharge
(average)
FIM change
(average)
LOS
Efficiency
(average)
Average #
of Health
Condition
s
Most Common Pre-admit
Diagnoses
Avg RIW
from
Acute
Care Stay
Top Most
Responsible
Diagnosis from
Acute Care
Stay
Source:
BCHS Inpatient rehab deb/med comp 1.39 56 1,306 23 76 79 95 35-96 80.4 7 73.5 102.9 28.3 1.33 9.8 Essential hypertension, anaemia,
hyperlipidemia, urinary
incontinence
2.7 Renal failure,
tendency to fall
NRS
HHS Inpatient rehab deb/med comp 4.5 280 6,614 24 78 86 95 35-97 88.9 9 84.4 103.6 18.1 0.88 13.9Essential hypertension,
malaise/fatigue, hyperlipidemia,
tendency to fall
4.5 Neoplasm,
delirium,
cellulitis of
lower limb
NRS
JBMH Inpatient rehab deb/med comp 54 1,024 19 81 89 93 48-95 85.2 6 76.4 97.3 17.8 1.32 6.8Hypertensive heart disease,
tendency to fall, osteoarthrosis,
atherosclerotic HD
2.7 CHF, cellulitis
of lower limb,
circulatory/heart
disease
NRS
HDS Inpatient rehab deb/med comp 23 758 33 66 52 78 37-95 73.9 4 81.9 106.9 21.0 0.64 4.4 Essential hypertension, obesity 6.7 Sepsis/infection NRS
SJHH Inpatient rehab deb/med comp 3 188 4,564 24 75 85 90 22-99 77.1 16 86.0 104.6 16.7 0.84 7.7Malaise/fatigue, Essential
hypertension, Hyperlipidemia, Atrial
fib
5.8 Sepsis,
neoplasm,
COPD, renal
failure
NRS
NHS Assess Restore Beds 3 251 6,057 23 80 91 43-96 86.8 1 Site
BCHS Assess Restore Beds 1.85 175 3,685 22 80 88 36-97 83 Site
St. Joseph's Villa Assess Restore Beds 0.5 331 14,698 46 19-101 74.1 Site
HWMH (to date) Assess Restore Beds (data to date) 30 70 81 90 9 Site
Wellington Park Assess Restore Beds (2010 data) 1 65 3,600 55 79 90 39-99 75 Site
Wellington Park Assess Restore Beds (2011 data) 1 55 2,854 51 81 96 58-97 Site
Wellington Park SSR/Reactivation (2011 data) 1 16 958 59 80 100 67-92 47 Site
NGH SSR/Reactivation 97 3,660 31 92.5 0 partial FIM:
25%
improveme
nt
Site
HDS SSR/Reactivation 2 104 4,363 47 76 80 30-99 75.3 70.08 105.01 32.75 Site
Dundurn Convalescent Convalescent Care Beds 114 59 75 76 41-95 68.1 4 Site
Shalom Village Convalescent Care Beds 94 5,044 50 76 77 <30->100 75.5 Site
HDS Restorative Beds in Complex care 1.8 10,184 45 80 89 44-97 90-100 Site
BCHS Restorative Beds in Complex care 1.85 129 6,890 36 77 83 35-98 52 Site
HHS Restorative Beds in Complex care 3 80 12,233 175 73 74 40-92 70 12 Site
JBMH Restorative Beds in Complex care 281 15,268 54 80 82 18-101 68.7 0 Site
HNHB LHIN Restorative Data Review

HNHB LHIN Current Complex Care Bed Numbers – Appendix E Site MC-
Vent MC- Dialysis
MC- Bariatric
MC ABI MC Behavioural Health
End of Life Care
Restorative Care
Total Complex Care Beds
Change
HHS Hamilton 0 63 63 50 44 220
Report 13 29 63 35 80 220 -18
SJHH Hamilton 5 15 6 25 51
Report 5 15 6 20 46 -6
JBMH Burlington
6 12 30 48
Report 19 12 28 59 +23
BCHS Brantford
13 8 19 40
Report 13 8 19 40 -18
HWMH Dunnville
4 3 6 13
Report 4 3 6 13 0
NGH Simcoe 6* 3* 7* 16*
Report 6 3 9 18 +2
DMH Fort Erie 10 6 24 40
Report 4 30 34 -6
PCG Port Colborne
1 13 2 5 25 46
Report 5 30 5 40 -6
GNG Niagara Falls
3 7 5 4 17 36
Report 5 20 3 28 -8
WH Welland 4 10 2 9 2 3 5 35
Report 5 10 4 8 3 30 -5
NOTL Niagara on the Lake
2** 3** 13** 18**
Report 6 10 16 -2
HDS St. Catharine’s
46 5 31 82
Report 20 5 40 65 -17
WLMH Grimsby
1 1 6 8
Report 6 4 9 19 +3
Totals 9 25 12 0 205 72 103 227 653
Report Totals 10 25 10 13 141 113 95 221 628
* Bed numbers to be confirmed February 2013
** NOTL Complex Care implementation on hold


















